Vivasure Medical has announced the submission of a premarket approval application to the US Food and Drug Administration (FDA) for its PerQseal Elite vascular closure system for arterial procedures.
In a recent press release the company has stated that the submission builds upon the successful results of the PATCH study as well as positive clinical use in Europe, reinforcing the system’s potential safety and performance profile. In addition, the company received European CE mark approval for an expanded indication for PerQseal Elite covering large-bore venous closure. This follows its first CE mark approval in April 2025 for arterial procedures and positions PerQseal Elite as the first fully bioresorbable, sutureless solution in Europe for both arterial and venous access closure.
“With the increasing adoption of minimally invasive therapies in structural heart and electrophysiology procedures, managing large-bore access sites remains a critical consideration,” said Azeem Latib, section head and director of interventional cardiology and director of structural heart interventions at Montefiore Health System in New York City. “PerQseal Elite was designed to address the growing need with a novel, fully bioabsorbable approach and we look forward to further progress in the programme.”
Leveraging Vivasure’s PerQseal technology, the PerQseal Elite vascular closure system is designed for fully absorbable, sutureless closure following percutaneous cardiovascular procedures. Currently, there are no fully bioresorbable devices available on the market for closure following large-bore procedures. Moreover, unlike other current devices, PerQseal Elite does not require any pre-procedure steps, further simplifying the process.
“We are proud to advance PerQseal Elite through these two key regulatory milestones as part of our commitment to delivering next-generation technologies for large-bore vascular closure,” said Andrew Glass, chief executive officer of Vivasure Medical. “Achieving CE mark expansion for venous indications and submitting our premarket approval application are important steps toward making our fully absorbable, sutureless solution more broadly accessible, while continuing to build a strong foundation for global commercial growth.”
The PerQseal Elite vascular closure system is placed from inside the vessel, making deployment simpler and more controlled than conventional closure techniques and returning the vessel to its natural state without leaving materials like collagen, metal implants, or sutures behind.
Embolization has announced that it has received 510(k) clearance from the US Food and Drug Administration (FDA). TheNitinol Enhanced Device (NED) is a vascular embolization device intended for arterial and venous embolization in peripheral vasculature.
Vascular embolization is a minimally invasive procedure where a physician intentionally blocks a blood vessel using tiny materials such as coils, particles or glue. This stops bleeding, reduces blood flow to tumours, or prevents damage from abnormal blood vessels, and is often used instead of surgery because it’s safer, quicker to recover from and very precise.
Using proprietary shape-memory biocompatible polymers, Embolization’s coil devices achieve better vascular occlusion while minimising artifacts in computed tomography (CT) and magnetic resonance imaging (MRI) that occur with traditional metal devices.
Embolization’s development represents the next generation in embolic coils, says Jim Kasic, Embolization chief executive officer. “The 510(k) clearance—which gives the company the ability to market the device—is a defining moment and major step forward in bringing this important device to the medical community, and ultimately, to the patients who will benefit.”
Kasic notes that the NED will be the only polymer-based coil on the market; all other available coils are metal-based. “Our pre-clinical work has shown that the coils have substantially reduced imaging artifact, significantly outperforming competitive devices,” he says. The coils, he adds, are still radiopaque under fluoroscopy even though the CT/MRI imaging artifact is minimal.
Studies also show shorter occlusion times and tighter coil packs. “With fewer devices per procedure, lower recanalisation rates and lower manufacturing costs, I believe the Embolization coil will substantially replace existing metal options,” states Kasic.
Further detailing use of the NED, Kasic explains that peripheral vasculature conditions such as great saphenous insufficiency, renal aneurysm and other vessel anomalies require blocking the flow in the vein, artery or aneurysm to prevent further damage, and to promote alternative flow pathways and healing. Interventional radiologists use surgical ligation when open surgery is indicated, but minimally invasive insertion of a coil into the vasculature has become a common approach to avoid open surgery.
Cook Medical has initiated a Class I recall of its Beacon Tip 5Fr angiographic catheter.
This follows reports of tip separation that could result in serious injury or death. The recall, identified as the most serious type by the US Food and Drug Administration (FDA), involves the removal of affected devices from clinical and commercial use.
In its notification to customers, Cook advised immediate examination of inventory to identify and quarantine any unused affected devices. Distribution and use of the affected catheters must cease immediately. The manufacturer also stressed that the recall information should be communicated throughout relevant departments and to any third parties who may have received the devices.
Cook Medical initiated the recall after field complaints revealed that catheter tips were separating both before and during patient procedures. Tip separation poses significant clinical risks, including catheter fragmentation and embolization, which may lead to severe complications such as sepsis, vessel perforation, thrombosis, embolism, cardiac arrhythmia, or death.
To date, three serious injuries linked to this issue have been reported, with no associated deaths.
Beacon Tip catheters are used by trained physicians to facilitate angiographic procedures, which provide imaging of blood vessels. These devices are commonly employed in combination with vascular access sheaths and guidewires using standard interventional techniques.
Healthcare providers and consumers in the USA are encouraged to report any adverse reactions or quality concerns related to this device to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program.
Endovascular Engineering (E2) has completed patient enrolment in the pivotal cohort of its ENGULF trial, involving the Hēlo pulmonary embolism (PE) thrombectomy system.
The investigational device exemption study was carried out at 19 interventional cardiology, radiology, and vascular surgery centres in the USA.
E2’s system features a patented dual-action mechanism that combines aspiration with clot disruption. It is designed to treat PE, a serious condition where blood clots in the lungs.
A recent press release made by the company describes that the Flow Mitigation Technology integrated into the system aids physicians in clot removal while reducing the loss of blood, a critical aspect of PE treatment.
The Hēlo PE thrombectomy system is still an investigational device.
ENGULF national principal investigator at Piedmont Atlanta Hospital in Atlanta, USA Andrew Klein said: “The ENGULF trial represents an impressive journey of innovation during which E2 and investigators were able to introduce and evaluate several new technologies within the trial.
“It is an exciting and dynamic period of evolution in the use of mechanical thrombectomy to treat and manage our patients with this potentially fatal condition.”
E2 noted that PE remains a leading cause of cardiovascular mortality and disability, with present treatments often requiring a balance between safety and effectiveness. The study aims to show that the system can address both concerns.
E2 chief executive officer Dan Rose said: “Our physician partners, patient volunteers, and the E2 team share the common purpose of improving the treatment of PE.
“We believe the Hēlo System offers distinct advantages over the current standard of care, and now, we are one very large step closer to making this life-saving technology available to patients across the USA.”
In February, the company secured an oversubscribed US$42m in a series B financing round to advance the development of its Hēlo system, targeting venous thromboembolism (VTE).
AngioDynamics has announced the first patient has been enrolled in the RECOVER-AV clinical trial, a prospective, multicentre, international, single-arm study evaluating the AlphaVac multipurpose mechanical aspiration (MMA) F1885 system in the treatment of acute, intermediate-risk pulmonary embolism (PE).
The study follows the US Food and Drug Administration (FDA) 510(k) clearance of the AlphaVac F1885 system for the treatment of PE in the USA in April 2024 and its CE mark approval in Europe in May 2024. The RECOVER-AV trial is designed to evaluate the safety and efficacy of the AlphaVac F1885 system in support of its adoption in the global market, as well as to assess long-term functional outcomes for patients following treatment.
“The first patient enrolment in the RECOVER-AV trial marks an important step forward as AngioDynamics continues to grow its global clinical presence and commitment to evidence-based care,” said Laura Piccinini, senior vice president/general manager, cardiovascular and international. “With AlphaVac already 510(k)-cleared in the USA and CE-marked in Europe for PE, we’re investing in high-quality data focused on functional recovery and quality of life that will equip clinicians, payers, and patients with even greater confidence in the system’s safe, effective performance and help broaden access to life-saving PE treatment across Europe and the wider global market.”
The trial is enrolling patients with confirmed acute, intermediate-risk PE at up to 20 hospital-based sites in Europe, Canada, and Hong Kong. The primary safety endpoint is the incidence of adverse events by type and seriousness through 12 months. Patients will be followed for 12 months, with functional and quality-of-life outcomes assessed at 30 days and 12 months. Additional investigations, including cardiac magnetic resonance imaging (MRI) and exercise testing, will provide a more comprehensive assessment of the long-term recovery of patients after mechanical thrombectomy with the AlphaVac MMA F1885 system.
The RECOVER-AV trial is led by co-principal Investigators Erik Klok (Leiden University Medical Center, Leiden, The Netherlands) and Andrew Sharp (Mater Misericordiae Hospital and University College Dublin, Dublin, Ireland).
“Pulmonary embolism continues to be a leading cause of morbidity and mortality across Europe, underscoring the need for treatment strategies that are both safe and effective,” said Klok. “We’re pleased to collaborate with AngioDynamics to generate evidence that could help shape future standards of care for intermediate-risk PE patients.”
Aleksander Araszkiewicz (Poznan University of Medical Sciences, Poznan, Poland), completed the first procedure as part of the trial.
“Performing the first case in the RECOVER-AV study marks an important step forward in expanding treatment options for patients with intermediate-risk pulmonary embolism,” said Araszkiewicz. “The AlphaVac F1885 system offers a promising mechanical thrombectomy solution, and I’m encouraged by its ease of use and the immediate clinical results we observed. I look forward to continuing to contribute to this critical research as we work to improve outcomes for PE patients.”
This study builds on the results of the company’s US-based APEX-AV trial, which demonstrated that the AlphaVac F1885 system is safe and effective for use in intermediate-risk PE patients, with significant improvements in right ventricular function and reduction in clot burden.
The AlphaVac F1885 system received CE mark approval in May 2024 for the non-surgical removal of thrombi or emboli from the pulmonary arteries. The system is designed to support frontline treatment of PE and expand options for healthcare providers managing patients with life-threatening venous thromboembolism.
Gore has announced that the Gore Tag thoracic branch endoprosthesis (TBE) is now approved by the US Food and Drug Administration (FDA) for use in Zones 0 and 1, expanding its indication for the endovascular repair of lesions in the aortic arch and descending thoracic aorta while preserving flow to a single aortic arch branch vessel.
The device becomes the first off-the-shelf, single-branch thoracic endoprosthesis indicated across Zones 0, 1 and 2, enabling or expanding minimally invasive aortic repair of all lesions involving the arch, the company has stated in a recent press release.
“With broader indications, we can confidently address a wider range of complex arch pathologies using a trusted solution that streamlines procedure planning and—critically—helps improve patient outcomes,” said Michael Dake, national co-principal investigator of the Gore Tag TBE clinical trial. “Of the 77 patients enrolled in the Zone 0/1 pivotal trial, more than 90% were treated in Zone 0 with no instances of device migration or wire fracture through 12 months, as well as low rates of type I and III endoleak.”
For Zone 0 and 1 procedure, TBE provides an on-label alternative to open surgical repair and reduces the overall impact of procedures like sternotomy, cardiopulmonary bypass and circulatory arrest.
“We’ve seen firsthand how this technology can transform patient care,” said Himanshu Patel, national co-principal investigator. “With a less invasive approach, we can reduce a significant procedural burden on patients.”
For Gore’s Jason Belzer, Americas business leader, Medical Products Division, “The expanded indication equips physicians with a versatile solution for the challenges of treating aortic arch pathologies—with the backing of rigorous data and a track record of procedural success. We are excited that more patients will have access to this technology.”
First approved in the USA in May 2022, this new indication for the use of TBE in Zones 0/1 further demonstrates how Gore is advancing the care of complex aortic disease with minimally invasive approaches for patients.
New regulations have come into effect in the UK which place a greater emphasis on medical device manufacturers to monitor the safety and performance of their products.
The new Post-Market Surveillance (PMS) regulations came into effect from Monday (16 June) requiring device manufacturers to actively track the safety and performance of products already in use. The reforms, which are a part of a wider effort by the Medicines and Healthcare products Regulatory Agency (MHRA) to overhaul the UK’s medical device regulatory framework, are intended to identify potential safety issues earlier and to strengthen protection for patients and the public through faster responses to incidents and emerging risks.
The reform applies to all UKCA- and CE-marked devices placed on the market in Great Britain after 16 June. This includes in vitro diagnostic devices, active implantable medical devices as well as other technologies used in a clinical setting and within the home.
Manufacturers are now required to collect and assess real-world safety and performance data; report serious incidents to the MHRA within 15 days (previously 30); submit essential communications on patient safety (Field Safety Notices) to the MHRA for review before sharing with users; and provide PMS Reports or Periodic Safety Update Reports (PSUR) within three days of request. For higher risk devices, UK approved bodies will monitor these reports ensuring these products receive a higher level of scrutiny.
“As innovation in health technologies accelerates, regulation must keep pace,” Lawrence Tallon, chief executive of the MHRA said. “Today’s reform is a critical step in ensuring safety standards evolve alongside this progress. By strengthening oversight of device once they’re in use and setting clearer expectations for manufacturers, these new regulations provide a robust framework for identifying risks earlier and responding to protect patients.
“This represents an important milestone in our work in building a modern, responsive regulatory system—one that puts patient safety first, while also supporting innovation in life sciences and medical technologies across the UK.”
The introduction of new data analysis reporting requirements will apply to all medical devices but are particularly valuable for improving oversight of lower-risk devices, MHRA adds. These rules will require manufacturers to regularly summarise and assess device performance over time.
As well as the reforms on medical device surveillance, the UK government has this week announced plans to make it easier for individuals to volunteer to participate in clinical trials. Patients will be able to sign up to participate in trials via the National Institute for Health and Care Research (NIHR) Be Part of Research service on the NHS app, where they will be able to browse and select trials best suited to their interests and needs.
Eventually this will automatically match patients with studies based on their own health data and interests, sending them push notifications to their devices about relevant trials that they may wish to sign up to participate in.
NIHR is also launching a recruitment drive to find as many volunteers for trials as possible, including those from underrepresented groups including young people, Black people and people of South Asian heritage.
Inquis Medical has announced that its Aventus thrombectomy system has received 510(k) clearance from the US Food and Drug Administration (FDA) for an expanded indication to treat pulmonary embolism (PE).
The Aventus System is a next-generation mechanical thrombectomy platform developed in close collaboration with physicians to address critical limitations of current technologies.
“The FDA’s clearance of the Aventus system marks a major milestone for the company,” said Vahid Saadat, co-CEO of Inquis Medical. “It validates the tireless efforts of our team and the deep partnerships we’ve built with our physicians, all focused on solving long-standing challenges in clot removal. Aventus is uniquely designed to meet the needs of physicians treating this life-threatening condition quickly, effectively, and safely.”
The Aventus thrombectomy system was previously cleared by the FDA for use in the peripheral vasculature. Additionally, the Aventus clot management system received FDA clearance for use with the Aventus thrombectomy system to enable autologous blood transfusion, allowing reinfusion of filtered aspirated blood and supporting efficient, blood-conserving clot removal. This most recent clearance extends the platform’s indication to include the treatment of pulmonary embolism.
“Treating PE requires both speed and precision,” said Mojgan Saadat, co-CEO of Inquis Medical. “The Aventus platform is the only thrombectomy solution with integrated tissue-sensing technology that enables precision removal of large clot burdens while streamlining blood return and reducing procedural complexity, all in a single, integrated approach. Receiving this clearance in record time speaks to the strength of our clinical data, the quality of our regulatory submission, and the incredible work of the Inquis team. We’re thrilled to launch this technology and deliver a state-of-the-art solution to physicians on the front lines of saving lives.”
This regulatory milestone follows the successful completion of the AVENTUS pivotal trial, the first US investigational device exemption (IDE) study to evaluate aspiration thrombectomy with filtered blood reinfusion in intermediate-risk PE patients.
The trial demonstrated excellent safety and performance across a broad range of clinical settings, with no device-related major adverse events and rapid improvement in right heart strain. The results were presented as a late-breaking clinical trial at the 2025 Society of Cardiovascular Angiography and Interventions (SCAI) scientific sessions (1–3 May, Washington, DC, USA) and were simultaneously published in JSCAI.
STORM-PE is a first-of-its-kind clinical trial comparing computer assisted vacuum thrombectomy (CAVT™) using Penumbra’s Lightning Flash™ with anticoagulation versus anticoagulation alone in the treatment of acute intermediate-high risk pulmonary embolism
Penumbra has announced the completion of enrolment in the STORM-PE clinical trial.
The pivotal, prospective, multicentre randomised controlled trial enrolled 100 patients to evaluate computer assisted vacuum thrombectomy (CAVT) using Penumbra’s Lightning Flash plus anticoagulation versus anticoagulation alone for the treatment of acute intermediate-high risk pulmonary embolism (PE).
“This is an important milestone that underscores Penumbra’s commitment to transforming care for patients with pulmonary embolism,” said James F Benenati, chief medical officer at Penumbra. “The trial successfully randomised patients well ahead of schedule thanks to the dedication of our clinical partners and the tireless efforts of our internal teams.”
Conducted in partnership with The PERT Consortium, a multidisciplinary group dedicated to improving the care of patients with PE, the trial aims to provide high-quality evidence on the role of CAVT in improving right heart function and clinical outcomes in this critically ill patient population.
“Pulmonary embolism remains a leading cause of cardiovascular morbidity and mortality, yet treatment strategies for intermediate-high risk patients are not well defined.” said Rachel Rosovsky, co-global principal investigator of STORM-PE and haematologist at the Massachusetts General Hospital. “The results of this trial will provide level 1 clinical evidence aimed at informing treatment guidelines and patient care.”
“We are pleased to announce that STORM-PE has successfully completed enrolment,” said Robert Lookstein, co-global principal investigator and professor of radiology and surgery at the Icahn School of Medicine at Mount Sinai in New York, USA. “We congratulate all the sites and the investigators for their dedication and commitment to answering the critical clinical question of whether endovascular therapy with CAVT is superior to medical therapy for acute intermediate-high risk pulmonary embolism.”
Penumbra’s Lightning Flash portfolio is the most advanced mechanical thrombectomy system on the market to address venous and pulmonary thrombus, states the company in a recent press release. It features Penumbra’s Lightning CAVT technology with the latest dual clot detection algorithms, using both pressure and flow-based processes to detect blood clot and blood flow.
The Lightning Flash catheter is made with MaxID hypotube technology, allowing an inner diameter similar to large-bore catheters while maintaining a lower profile and a soft, atraumatic tip design. They are designed to help remove blood clots with speed, safety and simplicity, allowing physicians to better navigate the body’s complex anatomy and deliver high power aspiration for clot removal, the company state.
David Madoff (Yale School of Medicine, New Haven, USA) highlights how syngo DynaCT and Embolization Guidance on the ARTIS icono system enhance tumour targeting in liver embolization.
Maximilian de Bucourt (Charité–Universitätsmedizin, Berlin, Germany) showcases how myNeedle Guide with integrated laser cross supports a wide range of percutaneous procedures by enabling precise, low-radiation needle placement.
Thomas Albrecht (Vivantes Klinikum Neukölln, Berlin, Germany) presents two cases demonstrating how Needle Guidance as well as syngo DynaCT allows for everyday, real-time therapy planning and assessment.
Aaron Fischman (Mount Sinai, New York, USA) shares a prostate artery embolization (PAE) case that underscores the value of low-dose, high-resolution vessel mapping and catheter guidance using ARTIS icono.
“We’re living in a new world order” when it comes to “no-option” chronic limb-threatening ischaemia (CLTI) patients, says Anahita Dua (Massachusetts General Hospital, Boston, USA). In recent years, into this arena has stepped transcatheter arterialisation of the deep veins (TADV), raising hopes of reducing amputation rates amid a rise in diabetes and other disease affecting microvascular dissemination. At the 2025 Vascular Annual Meeting (VAM; 4–7 June, New Orleans, USA), Dua put forward data from a new study comparing no-option CLTI patients enrolled in the PROMISE studies treated with TADV to a CLariTI study cohort who were treated using standard of care (SoC). So, “is TADV worth it?” she pondered. The one-year comparative data she presented seemed to provide an answer in the affirmative.
Positive PROMISE I and II data have seen TADV, also known as deep vein arterialization (DVA), gain traction, Dua told VAM 2025, but the “real question remains,” she said. “If you’re going to do a [TADV] procedure on a patient, then go forward with all the wound care, all the phone calls, and all the pain for the next six months to try to salvage the limb, does it really lead to better wound healing, better limb salvage rates and better amputation-free survival?”
With no randomised clinical trial data to call upon in the space to measure a difference between TADV and standard of care, Dua and colleagues compared the combined patient groups from PROMISE I and II to the real-world CLariTI group to “see whether or not limb salvage rates genuinely decrease” when the former modality is deployed.
“We did CLariTI after PROMISE, so we were able to design the study to match the PROMISE studies so that we could ensure we had matching across groups,” she explained. “As you can see, most importantly this is, again, a real-world study, with a significant number who were Black or African American, had Rutherford 5/6, and a significant history of CKD [chronic kidney disease].”
The data showed limb salvage rates of 82.2% vs. 51.3% in the TADV/ PROMISE I/II group and CLariTI, respectively; and amputation-free survival (AFS) rates of 71% for TADV vs. 34.1% for standard of care.
“For wound healing, 78% of patients at one year were either fully healed or healing in the DVA group versus the standard of care,” said Dua. “Going out, because durability matters, in the patient cohort for CLariTI—we are still collecting our data, because that was after the PROMISE study—but for the PROMISE data, we are at two years now and the limb salvage rate is still at 68%, which is excellent compared, already, to the 51% at one year for the standard of care.”
Overall, Dua concluded, “I think the data is relatively clear. Even though we don’t have an RCT, we have an excellent matched set from CLariTI compared to patients that have DVA and it is clear that DVA does have clinical benefit in patients selected appropriately. These benefits are consistent, especially if you use the LimFlow system [Inari Medical], which is kind of like the TCAR [transcarotid artery revascularisation] of the leg in that you are able to do the same thing every time. The off-the-shelf DVA that exist—and the data around that—is very variable so that is not included in any of this.”
Recent THRIVE study data show that Penumbra’s computer-assisted vacuum thrombectomy (CAVT) technology not only has the potential to improve outcomes for lower extremity acute limb ischaemia (LE-ALI) patients, but may also reduce healthcare resource use, thus potentially lowering overall costs for the healthcare system.
The latest data were presented at the 2025 Vascular Annual Meeting (VAM; 4–7 June, New Orleans, USA) by Charles Bailey (Emory University School of Medicine, Atlanta, USA).
The data show that US patients who underwent a CAVT procedure to manage LE-ALI had significantly shorter length of stays, higher discharge-to-home rates, reduced complications, and fewer related readmissions compared to other modalities.
“The THRIVE analysis reveals that LE-ALI patients who receive advanced therapies, such as CAVT, ultimately experience fewer complications and utilise fewer hospital resources compared to embolectomy,” said Bailey. “By showing important benefits for both patient care and healthcare system economics, these findings support the continued adoption of CAVT as a frontline therapy for LE-ALI.”
The THRIVE study compared CAVT to embolectomy alone and embolectomy with adjunctive bypass, and the results showed that CAVT was associated with:
The researchers performed the analysis by utilising the Vizient clinical database to identify adult patients discharged with LE-ALI over a three-year period. Sg2, a Vizient company, used propensity score matching at a 1:1 ratio based on demographics and comorbidities, payer, and hospital type to match CAVT patients (Lightning7 and Lightning 12) to embolectomy alone and embolectomy with adjunctive bypass patients, and completed the analysis with 2,619 patients in total.
HistoSonics has announced that it has completed enrolment in a pivotal trial to evaluate its histotripsy platform in treating kidney tumours.
The US company’s prospective, multicentre, single-arm pivotal #HOPE4KIDNEY trial is designed to evaluate the effectiveness and safety of the Edison system for the destruction of kidney tissue by treating primary solid renal tumours.
A total of 67 patients have been enrolled with a single, non-metastatic solid kidney mass ≤3cm. Patients will be treated with the Edison system and followed for five years post procedure, with data at the 90-day evaluation point to be submitted in support of regulatory approval with the US Food and Drug Administration (FDA).
The Edison system uses a technology called histotripsy, involving the delivery of non-thermal, non-invasive focused ultrasound waves to target and eliminate cancerous liver tissue. The system received de novo clearance from the US FDA in 2023 and last month secured its first major insurance coverage from a new healthcare policy from Healthcare payor Blue Cross Blue Shield of Michigan (BCBSM) and health plan option Blue Care Network, a recent company press release has shared.
HistoSonics’ vision is for its Edison system to become a “foundational, non-invasive” solution across a range of clinical applications, the company’s chief executive officer, Mike Blue stated.
“Completing enrolment in our pivotal kidney tumour trial represents a significant milestone toward that goal and reinforces our confidence in expanding histotripsy into additional tumour types and indications,” said Blue.
In May, Edison histotripsy system has been granted controlled early limited market access in the UK under an Unmet Clinical Need Authorisation (UCNA) under the UK’s Innovative Devices Access Pathway (IDAP), launched by the UK Government in 2023 to help fast-track ‘transformative medical technologies’ into the healthcare system.
Penumbra has announced the US Food and Drug Administration (FDA) clearance and launch of the Ruby XL system.
The Ruby XL system is designed to help physicians achieve more efficient embolization, potentially reducing radiation exposure, and optimizing outcomes—especially in large vessel and high-flow embolization, details a recent company press release.
“We’ve engineered Ruby XL to deliver more volume per coil than any other coil on the market, which may result in cost savings,” said Shruthi Narayan, president of Interventional Business at Penumbra. “Ruby XL embodies Penumbra’s commitment to innovation, delivering mechanical occlusion through more volume without sacrificing softness or deliverability.”
The Ruby XL System introduces three unique technologies—Ruby XL, POD XL, and Packing Coil XL—all of which can be delivered through a 0.035” diagnostic catheter. They have a primary diameter of .030” and are designed for procedural efficiency. These coils offer more volume (up to 40mm in size) and are available in extended lengths up to 70cm.
Engineered with a three-dimensional complex shape, Ruby XL coil is designed to frame aneurysms in a variety of clinical applications.
POD XL features a hybrid, multistage design and is engineered with three-in-one coil occlusion technology—an anchoring segment, a framing segment, and a dense filling segment. Designed for high flow vessels, POD XL offers smooth delivery and targeted vessel control.
Packing Coil XLfeatures an innovative liquid metal wave shape technology, which is designed to adjust dynamically to the size of any vessel (up to 70cm length).
TriSalus Life Sciences has announced the launch of the TriNav FLX infusion system.
The TriNav FLX infusion system retains the same trusted pressure-enabled drug delivery (PEDD) benefits as existing products but introduces an important advancement in design, states a recent company press release. The new system features twice the length of flexible material at the distal end, allowing for easier navigation through more tortuous vessels.
Key features of the TriNav FLX infusion system include:
Trackability: The more flexible distal end provides improved navigation through challenging pathways
Reduction in Force: In benchtop models, the TriNav FLX demonstrated a 28% reduction in force during navigation compared to the standard TriNav design
“We’re excited to further expand our TriNav portfolio with the introduction of the TriNav FLX infusion system,” said Mary Szela, chief executive officer of TriSalus Life Sciences.
“With TriNav FLX, we now offer a comprehensive suite of advanced technologies designed to support interventional radiologists in navigating a wide range of peripheral vessel sizes and complexities. Our continued investment in portfolio innovation underscores our commitment to making pressure-enabled drug delivery accessible to more patients. Importantly, TriNav FLX is also eligible for reimbursement under HCPCS Code C8004 for simulation—or mapping—as well as C9797 for treatment procedures. This dual coverage allows clinicians to use TriNav FLX for both planning and delivery in radioembolization, supporting greater precision and continuity of care.”
Portal vein embolization (PVE) is a crucial preoperative procedure designed to induce hypertrophy of the future liver remnant (FLR) in patients requiring major hepatectomy. Among the embolic agents available, n-butyl cyanoacrylate (nBCA) combined with lipiodol has emerged as one of the most effective options for PVE, shares José Hugo Luz (Brazilian National Cancer Institute, Rio de Janeiro, Brazil), promoting a high yield of liver hypertrophy and requires only a minimal volume of contrast media.
One of the most compelling reasons to advocate for nBCA plus lipiodol in PVE is its high embolic efficiency. Unlike particulate embolics, such as polyvinyl alcohol (PVA) or gel foam, which can migrate or recanalise over time, nBCA polymerises upon contact with blood, forming a durable cast within the embolized portal branches, ensuring complete occlusion and effectively preventing collateral formation and enhancing FLR hypertrophy.
Studies have demonstrated that nBCA plus lipiodol induces faster and more significantliver hy hypertrophy of the FLR compared to other embolic materials. This is because it creates permanent vascular occlusion, the liver responds with an accelerated regenerative process, reducing time to surgery. De Baere et al and Tsoumakidou et al published animal studies which compared different embolic materials for PVE.1,2 They were able to show that nBCA plus lipiodol promoted a greater increase in the size of hepatic lobules and number of hepatocytes per lobule when compared with other embolic materials. Also, an increased hepatocyte and Kupffer cell proliferation in the nBCA-lipiodol group was identified. Tsoumakidou et al evaluated FLR growth with computed tomography (CT) imaging 14 and 28 days after PVE, and demonstrated significantly higher liver hypertrophy at both endpoints.
Two systematic meta-analyses were published in 2020 and 2021, together gathering more than 6,000 patients.3,4 In both publications PVE with nBCA plus lipiodol promoted higher liver hypertrophy, shorter procedure times, less radiation, less use of contrast and for the first time, less cost. The BEST FLR trial was a pivotal study evaluating optimal strategies to maximise FLR in patients undergoing major liver resection.5 In this trial, PVE with nBCA plus lipiodol generated greater and faster liver regeneration as seen at CT, compared with PVA particles plus coils, allowing for earlier surgical intervention for liver cancer. In this study of 60 participants with liver cancer, PVE with nBCA plus iodised oil produced greater absolute liver hypertrophy at CT compared with PVA particles plus coils (absolute hypertrophy of 46% vs. 30% at 14 days and 57% vs. 37% at 28 days, respectively). More participants in the nBCA plus iodised oil group presented sufficient liver hypertrophy for surgery two weeks after PVE compared with the PVA particles plus coils group (87% vs. 53%, respectively). nBCA plus lipiodol is the gold standard for PVE, offering superior embolization efficiency, superior hypertrophy induction, faster procedure time, less radiation exposure and lower cost.
References
De Baere T, Denys A, Paradis V, et al. Comparison of four embolic materials for portal vein embolization: experimental study in pigs. Eur Radiol. Jun 2009;19(6):1435-42. doi:10.1007/s00330-008-1277-2
Tsoumakidou G, Theocharis S, Ptohis N, et al. Liver hypertrophy after percutaneous portal vein embolization: comparison of N-butyl-2-cyanocrylate versus sodium acrylatevinyl alcohol copolymer particles in a swine model. Cardiovasc Intervent Radiol. Oct 2011;34(5):1042-9. doi:10.1007/s00270- 010-0046-1
Ali A, Ahle M, Björnsson B, et al. Portal vein embolization with N-butyl cyanoacrylate glue is superior to other materials: a systematic review and meta-analysis. Eur Radiol. doi:10.1007/s00330-020- 07685-w
Soykan EA AB, Lopez-Yurda M, Kuhlmann KFD, et al. Predictive Factors for Hypertrophy of the Future Liver Remnant After Portal Vein Embolization: A Systematic Review Cardiovasc Intervent Radiol: Springer; 2021.
Luz JHM, Veloso Gomes F, Costa NV, et al. BestFLR Trial: Liver Regeneration at CT before Major Hepatectomies for Liver Cancer-A Randomized Controlled Trial Comparing Portal Vein Embolization with N-Butyl-Cyanoacrylate Plus Iodized Oil versus Polyvinyl Alcohol Particles Plus Coils. Radiology. Apr 2021:204055. doi:10.1148/radiol.2021204055.
José Hugo Luz is an interventional radiologist at the Brazilian National Cancer Institute in Rio de Janeiro, Brazil.
Disclosures: The author declared no relevant disclosures.
With a focus on magnetic resonance imaging (MRI)-guided procedures and cancer signalling pathways which promote cancer resistance to ablation, David Woodrum (Mayo Clinic, Rochester, USA) discusses how advancements in MRI have solidified its place in the diagnosis and treatment of prostate cancer.
Focal prostate ablation continues to challenge the standard paradigm for prostate cancer treatment. Prostate cancer was the most common cancer in men in 2024, with 299,010 new cases and 35,250 deaths in the USA alone.1 Standard treatments include surgery or radiation therapy, but no matter how expertly done, these therapies carry significant morbidity and risk to the patient’s quality of life, with an impact on sexual, urinary, and bowel function.2 Furthermore, screening programmes using prostatic-specific antigen (PSA) level and transrectal ultrasound-guided systematic biopsy have identified increasing numbers of low risk, low grade “localised” prostate cancer.
With this, prostate focal therapies with ultrasound and MRI guidance have become available, fuelling the debate on the suitability of focal or regional therapy for patients with low or intermediate risk prostate cancer. Some of the largest unresolved issues include prostate cancer multifocality, suboptimal staging with accepted imaging modalities, limitations of current biopsy strategies, and, most important, whether focal therapies can be safely and effectively used for prostate cancer.3
Advancements in MRI have made it the platform of choice for identifying prostate cancer, whether focal or multifocal, and in disease staging.4 Targeted biopsy of suspected cancer lesions detected with MRI is associated with increased detection of high-risk prostate cancer and decreased detection of low-risk prostate cancer, particularly with the aid of MRI/ultrasound fusion and direct in-bore biopsy platforms.5
Focal prostate ablation is often considered for patients with low to intermediate risk prostate cancer who may not require radical whole gland treatments like surgery or radiation therapy. Many focal ablation methods can be guided and monitored with ultrasound or MRI. Ultrasound is the most common imaging modality for guiding and monitoring focal ablation, but it cannot reliably depict the prostate cancer target and has limited capability to real-time monitor during the ablation. Although MRI requires more specialised hardware and training, it provides the most robust targeting and monitoring imaging guidance platform. Use of real-time MRI enables temperature mapping, allows for real-time visualisation of tissue heating, as well as real-time precise imaging of the ice ball as it forms in the case of cryoablation. It is important to note that long-term outcomes of MRI-guided focal prostate cancer ablation compared to traditional treatments are still areas of ongoing research and evaluation.
References
Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA: a cancer journal for clinicians. 2023;73(1):17-48.
Potosky AL, Davis WW, Hoffman RM, et al. Five-year outcomes after prostatectomy or radiotherapy for prostate cancer: the prostate cancer outcomes study. J Natl Cancer Inst. 2004;96(18):1358-67.
Onik G, Vaughan D, Lotenfoe R, et al. “Male lumpectomy”: focal therapy for prostate cancer using cryoablation. Urology. 2007;70(6 Suppl):16-21.
Spektor M, Mathur M, Weinreb JC, et al. Standards for MRI reporting-the evolution to PI-RADS v 2.0. Transl Androl Urol. 2017;6(3):355-67.
Siddiqui MM, Rais-Bahrami S, Turkbey B, et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA. 2015;313(4):390-7.
David Woodrum is a professor of interventional radiology at the Mayo Clinic in Rochester, USA.
Disclosures: The author declared no relevant disclosures.
FastWave Medical has announced the successful completion of initial first-in-human (FIH) procedures in its feasibility study of Sola, the coronary laser intravascular lithotripsy (IVL) system.
The multicentre study will assess Sola’s safety and performance in patients with calcified coronary artery disease. Sola is a rupture-resistant balloon catheter designed to help physicians treat hardened calcium in blood vessels with precision and control. Its laser energy delivers 360-degree pressure with each pulse, making therapy consistent and effective, even in challenging lesions.
“There’s a moment in every FIH study where you see if the technology lives up to its promise,” said Arthur Lee, director of Peripheral Vascular Services at The Cardiac and Vascular Institute (TCAVI), in Gainesville, USA. “With Sola, we saw that moment early on. It demonstrated exceptional crossability through complex anatomy where existing IVL technology might struggle, and its 5Hz pulse rate allowed us to deliver therapy efficiently—reducing ischaemic time in patients with compromised cardiac output.”
In a recent press release the company has highlighted that this milestone follows FastWave’s FIH study of Artero, its peripheral electric IVL (E-IVL) system, which demonstrated 100% procedural success and no adverse events at 30-day follow-up.
“Every step of developing Sola has focused on solving the real-world problems physicians face in treating complex arterial disease,” said Tristan Tieso, chief operating officer at FastWave Medical. “Early feedback from these cases shows we’re on the right path,” he said.
“Our team set out to reimagine what’s possible with coronary IVL,” added Sukanya Iyer, FastWave Medical’s head of technology. “Seeing Sola perform in human cases reinforces our commitment to give clinicians cutting-edge tools for their high-risk patients.”
The company state that findings from this study will help shape FastWave’s regulatory submissions and the design of its US pivotal trial, a key step toward broader US Food and Drug Administration (FDA) approval.
Reflow Medical recently announced that the US Food and Drug Administration (FDA) has granted de novo clearance for the company’s Spur peripheral retrievable stent system, which is designed for the treatment of de novo or restenotic lesions following predilatation in patients with infrapopliteal arterial disease.
According to Reflow Medical, the Spur stent system is the first and only retrievable stent system that features a self-expanding stent with an integrated dilatation balloon catheter on an over-the-wire system. It is designed for controlled lesion penetration and treatment through a series of radially expandable spikes. Known as retrievable scaffold therapy (RST), the spikes on the Spur stent penetrate the lesion to increase the acute luminal diameter and modify the lesion morphology to change vessel compliance and reduce vessel recoil effect.
Results of the recently concluded DEEPER REVEAL clinical trial (NCT05358353) to evaluate the Reflow Medical Spur stent system for below-the-knee (BTK) treatment of chronic limb-threatening ischemia (CLTI), demonstrated that following predilatation, the Spur stent system achieved a 99.2% technical success rate and 97% freedom from major adverse limb events (MALE) and perioperative death at 30 days.
“Clinical data submitted to the FDA demonstrated the safety and efficacy of the Spur stent system,” said Mahmood K Razavi (St. Joseph Heart and Vascular Center, Orange, USA). “This novel device will be a valuable and innovative expansion of our treatment toolbox as a unique device for the treatment of complex BTK disease,” he added.
S. Jay Mathews (Bradenton Cardiology/Manatee Memorial Hospital, Bradenton, USA) commented: “It’s exciting to see the clinical success of the DEEPER REVEAL trial enabling the de novo clearance of the Spur stent system. This first-of-its-kind technology offers a truly novel approach to treating patients with BTK CLTI disease. As an adjunct to standard balloon angioplasty, Spur RST enables us to address this complex disease in a more effective way, achieving these outcomes that go beyond what PTA [percutaneous transluminal angioplasty] alone can deliver.”
Both Mathews and Razavi were lead principal investigators for the study, which was conducted at 49 centres in the USA and enrolled 130 patients.
“Extensive research and development, which laid the groundwork for the DEEPER REVEAL trial, enabled the creation and clinical validation of the Spur stent system, an innovative mechanical endovascular device engineered to enhance lesion penetration and optimise the treatment of BTK peripheral arterial disease,” said Teo Jimenez, senior vice president of R&D at Reflow Medical.
According to Reflow Medical chief executive officer and co-founder, Isa Rizk, “The FDA’s de novo clearance, following positive clinical trial results in patients with CLTI, enables us to provide physicians with an effective therapeutic option for this growing patient population. We are fully prepared to launch our innovative technology through our dedicated sales force, ensuring it promptly reaches physicians to support patients.”
BD has announced plans to initiate a patient data registry for the Rotarex atherectomy system to measure real-world outcomes for patients with peripheral arterial disease (PAD).
Known as XTRACT, this prospective, multicentre, single-arm, post-market registry study will assess the clinical performance of the Rotarex atherectomy system in the treatment of US patients with PAD lesions. The XTRACT Registry is being led in partnership with co-principal investigators, Prakash Krishnan (Mount Sinai, New York, USA), an interventional cardiologist, and Todd Berland (NYU Langone Health, New York, USA), a vascular surgeon. The registry will enrol up to 600 patients at approximately 100 clinical sites across the USA, with the first patient enrolment expected later this year. Clinical follow-up evaluations will occur after 30 days, six months and 12 months post-procedure to assess safety and effectiveness of outcomes.
“This registry will provide valuable data to support clinical decision-making and enhance patient outcomes in the management of PAD,” said Krishnan. “The Rotarex system has been extensively studied internationally, and we are excited to further evaluate its adaptability in treating a wide range of PAD lesions within the US patient population.”
The Rotarex atherectomy system is a minimally invasive solution designed to efficiently remove both plaque and thrombus in peripheral arteries. Offering dual indications as both an atherectomy and thrombectomy device, the Rotarex atherectomy system is a proven tool for treating PAD.
“The XTRACT registry is the first comprehensive registry aimed at providing key insights into the real-world applications of the Rotarex system,” said Rima Alameddine, worldwide president of BD Interventional-Peripheral Intervention. “This study underscores our unwavering commitment to optimising treatment strategies in partnership with leading physicians to improve patient care.”
What should be done if a cryoablation of renal cell carcinoma (RCC) is performed successfully but follow-up imaging demonstrates a possible pseudoaneurysm? Here, Nassir Rostambeigi (Mallinckrodt Institute of Radiology, St Louis, USA) shares details of a case in an attempt to answer this question.
Renal cryoablation is a well-established technique for treating renal masses, offering comparable outcomes to partial nephrectomy while minimising morbidity. However, careful consideration of its safety profile, including both common and rare adverse events, is essential for care providers.
This case report highlights a rare and significant scenario. An 81-year-old woman with stage three chronic kidney disease initially presented with a left renal mass measuring 2.7cm. Follow-up imaging revealed an increase to 3.1cm, prompting a multidisciplinary decision to proceed with computed-tomography (CT)- guided biopsy and cryoablation. The procedure was successful, but subsequent imaging uncovered a suspicious arterially enhancing lesion, initially suspected to be a pseudoaneurysm.
Detailed evaluation of contrast-enhanced CT phases revealed a round structure at the ablation site, exhibiting contrast uptake similar to the aorta—raising concerns about a pseudoaneurysm. Then, coil embolization was performed to treat this suspected pseudoaneurysm, which initially seemed effective. However, persistent and recurrent enhancement on CT scans soon raised the possibility of residual or recurrent renal cell carcinoma.
Further investigation involved ultrasound evaluation, which identified the lesion as a solid mass without internal vascular pulsatility, ruling out a pseudoaneurysm. To confirm the diagnosis and for planning, an angiogram was performed, and, using lipiodol, the lesion was stained to enhance visualisation under CT guidance. Then, a percutaneous biopsy followed by cryoablation of the focal recurrence, was then carried out under CT guidance.
Pathological examination confirmed recurrent clear-cell renal cell carcinoma. The patient has maintained baseline urinary function and, 30 months after repeat cryoablation, remains free of recurrent disease.
This case underscores the importance of thorough post-ablation imaging, as recurrence can mimic vascular abnormalities like pseudoaneurysms. Careful evaluation with ultrasound or magnetic resonance imaging (MRI) is crucial in differentiating tumour recurrence from benign post-procedural changes, ensuring timely and appropriate intervention is provided.
Nassir Rostambeigi is an interventional radiologist at the Mallinckrodt Institute of Radiology, in St Louis, USA.
In a paper titled ‘Specialist awareness of interventional radiology: Current state of affairs and opportunities for improvement’, Mina S Makary (Columbus, USA) and his team surveyed specialist provider understanding of interventional radiology (IR) at their tertiary centre, which yielded unanticipated results. Here, he discusses the data they collected and their broader significance for the evolution of the specialty.
Our recent survey has revealed significant gaps in awareness and understanding of IR among specialist providers, raising concerns about missed opportunities for minimally invasive care. The study, conducted at a large academic medical centre, surveyed over 1,400 non-primary care specialists and received 516 responses. While IR continues to expand its scope across oncology, urology and women’s health, the findings show that many medical professionals remain unaware of the specialty’s full range of applications.
Nearly 60% of surveyed specialists rated their knowledge of IR as only ‘adequate’ or ‘poor’—a result we did not anticipate. When asked how frequently they offered IR procedures as alternatives to surgery, 20% admitted they never did. Conditions like abscesses and haemorrhages were commonly linked to IR, but recognition dropped significantly for areas such as infertility, benign prostatic hyperplasia (BPH) and bone cancer—indications where IR can play a critical role.
Advanced practice providers (APPs) demonstrated lower overall awareness than physicians but showed a stronger interest in learning more about IR services. In fact, 75% of APPs expressed a desire to improve their knowledge, positioning them as a key audience for targeted educational efforts.
Interestingly, the study found no significant difference in IR familiarity between surgical and non-surgical specialties, despite the procedural alignment between surgery and interventional radiology. Among specialist physicians, early-career practitioners—interns, residents and junior attendings—were less likely to report high confidence in their understanding of IR.
The results highlight an ongoing need to integrate IR education into medical training and continuing professional development. Previous efforts—such as presentations at specialty conferences— have been shown to effectively raise awareness, but the study suggests broader strategies may be necessary.
The findings carry clear implications for patient care. Without broader specialist recognition of IR’s expanding capabilities, patients may miss out on less invasive, lower-risk therapeutic options. Bridging the knowledge gap through structured education and interdisciplinary collaboration could significantly improve referral patterns and treatment outcomes.
As IR continues to innovate across multiple domains, its visibility within the wider medical community must keep pace. This study offers a timely reminder that increasing awareness is not just a professional courtesy—it’s a clinical necessity.
Mina S Makary is an interventional radiologist at The Ohio State University Wexner Medical Center, Columbus, USA.
A new geographic information system (GIS) analysis of Kenya has found “disproportionate” rates of maternal morbidity and mortality due to postpartum haemorrhage (PPH) in areas without interventional radiology (IR) capabilities.
Led by Ryan W England (Princeton Radiology Associates, Princeton, USA) and published in the Journal of Vascular and Interventional Radiology (JVIR), the study employed multilayered GIS mapping to pinpoint healthcare disparities and propose a framework for global IR outreach.
The authors detail that PPH is a leading cause of preventable maternal mortality globally, particularly in low- and middle-income countries. Minimally invasive endovascular procedures such as uterine artery embolization (UAE), performed as standard for interventional radiologists, can be used to treat severe cases of PPH that are unresponsive to first-line treatments.
“UAE has been shown to be safe and effective, with systematic reviews demonstrating a clinical success rate (as defined by controlled bleeding without need for additional procedure or surgery) of 89%,” write England and colleagues, referencing a 2021 paper by Matthew Brown et al. Although the treatment has been shown to control PPH while preserving the uterus, access to UAE in Kenya is currently limited to just six hospitals—all located in the capital city of Nairobi.
In their analysis, the authors reviewed publicly available Kenyan health and demographic data from 2014–2018. Using county-level statistics, they constructed three key indices: a PPH Risk Index (PRI), a Health Severity Index (HSI) and a Combined Risk Index (CRI). These indices were derived from variables such as adolescent pregnancy rates, maternal mortality ratios (MMRs), access to antenatal care, insurance coverage and physician density.
A total of f 14,718,288 female Kenyans of childbearing age were included in the geospatial analysis. Between 2014 and 2018, the number of maternal haemorrhages across the country was found to increase from 15,457 to 21,332, rising by 38% over the five-year period.
Notably, the highest MMRs were observed in the southeastern and northwestern counties, with standard deviations 1.5–2.3 above the national mean. This finding correlated with lower densities of healthcare facilities, longer travel times to a healthcare facility, and lack of IR services. In contrast, Nairobi’s MMR fell within the national average, despite housing the country’s only IR-equipped hospitals.
“Geospatial analysis has been successfully used for public health mapping and radiology outreach in the past,” write England and colleagues. “Prior research using GIS has shown that distance to quality healthcare facilities is a substantial factor in the utilisation of clinical services.”
Translating their findings into actionable measures, the authors examined the density of the study target population within a one-hour drive of each hospital overlaid onto the CRI for each county. By doing so, the authors were able to identify the hospital in which development of IR services may have the greatest impact on decreasing PPH morbidity and mortality. Among them, Homa Bay County Teaching and Referral Hospital in southwestern Kenya was highlighted as a high-priority site for IR development, due to its high CRI score and catchment population of women of childbearing age.
Despite Nairobi being relatively better equipped, England and colleagues emphasise that a broader nationwide expansion of IR services is critical. As of 2024, only around 10 practicing interventional radiologists serve the entire country, with all initially trained abroad. “This information only highlights the dramatic need in such a populated city for IR services to grow and expand,” the authors write.
Efforts are underway to bolster local capacity, including a dedicated IR fellowship programme at the University of Nairobi that began producing graduates in 2020.
“Moving forward, further investigation of targeted individual healthcare facilities in Kenya needs to be assessed to better understand the unique needs of each hospital and region. One approach includes performing an ‘IR Readiness Assessment’ to successfully create meaningful and sustainable solutions to each individual hospital’s radiology needs,” England et al state.
“Using a framework such as this may allow for a comprehensive examination of current and future barriers involved in implementing IR outreach and resource allocation in the regions identified through this analysis,” the authors write. They note that further research will aim to correlate GIS-driven service expansion with real-world maternal health outcomes as IR capacity in Kenya grows.
“At the publication of this public census, we’ve opened Pandora’s box and we’re going to have to make a change,” Pavan Najran (The Christie Hospital NHS Foundation Trust, Manchester, UK) said at a recent meeting, referencing a UK-wide survey looking at the use of medical devices that contain animal derivatives. Touted as the first and largest study of its kind, Najran underlined the poignancy of the results set against increasing patient autonomy, religious diversity in the UK and consent.
During his Global Embolization Symposium and Technologies (GEST; 15–18 May, New York, USA) presentation Najran shared that, during a drain removal as an interventional radiology fellow, he recalled being handed a pot of bovine collagen, realising that the patient on the table did not know that this was going to be used and had not consented.
“From that point, I kept reading small case reports and even legal documentation throughout the years about patients retrospectively taking action against hospitals because a mesh repair contained animal derivative, and I thought to myself that it’s time we had a true reflection from the population as to the use of these devices,” Najran explained.
Via an electronic survey, Najran and his team collected responses from 407 patients who were given examples of emergency and non-emergency scenarios in which devices with animal derivatives may be used. The majority of responders were white British/Welsh/Scottish/Northern Irish, followed by Asian/Asian British-Indian and Asian/Asian British-Pakistani. Most respondents had received higher education to undergraduate or postgraduate degree level. Those with no religion and meat-eaters made up a large proportion of respondents.
Religion as an influencing factor was a central focus for Najran and his team. Among respondents, 12 identified as Buddhist, 96 Christian (including all Christian denominations), 19 Hindu, six Jewish, 76 Muslim, two Sikh, nine preferred not to say and 16 marked ‘other’.
Ranging from completely unacceptable to completely acceptable, Najran shared that across groups “there is huge resistance to the use of both bovine and porcine products in either emergency or non-emergency settings”.
“Looking at the Christian population, there is a move toward slightly more acceptable in all groups, but there is a significant proportion of those rejecting the use of such products,” said Najran. “In the Muslim population, as expected, there is a greater rejection in the porcine group, but actually in the bovine group as well.”
Among responders who identified as having no religion (171) unacceptability was high, with 73.7% and 80.7% of responders stating no acceptability in an emergency and elective setting, respectively.
In the meat-eating group—which accounted for 149 respondents—33.5% specified no acceptability for the use of devices with animal derivatives in an emergency setting, and 40.9% responded no acceptability for their use in an elective setting. Vegetarians and vegans indicated greater rejection of these devices in any setting, a resistance Najran and his team had anticipated.
Given the UK’s increasing diversity, Najran raised that “there is an increasing possibility of a mismatch between what is medically possible and what is personally acceptable”. Demonstrating the gravity of this mismatch for some religious groups, the speaker drew attention to Jehovah’s Witness, who refuse to accept blood products, yet the use of animal derivatives in devices is a “neglected topic”.
“Right now, we can use such products in our patients without having to consent them or even discuss it with them before the procedure, which really needs to change,” Najran stated. “We need to approach our patients far more holistically and we need to consider the patient’s personal requirements and what is acceptable to them prior to performing a procedure.”
Najran’s approach to address this issue is twofold—he believes consent gained from patients after informing them of animal derivatives in devices that may be used in their procedure must be made a legal requirement, and industry must collaborate to provide the best option in these circumstances.
Recently, Najran and his team were called to discuss this research at the House of Commons and are seeking to secure funding for a national survey to gain “healthier data” from the UK population at large, he stated.
Merit Medical Systems has announced that it has acquired Biolife Delaware in a merger transaction through which Biolife has become a wholly-owned subsidiary of Merit. Biolife manufactures patented haemostatic devices under the brand names StatSeal and WoundSeal.
A press release made by Merit states that the aggregate transaction consideration, paid in cash and assumption of Biolife liabilities, was approximately US$120 million. This strategic acquisition positions Merit to provide clinicians with more products designed to standardise, simplify, and minimise post-procedure care and maintenance, the company adds.
Many Merit products operate through small openings in the skin that require efficient solutions to stop bleeding, help patients recover, and minimise costly complications. In such cases, StatSeal specifically works with the patient’s blood to rapidly form a protective seal over the procedure site. Adding StatSeal to Merit’s haemostasis portfolio is intended to provide healthcare partners with an additional effective solution that complements a wide range of percutaneous procedures, including interventional radiology and cardiology, dialysis, electrophysiology, biopsy, and drainage.
“We are excited to enhance the portfolio of haemostatic solutions offered to clinicians with the acquisition of Biolife,” said Fred P Lampropoulos, Merit’s chairman and chief executive officer. “The acquisition provides effective, differentiated, haemostatic solutions for all percutaneous devices with a broad range of clinical applications including vascular closure and indwelling catheter bleeding complications. BioLife’s StatSeal and WoundSeal products address an estimated US$350M global market opportunity, are clinically validated, and will enhance our ability to deliver comprehensive solutions to our customers. Moreover, with Merit’s resources and expertise, we believe we are well positioned to further develop and expand the reach of these product lines, ultimately benefiting patients and healthcare providers globally.”
Findings from the COVER-ALL trial suggest that software-based assessment of the minimal ablative margin during percutaneous thermal ablation significantly improves treatment precision and may reduce local tumour progression in liver cancer patients.
Published in The Lancet Gastroenterology & Hepatology, the randomised phase 2 trial represents the first prospective evaluation of a software-driven margin confirmation method, which integrates artificial intelligence (AI)-based autosegmentation and biomechanical deformable image registration.
Led by Bruno Odisio at The University of Texas MD Anderson Cancer Center in Houston, USA, the trial enrolled 100 patients with up to three liver tumours undergoing computed tomography (CT)-guided thermal ablation. Participants were randomised 1:1 intraprocedurally to receive either standard visual assessment or the experimental software-based margin analysis tool. The primary endpoint of the study was the post-ablation intraprocedural minimal ablative margin.
Patients were enrolled and treated with thermal ablation between 15 June 2020 and 5 October 2023. The interim analysis showed that the software-based assessment group achieved a mean ablative margin of 5.9mm, compared to 2.2mm in the visual assessment group, which prompted early halting of enrolment in the control group. Only 15% of patients in the control group reached the optimal 5mm threshold, versus 75% in the experimental arm.
Odisio and colleagues subsequently enrolled a further 50 patients to the experimental group. In this non-randomised cohort, the average margin further increased to 7.2mm, with 84% achieving optimal coverage.
Secondary endpoints, including the two-year cumulative incidence of local tumour progression, also favoured the software-based group, with a progression rate of 5%, compared to 16% in the visual assessment group. Although the authors note that this difference did not reach statistical significance, they believe that the trend is suggestive of the software’s potential long-term benefit.
“This is, to the best of our knowledge, the first randomised trial to establish the feasibility and efficacy of software-based assessment as an intraprocedural tool for optimising the minimal ablative margin during the thermal ablation of liver tumours,” Odisio et al write. The researchers assert that their study adds to the “growing evidence that this approach allows accurate quantification of the minimal ablative margin, which is predictive of local tumour progression”.
The COVER-ALL system uses biomechanical deformable image registration and AI-based autosegmentation algorithms to quantify the shortest distance between the tumour and ablation zone during the procedure. It provides visual feedback and real-time margin calculations to guide overlapping or repeat ablations if necessary, the authors describe.
Odisio and colleagues conducted a clinical usability survey using the Likert scale, which found that the software was rated “highly” by interventional radiologists, with 91% finding it helpful for evaluating technical success, and 89% agreeing it improved understanding of applicator positioning relative to the target tumour.
The use of software guidance was associated with a greater frequency of overlapping and repeat ablations, reflecting increased precision rather than complexity. Odisio et al note that procedure times were longer in the experimental arm, but without increased adverse events. The rate of grade 1–3 adverse events was low overall (5%) and comparable between groups.
The study authors note that historical overestimation of the minimal ablative margin using visual methods may explain the high variability in local control outcomes seen across institutions. By introducing a reproducible, objective approach, they believe that the COVER-ALL platform offers a means of “standardising intraprocedural decision-making”.
While acknowledging the study’s limitations— including its single-centre setting and small cohort— the researchers maintain that the evidence supports broader implementation of the software. “These results highlight the potential of integrating software-based assessment into the standard-of-care for liver thermal ablation, given its ability to improve the minimal ablative margin and potentially reduce rates of local tumour progression,” Odisio and colleagues conclude.
Histotripsy is a non-thermal, non-ionising and non-invasive focused ultrasound technique which relies on cavitation for mechanical tissue breakdown at the focal point. Leading research into the novel technique, Mishal Mendiratta-Lala (University of Michigan, West Bloomfield, USA)—principal investigator for the #HOPE4LIVER trial evaluating histotripsy in liver tumours— provides a deep dive into histotripsy, discussing its application and evolution in the near future.
In 2024, histotripsy has advanced significantly following its US Food and Drug Administration (FDA) approval in late 2023, allowing many institutions to acquire the technology for clinical use. Most systems were delivered this year, leading to the treatment of over 500 tumours with histotripsy.
Although enthusiasm is high among both patients and the medical community, it is still too early to report definitive new findings. The focus must remain on collecting and analysing data to assess long-term efficacy. A key priority moving forward is careful patient selection, ensuring that histotripsy is used appropriately rather than broadly applying it to all cases.
Histotripsy garners “excitement” in the cancer community
For patients deemed suitable for treatment with histotripsy, the procedure has demonstrated several benefits over alternative ablative techniques. These are largely due to the non-invasive nature of the procedure, minimal bleeding risk, and post-procedure pain and recovery times.
There is excitement in the cancer community about histotripsy’s potential to induce an abscopal response— a systemic immune reaction against cancer. However, this effect has not been reliably observed in clinical practice yet and we look forward to emerging research that may bear out evidence of this response.
Current data supporting histotripsy’s efficacy is limited but promising. To date, there are two peer-reviewed studies that are analysing histotripsy—the first-in-man THERESA trial evaluating histotripsy of hepatic tumours, and the #HOPE4LIVER trial which concerns the treatment of liver tumours with histotripsy. The former is a small early study focused solely on safety. The 36-hour data confirmed that treated volumes were effectively ablated, demonstrating initial safety. The latter #HOPE4LIVER trial involved 44 tumours and evaluated 30-day safety and efficacy. The results showed that histotripsy successfully treated the target lesions, with no enhancement of the treated tumours, confirming short-term efficacy.
These studies confirm that histotripsy is safe, but long-term efficacy, survival benefits, and recurrence rates remain unknown. To determine whether histotripsy improves overall survival and delays disease recurrence, more clinical trials and data-sharing across institutions are essential. Treating patients with only 30-day data in 44 tumours is premature for broad clinical adoption, emphasising the need for further research.
“Challenging” operator learning curve
Leading histotripsy technology innovation, the Edison (HistoSonics) platform has a notable operator learning curve due to its complexity and multiple components requiring proficiency. Challenges include setting up the water bath correctly to prevent leaks, accurately identifying the target, and properly defining treatment boundaries. The robotic head’s large and bulky design adds difficulty in positioning for optimal lesion treatment. Additionally, treatment limitations arise from factors such as lesion depth, adjacent structures, and device voltage constraints.
As for institutional implementation, while the platform can be highly effective when the target is appropriately selected, its adoption requires significant training, experience, and institutional investment in both personnel and infrastructure. Proper training programmes and support are essential for successful integration. I believe a successful histotripsy programme requires institutional commitment and resources, making it challenging to adopt easily.
While institutions can integrate the technology, its success will depend on the presence of a strong clinical team, institutional support, a general anaesthesia team, adequate space and finally, a financial bolster. Insurance reimbursement is not always guaranteed, and thus institutions will need a strong financial team to navigate funding and advocate for coverage.
What’s to come for histotripsy in 2025
The year 2025 will be an exciting one for histotripsy as the field evolves. With more institutions purchasing the device, the accumulation of clinical data will be crucial. However, the success of histotripsy will depend on strong collaboration within the clinical community to analyse outcomes and refine patient selection criteria. Not all patients will be ideal candidates, making ongoing clinical trials essential for optimising the technology’s impact in cancer treatment.
Global adoption of histotripsy is likely to grow, but its integration into standard care will require further validation through research. We need more clinical trials with combination therapies and we need more trials looking at treatment of different cancer types.
A key focus for 2025 will be ensuring that histotripsy is implemented effectively and safely. Additionally, while the potential for an abscopal response is intriguing, it remains unproven in patients, and caution is necessary to avoid unintended consequences.
In addition, histotripsy is being expanded to renal and pancreas applications which will be very exciting. Overall, histotripsy has significant promise, and 2025 will be a pivotal year in determining its role in the broader clinical landscape. The medical community plays a critical role in shaping the clinical narrative and ensuring responsible treatment decisions. Looking ahead, I hope to be able to lead clinical trials, which will be essential in identifying the ideal patient population and determining whether histotripsy can provide meaningful survival benefits for cancer patients.
Mishal Mendiratta-Lala is an interventional radiologist at the University of Michigan in West Bloomfield, USA.
L-R: Matthew Menard and Andrew Holden moderate a CX CLTI session
A comment from Andrew Holden (Auckland City Hospital, Auckland, New Zealand) conveyed surprise at new cost-effectiveness data from the BEST-CLI trial that were shared at the 2025 Charing Cross (CX) Symposium (23–25 April, London, UK). The findings were revealed as part of a series of four podium-first presentations from the landmark BEST-CLI and BASIL-2 trials delivered at the meeting that aimed to add nuance to the ongoing conversation around the best treatment option for chronic limb-threatening ischaemia (CLTI) patients.
Sharing the main conclusion to be drawn from new BESTCLI cost-effectiveness data, Matthew Menard (Brigham and Women’s Hospital, Boston, USA) shared with the CX 2025 audience: “I can tell you that, based on the data that we have—with the caveat that the final results are pending—we would predict that open will prove to be slightly superior to endo[vascular] with regard to cost per life year gained and that endo[vascular] will be slightly superior to open with regard to cost per quality-adjusted life year gained.”
Topline results from this trial were shared at the American Heart Association (AHA) scientific sessions in 2022, with investigators revealing that surgical bypass with adequate single-segment great saphenous vein is a more effective revascularisation strategy for patients with CLTI who are deemed suitable for either an open or endovascular approach. Both strategies were deemed safe and effective for CLTI treatment.
At CX, Menard added a further prediction that “given the small and statistically insignificant magnitude of the differences in the relevant inputs, it is very unlikely we will detect any meaningful cost-effectiveness difference,” noting that more granular data will be released later in the year.
Holden, who was moderating the session, homed in on these findings during discussion time. “Before you shared these data,” he said, “I intuitively thought that endovascular, while not being successful overall, was going to be more cost-effective and I thought it would be driven by lower hospital stay and certainly lower intensive care stay, but you actually found the opposite, so I find that counterintuitive.”
Holden asked Menard whether he could explain the findings, to which Menard responded that “our goal was to undertake a very comprehensive analysis,” in which all costs associated with the initial index procedure and hospitalisation were captured, along with all of the costs of follow-up reinterventions, hospitalisations, and rehabilitation care. “The challenge is figuring out what’s relevant to the disease,” he said, adding that “this is how the data are looking” when all of the costs that are associated with CLTI revascularisation are assessed in aggregate over time. “Hospital stay,” he stressed, “which is almost always the key driver in costeffectiveness analyses, appears to be the key metric in our evaluation as well.”
BASIL-2 triallist Matthew Popplewell (University of Birmingham, Birmingham, UK) noted that he was “quite relieved” on hearing the new findings. He explained that the length of stay in the BASIL-2 health economic analysis has been criticised for being “really long”, with the suggestion being that this could be due to a healthcare system issue. “Clearly it’s not, because it’s happening on both sides of the pond,” Popplewell commented.
Holden added that a “new lesson” to take from these cost-effectiveness data is that the driver of shorter hospital stay in these patients is perhaps not a less invasive procedure but instead making progress with wound healing to facilitate discharge.
Subsequently, Alik Farber (Boston Medical Center, Boston, USA) shared a new subset analysis from BEST-CLI. “We found that primary endo[vascular] may actually burn bridges for secondary bypass,” the presenter concluded, noting that primary bypass was associated with “significantly better” outcomes.
A question from the audience probed whether there are enough granular data available to know how a primary endovascular intervention “actually burns the bridge”. Farber responded: “There are many potential reasons as to how endovascular therapy may burn bridges for a future bypass. It may occur due to disruption of vulnerable plaque, wire injury, compromise to collateral vessels, damage to runoff vessels, compromise of a bypass target, progression of tissue loss and concomitant loss of optimal window for intervention, or it could simply be a marker for a higher risk patient or disease pattern. Which of these reasons are at play is not clear; however, our findings do show that the amputation rates are higher after secondary bypass.”
Here, Farber pointed to future research that might bring answers. He shared that the Novo Nordisk Foundation has provided a grant to the BEST-CLI team to fully unpack the BEST-CLI dataset.
Menard added that the National Institutes of Health (NIH) has granted the BEST-CLI team permission to look more closely at the first major adverse limb events (MALE) data in the trial. He remarked: “We have been able to obtain the source data and so will be able to look at the aetiology of treatment failures. We are hopeful this will help us understand the important questions related to the need for reinterventions following an initial open or endovascular revascularisation.”
Summarising this part of the discussion, Holden remarked: “I think it’s fair to say that we are learning that endo[vascular] may burn bridges, and I never used to like to hear that, but I think it is potentially true.”
Elsewhere in the session, Popplewell shared for the first time the outcomes of the 61 patients treated conservatively who were screened for BASIL-2 as part of the BASIL prospective cohort study. He noted that this figure represented 13% of those screened for the trial at the lead institution, a proportion that was “a lot bigger” than the researchers were expecting. These patients, he explained, were not amputated, nor was any attempt made to revascularise them due to frailty or lack of options.
Popplewell concluded that patients managed conservatively in this group were “more likely to be older, female and sicker, and less likely to receive best medical therapy” than those who underwent infrainguinal revascularisation.
Initial results from this trial were presented at CX 2023, with the main conclusion being that a patient who needs a below-the-knee revascularisation with or without a femoropopliteal revascularisation is likely to do better if they are treated with a best endovascularfirst strategy rather than a vein bypass-first approach if clinicians had clinical equipoise between the two strategies.
At CX 2025, Popplewell also shared BEST-CLI and Global Limb Anatomic Staging System (GLASS) angiographic scoring data from BASIL-2.
He concluded that over two-thirds of patients enrolled in BASIL-2 had GLASS stage II or III disease, adding that half had mild or minor femoropopliteal disease, while one-third had long femoropopliteal occlusive disease.
The presenter also reported that most (two-thirds) of the tibial disease in the least diseased artery was confined to less than one-third of the vessel or short occlusions of less than 3cm in length and that the majority had some form of pedal arch. He noted that there were no significant differences in presentation between those patients treated with either best endovascular therapy or vein bypass.
Discussion following the four presentations considered whether clinical practice has changed following the release of BEST-CLI and BASIL-2 data.
“Anecdotally,” Farber shared, “I can tell you that it has,” while acknowledging that it is as yet hard to give an evidence-based answer to this “important” question.
Panellist Robert Hinchliffe (University of Bristol, Bristol, UK) stated that it should be possible to track any change in practice in the UK via the National Vascular Registry (NVR).
Menard commented that “it seems like people are listening” while noting it “obviously depends on who you talk to”. He acknowledged that there are specialists who are reluctant to change practice regardless of what the evidence says and that there is a “huge educational challenge” moving forward. “Hopefully it’s not going to take 10 years, which is the average for guidelines to affect practice,” he said.
Referencing some data on the topic, Menard noted that within the Vascular Quality Initiative (VQI)—which he recognised is “not necessarily the perfect place to look” because it only represents around 50% of providers in the USA—it “definitely seems like there’s an uptick” in bypasses.
Taking a step back, Popplewell stressed that there is a need to “act carefully” and refrain from “blanketly applying” the results of the two studies to all CLTI patients. “I think we have to remember that these are a subset of patients with CLTI where we have genuine equipoise between two different strategies,” he said.
Holden shared that he and his team are now “more rigorous” with assessment of conduits. Hinchliffe agreed on this takeaway message, noting: “In terms of the algorithm for evaluation, conduit assessment is absolutely key early in the assessment and evaluation phase.”
Imperative Care today announced the completion of patient enrolment in its SYMPHONY-PE study, a pivotal investigational device exemption (IDE) trial evaluating the safety and efficacy of the company’s Symphony thrombectomy system for the treatment of acute pulmonary embolism (PE).
Designed to expand Symphony’s current indication for use to include PE, the study was conducted at 19 leading interventional radiology, interventional cardiology and vascular surgery centres across the USA.
“While progress has been made in the treatment of pulmonary embolism, there is still a need for therapies that may offer improvements in safety, efficiency and long-term patient outcomes,” said interventional radiologist, Vivian L Bishay (Mount Sinai Health System, New York, USA) and national co-principal investigator of the SYMPHONY-PE study. “This study represents a promising step forward in evaluating next generation technology to expand treatment options for physicians and their patients.”
“Early clinical use of Symphony—including both 16Fr and 24Fr catheters—has shown promising potential for fast, safe and efficient clot removal for PE utilising powerful precision thrombectomy,” said Sripal Bangalore (NYU Grossman School of Medicine, New York, USA) and national co-principal investigator of the SYMPHONY-PE study. “We thank the patients, investigators, and clinical research teams whose efforts were instrumental in helping us complete enrolment. We look forward to sharing topline results later this year.”
“Initial experience with the novel Symphony thrombectomy system at our centre has been promising,” said Dana Tomalty, peripheral and neuro interventional radiologist at Huntsville Hospital in Alabama, USA and the site principal investigator. “I believe the study data may offer further insight into Symphony’s potential to transform the treatment of patients with PE.”
“At Imperative Care, our mission to elevate thrombectomy care is rooted in a commitment to validating our innovations with robust clinical data to ensure we are engineering solutions that make a measurable impact on patient outcomes,” said Fred Khosravi, chief executive officer of Imperative Care. “Symphony is a critically important technology that is poised to transform treatment for patients with devastating pulmonary embolisms, a major cause of global morbidity and mortality. We greatly appreciate the investigators, clinical sites, and patients who have participated in this trial.”
Narayanan and a team member following their first case using IntelliBlate
This advertorial, sponsored by Varian, is intended only for readers in the USA.
Govindarajan Narayanan
Govindarajan Narayanan (Baptist Health, Miami, USA) recently spoke to Interventional News about the role of microwave ablation and confirmation software in his practice, charting his team’s early impression of their updated set-up.
Narayanan, who is an interventional radiologist and chief of interventional oncology at the Miami Cardiac and Vascular Institute for the Miami Cancer Institute—both of which are part of Baptist Health—has been performing ablations since 2001. During his earlier training, interventionalists commonly used radiofrequency ablation and gradually developed their practice through early iterations of microwave ablation.
In the literature, evidence for the efficacy of microwave ablation has grown, particularly via the recent publication of the COLLISION trial results in the January issue of The Lancet Oncology. The randomised, international, multicentre, phase III non-inferiority trial, led by Martijn Meijerink (Amsterdam UMC, Amsterdam, The Netherlands) et al, demonstrated comparable results between thermal ablation and surgical resection for small-size colorectal liver metastases—initiating re-evaluation of clinical practice and the previously held assumption that ablation should be reserved for unresectable lesions only.
“This study showed that ablation was non-inferior to surgical resection, but more importantly, that they had durability of outcomes and a shorter hospital stay for the patients who underwent ablation. Clearly, this level I evidence is already having an impact. In our practice, we have seen our surgical and medical oncology colleagues embrace these outcomes. This is going to make a huge impact on microwave ablation around the world, providing interventional oncologists with high-level evidence to show that ablation can go toe-to-toe with surgical resection in select patients,” Narayanan said.
For Narayanan, microwave ablation has become an “integral” part of his ablation programme. “It’s the workhorse of all of the ablation procedures that we do,” he commented. Used predominantly in the liver for colorectal liver metastases (CRLMs) and hepatocellular carcinoma (HCC), he added that microwave ablation is “quick, effective, and occupies an important part of helping us manage these patients”.
In early 2024, Narayanan and his team initiated the first robotic ablation programme with confirmation software. The planning and confirmation software “changed the way [his team] looks at ablation confirmation”, Narayanan said.
Narayanan reported that he and his team have observed a positive adjustment in their practice when using planning and confirmation software. “In the past, we would rely on contrast enhancement or lack of enhancement after the ablation procedure, and just try to use measurements to see whether we created an adequate margin,” he stated.
Now, however, Narayanan and colleagues are able to perform a volumetric assessment of the tumour prior to the ablation. Then, following the ablation, they carry out a post-ablation volume measurement and overlay the two images, “which gives us a clearer visual representation of whether our margins were correct, and, if we need to make adjustments, we can do that right away rather than waiting for first follow-up”.
Narayanan and a team member following their first case using IntelliBlate
At the end of 2024, Narayanan and his team were one of the first sites to trial the IntelliBlate microwave ablation system. The system, Narayanan described, is compact, reducing its footprint in their department. Using a touchscreen that provides real-time assessments and temperature readings of the ablation zone, his team reports that the system has been easy to implement and use. With the system’s dual-probe functionality, Narayanan is able to place two probes for simultaneous burns, creating a larger ablation zone than what could be achieved with one probe alone. “This is very helpful, it raises the bar, given that we are now expanding ablations to larger tumours,” he stated.
“In many ways, the IntelliBlate system has changed the way we perform ablation, and given the data that have emerged showing the importance of acquiring adequate margins, this change is crucial,” Narayanan added.
“Reliability used to be a problem when performing microwave ablation, as we were not able to predict exactly where the ablation zone might be, but this is a problem of the past with these newer devices. We feel that using confirmation software that provides this information in a reliable fashion right away, will definitely go a long way to producing good outcomes for our patients.”
“In our experience of using different devices, we’ve learned that each has its own nuances and advantages. Some of them also have disadvantages. So, to come up with a device that addresses some of the limitations or problems we’ve experienced with microwave ablation, and has been executed in the way IntelliBlate has, is a welcome addition to the microwave space.”
Narayanan and his team are currently collecting data on the combination of IntelliBlate with their robotic technology and planning software for microwave ablation. “So far, it has worked very well,” he stated, “but the more patients you treat, the more your experience is enhanced. We believe in collecting data and analysing it. In a few years, we will be able to see the picture this creates for the technology and publish on that,” he continued.
Of his final conclusions, Narayanan added that through the combination of quality data and more attuned technology, microwave ablation is fast being established as an “important player” in the management of patients with CRLMs. “We’re looking forward to seeing how our data look a year from now,” he said, maintaining that, with experience of the latest advancements in ablation technology, he believes that microwave ablation will continue to be a “mainstay” part of most interventional oncology practices worldwide.
A keynote session on the future of interventional oncology (IO) brought artificial intelligence (AI) to the forefront of discussion, highlighting both its potential and the ethical, legal, and regulatory challenges it presents. During his talk at the European Conference on Interventional Oncology (ECIO; 12–16 April, Rotterdam, The Netherlands), Gianpaolo Carrafiello (University of Milan, Milan, Italy) discussed the concept of “hybrid intelligence” as the likely future model, in which AI augments, rather than replaces, clinical expertise.
Beginning with a historical definition from AI pioneer John McCarthy, who described AI as “the science and engineering of making intelligent machines,” the speaker framed the discussion around AI’s emerging applications in IO. These include image analysis, segmentation, predictive modelling, decision support systems, and training for interventional radiologists. Particularly in education, AI has shown potential to help standardise and accelerate the training of new interventionists.
The session touched on the responsibility associated with deploying AI in clinical environments. “The decision to accept or override AI-generated recommendations requires careful justification,” Carrafiello explained, noting that regulation may demand well-documented reasoning from physicians who diverge from algorithmic suggestions.
Responsibility in AI use was broken down into three core elements: accountability, culpability, and liability. Carrafiello said that, while AI systems can be held accountable to the extent of explaining their processes and outputs, they cannot be held culpable, “as they lack consciousness, intent, or free will”. Legal liability, however, remains a more complex issue, often extending to developers, institutions, or clinicians depending on the case and regulatory framework.
The speaker identified transparency as a key principle in bridging these gaps. Carrafiello advocated for moving from a “black box” model— where internal AI decision-making is “opaque”, to a “glass box” approach where processes are “visible and understandable”.
“This is essential for building explainable AI systems that foster trust and accountability,” he said.
Yet, Carrafiello believes that transparency may come at a ‘cost’: “Simplifying models to enhance explainability can sometimes reduce predictive accuracy.” In healthcare, where outcomes may depend on precise treatment planning, this trade-off presents a practical challenge.
The legal frameworks guiding AI use in Europe was another focal point. The European Union’s Medical Device Regulation (MDR) currently classifies certain AI tools as medical devices, requiring CE marking unless developed exclusively for in-house use. Additionally, the 2021 EU Artificial Intelligence Act introduced a risk-based regulatory system, categorising AI in healthcare as “high risk” due to its potential impact on patient safety.
However, the speaker argued that these policies still fall short: “Current EU legislation does not sufficiently address the specific regulatory needs for AI in clinical specialities like interventional oncology,” Carrafiello noted. Gaps in legislation may hinder the development and deployment of AI tools in IO and leave gaps in regulation concerning post-market surveillance and algorithm bias, he added.
Expanding on bias in AI algorithms, Carrafiello pointed out that “AI algorithms may be less accurate for underrepresented or marginalised populations, reinforcing systemic inequities in access and outcomes,” and adding that this is particularly “troubling in oncology, where timely interventions can dramatically alter prognosis”.
The speaker then urged that interventional radiologists retain ultimate responsibility, explaining that “AI should be a support tool, not a decision-maker.” Carrafiello advocated for ongoing development in AI systems in IO, regular audits of AI-driven decisions, and transparent communication with patients about the use of AI in their care.
Carrafiello then suggested that hybrid intelligence, defined as the combination of human expertise with AI augmentation, will define the future of IO, however, interventionists that fail to adapt may fail to keep up, and will be left behind. “AI will not replace interventional radiologists, but those who use AI will replace those who don’t,” he said.
David Breen says that registries can quickly accrue data to prove the merits of certain interventions
David Breen
“Although [real-world registries] seem unsexy, it’s the direction of travel,” said David Breen (Southampton University Hospitals, Southampton, UK), describing the comparative advantages and challenges of randomised controlled trials (RCTs) and real-world registries in providing kidney tumour ablation data.
“Let’s talk honestly about RCTs. There are problems,” began Breen, during his talk at the European Conference on Interventional Oncology (ECIO; 12–16 April, Rotterdam, The Netherlands).
“Clearly, they set out to avoid bias and establish causality, but it’s a trade-off between experimental rigor and being able to generalise our data for its real-world applicability in daily practice.”
In general, Breen stated that RCTs are becoming “increasingly unaffordable” outside of a pharma industry setting. Conducting research in the interventional space sometimes means that professional “boundaries” will be crossed between surgery and interventional radiology (IR)— “we know that can bring problems for recruitment to randomised trials”.
The “unfortunate truth” is that some major steps in medicine have made it into standard practice without an RCT, Breen said, such as penicillin or resection for colorectal liver metastases, the latter of which exists at the level of 3b on the Evidence (EBM) Pyramid.
Returning to the kidney, Breen added that since the uptake of robotic-assisted partial nephrectomy, there has been no trial comparing the technique to open or limited-access partial nephrectomy.
Conducting RCTs evaluating ablation for kidney tumours comes with unique challenges, he went on to detail, describing renal cancer as an indolent disease process which negates the investigation of early outcome markers at one to two years. Coupled with the time and cost of setting up an RCT in this space, this often means “your new intervention is an anachronism by the time you’ve got data,” Breen stated.
So, what is real-world data? Breen asked, labelling it naturalistic data, often pulled by “digging into electronic health records [EHR]” which record a large volume of real patient data. In the UK, Breen highlighted the National Health Service (NHS) and UK Biobank, which he states are “phenomenally rich” datasets.
“There’s a reason Mark Zuckerberg and Jeff Bezos are our new best friends in the UK,” said Breen. “The NHS owns one of the largest volume and most consistent healthcare datasets exploitable in global healthcare.”
He went on to highlight the successes and failures of recent registries, highlighting ongoing efforts of the EUropean REnal Cancer CryoAblation Registry (EuRECA), established by a European Hospital network, with which Breen’s centre in Southampton is involved.
Awaiting release, Breen stated the registry team is currently sitting on prospectively collected data from approximately 1,700 patients treated with percutaneous cryoablation.
“Almost 1,500 of them are biopsy-proven, 14% in a single kidney,” said Breen. “There’s no partial nephrectomy series that is so rich with single-kidney data. The data is in preparation; it is clearly chronologically mature, this is going to be the practical direction of data accrual for healthcare providers and commissioners.”
“We’ve got to look at large real-world registries. If granular enough, we should ultimately be able to exploit artificial intelligence to try and get signals from the raw data and then go after those signals with much more targeted and hopefully easier to deliver RCTs,” Breen stated.
How are children treated at your local hospital? Asks paediatric interventional radiologist Alex Barnacle (London, UK) of healthcare providers today. Her question brings attention to the “insurmountable barriers” which paediatric interventional radiology (IR) faces, even in large, specialised centres. Affecting change, Barnacle’s outreach efforts span the globe, and her involvement with international societies is ongoing. Here, Barnacle—consultant paediatric interventional radiologist at Great Ormond Street Hospital for Children—shares the lasting impact made by her mentors, an early case that changed treatment management for the condition, and the collaborative work that must be done to resolve inequalities in paediatric IR.
What attracted you to a career in medicine, and what made you choose paediatric IR?
I was fascinated by paediatrics even as a medical student, but it took a long time to work out where exactly in paediatric healthcare I would thrive. I trained in neonatal intensive care, paediatric surgery and general paediatrics before being inspired by a wonderful paediatric radiologist and mentor—Jo Fairhurst—to consider paediatric radiology. After obtaining my paediatric qualifications, I transferred into radiology with the firm intention of becoming a diagnostic paediatric radiologist but fell in love with IR along the way.
For a while I was in turmoil, trying to choose between the two. I was fortunate enough to then be introduced to another key mentor, Derek Roebuck, who was developing a paediatric IR service at Great Ormond Street Hospital in London, UK. It was incredible timing, because he was probably the only one practising paediatric IR in the UK at the time and I immediately knew this was the career I had been searching for.
Who have been your mentors throughout your career and what is the best advice they have given you?
I have been inspired and encouraged by so many people along the way, and it continues, of course. Often, all it takes is one small thing someone says or does to leave a lasting impression or prompt us to reflect and change.
I am inspired by colleagues in industry, by the nurses and radiographers I work with, and by trainees as much as I am by senior interventional radiologists. Adam Mitchell was an inspiration in my very first year as a radiology trainee and taught me to be brave. James Jackson instilled in me a passion for treating vascular malformations. Within paediatric IR, Roebuck shaped both my career and my ambitions but I have also been inspired by many senior interventional radiologists within the wider paediatric IR community around the world.
Anna Maria Belli has been a key influence and support in my career, always encouraging me to break down barriers and aim high. And there are many brilliant women in IR who are role models for me and continue to inspire me to pursue excellence in IR and equality in our field—Laura Crocetti, Maureen Kohi, Gloria Salazar, and Tze Wah are just a few of these women.
Could you describe a case that has been the most memorable throughout your career thus far?
Only three years into my consultant career, I was referred a very young child with a lymphatic malformation of her orbit which had caused devastating consequences. I was familiar with treating malformations elsewhere in the body but never in the posterior orbit and I couldn’t find anyone in the UK who had treated one. I reached out to colleagues in the USA and Australia who supported me remotely. I performed three sclerotherapy procedures for her, with great trepidation. But the response of the malformation was truly remarkable and in a very short space of time she was pain free and getting back to being a happy and wonderfully courageous child. Since then, I have treated many, many children with this condition and together with some other interventional radiologists around the world, we have changed the management of this condition and the lives of these children. I am still in touch with this first patient and will always be grateful to her parents for trusting me with their precious daughter’s health when this was such a novel approach.
You are currently involved with the first Getting It Right First Time (GIRFT) initiative for IR in the UK. How has this experience been and what has been learned during the process so far?
It is a really innovative programme in England which takes a very detailed look at individual clinical specialties. Last year, the GIRFT programme for IR was launched and I am honoured to be the clinical lead. We review all the national IR data available and visit every hospital in England that performs IR. So far, my colleague Gill Kitching and I have visited 10 hospitals—only 112 to go!
We are looking for unwarranted variation in practice, particularly in patient outcomes, efficiencies in clinical care pathways and costs. Many departments are facing significant challenges in delivering the level of care they aspire to, particularly with current economic constraints, and we are often seeking support and advocate for them. And there are also teams who have developed novel ways of working and are delivering excellence in some areas of IR; we are mining for those pockets of excellence and aiming to disseminate examples of best practice. It is a privilege to visit so many IR departments and explore these themes with colleagues around the country. We are still in the early stages of the programme but emerging themes for me have been the relative disadvantages that some non-vascular IR services encounter compared to vascular IR services, and the lack of specialised training for nurses in IR. At the end of the project, we will publish a national report of our findings and recommendations.
You are currently on the executive committees of CIRSE and BSIR. How do these roles cross-pollinate with your daily practice?
It has been one of the unexpected privileges of my career to work with senior colleagues in the executive committees of the British Society of Interventional Radiology (BSIR) and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), as well as previously in the Society for Pediatric Interventional Radiology (SPIR). I find it hugely rewarding to collaborate on exploring future directions for our specialty and finding ways to support our talented colleagues at the coalface of IR. Leadership roles like these challenge me to develop very different skills to those typically used at the angiography table, and to broaden my horizons. I love exploring ways to bring people together to achieve their goals. It is an honour.
Are you still involved with ICECaP, the first paediatric ablation registry in Europe? If yes, what is the status of the registry?
The ICECaP registry is recruiting patients undergoing cryoablation for both benign and malignant disease. Our aims are to confirm that cryoablation is safe in small children and to establish which diseases cryoablation is most effective for. Paediatric IR case numbers for procedures like this are always going to be low in individual centres so it is imperative that we collaborate across institutions and countries to collate and examine our practice and provide much-needed outcome data to guide the development of IR for children.
What is an unmet need in paediatric IR today?
There are so many unmet needs in paediatric IR. Paediatricians, paediatric surgeons and children’s hospitals are still frustratingly slow to recognise the value that IR brings for children and their families. There is huge underinvestment in paediatric IR; it is maddening to see colleagues struggling to deliver IR procedures with exceedingly limited resources, even in large, specialist institutions. There are very few training posts in paediatric IR, especially outside of North America, which of course means a lack of paediatric interventional radiologists.
Paediatric interventional oncology (IO) is significantly hampered by the absence of IR options in almost all treatment and study protocols. And we are held back by the lack of paediatric-specific equipment. Most of the time we can find workarounds with standard adult IR devices and kit, but now even this is heavily impacted by the recent changes in European medical device regulation. There are now almost insurmountable barriers to device development for paediatric use and we are seeing longstanding devices removed from the market or being labelled as ‘contraindicated for paediatric use’.
My colleagues and I recently published a research needs assessment for paediatric IR which highlighted a number of barriers to meaningful research in our field, despite widespread interest within the paediatric IR community for collaborative research.1 The paper emphasises some important areas for us and our clinical teams to focus on going forward.
In my opinion, the area of greatest need, and an area in which IR can undoubtedly impact children’s healthcare, is in paediatric oncology. As in adult IO, we need to keep pushing our oncology colleagues for a seat at the table, so that we can demonstrate to them what we can do and together explore how IR can contribute to paediatric cancer care. I am thrilled that the European Society for Paediatric Oncology (SIOP Europe) will be welcomed as part of the CIRSE 2025 congress (13–17 September, Barcelona, Spain). SIOP Europe is the only pan-European organisation representing all professionals working in the field of childhood cancer and our most valuable partner in furthering paediatric IO in Europe.
What is your advice to young interventional radiologists entering the field of paediatrics today?
Paediatric IR is a hugely rewarding career path, and you will be part of an immensely warm and welcoming international community. Seek out paediatric IR colleagues at all of the major IR congresses to develop links with us and share ideas, and join us at the annual SPIR meeting (14–16 October, Sydney, Australia). Reflect on how children are treated in your local hospitals—are they are being offered the same IR options that adult patients are? Almost certainly not. Can you influence that? It will take all of us to change many of the current inequalities in paediatric IR care.
What does your life outside of medicine look like?
I have a busy and fun life outside of work. My husband Andy and I play a lot of tennis, and we enjoy travelling together. I am passionate about art, exploring and appreciating fine art in galleries around the world, but also drawing and painting myself. I have recently gone back to art school in the evenings and have a very small exhibition coming up at the end of the year.
References
Temple et al. Fostering research in pediatric interventional radiology: needs assessment and suggestions for support. Pediatr Radiol 2023 Oct;53(11):2245-2252. doi: 10.1007/s00247- 023-05722-6).
Results from the prospective, multicentre Liquid Embolization of Arterial Haemorrhages in Peripheral Vasculature (LAVA) study evaluating the Lava (Sirtex) ethylene vinyl alcohol (EVOH) liquid embolic have demonstrated a 94.3% primary effectiveness rate, exceeding a clinical performance goal of 72%.
“In the past five decades, many agents have been used in PAH [peripheral arterial haemorrhage], such as coils, plugs, particles, stent grafts, gelatine sponge, and liquid embolics,” write the study’s authors, led by Bulent Arslan (Rush University, Chicago, USA). Their paper, which was recently published in the Journal of Vascular and Interventional Radiology (JVIR), set out to identify whether liquid embolic agents could overcome some of the limitations of nonliquid agents. Liquid materials have been seen in some single-centre experiences to cause “near-complete, predictable, and permanent vessel occlusion, with reduced risk of incomplete occlusion due to coagulopathy and delayed recanalisation”, Arslan et al exposit.
The study included individuals aged 18 years or older with active haemorrhage in the peripheral vasculature, but no previous embolization in the target vessel and a life expectancy of more than 30 days. Enrolees were gained across 19 centres in the USA. PAH was defined as the presence of either active haemorrhage or pseudoaneurysm as diagnosed at endoscopy or catheter angiography or by computed tomography (CT) angiography.
Overall, 141 lesions were identified in 107 patients. Patients enrolled had a mean age of 57.4 years and 63.7% were male. Targeted areas included non-gastrointestinal visceral arteries (31.1%), kidneys (26.3%), upper gastrointestinal (GI) (11.5%), lower GI (6.8%), and extremities (6.1%). Arslan and colleagues describe that training was provided to all clinicians prior to the delivery of the EVOH agent. Ideally, the agent would be delivered via slow infusion not exceeding 0.3ml/ min from distal to proximal, with a gradual pull back to prevent catheter entrapment.
The primary effectiveness endpoint— clinical success at 30 days—was achieved in 133 of 141 lesions, and in 102 of 107 patients. Clinical success was defined as having satisfied four conditions: no bleeding from target lesion, no emergency surgery, no re-embolization, and no target esion reintervention.
Concerning procedural outcomes, adjunctive embolotherapy was used in 38 lesions. Bleeding following EVOH treatment was reported in nine lesions, while 144 lesions had “less bleeding” following the index procedure. Two target lesions treated with EVOH required subsequent re-embolization. A total of six (4.4%) adverse events occurred in five of 113 patients and the all-cause mortality rate at 30 days was reported as nine (8.3%) of 109—four patients exited the study before 30-day follow-up.
In a subgroup analysis, Arslan and colleagues add that clinical success was higher in males than in females, 98.9% and 86.3%, respectively, although major adverse event rate, technical success and intact retrieval of microcatheter rate at 30 days were similar between groups.
In their discussion, Arslan et al note that liquid embolic agents and mechanical occlusion devices can be “complementary” in certain settings, highlighting that 25.7% of treated lesions in their cohort required adjunctive embolics which were used concurrently with EVOH.
Although their study suggests that EVOH is safe and effective in PAH, the authors bring awareness to the diverse range of aetiologies and locations of bleed in their patient cohort which mean that their results cannot be generalised to a population that does not parallel the study’s population.
“The low rate of adverse events noted with EVOH is encouraging,” Aslan and colleagues write. “As with other liquid agents, the successful use of this device is associated with a short but steep learning curve.” The authors reiterate that the clinicians each had experience treating lesions with EVOH, and warn that adverse events may be more common if the operator is not experienced with the liquid agent.
Arslan et al state that these data provide a “higher level of evidence” in support of embolization of PAH than those in prior studies, which work to expand treatment options for the potentially life-threatening condition.
“For me, it was essentially love at first sight,” confessed Gary Siskin (Albany Medical Center, Albany, USA), stating his enthusiasm for liquid embolics—an enthusiasm that is shared by an increasing number of interventionists year on year, he says. As with many emerging technologies, however, benefit, risk and research must be considered before widespread adoption. Here, Siskin and other users speak on the current “fascination” with liquid embolic agents, their future, and the concerns that remain.
For Siskin, the incorporation of liquid embolics into his practice began with glue, “the earliest embolic agent” that was available to him and his team. “However, it’s hard to argue the effectiveness of glue,” he stated, due to the “artistry” of diluting glue to ensure successful deployment. As newer embolic agents emerged, the “idea of diluting the product and tailoring it to the indication that you’re using it for has kind of gone away,” said Siskin, leaving space for premade products.
“I think we’re approaching an ease-of-use era, which is going to allow for wider adoption and adaptation of liquid embolics,” he continued. This, he believes, will provide several benefits to interventionists, including reaching hard-to-access vessels, improved packing density and cost-effectiveness.
Enabling him to reach the previously unreachable, Siskin told Interventional News that he frequently uses liquid embolic agents to treat peripheral haemorrhage, vascular malformations, and endoleaks, while having recently expanded to some venous indications. However, “we always need to be comfortable with where the liquid might travel”, he added, noting that this factor plays a large part in identifying a “good” or a “bad” case for the use of a liquid embolic.
“For example, we do bronchial embolization. It might be nice to use a liquid, but there’s a risk of embolizing the spinal cord and sometimes this is not easy to see, so we don’t take the chance,” Siskin said. “I also don’t necessarily think we should be [using liquid embolic agents] in fibroids or knee arthritis—people are starting to use them in prostate embolization, but I think we have a way to go before we can routinely recommend that.”
Siskin described that the “most valuable” quality of liquid embolics are their superior packing density, which he believes rivals coils in both level of occlusion and efficiency. He explained that it is often challenging to fill a vessel with coils, despite only needing to fill a third of the vessel lumen. “It’s difficult to conceptualise that you aren’t filling as much of the vessel as you think,” but with a liquid embolic “if done the right way, it can fill close to 100% of the vessel, maximising packing density in a way that other products can’t ever hope to achieve,” Siskin stated.
“Generally, the teaching that we give people for liquids is to inject them very slowly, especially agents like LAVA [Sirtex] or Onyx [Medtronic]. Even injecting them as slow as you need to, it still results in an occlusion that takes less time than putting in multiple coils or other embolics. I have found that using liquids is a very efficient way to embolize blood vessels,” said Siskin.
Ascribing improved efficiency to enhanced cost-effectiveness, Siskin stated that theirs has become a “liquid-first” practice. Although liquid embolic agents “look cost prohibitive at first glance”, Siskin revealed that a small amount of product is needed to embolize the average vessel, which initiated a “wholesale change” in his practice.
Siskin added: “The reality is that all of the products that we use are getting progressively more expensive. If you’re using, let’s say, pushable coils and first-generation detachable coils, you’re probably not going to be able to make an economic case for liquids. But, if you are using the next endovascular coils or packing coils, you will find that these are very cost-effective and will make a lot of sense for your practice.”
Several studies have recently provided data on liquid embolic agents, including data from the LAVA (Sirtex) trial which found ethylene vinyl alcohol to be safe and effective for peripheral arterial haemorrhage. For Siskin, gaining these insights through clinical trials is “critical”, especially for the peripheral use of liquid embolic agents, so that “appropriate training can finally be given to interventional radiologists”.
Siskin highlighted that enthusiasm for liquid embolic agents is deserved, but interventionists should take adoption “slow”. In the near future, he hopes that ongoing trials will bear out the safety and efficacy of deeper penetrating embolic agents which he believes will have “big potential” for IR.
For now, he asserted that interventionists should aim to understand when is best to use liquid embolic agents: “You’re going to want to look at risk—risk of distal or non-target embolization. Understand the flow in your target vessel. Look at vessel size. Understand the volume of embolism that we reach.”
“We can play two truths and a lie here and say: interventional radiology [IR] is dependent on technology; there will always be new technology that can be easily taken up by interventional radiologists; and IR will always want these technologies. The lie is that it’s easy. Interventional radiologists are largely always interested in learning something new, but I think it’s concern that may hold people back,” said Siskin. “It’s just a question of the interest in bringing something new into your practice and then getting the education and the experience that gives you the confidence to use it correctly.”
Conventional pre-shaped microcatheter technology has evolved over the last decade, yet significant limitations still exist. In particular, the shape of a standard microcatheter cannot be changed or manipulated while inside a patient’s vasculature. As a user of this innovative technology, Jason C Hoffmann (New York, USA) details his first-hand experience.
Selective cannulation of small arterial branch vessels for targeted/superselective angiography or embolization is commonly performed; however, conventional pre-shaped microcatheter use has limitations when in complex arterial vasculature, including tortuous or angulated vessels.
In these scenarios, the operator must often perform multiple microcatheter and wire exchanges to select the target vessel. This can take a considerable amount of time, require use of numerous devices, and may result in a substantial radiation dose to the patient and procedural staff. If the target vessel cannot be superselected, a less-targeted embolization must be performed, or the procedure is abandoned altogether. In either scenario, the case will take longer, with implications for increased cost and resource use, and has the potential for complications and untoward events.
The development of a steerable microcatheter (SwiftNINJA® steerable microcatheter; Merit Medical Systems) is an innovation that offers an alternative approach to selective cannulation. This technology represents a new class of device, designed with a tip that articulates up to 180 degrees in opposing directions, providing real-time ability to change the angulation of the microcatheter tip while navigating through the vasculature.
The device can be used with or without a microwire which allows the injection of contrast while advancing or manipulating the steerable microcatheter. In my experience, this consistently leads to efficient selective cannulation of small vessels throughout the body, with a level of steerability that simply is not provided by any pre-shaped conventional microcatheter.
I can also inject contrast while advancing or manipulating the steerable microcatheter, allowing for precise control and improved vessel targeting. Decreased time to target vessel selection can have multiple benefits for the patient, primary operator, and procedural staff in the room. Advantages include decreased procedure times, increased procedural efficiency, fewer microcatheter and microwire exchanges, reduced fluoroscopy times, and lower radiation exposure.
SwiftNINJA steerable microcatheter use in moderate and high complexity angiography and/or embolization has routinely helped me to be successful and efficient. In 2019, I published my results, comparing steerable microcatheter to conventional microcatheter use in 40 procedures that involved moderate to highly difficult vessel selection.1 Statistically significant improvements in target vessel selection time—12 vs. 462.5 seconds (Figures 1a-b)—number of microwires used (0 vs. 2), total procedure time (75 vs. 112.5 minutes), and body-mass index (BMI) adjusted radiation exposure were found in the steerable microcatheter group.
Since publishing my early steerable microcatheter results, I have used the device in hundreds of prostate artery embolization (PAE) procedures, as well as superselective embolization of distal hepatic, renal, bladder, visceral and small pelvic arterial branches in a variety of scenarios. Cases have included treatment of traumatic injury, benign prostatic hyperplasia (BPH), hematuria, malignancy and non-traumatic causes of bleeding. Most of these procedures were performed with only the steerable microcatheter, and no microwire was needed. I continue to find that patients and my team benefit from steerable microcatheter use due to increased efficiency, high technical success rates, reliable target vessel selection and decreased radiation exposure.
Reducing vessel selection time in a prostate artery embolization case
An 85-year-old man with a long-standing history of BPH presented with severe lower urinary tract symptoms (LUTS) and intermittent gross hematuria. Despite multiple medical treatments, including three transurethral resection of the prostate (TURP) procedures over the past two years, the patient’s condition had not improved. His International Prostate Symptom Score (IPSS) was 29 (severe), and his Urinary Quality of Life Score was 5 (unhappy).
Using a 2.4Fr SwiftNINJA through a 5Fr guide catheter, the left prostatic artery was selected in 12 seconds without a guidewire thanks to the steerability of the microcatheter tip. Proximal and then distal embolization of the left prostate artery with 300–500μ Embosphere microspheres (Merit Medical) was performed following the proximal embolization first, then embolize distal (PErFecTED) technique. The right prostate artery was then selected–again using the SwiftNINJA without a guidewire—in nine seconds and embolization was performed using the same technique.
Figure 1. Left prostatic artery selected with SwiftNINJA steerable microcatheter. Initial internal iliac artery angiogram demonstrates Type 1 anatomy, with common origin of the left superior vesical artery and prostate artery (a). The microcatheter was moved from tip of 5Fr catheter to target vessel (distal aspect of main left prostate artery) in 12 seconds (b).
Final angiography confirmed successful embolization of both left and right prostatic arteries. The patient was discharged the same day, with no hematuria or urinary retention reported since the procedure. At one month post-procedure, patient’s IPSS decreased from 29 to 7 and Urinary Quality of Life score decreased from 5 to 1.
Successful gonadal vein embolization through extremely tortuous anatomy
A 43-year-old female presented with chronic pelvic pain. Despite extensive diagnostic work-up, no definitive cause for the pain was found, except for prominent left parauterine veins/varicosities and an enlarged left ovarian vein.
The patient was diagnosed with symptomatic pelvic venous reflux/pelvic congestion syndrome, and the plan was to proceed with venography and embolization. Due to extreme tortuosity of the gonadal venous vasculature preeminently, a 2.4Fr SwiftNINJA steerable microcatheter was used to efficiently navigate through the extremely tortuous vessels and into the inferior aspect of the left ovarian vein. Embolization was performed with sodium tetradecyl sulfate sandwiched in between packs of platinum microcoils.
Post-embolization digital subtraction venography demonstrated an appropriate angiographic result, with embolization of the left ovarian vein, but brisk antegrade blood flow in the left renal vein. The patient was discharged home in stable condition four hours post procedure, and experienced only mild flank discomfort for 24–36 hours post-procedure, relieved with ibuprofen. Her pelvic congestion syndrome symptoms markedly improved by the time she was seen for a post procedure office visit approximately six weeks later (Figure 2a-b).
Figure 2. Left renal vein digital subtraction venography (DSV) via 5Fr catheter demonstrates patency of the left renal vein and inferior vena cava, with very prominent, tortuous and enlarged left gonadal vein (a). A 5Fr catheter was only able to select the most superior aspect of the left ovarian vein due to its extreme tortuosity. The SwiftNINJA steerable microcatheter was used to navigate through the multiple 180 and 360-degree turns to easily be passed inferiorly to the pelvis to perform embolization (b).
References
Hoffmann, J.C., Minkin, J., Primiano, N. et al. Use of a steerable microcatheter during superselective angiography: impact on radiation exposure and procedural efficiency. CVIR Endovasc 2, 35 (2019). https:// doi.org/10.1186/s42155-019-0078-9
Jason C Hoffmann is an interventional radiologist with NYU Langone Health in Mineola, New York, USA.
Musculoskeletal (MSK) embolization—including techniques such as transarterial microembolization (TAME) and genicular artery embolization (GAE)—has emerged as a novel, minimally invasive treatment for chronic joint and tendon pain. Initially applied to conditions such as knee osteoarthritis (OA), frozen shoulder, and tendinopathies, these procedures target hypervascular inflammation, a key contributor to chronic MSK symptoms. While early data are promising, the field is still maturing. Here, Gerard Goh (Alfred Hospital, Melbourne, Australia) and Yuji Okuno (Okuno Clinic, Tokyo, Japan) collaborate to raise several critical questions that, at present, remain unanswered.
Top 5 unanswered questions
Generating high-quality evidence
To date, much of the literature on MSK embolization consists of case series and single-arm studies. While these have reported significant reductions in pain and improvements in function, randomised controlled trials (RCTs) remain limited. Notably, the few RCTs published have produced mixed results—one demonstrated clinical benefit, while another showed no significant difference from placebo.1,2 These findings raise concerns about placebo effects and highlight the need for more rigorous evidence. Larger trials in the UK, France, and US are ongoing and may help define the clinical value of these procedures.3,4,5
Optimising indications and patient selection
Knee OA is a heterogeneous disorder with varying underlying causes and pathologies. While GAE appears beneficial for many, it is still unclear which patients are most likely to respond. Pre-procedural magnetic resonance imaging (MRI) findings have shown potential in predicting outcomes, but reliable imaging-based criteria for patient selection remain underdeveloped.6,7 Similar uncertainties exist for other conditions such as frozen shoulder and sports-related injuries, where the roles of contrast-enhanced MRI and other imaging modalities are still being clarified.
Additionally, as pain is a subjective experience, psychological factors such as catastrophising, anxiety, and depression may influence outcomes. These aspects should be considered in future studies aimed at refining patient selection frameworks.
Improving outcome assessment methods
Pain assessment traditionally relies on tools such as the Visual Analog Scale (VAS) and Numerical Rating Scale (NRS), which capture pain at a single time point. However, these tools are susceptible to environmental and emotional factors, leading to variability. Broader functional scoring systems—such as Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) or Knee Injury and Osteoarthritis Outcome Score (KOOS)—offer more comprehensive evaluations but depend on retrospective recall and may introduce bias.
Emerging approaches like Ecological Momentary Assessment (EMA) allow for multiple real-time inputs, providing more granular insights into daily symptom variability. Likewise, wearable devices can objectively track activity levels and function. Integrating these multidimensional tools into outcome assessment may improve the reliability and relevance of future research.
Refining embolic materials and techniques
One consistent finding in the literature is that embolic materials smaller than 100 micrometers are associated with higher complication rates, irrespective of whether they are temporary or permanent. Beyond this, however, consensus on the optimal type of embolic agent is lacking.
Temporary embolic agents are widely regarded for their safety, while permanent agents may offer longer-lasting benefits, particularly in progressive conditions like knee OA. Some propose combining both— utilising the short-term safety of temporary materials with the durable effects of permanent embolics. This hybrid approach could offer a balanced therapeutic profile.
Outside the knee, evidence is even scarcer. Recent findings suggest that in the elbow joint, using smaller embolic volumes can minimise complications and enhance clinical results. As the field evolves, tailored strategies for each joint and disease type must be developed, accounting for anatomical and physiological nuances.
Clarifying long-term outcomes
While many patients report sustained symptom relief for up to two years post-embolization, data on long-term durability remain sparse. It is unclear whether embolization alters the course of disease or simply provides temporary relief. Key questions remain: Can embolization delay or prevent joint replacement surgery? What is the efficacy of repeat embolizations? And how does embolization affect joint structure over time?
To address these, extended follow-up of existing cohorts and the establishment of prospective registries will be critical. Understanding long-term safety and efficacy will determine the role of MSK embolization in the treatment continuum.
MSK embolization is an innovative and promising addition to the therapeutic arsenal for chronic musculoskeletal pain. Offering a minimally invasive, targeted alternative for patients unresponsive to conservative care, it has the potential to bridge the gap between medication and surgery. However, its future depends on addressing key uncertainties through robust clinical trials, refined patient selection, optimized embolic techniques, and comprehensive long-term data. The next few years will be pivotal in determining whether MSK embolization becomes a standard of care or remains a specialised intervention for select cases.
Gerard Goh is an interventional radiologist at the Alfred Hospital in Melbourne, Australia and Yuji Okuno is an interventional radiologist at the Okuno Clinic in Tokyo, Japan.
References
Bagla S, Piechowiak R, Sajan A, et al. Multicenter Randomized Sham Controlled Study of Genicular Artery Embolization for Knee Pain Secondary to Osteoarthritis. J Vasc Interv Radiol. 2022 Jan;33(1):2- 10.e2
van Zadelhoff TA, Bos PK, Moelker A, et al. Genicular artery embolisation versus sham embolisation for symptomatic osteoarthritis of the knee: a randomised controlled trial. BMJ Open. 2024 Oct 1;14(10):e087047.
Little MW, Harrison R, MacGill S, et al. Genicular Artery Embolisation in Patients with Osteoarthritis of the Knee (GENESIS 2): Protocol for a Double-Blind Randomised Sham-Controlled Trial. Cardiovasc Intervent Radiol. 2023 Sep;46(9):1276-1282.
van Zadelhoff TA, Okuno Y, Bos PK, et al. Association between Baseline Osteoarthritic Features on MR Imaging and Clinical Outcome after Genicular Artery Embolization for Knee Osteoarthritis. J Vasc Interv Radiol. 2021 Apr;32(4):497-503.
Choi JW, Ro DH, Chae HD, et al. The Value of Preprocedural MR Imaging in Genicular Artery Embolization for Patients with Osteoarthritic Knee Pain. J Vasc Interv Radiol. 2020 Dec;31(12): 2043-2050.
Recently published in the British Journal of Radiology (BJR), a retrospective case-control study has found nulliparity to be “strongly associated” with the incidence of clinically significant post-embolization syndrome (csPES) after uterine artery embolization (UAE).
“This risk factor has not previously been shown to be associated with csPES,” write the authors of the PREDICT-PES study, led by Warren Clements (Alfred Health, Melbourne, Australia). Their cohort, comprised of 69 patients with a mean age of 46.2 years and a mean uterine volume of 393ml, all underwent UAE for symptomatic fibroids between 1 March 2022 and 1 September 2023.
Clements and colleagues defined csPES as the maximum pain score on visual analogue scale of greater than five out of 10, plus at least one of: morphine patient-controlled analgesia dose of less than 10mg, fever, or the use of two or more antiemetics.
The rate of csPES in their cohort was 47.8%, Clements et al report. Most patients had a single fibroid and fibroid disease that was largely intramural in location, while previous pelvic surgery and/or preoperative anaemia was common in both groups. Their results showed that nulliparity increased a patient’s risk of developing csPES by 5.5 times compared to patients who are primiparous or multiparous. Additionally, after adjusting for confounding, the authors report a trend that shows 13% reduced odds of developing csPES for every year increase in age.
The authors note that there have been very few studies identifying which patients are at higher risk of developing a more significant form of PES. In 2009, Ruuskanen et al assessed 62 patients with csPES following UAE and found that a larger volume of embolic agent plus more ischaemia via magnetic resonance imaging (MRI) correlated with the level of pain experienced. Thus, it was suggested that if ischaemia causes pain, larger fibroids and/ or smaller particles are more likely to cause csPES.
Yet, Clements and colleagues detail that this hypothesis has been refuted in a small number of studies to date, showing that postoperative pain did not show an association between median uterine volumes.
“While the univariate analysis in this study did show an association between median uterine volume and csPES, after adjusting for confounders, this was no longer significant and suggests that the effect in our cohort was due to the influence of other variables,” Clements et al write. “This is important as, in the experience of the authors, many women with very large fibroids do not get referred for embolization and are also often not considered suitable for myomectomy. Thus, they may miss out on an opportunity for a uterine-spring treatment.”
Clements et al note several limitations of their study, stating that the Australian demographic and awareness of UAE are reflective of “current referral patterns” resulting in their relatively small cohort size. They state that the short time span of the study was due to the implementation of premedication protocol, which changed from oral to intravenous, meaning the authors were able to evaluate “a controlled group without external influences”.
Practically, the authors state that these results will improve their informed discussion process. As pre-procedure counselling of a patient’s csPES risk is “difficult to predict”, Clements and colleagues note that they previously provided a “more generalised warning to all patients regarding likelihood of pain” following UAE, particularly in nulliparous patients.
“We can use this information to better counsel our patients regarding the odds of csPES when these risks are present, leading to an improved consent process, and the ability to plan more targeted pain management for women who are known to be nulliparous,” the authors conclude.
Left to right:
Pereira, Burgmans, Crocetti, and Arnold
Left to right: Pereira, Burgmans, Crocetti, and Arnold
In a discussion among leading figures in interventional oncology (IO), consensus developed around the growing clinical relevance of the field and the pressing need for data to match this. Speaking during a panel debate at the recent European Conference on Interventional Oncology (ECIO; 12–16 April, Rotterdam, The Netherlands), participants tackled the practical and philosophical challenges of positioning IO alongside surgery, systemic therapy, and radiation as the fourth pillar of modern cancer care.
Kicking off the session, Laura Crocetti (Cisanello University Hospital, Pisa, Italy) emphasised the need for guideline inclusion beyond liver-focused indications. “We are involved in the treatment of many kinds of cancer, not only colorectal liver metastases. I’m thinking about thyroid, about kidney—we should be in all the guidelines, but we need research. We must produce data; this is very important. Research is a major point for us.”
This sentiment was echoed throughout the session, as speakers repeatedly returned to the theme of high-quality clinical service and evidence generation. “We must provide a clinical service—without that, [IO] is never going to fly,” said Mark Burgmans (Leiden University Medical Center, Leiden, The Netherlands). He described that in providing a clinical service, equipped with all of the new tools and techniques the field has gained over recent years, interventional oncologists will need to prove themselves in clinical studies. He cited Martijn Meijerink et al’s COLLISION trial—which was a randomised, international, multicentre, phase III non-inferiority trial which demonstrated comparable results between thermal ablation and surgical resection for small-size colorectal liver metastases, as a benchmark example of how IO can deliver high-quality randomised controlled trial (RCT) data.
Yet others questioned whether RCTs should be the default path forward. Dirk Arnold (Asklepios Tumorzentrum Hamburg, Hamburg, Germany) reflected on his shift in thinking that he presented during his ECIO Honorary Lecture in 2023: “Two years ago, I made the claim that you should not focus too much on randomised trials, because it’s a therapeutic principle between widespread metastatic disease and localised metastatic disease, localised disease. You will get so much evidence by optimally treating patients and integrating therapeutic algorithms. This may be enough.”
However, Arnold stated that the publication of COLLISION results “contradicts” this thinking, acknowledging that RCT data instils greater confidence in situations where it is necessary to compare local ablative treatment to resection. To this, Burgmans stated that RCTs are not always necessary, “but unfortunately we sometimes face debates with colleagues and health insurance, with authorities who say that they want us to provide randomised, phase 3 trials with a survival benefit,” he said.
“Sometimes medical oncologists annoy me a bit with their rigid thinking that we always need RCTs to prove that something is worth doing,” continued Burgmans. He added that endpoints like progression-free survival and quality of life should also be accepted, especially where overall survival is difficult to assess.
Phillippe Pereira (SLK-Clinics GmbH, Heilbronn, Germany) reinforced the financial burden of trials, calling RCTs “very expensive” and arguing that real-world data and registries could provide a more feasible evidence base. “Interventional oncologists are very strong in producing registries. Some papers have shown that there is a very good correlation between the result of [an] RCT and the result of the real-world analysis,” Pereira explained.
Moving on, the panel turned to the increasing complexity of IO, given the rapid innovation in tools and technology, and the workforce’s capacity to keep up. “We all agree that we will need to move forward in a multidisciplinary way, but it will be very complicated,” said Pereira. “There are so many drugs and possibilities— local treatment, sequential treatment, and so on. We will need artificial intelligence.”
Arnold agreed, suggesting a reversal in the traditional scientific methodology. “We must collect what we see. We must document and analyse this with artificial intelligence to detect the factors that influence long-term survival, reverting the art of science. We don’t bring a theory to an experiment and observe. We observe, and then we have to ask what led us to this observation,” said Arnold.
Though the discussion ended with cautious optimism, Crocetti stating that they must “continue to dream” for a better future for IO, Pereira pushed for pragmatism. “I don’t like to end the discussion with a dream. We have been dreaming for the last 30 years, but IO has reached a crucial point now,” he said.
Photo by EPNAC.com courtesy of Society of Interventional Radiology
Celebrating the 50th anniversary of the Society of Interventional Radiology’s (SIR) annual scientific meeting (29 March–2 April, Nashville, USA), Lindsay Machan’s (University of British Columbia, Vancouver, Canada) Charles T Dotter Lecture turned to innovating innovation, honouring Dotter to show the strides technology has made since interventional radiology’s (IR) inception.
“In the 50th year of SIR, it seems best to talk about how innovation is changing,” Machan said. He recalled how IR pioneer Ernest Ring had described the meeting as ‘a bunch of people excited to see others who were doing the same things they were’—“and that’s actually how I think all of us feel about this meeting today,” Machan reflected.
Sink or swim
Individually, Machan’s relationship with innovation has been unique. He described his first staff job at Hammersmith Hospital in London, UK in 1989, when Hans Walsten was promoting the Wallstent (then Medinvent, now Boston Scientific). “Over 1,200 had been inserted into bile ducts and virtually every artery throughout the body in Europe. All the dogma at the time said that there was a 2% failure rate. Especially in certain places, they were restenosis machines, you could see that,” he described. Machan tried various methods of preventing this outcome to no avail, until encountering a medical student presenting his premedical work on cartilage-derived angiogenesis inhibitors in animal models of rheumatoid arthritis.
“The room was empty, almost nobody was there. Bill Hunter began talking about new blood vessel formation and the fact that tissue can’t grow more than two millimetres away from a capillary unless it’s cartilage or cornea—so in essence, inhibition creates zones of exclusion,” said Machan. Approaching Bill after his talk, Machan admitted that he knew little about animal models of rheumatoid arthritis, but that he believed it would make the ideal stent coating.
Starting their company, Machan, Bill and Larry Arsenault promptly raised CDN$100,000. “And then we made a very important discovery—it didn’t work,” Machan stated. Consulting an expert in biochemistry, the three founders shortly discovered that by coating their stent with paclitaxel, the active ingredient in the chemotherapeutic agent Taxol, they were able to achieve angiogenesis inhibition, creating their desired exclusion zone.
“We’re back in business, baby,” said Machan. “So, we do some bench, small and large animal experiments, but we needed to deal with one big problem and that was that, at the time, Taxol had up to a 30% anaphylactic rate.” Machan notes that this reaction was considered attributable to a solubilisation agent, Cremophor—a castor oil derivative—but there were lingering concerns it could be related to paclitaxel itself, which threatened “to sink us”, he stated.
During this time, however, Machan described a patient who had oesophageal cancer who had had two failed attempts at dilation.
“His grandkids wouldn’t come to visit him because he couldn’t swallow so was always spitting up. He just said he wanted to be able to eat ice cream and drink scotch. So—and I would go to jail for this now—I went across to our lab and we packed as much paclitaxel and ethylene vinyl acetate as humanly possible onto this removable oesophageal stent,” Machan told the SIR 2025 audience. “I sweated bullets overnight. I went in the next morning and there he was with three little dixie cups on his mail stand, and he threw me this presumed scotch-induced grin, so we knew were in business,” recounted Machan.
Photo by EPNAC.com courtesy of Society of Interventional Radiology
In 1992, Machan and his other co-patentors signed a co-exclusive license with Boston Scientific and Cook Medical for their paclitaxel-coated stent, despite five years of talks with various companies. “We had received a cash offer, so I went up to Boston and Cook and said, ‘I don’t know if you guys are just being nice to me but if an alternative doesn’t arise, this deal is going to go through on Monday’. By that Saturday at 9am, we confirmed that FOMO [fear of missing out] is still the most important factor in so many ways,” Machan said.
“What did I learn from all of this?”
His trajectory through innovation taught Machan that observing opportunities for innovation is key, he stated. “‘Honour every opportunity to learn something new’—it’s a fantastic quote. My first instinct was to not go to that premedical presentation because it was on something I didn’t understand, but I went and it changed my life. Work with people who have other skills,” Machan continued. “But, boy, are luck and timing everything. Then finally, work on a problem that someone will pay for. It’s great to do research, but if you want to get it into a patient, unfortunately you have to have a commercial alliance.” It is this commercial element that has become a larger part of innovation today, stated Machan, but the “cascade of steps” to take “an idea on a napkin to getting it patented and regulated hasn’t changed, and you can’t skip any of them,” he added.
What has changed, however, is where innovators look for opportunities, Machan said. “First of all, you follow the money,” he stated. On one side, there are the “inconvenient truths” of needing to control unsustainable healthcare costs; at the same time there are significant changes set to transform future healthcare, including casting the patient as a consumer and the integration of artificial intelligence (AI) within the treatment algorithm.
Regarding the former, Machan spoke on the democratisation of cardiovascular care at home. Using the example of smartwatches that can monitor and record your heart rate and sympathetic tone, the speaker stated that “this new era of health has resulted in the combination of digitalisation and consumerisation”. The result of this has meant that companies such as Google and Meta, “who haven’t gone through the slings and arrows that other medical companies have, and with the irrationality of the business of healthcare,” Machan added, create a new landscape for patients and healthcare providers to navigate.
“But I said follow the money,” Machan continued. “Think about efficiencies, quantum leaps, efficacy and safety, while empowering lesser trained members of the healthcare team.” To exemplify this stance and the democratisation of teaching, the speaker described the history of the stethoscope, and how the tool required specialised expertise which created barriers as to who could deliver healthcare.
“Now, in everyone’s pocket there is a device that can interface with a digital stethoscope, recognising heart and lung sounds, and can tell you what these represent,” described Machan. “This means that every general or nurse practitioner now has the expertise of an Ivy League cardiologist immediately available to them. This reduces, for instance, unnecessary referrals from rural areas or for functional murmurs in children.”
AI in the real world
Machan subsequently touched on AI and the introduction of AI innovation at a societal level. Machan noted how Truveta, among a growing number of comparable companies, is able to extract and interrogate healthcare data from millions of patients daily, drawing on these data to further clinical research. Referencing a publication by Monteleone et al, comparing ultrasound-assisted catheter-directed thrombolysis versus mechanical thrombectomy in over 83 million patients, Machan drew attention to the wealth of procedures and outcomes that can be studied.
With the ability to provide real-world data, these emerging AI programmes are bringing to the fore the realisation that “what happens in the real world doesn’t necessarily happen in controlled company-sponsored trials”, Machan stated.
Finishing his talk, Machan ruminated on what Dotter would say to early career interventional radiologists seeking to innovate today. In his view, Dotter would urge them to be curious, collaborate and record what they learn, and to protect the spirit of IR, leaving the speciality better than they found it.
Key updates from several meetings including the Society of Interventional Radiology (SIR; 29 March–2 April, Nashville, USA) annual scientific meeting, the Charing Cross (CX) Symposium (23–25 April, London, UK), and the European Congress of Interventional Oncology (ECIO; 12–16 April, Rotterdam, The Netherlands)
Raising critical unanswered questions, Gerard Goh (Melbourne, Australia) and Yuji Okuno (Tokyo, Japan) give their point of view on musculoskeletal embolization and its development as a novel technique
Geographic information mapping identifies IR expansion opportunities to combat postpartum haemorrhage in Kenya
Key updates from several meetings including the Society of Interventional Radiology (SIR; 29 March–2 April, Nashville, USA) annual scientific meeting, the Charing Cross (CX) Symposium (23–25 April, London, UK), and the European Congress of Interventional Oncology (ECIO; 12–16 April, Rotterdam, The Netherlands)
Raising critical unanswered questions, Gerard Goh (Melbourne, Australia) and Yuji Okuno (Tokyo, Japan) give their point of view on musculoskeletal embolization and its development as a novel technique
Geographic information mapping identifies IR expansion opportunities to combat postpartum haemorrhage in Kenya
Imperative Care has today announced that the Zoom stroke system has been further expanded with the launch of the Zoom DuoPort technology, which allows physicians to use the novel continuous dual aspiration technique (CDAT) on two Zoom aspiration catheters simultaneously from a single vacuum source.
“The launch of CDAT and Zoom DuoPort is the result of our direct partnership with physicians who participated in the Imperative trial and provided feedback on the need to make their procedures more efficient when applying aspiration to two Zoom catheters at the same time,” said Ariel Sutton, general manager of Imperative Care’s stroke business. “We have introduced a full-system approach, starting with arch access and 0.088-inch intracranial access, through complete clot ingestion with asymmetric aspiration. Now, the CDAT approach allows physicians to achieve the benefits of our full system using dual aspiration.”
Earlier this year, the company received US Food and Drug Administration (FDA) 510(k) clearance for its Zoom system, the first comprehensive stroke thrombectomy system to include large-bore 0.088-inch catheters indicated for both access and aspiration when used with a Zoom catheter. In a press release, the company has stated that clinical data from the Imperative trial supporting clearance of the Zoom system showed that dual aspiration with Zoom is fast, effective, and safe in patients with a range of complex anatomies. Now with the introduction of CDAT and Zoom DuoPort, the Zoom system is the first and only system to enable continuous dual aspiration for stroke thrombectomy.
“Data from patients treated with dual aspiration in the Imperative trial demonstrated a 19-minute median case time from groin puncture to mTICI ≥2B reperfusion—the fastest reported time of major prospective mechanical thrombectomy trials. Zoom DuoPort and the CDAT approach elevates the benefits of dual aspiration even further, with the goal of making stroke thrombectomies with the Zoom system faster, easier, and more effective,” Sutton added.
In one of the first cases, performed by Hakeem Shakir (Oklahoma University Health, Oklahoma City, USA), the patient presented with an occlusion of the ICA-terminus. The Zoom VTK insert catheter was used to select the vessel, followed by access with Zoom 88.
Both Zoom 88 and Zoom 71 maintained continuous dual aspiration from a single Zoom Pump, enabled by Zoom DuoPort, which resulted in a first-pass TICI 3 revascularisation with clot captured in the Zoom 88 catheter.
“In this case, a first-pass TICI 3 result was made possible because of the control I was able to achieve with continuous dual aspiration. Without CDAT, an additional pass would likely have been required,” said Shakir. “The CDAT approach using the Zoom System represents a significant clinical advancement in the field of stroke care that allows for continuous aspiration on two catheters and rapid, real-time feedback within the sterile field with Zoom POD. Prior to the introduction of Zoom DuoPort and CDAT, I would have to use two pumps to maintain aspiration, or sacrifice aspiration control with a syringe. In my experience, CDAT is a more common-sense approach to aspiration thrombectomy that streamlines the process, optimises efficiencies and brings me immediate confidence that the stroke-causing clot has been captured.”
iVascular has announced that its Luminor drug-coated balloon (DCB) is now available in Japan.
“This approval from the MHLW [Ministry of Health, Labour and Welfare of Japan] is evidence of the quality, safety, and efficacy of Luminor DCB,” said Lluis Duocastella, chief executive officer at iVascular. “We are thrilled to bring this innovation to the Japanese market together with Medico’s Hirata, as we continue our mission to improve vascular health worldwide.”
iVascular notes that Medico’s Hirata is a renowned Japanese medical company specialised in the distribution of advanced healthcare solutions. “This partnership will ensure that Japanese healthcare professionals and patients have access to a safe and effective DCB, with excellent clinical evidence,” the company states in a press release.
iVascular shares that it has developed a Luminor specifically for Japan—Luminor 18 RX, which the company claims is the most capable peripheral rapid exchange DCB currently available in the Japanese market.
Yoshimitsu Soga (Kokura Memorial Hospital, Fukuoka, Japan), coorinatimg investigator of Luminor’s trial in Japan (SOL-Japan trial), states in a press release: “We have been eagerly awaiting the availability of this product in Japan. The excellent navigation capabilities of the Oceanus platform and the strong clinical results of Luminor in the SOL- Japan trial (99.2% fTLR [freedom from target lesion revascularisation] at one year), make it a highly promising solution for our patients.”
R3 Vascular recently announced that the first patient in its ELITE-BTK pivotal trial has been treated by Brian DeRubertis (New York-Presbyterian and Weill Cornell Medicine, New York, USA). The trial evaluates R3 Vascular’s next-generation drug-eluting bioresorbable scaffold, Magnitude, for below-the-knee (BTK) peripheral arterial disease (PAD).
“The treatment of the first patient in our ELITE-BTK pivotal trial by distinguished vascular surgeon and researcher Dr Brian DeRubertis is a significant milestone as we commence our effort to fully demonstrate the efficacy and safety of our next-generation Magnitude scaffold,” said Christopher M Owens, president and chief executive officer of R3 Vascular. “Moving forward we look to accelerate enrolment, paving the way for a PMA [premarket approval] market application with the FDA [US Food and Drug Administration].”
DeRubertis commented on the importance of the ELITE-BTK pivotal trial, saying: “I am honoured to have enrolled the first two patients in R3 Vascular’s ELITE-BTK pivotal trial, primarily because this type of technology has been needed by our patients for years. I have spent much of my career researching novel devices for vascular disease, including bioresorbable scaffolds, and while there have been some recent successes in the BTK PAD trial landscape, there remain significant unmet needs in this area. We expect the results of this important trial will reveal Magnitude’s unique potential to further advance treatment and improve patient outcomes for patients with vascular disease.”
“The start of this trial marks the continuation of our journey in providing a groundbreaking technology for patients who have suffered from this debilitating disease for many years without effective therapeutic options,” said Kamal Ramzipoor, founder and chief technology officer of R3 Vascular. “Magnitude is a next-generation bioresorbable scaffold with the potential to address one of the greatest needs for patients suffering from chronic limb-threatening ischaemia due to below-the-knee PAD. R3 Vascular’s novel bioresorbable scaffolds are made from a unique, ultra-high molecular weight polylactic acid polymer. This polymer, combined with the company’s scaffold design and proprietary processing technology allow for superior biomechanical properties with strength and ductility. We believe these properties will drive extremely positive outcomes, especially long-term for real-world patients. We look forward to advancing our product through its clinical development with the ultimate goal of having a market-leading position.”
Vivasure Medical has announced European CE mark approval of the PerQseal Elite vascular closure system, a sutureless and fully bioresorbable large-bore vessel closure device. The company plans to launch the product in select European markets this summer.
Leveraging Vivasure’s PerQseal technology, the PerQseal Elite vascular closure system is designed exclusively for sutureless and fully absorbable large-bore closure following percutaneous cardiovascular procedures such as transcatheter aortic valve implantation (TAVI) and endovascular aortic repair (EVAR). Currently, there are no fully bioresorbable devices available for closure following large-bore procedures. Moreover, unlike other current devices, PerQseal Elite does not require any pre-procedure step, further simplifying the procedure.
“Vascular closure remains a challenge for the growing cardiovascular procedures that require large bore access. The introduction of PerQseal Elite is an exciting advancement for large-bore cardiovascular procedures,” said Mohamed Abdel-Wahab, professor of interventional cardiology and head of Structural Heart Disease Department at the Heart Center in Leipzig, Germany. “Having a fully absorbable, sutureless closure option simplifies the procedure and has the potential to reduce complications associated with traditional closure methods. We look forward to utilising this technology to treat our patients.”
“Securing CE Mark approval for PerQseal Elite marks a major milestone for Vivasure and for patients undergoing complex structural heart procedures,” said Andrew Glass, CEO of Vivasure Medical. “PerQseal Elite represents a significant advancement in procedural efficiency and patient care. We’re proud to bring this innovative technology to clinicians across Europe.”
The PerQseal Elite vascular closure system is placed from inside the vessel, making deployment simpler and more controlled than conventional closure techniques and returning the vessel to its natural state without leaving materials like collagen, metal implants or sutures behind.
Maedeh Rouzbahani (Tehran University of Medical Sciences, Tehran, Iran) spotlights current innovations in stem cell therapy in interventional radiology (IR) and its potential within precision medicine.
Stem cell therapy has emerged as a transformative approach in IR, focusing on targeted treatments for various organ systems and ischaemic conditions. This innovative technique’s integration in IR stems from its ability to precisely deliver therapeutic cells directly to affected tissues, enhancing efficacy while minimising systemic side effects. We named this area of science “Intervencell”.
One of the primary advantages of IR in stem cell therapy is its precision. Intra-arterial delivery is a preferred method and ensures higher retention of stem cells at the target site compared to traditional intravenous methods. Studies in ischaemic heart disease and brain stroke have demonstrated superior outcomes when intra-arterial delivery is employed, such as improved cell engraftment and tissue repair.
This precision is particularly significant in treating conditions like chronic kidney disease, liver fibrosis, diabetes, and osteonecrosis of the femoral head, where localised treatment is critical for successful outcomes. The results of intra-arterial stem cell therapy in clinical settings are notable. In kidney disease, mesenchymal stem cell (MSC)- derived extracellular vesicles have shown the ability to enhance renal function by reducing inflammation and promoting tissue regeneration. Similarly, in liver disease, stem cell injections have reduced fibrosis and improved metabolic control. For neurodegenerative diseases like Parkinson’s, intra-arterial delivery has resulted in enhanced motor function and improved quality of life, highlighting its therapeutic potential.
Despite its promise, this approach is not without challenges. Technical limitations, such as the effects of shear stress during catheter-based delivery, can compromise cell viability. Additionally, exposure to contrast agents and radiation during imaging may negatively impact stem cell integrity. Strategies like reducing infusion rates and minimising radiation are essential to mitigate these issues. Furthermore, the inherent risks associated with stem cell therapy— such as tumour formation in pluripotent stem cells and immune reactions in allogenic transplants—remain key concerns. Ethical considerations also arise, particularly with embryonic stem cells. However, advancements in cell engineering, such as induced pluripotent stem cells (iPSCs), offer solutions by providing patient-specific therapies with reduced ethical and immunological challenges.
Stem cell therapy facilitated by IR represents a cutting-edge approach to precision medicine. While limitations persist, continuous refinement of delivery methods and safety protocols will pave the way for broader clinical application, ultimately improving outcomes for complex diseases and advancing the field of regenerative medicine. This work would not have been possible without the invaluable guidance and support of my mentor Hossein Ghanaati, whose insights and expertise have been instrumental in shaping my understanding of this field.
Maedeh Rouzbahani is an medical doctor at the Tehran University of Medical Sciences, Tehran, Iran.
Disclosures: The author declared no relevant disclosures.
In an interview with Interventional News, John Kaufman—Frederick S Keller chair of interventional radiology at Oregon Health and Science University, in Oregon, USA, president-elect of the American Board of Radiology (ABR) board of governors, and chief medical officer for Cook Medical—looked back to see ahead, addressing what is next for device development in the interventional arena.
IN: Earlier this year you gave a talk at the Society of Interventional Oncology (SIO) 25 Years Past and Future session during this year’s meeting (30 January–3 February, Las Vegas, USA)— what were your main points of discussion?
The topic that was assigned to me was the kind of overview subject matter you receive when you reach the later period of your career. My talk focused on how we in interventional oncology (IO) evolved from very focused, limited interventions—either the early transvascular, which was all embolization and initially just ischaemic to kill the tumour, then to the delivery of therapies and the evolution of said therapies. That has been one trend that continues to grow, particularly concerning transvascular intervention in the liver and kidney.
I also spoke on ablation becoming much more mainstream than it was 25 years ago. Although there was ablation back then, a lot of it was ill-directed alcohol ablation. Today, ablation technologies have taken off and expanded to new approaches such as the delivery of energy to tumours. What I think will be interesting, is the development of ablation to target malignant disease states that we haven’t had a significant role in, such as pancreatic and lung cancer.
One of the nice things about IO is that the multidisciplinary approach will continue to be important as our interventions are never in isolation. We can use a combined approach with other modalities, immunologic modalities, and oncologic radiotherapy, to expand in a more synergistic direction, so that’s going to be really important.
On the device front, I’m very interested in devices that do more than just deliver treatment. Devices that can help to monitor or share information, can tell you the flow, or give you viability information. It sounds crazy, but a device that can tell you about the local genetic environment it’s sitting in, such as whether you’ve got tumours that are changing — devices that have functionality in addition to delivering therapy, I believe that’s the direction we’re going in.
IN: Artificial intelligence (AI) is playing a larger role in medical device development and function—do you think AI will be integrated with IO?
In oncology, AI may support screening—figuring out which patients appear to be on a trajectory that is approaching a threshold for treatment. With AI as a background system that can collect data on lung nodules, for example, you can compare data from the entire programme. Radiomics is very important for cancer and the digital information management that AI can provide is crucial at pre- or post-treatment to understand what we’re doing and what results we’re getting. In the visualisation world AI is going to be huge. I think we’re only just getting to the most interesting part of IO, particularly in the image-guided oncology space.
In terms of clinical information processing, in the end we need to realise that programmes like ChatGPT are an echo chamber—it’s just what’s available in the world and all you’re going to get back is information based on what is already accessible. We will always have a level of scepticism, and you have to be a little bit critical.
IN: Do you see 3D-printed medical devices playing a role outside of prototype creation in the future?
Outside of prototypes, 3D printing medical devices is a sort of magical concept that says—I’m going to place a stent, here’s the computed tomography (CT) scan, it goes to your printer and out pops the stent tailored to that patient. That’s the holy grail, but the regulatory pathway for that would be unbelievable—impossible, although it has happened in the aortic space through custom-made devices. The process is becoming more mechanised with inputs from the imaging actually felt throughout the device manufacturing process.
But, will you end up being able to print patient-specific devices on the fly? Where a patient is on the table and you say ‘I need this stent—print if for me!’, That would be awesome, but I’m not sure we’ll get there. In terms of managing inventory, 3D-printed devices would be incredible, but maintaining and certifying them is unlikely.
“I believe smart devices that give us feedback, pain scores and procedural follow-up are going to change people’s lives immensely”
IN: How often have you seen new devices be applied to treat disease states that have long been managed medically rather than cured?
Portal vein reconstruction is a great example of this. Tumour invasion or adhesion to the portal vein is a disease state that has been sitting in front of us forever. We have been able to image and diagnose the problem, but it is what it is, you just have to live with it, and we manage the complications. Then taking tools from peripheral intervention, taking knowledge from liver access that we use in the biliary area, and portal vein embolization, taking knowledge of access and recanalisation, we’ve been able to open up veins no one ever thought could be opened. There’s a tremendous amount of interest because there are many patients with this issue.
Now it’s one of these situations in which you have nothing to offer— you’re not looking for a solution so you’re not paying attention to how often you’re seeing it. When you suddenly have the ability to treat something, you see patients with this all the time.
Another area where I have seen this development is pulmonary embolism (PE). Fifteen years ago, how often were interventional radiology (IR), cardiology and vascular surgery involved in PE? Almost never. The patient was managed medically. Yet now, with the thrombectomy tools at our disposal, we treat patients with PE up to three or four times a week. This is something IR does a lot, where you are always taking tools and skill sets and looking for new applications, which I believe will also play out in the IO world.
IN: US President Trump revealed plans to impose tariffs on imported goods which will affect a significant proportion of available medical devices that are manufactured outside of the USA. What are your thoughts on this?
There is a lot of concern, certainly for any of the international corporations, not over what’s going to come in but what’s going to happen to devices going out. I am concerned that the proposed tariff will drive up the already excessive cost of healthcare. Many companies have moved device manufacturing overseas or across borders, and if this suddenly becomes a much more expensive proposition, it ends up trickling down to the price of available medical devices. It remains to be seen how real this will be.
IN: What has been the most significant area of device development in the last five years, and in the next five, what development will be the most influential?
For me, the biggest change has been within PE intervention. We now have very good devices for dealing with large embolisms, and these devices have been pivoted to in endovascular IR, vascular IR and elsewhere. In the next five years, I believe smart devices that give us feedback, pain scores and procedural follow-up are going to change people’s lives immensely.
Terumo Neuro has announced that its carotid stent system has received premarket approval (PMA) from the US Food and Drug Administration (FDA).
This milestone marks the first dual-layer micromesh carotid stent approved in the USA, offering physicians a clinically proven option to improve patient outcomes in carotid artery disease treatment, as per a Terumo Neuro press release.
The company’s carotid stent system is indicated for the treatment of carotid artery stenosis in patients at increased risk for adverse events following a carotid endarterectomy procedure.
The device is intended to treat patients with de novo atherosclerotic or post-endarterectomy restenotic lesions in the internal carotid arteries, or at the carotid bifurcation, with ≥50% stenosis in symptomatic patients or ≥80% stenosis in asymptomatic patients—as determined by angiography.
According to Terumo Neuro’s recent release, the device also accommodates vessel reference diameters between 3.5mm and 9mm at the target lesion.
Cagent Vascular has announced its first patient enrolment of the Serranator versus plain balloon angioplasty optical coherence tomography (OCT) study.
This prospective, randomised (2:1 treatment to control) dual-centre study will enrol up to 60 patients. The study will utilise intravascular OCT imaging to demonstrate the mechanism of action (MOA) of the Serranator and compare the serration MOA to conventional angioplasty across a wide range of lesion morphologies in below-the-knee arteries.
The study will be taking place at Columbia University Medical Center and Weill Cornell Medicine led by co-principal investigators Sahil Parikh and Brian DeRubertis. A press release reports that this will be the first study of its kind, a randomised trial utilising OCT imaging to compare acute outcomes between serration angioplasty and plain balloon angioplasty. Cardiovascular Research Foundation in New York, USA will serve as the Core Lab for the study.
“Past data has suggested that serration angioplasty may provide greater lumen gain versus conventional plain balloon angioplasty; however, no study to date has used OCT analysis to definitively show how the serrations remodel lesions of various morphological characteristics,” said Parikh. “The information we gather in this study will be valuable in emphasising guidance on what clinical presentations may be most appropriate for intervention with serration technology.”
“OCT provides a novel visualisation of vascular disease and therapeutic results. With 10x the resolution of IVUS [intravascular ultrasound], we believe this study will allow us to understand how serration angioplasty and plain balloon angioplasty interact with the intima, internal elastic lamina, and media. We’re eager to assess this visually and quantitatively in this first-of-its-kind study,” stated DeRubertis.
What computational advancements are set to transform interventional radiology (IR)? Interventional radiologist, Judy Wawira Gichoya (Emory University, Atlanta, USA) weighs in, providing a realistic outlook on developments so far.
The enthusiasm of interventional radiologists for new devices that have enhanced our clinical work reveals a notable gap when considering artificial intelligence (AI) as a significant component of our toolkit. During the 2024 Western Angiographic Society meeting (21–26 September, Kauai, USA), I surveyed hundreds of practicing interventional radiologists regarding their current or planned use of robotic technology. The prevailing sentiment can be summarised in one word: indifference. In my reflection during the ‘25 years of Computational Advances’ session at the 2025 Society of Interventional Oncology (SIO) annual scientific meeting (30 January–3 February, Las Vegas, USA), I contended that action should be the focus for every interventional radiologist moving forward.
Most AI tools available today are primarily designed for diagnostic radiology and are used by interventional radiologists incidentally. Some of us who participate in pulmonary embolism response teams (PERTs) have indirectly interacted with the triage algorithms that detect incidental pulmonary embolism. Conference exhibitions often mention AI to inform us about the latest advancements, but these systems are not commonly used in our daily work. In fact, after one year of using a percutaneous biopsy robot at Emory University’s IR department, in Atlanta, USA, the robotics company went bankrupt, and our practice has continued without “the robot”. Our residents are happier with their education without the robot.
While IR continues to be a lesser-known branch of radiology, primary care clinics and electronic medical record systems are advancing with AI integration. One such application is ambient listening, where AI transcribes and writes clinical notes, which has become essential for primary care providers in hospitals. The dream of every interventional radiologist who wants to have a working clinic is being achieved outside radiology supported through AI-generated drafts to patient messages, AI-assisted discharge summaries and differential diagnosis, and even end-to-end AI-assisted radiology interpretation. Yet, new data reflect the reality of IR—data showing the impact of workplace injuries from many years of wearing lead in rooms not designed for ergonomic flexibility, lack of evidence to show the value of IR in multidisciplinary care, continued workforce shortage and persistent IR deserts where tele-procedural interventions remain a dream.
The call to action begins with understanding the advancements of AI architectures with increased development of foundation models. These models are trained by compressing data like text, videos and pictures into a representation space and then generating content in response to a prompt. The self-supervised nature of learning, which can be thought of as ‘fill in the blanks’, allows for training of these models with minimal human input. Several models have been developed for radiology, and the same technology developed for IR would overcome prior limits of small datasets for AI development, capture multimodal data, and reduce annotation cost and effort. This model base, if properly designed, could then be used to power agents that can participate in tumour board discussions, assist with clinic and procedural documentation, provide infrastructure to develop digital twins for patient trajectory mapping and robot environment simulation.
In 2024, I teamed with authors for a two-part series article on AI for IR.1,2 The articles introduce a patient case for PE thrombectomy that is automatically flagged from the overnight list by an AI triage system. It subsequently touches on all possible points of digital transformation including patient consent and chatbot interaction, multisensory monitoring for physiologic and pain status, 3D printing of a personalised angiographic catheter, AI-generated orders and procedural documentation
While futuristic, I believe that the technological advances are getting there but need the input of the interventional radiologist to not continue to develop monolithic applications in isolation, but envision an enabled future that allows us to provide excellent care to all patients.
References
Warren, B.E., Bilbily, A., Gichoya, J.W, et al. An Introductory Guide to Artificial Intelligence in Interventional Radiology: Part 1 Foundational Knowledge. Canadian Association of Radiologists Journal, 75(3), pp.558–567. doi: https://doi. org/10.1177/08465371241236376.
Warren, B.E., Bilbily, A., Gichoya, J.W, et al. An Introductory Guide to Artificial Intelligence in Interventional Radiology: Part 2: Implementation Considerations and Harms. Canadian Association of Radiologists Journal, 75(3), pp.568–574. doi: https:// doi.org/10.1177/08465371241236377.
Judy Wawira Gichoya is an associate professor of interventional radiology and informatics at Emory University,
Disclosures: The author declared no relevant disclosures.
The study was performed at three leading medical centres in the USA: Memorial Sloan Kettering Cancer Center (New York, USA), Baptist Hospital of Miami (Miami, USA) and Brigham and Women’s Hospital (Boston, USA). The late-breaking podium presentation was given by Francois Cornelis of Memorial Sloan Kettering Cancer Center.
The data concluded that robotic endovascular procedures using Microbot Medical’s Liberty endovascular robotic system are feasible and significantly minimise radiation exposure.
Highlights of the ACCESS-PVI study
Successful robotic navigation was achieved in every case (n=20), yielding a success rate of 100%, meeting the primary endpoint of the study.
No adverse device events (ADE=0%) were reported through the duration of follow-up.
Mean difference in radiation exposure between operator and control was (-)29.8µS, resulting in a mean 92% relative reduction in radiation exposure.
Median robotic navigation time to target was three minutes.
Participating physicians reported Liberty performed as planned with a 100% satisfaction rate.
“The ACCESS-PVI data and the performance of the system throughout the study reflect the hard work that the team has put into Liberty over the past few years,” commented Harel Gadot, chairman, chief executive officer and president of Microbot Medical. “We are extremely pleased with the results in all aspects. As we shift focus to building our commercial capabilities and preparing for launch, we are confident that Liberty will be well received in the market.”
“We are very satisfied with the clinical data, as well as with the investigators’ feedback in terms of the short learning curve and intuitive operation of the device,” commented Juan Diaz-Cartelle, the company’s chief medical officer. “We are looking forward to working with interventional physicians and staff upon FDA’s [US Food and Drug Administration] clearance.”
Microbot Medical advises that Liberty is an investigational device pending FDA 510(k) clearance, and is currently not available for sale in the USA.
Resorbable microspheres are making waves in musculoskeletal (MSK) embolization, challenging the use of permanent embolics. As clinical evidence supporting their safety and efficacy accelerates, these agents could reshape treatment strategies— offering effective pain relief while reducing long-term risks. In an interview with Interventional News, Ziv Haskal (University of Virginia, Charlottesville, USA) gives pragmatic shape to the emerging future of resorbable microspheres in MSK embolization.
IN: Why are resorbable microspheres in the spotlight, particularly for MSK embolization?
We’ve danced around resorbable embolics for decades, mostly for hepatocellular carcinoma and fibroid embolization—and trauma of course. Thus far, there have been no proven therapeutic advantages for resorbables over permanent embolics for tumours, be they benign or malignant. But that does not mean that this paradigm cannot shift. Consider Kichang Han (Yonsei University College of Medicine, Seoul, South Korea) et al’s September 2024 publication titled ‘Resorbable microspheres versus trisacryl gelatin microspheres for uterine artery embolization’ which showed equivalent outcomes. Wouldn’t any woman considering uterine artery embolization (UAE) now lean toward a resorbable agent?
Until this decade, we’ve had a dearth of calibrated resorbable microspheres with task-specific dissolution characteristics, because of both technical innovation and clear opportunity. MSK embolization has remade that landscape. I remind readers how controversial Yuji Okuno’s (Okuno Clinic, Tokyo, Japan) groundbreaking early papers were. As the two-term Journal of Interventional Radiology (JVIR) editor, I discussed his 2013 seven patient imipenem/ cilastatin genicular artery embolization (GAE) paper with nine reviewers and editors, and all insisted the paper was preposterous and should be rejected: an antibiotic injected intra-arterially? Used as an embolic? For treating arthritis? I published it anyway because it was a well done range-finding study—and the scientific literature is a place for controversy and discussion. It’s already been cited 100 times.
Fast forward to now and the literature has been steadily accumulating, mostly in clear support of MSK embolization of the neovessels that develop in inflammatory conditions, be they osteoarthritis (OA), epicondylitis, frozen shoulder or other enthesopathies and tendinopathies—all intended to provide meaningful control of pain. My own partly torn rotator cuff was overlaid by painful adhesive capsulitis that cost me eight months of rehab and recovery; I might have had a different outcome had I lived in Japan and seen Okuno.
Imipenem/cilastatin is essentially a rapidly dissolving crystal—a short-term mechanical embolic. Amazingly, the clinical effects of MSK embolization are lasting six months to a year—using these rapidly disappearing agents, suggesting that the treated neovessels might remain embolized, beyond the recanalisation of normal vessels, but it’s still an area for deep inquiry. Over-embolization can lead to skin and muscle changes and injury, wounds, and prolonged pain. Beyond proof of concept, imipenem is a therapeutic dead end. There will never be an on-label indication, pursued by a pharmaceutical company, for an antibiotic to be approved as an intra-arterial embolic agent. Forget about it. So, we are in the post-imipenem panorama, where a number of resorbable agents are planned for MSK embolization evaluations. There are a lot of skunkworks on this.
IN: Are you in favour of a ‘leave nothing behind’ approach for embolics?
The European Union has at least one widely available rapidly resorbable CE-marked microsphere (Nexsphere F)—I expect others to arrive shortly. US physicians are lagging; we are still limited to permanent embolics. Therapeutic improvement with MSK embolization is certainly achieved with permanent embolics. But the margins of safety surrounding efficacy are much narrower with permanent embolics. When this procedure spreads in ‘the wild’, e.g., is performed widely, then adverse events will definitely increase with permanent embolics only. Okuno has even identified safety differences between three different temporary agents that he’s used.
Thus, we have to maximise safety— excessive embolization will cause skin and nerve injury, pain, and worse. The blowback could stop this in its tracks—pounced upon, “Aha!” by sceptical other specialties and reluctant insurers. Medicine is tribal, and competing therapies are always under unique scrutiny. Even though I’m a sceptical clinical trialist by nature, I’m a believer in this, so we have to proceed methodically and protect our patients and outcomes, because we have millions of patients suffering with painful presurgical OA, joint and tendon pains and injuries—areas where we might provide a meaningful alternative to failing oral or injection therapies.
“Even though I’m a sceptical clinical trialist by nature, I’m a believer in this, so we have to proceed methodically and protect our patients and outcomes, because we have millions of patients suffering with painful presurgical OA”
IN: A change in technological approach often requires refinement in technique. Is this likely true of embolics in MSK interventions?
Safety, safety, safety—repeat the mantra like a scratched vinyl record. In areas of competitive interventions across multiple specialties, it’s paramount. Endless interventional radiology (IR) examples exist. Consider prostatic artery embolization (PAE)—a procedure designed by interventional radiologists, sought by men, performed in a space owned by urologists. I have been performing PAE continuously for more than 10 years, starting out under our investigator-sponsored investigational device exemption (IDE). Even now, I hear some urologists still describing the procedure as dangerous and investigatory and some US insurers deny it in nearly every case. When you are innovating in your own specialty space, the parameters are different than when you’re under the suspicious watch of others. So, this means primum non nocere—first, do no harm—and proventus scientificus immaculatus esse debet—the scientific results must be immaculate. Hence fast-dissolving resorbables.
IN: Regarding ‘first, do no harm’—does resorbability need to prove repeatability?
Prospective trials are being conducted and are imminent worldwide. There are commercial US trials evaluating permanent embolics for GAE. There are pending commercial trials for resorbable agents—some in ‘quiet mode’—or seeking federal funding. The Nexsphere-F RESORB multicentre IDE trial has been approved by the US Food and Drug Administration (FDA) and will be enrolling patients shortly.
The embolic is a rapidly dissolving gelfoam microsphere that mechanically dissociates at a rate mimicking imipenem/cilastatin by design. It has been included in trials in South Korea and several multicentre trials set to launch in Europe, as well as a UK National Health Service (NHS) trial. It’s also being used in shoulders and elbows. I expect similar trials with other resorbables and liquids. This multi-front approach is critical—to fully evaluate and protect this field we need a variety and multitude of replicative trials and populations.
IN: There are several resorbable embolics being examined in trial settings so far. What do you think needs to happen to differentiate between their safety and effectiveness?
I hope we’ll see strong positive results from multiple resorbable agents. It’s a moving target, as we are also working out the techniques of MSK embolization. How much to embolize, how many vessels, and what are the patient and angiographic-specific embolization endpoints that result in valuable symptom improvement, while avoiding injury. To provide meaningful pain relief in the knee, we might have to treat more vessels than originally thought. There is plenty of opinion, discourse, and argument. What qualifies as an angiographic ‘blush’ warranting treatment? How much do you embolize those vessels—as embolization short of injury is paramount and agent-specific endpoints will vary, as will angiographic embolization endpoints? It’s a recipe for a dog’s breakfast.
IN: Where is standardisation of technique in this landscape? Is GAE a standardised technique?
We published a Society of Interventional Radiology (SIR) Research Reporting Standard for GAE and specifically dodged that question; it’s simply too early to answer. We’ll gradually build that answer upon the empirical results of as many resorbable trials as we can get.
Recently presented at the Society of Interventional Radiology (SIR) annual scientific meeting (29 March–2 April, Nashville, USA), data from the Jet Enhanced Thrombectomy intervention Hydrodynamic Thrombectomy System (JETi; Abbott) registry has demonstrated the device’s effectiveness having surpassed prespecified safety and efficacy thresholds for the removal of thrombus in lower extremity deep vein thrombosis (DVT).
The JETi system is a hydromechanical aspiration system intended to remove intravascular thrombus. To evaluate its efficacy, the prospective, single-arm, all-comer, real-world venous registry was devised, enrolling 116 patients will iliofemoral DVT from 14 global sites.
Primary effectiveness was assessed by the percent of treated vessel(s) with ≥75% venous thrombus reduction from baseline to final venogram following all primary and adjunctive therapies per core lab-assessed modified Marder score. Safety was assessed by the composite rate of JETi-related major adverse events that included death, symptomatic pulmonary embolism (PE), major bleeding, and re-thrombosis of JETi-treated vessel(s) up to 30 days post procedure per clinical events committee adjudication.
Patients in this cohort had a mean age of 56.6 years, and half were female. Prior rates of DVT (21.6%) and PE (19.8%) were high in this patient population, with significant rates of other conditions such as hyperlipidaemia, diabetes and hypertension. Nearly three quarters of the population (74.1%) had onset of signs and symptoms ≤14 days, 16.4% were >14 days but ≤42 days, and the remaining (9.5%) >42 days.
The total index procedure time was reported as 124.5 minutes, while the JETi device use time was 23.5 minutes; 72.4% of patients were treated in a single session with the device. Concerning adjunctive treatments or additional interventions, 83.6% required a balloon and 55.2% a stent. Two patients required the use of the JETi HyperPulse (Abbott) thrombolytic; 13.8% of patients requiring a hand-infused thrombolytic. Catheter-directed thrombolysis was performed in 25.9% of patients—4.3% prior to JETi use and 21.6% following.
Regarding primary effectiveness, at least 75% thrombus reduction was achieved in 84.5% of treated limbs via modified Marder score, which met the prespecified performance goal of 64%. Major adverse events were reported in 1.7% of patients, including symptomatic PE and rethrombosis of JETi-treated vessels.
Patients reported improved Villalta post-thrombotic syndrome (PTS), leg pain, and quality of life scores at 30 days post procedure. Importantly, despite disclosing moderate to extremely severe pain at baseline, 81% of patients reported that they had no pain to mild pain at follow-up.
Meeting its prespecified effectiveness and safety criteria, the trial investigators highlight the marked improvement in clinical and patient-reported outcomes, and state that the registry’s one-year results which are set to be released in due course will bear out these data in greater granularity.
Twelve-month results from the WRAPSODY Arteriovenous Access Efficacy (WAVE) pivotal trial show a statistically significant improvement in target lesion primary patency (TLPP) with the Wrapsody (Merit Medical) cell-impermeable endoprosthesis (CIE) when compared to percutaneous transluminal angioplasty (PTA).
The prospective, multicentre, international WAVE trial, conducted across 43 centres in the USA, South America and the UK, includes patients with arteriovenous fistula (AVF) with venous outflow stenosis or occlusion in their peripheral venous outflow circuit.
These results were presented by Dheeraj Rajan (University of Toronto, Toronto, Canada) at the Society of Interventional Radiology (SIR) annual scientific meeting (29 March–2 April, Nashville, USA). Rajan detailed that treatment efficacy was determined by the proportion of patients with TLPP, defined as freedom from clinically driven target lesion revascularisation or target lesion thrombosis. A key secondary endpoint at 12 months was access circuit primary patency (ACPP).
A total of 245 patients were randomised, 122 to treatment with Wrapsody and 123 to PTA. Rajan reported that no statistically significant difference in the proportion of patients free from a safety event was observed through to 30 days post procedure (Wrapsody CIE: 96.6%; PTA: 95%; non-inferiority p<0.001). At six months, the TLPP was higher for patients treated with Wrapsody versus PTA (89.8% vs. 63%; p<0.0001) and remained higher than the PTA cohort at 12 months (70.1% vs. 41.6%, p<0.0001). The six-month ACPP was higher for patients treated with Wrapsody versus PTA (72.8% vs. 58%, p=0.014) and remained higher at 12 months (58.1% vs. 34.4%, p=0.0003).
“Looking at our 12-month primary patency, you can see the survival benefit is maintained and actually separates over time,” said Rajan, reflecting on their results. “As the curves continue to separate, I argue that there’s a continued therapeutic benefit [with Wrapsody] over time, and for access circuit primary patency as well.”
Rajan added: “Within dialysis access, those of us that do it, we know that the outcomes of vascular access directly contribute to the mortality and morbidity of patients. There’s a really high cost to maintaining these accesses, and to date, all comparative studies still consider PTA as the gold standard for treatment.
“Although PTA has done reasonably well [in trial settings], there has always been room for improvement, and we’ve chased that [via the WAVE trial],” Rajan told the SIR audience. “We’ve seen improved TLPP with covered stents in the past, but the access circuit primary patency doesn’t change much. The argument has always been why would you use these devices if you aren’t changing the overall lifespan of the access,” said the speaker.
The WAVE trial is currently ongoing and 24-month results are forthcoming, announced Rajan. In light of the sustained improvement in TLPP and ACPP with Wrapsody, and the “limited options available to restore and maintain access circuit primary patency”, the authors state that these findings are of “high value” to clinicians who treat stenosis/occlusion in the venous outflow circuit of haemodialysis patients, and for the patients themselves.
Editor-in-chief Brian Stainken, author of this letter
How can it be that this specialty society, so associated with concepts of ‘newness’, is old?
We know that in 1974 a group of ‘gadgeteers’ (credit to Mike Dake for the term), dressed in plaid bellbottoms, convened in Key Largo in Florida, USA to talk geek. They munched on that year’s new snack called Skittles, and organised their thoughts and schedules with the new-fangled sticky, but not so sticky, Post-it notes.
Fast forward five decades and we have the newest American board-certified discipline, the most competitive primary residency, a thriving pipeline of discovery, robust global collaboration, and many imitators. We do still have the candy and the note pads, but they have not really changed.
So, how did this remarkable transformation happen? Why, of all the millions of good ideas from 1974 did this one not only survive, but thrive? I don’t know, but here’s my best guess.
A good idea
‘Virtual reality’ guidance obviated any need for dissection and exposure. More precise, less risk. Without image guidance we are surgeons. With it, we are superheroes able to access any structure, anywhere. Shazam! Most medical historians place medical imaging high on the list of greatest medical discoveries of the last century—Sven Ivar Seldinger was in the right place at the right time and interventional radiology (IR) as we know it now is a beneficiary.
Visionaries
The Mount Rushmore of IR should show Charles Dotter of course, probably in the centre. Nearby would be, well, a lot of folks, frankly too many to mention. If the idea that we could in fact take the Fantastic Voyage— the 1966 sci-fi thriller where a submarine is miniaturised and injected into a scientist suffering from a clot, was crazy, imagine dreaming up a system for reimbursement from scratch, or inventing the concept of societal quality guidelines. Imagine saying to an incredulous medical establishment that someday we would be delivering intra-arterial drugs or percutaneously draining abscesses or convening a task force to build a primary specialty and succeeding! The visionaries of the Society of Interventional Radiology (SIR) all deserve to be on that mountain. IR seems to attract a certain type of inventive zealot. We are fortunate for that.
Culture
I think this is where SIR’s light shines brightest. From its earliest days, this society and its meeting was a home for big (outrageous) thinkers, inclusive, open, and representative. We’ve pursued some boneheaded ideas along the way to be sure, and paid for some, but what distinguishes us is our willingness to engage. As our society and specialty mature, the price for taking risks grows, but our future depends upon our ongoing willingness to listen to new ideas.
Teamwork
We are a society of volunteers. It’s extraordinary that in 2023, nearly 10% were active volunteers, and many more were active at the hospital, and local levels. It is also a recipe for operational chaos. That’s where the SIR staff over the years have evolved into essential partners. They mirror the membership. They too believe in the promise of IR. Without the support and guidance of the many association professionals we’ve teamed with, we would be nowhere. Thank you.
Of course, with any big anniversary one begins to look forward. From the perspective of a past SIR leader, here is what I hope the next 50 years bring:
Introspection
There are some things we do in IR that are not sufficiently complex or risky to justify our very expensive time. To stay competitive, our time spent supervising and developing protocols and practice standards should be maintained, but we must advocate for the best care, by the most appropriate trained and supervised providers, both in terms of outcomes and cost. That said, we also must pay more attention to the central operational role we play in nearly every hospital in the country. What percentage of inpatients are touched by IR? What percentage of discharges expedited, complications averted? What savings are attributable to our presence? Core IR merits more attention, tighter definition, better practice models factoring in clinical time, more research, and better economic validation.
Accreditation
The society reflects the field, and its growing diversity. In order to serve membership, the structure of the society must continue to evolve. Pending the future adoption by the American Board of Radiology (ABR), we should follow or join in the Cardiovascular and Interventional Radiological Society of Europe (CIRSE)’s example and embrace voluntary society-based accreditation for subspecialised practice areas. Such a scheme should include clinical practice mandates and span the full scope of the specialty.
Full time IR
With the number of trainees and full members approximately equal—as per the 2003 SIR annual report—a primary residency, clinical practice requirements, and evolving specialty focus areas, I expect that market forces will drive this shift, where the potential exists and individuals are willing to take risks. No need for an edict. That said, in a world where no hospital can function without IR, some geographies will always require part-time providers as long as they have the need for clinical time.
Leave radiology? Keep the ‘R’, drop the ‘D’. Whether you can evolve into a new department or service line, or should stay as you are is a local issue based on strength, level of leadership support and finances. If you are strong enough to stand alone, fine. However, it’s unlikely that leaving alone will somehow make you stronger. As our specialty evolves toward a collection of subspecialised focus areas, and as we mandate clinical practice, we should grow stronger, and fit and be valued in several departments. It’s good to have many friends.
Global IR
IR is a small specialty until you look at it from a global perspective. Collaboration, adherence to standards, and excellence in research, training and practice are our unifying themes. I believe that our growth and continued evolution opportunities for the next 50 years will come through increasing our efforts to effectively network and share our successes and strategies. We are all in this together.
In a subgroup analysis of the STRIKE-PE study regarding patients treated with the latest iteration of Penumbra’s 16Fr Lighting Flash computer-assisted vacuum thrombectomy (CAVT) device, Brian J Schiro (Miami Cardiac & Vascular Institute, Miami, USA) reported improved haemodynamic markers, right/left ventricle (RV/LV) ratio, dyspnoea, and overall, a “highly” improved device use time of 25.5 minutes.
In the outset of Schiro’s presentation at the Society of Interventional Radiology (SIR) annual scientific meeting (29 March–2 April, Nashville, USA), he described that the goals of pulmonary embolism (PE) treatment are haemodynamic stability, perfusion restoration and right heart strain relief, among others. “Functional analysis is also important,” Schiro noted, stating that the consideration of long-term issues in these patients is as important as immediate improvement in symptoms.
Initially, he described the evolution of endovascular treatment of PE, outlining the progression from thrombolytics, to continuous aspiration, and now, CAVT, the “next-generation” treatment modality.
The present analysis of the STRIKE-PE study evaluated periprocedural and functional results of the first 164 acute PE patients enrolled and treated with CAVT using the 16Fr Lightning Flash system. The device comprises an aspiration catheter and a microprocessor programmed to optimise regulation of aspiration by using pressure differential and flow-based algorithms to rapidly detect thrombus from blood flow.
Among their 164 acute PE enrollees, the average patient age was 61.6 years, and 53.7% were male. PE risk stratification was high in 4.9% of patients, intermediate-high in 86.6% and intermediate-low in 8.5%. The median thrombectomy time was 25.5 minutes and median procedure time was 59 minutes. Schiro reported that mean on-table pulmonary artery pressures (PAPs) “significantly decreased”—systolic PAP from 50.8mmHg to 38.8mmHg (23.4%, p<0.001), and mean PAP from 31.2mmHg to 23.5mmHg (24.5%, p<0.001)—demonstrating the device’s effect, providing “quick haemodynamic improvement and stability”.
Mean RV/LV ratio decreased from 1.34 at baseline to 0.94 at 48 hours (27.8%, p<0.001). The speaker noted that one composite major adverse event (0.6%) occurred within 48 hours; however, no device-related serious adverse events were reported. Six patients required pre-discharge transfusion. “Most of these were related to the patient’s underlying conditions”, Schiro stated; however, no major bleeding required transfusion and there were no device-related transfusions. Additionally, median Borg dyspnoea score at rest decreased from 5 (severe [heavy]) at baseline to 0.5 (very, very slight [just noticeable]) at discharge.
“What we really want to highlight here is the procedure time and the time of thrombectomy,” Schiro told SIR delegates. He compared the 16Fr Lightning Flash to devices used in the APEX-AV, FLASH and PEERLESS trials, which had procedure times of 37.2, 43, and 47.5 minutes, respectively.
“The most impressive figure really is that short device time. We achieved exceedingly short procedures compared with some of the other trials that have been reported,” Schiro said. “With the [16Fr Lightning Flash] device, we continue to see significant improvements in the patient’s status, including RV/LV ratio, functional status and an excellent safety profile,” he stated.
A STRIKE-PE interim analysis of clinical outcomes of acute pulmonary embolism (PE) patients with or without syncope—an indicator of compromised cardiac output and so increased short-term mortality—has found that patients with syncope who had a higher right/left ventricle (RV/LV) ratio at baseline were restored to a condition similar to patients without syncope following treatment with the Lightning Flash (Penumbra) computer-assisted vacuum thrombectomy (CAVT) device.
“Syncope is a frequent conundrum,” said John Moriarty (University of California Los Angeles, Los Angeles, USA) during his late-breaking presentation at the Society of Interventional Radiology (SIR) annual scientific meeting (29 March–2 April, Nashville, USA). “Often we are uncertain whether this is a group of patients with acute intermediate risk, or whether they are within a worse group when considering outcomes or at higher risk of [repeated] intervention, so we felt it was important to study this patient cohort,” he stated.
Initially powered to evaluate 600 patients, the STRIKE-PE cohort was extended, subsequently enrolling 1,500 patients. The prospective, international, multicentre study included patients with acute PE symptoms of ≤14 days and an RV/LV ratio of ≥0.9. Patients from this interim analysis with (n=72) versus without (n=228) syncope were compared.
Moriarty highlighted that there was a statistically significant difference in Miller score of those ≥12 (91.7% vs. 80.7%, p=0.03) in the syncope cohort, taking this to demonstrate a large clot burden, which was seen more frequently in patients with syncope than in those without. These patients also presented with a shorter time from symptom onset to venous puncture (47.5 hours vs. 81 hours p=0.04), and a higher RV/LV ratio (1.48 vs. 1.37, p=0.03).
At 48-hour post-procedure follow-up, RV/LV ratio improved in both groups, however improvement was significantly greater for patients with syncope (0.51 vs. 0.37, p=0.004; 31.7% vs. 25.2%, p=0.002). No significant difference was found between the groups for rate of composite major adverse events within this timeframe, nor concerning 30-day mortality.
“In other words, by imaging characteristics, [patients with syncope] got better, although both cohorts did well,” Moriarty told SIR 2025 delegates. “When we look at safety, there are essentially no differences between the patients who had syncope and those who didn’t. Again, this is—we think—going to be clinically important because there has been a theory that patients who present with syncope are at increased risk, whether it’s primary safety or device-related safety outcome during the procedure.”
Both groups had reduced dyspnoea via the Borg scale at rest from baseline to discharge, and no significant differences in dyspnoea were reported between the groups following a six-minute walk test at discharge.
“Syncope is a common problem,” Moriarty described. “We believe that it’s an indicator of compromised cardiac output, and then therefore it portends to people who have a bad outcome due to the severity of their haemodynamic instability or right ventricular outflow tract obstruction, with an increase in RV dysfunction at presentation, an increase in short-term mortality and risk of early PE-related adverse outcomes, making this is a very fertile area of evaluation,” he added.
“So far, we believe that the clinical benefits of CAVT that are shown in this study may be especially valuable for patients who present to this theoretically high-risk cohort,” Moriarty commented. Moving forward, he and his team add that there is need to elucidate clinical markers to further the understanding of patients with acute PE.
Transcending region and socioeconomic status, a global survey has revealed patient awareness to be a “universal obstacle” that faces interventional radiology (IR) worldwide. These data have also highlighted disparities in training, practice, education, and reimbursement. The survey was aimed to describe the current global state of IR education and practice in different geographic locations, identify factors limiting development and propose strategies to address these challenges.
“Understanding the factors underlying such disparities is essential in helping to develop IR as a discipline. Such developments will better serve patients in need while also bringing value to the global healthcare system,” write Justin J Guan (Cleveland Clinic, Cleveland, USA) alongside Constantinos Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA) and co-authors of the survey. According to the World Health Organisation (WHO) in 2021, more than half of the world’s population lacked access to crucial radiology services and even more so departments with interventional capabilities.
Endorsed by the Society of Interventional Radiology (SIR), Guan et al designed an online survey to gather information including respondent demographic information, IR practice characteristics, and respondent opinion on challenges and needs. The survey was distributed among global IR societies and shared on social media platforms, remaining open between June 2022 and September 2023.
Guan and colleagues collected 1,263 responses. Of the 993 respondents who reported speciality affiliation, 811 were interventional radiologists, 85 diagnostic radiologists and 91 identified as both specialties. The majority of respondents were located in Asia, Europe or Africa. Most respondents reported practising in an academic hospital (34.3%), a public hospital (31.8%) or a private hospital (27.9%). The USA was not included in these results, as statistical analyses of US IR practice were used as the basis for comparison.
Over half of the respondents reported having graduated from an accredited radiology training programme, although 24% stated that no structured training programme existed in their country, and 20% indicated that their radiology training offered no exposure to IR. IR teaching responsibilities were least prevalent in Africa (40%) and most prevalent in Europe (83%). Reflecting these disparities, 92% of respondents expressed support for establishing unified global IR training standards.
In terms of IR practice, the most commonly performed procedures worldwide included biopsies, drainages, angiograms, embolization, and venous access procedures. Regionally, biopsies were the most frequently performed procedures in Asia, North America, and Africa, while venous access procedures were most common in South America and Oceania. In Europe, angiograms and embolization were the most widely conducted IR interventions.
The survey also examined reimbursement models, asking repondents to select all that apply, the authors found that national health plans were the primary source of payment for IR procedures globally, covering 66% of cases. Private insurance was the second most common form of reimbursement at 53%, while out-of-pocket payments accounted for 35% and hybrid models 24%. Private insurance was the dominant model in North America, South America, Africa, and Asia, whereas national health plans were the primary source of payment in Europe and Oceania. “Interestingly”, Guan et al write, in Asia, the distribution of payment sources was relatively even, with 54.7% of cases covered by private insurance, 53.7% by national health plans, and 52.4% paid out of pocket.
Several key barriers to the expansion of IR services were identified via the survey, with patient awareness and education emerging as the most critical issue. On a scale of 1 to 3, where higher values indicated greater relevance, patient awareness received a weighted mean score of 2.7 and was cited as the most significant barrier by 72% of respondents. Patient referrals followed closely with a score of 2.6, reported by 65% of respondents. Other significant barriers included limited IR training (2.5, 57%) and reimbursement issues (2.5, 56%). While patient awareness and referrals were the dominant concerns globally, Africa was the only region where IR training was ranked as the highest priority, scoring 2.8, followed by patient awareness at 2.6.
Among practising interventional radiologists, the study highlighted key professional challenges, with patient awareness and hospital support ranking highest. Competition with other specialties was another major concern cited by respondents. These challenges varied by region—in North America, Asia, and Europe, the primary issues were patient awareness and hospital support, while in Africa and Oceania, patient awareness remained a leading concern. In South America, competition with other specialties and reimbursement challenges were ranked as the most significant obstacles.
In their discussion of the survey results, Guan and colleagues underline that not only is awareness about IR low among patients, but “also among referring and primary care physicians, healthcare workers and the public at large”. The authors reference a 2023 Rodgers et al study which published results of a population survey evaluating public awareness of IR in the USA. Of 1,000 respondents, only 40% knew of IR, and less than half described the specialty correctly. “[The USA has] arguably the most developed IR infrastructure in the world”, Guan et al state, casting awareness of IR in other geographies in stark relief.
“Ultimately, there must be global recognition of IR as a medical discipline that offers significant value to the healthcare system,” the authors write. “Global collaboration of IR societies with backing from governments, industry, and other supportive entities is crucial in fostering positive changes and overcoming challenges that hinder the development of IR training worldwide.”
The authors highlight IR’s added value to the healthcare system across numerous specialties and state that the “increasing demand for minimally invasive procedures, coupled with patient-centred care, tailored management plans and the rising incorporation of artificial intelligence and robotics, further enhance IR’s market value”.
Guan and colleagues add that, while North America has the largest IR market share currently, the Asia-Pacific region is projected to have the highest future growth rate, while investment from IR societies, government and industry into regions with less robust IR infrastructure such as Africa and South America is set to improve training and education.
Naming microwave ablation as the “workhorse” of all ablation procedures performed by he and his team, Govindarajan Narayananan (Miami, USA) details his current practice and his early impressions using the IntelliBlate (Varian) solution.
For interventionalists who have been performing microwave ablation since its inception, they will know that reliability has long been an issue, Narayananan states, as “in the past, we would not be able to predict where the ablation zone might be”. However, he believes that this problem “has mostly been one of the past” with newer devices, such as IntelliBlate. “With this particular device, we have been able to get the ablation zone we have planned,” he elaborates.
Describing he and his team’s new approach using the IntelliBlate solution, Narayananan describes their first impressions, detailing how the system has changed their microwave ablation practice.
This video is sponsored by Varian (Siemens Healthineers).
Preliminary results from the prospective, randomised, multicentre Instylla Hydrogel Embolic System (HES; Instylla) trial show the liquid embolic met primary safety and effectiveness endpoints, with a 99% freedom from major adverse event rate at 30 days follow-up, compared to a literature-derived performance goal of 75%.
The results of the trial were presented by Nadine Abi-Jaoudeh (University of California, Irvine, USA) at the Society of Interventional Radiology (SIR) annual scientific meeting (29 March–2 April, Nashville, USA) during a late-breaking abstract session.
Described as the “first” randomised controlled pivotal study of a liquid embolic for treatment of hypervascular tumours, Abi-Jaoudeh outlined that the Instylla HES is intended for the occlusion of hypervascular tumours, which was compared with standard of care-transarterial embolization/conventional chemoembolization (TAE/TACE).
Instylla HES is a biocompatible, aqueous, polyethylene glycol liquid embolic provided as two precursors that forms a hydrogel in situ when they mix at the target location. A total of 150 patients presenting with hypervascular tumours were enrolled from 22 centres, 84 enrollees were men and 66 women, with an average age of 65.4 years. Inclusion criteria included subjects with a Eastern Cooperative Oncology Group (ECOG) performance status of between 0–2 (except for metastastic disease where it was 0-1) with at least one target vessel <5mm.
Patients were randomised 2:1 to the Instylla HES treatment or the institutionally-indicated standard of care treatment. Patients underwent clinical and imaging follow-up at 30 and 90 days, with an additional clinical follow-up at 180 days post procedure. The majority of patients (44.7%) included in the trial presented with primary liver hepatocellular carcinoma (HCC), liver metastases (18%), benign liver tumours (6.7%), bone tumours (6%), and renal tumours (24.7%).
Addressing SIR 2025 delegates, Abi-Jaoudeh defined their primary safety endpoint as freedom from major adverse events which were “definitely or probably attributable” to the device and/or procedure and Grade ≥3 events per the 2017 SIR guidelines for events of death, non-target embolization, unintended target tissue ischaemia, pulmonary embolism, vascular injury requiring intervention, renal or hepatic failure, abscess in target organ/tissue, or toxic/allergic reaction to HES. The primary effectiveness endpoint was the delivery of the embolic agent to the index tumour feeding vessel with stasis of flow assessed by an independent imaging core laboratory.
Abi-Jaoudeh reported that their preliminary results showed a 99% freedom from major adverse event rate, with a single event attributed to the procedure and not the embolic. Their analysis for technical success was based on 132 vessels in 97 subjects who received HES and 66 vessels in 48 subjects who received standard of care. The speaker detailed that the primary effectiveness endpoint met and surpassed their predefined non-inferiority margin of 10% and technical success was 88.6% and 77.3% for HES and standard of care, respectively.
The Instylla HES data showed a lower numerical incidence of additional embolization procedures beyond the 90-day follow-up, reported at 8.8% for HES and 14.6% for standard of care. Further, no clinically significant non-target embolization was associated with HES, Abi-Jaoudeh outlined.
Speaking to Interventional News about the significance of these findings, Abi-Jaoudeh reiterated that this is the first trial to evaluate liquid embolics in tumours of any kind. “Liquid embolics have largely been used in the neurointerventional space for malformations or aneurysms and more recently in active haemorrhage, but not in hypervascular tumours, so this is very exciting,” she stated.
“Research has shown that ischaemia is really what we’re looking for in these tumours, and [when using embolics] you want deep uniform penetration, ideally into the vasculature down to the capillaries. That’s what’s exciting about this liquid embolic, as it’s made to mould to the vessels and achieve complete embolization,” Abi-Jaoudeh said.
Abi-Jaoudeh continued that combining Instylla HES with other drugs is where she hopes research will go next, as well as evaluating patients treated with the embolic long term. “It’s still early,” she stated, but notes that their team is focused on following up the 66% of patients with malignant tumours in their cohort to gain these long-term data.
Surmodics has announced the commercial release of the Pounce XL thrombectomy system, the latest in a suite of Pounce thrombectomy systems that provide endovascular removal of acute or chronic clot from peripheral arteries.
Intended for removal of thrombi and emboli from peripheral arteries ranging from 5.5–10mm in diameter, sizes typical of iliac and femoral arteries, the Pounce XL thrombectomy system accompanies the Pounce and Pounce low-profile thrombectomy systems, which are intended for use in 3.5–6mm and 2–4mm peripheral arteries, respectively. With a combined vessel diameter range of 2–10mm, the Pounce thrombectomy platform provides a standalone solution for rapid removal of peripheral arterial thrombi and emboli throughout the lower and upper extremities.
The Pounce XL thrombectomy system has been in limited market release (LMR) since January 2025. Anna Marjan, a vascular surgeon at Allina Health Mercy Hospital in Coon Rapids, USA, was among the physicians who used the Pounce XL thrombectomy system during the product’s LMR, a press release made by the company describes.
“Removing organised clot from large peripheral arteries without a surgical cutdown can be very challenging,” she said. “In our first use of the Pounce XL thrombectomy system we were able to extract a large amount of acute and subacute clot from the infrarenal aorta and common iliac arteries in a severely ischemic patient with just three passes of the device. Avoiding surgical cutdown reduces the need for general anaesthesia and reduces risk of surgical-site infection, which benefits patients. The Pounce thrombectomy platform is my first-line, go-to solution for endovascular thrombectomy in peripheral arteries.”
Surmodics states that the effectiveness and safety of the Pounce and Pounce LP thrombectomy systems are supported by real-world data from the PROWL registry, an open-label, retrospective, multicentre, US study of the Pounce thrombectomy platform for the removal of emboli and thrombi in the peripheral arterial vasculature. In an interim analysis of 74 patients with acute, subacute, and chronic native infrainguinal vessel limb ischaemia, average Pounce thrombectomy platform use time was 20.3 minutes, with 79.7% of patients receiving no additional clot removal treatment of the target lesion after Pounce thrombectomy platform use. Device-related adverse events were limited to one report of flow-limiting dissection.
“The addition of the Pounce XL thrombectomy system fulfils our vision of providing a simple, effective platform for removing peripheral arterial blood clots throughout the leg,” said Gary Maharaj, president and chief executive officer of Surmodics. “When minutes matter, physicians appreciate the availability of a readily deployable solution with a track record of dependable and safe results. We’re proud of the growing clinical adoption of this product and the benefits it is bringing to limb ischaemia patients in need of urgent care.”
VentiV Scientific has announced the US Food and Drug Administration (FDA) clearance of VentiV mechanical thrombectomy system to remove blood clots from the peripheral vasculature including the new VentiV Pulse platform.
“Electric pump-based thrombectomy systems can unexpectedly clog and/or remove 5–15ml per second of blood before removing blood clots,” said Dan Ryan, board of directors, VentiV Scientific. “The Pulse is designed to instantly start, stop, increase, and/or decrease thrombectomy force at the tip, decrease clogging inside the catheter, and decrease blood-loss with use of any aspiration pump currently in the hospital.”
“Patients, physicians, nurses, and technologists need more tools to treat diverse patient needs,” continued Ryan. “This FDA clearance includes 18Fr large-lumen catheter systems designed to solve unmet clinical needs and reduce procedural costs.”
The VentiV Scientific product line includes FDA-cleared over-the-wire catheters indicated for use in the peripheral vasculature plus rapid-exchange catheter systems cleared for use in the peripheral and coronary vasculature. VentiV’s unibody multi-strut thrombectomy basket retriever technology is under development and not FDA cleared at this time.
The Society of Interventional Radiology (SIR) Foundation has announced the launch of the SIR Foundation Endowment, a new funding stream designed to support interventional radiology (IR) research and education.
“Research frequently struggles due to inconsistent financial support, creating significant gaps in critical areas,” said SIR Foundation chair and the Ernest H Wood Distinguished Professor, Maureen P Kohi (University of North Carolina-Chapel Hill, Chapel Hill, USA). “The SIR Foundation is uniquely equipped to tackle this challenge, leveraging its expansive network of dedicated donors and researchers united in their commitment to advancing IR research.”
A press release issued by SIR states that the endowment offers a reliable and sustainable revenue stream to support SIR Foundation’s strategic mission to advance IR through research and education that supports research.
During SIR Foundation’s annual Gala (30 March, Nashville, USA), the foundation celebrated the first gift to the new endowment, made by interventional radiologist Barry T Katzen and his wife Judith S Katzen.
“Changes in healthcare policy and the resulting funding fluctuations can have detrimental effects on long-term research. We need to support the pioneering innovations that interventional radiology brings to healthcare. That is why Judith and I felt it was so important to invest in, and help launch, the SIR Foundation Endowment,” said Katzen, who is chief medical innovation officer of Baptist Health South Florida, and founder and chief medical executive emeritus of Miami Cardiac and Vascular Institute. “Long-term philanthropic investments, like the SIR Foundation Endowment, ensure that essential research projects can continue without interruption, despite external forces.”
“These crucial results will help to shape next steps in research, including ongoing randomised controlled trials comparing bioresorbable scaffolds to angioplasty, and eventually, to drugeluting stents.” These are the words of Michel Bosiers (University Hospital Bern, Bern, Switzerland), sharing his initial predictions ahead of several new data releases during the Peripheral Arterial programme at the 2025 Charing Cross (CX) Symposium (23–25 April, London, UK). Set to address critical challenges in the treatment of intermittent claudication and chronic limb-threatening ischaemia (CLTI), the programme will host over 30 podium firsts, including breaking data from the BASIL-2 and BASIL-3 trials.
Bosiers, who will present on day one of the peripheral programme, will deliver three-year results from the MOTIV bioresorbable scaffold (Reva Medical) trial. The trial aims to evaluate safety and efficacy of the device for the treatment of patients with rest pain or minor tissue loss due to the presence of lesions of a maximum length of 100mm at the level of the below-the-knee (BTK) arteries.
“Research on bioresorbable scaffolds is crucial because these devices offer unique advantages over traditional treatments, addressing some of the most significant challenges associated with managing peripheral arterial disease in chronic limb-threatening ischaemia patients,” says Bosiers, speaking to Vascular News ahead of this year’s symposium.
To address the increasing incidence of peripheral arterial disease (PAD) worldwide due to aging populations and rising diabetes diagnoses, Bosiers hopes that “these results will provide crucial insights into the long-term efficacy and safety of bioresorbable scaffolds in treating CLTI patients, significantly contributing to the investigation of advanced treatment options”.
Following Bosiers, Andrew Holden (Auckland City Hospital; University of Auckland, Auckland, New Zealand)—CX co-chair and member of the peripheral arterial executive board—will begin his series of podium first presentations during the first day of the symposium.
Set to deliver a first data release on drug-eluting resorbable scaffolds in the femoropopliteal segment, Holden comments that there has been “renewed interest” in resorbable scaffolds in lower limb arterial intervention following the LIFE-BTK trial results which facilitated the approval of the ESPIRT BTK (Abbott) scaffold.
“Most companies that are investigating peripheral arterial indications for drug-eluting resorbable scaffolds are focusing on tibial artery applications. However, the advantages of drug-eluting resorbable scaffolds— which include providing an acute scaffold to optimise angioplasty results and resorbing without a permanent implant—are even more relevant in the femoropopliteal segment,” Holden describes.
In his talk, Holden will present an interim analysis from the first-in-human Efemoral-1 trial, including six-month follow-up of the Efemoral (Efemoral Medical) device, which was designed to manage the anatomic and restenotic challenges of the femoral artery. “These clinical outcomes will ultimately determine if this device translates from one of promise, to a standard tool for femoropopliteal arterial intervention. I believe these data have the potential to stimulate further interest and excitement around this important advancement in vascular care,” he adds.
Later in the peripheral programme, Holden will also deliver a podium-first talk on new intravascular lithotripsy (IVL) technologies and trial data for calcified tibial artery disease. He tells Vascular News that, in several vascular territories, IVL has achieved “excellent acute luminal gain” in calcified arteries with a “low incidence of dissection of provision stenting”. Yet, Holden notes that there has been limited evidence supporting IVL use in tibial arteries, calling for a successful technology which can address calcification in these vessels and achieve better results than when treating with angioplasty.
“These data will help support discussion on the optimum management algorithm for CLTI patients with calcified tibial artery disease,” says Holden, who adds that delegates can expect interesting debate on whether the two technologies presented are “complimentary or competitive”.
Elsewhere in the day one peripheral itinerary, Hany Zayed (Guy’s and St Thomas’ NHS Foundation Trust, London, UK) will present during a session dedicated to vessel preparation techniques, comparing plain balloon angioplasty, IVL and atherectomy prior to the application of a drug-coated balloon (DCB).
Zayed comments: “Vessel preparation is an evolving concept which is gaining popularity amongst interventionalists, with the aim to enhance the outcomes of definitive treatment of arterial lesions. It is therefore important that we appraise the available research in order to highlight areas in need of further research to help guide our routine daily practice.”
Zayed states that their first-release data to be presented at CX 2025 will highlight that the current evidence is still heterogeneous, particularly in regard to patient cohort e.g. CLTI or intermittent claudication, lesion characteristics and complexity, as well as duration of follow-up.
During a ‘Challenges in aortoiliac occlusive disease’ session, Maria Antonella Ruffino (IIMSI, Ente Ospedaliero Cantonale, Lugano, Switzerland) will present on new large balloon IVL in the treatment of aortic lesions. Importantly, she will question whether IVL is an effective therapy when used alone or in combination with stenting as a means of vessel preparation.
In conversation with Vascular News ahead of her presentation, she details that there is growing evidence in support of polytetrafluoroethylene (PTFE)-covered stents for the treatment of infrarenal occlusive disease of the abdominal aorta as an alternative to surgical reconstruction.
“Despite the type of stent we want to implant, suboptimal vessel expansion still represents a limit in the treatment of isolated aortic lesions, where neither high pressure balloon angioplasty nor atherectomy can significantly impact on wall calcifications,” says Antonella Ruffino.
Today, with the advent of ‘non-stent’ technology such as IVL that can be applied to large vessels and facilitate vessel expansion, Antonella Ruffino underlines the importance of confirming its safety and efficacy in aortic lesions. She hopes their research will highlight IVL technology as an “additional weapon” to treat very calcified isolated aortic lesions, and demonstrate that the combination of IVL and stenting could “help to overcome the risk of incomplete stent expansion with consequent restenosis”.
The CX 2025 peripheral programme will also showcase several challenging debates on technologies and techniques including vessel preparation devices versus high-quality plain balloon angioplasty, and whether endovascular techniques should only be offered to patients with common femoral artery disease who cannot undergo endarterectomy. Additionally, attendees will see the launch of the CX Hurting Leg campaign—an initiative to reduce amputations through increasing awareness in deprived communities and to promote systemic healthcare reform.
Adept Medical has announced two updated product launches, coinciding with the Society of Interventional Radiology’s 50th annual scientific meeting (29 March–2 April, Nashville, USA).
This includes the launch of the Retrograde IR Platform–Narrow, a complementary addition to its existing range, and the Overhead Arm Support MR Safe–Small. Both are available commercially from 14 April.
Developed in response to post-market feedback and extensive research, the new size Retrograde IR Platform–Narrow addresses the need for a more compact over-patient work surface for guidewire management during femoral access procedures.
It is designed for clinicians who prefer a compact surface, closer patient access, rail-mounted equipment clearance and compatibility with shorter wires and rapid exchange catheter systems. It remains easy to setup, offering operational security during instances of restlessness due to its positioning above the patient’s legs and ability to be locked in place, Adept Medical says in a press release.
It is height adjustable, radiolucent, durable, lightweight and continues to provide clinical benefits around the current practice of laying equipment on the mattress and patient, reducing the need to retrieve equipment from behind for a more ergonomic workflow.
“While a lot of customers found the wider platform really useful for placement of all their procedural devices, some customers did feedback to us that the width did restrict placement of some of their auxiliary rail mounted equipment. It was a no brainer to develop a narrow version that enabled this,” says Matt Lazenby, Adept Medical product development manager.
Overhead Arm Support–Small
The Overhead Arm Support MR Safe–Small builds on Adept’s 2021 MR Safe model, developed in response to market feedback around a need to better support children and small adults.
The Small support is approved for use in computed tomography (CT) and magnetic resonance (MR) imaging centres with bore sizes of 600mm and larger and is compatible with any C-arm imaging system.
It features two strap mount locations per arm, positioned for shorter arm proportions while allowing flexibility for IV access. For added security and comfort, soft, pliable, latex-free polyurethane straps help secure the arms and reduce the risk of displacement.
“Our goal was to provide our customers with the same trusted support across a wider patient range. The new small size ensures better positioning and comfort for smaller patients while maintaining the ease of use and stability clinicians rely on,” says Mike Oxborough, Adept Medical senior product designer.
Cook Medical has announced that itsZilver PTX drug-eluting stent (DES) haslower rates of in-stent occlusions among patients with restenosis at three years than the Eluvia DES (Boston Scientific), according to real-world data from the REALDES study. The company notes that the data, published by Tsuyoshi Shibata (Sapporo Medical University Hospital, Sapporo, Japan) et al in the European Journal of Vascular and Endovascular Surgery (EJVES), are the first to compare Zilver PTX and Eluvia in real-world practice at three years.
“There have been many unanswered questions on the reliability of the current data comparing the different drug-eluting stents on the market. REALDES helps paint a more complete picture on DES differences, evaluated by independent investigators in a real-world setting,” said Alec Cerchiari, director of product management for Cook’s peripheral arterial disease and venous specialty. “We are grateful to the physicians and hospitals that participated in this study.”
REALDES is an investigator-initiated multicentre, prospective, observational study designed to compare the Zilver PTX DES and Eluvia DES in a real-world setting for treating symptomatic femoropopliteal lesions. Overall, 200 limbs with native femoropopliteal artery disease were treated with Zilver PTX (96 limbs) or Eluvia (104 limbs) at eight Japanese hospitals between February 2019 and September 2020. The primary outcome measure of this study was primary patency at three years, defined as freedom from restenosis or occlusion without reintervention.
Key three-year study outcomes include:
There was no significant difference in primary patency (Zilver PTX, 70% vs. Eluvia, 65.2%; p=0.74) or freedom from clinically driven target lesion revascularisation (CD-TLR; 79.4% vs. 76.3%; p=0.27), despite the Zilver PTX arm having longer lesions (185.7±92mm vs. 160±99mm; p<0.005).
In patients with restenosis at three years, there was a significantly higher rate of in-stent occlusions (Tosaka class III) for those treated with Eluvia (57.7%) compared to Zilver PTX (29.2%; p=0.041).
“These findings contribute valuable insights into optimising treatment outcomes and guiding future stent selection,” said Shibata.
Evident Vascular has announced the successful closing of its Series B financing with new investors Shangbay Capital and two undisclosed multinational strategics joining founding investor Vensana Capital. A press release details that the funding will accelerate development of the company’s advanced intravascular ultrasound (IVUS) technology designed to enhance vascular imaging and patient outcomes and support 510(k) US Food and Drug Administration (FDA) clearance ahead of US market launch.
“We are proud to continue supporting Evident Vascular, which is at the forefront of innovation in intravascular imaging that has become the standard of care in peripheral vascular and complex coronary interventions,” said Cynthia Yee, partner at Vensana Capital. “Evident’s next-generation IVUS platform represents a transformative step forward in vascular care, offering clinicians powerful tools to enhance diagnosis and guide treatment consistent with clinical evidence and today’s medical guidelines.”
Evident Vascular notes in a press release that its vision is to transform vascular imaging through innovations that expand the adoption of IVUS by increasing its utility and accessibility in clinical practice.
“This significant investment underscores our investors’ confidence in Evident Vascular’s mission and technology while highlighting the vital role of intravascular imaging in optimising patient outcomes, clinical decision-making and procedural success,” stated Howard Rosen, chief executive officer and co-founder of Evident Vascular. “We will accelerate our progress toward FDA clearance and further the development of our AI [artificial intelligence]-powered IVUS solution, which aims to set a new standard in vascular image-guided therapy.”
Merit Medical Systems has announced that the six-month results from the randomised arm of the Wrapsody arteriovenous access efficacy—WAVE—trial are scheduled for publication in the April issue of Kidney International, ahead of the presentation of 12-month results from the trial at the Society of Interventional Radiology’s 50th annual scientific meeting (29 March–2 April, Nashville, USA).
The creation of an arteriovenous fistula (AVF) to achieve long-term access to blood vessels is required for patients undergoing haemodialysis. However, narrowing of blood vessels in and around the AVF can interfere with haemodialysis delivery, resulting in potentially life-threatening consequences. The Wrapsody cell-impermeable endoprosthesis (CIE) is designed to help clinicians restore vascular access in patients on haemodialysis who experience stenosis in their venous outflow circuit.
The WAVE trial is a multicentre, international, investigational device exemption (IDE) trial designed to evaluate the Wrapsody CIE’s safety and efficacy over two years. In the randomised arm of the trial, 245 patients on haemodialysis who experienced stenosis in the venous outflow of their AVF were treated with the Wrapsody CIE (n=122) or standard percutaneous transluminal angioplasty (PTA, n=123).
Treatment efficacy was defined as the proportion of patients who did not require an intervention due to clinically driven target lesion revascularisation or target lesion thrombosis (target lesion primary patency). An additional efficacy endpoint was the proportion of patients without loss of vascular access anywhere within the circuit from the time of their initial treatment to the need for reintervention or abandonment of vascular access (access circuit primary patency).
Primary safety was defined as the proportion of patients with safety events that negatively affected the vascular access or venous outflow circuit, excluding target lesion revascularization or thrombosis, which resulted in reintervention, hospitalization, or death.
Initial results at six months demonstrated that the target lesion primary patency was significantly higher for the Wrapsody CIE vs. PTA (89.8% vs. 62.8%, p<0.0001). Similarly, the access circuit primary patency was significantly higher for the Wrapsody CIE vs. PTA (72.6% vs. 57.9%, p=0.015). No significant difference in the safety outcome was observed between treatments.
At 12 months, the Wrapsody CIE remained significantly higher than PTA for both target lesion primary patency (70.1% vs. 41.6%, p<0.0001) and access circuit primary patency (58.1% vs. 34.4%, p=0.0003).
“The Wrapsody CIE’s positive outcomes at one year address an important knowledge gap regarding the potential durability of the device,” said Dheeraj K Rajan (University of Toronto, Toronto, Canada, and WAVE trial investigator. “It is encouraging to know there is a new device available to help us prolong functional vascular access in our patients.”
“At Merit, we are pleased to continue building on the superior results of the Wrapsody CIE,” said Fred P Lampropoulos, Merit’s chairman and chief executive officer. “We are committed to improving patient care and providing clinicians with the data they need to make evidence-based decisions.”
The Wrapsody CIE received premarket approval (PMA) from the US Food and Drug Administration (FDA) in December 2024. Merit began commercialisation of the device in the USA in January 2025. The device previously received the CE mark for commercial use in the European Union (EU) and is available in Brazil.
Imperative Care today announced US Food and Drug Administration (FDA) 510(k) clearance of the 82cm version of its Symphony 16Fr catheter, the company’s latest innovation designed to elevate care for patients with venous thrombosis.
“Thrombectomy procedures have emerged as one of the most powerful treatments in medicine, restoring vital blood flow in minutes. Historically, peripheral vascular thrombectomy has lacked technologies that effectively address challenging clot and preserve vessel health for the patient,” said Doug Boyd, senior vice president and general manager of Imperative Care’s Vascular business. “Imperative Care set out to transform vascular care through purpose-built precision thrombectomy technologies that combine large-bore power with a precisely controlled deep vacuum within the sterile field, along with a focus on minimising blood loss. The Symphony thrombectomy system has introduced precision thrombectomy to the market, and we are confident it will deliver faster, safer and more precise clot removal that will ultimately benefit patients impacted by devastating vascular diseases.”
Initial cases
The company also announced the successful completion of initial patient cases using the Symphony 16Fr 82cm catheter. Several of these were completed by Bennet George, interventional cardiologist at Vital Heart & Vein in Houston, USA.
“In my early experience, I’ve been able to consistently achieve 97% clot removal in, on average, two passes, with minimal blood loss (<120ml) in less than ten minutes. With a large-bore catheter and powerful deep vacuum, Symphony allows me to effectively treat highly challenging clot morphologies in minutes and in a blood-efficient way, ensuring the best possible outcomes for my patients,” said George. “The customised length of the 16Fr 82cm catheter gives me an additional capability to address both acute and organised clot in my venous procedures, and I look forward to its continued impact on the patients we treat.”
This latest innovation expands the Symphony thrombectomy system offering to include 16Fr 82cm, 16Fr 117cm and 24Fr 85cm catheters.
Imperative Care details that Symphony has an integrated controller that delivers nearly three times the clot removal force compared to legacy aspiration systems. Additionally, the system includes the ProHelix Mechanical Assist, a unique tool designed to facilitate clot ingestion, along with the Imperative Care Generator, which the company claims is the most powerful aspiration pump available on the market.
“At Imperative Care, we have always started by looking at critical unmet needs across the patient journey and working with a connected-care mindset to purposefully engineer solutions that put patients in the best position to live full and independent lives,” said Fred Khosravi, chairman and chief executive officer of Imperative Care. “With this latest offering and the enabling innovations in development at Imperative Care, we are poised to further advance the paradigm of care and provide physicians with the technologies that allow them to swiftly address these urgent ischaemic diseases and best care for their patients.”
Sarah B White (Milwaukee, USA) dons many titles, namely she is a tenured professor of vascular and interventional radiology, a professor of surgery and surgical oncology, as well as associate dean at the Medical College of Wisconsin (MCW). Among her designations, White has been recognised as a ‘triple threat’, excelling as a researcher, clinician and professor, breaching brand new territory, not only for women in the field of interventional radiology (IR), but for all, taking on previously unexplored topics. Through research, White’s focus has been interventional oncology (IO), specifically developing new drug platforms and delivery methods to overcome treatment resistance, and to better understand the role of the tumour microenvironment including hypoxia. Here, White speaks to Interventional News about her love for IR and how she built her career in the field.
What attracted you to a career in medicine, and what made you choose IR?
I was born at Oregon Health & Science University (OHSU) in Portland, USA, when Charles Dotter was walking the halls. I am convinced that when I was born, Dotter sprinkled fairy dust on my mother and that’s what drove my ever-present and undying loyalty and devotion to IR. In reality, we had a close family friend, Robert Seigel, who practiced neurointerventional radiology (NIR). I remember being at his house playing with his kids when he came home from work. He told me about a tough case he had, where he performed the balloon procedure on a sick woman. It was at that moment, that I knew there was no other career for me. All these years later, Bob actually called me to refer a patient, who flew across the country to seek care with me here at MCW.
Who have been your mentors throughout your career?
I have had the absolute privilege of having truly amazing mentors throughout my career. After graduating from college with a degree in German, I was lucky enough to attend a post baccalaureate programme and the University of Pennsylvania (PENN) where I completed my prerequisites for medical school. During this time, despite having virtually no experience in research, Frank Lee hired me after I responded to an ad in the newspaper. He was a new principal investigator and needed lab staff. Only two short years later, we published, with me as first author, a truly novel finding in science. Hypoxia-inducible factor 1 (HIF)-1 was modified by a proline hydroxylation. I went off to medical school and had the good fortune of working with Brad Wood, who saw the fire in my belly. He has written letters of recommendation for me for residency, FSIR, and all my promotions. His charisma and undying love of IR was contagious.
During residency, I had the privilege of working with a phenomenal team and was mentored by Rich Schlansky-Goldberg, Scott Trerotola, Bill Stavaropolous, Max Itkin, Jeff Solomon and Aalpen Patel. This team of amazing mentors challenged me every day and made sure that I would be not only a good interventional radiologist, but a good partner, teacher and researcher. I am still in touch with each and every one from PENN IR and continue to learn from them. I do not include Michael Soulen in the list with the other PENN faculty, because Michael has been more than a mentor. He has been a mentor, a coach, a sponsor, and now, a true friend. His frank feedback and ongoing expectation of excellence helped me grow and led me into a career that I truly love. His best advice was that if you have the fire in your belly, you will be successful.
Now, I have the good fortune or working alongside a brilliant group of interventional radiologists that continue to mentor me today. Bill Rilling stood beside and mentored me as I fumbled through cases early in my career and has helped guide me though all of my leadership roles. Bill has an unending cadre of wisdom. I was on call and called him for advice and he said: “You know what to do, go get ‘em tiger”. Robert A Hieb has been my biggest cheerleader and always answers my calls at 2am when I’m stuck doing a challenging vascular case. Parag Patel has been a quiet voice in the background keeping me sane and helping me through the challenges of academic medicine. Sean Tutton taught me how to have a voice among the many loud voices in academic medicine. Eric Hohenwalter has been the voice of reason and clarity and always showed me kindness and compassion.
Nationally, I have had the good fortune of having a tremendous network of mentors including Alda Tam, Nishita Kothary, Reed Omary, Andrew Larsen, Matt Callstrom to name a few.
Could you describe a case that has been the most memorable thus far?
I have had innumerable memorable cases throughout my career. I will however relay a story of one of the kindest patients I had the honour of treating. She initially presented to me for consideration for a transjugular intrahepatic portosystemic shunt (TIPS), because she had refractory ascites. I reviewed the imaging which revealed that she had a recurrence of her pancreatic cancer, which she believed to be in remission. She walked in thinking that we were having a conversation of fluid management and walked out with the devastating news that her cancer was back. I had never met this patient before that visit and had no relationship with her. I however delicately and carefully explained the situation to her. We ended up agreeing to placing a Denver shunt to manage the ascites. A week later, while doing the procedure, she kept telling me that I was doing a good job. It turned out that she was a seamstress and was making her daughter’s wedding dress for a wedding that was just a few short months away.
She re-presented a week before the wedding and I was called by the intensive care unit (ICU) as she had been admitted with septic shock, and the ICU team were advising that the patient and her family transition to a hospice. She and her family however were unwilling to make any decisions without first talking to me. I immediately went up to the ICU. They believed that the source of her infection was the Denver shunt, and because her daughter’s wedding was just a week away, I convinced the ICU team to aggressively treat her, as we just needed to get to the wedding. I went bedside and removed the shunt, again, all the while her cheering me on and repeatedly telling me what a good job I was doing. The procedure was successful, and she was discharged with enough time to finish the wedding dress and attend the wedding, although in a wheelchair.
After the festivities, she went home to find a kitten eagerly awaiting her, something she had always wanted. She died a few days later, surrounded by family and while petting her kitten. Though we can’t always cure patients, we can advocate for them to achieve their goals, and help them die peacefully and with grace. This dear patient also showed me that complications don’t define you, but how you handle them does.
You were the first in the USA to be accepted and graduate from the direct pathway at the University of Pennsylvania Hospital. How did this come about and what was your experience?
As a medical student, I went to the Society of Interventional Radiology (SIR) conference. They held a medical student breakfast, which was attended by Al Nemcek and Bob White. There were eight medical students at the breakfast. Nemcek told me about this new training pathway that was going through the approval process and would not be ready for me. As soon as I heard about it, I went to the SIR website and emailed all of the programme directors at the schools listed as being part of the direct pathway. Michael Soulen, at the hospital of the University of Pennsylvania, was the only person to respond. He sent me some detailed information, but told me that he didn’t want to discuss anything further and to contact him “if” I got an interview at PENN.
Within minutes of being offered an interview a few years later, I contacted Michael again. Back then, all the interviewees came to PENN during the same weekend. At the dinner on Friday night, Michael found me, and I sat and had dinner with all of the PENN IR faculty. When it came time for the match, Michael called me and told me that I had been selected to join them as the first direct pathway resident in the country. The caveat was that the programme had not been officially approved yet. I jumped at the chance, matriculated that July and luckily, the programme was officially approved.
In 2024 you published a paper outlining why IR and diagnostic radiology (DR) should stay in alignment. If they were to be separated, how do you believe IR would be affected?
As the US healthcare system moves more towards a work relative value unit (wRVU)- based reimbursement structure, IR separating from DR will make us vulnerable by falling short of financial metrics. DR also has a larger footprint and therefore is more often invited to sit at the table with hospital executives and policymakers to pursue the ongoing needs of IR. Globally, IR sees patients have limited access to our specialty, and a break may further prevent access to care. Finally, the core of our specialty is our expertise in marrying imaging with procedures. If we lost the robust education we have in imaging, I believe our specialty would suffer greatly.
What have been some of the most important developments in IR and IO over the course of your career so far?
IR has undergone tremendous change during my career. We have moved from a subspecialty designation, to designation as a primary specialty. Medical students can now match directly into IR residency programmes. We have evolved in the research realm from being perceived as proceduralists, to being perceived as true scientists, by running such pivotal trials as ATTRACT, CTRACT, PE-TRACT and RETNET. We have secured a seat at the table in oncology care by being on the National Comprehensive Cancer Network (NCCN) panels and founding a society solely dedicated to oncology procedures, with the Society of Interventional Oncology (SIO).
What does your life outside of medicine look like?
I am the mother of three amazingly kind, respectful, empathetic and intelligent children. My mornings are filled with making lunches and walking the kids to school. Evenings are filled with lots of laughter, violin practice, homework and reading bedtime stories. My kids constantly remind me to not sweat the small stuff and that joy and fun can be found everywhere. I love the outdoors, hiking, travelling and cooking.
Recently published in The Lancet Oncology, the randomised, international, multicentre, phase III non-inferiority COLLISION trial demonstrated comparable results between thermal ablation and surgical resection for small-size colorectal liver metastases, initiating re-evaluation of clinical practice and the previously held assumption that ablation should be reserved for unresectable lesions only. Speaking to Interventional News, principal investigator Martijn Meijerink (Amsterdam UMC, Amsterdam, The Netherlands) recognised “completely unexpected” results in their data concerning local control and tumour progression, with the potential to push the needle toward minimally invasive intervention in a broader range of lesions.
Between August 2017 and February 2024, 300 patients were randomly assigned to two groups—148 to the experimental treatment and 148 to the control treatment. Four patients in total were excluded as they were found to have other disease pathology. The trial met predefined halting criteria for early benefit, and it was deemed unethical to continue. It was determined that thermal ablation resulted in fewer side effects (28 cases [18.9%] vs. 67 cases [45.9%]) and shorter hospital stays. Serious side effects occurred in 11 patients (7.4%) in the ablation group and 29 patients (19.9%) in the surgery group—these included bleeding that needed intervention (one patient [1%] vs. eight patients [5.5%]) and infections requiring treatment (six patients [4%] vs. 11 patients [7.5%]). In the researchers’ analysis, local control was found to be superior following ablation—an “unanticipated” result, said Meijerink— with only a single patient in this group for whom local control was not achieved.
When asked if these results were close to his predictions, Meijerink commented that he expected overall survival to be identical. “What was completely unexpected was local control and tumour progression,” he said. “This outcome means that in small-size tumours, the vast majority can be locally controlled with ablation. Even if you had a perfect surgeon, it would still be unacceptable to continue resecting small-size tumours. We should focus on what I think is the next standard of care— ablation—because in high-volume, dedicated centres you can locally control tumours with this technique.”
The path Meijerink and colleagues at Amsterdam UMC took to arrive at this conclusion was one built from “trust”, he described, and was forged from over a decade’s worth of observation showing improved outcomes via thermal ablation. “We saw the majority of tumours weren’t coming back and our surgeons were completely open to a potential future where resection for smaller tumours is no longer the first option, then we started to make this principle concrete,” Meijerink stated.
Admittedly, he added that this collaborative relationship between interventional radiologists and surgeons at his institution is “unique” and that they are “lucky” to operate in this way. Although, Meijerink stated that part of the reason for initiating the COLLISION trial was to seek an “end to the discussions” between their departments on the best course of treatment.
The COLLISION trial included patients from 14 centres in The Netherlands, Belgium and Italy, with ten or fewer small-size (≤3cm) colorectal liver metastases, no extrahepatic metastases, and an Eastern Cooperative Oncology Group (ECOG) performance status of 0–2, stratified per centre, and according to their disease burden, into low, intermediate, and high disease burden subgroups.
Meijerink reflected that the process of setting up the trial was lengthy. Having finalised the study protocol in 2015, the search for funding “took a long time”, he said, but believes this extension was “a good thing”.
“We would have had a negative trial because we weren’t as good back then. We would have had more recurrences when compared to surgical resection, whereas now, we are much better at completely eradicating the disease. Even though it was frustrating, it’s good we have the results now and not ten years ago,” Meijerink explained.
In part, Meijerink added that technological advancements such as confirmation software are a central reason for the positive results of the COLLISION trial. “It’s a no-brainer. Eyeballing the tumour is not good enough—sitting down to check the margins and bring the needle back for any residual tumour while the patient is still under anaesthesia dramatically improved our results,” he said.
Despite advancements in devices and targeting software, Meijerink highlighted that inclusion criteria for the COLLISION trial stipulated institutions have ample experience with thermal ablation and must have performed more than 100 cases to meet this description. Although he believes their data are convincing, he cautioned less experienced centres from changing their practice too quickly, without first achieving recurrence rates below 10% in patients with small-size tumours.
“My suggestion for centres that want to change their practice—and I agree that we should all strive to—is to first look at your last 50 or 100 cases and see if your recurrence rates are below 10%. If they are not, I wouldn’t change anything for now. We cannot generalise the results without first making sure you’re doing a good job,” he stated.
To address the “steep learning curve” institutions can be met with when looking to implement change, Meijerink offered the COLLSION-2 trial, a stepped-wedge cluster trial comparing current practices to best practices. From confirmation software to antibiotic use and general anaesthesia, Meijerink et al—via a consensus panel meeting—will seek to define best practice and subsequently randomise centres.
“If your centre is enrolled in the trial, you will receive a call disclosing details of ‘best practice’ in regard to thermal ablation and will be given six weeks to implement it. These trials are very often positive because, not only do you improve your outcomes, but it’s a way for centres to achieve outcomes equal to the best performing centres,” Meijerink described.
“There’s a lot to improve and why should we do that? I think we, as interventional radiologists who are stepping into oncology should realise that we need to be highly dedicated. The patient is on the table to have their cancer eradicated—it’s not inflating a balloon and maybe it comes back and needs to be reinflated. We have to do a better job. It’s in human nature to say, ‘I think I got it, and if I didn’t, I’ll do it again in six months’, but that’s not our future. Our future is making sure you treated that patient the best way possible and to standardise this care among centres,” said Meijerink.
Meijerink and colleagues’ research efforts to solidify thermal ablation as the new standard of care are ongoing; the COLLISION XL trial, a randomised controlled trial comparing thermal ablation to stereotactic body radiotherapy (SBRT) for larger-size and unresectable colorectal liver metastases 3–5cm, is currently recruiting. “Thermal ablation more often fails to provide local control in larger tumours, but has shown equal recurrence rates to SBRT,” explained Meijerink. Their team is also recruiting for the COLLISION RELAPSE trial, comparing upfront repeat local treatment with thermal ablation and/or surgical resection versus neoadjuvant chemotherapy followed by local treatment for patients with new colorectal liver metastases in the first year after the initial local treatment.
Through these trials, Meijerink hopes to provide data that will place tumours up to 5cm within the remit of interventionalists who can provide minimally invasive, efficacious treatment. “Technological advancements are not stopping. In the future I’m sure we will be able to compete with surgery for patients with larger tumours,” Meijerink stated.
Life Seal Vascular has announced the appointment of Matt Thompson as chief executive officer (CEO).
A company press release has stated that Thompson’s career as a vascular surgeon and medical device executive positions Life Seal Vascular to accelerate the development and commercialisation of its vascular technologies.
“We are thrilled to welcome Thompson as our CEO,” said Robert Mitchell, executive chairman of Life Seal Vascular. “His unique combination of clinical expertise and executive leadership in the vascular medical device industry makes him the ideal leader to drive our next phase of growth. His prior service on our board has provided him with deep insight into our company’s mission and we are excited for his leadership as we advance our technologies into clinical use.”
From 2002 to 2016, Thompson served as a leading vascular surgeon at St. George’s Hospital in London, UK, where he gained international recognition for his expertise in complex aortic repair, the company states. Transitioning to the medical device industry, he held key leadership roles, serving as chief medical officer at Endologix from 2016–2021 and chief executive officer from 2021–2025. He currently continues to contribute to Endologix as chief medical officer.
“I am honoured to join Life Seal Vascular at this pivotal stage,” said Thompson. “The company is developing breakthrough endovascular solutions that address critical unmet clinical needs, particularly in the prevention of type II endoleaks following endovascular aneurysm repair. I look forward to working with the team to bring these innovations to patients and clinicians worldwide.”
Xeltis has today announced the appointment of clinical nephrology experts An De Vriese and Haimanot (Monnie) Wasse to its medical advisory board.
De Vriese is currently head of the division of nephrology and infectious disease in AZ Sint-Jan Brugge, in Brugge, Belgium and guest professor at Ghent University in Gent, Belgium, while Wasse serves as the interim chair of the department of internal medicine, and the chief of nephrology and director of interventional nephrology at the Rush University Medical Center in Chicago, USA. A press release by Xeltis has stated that both add considerable clinical nephrology expertise to the company’s medical advisory board and will work alongside current members to offer strategic and clinical guidance as Xeltis advances aXess towards commercialisation.
Eliane Schutte, chief executive officer of Xeltis said: “We are pleased that both De Vriese and Wasse have chosen to join our medical advisory board, bolstering our already stellar team of advisors. The appointments represent significant validation of the unique and promising nature of our technology from leading experts in the field. Their experience across nephrology and vascular access will be invaluable as we continue to progress aXess through its pivotal trials in the EU and US, with primary readouts for our EU pivotal trial expected in mid-2025.”
“It is an honour to join Xeltis’ MAB at such a pivotal time in the company’s development,” commented De Vriese. “I am truly excited by Xeltis’ innovative technology which, through its avoidance of the frequent reinterventions and infections associated with current treatment options, has the potential to transform patient outcomes for those with end-stage renal disease.”
On his recent appointment, Wasse stated: “I am familiar with the important work of Xeltis, having kept a keen eye on the continual clinical progress of its technology. aXess has an immensely promising medical profile, and I am proud to now be in a position to offer my expertise in interventional nephrology and vascular access to further the clinical development of this innovative technology.”
Currently, Xeltis is advancing pivotal trials in both the EU and the US for aXess; enrolment was recently completed in the EU while ten patients have now been implanted in the USA.
First RETNET data show no difference in progression-free survival between TAE and TACE for neuroendocrine liver tumours
Key research updates in lower extremity peripheral arterial disease (PAD) from the Leipzig Interventional Course (LINC 2025; 28–30 January, Leipzig, Germany) and the International Symposium of Endovascular Therapy (ISET; 2–5 February, Hollywood, USA)
Interview: Ziv Haskal (Charlottesville, USA) gives pragmatic shape to the emerging future of resorbable microspheres in MSK embolization
Profile: Sarah White (Milwaukee, USA)
Research supports combined treatment approach for erectile dysfunction due to mixed arteriovenous disease
First RETNET data show no difference in progression-free survival between TAE and TACE for neuroendocrine liver tumours
Key research updates in lower extremity peripheral arterial disease (PAD) from the Leipzig Interventional Course (LINC 2025; 28–30 January, Leipzig, Germany) and the International Symposium of Endovascular Therapy (ISET; 2–5 February, Hollywood, USA)
Interview: Ziv Haskal (Charlottesville, USA) gives pragmatic shape to the emerging future of resorbable microspheres in MSK embolization
Profile: Sarah White (Milwaukee, USA)
Research supports combined treatment approach for erectile dysfunction due to mixed arteriovenous disease
Inari Medical, now part of Stryker, recently announced the launch of its Artix thrombectomy system. Purpose-built for the distinct needs of the peripheral arterial system, Artix is a combined aspiration plus mechanical thrombectomy solution that delivers procedural control and versatility, and is designed to set a new standard for arterial thrombectomy.
Stryker notes that the Artix system builds on the success of Inari’s venous thrombectomy devices and is its inaugural entry into the arterial space. “Inari offers a comprehensive toolkit approach to arterial thrombectomy with an innovative, over-the-wire system that provides physicians with the flexibility to aspirate and/or mechanically extract a clot,” a press release reads.
Jonathan Bowman (Norwalk Hospital, Norwalk, USA) performed the first commercial case with Artix on 19 October 2024. “The Artix thrombectomy system marks a significant advancement in peripheral arterial thromboembolism treatment,” said Bowman. “With Artix, I finally have a solution that effectively addresses a wide range of clots while enabling me to maintain vessel access and retain control throughout the entire case. I expect Artix will take the place of open surgical repair in many of my arterial cases.”
Key distinctive features of the Artix system include:
Dual mechanical thrombectomy and aspiration toolkit designed to remove acute to chronic clots in a single session via a streamlined procedure
Aspiration-capable, 8Fr low-profile, trackable, kink-resistant sheath in both 65cm and 90cm lengths expands treatment options by enabling more complex and distal interventions
Innovative over-the-wire mechanical element designed to effectively collect and retrieve acute-to-chronic clot
Covered nitinol mesh funnel provides temporary flow restriction during the procedure to minimise the risk of arterial clot migration
“There is a real clinical need to address chronic thrombi and decrease the risk of clot migration. Artix will raise the bar of effective arterial thrombectomy,” said Tom Tu, chief medical officer of Inari Medical. “We are excited to bring Inari’s core competency in thrombectomy to the arterial space with the goal of improving outcomes.”
Philips has recently announced that it will no longer sell its Tack endovascular system in the USA following a Class I recall issued by the US Food and Drug Administration (FDA).
A Class I recall is the FDA’s most serious classification, which denotes that the continued use of the affected product could result in severe injury or death.
The FDA’s decision follows reports that the Tack endovascular system—designed to treat arterial dissections—has posed challenges for users, sometimes necessitating additional interventions to retrieve or remove the implant. The self-expanding device is composed of nitinol, a nickel-titanium alloy.
The device is used following angioplasty, a procedure that widens narrowed or blocked arteries. While rare, tears in blood vessels can be a serious complication, and the Tack implant is designed to repair these by securing damaged tissue to the artery wall.
The FDA warned that continued use of the device could lead to significant health risks. Short-term complications include partial or complete blockage of blood flow, perforations in the artery’s inner lining, or full-thickness arterial tears. Long-term consequences may involve pain, tissue loss, re-narrowing of the vessel, and, in more severe cases, bypass surgery, amputation, or death.
Philips has reported 20 injuries linked to the Tack system but has not received any reports of fatalities.
The Tack system was initially approved by the FDA in April 2020. It was developed by Intact Vascular, a cardiovascular company acquired by Philips for US$275 million later that year.
Results from CIREL—the largest, pan-European, prospective study of irinotecan-eluting transarterial chemoembolization (TACE) for colorectal liver metastases (CRLMs), show a comparably long median overall survival (OS) when used as salvage therapy and “promising” hepatic progression-free survival (HPFS) when used with systemic therapy or thermal ablation as a post-inductive or consolidation therapy.
The study, published in European Society for Medical Oncology (ESMO) Open by Dirk Arnold (Asklepios Tumor Centre Hamburg, Hamburg, Germany) et al, was led by Philippe L Pereira (SLK Kliniken Heilbronn, Germany) and Julien Taieb (Georges Pompidou European Hospital, Paris, France), who sought to evaluate when and for whom irinotecan-TACE should be preferred over other locoregional treatments, or may be added to other treatments.
CIREL was conducted across 11 European countries including 20 centres, and enrolled 152 patients in total between February 2018 and August 2020. Patients aged ≥18 years with histologically confirmed CRLMs were eligible for inclusion following a multidisciplinary team (MDT) decision to be treated with irinotecan-TACE. All patients underwent at least one treatment session with LifePearl (MicroVention) microspheres and attended follow-up sessions between 4–8 weeks and 12–16 weeks following the last treatment session. Subsequent follow-up was then conducted every eight weeks until loss to follow-up, death or until the end of data collection.
The primary endpoint of the study was to identify the number of indications that the device is used for, assessed by stage and previous treatment(s). To this end, irinotecan-TACE was categorised into two treatment intentions: salvage therapy, which was defined by the authors as intensification of treatment with concomitant systemic therapy, and salvage treatment in progressive patients pre-treated with systemic therapy, with or without concomitant systemic therapy, and, as post-inductive/consolidation therapy, defined as LifePearl irinotecan as a first-line, consolidation or closing treatment with or without systemic therapy, or as combination treatment with ablation with curative intent.
The study cohort had an average age of 66 years, 61.2% of patients were male and extrahepatic metastases were present in 56.6% of patients. Irinotecan-TACE was used in 57.2% of patients as salvage therapy for those who had progressive disease after at least one line of systemic therapy, whereas 42.8% of patients received irinotecan-TACE as a post inductive/consolidation therapy with irinotecan-TACE before/after systemic therapy or before/after thermal ablation. The prespecified treatment plan was completed in 89% and 72% of patients in each respective group.
Overall, the median OS was 14.5 months. In the irinotecan-TACE as salvage therapy group, median OS was 9.9 months (7.4–12.8 months) and the median PFS was 3.8 months (2.9–4.7 months). The median OS for the treatment as post-inductive or consolidation therapy when used in combination with systemic therapy or thermal ablation was 19.1 months (16.2–24.2 months), and the median PFS was six months (4.5–8.7 months).
The authors highlight that the median HPFS was 6.2% with six- and 12-month HPFS rates of 52% and 24%, respectively. In the irinotecan-TACE as post-inductive/consolidation therapy group, HPFS was reported as 8.7 months, which “since irinotecan-TACE is a locoregional treatment that acts directly in the liver, an HPFS of 8.7 of the post-inductive/consolidation therapy should be highlighted”, state the authors.
Following a multivariable analysis, Arnold et al identified negative prognostic factors to be Eastern Cooperative Oncology Group performance status ≥2, >50mm lesion size, progressive extrahepatic disease, ≥2 prior systemic therapy lines, and >50% liver involvement. For PFS, progressive disease outside the liver and liver involvement of 25%-50%, or >50%, were identified as negative prognostic factors. Health-related quality of life (HRQoL) score was generally stable or improved overall, Arnold and colleague state.
“In both cohorts of patients receiving either salvage or post-inductive/consolidation therapy, HRQoL considerations can contribute to a better understanding of patient-oriented treatment selection,” Arnold and colleagues write. “Ultimately, since irinotecan-TACE is a locoregional therapy that can be repeated for progressive or new lesions or followed up by other locoregional or systemic therapies, early response and disease control should not be neglected.”
Moreover, the authors emphasise the potential for irinotecan-TACE to be combined with other treatment strategies to “either intensify the liver-directed treatment or target extrahepatic disease”. However, randomised trials are needed to provide “robust evidence on how irinotecan-TACE can be integrated into a treatment pathway that minimises patient burden while preserving HRQoL”, Arnold et al conclude.
Shockwave Javelin Peripheral IVL Catheter, a novel intravascular lithotripsy (IVL) platform designed to modify calcium and cross extremely narrowed vessels in patients with peripheral artery disease (PAD).
Shockwave Javelin
Today, Shockwave Medical announced the US launch of its Shockwave Javelin peripheral intravascular lithotripsy (IVL) catheter, a platform designed to modify calcium and cross narrowed vessels in patients with peripheral artery disease (PAD).
PAD is the narrowing or blockage of the vessels that carry blood from the heart to the legs, reducing blood flow and affecting more than eight million people aged 40 years and older in the United States. People suffering from PAD have impaired quality of life and increased risk of heart attack or stroke.Chronic limb-threatening ischemia (CLTI) is the most advanced and serious form of PAD, impacting nearly two million patients in the US It is associated with 40% major amputations at one year and a 50% mortality rate at five years, worse than most forms of cancer.
“Physicians have faced significant challenges in tackling complex calcific lesions in narrowed peripheral vessels, and there is a growing need for more effective crossing and treatment tools,” said JD Corl, medical director of the PAD/CLTI programme at The Lindner Center for Research and Education at The Christ Hospital in Cincinnati, USA. “With proven safety and effectiveness similar to existing IVL devices, Shockwave’s new IVL platform will bring a transformative approach to our peripheral practices, enabling us to make cases more efficient and optimise outcomes for our patients living with PAD, especially those with more complex CLTI.”
The forward IVL platform is designed to modify calcium and cross calcified occlusive disease or extremely narrowed lesions where a wire will cross but devices might not. Shockwave Javelin has a working length of 150cm and features a single distal emitter that creates up to 120 shockwave pulses. Each shockwave pulse creates a spherical energy field that extends beyond the tip of the catheter. This novel design delivers lithotripsy closer to calcium than the balloon-based platform. Despite the challenging nature of the calcified lesions studied, the clinical outcomes from the FORWARD PAD investigational device exemption (IDE) trial demonstrated that Shockwave Javelin has a similar safety and effectiveness profile to balloon-based Shockwave IVL catheters, a company press release states.
“As the pioneer of IVL technology, our goal is to continue to deliver innovations that address the unmet needs of the physicians that we serve,” said Nick West, chief medical officer, Shockwave Medical. “By listening to and leveraging their valuable insights, we developed our transformational forward IVL platform with the unique capability to both modify calcium and cross extremely narrowed vessels. We are proud to be leading the charge in offering endovascular interventionalists more flexibility to address critical treatment needs and potentially reduce the risks associated with CLTI for their patients.”
Stereotaxis has announced a US Food and Drug Administration (FDA) regulatory submission for the first robotically navigated catheter designed to expand usage of robotic magnetic navigation into the broader endovascular field.
Emagin 5F is the first in a family of robotically navigated endovascular devices being developed by Stereotaxis. The Emagin brand—short for Endovascular Magnetic Intervention—will encompass a portfolio of robotic catheters and wires.
Emagin 5F is a catheter guide with a 5Fr diameter used to navigate tortuous venous and arterial vasculature. Robotic navigation of the catheter directly from the distal tip, using precise magnetic fields, is designed to enable efficient and safe navigation to otherwise difficult-to-reach vascular anatomy.
It expands the established benefits of Robotic Magnetic Navigation into multiple new clinical applications including minimally-invasive procedures used to treat stroke, cancer, and cardiovascular disease.
“Robotic Magnetic Navigation offers significant promise to address clinical challenges we face in the neurointerventional field by enabling safe and rapid navigation through tortuous vasculature,” said Timo Krings (Beth Israel Lahey Health, Boston, USA). “I’m excited by the opportunity to help pioneer this technology, evaluate and demonstrate its clinical value, and explore entirely new applications that may become possible. Our field is uniquely poised to benefit from robotics and we look forward to advancing the technology and clinical science over the coming years.”
“The evolution of robotics in interventional cardiology is inevitable and will be of significant benefit to patients, physicians, and healthcare systems,” said Kalpa De Silva (Guy’s and St Thomas’ NHS Foundation Trust, London, UK). “I see significant promise in the use of the robotically-steered Emagin catheter to enhance the safety, precision, and efficiency of various challenging procedures including renal denervation and complex percutaneous coronary interventions. I look forward to helping pioneer this technology.”
Stereotaxis submitted a 510(k) application for Emagin 5F with the FDA and expects to submit the catheter for European CE mark clearance this month. Emagin 5F was designed and is manufactured by Stereotaxis’ fully-owned subsidiary Access Point Technologies in Minnesota (USA).
Stereotaxis expects to launch Emagin 5F following anticipated approvals in the second half of this year, with a focus on demonstrating clinical value for Robotic Magnetic Navigation in multiple new endovascular applications.
“Robotic Magnetic Navigation is a platform technology that can offer significant clinical value across endovascular medicine,” said David Fischel, Stereotaxis chairman and CEO. “We are thrilled to announce this milestone as we embark on the journey to make Stereotaxis a multi-specialty robotics leader advancing clinical care in interventional cardiology, radiology and neurology.”
The HyperQure extravascular renal denervation device
The HyperQure extravascular renal denervation device
DeepQure has announced progress of clinical trials of its extravascular renal denervation device, HyperQure.
The company is actively conducting clinical trials in both South Korea and the USA, which it says demonstrate “promising” results. In South Korea, seven patients have undergone the procedure, showing meaningful reductions in blood pressure without any adverse events during- or post-operation. The company aims to complete enrolment for its Korean clinical trial within the first quarter of 2025.
In the USA, DeepQure successfully completed its first clinical case on 17 January 2025, at the University of California, Irvine (UC Irvine). The procedure, performed by Pengbo Jiang, yielded significant blood pressure reductions one month after the operation with no reported complications. The next patient is scheduled for treatment in March, with additional institutional review board (IRB) approvals secured from institutions including Mayo Clinic and Stanford University.
DeepQure’s US clinical trial spans six university hospitals, with IRB approvals finalised. The company plans to enrol 15 patients in the first half of 2025, with the ultimate goal of initiating a pivotal study by year-end to establish the safety and efficacy of HyperQure.
Beyond hypertension, DeepQure is expanding its technology to address atrial fibrillation (AF), one of the most common cardiac arrhythmias. The company has submitted an application to South Korea’s Ministry of Food and Drug Safety (MFDS) to initiate clinical trials for AF treatment.
Currently, pulmonary vein isolation (PVI) is the standard treatment for AF, but its major drawback is a high recurrence rate. DeepQure’s renal denervation technology is expected to enhance the effectiveness of PVI procedures by reducing recurrence rates, offering a breakthrough solution in a field where drug therapy has shown limited success.
Boston Scientific's global headquarters in Marlborough, USA
Boston Scientific’s global headquarters in Marlborough, USA
Boston Scientific has entered into a definitive agreement to acquire SoniVie Ltd, a privately held medical device company that has developed the TIVUS intravascular ultrasound system. An investigational technology, the TIVUS system is designed to denervate nerves surrounding blood vessels to treat a variety of hypertensive disorders, including renal artery denervation for hypertension.
The TIVUS system is designed to perform renal denervation that can help reduce activity in the kidney’s renal nerves and serve as an alternative or adjunctive therapy to medications to help regulate blood pressure. Compared to radiofrequency energy, ultrasound energy has the potential to penetrate the tissue more deeply, which may result in faster procedures with effective nerve ablation, a press release from Boston Scientific states.
“Renal denervation for hypertension is an exciting medical advancement for the millions of patients it may help and is supported by positive results from contemporary clinical trials and ongoing research,” said Lance Bates, senior vice president and president, Interventional Cardiology Therapies, Boston Scientific. “We believe the addition of the differentiated, ultrasound-based TIVUS system can complement our expansive interventional portfolio with a minimally invasive therapy for patients with hypertension and provides opportunity for future advancements in this space.”
The catheter-based TIVUS system generates precise ultrasound energy that passes through the blood and into renal arteries supplying blood to the kidneys without anchoring to the artery wall, which allows for continual blood flow to cool the treatment area.
Energy is designed to heat and ablate the bundles of nerves outside the arteries, stopping their ability to pass signals and reducing the sympathetic hormones that are released from the nerves. As a result, the blood vessels relax and the pressure within them is reduced.
Last year, SoniVie announced positive efficacy data from an investigational device exemption (IDE) pilot trial of the TIVUS system in the USA and Israel. The company recently initiated the THRIVE global IDE pivotal trial of the device.
As a strategic investor in SoniVie, Boston Scientific currently holds an equity stake of approximately 10%. Therefore, the transaction consists of an upfront payment of approximately US$360 million for the 90% stake not yet owned and up to US$180 million upon achievement of a regulatory milestone.
Boston Scientific anticipates the transaction to be completed in the first half of 2025, subject to customary closing conditions.
Cook Medical’s Zenith Alpha 2 (ZTA2) thoracic endovascular graft is now available throughout the United States. A company press release states ZTA2 is the first aortic device on the market that has evolved to accommodate CO2 flushing and has an approved flushing protocol.
The press release continues, outlining that ZTA2 is the latest iteration of Cook’s original Zenith Alpha Thoracic, built on Cook’s proven Zenith graft system and deployment technology. It has the same durability that physicians have come to rely on from the original Zenith Alpha Thoracic product, now with enhanced features.
When physicians are performing thoracic endovascular aortic repair (TEVAR) procedures, there’s a risk of introducing air bubbles into the vascular system, which can lead to severe injury to the patient, including stroke and/or death. ZTA2 offers physicians the option to flush the device with either saline alone or saline and CO2. Flushing with CO2, which is denser than air, helps to displace any remaining air within the device and minimise air emboli, thereby reducing risks to the patient.
“Cook is committed to innovating and delivering products and services in the aortic space. The company is heavily investing in our aortic strategy, and we have more exciting advancements coming in the near future,” said Johnny LeBlanc, a product director in Cook Medical’s vascular division. “With its unique indication for CO2 flushing, ZTA2 offers physicians more options for on-label procedures as part of Cook’s comprehensive portfolio of aortic products.”
In addition to CO2 flushing, ZTA2 also comes with the following advancements:
Changes to the gray positioner provide access to flush residual air spaces in the introduction system
Redesign of proximal diameter reducing suture improves conformability for larger sizes
Redesign of the bottom cap system on distal component helps avoid distal stent release failure
Since ZTA2 received US Food and Drug Administration (FDA) approval, select physicians have received early access through pre-launch partnerships with Cook. The company has congratulated Fernando Fleischman, Sukgu Han and Alyssa Pyun at Keck Medicine of USC in Los Angeles, USA for performing the first global implant of ZTA2 in January 2025.
Biotronik is partnering with Egg Medical to co-sell Egg Medical’s EggNest radiation protection systems for healthcare workers in the USA.
The EggNest Systems—EggNest XR, EggNest Protect & EggNest Complete—are radiation protection platforms that can be used across a wide variety of fluoroscopy procedure types without impacting workflow.
The EggNest Systems are the only products commercially available in the USA able to protect everyone in the interventional suite, the companies said in a press release. Radiation reductions of up to 97% are possible with EggNest XR and EggNest Protect, and up to 99% reductions are possible with EggNest Complete.
“Partnering with companies like Egg Medical in the radiation protection space allows Biotronik to bring our vision of ‘Excellence for Life’ to healthcare professionals as well as their patients. These products will allow us to bring a safer environment to every member of the EP lab, cath lab, and other procedure suites,” said Matt Roberts, vice president, National and Corporate Accounts at Biotronik.
“We are thrilled to partner with Biotronik, who has been focused on providing radiation protection to their customers for many years. This partnership expands our ability to provide protection for everyone in the procedure room across the USA,” said Gavin Philipps, chief commercial officer at Egg Medical.
Teleflex has today announced it has entered into a definitive agreement to acquire Biotronik’s Vascular Intervention business.
The acquisition reflects Teleflex’s commitment to investing in the estimated US$10 billion interventional cardiology and peripheral vascular market. A company press release states that the acquired business will expand the Teleflex portfolio to include a broad suite of vascular intervention devices such as drug-coated balloons, drug-eluting stents, covered stents, balloon and self-expanding bare metal stents, and balloon catheters.
“We are excited to announce the acquisition of Biotronik’s Vascular Intervention business, which we anticipate will significantly enhance our global presence in the cath lab, expand our suite of innovative technologies, and improve patient care” said Liam Kelly, chairman, president and chief executive officer of Teleflex.
“We believe the acquisition will allow us to position this advanced coronary portfolio alongside our existing Interventional business and establish our global footprint in the fast-growing peripheral intervention market. In particular, the acquired coronary products will be highly complementary to our well-established complex percutaneous coronary intervention (PCI) platform and expand and enhance the legacy Interventional salesforce and offerings by combining existing Teleflex access products with the Vascular Intervention therapeutic devices.
The acquired business is rooted in robust research and development, clinical expertise, and global manufacturing capabilities, which we believe will further bolster Teleflex’s innovation pipeline, and position the company to participate in the emerging potential for resorbable scaffold technologies. We believe the acquired business will be a meaningful contributor to our growth in the coming years, diversify our geographic revenue mix with 50% of the acquired revenues generated in Europe, the Middle East and Africa, and provide additional scale for investment into innovation.”
The company states that the acquisition of the Vascular Intervention business will also allow Teleflex the opportunity to invest in and expand the clinical trial programme for Biotronik’s Freesolve, a sirolimus-eluting resorbable metallic scaffold (RMS) technology, including possible pursuit of the US market. Freesolve, which received its CE mark in February 2024, is indicated in CE-mark accepting countries for de novo coronary artery lesions.
The combination of temporary scaffolding with drug delivery is anticipated to address the current trend in interventional coronary and endovascular procedures toward leaving behind less permanent hardware. As demonstrated in the BIOMAG-I study, Freesolve RMS demonstrated resorption after 12 months, a target lesion failure rate comparable to contemporary drug-eluting stents, and no definite or probable scaffold thrombosis. The European pivotal BIOMAG-II study is now enrolling.
As the interventional cardiology and peripheral intervention markets grow on a global basis, Teleflex anticipates that this acquisition will enhance its offerings to cardiac and peripheral care specialists, while significantly advancing its corporate growth objectives.
GE HealthCare has today announced that Yihao Zhang, president and chief executive officer (CEO), China, will retire from the company effective July 1, 2025. Will Song, past chairman of Johnson & Johnson China and global senior vice president of Johnson & Johnson Medical China, has been named GE HealthCare’s new president and CEO, China, and will join the company on April 1, 2025, ahead of leading the region starting July 1 following Yihao’s departure.
A company press release states that Yihao’s planned retirement allowed GE HealthCare to purposefully identify and prepare a qualified successor in Will, an exceptional leader with a strong track-record and the right skillsets to help deliver the company’s local strategy.
The press release continues, outlining that, since joining GE HealthCare in 2019, Yihao has been responsible for GE HealthCare’s strategic development and operations in China, driving the company’s long-term growth in the market. He has redefined the company’s localisation, innovation and partnership strategy in China, establishing a clear blueprint for long-term growth in the region. His efforts in developing and promoting industry-leading localisation have been critical in transforming the industry and helping the company navigate in the highly evolving, policy-driven and competitive market. He also doubled innovation investment within five years and expanded the company’s manufacturing footprint in Beijing, Wuxi, Tianjin and Shanghai and built two new manufacturing sites in Chengdu and Shenzhen.
“Yihao has proven himself to be a humble, energetic, people-focused leader who embraced our company culture, strategy and purpose. He has made an indelible mark on our colleagues and the industry,” said Peter Arduini, president and CEO, GE HealthCare. “I want to personally thank Yihao for his leadership and contributions through the years, and for positioning GE HealthCare as a leading innovator in China. I wish him a healthy and happy retirement. Looking ahead, I am confident that Will’s stellar reputation and in-depth knowledge of the China market, along with his robust relationships with key stakeholders and deep understanding of our customer base, will help enhance our position in China and move the region forward to effectively deliver on the future of healthcare.”
GE HealthCare has recently launched Freelium, a sealed magnet platform that aims to enable high-quality magnetic resonance (MR) imaging with less than 1% of helium used in conventional magnet technology to help support diagnostic accuracy and sustainability goals, a company press release states.
The platform is set to launch at the European Congress of Radiology (ECR; February 26-March 2, 2025, Vienna, Austria). Freelium marks the evolution of GE HealthCare’s established lightweight intelligent platform magnet technology, which was first introduced in 2020.
Freelium is designed to reduce liquid helium usage without compromising power efficiency and operational security. To maintain power efficiency, Freelium aims to operate with no additional cooling and power requirements. Additionally, the company states that the platform’s intelligent sensor technology intends to remotely monitor the MR system and enable automated magnet protection and recovery capability without the need for field engineer intervention. This is particularly important in the event of power outages or disruptions caused by natural events.
To support diagnostic accuracy and confidence, Freelium aims to uphold GE HealthCare’s advanced quality and performance standards. The platform also will be optimised to be compatible with GE HealthCare’s leading AI-enabled solutions. Freelium magnets will be able to be transported and installed in hospitals and in markets where access to helium is limited and without significant helium loss during transport, enhancing patient access to care.
“The unveiling of Freelium reinforces our commitment to provide equitable and sustainable access to MR to any patient and user, while maintaining imaging performance and ensuring seamless operational security for our customers,” said Kelly Londy, president and chief executive officer of Global MR at GE HealthCare. “We’re excited about Freelium’s compatibility with AI-enabled solutions and ability to unlock the full potential of deep learning applications for enhanced diagnostic insights in the future.”
Stryker recently announced that it has completed the acquisition of Inari Medical. A press release notes that the addition of Inari brings an established peripheral vascular position to Stryker in the fast-growing venous thromboembolism (VTE) segment.
“The acquisition of Inari Medical marks a significant milestone in expanding our interventional endovascular portfolio,” said Kevin Lobo, chair and chief executive officer, Stryker. “We look forward to welcoming the talented Inari team to Stryker and working together to improve outcomes for patients worldwide.”
The company states in a press release that Inari’s product portfolio is “highly complementary” to Stryker’s neurovascular business and includes two novel mechanical thrombectomy solutions—the FlowTriever system for the treatment of pulmonary embolism and the ClotTriever system for thrombectomy in the peripheral vessels—as well as emerging therapies.
Emboa Medical has announced a novel microstructured catheter which mimics the snake’s evolutionary advantage to improve the retrieval of blood clots that cause stroke.
The company has stated that the catheter has been validated to improve outcomes for stroke patients. Its patent-pending platform, called TRAP, or Thrombus Retrieval Aspiration Platform, emulates a boa constrictor’s teeth arrangement in its biomimetic design to grab onto blood clots without tearing them.
Chief executive officer of Emboa Medical Ángel Enríquez has commented that the TRAP design demonstrated a greater than 200% increase in blockage removal force compared to a traditional catheter.
“Additionally, the TRAP catheter showed significant benefits in removing clots on the first attempt in a worst-case neurovascular model,” he said. “It achieved a 40% success rate compared to 10% for conventional smooth inner diameter catheters.”
Emboa Medical was founded by clinical experts at Goodman Campbell Brain and Spine in Carmel, USA and NYU Langone Health in New York, USA and medical device researchers at Purdue University’s College of Engineering in West Lafayette, USA. TRAP was designed by Enríquez and Hyowon Lee, professor at Purdue’s Weldon School of Biomedical Engineering and director of the Center for Implantable Devices.
Enríquez said Emboa has been diligently working on finalising the design of the microstructures through physiologically relevant models to further establish differentiation among current catheters in the market.
“We have conducted in vitro experiments that quantitatively demonstrate the advantages of TRAP catheters,” he said. “Additionally, we will conduct an in vivo porcine model study and preliminarily validate TRAP’s safety and effectiveness by end of the first quarter of 2025. The successful completion of this animal model study will lead to more functional and robust TRAP devices that can facilitate the transition to larger-scale verification activities toward regulatory approval.”
“The use of traditional stent retrievers results in higher rates of perforation due to the metal struts interacting with the vessel walls. This causes intracranial haemorrhages at a higher rate than aspiration catheters, which apply suction through a tube. This can be asymptomatic or symptomatic, but the truth is no doctor is comfortable causing damage to a patient’s blood vessels,” Enriquez said.
“Thus, aspiration catheters are an attractive tool because they achieve reported faster reperfusion times, lower rates of distal emboli (13.2% versus 3.4%) and vessel injury (9.3% versus 1.8%) at lower costs. Yet the aspiration force is dramatically decreased and limited by the smaller vessel diameter. TRAP was designed to address this obstacle.”
Critical challenges in open and endovascular treatment of aortic disease will be brought into focus when world leaders in cardiac, aortic, and vascular therapies return to London this spring for the 47th annual Charing Cross (CX) Symposium 2024 (23–25 April, London, UK).
CX, the world’s largest vascular meeting, has a three-year cycle of raising vascular and endovascular controversies to challenge the available evidence and reach a consensus after discussion with an expert audience.
“The highlight this year is challenges, and we have challenges in clinical practice in aortic care every day,” CX co-chair Dittmar Böckler (University Hospital Heidelberg, Heidelberg, Germany) tells Cardiovascular News, looking ahead to the highlights on the aortic programme in 2025. “We need evidence, we need teaching, we need technical skills and tips and tricks, [and] all this will be provided by a really outstanding programme with key opinion leaders in the field of aortic disease and aortic care.”
The CX 2025 programme has sessions touching upon all vascular domains, spanning aortic, peripheral, venous, acute stroke and vascular access. The aortic pillar of the programme offers attendees insights from 119 presentations, augmented by 11 edited cases, with new data set to be brought to light in 12 podium first presentations, alongside debates on five hotly contested issues. There will also be opportunities for attendees to translate theory into practice through a series of hands-on workshops running throughout the three days.
Aortic techniques and technologies will be the focus on day one, with Böckler highlighting a case involving the treatment of a thoracoabdominal aneurysm using a four-inner-branched device as one to look out for. “We need off-the-shelf devices to treat these emergent and urgent patients, as customised devices are not available. How to handle those devices, how to implant them, [and] what the evidence is so far is the focus,” he says of the case.
Turning to the highlights among the many podium first presentations featuring at CX 2025—with more than 50 across the full programme—Böckler mentions the SUNDAY trial, a randomised trial looking at treatment options for uncomplicated type B aortic dissection (TBAD), as being of particular importance. “We have a lack of evidence there, and we are going to have the first insight into early outcomes of this trial,” he comments. Other podium first presentations include data on the impact of blood pressure on abdominal aortic aneurysm (AAA) growth rates, risk stratification after endovascular aneurysm repair (EVAR), a multicentre study on physician-modified endografts for very large and urgent complex AAA, and more.
The use of artificial intelligence (AI) in patient evaluation is among the “disruptive” technologies featuring alongside topics that impact daily clinical practice such as sarcopenia, the risk of abdominal cancer after EVAR, the use of proteomics to predict sac shrinkage after EVAR and quality-of-life assessment following vascular care.
“Something we have really neglected for years, in my mind, is quality-of-life assessment after vascular care, specifically in TBAD,” explains Böckler. “Many patients get conservative treatment, but we didn’t pay attention to their psychological status, how they behave, how they feel, so quality of life is something very new. And that’s in the programme of the aortic sessions this year.”
Among other highlights, Gustavo Oderich (University of Texas Health Science Center at Houston, Houston, USA) will deliver the inaugural Roger M Greenhalgh memorial lecture, speaking on the challenges of 21st century aortic education, innovation and evidence. Citing this as one of the event’s must-attend presentations, Böckler says that the talk will continue CX founding chair Roger Greenhalgh’s legacy of advocating for the best medical education for the optimal care of patients with vascular disease.
“The unique and special thing about Charing Cross is the style of discussion”
“The unique and special thing about Charing Cross is the style of discussion,” Böckler adds, paying tribute to another of Greenhalgh’s CX legacies. “We have a one-to-one relationship between presentations and discussions. I love the discussion culture at Charing Cross. This makes it unique and special. We have a special style, a special atmosphere. Everybody can go to the microphone, ask questions, and you will get excellent answers from the leading physicians of the world.”
Attendees can join world-leading experts in the management and treatment of aortic disease from the cardiovascular, vascular and endovascular worlds who are participating in 2025 including CX aortic executive board members Oderich, Tilo Kölbel (University Heart Center Hamburg, Hamburg, Germany), Joseph Bavaria (University of Pennsylvania, Philadelphia, USA), Alexander Zimmermann (University Hospital Zürich, Zürich, Switzerland), Aung Oo (St Bartholomew’s Hospital, London, UK). Registration and programme details for CX 2025 can be found online at cxsymposium.com.
A new guideline from the American Society of Echocardiography (ASE) aims to provide more detail for clinicians performing ultrasound-guided vascular cannulation.
The new document provides expert consensus on the best practices and techniques for using ultrasound in vascular access procedures.
“Ultrasound guidance is currently not a standard of care for all vascular access, but it is becoming increasingly common in daily clinical practice due to its ability to enhance success rates and reduce complications,” says lead co-author Annette Vegas, an anesthesiologist and director of Perioperative Echocardiography at Toronto General Hospital (Toronto, Canada). “Adopting the recommendations in this guideline will help clinicians better minimise risks, maximise technical competencies and ultimately, improve patient outcomes.”
The guideline uses descriptions, diagrams and ultrasound images to explain the general aspects of anatomic and ultrasound imaging of vessels, ultrasound-guided vascular cannulation techniques, and the identification of local vascular cannulation complications. Additionally, it emphasises the fundamental roles of ultrasound during vascular access, including: pre-cannulation vessel assessment, dynamic ultrasound guidance, and identification of local complications.
Guerbet has announced that the US Food and Drug Administration (FDA) has granted Breakthrough Device designation to Lipiojoint, the company’s transient liquid embolic agent designed to alleviate pain and the related burden of reduced mobility in patients with knee osteoarthritis (OA).
This recognition highlights the potential of Lipiojoint as a minimally invasive and targeted approach for knee OA patients who have not found relief through non-surgical treatment modalities.
“Being part of the Lipiojoint FDA Breakthrough programme is a major milestone for Guerbet but most importantly for patients suffering from osteoarthritis. Working closely with the US administration will give a unique opportunity to bring an innovative approach aiming to release pain for a large part of the population. A unique collaboration for a medical unmet need” said Dan Raffi, global chief commercial officer and president for Gubert France.
An 11-year prospective study of magnetic resonance (MR)-guided cryoablation in the treatment of recurrent cancer in the prostate bed has demonstrated “significant” prostate-specific antigen (PSA) reduction at both six- and 12-month follow-up.
Sotoudehnia began by outlining current treatment options and their associated recurrence rates, stating that surgery is estimated to have a recurrence rate of between 15–20%, radiation 20–30%, and hormone therapy, which has a two-to-three-year efficacy rate. Of available focal therapies, the speaker listed cryoablation and laser ablation.
In order to evaluate the efficacy and safety of MR-guided cryoablation in this patient population, Sotoudehnia and colleagues enrolled 90 patients between September 2011 and September 2023. The patients had a mean age of 73 years and had previously received radiation therapy or prostatectomy.
Patients in the study cohort were treated with four cryoablation needles on average, typically with three freeze/thaw cycles and a urethral warmer for protection during the procedure. Sotoudehnia stated that their team carefully monitored ice ball expansion via magnetic resonance imaging (MRI) to ensure target coverage.
At three and six months post-ablation, patients were assessed via PSA and prostate-specific membrane antigen (PSMA) positron emission tomography (PET) imaging. Urinary symptoms and sexual health were measured using the American Urological Association Symptom Score (AUASS) and the Expanded Prostate Cancer Index Composite (EPIC).
Sharing the team’s results with the SIO 2025 audience, Sotoudehnia stated that average lesion size was 1.3cm and mean pre-ablation PSA was 3.57±4.38. Following treatment, average PSA levels “significantly decreased”—at six months, average PSA fell to 1.41±3.70, a 60.5% reduction, and at 12 months, PSA was reported as 1.52±4.88, a 57.5% reduction on pre-ablation assessment.
“PSA reduction was maintained through to 12-month follow-up,” Sotoudehnia stated. “Overall, we had 34 of 90 patients show recurrence, and only 12 patients who experienced recurrence within the ablation zone.” The speaker reported that 22 patients experienced out-of-field recurrence, developing new lesions outside of the original treatment area.
Sotoudehnia then detailed a subgroup analysis carried out by their team, evaluating alternative treatments and their recurrence rates in this patient population. The analysis showed that in-field recurrence rates were highest when patients were treated with combined prostatectomy and radiation (13.9%), while radiation alone (13.5%) and prostatectomy (11.7%) showed lower rates of recurrence.
The speaker noted that they observed a 4% complication rate in this cohort, which included three patients who experienced a breakdown of the posterior urethral wall. Two of these patients had received prostatectomy and radiation combined, while one patient had received radiation alone. Further, another patient with a history of prostatectomy reportedly experienced vesicorectal fistula, Sotoudehnia explained.
Sotoudehnia summarised that their data shows cryoablation to be effective in reducing PSA in patients with recurrent prostate cancer. On reflection, she noted that “cryoablation gives us superior soft tissue resolution for targeting and monitoring,” stating that the modality helped her team achieve minimal in-field recurrence rates in these patients.
Akura Medical has announced today the first patient enrolment in the QUADRA-PE study evaluating the Katana thrombectomy system in patients with acute pulmonary embolism (PE). The initial procedure was successfully performed by Samuel Horr, director of cardiovascular research at TriStar Centennial Medical Center in Nashville, USA.
“TriStar Centennial is thrilled to be a part of research trials that hold the potential to deliver better care to patients,” commented Horr. “With this trial, the hope is to provide physicians with continuous, real-time pulmonary artery pressure readings throughout the entire procedure to streamline the removal of the blood clot.”
“One of the biggest challenges in thrombectomy procedures for PE is determining when you’ve successfully removed the thrombus entirely, as incomplete removal can may lead to suboptimal outcomes,” said Sanjum Sethi (Columbia University Medical Center, New York, USA) co-principal investigator for the QUADRA-PE trial. “The Katana System’s display of real-time pressure data represents a significant advancement, providing physicians with clinically useful insights during the procedure.”
A recent press release shared by the company has stated that the Katana system includes:
A bidirectional, low-profile sheath designed to facilitate smoother navigation in complex vasculature and enable contrast injection without requiring catheter exchanges.
High velocity saline jets that are engineered to effectively break up clots independent of morphology and prevent catheter clogging for procedural efficiency.
Sensors that provide real-time pulmonary artery pressure data to provide insights into procedure progress.
The Sentinel console, which displays clot engagement and blood loss to inform the physician and to potentially minimise uncertainty.
“Pulmonary embolisms can be life-threatening and demand swift and effective intervention. Meaningful strides have been made in the thrombectomy landscape, but challenges remain in navigating complex vasculature and simplifying decision making,” said Ann Gage (TriStar Centennial Medical Center, Nashville, USA), co-principal investigator for the QUADRA-PE trial. “I am incredibly excited to be involved in this study as it represents a significant milestone in the forward trajectory of pulmonary embolism treatment.”
The QUADRA-PE study is a multicentre, international trial designed to enrol up to 118 patients with clinically significant acute PE, at up to 26 sites globally. The primary effectiveness endpoint is the reduction in right ventricular/left ventricular (RV/LV) ratio from baseline to 48 hours post-procedure as assessed by CT angiography. The primary safety endpoint is the composite rate of major adverse events (MAEs) within 48 hours post-procedure.
Surmodics has announced the successful early clinical use of its Pounce XL thrombectomy system. The device received US Food and Drug Administration (FDA) 510(k) clearance in September 2024, and is currently in limited market release (LMR), with full commercial launch planned following completion of the LMR.
A press release notes that Surmodics Pounce thrombectomy systems are intended for the non-surgical removal of thrombi and emboli from the peripheral arterial vasculature. The new Pounce XL thrombectomy system is indicated for use in vessels ranging from 5.5–10mm in diameter, sizes typical of iliac and femoral arteries. The Pounce XL system complements the Pounce and Pounce LP thrombectomy systems, which are indicated for 3.5–6mm and 2–4mm vessels, respectively.
Walter Rizzoni (University of Pittsburg Medical Center [UPMC] Hamot, Erie, USA) successfully used the new Pounce XL thrombectomy system to restore blood flow in a thrombosed stent graft 8mm in diameter. This marks Rizzoni’s first case using the device at UPMC Hamot.
“The Pounce XL thrombectomy system removed a significant amount of chronic material during our first use,” said Rizzoni. “In that respect, its performance was right in line with our experience using the Pounce and Pounce LP systems.”
“We’re excited about the positive feedback we’ve received from early users of the Pounce XL system,” said Gary Maharaj, president and chief executive officer of Surmodics. “The addition of this larger-profile device to the Pounce thrombectomy platform fulfils our goal of providing physicians a standalone solution for rapid removal of acute or chronic peripheral arterial clot throughout the lower extremity. With hospitals under growing pressure to reduce costs, we believe the standalone Pounce thrombectomy platform may help reduce the need for hospitalisations and follow-up procedures.”
A press release notes that Serranator SL-PRO utilises Cagent’s proven serration technology on a redesigned platform, offering improved deliverability and trackability, while offering Serranator’s proven 1,000 times increase in point force versus plain balloon. The release adds that Serranator SL-PRO’s innovative mechanism of action allows for predictable and controlled lumen gain with minimal dissection.
Michael Lichtenberg (Arnsberg Clinic, Arnsberg, Germany) commented: “As an experienced Serranator operator, my team has grown accustomed to the benefits of serration, including great lumen gain, low complication rate, and low 6% BTK [below-the-knee] vessel recoil vs. 55% measured recoil with plain balloon.”
Lichtenberg continued: “We also appreciate Serranator’s ability to safely and effectively treat complex disease, even down into the pedal arteries. With SL-PRO, we’re eager to experience the advantages of serranation in this new, more deliverable platform.”
Cagent Vascular chairman and chief executive officer Brian Walsh added: “We are committed to consistently developing and advancing solutions for physicians treating PAD [peripheral arterial disease] patients, and winning the fight against this debilitating disease. With over 20,000 procedures now completed and a growing library of clinical data, Serranator has proven itself to be a valuable tool in this fight. The Serranator SL-PRO is a purpose-built tool for pedal intervention, and with it, the Serranator product family can now treat from hip to toe.”
Cagent Vascular advises that the Serranator and Serranator SL-PRO PTA serration balloon catheters are US Food and Drug Administration (FDA)-cleared, novel balloons using proprietary stainless steel micro-serration technology, designed to create linear, interrupted scoring along the endoluminal surface. “With 1,000x more point force compared with plain balloon angioplasty, serration occurs during slow-and-low balloon inflation and is designed to aid arterial expansion, effectively achieving luminal gain in all lesion morphologies,” the company explains.
New data from a prospective, multicentre randomised controlled trial show similar hepatic progression-free survival (hPFS) using bland transarterial embolization (TAE) or transarterial chemoembolization (TACE) when treating neuroendocrine tumour metastases in the liver. Michael Soulen (University of Pennsylvania, Philadelphia, USA) presented these findings at the Society of Interventional Oncology (SIO) annual scientific meeting (30 January—3 February, Las Vegas, USA).
Soulen, for the first time, was presenting the results of the the Randomized Embolization Trial for NeuroEndocrine Tumor Metastases to the Liver (RETNET). He set out that TAE and TACE have been used to treat neuroendocrine liver tumours for over 50 years and are equally weighted in the National Comprehensive Cancer Network (NCCN) guidelines, due only to lack of controlled comparative data.
To gain better insight, RETNET was designed to analyse efficacy, toxicity and patient-reported outcomes for patients with liver-dominant neuroendocrine tumours randomised 1:1:1 to TAE with 40–500μm microspheres, TACE with lipiodol-docorubicin 40–500μm microspheres, and drug-eluting bead doxorubicin (DEBDOX) delivery. Patients received clinical, imaging and laboratory assessment, as well as patient-reported outcome assessments, every three months for two years following treatment.
Highlighting strict safety parameters in their study’s design, Soulen commented on “controversy” that had previously arisen during trials of DEBDOX which were halted early due to high complication rates. To acknowledge this, his team implemented a stopping rule which defined a 20% incidence of major complications to be grounds to close an arm.
Soulen and colleagues enlisted 14 sites in the USA, Canada, Argentina and Italy, with a total of 162 patients enrolled. He described that, during an early safety review while enrolling, they elected to close the DEBDOX arm due to a 40% treatment-related serious adverse event rate resulting in two intensive-care unit admissions, two permanent hepatobiliary injuries and two patients who could no longer participate in the trial.
“The good news is that we confirmed that DEBDOX is bad in neuroendocrine tumours,” Soulen told SIO attendees, a fact that has now been reflected in the NCCN guidelines. Going forward, their cohort was comprised of 78 patients randomised to TAE and 73 to TACE, with no significant baseline characteristic differences between groups, he stated.
Soulen reported that hPFS at two-year follow-up showed no difference (p=0.2) between TAE and TACE. Further, breaking hPFS down by grade, tumour burden, Eastern Cooperative Oncology Group (ECOG) performance status, and histology, Soulen and his team reported equivalent results between study arms.
His team analysed each arm by objective response rate (ORR), demonstrating TACE to have achieved a 40% ORR at three months which was sustained to two years, while TAE achieved a 60% ORR at three months, which “significantly declined” over two years to 20%, Soulen described.
Detailing unexpected insights from their data, Soulen stated that syndromic and female patients had better hPFS than non-syndromic patients or men. “This was very interesting and unexpected, and this is an outcome that still remains to be explored,” Soulen told delegates.
The speaker additionally reported a total of 101 severe adverse events in the TAE arm, versus 39 in the TACE arm—a large difference in event rate between groups which is awaiting detailed further analysis.
Summarising, Soulen stated TAE and TACE equally provided durable symptom control up to two years which was not influenced by tumour grade, burden or histology. Later, when asked where they go next by an audience member at his SIO 2025 talk, Soulen noted that further analysis of their data is set to be released in due course, focusing on overall survival and patient-reported outcomes.
“[These outcomes] are raising a lot of questions that were unexpected. I don’t know the answer, but we will need to pick apart these data in the context of these questions,” Soulen concluded.
The Society of Interventional Oncology (SIO) has announced the launch of a new research database and educational initiative, the Clinical Trial Collaborative (CTC).
The launch of this initiative was announced today at the SIO (30 January—3 February, Las Vegas, USA) annual scientific meeting. The CTC features a principal investigator (PI) online certificate course and a first-of-its-kind, searchable directory of interventional oncology (IO) and interventional radiology (IR) investigators, including relevant trial site information and available resources to support clinical study development and execution.
The development of the CTC addresses a critical need in the IO field for research education and an organised research community for qualified investigators to explore and access site-specific resources for conducting trials, meeting enrolment requirements, completing protocol endpoints, and maintaining compliant research practices. The database is expected to become available for industry subscription and access by 2026.
“The Clinical Trial Collaborative is the first of its kind and will provide the community an infrastructure to advance science as well as advance the technologies and clinical treatments for the betterment of patient care,” said SIO president Muneeb Ahmed (Beth Israel Deaconess Medical Center, Boston, USA). “SIO is answering an unmet need to train, develop, and provide a community to bring together all those practicing within the interventional oncology field.”
The SIO has stated that the CTC directory will provide the foundation for a robust clinical site network. The PI certificate course is geared towards early-career professionals looking to advance their experience in clinical research, as well as industry members and fellow IO physicians and researchers looking for qualified sites who share similar research interests to enrol patients in their specific trial.
“The development of the Clinical Trial Collaborative is a multi-layered effort by SIO to grow a clinical trial base of qualified investigators and sites for industry or investigator sponsored trials,” said SIO research advisor Michael Soulen (University of Pennsylvania, Philadelphia, USA). “Partners will identify sites for multicentre trials and, with the SIO training, have a level of confidence that the individuals in those instances understand how to be study collaborators and conduct studies to successful completion.”
Instylla has announced the US Food and Drug Administration (FDA) 510(k) clearance of the Tembo embolic system.
According to the company, Tembo is a bioresorbable embolization agent composed of irregularly shaped, dry-gelatine particles of a size range from 85 to 255µm. These particles are designed for the embolization of hypervascular tumours and blood vessels to occlude blood flow in the peripheral vasculature.
“We hope that this innovation in short-term absorbable embolics, characterised by its irregular shape, easy preparation and use, high visibility, and capacity to pack treated vessels densely, will potentially address the limitations associated with currently available permanent spherical embolics,” commented Venkatesh Krishnasamy (University of Alabama at Birmingham, Birmingham, USA) in the company’s press release. “The Tembo embolic also has the potential to play a key therapeutic role in various other clinical applications and vascular territories.”
Krishnasamy is director of interventional oncology and interventional research and associate professor at the University of Alabama in Birmingham, Alabama.
Additionally, Amar Sawhney, chief executive officer of Instylla and managing director of Incept stated: “We are excited to achieve 510(k) clearance for the Tembo embolic system and eagerly anticipate introducing this product to the US market. We plan to collaborate with leading experts in interventional radiology to maximise the clinical benefits of the Tembo embolic system. While our primary focus continues to be the completion of the premarket approval process for our flagship product, Embrace hydrogel embolic system, we pride ourselves on providing novel resorbable embolic agents to interventional radiologists specifically designed for new and existing embolotherapies.”
The TRIBUTEstudy, a multimillion-dollar project, is also the second multi-industry supported clinical study to be executed by the society since its first announcement of the ACCLAIM trial in 2021.
TheTribute study is collectively supported by the study’s exclusive pioneer trial partner Varian, a Siemens Healthineers, the study’s catalyst trial partner, Stryker, and the study’s advocate trial partner, Boston Scientific.
This is the first prospective, multicentre study to evaluate real-world outcomes (e.g., pain, patient reported outcomes, skeletal related events, healthcare utilisation) in adult patients treated with both percutaneous ablation and palliative radiation therapy (RT) for symptomatic, high-risk metastatic bone lesions. The study was collaboratively designed and developed with the partnership of radiation oncology, which SIO sees as a critical multidisciplinary partner to the success of the study.
The Tribute study clinical leadership will include Jack Jennings (Washington University School of Medicine, St. Louis, USA) Sean Tutton (University of California, San Diego, USA), Clifford Robinson (Washington University School of Medicine, St. Louis, USA) and James Urbanic (University of California, San Diego, USA). “The results from the Tributetrial have the potential to reshape treatment guidelines for metastatic bone disease. Research is the cornerstone of progress in interventional oncology, and SIO remains committed to driving ground-breaking efforts that elevate the impact of clinical research in our field,” said Jennings.
Percutaneous ablation and RT have different mechanisms of alleviating pain and causing tumour death that may work synergistically. Radiation therapy is a widely accepted treatment for painful bone metastases and provides palliation of pain for patients. Percutaneous ablation, a minimally invasive therapy for painful metastatic bone disease, can be performed with thermal modalities (e.g., radiofrequency, microwave, cryoablation) and requires minimal recovery. “This approach combines the strengths of both percutaneous ablation and radiation therapy. By leveraging their complementary mechanisms, we can offer patients an effective and minimally invasive treatment option for pain relief and tumour management in metastatic bone disease,” said Tutton.
Muneeb Ahmed (Beth Israel Deaconess Medical Center, Boston, USA), president of the SIO commented: “The success of studies like Tributeare fuelled by strong, long-term collaborations with our multidisciplinary physician colleagues and dedicated industry partners. We deeply value the ongoing commitment of our industry partners, whose investment is vital to advancing these critical research areas. The Tributestudy is not just a step forward—it’s a bold leap in SIO’s vision to further establish the interventional oncology specialty, setting an ambitious pace for the entire field to follow.”
The Tributestudy is set to launch in 2025 with the enrolment of 120 subjects across sites in the USA.
Pending the results of several trials and “iterative changes” to device design, bioabsorbable scaffolds are set to change the treatment paradigm for lower extremity peripheral arterial disease (PAD) within the next decade. So concluded Eric Secemsky (Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, USA) during a presentation at the Leipzig Interventional Course (LINC 2025; 28–30 January, Leipzig, Germany).
Secemsky was speaking on the future of bioabsorbable scaffolds, providing an overview of the key features of this “ideal” device type for the treatment of below-the-knee (BTK) disease. The first characteristic is drug elution, he noted, which inhibits restenosis and provides drug-modulated healing for sustained patency; second, a scaffold design provides transient support in the vessel and addresses recoil and dissection; and finally, resorbability ensures nothing is left behind.
“The era of bioabsorbable scaffolds has really begun with the Esprit drug-eluting resorbable scaffold (DRS),” Secemsky commented, noting that this Abbott innovation “is what created the market in the USA”. Esprit DRS is the first device of its kind to receive approval from the US Food and Drug Administration (FDA), the presenter shared, highlighting positive data from the prospective, multicentre, randomised LIFE-BTK trial that now has results available out to two years.
Secemsky stressed, however, that the technology is still in its infancy. The Esprit BTK device is “only the first step on a long pathway to solving BTK interventions for both US and non-US patients,” he told the LINC audience.
Here the presenter listed a number of other devices with bioabsorbable properties that are being evaluated in the USA, focusing in particular on the Motiv (Reva Medical) and Magnitude (R3 Vascular) scaffolds.
The Motiv device, Secemsky detailed, is CE mark approved, has been granted FDA breakthrough designation, and is currently being assessed in the recently completed MOTIV BTK randomised controlled trial. Led by Ehrin Armstrong (Adventist Heart and Vascular Institute, St Helena, USA) and Andrej Schmidt (University of Leipzig, Leipzig, Germany), the trial enrolled its target cohort of 292 patients across 35 centres in the USA and Europe and is awaiting completion of follow-up.
“We saw results of their early postmarket trial in the EU looking at 60 limbs, 58 patients, and [the device] demonstrated really impressive patency outcomes through three years,” Secemsky shared. Continuing, the presenter stressed the significance of this result: “It’s hard for a BTK device in vessels that are less than 3.5mm to maintain 88% patency through 36 months.”
Moving on to Magnitude, Secemsky disclosed that he is the co-principal investigator for the US pivotal trial of this device. “[Magnitude] is really as resistant to compression and supportive as a metallic stent, but has unique flexibility to optimally perform in challenging anatomical locations,” Secemsky noted, also pointing out the device’s ability to “maintain its structure in a compromised situation, including in the infrapopliteal space”.
The results of early feasibility study RESOLV I, Secemsky shared, were “very supportive of moving forward to an IDE [investigational device exemption] trial”. In total, he noted that 36 lesions in 35 limbs were treated in this trial with >90% freedom from occlusion or restenosis, which included “really impressive real-world patien t and lesion characteristics”.
“Bioabsorbables have the promise to change clinical practice for infrainguinal arterial disease,” Secemsky posited, drawing his presentation to a close.
The presenter continued, considering timelines: “As iterative changes allow for longer scaffold lengths, larger diameters and consistent tensile strength, the treatment paradigm for lower extremity disease may look much different in the next five to 10 years.
“I think we’ll continue to have these conversations over the years, see more data, and I think we’ll see many of these scaffolds make it to clinical practice.”
AMBITION BTK is a multicentre, randomised controlled trial (RCT) designed to evaluate the clinical outcomes of the Auryon atherectomy system in combination with standard balloon angioplasty compared to standard balloon angioplasty alone for the treatment of infrapopliteal lesions in patients with CLTI. The trial will enrol up to 200 patients across up to 30 hospital-based sites. Additionally, up to 1,500 patients treated with the Auryon atherectomy system at the same sites who do not meet the eligibility criteria of the RCT will be enrolled in a companion registry.
“We are dedicated to expanding innovative treatment options for peripheral arterial disease, particularly in challenging cases like below-the-knee lesions,” said Juan Carlos Serna, AngioDynamics senior vice president of scientific and clinical affairs. “The AMBITION BTK RCT and registry represent an important advancement in evaluating the clinical benefits of the Auryon atherectomy system. Physicians have expressed strong interest in the platform’s unique capabilities, and we are eager to demonstrate further its potential to improve outcomes for patients with chronic limb-threatening ischaemia.”
A press release notes that the Auryon laser can be used to treat all infrainguinal lesion types, including above-the-knee (ATK), BTK and in-stent restenosis (ISR) and to date, it has been used to treat more than 100,000 patients in the USA and worldwide.
“With the global rise in diabetes, we are seeing a growing number of patients with severe tibial disease,” said AMBITION BTK co-principal investigator Anahita Dua (Massachusetts General Hospital and Harvard Medical School, Boston, USA). “In the USA, treatment options for below-the-knee lesions remain limited, often relying primarily on plain balloon angioplasty. These patients frequently present with tibial disease that can extend throughout the entire vessel. An innovative tool like the Auryon laser, which can restore laminar flow, could be a gamechanger in their care.”
AMBITION BTK builds upon the positive outcomes of a prior multicentre, prospective trial that evaluated the safety and effectiveness of the Auryon laser atherectomy system in treating BTK lesions in patients with limb ischaemia. The earlier study successfully treated 61 complex, calcified lesions in 60 patients across four US centres, achieving strong clinical outcomes with minimal complications. These results demonstrated the system’s ability to safely and effectively address challenging BTK cases, leading to the development of the AMBITION BTK RCT and registry.
“The AMBITION BTK RCT and registry represent an important advance in the evidence supporting the benefits of laser atherectomy in achieving acute and long-term procedural success,” said AMBITION BTK co-principal investigator Ehrin Armstrong (Adventist Heart and Vascular Institute, St Helena, USA). “The trial will address an important unmet need for patients with chronic limb-threatening ischaemia and tibial artery disease. The data for the trial will also help better understand the Auryon laser’s unique mechanism of action in complex and calcified lesions.”
Samsung Medison has announced the launch of the Samsung Z20 in the USA—a AI-powered ultrasound system designed for advanced obstetrician and gynaecologist (OB/GYN) applications.
A recent press release by the company states that the Z20 introduces innovations aimed at overcoming various diagnostic challenges such as high body mass index (BMI) patients, and operator variability, compounded by staffing shortages which impact exam quality and efficiency.
“The Z20 showcases Samsung’s mission to transform women’s health imaging with breakthrough technology that addresses today’s toughest clinical challenges and delivers the quality care every patient deserves,” said Kyu Tae Yoo, chief executive officer of Samsung Medison. “We are thrilled to introduce the Z20 to the US market, reflecting our substantial investment in artificial intelligence and our commitment to maintaining a rapid pace of innovation.”
A key addition is Live ViewAssistTM, a real-time deep learning tool that enhances precision and simplifies advanced OB exams. Key capabilities include:
Streamlines advanced OB exams with automatic identification of 39 views, real-time quality evaluation, and extraction with no user interaction.
Automatically labels up to 47 anatomic structures and performs 46 essential measurements.
Reduces keystrokes by up to 94%1, minimising repetitive tasks.
“The Z20 represents a significant technology milestone for both Samsung and the broader ultrasound industry,” said Tracy Bury, USA business leader, Women’s Health Ultrasound. “The Z20 not only highlights Samsung’s remarkable journey from a fast follower to a technology leader, but also reflects our commitment to breaking the iron triangle of healthcare cost, access, and quality by integrating the Z20 with a digital ecosystem for telesonography, reporting, and fleet management.”
The US Food and Drug Administration (FDA) has granted 510(k) clearance to GE HealthCare’s enhanced Voluson Expert Series ultrasound systems, which include the Voluson Expert 22, 20, and 18 models.
These systems are designed to improve imaging performance and efficiency in women’s healthcare by integrating ‘high-resolution’ image quality with the latest ultrasound technology and an ergonomic design. Equipped with artificial intelligence (AI)-driven features alongside automation tools, the systems aim to support rapid assessments and early identification, intervention, and diagnosis of complex and high-risk pregnancies.
Lyric Architecture of the systems claims to enhance imaging and processing capabilities, providing detailed images that disclose intricate anatomical details, even in challenging scanning conditions.
The SonoLyst set of AI tools is tailored to streamline examinations by recognising images and automating annotations and measurements, thereby enhancing the ‘accuracy’ and ‘speed’ of exams.
GE HealthCare Advanced Visualization Solutions Women’s Health general manager Gerald Seifriedsberger said: “We are proud to introduce these updates to the Voluson Expert ultrasound systems, which represent our ongoing commitment to advancing technology that addresses women’s health needs of today, and the future.”
The latest update includes SonoLystlive for use during 11 to 14-week anatomical exams, ensuring that essential views are captured for diagnostic precision.
Moreover, the ultrasound systems feature Graphicflow, an expanded colour Doppler offering that graphically represents blood cell trajectories in real-time.
Enhancements to select Voluson AI tools have also been introduced, including SonoPelvicFloor, which can minimise the time required for pelvic floor measurement exams by 80%.
Additionally, SonoAVCfollicle leverages AI to enhance the ‘accuracy’ and ‘precision’ in identifying follicles. The systems are compatible with a variety of speciality probes such as the new lightweight 2D/3D RAB7-D probe and the wireless Vscan Air dual probes.
This development follows a significant £200m agreement between the company and Nuffield Health to strengthen diagnostic imaging services across Nuffield Health’s hospitals in the UK, a recent press release has stated.
Cagent Vascular has announced the start of the POINT FORCE registry, a postmarket clinical follow-up study of the Serranator percutaneous transluminal angioplasty (PTA) serration balloon catheter.
This prospective, multicentre, single-arm study will enrol a minimum of 500 patients at up to 30 centres in the USA. The objective of this study is to evaluate the safety and efficacy, under local standard of care, of serration angioplasty for the treatment of peripheral arterial disease (PAD) throughout the entire leg.
The primary endpoint for this study is device success, defined as the achievement of successful delivery, balloon inflation and deflation, and retrieval of the study device with a post-Serranator residual stenosis of ≤30%, as assessed by an independent angiographic corelab. Yale Cardiovascular Research Group in New Haven, USA, will serve as the corelab for this study.
Led by national co-principal investigators (PIs) S Jay Mathews (Manatee Memorial Hospital, Bradenton, USA) and Michael Siah (University of Texas Southwestern [UTSW] Medical Center, Dallas, USA), this registry will build the body of clinical evidence for serration angioplasty. Siah enrolled the first POINT FORCE patient.
“We’re excited to launch the POINT FORCE registry with the initial enrolment here at UTSW,” said Siah. “Serranator is a key part of our ATK [above-the-knee] and BTK [below-the-knee] treatment algorithm, and our team is eager to analyse this large, corelab-adjudicated dataset to capture the results of treating with serranation across a wide spectrum of treatment strategies and clinical presentations.”
“We know from prior corelab-adjudicated studies that Serranator provides an efficacious result for patients, with a very low rate of complication and mitigated recoil,” stated Mathews. “What we endeavor to understand in POINT FORCE is the role serranation can play in routine clinical practice. We anticipate reviewing iliac, fempop, infrapop, and inframalleolar vessel territories, along with AV [arteriovenous] access.”
Brian Walsh, chairman and chief executive officer of Cagent Vascular, added: “Despite having performed over 20,000 procedures, Serranator remains a new and disruptive PAD therapy. We expect POINT FORCE will illuminate the benefits of serranation and help share the impact in all common clinical algorithms. We’re excited to get started and grateful for the support of our PIs and all participating centers.”
Amplitude Vascular Systems (AVS) recently announced that it has completed a Series B round of financing of US$36 million. The funding will support the US peripheral commercial launch as well as US coronary and carotid investigational device exemption (IDE) trials for the company’s Pulse intravascular lithotripsy (PIVL) device.
“We are pleased to see strong, sustained investor excitement around this technology,” said Mark Toland, chairman of the board for AVS. “Intravascular lithotripsy now represents a large and well-proven therapy that demands new solutions for patients with severely calcified arterial disease. This investor confidence reflects accelerated execution of critical company milestones in 2024, including the initiation of our US peripheral IDE. The commitment from our partners at BioStar Capital and Cue Growth Partners reinforces the great progress toward commercial approval with this technology in the IVL space.”
AVS began enrolling patients in October 2024 in the POWER PAD II US IDE trial, which is a prospective, single-arm, multicentre study evaluating the technical and clinical success of the Pulse IVL system for treating patients with calcific femoropopliteal arteries. The study will enrol up to 120 patients at 20 US sites and enrolment is expected to be completed mid-year 2025.
“AVS is the second company to conduct a peripheral intravascular lithotripsy pivotal IDE trial in the USA. By introducing a new, innovative treatment for calcified arterial disease, we can make a dramatic impact on patient lives and improve outcomes,” said interventional cardiologist Chris Metzger (OhioHealth Riverside Methodist Hospital, Columbus, USA), national principal investigator of the POWER PAD II study.
The funding will also support the company’s coronary US IDE study. “Because the Pulse IVL device uses a unique mechanism of action that eliminates the need for electrical emitters, the deliverability, crossability and efficiency are optimised for very challenging and tortuous coronary cases,” said Steven Yakubov, medical director of the OhioHealth Research Foundation (Columbus, USA) and member of AVS’ physician steering committee.
Lastly, the capital raised will support the US carotid IDE trial, as part of its partnership with the Jacobs Institute in Buffalo, USA, led by Adnan Siddiqui. “We are looking forward to studying the Pulse IVL system in carotids to improve stroke care. We believe the differentiated efficiency of this device versus other IVL catheters will be an important solution for our carotid disease patients, where a shorter treatment time is of utmost importance,” said Siddiqui.
New data from a large, real-world study support the use of drug-eluting devices to reduce amputations, readmissions, and healthcare costs in the treatment of peripheral arterial disease (PAD), Marianne Brodmann (Medical University of Graz, Graz, Austria) informed attendees at the Leipzig Interventional Course (LINC 2025; 28–30 January, Leipzig, Germany).
Brodmann was, for the first time, sharing the results of TRUE-PTX. This study sought to evaluate the use of paclitaxel drug-eluting versus non-drug-eluting devices for the treatment of PAD in a large patient population, focusing specifically on above-ankle amputation, hospital readmission, and mortality rates at 12 months.
Several studies have demonstrated the benefits of drug-eluting therapy for femoropopliteal lesions, Brodmann noted, including sustained vessel patency, clinical improvement, and fewer reinterventions. The question of whether these benefits transfer to real-world practice, however, remains unanswered.
In order to address to address this gap in the literature, Brodmann and colleagues identified 10,000 patients on the Truveta platform who had undergone either drug-eluting therapy (5,000 patients) or non-drug-eluting therapy (5,000 patients) for PAD and analysed their outcomes.
Regarding patient characteristics, Brodmann shared that 40% were female and 82% were white. The presenter also pointed out that race and ethnicity distributions varied between the treatment groups. “Drug-eluting devices were used more frequently for white and Hispanic patients, and less frequently for Black patients,” the presenter noted.
On comorbidities, Brodmann detailed that approximately 32% of patients across the two groups had chronic limb-threatening ischaemia (CLTI), and that other comorbidities were far more prevalent in those patients treated with drug-eluting devices.
Brodmann reported that, before matching, 12-month amputation and readmission “occurred significantly less frequently for patients receiving drug-eluting treatment”. The presenter added that there was no significant difference between the two groups regarding mortality. “So, once again, a severe hint that drug-eluting technology, paclitaxel-coated technology, is not relevant for mortality,” she remarked.
After propensity-score matching, there were around 4,000 patients remaining in the drug-eluting device group and around 3,700 in the non-drug-eluting device group, Brodmann relayed. The proportion of patients with CLTI stayed broadly the same, at close to 30%.
Patients in this matched cohort treated with non-drug-eluting treatment were more likely to have above-ankle amputation, any readmission, and readmission associated with a repeat procedure, Brodmann communicated.
The presenter summarised that, in a contemporary, real-world patient cohort with a high prevalence of CLTI, above-ankle amputation and readmission within 12 months occurred more frequently with non-drug-eluting therapy versus paclitaxel drug-eluting devices in propensity-score-matched patients.
“This large study of real-world evidence parallels the results of formal randomised controlled trials,” Brodmann said in her concluding remarks. “The TRUE-PTX results support the use of drug-eluting devices to reduce amputations and readmissions, and the results have implications for reducing healthcare costs.”
“It’s not only about patient satisfaction, about patient quality of life; it’s also about expense,” Brodmann continued, elaborating on this final point. “Major amputation is expensive and avoiding amputation has the potential for substantial cost savings.”
Based on these conclusions, Brodmann shared her take-home message from the presentation: “Drug-eluting technologies should be the de facto standard of care for PAD.”
Koen Deloose (second from the right) and his vascular team
Bentley today announced the market launch of its BeFlow iliac covered stent system at the Leipzig Interventional Course (LINC 2025; 28–30 January, Leipzig, Germany).
A press release notes that the BeFlow has been designed for the treatment of iliac occlusive and stenotic diseases and enables physicians to treat patients suffering from arteriosclerosis with a covered stent, ensuring safe treatment, long-term patency and durability.
“Our target is to provide a specialised solution for the growing number of patients suffering from diseased iliacs. Bentley has designed the BeFlow covered stent as a focused stent platform addressing stenotic and occluded iliac lesions. Combining all aspects of Bentley covered stent quality, the BeFlow has the potential to become a very competitive alternative in a price-sensitive market segment,” says Martijn Nugteren, director of sales and marketing at Bentley. The BeFlow comes in four diameters of 7 to 10mm and two nominal lengths of 37 and 57mm. A higher degree of product standardisation has a positive impact on production as well as logistic cost, making the BeFlow an affordable solution for the treatment of stenosed iliacs.
Nugteren adds: “Bare metal stents are still frequently used in heavily stenosed iliac arteries where a covered stent would have been the preferred option. Here, financial aspects influence the decision. With the BeFlow we hope to narrow the cost gap between bare metal stents and covered stents so that patients can be treated with a device that really makes a difference.”
Koen Deloose (AZ Sint-Blasius Hospital, Dendermonde, Belgium), who conducted the first-in-human BeFlow procedure involving a 78-year-old patient suffering from severe claudication, comments: “The BeFlow is a great solution for patients with complex aortoiliac occlusive disease. When dealing with more simple lesions, Bentley offers an established uncovered balloon expandable stent, the BeSmooth, with the same product features such as a low profile, high visibility and flexibility that we know from the already proven design from the BeGraft. Regarding ease of use during the endovascular intervention, the new BeFlow fulfils all requirements. Particularly, in heavily stenosed or even occluded iliacs, a covered stent is the preferred solution, as it will ensure long-term patency and is in line with the ESVS [European Society for Vascular Surgery] guidelines for iliac stenting, where it is stated that covered stents may be considered due to higher patency rates.”
Bentley advises that the BeFlow is CE certified and will be commercially available as of February 2025. After the market launch, Bentley plans a postmarket clinical follow-up (PMCF) study, led by Maria Antonella Ruffino (Ente Ospedaliero Cantonale, Lugano, Switzerland), as principal investigator.
Imperative Care has today announced the receipt of US Food and Drug Administration (FDA) 510(k) clearance of the company’s Zoom system, making it the first comprehensive stroke thrombectomy system to include large-bore 0.088-inch catheters indicated for both access and aspiration when used with a Zoom catheter.
As per an Imperative press release, this clearance expands the company’s current portfolio of 0.035-inch to 0.071-inch aspiration catheters to now include the Zoom 0.088-inch catheters—Zoom 88, Zoom 88 Support and TracStar—for aspiration as part of the Zoom system.
Clinical evidence submitted to the US FDA to support the clearance included final data from the Imperative trial. This prospective, multicentre trial evaluated the clinical benefits of the Zoom system in patients treated across 26 US institutions. The analysed cohort included 211 patients who were treated with concomitant aspiration thrombectomy using two catheters.
“At Imperative Care, we are focused on developing a patient-centric and well-studied comprehensive stroke system for physicians to best care for their patients based on their specific needs and anatomy,” said Ariel Sutton, executive vice president and general manager of Imperative’s Stroke business. “We know that, with stroke, time is the most critical factor in driving positive patient outcomes. The Zoom system is the first purpose-built technology from access to aspiration that maximises versatility for rapid and effective procedures—as validated by the Imperative trial and previous clinical studies of the Zoom stroke solution. Thank you to all the physicians, patients and their families who participated in this landmark trial, and placed their trust in our technology.”
Key results from the Imperative trial, submitted to the FDA to support clearance, demonstrated:
Median time from groin puncture to modified thrombolysis in cerebral infarction (mTICI) ≥2b reperfusion of 19 minutes; fastest among prior thrombectomy trials including ARISE II, TIGER, Penumbra 3D and PROST, according to Imperative
A core lab-adjudicated rate of mTICI ≥2b reperfusion was achieved in 84% of patients within three passes or less without the use of any additional thrombectomy devices as rescue therapy—similar to prior trials (82%), including SWIFT PRIME, Penumbra 3D, ARISE II, TIGER, ETIS and PROST
Stent-retriever rescue therapy used in only 4.7% of cases to achieve mTICI ≥2b reperfusion
A core lab-adjudicated rate of symptomatic intracranial haemorrhage of 0.9%, lower than the rate of prior trials (4.7% [SWIFT PRIME, Penumbra 3D, ARISE II, ETIS and MR CLEAN De Novo 510(k) data]); and a rate of independently adjudicated dissection and vessel perforation of 0.5%, lower than prior trials (1.3% [SWIFT PRIME, Penumbra 3D, ARISE II, PROST and MR CLEAN De Novo 510(k) data])
“In addition to the remarkable efficacy of the Zoom system, I was impressed by the demonstrated safety profile as evidenced by a 0.5% instance of serious vessel injury reported in the study,” said William Mack (University of Southern California, Los Angeles, USA), co-principal investigator of the Imperative trial. “Even more impressive was the 0.9% rate of symptomatic intracranial haemorrhage. These data, combined with our extensive experience with the Zoom system, reinforce our confidence in the technology and its clinical benefits for our practice, and the patients we treat.”
The Mount Sinai Hospital has announced that it has performed its first procedure—and the first in New York City, USA—using the Hydros (PROCEPT BioRobotics) robotic system designed to treat benign prostatic hyperplasia (BPH), or an enlarged prostate.
The minimally invasive procedure offers “new hope” for patients experiencing the symptoms of BPH, including frequent urination, incomplete bladder emptying, and night time urgency, a press release by the company has stated.
Urologists at the hospital recently performed the health system’s first three procedures, with all patients responding well to the treatment and being discharged the following day.
“This technology provides a much-needed option for men dealing with the burdens of BPH,” says Steven A Kaplan, director of the Men’s Wellness Program, Mount Sinai Health System, and professor of urology, Icahn School of Medicine at Mount Sinai. “What makes Hydros stand out is how it combines advanced imaging, robotic precision, and a heat-free approach to tissue removal, all while preserving crucial functions like continence and sexual health.”
The Hydros system builds on traditional surgical methods for treating BPH, such as transurethral resection of the prostate (TURP) and laser treatments, by introducing several notable innovations. It features artificial intelligence (AI)-powered treatment planning through FirstAssist AI (PROCEPT BioRobotics), a sophisticated image recognition software that identifies critical anatomical structures using ultrasound. This technology aids in creating personalised treatment plans tailored to each patient’s prostate anatomy.
Additionally, the system combines advanced ultrasound imaging with digital cystoscopy, providing surgeons with a detailed, multidimensional view of the prostate. This improved visualisation supports greater precision during procedures and enhances surgical planning.
Hydros also employs a robotic-assisted heat-free waterjet for tissue resection, allowing for effective removal of obstructive tissue while preserving key anatomical structures. This approach reduces the risk of complications, such as incontinence or erectile dysfunction.
Finally, the system is designed to streamline the surgical workflow with features like an integrated tower for setup, an adjustable touchscreen for better ergonomics, and user-friendly software to guide surgeons through each step of the procedure.
These advancements provide a more precise and patient-friendly treatment option compared to traditional methods, addressing common challenges such as tissue damage and unwanted side effects.
To expand access to this technology, Mount Sinai has prioritised training for its urology team. Kaplan, who has performed well over 400 aquablation procedures with the earlier model, recently completed advanced HYDROS training. He will be joined by Mount Sinai surgeons who will begin performing the procedure in the coming months.
“This new technology is part of our commitment to delivering the most advanced and patient-centred care,” says Kaplan. “The positive outcomes we’ve seen so far are a testament to the potential of Hydros to redefine how we approach BPH treatment.”
“Calcified arteries remain one of the most difficult conditions to treat in our field,” said interventional cardiologist Amir Kaki (Henry Ford St. John’s Hospital, Detroit, USA). “FastWave’s laser IVL platform is a compelling advancement that should provide a more precise, efficient, and predictable way to manage complex arterial disease.”
“This milestone reflects the incredible talent of our entire team and our dedication to equipping physicians with cutting-edge tools for their most challenging cases,” said Scott Nelson, co-founder and chief executive officer of FastWave Medical.
FastWave’s chief operations officer Tristan Tieso added: “Our laser IVL technology continues to push the boundaries of what’s possible in treating calcified arteries, getting us closer to our primary goal of helping interventionalists ensure the best care for their patients.”
Concept Medical has announced the successful completion of patient enrolment in the SirPAD trial, with over 1,250 patients now enrolled.
A press release notes that the SirPAD (Major adverse limb events in patients with femoropopliteal and below-the-knee peripheral arterial disease treated with either sirolimus-coated or uncoated balloon) randomised controlled trial is the world’s largest study evaluating the treatment of PAD using the MagicTouch PTA sirolimus-coated balloon versus uncoated balloons and one of the largest device studies ever performed for PAD.
More than 1,250 patients have been enrolled and will be followed up at 12 months to assess the primary outcome of major adverse limb events (MALE). Final results are expected by Q1–Q2 2026.
SirPAD is an investigator-initiated, multicentre, randomised, open-label trial that aims to determine whether the MagicTouch PTA sirolimus-coated balloon is non-inferior to plain balloon angioplasty. The trial will also explore the potential for superiority.
Principal investigators Nils Kucher and Stefano Barco from the University Hospital Zurich (Zurich, Switzerland) said in a press release: “Sirolimus-coated balloons represent a promising technology in treating symptomatic PAD, supported by evidence primarily from studies with surrogate endpoints. While trials like SIRONA and ongoing studies such as SirPAD are expanding knowledge, robust data from randomised controlled trials with clinical outcomes are needed to guide treatment and shape future guidelines. This result, having been able to randomise so many patients in a PAD device study, is unprecedented and we are very thankful to all investigators and patients for having supported the trial.”
FDA has issued new guidance for the use of paclitaxel coated devices in peripheral arterial disease
The US Food and Drug Administration (FDA) has issued a statement outlining measures to enhance protections against medical device shortages.
According to Michelle Tarver, director of the FDA’s Center for Devices and Radiological Health (CDRH), supply chain disruptions—often caused by natural disasters, limited production capacities for specialised devices, or manufacturing and quality issues—pose the greatest threat to device availability. Tarver warned that as the global regulatory environment evolves, the USA might risk falling behind in ensuring device availability to protect patients.
On January 10, 2025, new European Union (EU) regulations came into effect, requiring medical device manufacturers to notify authorities about any anticipated supply shortages at least six months in advance. Tarver remarked, “Now, the European Commission and member countries will have access to vital information about medical device shortages that could impact their population. In contrast, there are no mandatory reporting requirements for potential medical device shortages in the USA except, as required, during or in advance of a public health emergency.”
To address this gap, the FDA is seeking new statutory authority to amend Section 506J of the Coronavirus Aid, Relief, and Economic Security Act (CARES Act)—which was passed in 2020 to address the economic impact of the pandemic—by removing the current limitation that ties device shortage reporting to public health emergencies. The FDA is also advocating for increased funding to support the CDRH Supply Chain Program, which works to identify and mitigate device shortage issues.
“These changes are essential for enabling proactive responses to prevent supply chain disruptions before they impact patient care, and the future of our healthcare system. In recent years, congress has provided resources to support CDRH’s efforts to respond to supply chain disruptions, and while these resources have been helpful, additional funding will be needed to sustain and enhance our abilities to help identify, prevent, and mitigate shortages,” Tarver explained.
Without comparable transparency in the USA, the EU’s new regulations provide critical information to healthcare providers, giving them the opportunity to act in advance to mitigate device shortages. In contrast, Tarver noted that US hospitals and healthcare systems are left “ill-prepared to address shortages, forcing them to rely on unpredictable or ad-hoc solutions.”
Tarver emphasised that safeguarding patients, particularly neonates and children, during medical device shortages is crucial. “When shortages arise, there are few options that may accommodate children—compelling clinicians to adapt adult-sized equipment, which can lead to suboptimal outcomes and increased risks for patient safety,” she said.
In conclusion, Tarver reaffirmed the FDA’s commitment to collaborating with relevant authorities to strengthen the domestic supply chain and address vulnerabilities. “Together, the FDA, healthcare providers, patients, hospitals, and congress can work to ensure that paediatric and other patient populations receive the care they need without interruption,” she said.
Nextbiomedical has announced that it has received investigational device exemption (IDE) approval from the US Food and Drug Administration (FDA) for its clinical trial RESORB featuring Nexsphere-F.
Designed to alleviate pain in knee osteoarthritis (OA) patients, the fast resorbable embolic microsphere will undergo a multicentre trial in the USA for market approval, marking a significant milestone in its global expansion strategy.
Knee OA is a debilitating condition affecting over 654 million people aged 40 and above globally, making it one of the leading causes of pain and disability among older adults. While existing treatments, such as non-steroidal anti-inflammatory drugs (NSAIDs) and hyaluronic acid injections, provide temporary relief, their long-term efficacy is limited, and side effects are a significant concern. The RESORB trial aims to address these unmet needs by introducing a more sustainable and patient-friendly solution through genicular artery embolization (GAE) and Nexsphere-F.
RESORB is a multicentre, randomised, open-label study designed to assess how Nexsphere-F performs in alleviating pain and improving mobility in patients with knee osteoarthritis. The trial will enrol participants across leading healthcare institutions in the USA, focusing on the novel approach of GAE to treat OA-related symptoms.
Ziv J Haskal (University of Virginia, Charlottesville, USA) national principal investigator for RESORB, stated that Nexsphere-F has already received CE-mark approval for use in arthritis embolization, and has proven its superior safety and efficacy in thousands of musculoskeletal embolization patients in Asia and Europe. The company is actively seeking and securing its clinical trial sites for the US pivotal trial now.
Additionally, chief executive officer Don Haeng Lee emphasised that obtaining FDA approval for Nexsphere-F marks a pivotal milestone for the company, reflecting its commitment to advancing innovative medical solutions. He expressed pride in the successful completion of the essential IDE approval and shared optimism that the upcoming RESORB clinical trial will proceed seamlessly, paving the way for timely FDA approval. He further highlighted the company’s vision of making Nexsphere-F available globally to improve the quality of life for arthritis patients worldwide.
Concept Medical has successfully enrolled the first patient in the MAGICAL BTK US investigational device exemption (IDE) pivotal trial, a press release reveals.
Following the recent IDE approval by the US Food and Drug Administration (FDA) for the MagicTouch PTA, this enrolment heralds the beginning of Concept Medical‘s peripheral clinical trial programme in the USA.
“The enrolment of the first patient in the MAGICAL BTK trial represents an important stride toward improving the standard of care for below-the-knee disease in patients with peripheral arterial disease,” said Prakash Krishnan (Icahn School of Medicine at Mount Sinai, New York, USA), who enrolled the first patient. “Sirolimus-coated balloon technology has the potential to significantly enhance limb salvage and patient quality of life. I am honoured to be part of this landmark study and look forward to the meaningful clinical evidence it will generate.”
The MAGICAL BTK pivotal trial is designed to evaluate the safety and effectiveness of the MagicTouch PTA sirolimus-coated balloon compared to standard percutaneous transluminal angioplasty (PTA) for the treatment of below-the-knee (BTK) arterial disease. The primary endpoint, measured at 12 months, is primary patency.
This global, multicentre study is led by Sahil Parikh (Columbia University Irving Medical Center, New York, USA), with a panel of principal investigators including Eric Secemsky (Beth Israel Deaconess Hospital and Harvard Medical School, Boston, USA), Brian DeRubertis (NY Presbyterian Weill Cornell Medical Center and Cornell University Medical College, New York, USA), Edward Choke (Northern Heart Hospital, Georgetown, Malaysia), and Osamu Iida (Osaka Keisatsu Hospital, Osaka, Japan).
“The initiation of the MAGICAL BTK trial heralds a new era in the treatment of patients with chronic limb-threatening ischaemia and offers hope to the millions of patients with this condition who are at risk for limb loss because of insufficient arterial circulation in their legs,” stated Parikh.
A press release notes that sirolimus-coated balloon technology has already reshaped coronary and peripheral arterial disease management, with MagicTouch achieving positive results in large-scale trials across Asia and Europe. Now, with the MAGICAL BTK trial, US patients have the opportunity to benefit from this approach. Concurrently, the release continues, patient enrolment from Asia will broaden the global patient cohort, offering a more comprehensive understanding of the therapy’s benefits across diverse populations.
Sutter Health and GE HealthCare today announced a seven-year strategic partnership, known as a Care Alliance.
The long-term collaboration will increase access to essential diagnostic care across California, USA, providing patients with advanced technology in their own communities that can help enable quicker appointment scheduling, accelerated diagnostic imaging scan results, early diagnoses, greater convenience, and more consistent and timely care. This Care Alliance marks one of GE HealthCare’s largest ever enterprise strategic partnerships, a recent press release states.
For Sutter, this alliance will help achieve faster access to novel equipment and technology solutions, as well as provide an innovative service delivery model with enhanced, reliable equipment availability. It is grounded in key goals, including expanded access to care, improved patient experience, more consistency regardless of care location, increased patient capacity, greater system integration and interoperability, and a timely refresh of needed equipment. It centres on several areas of collaboration, including optimised technology, an innovative service delivery model, advancing service line care at destination centres of excellence and digital integration.
“This strategic partnership is rooted in our commitment to providing innovative, high-calibre care to our 3.5 million patients across Northern California and the central coast,” said Warner Thomas, president and chief executive officer of Sutter Health. “We’re responding to what we’ve heard from our physicians and making comprehensive upgrades with the latest technology to boost our capacity and expand access points. This collaboration ensures that no matter where patients enter the Sutter Health system, they’ll receive seamless and coordinated care.”
The first key focus area of the Care Alliance is an accelerated technology programme across the Sutter Health system that will focus on some of the most advanced artificial intelligence (AI)-powered imaging technology and digital solutions available to patients, including PET/CT, SPECT/CT, MRI, CT, X-ray, nuclear medicine and ultrasound. GE HealthCare’s interventional, mammography, diagnostic cardiology, maternal and infant care and anaesthesia solutions will also be included in Sutter Health’s ambulatory care centres, helping to address the growing need for care outside of the traditional hospital setting. This comprehensive technology refresh covers the breadth of GE HealthCare’s portfolio of solutions, providing clinicians with innovative options to meet changing patient needs more efficiently and quickly.
“We are committed to support Sutter Health in its mission and have deep respect for their openness to a collaboration that meets the heart of their needs,” said Catherine Estrampes, USA and Canada president & chief executive officer at GE HealthCare. “This Care Alliance is a customised, clinician-focused approach aligned with our shared goals. It was jointly designed with expert assessment of how we provide our latest imaging technology in the right settings to serve patients most efficiently throughout their care journey, closer to home. We look forward to supporting Sutter Health physicians and clinicians in delivering enhanced patients’ outcomes.”
Dr. Ripal Gandhi and Dr. Nima Kokabi, with Alexander Villalobos acting as moderator, discuss their utilization and best practices with SIR-Spheres through 5 topics:
Dr. Ripal Gandhi and Dr. Nima Kokabi, with Alexander Villalobos acting as moderator, discuss their utilization and best practices with SIR-Spheres through 5 topics:
1/ Order-Map-Treat Program – The ability to Order before you Map to accelerate your SIRT program
“Map on one day and treat the next day is good for the patient, is great for the referring physicians and really interrupts any delays. […] It is also very valuable for me […] I am not tied to treat on a specific day” – R Gandhi
2/ Dose Thresholds – How your treatment intent determines your dosimetry
“When it comes to dosimetry planning, you really need to keep in mind what is the intent of the treatment. […] If you’re doing a curative intent treatment […], then you can actually significantly increase your thresholds” – N Kokabi
3/ Tumor Coverage – The impact of number of spheres on the radiobiological effect
“As you increase the number of particles you’re going to have better coverage and you should have better radiobiological effect” – R Gandhi
4/ FLEXdose Delivery Program – How to personalize activity and coverage with respect to the treated volume
“For radiation segmentectomy I prefer higher activity and fewer particles” R Gandhi “for larger and multifocal distribution I use either 1-day pre-cal (4.6GBq) or day of calibration (3.6GBq)” – N Kokabi
5/ Patient Case
“The ability to take your […] vial and fractionate it […], you just basically draw up what you need, which to me is that flexibility and that personalization up to the time of treatment which is extremely valuable.” – R Gandhi
This video was filmed by Sirtex Medical Limited and is being sponsored for distribution in association with Interventional News. Biba Medical bears no responsibility for the assets used in the production of this video.
Argon Medical Devices, Inc. Logo. (PRNewsFoto/Argon Medical Devices, Inc.)
Argon Medical has announced the acquisition of Accurate Medical Therapeutics’ SeQure and DraKon microcatheters.
Microcatheters such as SeQure and DraKon are commonly used by physicians to conduct interventional procedures in which therapeutic agents or devices are introduced into the small vessels delivering blood to a tumour or abnormality. As such, physicians often select a microcatheter for a procedure based on the catheter’s ability to navigate to the target and its compatibility with therapeutic agents or devices.
Both the SeQure and Drakon catheters earned a strong reputation for being easy to navigate and broadly compatible, a recent press release states. Further, the company shares that SeQure is the only reflux control microcatheter designed to create a fluid barrier that directs the flow of therapeutic agents and devices toward the intended target.
“A microcatheter can make or break a procedure,” said Neal Khurana, interventional radiologist and co-founder of EmboPartners, a physician-run organisation that specialises in minimally invasive vascular embolization procedures for improved patient care. “A well-designed microcatheter determines whether you achieve precise navigation, efficient delivery of embolic materials, and ultimately, optimal patient outcomes. The DraKon and SeQure microcatheters have become preferred tools in my practice due to their dependable trackability through tortuous vessels, the performance of their hydrophilic coating, and their ability to deliver contrast and embolics efficiently, even through the smallest catheter sizes.”
“Adding the SeQure and DraKon microcatheters to our existing product portfolio marks an important first step in expanding the products we offer interventional oncologists beyond diagnostic procedures and into therapeutic delivery,” said George Leondis, president and chief executive officer, Argon Medical. “As we do so, we also expand the ways in which we can improve the lives of patients and caregivers through the delivery of best-in-class medical devices and superior service, in alignment with our company mission.”
Biotronik has today announced the approval of two new indications for the Orsiro Mission drug-eluting stent (DES):
One-month dual antiplatelet therapy (DAPT) for high bleeding risk (HBR) patients: Allows practitioners to offer personalised, shorter DAPT durations to their patients at high risk of bleeding events, in accordance with the most recent guidelines.
Calcified lesions: Allows practitioners to target more complex lesions with moderate or severe calcification.
These new indications follow the company’s recent global regulatory approval of the Orsiro Mission DES for an increased maximum allowed diameter (MAD) post-dilation (Ø2.25–3mm, MAD: 4mm, Ø3.5–4mm, MAD: 5mm).
The Centers for Medicare & Medicaid Services (CMS) is opening a national coverage analysis (NCA) on renal denervation, with a view to reviewing and developing a national Medicare coverage policy for the therapy for patients with hypertension.
The expected completion date for the national coverage analysis is 11 October 2025. Until a national coverage determination is put into effect, renal denervation procedures will continue to be evaluated for coverage based on medical necessity for individual Medicare patients.
This latest news follows the announcement in late 2024 that CMS had granted transitional pass-through (TPT) payment for Medtronic’s Symplicity Spyral renal denervation (RDN) catheter and Recor Medical’s Paradise ultrasound RDN (uRDN) system.
TPT payment, which is effective for up to three years beginning 1 January 2025, aims to support patient access to new and innovative technology.
Both the Medtronic and Recor Medical renal denervation systems gained US Food and Drug Administration approval in November 2023. Medtronic‘s Symplicity Spyral system is a minimally invasive procedure that delivers radiofrequency energy to nerves near the kidneys that can become overactive and contribute to high blood pressure, whilst the Paradise system is an ultrasound-based technology.
In a press release, Medtronic says that the national coverage analysis was initiated by CMS in response to its request to support Medicare beneficiary access to the Symplicity Spyral system.
“Hypertension is a global health epidemic that impacts a wide variety of patients,” said Jason Weidman, senior vice president and president of the Coronary and Renal Denervation business within the Cardiovascular Portfolio at Medtronic. “As the leader in developing a minimally invasive treatment option for hypertension, Medtronic has been closely engaged with CMS to establish a national coverage pathway for Symplicity Spyral. We appreciate CMS’ efforts in creating new pathways to expedite access to breakthrough technologies like Symplicity Spyral and look forward to our continued partnership in developing a national coverage policy.”
Recor Medical has similarly welcomed the commencement of the analysis, describing it as the first step in the National Coverage Determination (NCD) process towards the potential expansion of coverage of the Paradise system among Medicare beneficiaries.
In a press release, Recor states that it appreciates CMS’ consideration of potential national coverage of renal denervation as a hypertension treatment option for Medicare beneficiaries and will continue to work closely with CMS throughout the NCD process.
AngioDynamics has announced the publication of the results from the Acute Pulmonary Embolism Extraction Trial with the AlphaVac system—APEX-AV—in the Journal of the Society for Cardiovascular Angiography & Interventions (JSCAI).
The primary efficacy endpoint of the APEX-AV trial was the reduction in right ventricle to left ventricle (RV/LV) ratio between baseline and 48 hours post-procedure. The primary safety endpoint was the rate of major adverse events (MAEs), including events such as major bleeding and serious device-related clinical deterioration, pulmonary vascular injury, and cardiac injury within the first 48 hours. Patients were followed for 30 days post-index procedure. The results demonstrated the device as a safe and effective treatment for acute intermediate-risk PE with a significant reduction in RV/LV ratio and clot burden with a low rate of adverse events.
The APEX-AV trial demonstrated a 35.5% reduction in clot burden (via the Modified Miller index score), comparing favourably to other mechanical aspiration devices on the market. The unique design features of the device, including its funnel tip, optional wireless navigation, and blood loss mitigation, contributed to clinically significant improvements in both safety and efficacy.
“Achieving publication in a respected, peer-reviewed journal underscores the strength and importance of the APEX-AV trial findings and their potential impact on patient outcomes,” said Juan Carlos Serna, AngioDynamics’ senior vice president of scientific and clinical affairs. “The inclusion of the AlphaVac F1885 System in JSCAI validates our commitment to advancing meaningful solutions for pulmonary embolism, a life-threatening condition affecting hundreds of thousands of people each year. This milestone caps a transformative year for the AlphaVac F1885 System, following its US Food and Drug Administration (FDA) clearance for PE thrombectomy and its spotlight at the SCAI Scientific Sessions. We are proud to deliver innovations that equip physicians with effective tools to improve care and save lives.”
The APEX-AV trial was initiated in partnership with the widely respected Pulmonary Embolism Response Team (PERT) Consortium and was led by co-principal investigators William Brent Keeling, associate professor at the Emory School of Medicine (Atlanta, USA), and Mona Ranade, assistant professor, interventional radiology, at the David Geffen School of Medicine at University of California, Los Angeles (UCLA, Los Angeles, USA). The trial results were initially presented at The Society for Cardiovascular Angiography & Interventions (SCAI) 2024 Scientific Sessions (2–4 May, Long Beach, USA).
“We are incredibly excited by the results of the APEX-AV trial, which demonstrate the safety and efficacy of the AlphaVac F1885 System in treating patients with pulmonary embolism,” said Keeling. “These outcomes are critical for PE patients, where timely and efficient intervention can greatly improve long-term health outcomes and reduce the risk of complications.”
In December 2023, AngioDynamics announced the completion of patient enrolment in its APEX-AV trial, a single-arm investigational device exemption (IDE) study that enrolled 122 patients with confirmed acute, intermediate-risk PE across 25 hospital-based sites in the USA to assess the AlphaVac F18⁸⁵ System for the treatment of PE. In April 2024, the FDA cleared the AlphaVac F1885 System for the treatment of PE.
“The results from the APEX-AV trial demonstrate the significant impact of the AlphaVac F1885 technology in treating pulmonary embolism,” said Mona Ranade, assistant professor, interventional radiology, at the David Geffen School of Medicine at UCLA. “We observed a significant reduction in clot burden pre- and post-treatment, and saw a notable improvement in pulmonary artery pressures, underscoring the efficacy of this innovative approach. The procedure was completed with remarkable efficiency, with a short procedure time, making it a promising option for patients in need of rapid and effective intervention.”
The published article concluded: “Percutaneous mechanical aspiration thrombectomy with the AlphaVac system provided a safe and effective treatment for acute intermediate-risk PE with a significant reduction in RV/LV ratio and clot burden with a low rate of adverse events.”
Inquis Medical has announced completion of patient enrolment in its AVENTUS clinical trial, a pivotal investigational device exemption (IDE) trial evaluating the safety and efficacy of the company’s Aventus thrombectomy system for the treatment of pulmonary embolism (PE).
A total of 130 patients with intermediate-risk PE were enrolled in the AVENTUS clinical trial, a multicentre, prospective, single-arm trial conducted at more than 20 clinical sites across the USA.
“This trial is a key step toward delivering a more streamlined, efficient, and precise thrombectomy solution for treating life-threatening blood clots,” said Jun Li, co-director of the Vascular Center and Pulmonary Embolism Response Team at University Hospitals Harrington Heart & Vascular Institute (Cleveland, USA) and the trial’s national co-principal investigator (PI). “The AVENTUS system stands out with its unique combination of streamlined blood return, directional aspiration, and the elimination of multiple dilator or wire exchanges, offering an elegant and efficient solution for removing thrombi in PE patients.”
“The AVENTUS pivotal trial represents a new option for treating pulmonary embolism,” said the trial’s national co-principal investigator, Saher Sabri, professor of Radiology at Georgetown University School of Medicine, Chief of Interventional Radiology at MedStar Health, and Division Chief of Interventional Radiology at MedStar Georgetown University Hospital (Washington, DC, USA). “We are grateful to the 130 patient volunteers in this trial and to our colleagues who helped rapidly enrol participants reflecting the clinical community’s strong dedication to advancing care in this field.”
“Completing enrolment in the AVENTUS pivotal study marks a significant milestone, highlighting the potential of the AVENTUS system to streamline and enhance treatment while underscoring Inquis Medical’s commitment to driving innovation and elevating standards of care in venous thromboembolic disease management,” said Mojgan Saadat, co-founder and co-CEO of Inquis Medical. “We sincerely thank the patients, investigators, and site clinical research staff for their efforts in bringing this trial to fruition.”
Medtronic announced today that it has entered into an exclusive US distribution agreement with Contego Medical. Under the agreement, Medtronic will be the sole US distributor for Contego’s portfolio of commercially available products, which provide revascularisation treatment for carotid and peripheral vascular disease.
The agreement also includes an increased investment in Contego and an option to acquire the company. Medtronic has held a minority investment in Contego since 2020.
“Contego’s innovations—backed by excellent data—are transforming how carotid disease is treated, and complement the Medtronic peripheral and stroke protection portfolio,” said David Moeller, senior vice president and president of Medtronic Peripheral Vascular Health, which is part of the company’s Cardiovascular portfolio. “This strategic agreement with Contego Medical expands our commitment to this fast-growing carotid market, and exemplifies Medtronic’s steadfast dedication to advancing innovation and enhancing patient care.”
This agreement includes Contego’s portfolio of commercially available products, including the recently US Food and Drug Administration (FDA)-approved Neuroguard IEP system—a unique, three-in-one carotid stenting system that combines a high-performance stent, post-dilation balloon, and an integrated embolic protection (IEP) filter—as well as Excipio peripheral thrombectomy devices.
Medtronic’s press release notes that the Neuroguard IEP system is backed by clinical data demonstrating the safety and effectiveness of the system, with PERFORMANCE I and PERFORMANCE II investigational device exemption (IDE) trial data consistently recording “unprecedented low event rates”—including zero major strokes, zero neurologic deaths, and zero stent thromboses up to two-year follow-up.
Additionally, Contego is currently evaluating the Neuroguard IEP system with a next-generation direct transcarotid access and protection system—TCAR-IEP—to demonstrate advanced stroke protection regardless of vascular approach, in the PERFORMANCE III trial. The Neuroguard IEP Direct system is currently limited by federal law to investigational use only and is not commercially available in the USA.
“This strategic agreement marks a significant milestone for both Contego Medical and Medtronic. By combining our innovative product portfolio with Medtronic’s extensive market presence and clinical leadership, we are positioned to revolutionise revascularisation treatment in the carotid and peripheral vascular disease space,” said Ravish Sachar, founder and chief executive officer (CEO) of Contego. “This partnership enhances our ability to deliver state-of-the-art solutions to patients and reinforces our commitment to expanding access across the USA.”
Medtronic intends to leverage its peripheral vascular and neurovascular commercial teams to distribute Contego’s portfolio of products in spring 2025, the release adds.
Piccolo Medical has announced an exclusive distribution agreement with Spectrum Vascular. Spectrum Vascular offers a portfolio of venous catheters that leverage the Spectrum antimicrobial and BioFlo thrombus reduction technologies.
Under the partnership, Spectrum Vascular will serve as the sole distributor of the Piccolo Medical catheter navigation and tip confirmation devices, including the ECGuide and SmartPICC product lines. This collaboration is
designed to expand the reach of these innovative and cost-effective technologies, ensuring broader access for vascular access professionals worldwide, a recent press release sates.
“We are excited to partner with Spectrum Vascular as our exclusive distributor,” said Augie Shanahan, chief executive officer of Piccolo Medical. “By integrating our advanced catheter navigation technology with the state-of-the-art Spectrum Vascular catheter products, we aim to transform vascular access procedures, delivering enhanced accuracy, efficiency and cost savings to clinicians across the USA and abroad.”
Chris Yamamoto, board member of Spectrum Vascular and managing partner of Event Capital Strategies, shared enthusiasm for the partnership: “We are delighted to collaborate with Piccolo Medical in support of innovative technologies that ensure professionals and patients have access to the most advanced tools to improve outcomes.”
R3 Vascular today announced that it has received WCG Institutional Review Board (IRB) approval for the ELITE-BTK pivotal trial of its Magnitude drug-eluting next-generation bioresorbable scaffold for below-the-knee (BTK) peripheral arterial disease (PAD). This approval allows the trial to take place at institutions that utilise WCG IRB as their central IRB in the USA. Additionally, the company has announced that the Centers for Medicare and Medicaid Services (CMS) has granted category B approval for the investigational device exemption (IDE) study, ensuring Medicare coverage for the device, related and routine items, and services for the ELITE-BTK trial.
Commenting on the announcements, Christopher M Owens, president and chief executive officer of R3 Vascular, said: “We are very pleased to have received IRB and CMS category B approval so quickly. These important milestones validate the potential of R3 Vascular’s breakthrough technology and help accelerate our path to first enrolment of our ELITE-BTK pivotal trial to measure the impact of Magnitude on patient outcomes and its ability to meet this critical and growing clinical need.”
Josh Smale, vice president of global clinical and scientific affairs of R3 Vascular, added: “Securing WCG and CMS approvals enables us to move forward quickly with investigational site activation activities, which brings us one step closer to first subject enrolment. I’m extremely proud of the great work our team has done to continue to accelerate and maintain our momentum between these milestones, as well as our continued urgency to get this next-generation product delivered to patients.”
Eric A Secemsky (Beth Israel Deaconess Medical Center, Boston, USA), lead investigator for the ELITE-BTK pivotal trial, said: “R3 Vascular’s novel approach in the design of its next-generation bioresorbable drug-eluting scaffold is of great interest to the physician community and has the potential to transform the field of peripheral interventions. We are eager to assess the impact of the Magnitude scaffold on patient outcomes, which is now even closer to reality with the completion of these latest important milestones.”
In May of 2024, R3 Vascular announced the closing of its US$87 million Series B financing round to support the ELITE-BTK IDE pivotal trial as well as additional research and development, global regulatory submissions, scale up of manufacturing processes, and initial commercialisation.
Gore has announced recent CE mark of a lower profile Viabahn VBX balloon expandable endoprosthesis (VBX stent graft).
Medical Device Regulation (MDR) approval of this innovation builds on a proven device which has become an important tool for treating complex vascular disease, the company says in a press release. In addition to offering the longest balloon expandable stent on the market with its 79mm configuration, and the widest range of stent diameter adjustability, the VBX stent graft now also offers the most 6 Fr compatible configurations, the press release adds.
“We are thankful to Gore for being able to be one of the first implanters of the new lower profile VBX stent graft in Europe,” said Michele Antonello, director of the School of Specialization in Vascular Surgery of the University of Padua (Padua, Italy). “Combined with the device flexibility, its accuracy and trusted performance, the new lower profile will enable me to treat my complex cases with a 6 or 7 Fr device.”
No changes to the stent graft design were made to achieve the lower profile. By focusing on improvements to the delivery system only, the characteristics and performance of the stent graft itself remain unchanged and are joined by the enhanced versatility a lower profile provides, Gore states. Depending on the practice, physicians may be able to use the VBX stent graft with a broader set of patients, experience a lower risk of complications at the access site, find improved procedure efficiency and/or a general improvement in ease of use.
“With the recently published five-year data and being part of the current Gore VBX FORWARD clinical study that aims to investigate the superiority of the VBX stent graft compared with bare metal stents for the treatment of complex iliac occlusive disease, this lower profile innovation provides yet another reason to feel confident in the proven outcomes of the VBX Stent Graft and the broad applicability of its use in my practice,” said Ash Patel, vascular surgeon, Guy’s & St Thomas’ Hospital NHS Foundation Trust, London, UK.
Since its US launch in 2017, more than 500,000 VBX stent grafts have been implanted worldwide. The VBX stent graft is indicated in the EU for the treatment of: De novo or restenotic lesions in the iliac arteries, including lesions at the aortic bifurcation; De novo or restenotic lesions in the visceral arteries; Isolated visceral, iliac and subclavian artery aneurysms; or Traumatic or iatrogenic vessel injuries in arteries that are located in the chest cavity, abdominal cavity, or pelvis (except for aorta, coronary, innominate, carotid, vertebral and pulmonary arteries).
The lower profile device will be rolled out to the European market over the coming months.
“The approval and release of the lower profile VBX stent graft serves as a demonstration of the Gore Medical Products Division’s commitment to continual improvement and lifelong innovation in collaboration with physicians to solve tough challenges where there is a critical patient need,” said Jill Paine, leader of Gore’s peripheral business. “We look forward to supporting our physicians and their patients through the delivery of this exciting innovation to their treatment toolbox.”
Which stories resonated most with the interventional community in 2024? Explore our roundup of the most popular stories from Interventional News over the past year.
Following her presentation on uterine artery embolization (UAE) for fibroids at the Global Embolisation Oncology Symposium Technologies (GEST; 16–19 May, New York, USA), Abeer AlDhawi (Riyadh, Saudi Arabia), describes the “significant relief” that can be provided to patients through this minimally invasive procedure.
Hotly debated across the Society of Interventional Oncology (SIO; 25–29 January 2024, Long Beach, USA) annual conference programme, speakers took to the stage to contest the survival of transarterial chemoembolization (TACE) in the age of yttrium-90 (Y90) transarterial radioembolization (TARE) and immunotherapy, their compelling arguments making some audience members “more confused and others happy”.
A recent survey conducted by The Harris Poll on behalf of the Society of Interventional Radiology (SIR) has revealed that more than half (53%) of women diagnosed with uterine fibroids were primarily offered a hysterectomy. In contrast, fewer than 20% were presented with less invasive alternatives such as over-the-counter non-steroidal anti-inflammatory drugs (NSAIDs; 19%), uterine fibroid embolization (UFE; 17%), oral contraceptives (17%), and endometrial ablation (17%). Additionally, 17% of women surveyed “mistakenly” believe that hysterectomy is the only available treatment, a misconception held by over 27% of women aged 18–34.
The Society of Interventional Radiology (SIR) Foundation, The VIVA Foundation and Penumbra, today announced the launch of the EMBOLIZE trial, a first-of-its-kind prospective, randomised controlled trial studying the effects of ovarian vein embolization (OVE) and pelvic vein embolization in reducing pain in women experiencing chronic pelvic pain due to pelvic venous disease (PeVD).
Andreas Adam, emeritus professor of interventional radiology at King’s College London, UK and joint editor-in-chief of Interventional News, describes his personal experience entering the field of interventional radiology.
In a new global statement, aimed to set forth the essential elements of interventional radiology (IR) and continuing challenges facing the specialty, the Cardiovascular and Interventional Radiology Society of Europe (CIRSE) and the Society of Interventional Radiology (SIR) query: Have we reached the tipping point?
An analysis of data collected on interventional radiology (IR) practice in the UK has shown an increasing trend in the number and complexity of procedures between 2017 and 2021, despite an imbalance in provision and demand of IR services, as well as a “striking” lack of records regarding safety and service-cost data.
In a paper published in the July 2024 issue of the Journal of Hypertension, Andrew Sharp (University Hospital of Wales and Cardiff University, Cardiff, UK) et al reviewed 16 randomised controlled trials to assess the evidence of renal denervation’s (RDN) efficacy, concluding that, in uncontrolled arterial hypertension, RDN leads to a consistent reduction in blood pressure.
A minimally invasive procedure provides significant relief from knee pain and may prevent the need for knee replacement surgery in people with osteoarthritis, according to a study presented at the Radiological Society of North America (RSNA) annual meeting (1–5 December, Chicago, USA).
At the recent Endo Vascular Access (EVA) meeting (14–15 June, Patras, Greece), Ziv Haskal (University of Virginia School of Medicine, Charlottesville, USA) spoke to Timothy Clark (Perelman School of Medicine at the University of Pennsylvania, Philadelphia, USA) about what they referred to as the “gold rush” of thrombectomy devices for large-calibre blood vessels.
Argon Medical Devices, Inc. Logo. (PRNewsFoto/Argon Medical Devices, Inc.)
Argon Medical announces the first patient enrolment in the CLEAN-PE study. The prospective, multicentre CLEAN-PE study aims to evaluate the safety and efficacy of the Cleaner Pro thrombectomy system for removing blood clot from the lungs in patients diagnosed with pulmonary embolism (PE). CLEAN-PE is estimated to enrol over 100 patients at various hospital facilities across the USA.
The multicentre study is led by principal investigator Aravinda Nanjundappa (Cleveland Clinic, Cleveland, USA). The first patient procedure took place at Buffalo General Medical Center in Buffalo, in New York, USA by David M Zlotnick.
“We are proud to enrol the first patient in the CLEAN-PE study utilising the Cleaner Pro thrombectomy system. Unique treatment options are emerging for the management of this patient population. We are excited to evaluate a new device for patients diagnosed with pulmonary embolism.” said Zlotnick.
“Data indicates that pulmonary embolism mortality rates have increased in the last decade. We aim to help physicians improve patient outcomes by developing new solutions that enable quicker and easier PE interventions. Enrolling the first patient into the CLEAN-PE study is a monumental step forward for the solution we designed, and we are excited to discover the difference the Cleaner Vac thrombectomy system can make for patients with this life-threatening condition.” said George Leondis, president and chief executive officer at Argon Medical.
The Cleaner Pro thrombectomy system is a catheter-based aspiration thrombectomy device comprised of a user-controlled handpiece, a large-bore aspiration catheter, a dilator, and a single-use aspiration pump and canister.
Boston Scientific's global headquarters in Marlborough, USA
Boston Scientific’s global headquarters in Marlborough, USA
Boston Scientific has announced it has entered into a definitive agreement to acquire Bolt Medical, the developer of an intravascular lithotripsy (IVL) advanced laser-based platform for the treatment of coronary and peripheral artery disease.
“Representing one of the fastest growing medical device segments, intravascular lithotripsy therapy addresses a significant unmet need for patients with complex calcified arterial disease through a minimally invasive approach,” said Lance Bates, senior vice president and president, Interventional Cardiology Therapies, Boston Scientific. “Bolt Medical is developing a next-generation technology that is highly complementary to our existing portfolio. The addition of this system to our offerings can help us better serve physicians and their patients and provides a platform for future innovation.”
Lithotripsy is a procedure in which a physician breaks up hardened masses such as calcium to help restore blood flow. The Bolt IVL system is designed with a novel application of lithotripsy to fracture calcium by creating acoustic pressure waves inside of a balloon catheter. The system also includes visible, directional emitters for consistent energy delivery in the treatment of the calcified lesions.
Boston Scientific initially developed the concept for the Bolt IVL system which helped establish Bolt Medical in 2019. As a strategic investor in Bolt Medical, Boston Scientific has an equity stake of approximately 26%. As a result, the transaction consists of an upfront payment of approximately US$443 million for the 74% stake not yet owned and up to US$221 million upon achievement of certain regulatory milestones.
Bolt Medical recently announced the completion and results of the RESTORE ATK and RESTORE BTK pivotal clinical trials investigating the Bolt IVL Above the Knee (ATK) and Below the Knee (BTK) systems for the treatment of peripheral artery disease in patients with moderate to severely calcified lesions. The data from both studies will be used to support US Food and Drug Administration (FDA) and CE mark regulatory submissions for the devices. In December 2024, Bolt Medical received FDA approval to commence the global FRACTURE IDE clinical trial in the USA, which is investigating the use of the Bolt IVL coronary system for the treatment of coronary arterial disease with severely calcified lesions.
Boston Scientific anticipates the transaction to be completed in the first half of 2025, subject to customary closing conditions.
FDA has issued new guidance for the use of paclitaxel coated devices in peripheral arterial disease
The US Food and Drug Administration (FDA) has issued draft guidance that includes recommendations to support development and marketing of safe and effective artificial intelligence (AI)-enabled devices.
The guidance, if finalised, would be the first guidance to provide comprehensive recommendations for AI-enabled devices throughout the total product lifecycle, providing developers an accessible set of considerations that tie together design, development, maintenance and documentation recommendations to help ensure safety and effectiveness of AI-enabled devices, a recent press release states. This guidance complements the recently issued final guidance on predetermined change control plans for AI-enabled devices, which provides recommendations on how to proactively plan for device updates once the product is on the market.
“The FDA has authorised more than 1,000 AI-enabled devices through established premarket pathways. As we continue to see exciting developments in this field, it’s important to recognize that there are specific considerations unique to AI-enabled devices,” said Troy Tazbaz, director of the Digital Health Center of Excellence within the FDA’s Center for Devices and Radiological Health. “The draft guidance brings together relevant information for developers, shares learnings from authorised AI-enabled devices and provides a first point-of-reference for specific recommendations that apply to these devices, from the earliest stages of development through the device’s entire life cycle.”
The draft guidance includes recommendations for how and when, in marketing submissions, sponsors should describe the post market performance monitoring and management of their AI-enabled devices. The proposed recommendations reflect a comprehensive approach to the management of risk throughout the device total product life cycle. The FDA encourages sponsors to engage with the agency early and often, and to use this guidance, once finalised, to guide their activities throughout the life cycle of the device, including during planning, development, testing and ongoing monitoring.
Importantly, this draft guidance also includes the FDA’s current thinking on strategies to address transparency and bias throughout the life cycle of AI-enabled devices. The draft guidance describes specific recommendations intended to help a sponsor demonstrate they have addressed risks associated with bias and provides suggestions for the thoughtful design and evaluation of AI-enabled devices.
Notably, this announcement is specific to AI-enabled devices. This week, the FDA also published draft guidance with recommendations regarding the use of AI to support development of drug and biological products. The publication of the guidelines among other actions, continues to demonstrate the agency’s efforts to provide transparency and to help ensure product safety and effectiveness while supporting innovation in this rapidly growing field, the company states.
A recent analysis of over 270,000 Medicare fee-for-service beneficiaries has found an increase in adverse outcomes and death after a US Food and Drug Administration (FDA) warning led to decreased use of paclitaxel-coated devices for peripheral revascularisation procedures.
Writing in the Journal of the American College of Cardiology (JACC), a team of researchers from the Richard A and Susan F Smith Center for Outcomes Research at the Beth Israel Deaconess Medical Center (Boston, USA) begin by stating that peripheral revascularisation has faced “intense scrutiny” in the past decade.
The authors—Joseph M Kim and colleagues—first cite the impact of a 2018 meta-analysis associating paclitaxel-coated devices with increased mortality when used for peripheral revascularisation. The paper led the FDA to warn against routine use of such devices. It was not until 2023, the authors add, that the FDA reversed its warning following the publication of several further studies showing no mortality signal.
COVID-19 also impacted peripheral revascularisation, Kim et al continue, noting that the pandemic “complicated peripheral arterial disease (PAD) management by reducing access to patient care”.
To assess the impact of these events, the researchers conducted a study to evaluate trends in femoropopliteal revascularisation from 2016 to 2023 and to analyse safety outcomes during three key time periods: 1) before the paclitaxel safety concern; 2) after the onset of the paclitaxel safety concern; and 3) during and after the COVID-19 pandemic.
Kim and colleagues detail that their study included all Medicare fee-for-service beneficiaries aged ≥66 years who underwent femoropopliteal revascularisation by International Classification of Diseases-10th Revision codes between 1 January 2016 and 31 December 2023.
Regarding statistical analysis, the authors state that they examined trends of femoropopliteal artery revascularisation procedures by quarter year across the eight-year study period. Endovascular revascularisation procedures were stratified by percutaneous transluminal angioplasty (PTA) alone, drug-coated balloon (DCB) alone, bare metal stent (BMS) alone, or drug-eluting stent (DES) alone.
The study’s primary outcome was the composite of major amputation and all-cause mortality.
“During the study period, the number of endovascular revascularisation procedures declined 38.2%; the number of surgical revascularisation procedures declined 59.7%,” Kim et al report in JACC.
The authors share that PTA was the primary method (27.72%) used for endovascular revascularisation before the onset of the paclitaxel-coated device safety concern, followed closely by DCB (24.91%). After the paclitaxel safety concern, the use of DCBs declined to a low of 17.89% by 2019, with a proportional increase in the use of uncoated PTA (34.52%).
In addition, Kim and colleagues write that the proportion of DCB use increased after the onset of COVID-19. “By the time of the FDA’s reversal of its warning against routine use of drug-coated devices in 2023,” the authors continue, “DCB use had reached 23.46%.” They go on to note that the use of uncoated PTA stabilised at a proportion higher than was seen before the safety concern.
Furthermore, Kim et al reveal that revascularisations performed between the paclitaxel safety concern and the COVID-19 pandemic were associated with a higher rate of the primary outcome compared with procedures performed before the paclitaxel safety concern. They note that this was driven by increased risk of all-cause mortality.
“By contrast,” Kim and colleagues report, “there were lower rates of major amputation after the paclitaxel safety concern.”
“The paclitaxel safety concern sparked a rapid shift away from the use of paclitaxel-coated devices and toward the use of uncoated devices, particularly PTA,” the authors write in their discussion. “The use of DCBs has only recently regained some ground since its nadir in 2019, but their use remains remarkably low relative to PTA despite evidence supporting their superior efficacy and the FDA’s reversal of its warning against their routine use.”
Regarding limitations to their study, Kim et al recognise that claims data lack detailed anatomical and procedural information, and that the Medicare population “may not represent the US population at large, including those who are younger, are of minority background, or are privately insured”.
Eric Secemksy, senior author of the study, remarks on the significance of the findings: “This analysis is critical in informing how external events impact patient care. Between device safety concerns and the COVID-19 pandemic, treatment approaches changed dramatically for lower extremity interventions and patient outcomes were negatively impacted. How we approach existential threats to peripheral vascular care will require thought and caution, as informed by these novel data that were generously supported by the SCAI [Society for Cardiovascular Angiography and Interventions] Early Career Research Grant.”
Detailing the positive impact Allia IGS 7 has had on his daily practice, Vincent Vidal (Marseille, France) pinpoints usability, visualisation and radiation reduction as particular areas of marked improvement.
When performing cone beam computed tomography (CBCT) imaging prior to prostate artery embolization (PAE), Vidal describes how the system’s three-dimensional (3D) roadmap “fuses” with the captured image, reconstructing the patient’s intricate anatomy. In doing so, Vidal is able to ensure their targeting is “perfect” prior to treatment.
Previously, Vidal and his team state that, when they first began performing CBCT, they were concerned about radiation dose. With Allia IGS 7 however, he contends that image quality has not been compromised for dose reduction, which is due to the capabilities of the tools they have to their disposal.
Xeltis has announced the completion of enrolment in its EU pivotal trial for aXess, its restorative vascular access conduit, in adults with end-stage renal disease. The trial is taking place in 22 centres across Europe.
The aXess EU pivotal trial is a prospective study investigating the patency, safety, and performance of aXess in adult patients with end-stage renal disease requiring vascular access to start or maintain haemodialysis therapy. A total of 120 patients have been recruited across 22 centres in nine countries across Europe. This trial follows outstanding 12-month data from the first in human EU trial, which demonstrated a significant improvement in performance compared to current haemodialysis vascular access solutions and showed 0% (zero) infection rate.
Xeltis is currently enrolling up to 140 patients in the aXess US pivotal trial, with John Lucas III, surgeon at Lucas Surgical Group (Greenwood, USA), as the national principal investigator.
Loreto Gesualdo, principal investigator, Bari, Italy, commented: “I am very proud to be contributing to this EU pivotal trial, which is a vital step towards demonstrating the potential of aXess to transform patient outcomes for those with end-stage renal disease. Xeltis’ technology allows for the natural creation of living and long-lasting vessels, effectively addressing the issue of fistula non maturation, without the risk of reverting to catheter use. This results in an improved dialysis patient experience, a clear unmet medical need. We extend our thanks to the patients involved, who made it possible to advance this study.”
Paulo Neves, chief medical officer, Xeltis said: “The smooth completion of enrolment speaks to the promising medical profile of aXess and means we are one step closer to improving the standard of care for patients with end-stage renal disease. I look forward to the progress we are making as we advance towards CE approval. We are deeply grateful to the trial participants and all our investigators and study teams.”
Xeltis has also announced the addition of Rob Eyers to its team, bringing over three decades of in-depth experience in the cardiovascular medtech industry, in both corporate and start up environments. He joins from Veryan Medical where he served as CTO, having previously worked for CR Bard (now Medtronic), Merit Medical, Proxy Biomedical, and Boston Scientific. He has a proven track record of taking cardiovascular implant devices through regulatory approval to commercialisation, the company says in a press release.
Eyers, newly appointed chief technology officer, Xeltis said: “Xeltis’ novel Endogenous Tissue Restoration (ETR) technology sets a new benchmark for innovation in medical devices. Capable of regenerating a patient’s own tissue while avoiding the frequent reinterventions and infections associated with current treatment options, it has the potential to transform patient outcomes. The company is progressing rapidly towards commercialisation and delivering strong clinical results, and I am pleased to be joining such a dynamic team and continuing to build on this strong momentum to fast track regulatory approvals and contribute to the development of the platform.”
Stryker has announced a definitive agreement to acquire all of the issued and outstanding shares of common stock of Inari Medical for US$80 per share in cash, representing a total fully diluted equity value of approximately US$4.9 billion.
A Stryker press release notes that Inari, which was founded in 2011, will bring a leading peripheral vascular position in the fast-growing segment of venous thromboembolism (VTE) to Stryker. “Inari’s innovative product portfolio is highly complementary to Stryker’s Neurovascular business and includes mechanical thrombectomy solutions for peripheral vascular diseases such as deep vein thrombosis and pulmonary embolism,” the release reads.
“The acquisition of Inari expands Stryker’s portfolio to provide life-saving solutions to patients who suffer from peripheral vascular diseases,” said Kevin Lobo, chair and chief executive officer, Stryker. “These innovations elevate the standard of care for venous thromboembolism patients and will accelerate Stryker’s impact in endovascular procedures.”
“Inari has positively impacted the lives of hundreds of thousands of patients through the development of purpose-built tools that address unmet patient needs,” said Drew Hykes, chief executive officer, Inari. “With Stryker’s capabilities and global infrastructure, we will be even better positioned to accelerate the development of innovative new solutions and expand our footprint.”
Under the terms of the definitive agreement, Stryker shares that it will commence a tender offer for all outstanding shares of common stock of Inari for US$80 per share in cash. The boards of directors of both Stryker and Inari have unanimously approved the transaction. Consummation of the tender offer is subject to a minimum tender of at least a majority of then-outstanding Inari common shares, the expiration or termination of the waiting period under the Hart-Scott-Rodino Antitrust Improvements Act and other customary conditions. Following successful completion of the tender offer, Stryker will acquire all remaining shares not tendered in the offer through a second step merger at the same price as in the tender offer.
Stryker advises that the transaction is anticipated to close by the end of the first quarter of 2025, subject to customary closing conditions. Expected impacts to 2025 financial results will be discussed on Stryker’s upcoming fourth quarter 2024 earnings call scheduled for 28 January 2025.
Merit Medical Systems announced today that the Wrapsody cell-impermeable endoprosthesis has received premarket approval from the US Food and Drug Administration (FDA). With this approval, a press release notes, Merit can begin commercialisation of the device in the USA in 2025.
The company details that Wrapsody is designed to extend long-term vessel patency in dialysis patients. “Preserving vascular access for dialysis patients is critical for them to maintain lifesaving treatment,” said Bart Dolmatch (Palo Alto Medical Foundation, Palo Alto, USA), who is credited as co-inventor of the Wrapsody device, in a Merit press release. “I believe the advancements that the Wrapsody device offers will translate to better outcomes for haemodialysis patients.”
The Wrapsody cell-impermeable endoprosthesis consists of a proprietary covering that features a nitinol stent frame enveloped by an expandable polytetrafluoroethylene (ePTFE) outer layer, an inner-luminal layer of novel “spun” PTFE designed to reduce platelet and fibrin formation, and a middle cell-impermeable layer designed to prevent transgraft tissue migration or accumulation. Merit claims that the nitinol frame provides enhanced radial force, compression resistance, and softened ends to help the device conform to vessels, withstand physiological compression, and reduce stress on vessel walls.
Results from the WRAPSODY WAVE pivotal trial demonstrated that arteriovenous (AV) fistula and AV graft patients receiving treatment with the Wrapsody device for dialysis outflow lesions achieved a target lesion primary patency of 89.8% and 82%, respectively, at six months. The primary patency of the entire access circuit at six months in patients with an AV fistula and AV graft were 72.6% and 68.8%, respectively.
“Historically, interventions for patients who experience a stenosis in their AV fistula or AV graft have not provided sustained clinical benefits and often require multiple reinterventions,” said Mahmood K Razavi (St Joseph Heart and Vascular Center, Orange, USA), co-principal investigator of the WAVE trial. “Results from the WAVE trial have demonstrated that the Wrapsody device is associated with high patency rates and is likely to become the new standard of care.”
“Over the past decade, Merit has worked to ensure that the Wrapsody device helps physicians achieve the best possible outcomes for patients,” said Fred P Lampropoulos, Merit’s chairman and chief executive officer. “We are proud to design and deliver such an innovative solution that has demonstrated the highest efficacy to date.”
Data from a new study have found that venous leak embolization yields additional clinical improvement and treatment potential in patients with vasculogenic erectile dysfunction (ED) resistant to phosphodiesterase-5-inhibitors (PDE5i) due to mixed arterio-venous disease. These findings were recently published in the journal CardioVascular and Interventional Radiology (CVIR).
The single-centre observational study was led by Nicolas Diehm (Vascular Institute Central Switzerland, Aarau, Switzerland) et al, who collected data from 26 patients treated at their institution between October 2019 to September 2022. All patients were diagnosed with ED resistant to PDE5i without significant clinical benefit following arterial revascularisation of erection-related arteries.
In their description of the study, Diehm and colleagues write that endovascular therapy of vasculogenic ED has recently made “significant progress”, and while several studies have investigated clinical outcomes following either arterial revascularisation or venous embolization, data on combined arterio-venous diseases are “scarce”.
The study authors outline that the combination of arteriogenic and venogenic ED may be prevalent in a subset of patients. They describe that arteriogenic ED is often caused by atherosclerosis triggered by cardiovascular risk factors leading to narrowing of the erection-related arteries. Venogenic ED, however, is caused by incomplete relaxation of cavernosal smooth muscle cells during arterial inflow and subsequent failure to occlude the penile venous outflow tracts.
Thus, to investigate the potential combination of therapies, Diehm and colleagues performed 807 procedures—663 arterial and 144 venous interventions. Technical success for arterial revascularisation was defined as successful vascular access and completion of the endovascular procedure and immediate morphological success with less than 30% residual diameter reduction. Technical success after venous embolization was defined as complete target vein embolization.
Procedural success was achieved in all patients with no major adverse events at six-month follow-up. The primary feasibility endpoint was defined as an International Index of Erectile Function-6 (IIEF-6) score improvement of ≥4 points at six-week follow-up post intervention, which was achieved in three of the 26 (11.5%) patients following arterial revascularisation only. Following an additional venous embolization performed 458±424 days after the initial arterial procedure, the authors report that the primary feasibility endpoint was reached in 17 of 26 (65.4%) patients.
In addition to the IIEF-6 score, Diehm et al also requested patients complete the global patient impression of improvement (PGI-I) questionnaire six weeks post intervention. This showed that two (8%) patients with mixed arterio-venous ED had improved post arterial revascularisation alone, whereas 24 (92%) patients had no change or experienced deterioration. Following the additional venous embolization, 15 (57.5%) patients had improved, nine (34.6%) experienced no change and two (7.7%) had deteriorated when compared with baseline. In addition, at six weeks follow-up, 18 (69.2%) patients stated that they would undergo the endovascular procedures again.
In their discussion of the results, Diehm and colleagues note that a staged combined treatment approach for mixed-arterio ED was “safe and feasible”, highlighting the clinical improvement rate of 65.4% in patients who initially failed to respond to arterial ED treatment alone. The authors determine that their results show that venous leak embolization has potential to further improve clinical outcomes in patients with severe ED who have not responded to arterial revascularisation.
In their conclusory statement, Diehm et al write that their all-comers feasibility study is limited by the relatively small number of patients enrolled with short follow-up. Further, they state that more stringent exclusion criteria may yield better outcomes in future studies in this area, as, in the current cohort, patients with comorbidities such as diabetes mellitus were not excluded.
Biotronik announced this week that it has enrolled the first patients in its BIO-OSCAR FIRST trial, a study designed to confirm the safety and clinical performance of the Oscar peripheral multifunctional catheter for dilation of lesions in the femoral, popliteal and infrapopliteal arteries, including both above-the-knee (ATK) and below-the-knee (BTK) lesions.
The BIO-OSCAR FIRST trial is a prospective, multicentre, single-arm observational study involving 16 European sites within CE mark-accepting territories. Over the next 12 months, the trial aims to enrol 200 patients—100 for ATK and 100 for BTK lesions. This study is designed to evaluate Oscar’s performance in a practical clinical setting.
“The Oscar catheter design holds exciting possibilities for peripheral arterial disease (PAD) care, particularly in the more challenging cases,” says Koen Deloose (AZ Sint Blasius Hospital, Dendermonde, Belgium). “This trial will provide key data on how we can better streamline procedures, assess the algorithm of treatment and reduce the need for reinterventions.”
The first patients were included in the trial by Deloose and Marianne Brodmann (Medical University of Graz, Graz, Austria).
The primary endpoint of the study is the Oscar device procedural success rate, which is defined by successful lesion crossing and a residual stenosis of ≤30%, without significant Oscar-related procedural complications such as distal embolisation, vessel rupture, perforation, or acute occlusion.
“With the BIO-OSCAR FIRST study, we’re looking to validate Oscar’s potential to simplify complex interventions while confirming safety and efficacy,” says Stuart Perks, Vice President at Biotronik Vascular Intervention. “Many physicians have reported excellent procedural outcomes with Oscar. Our focus now is to generate the hard clinical evidence to support clinicians’ decision-making and the care they deliver to their patients.”
A company press release details that the Oscar device is an all-in-one solution indicated for femoral, popliteal and infrainguinal lesions. The Oscar support catheter and dilator are used in tandem to enable lesion access and crossing with a compatible guidewire, offering a range of support strength dependent on the extension of the dilator.
FastWave Medical has announced the close of a US$19 million funding round earlier this year, increasing the total capital invested into the company to over US$40 million.
This investment round was led by Epic Venture Partners with participation from M&L Healthcare Investments and the company’s existing investors, and looks to develop FastWave’s ongoing regulatory and clinical initiatives of its portfolio of intravascular lithotripsy (IVL) platforms.
FastWave Medical co-founder and chief executive officer Scott Nelson expressed the team’s excitement: “We are beyond thrilled to partner with physician-led investors like Epic and M&L who see the clinical promise and commercial viability of both our IVL systems. This round of stage-appropriate funding is a testament to the confidence the market has in our approach and takes us one step closer to our goal of empowering interventionalists across the world with next-level IVL therapies.”
Since its formation in 2021, FastWave has been moving in its efforts to tackle the challenges of artery calcification with IVL solutions. As the global population ages, the demand for effective, minimally invasive treatments is escalating. In a recent press release, FastWave have stated that its commitment to providing physicians with highly deliverable IVL catheters that offer durable, 360-degree sonic output has led to the rapid development of a pipeline of IVL systems that hold the potential to positively impact patient care.
“On every metric, FastWave’s pace of innovation stands out,” said Bryan Edelstein, managing partner of Epic Venture Partners. “We are excited to be a part of helping FastWave build on their impressive cadence to reach the company’s next key clinical and regulatory initiatives.”
Arthur Lee, managing partner of Epic Venture Partners, added: “FastWave is moving quickly and decisively to become best-in-class in the IVL space. We are excited to support the FastWave team, as they continue to take down milestone after milestone in their mission to save lives and offer this groundbreaking technology to all who need it.”
Steven Kum, chief medical officer of M&L Healthcare Investments, holds similar optimism: “FastWave Medical has all the hallmarks of a company poised for significant growth and impact. Their commitment to evidence-based development aligns perfectly with our investment philosophy, and we’re excited to be a part of a new era of IVL innovation that addresses the gaps left by current technologies.”
Boston Scientific today announced the appointment of Kathleen Van Vlierberghe as the new vice president for the Peripheral Interventions division in Europe, Middle East and Africa (EMEA), effective 1 December 2024.
A news story on the company’s website details that Van Vlierberghe brings over 25 years of experience to her new position, having held various leadership roles across sales and marketing in the healthcare industry, including 19 years working at Boston Scientific.
Most recently, she led the Healthcare Solutions & Partnerships (HS&P) and Inside Sales division at Boston Scientific in EMEA, developing services and solutions that directly address some of the most pressing challenges in healthcare systems.
“I am excited to take on the challenge of leading the Peripheral Interventions business in EMEA,” said Van Vlierberghe. “It’s a privilege to be part of a company whose innovative solutions have helped transform the way healthcare professionals diagnose and treat people with vascular conditions and cancer, resulting in improved outcomes and quality of life, and reduced costs for healthcare services. I look forward to working collaboratively with the Peripheral Interventions team and other colleagues at Boston Scientific to make a positive difference to our customers and the patients they serve.”
A minimally invasive procedure provides significant relief from knee pain and may prevent the need for knee replacement surgery in people with osteoarthritis, according to a study presented at the Radiological Society of North America (RSNA) annual meeting (1–5 December, Chicago, USA).
“This study addresses osteoarthritis, which is a significant public health issue and the leading cause of chronic pain and disability worldwide,” said the study’s lead author and interventional radiologist, Florian Nima Fleckenstein (Charité University Hospital Berlin, Berlin, Germany). “With millions of people affected by knee osteoarthritis, particularly in aging populations, finding effective, minimally invasive treatments is critical.”
Osteoarthritis, a chronic, degenerative and progressive condition, is the most common cause of chronic joint disorders. According to the World Health Organization (WHO), knee osteoarthritis affects over 365 million adults worldwide.
Most available therapies, such as pain medication and steroid injections, only mask the symptoms of osteoarthritis. They don’t slow progression of the disease. As osteoarthritis worsens and conservative treatments become ineffective, many people turn to joint replacement surgery.
Genicular artery embolization (GAE) is a minimally invasive therapy for patients with symptomatic knee osteoarthritis. The genicular arteries have several branches that form a network around the knee joint. These vessels are altered in patients suffering from osteoarthritis. In GAE, an interventional radiologist injects small particles into selected branches that correspond to the site of knee pain to block blood flow to that area. Embolization of the abnormal blood vessels helps to disrupt the cycle of inflammation, cartilage destruction and sensory nerve growth that characterises osteoarthritis.
For the study, Fleckenstein and colleagues conducted a retrospective analysis of 403 cases from patients (aged 40 to 90) with moderate to severe knee osteoarthritis that didn’t respond to conservative treatments. All patients underwent GAE at the Charité University Hospital Berlin. The study was designed to evaluate both the safety and efficacy of GAE across a broad spectrum of osteoarthritis severities. The effectiveness of the procedure was measured using the Visual Analog Scale and the Knee Injury and Osteoarthritis Outcome Score. These standardised scores, which measure pain and quality of life (QoL), were recorded at baseline and during follow-up visits at six weeks, three months, six months and one-year post procedure.
Technical success was achieved in 100% of procedures. Temporary slight skin discoloration and mild knee pain immediately after the procedure were noted in 18% of all cases. No severe complications were reported. The QoL index and pain score improved by 87% and 71%, respectively, at one-year follow-up.
The findings show that GAE is a safe and effective treatment option across all severity grades of knee osteoarthritis, including advanced cases where other treatments have very limited efficacy.
“Our study found that GAE can effectively reduce knee pain and improve quality of life early after the treatment, with these benefits being maintained over the long term, especially for people who haven’t had success with other treatments like physical therapy or pain medications,” Fleckenstein said. “This could potentially offer a new lease on life for many patients who suffer from debilitating pain and mobility issues caused by osteoarthritis.”
The study also showed that GAE is particularly effective in the early stages of knee osteoarthritis. This indicates that early intervention could potentially delay or even prevent disease progression, reducing the need for more invasive treatments, such as surgery.
The researchers hope that by demonstrating the procedure’s success in a large and diverse patient population, the study could influence medical practice and policy, encouraging broader adoption of GAE in clinical settings worldwide.
“GAE has the potential to reduce the need for more invasive surgeries, lower health care costs and significantly improve the quality of life for countless individuals suffering from knee osteoarthritis,” Fleckenstein said.
He and his team plan to continue their research on degenerative joint disorders to provide patients with new options in the field of interventional radiology.
Sensome today announced positive results from two studies of its Clotild smart guidewire system demonstrating its ability to successfully identify fresh clot—thrombus rich in red blood cells (RBCs)—in peripheral arterial disease (PAD) and differentiate it from other tissue encountered during PAD procedures. Results from the SEPARATE and E-SEPARATE studies were presented at the Paris Vascular Insights (PVI) course 2024 (12–14 December, Paris, France).
A press release details that the Clotild clot-sensing guidewire integrates the world’s smallest electrical impedance sensor with machine learning. For PAD, the clot-sensing technology is being developed to instantly identify fresh clot and differentiate it from organised clot as well as plaque, calcium and other tissue in real-time in order to inform individualised PAD treatment. Sensome notes that the technology can be integrated into devices commonly used during PAD procedures, such as guidewires and catheters, and has the potential to enable the first device capable of objectively identifying fresh clot during a procedure without changing current workflow.
The prospective, single-arm SEPARATE study encompassed 17 patients treated by Koen Deloose (AZ Sint Blasius Hospital, Dendermonde, Belgium). The study showed in a post-procedure analysis that there was a high level of agreement between the technology’s identification of fresh clot, the expert’s assessment of fresh clot and the treatment decisions appropriate for fresh clot.
“Differentiating among tissues in an obstructed vessel in order to achieve successful peripheral revascularisation is often limited by indistinct angiographic imaging, inaccurate patient medical history and a lack of tactile guidewire feedback. The SEPARATE study shows us that Sensome’s clot-sensing technology could become a novel, real-time modality to reliably identify fresh clot at an expert level in interventional procedures, with the potential to improve vessel preparation and treatment decision-making for physicians of all experience levels treating PAD,” said Deloose.
A second study of the Sensome technology—E-SEPARATE—was conducted with 15 PAD patients (scheduled for amputation or bypass) at a single centre in France and had two interesting findings, according to a press release. The study showed the technology’s ability to differentiate fresh clot from other tissue collected from these PAD patients and examined ex vivo. It also demonstrated an excellent correlation between the technology’s ability to determine the RBC content of clots collected from PAD patients with subacute and chronic lesions, and a histological analysis of the same clot by an outside core lab.
“The E-SEPARATE study findings clearly demonstrate that symptom onset is an unreliable way to judge clot composition prior to treating a patient with PAD. The clots retrieved from both chronic and subacute lesions contained both RBC-rich fresh clot and organised RBC-poor clots. In light of this, it’s important for us to know the clot type to decide how to treat these patients…do we aspirate, dissolve the clot, or use another method? The Sensome technology has the potential to provide us with important information we are missing today to more effectively guide treatment and achieve better patient outcomes,” said Yann Gouëffic (Groupe Hospitalier Paris Saint-Joseph, Paris, France).
In two previous peer-reviewed publications, the company’s microsensor technology was shown to reliably predict the composition of RBCs in retrieved clot with good sensitivity and specificity consistent with histologic findings.
Koen Deloose presents BIO-OSCAR SOC data at PVI 2024
Biotronik today announced that it has concluded the BIO-OSCAR SOC study evaluating the baseline against which to measure the Oscar multifunctional catheter in treating complex peripheral arterial disease (PAD). The outcomes were presented at the Paris Vascular Insights (PVI) course 2024 (12–14 December, Paris, France) by principal investigator Koen Deloose (AZ Sint Blasius Hospital, Dendermonde, Belgium).
BIO-OSCAR SOC is a prospective, multicentre, observational trial assessing the current standard of care, procedural outcomes, complication handling and device use in endovascular treatments for atherosclerotic lesions both above the knee (ATK) and below the knee (BTK).
The study analysed data from 247 patients across 16 European CE-mark territories, aiming to deliver insights into real-world practices for managing PAD.
“BIO-OSCAR SOC is an important step toward understanding the treatment of complex infrainguinal lesions under current standard-of-care practices, and especially how important vessel preparation can be,” Deloose remarked in a press release announcing the results. “With this baseline study, we aim to evaluate [how] the Oscar catheter can streamline procedures by minimising the need for multiple device exchanges, reducing procedural steps, and lowering complications.”
The primary endpoint of BIO-OSCAR SOC was procedural success, defined as a combination of technical success—achieving ≤30% residual stenosis following vessel preparation and prior to the definitive treatment—and the absence of complications such as target-vessel perforation, rupture, acute occlusion, or distal embolisation.
The outcomes, as outlined in the press release, show:
50% procedural success in ATK and 59% in BTK lesions.
94% crossing success in chronic total occlusions (CTO) for ATK and 90% for BTK.
50% bailout stenting rate in ATK cases, highlighting that vessel preparation is often insufficient. Biotronik notes that appropriate vessel preparation may significantly improve short- and long-term outcomes.
The procedural cost related to access, crossing and vessel preparation averages €750, while for complex cases the cost can go up to €1,100.
Biotronik shares that the clinical evidence will be further validated by the BIO-OSCAR FIRST study, which is designed to confirm the safety and clinical performance of the Oscar catheter for dilation of lesions in the femoral, popliteal, and infrapopliteal arteries, including both ATK and BTK lesions.
“This study provides the vascular community with valuable insights into existing procedural success rates and cost-efficiency data,” said Stuart Perks, vice president marketing at Biotronik Vascular Intervention. “BIO-OSCAR SOC is pivotal in validating Oscar’s role in improving the standard of care for PAD and optimising treatment strategies for patients with complex lesions.”
A press release summarises that the BIO-OSCAR SOC study establishes the baseline of standard of care, which will be used to evaluate the outcomes of the BIO-OSCAR FIRST study.
In November, the most read stories from Interventional News included a profile of current Society of Interventional Oncology (SIO) president, Muneeb Ahmed (Beth Israel Deaconess Medical Center, Boston, USA); an update on liquid biopsy and its application in interventional radiology practice according to Bruno Damascelli (Fondazione Falciani ONLUS, Milan, Italy) et al; and two-year SPYRAL HTN-ON MED results regarding renal denervation.
Andreas Adam, emeritus professor of interventional radiology at King’s College London, UK and joint editor-in-chief of Interventional News, writes on his path to becoming an interventional radiologist: “I became an interventional radiologist by accident. As a resident in cardiology, I had an unusual chief: he belonged to a new breed of cardiologists…”
Tracing back his line to interventional radiology (IR), Muneeb Ahmed, interventional radiologist and the current president of the Society of Interventional Oncology (SIO), told Interventional News of how he followed in the footsteps of his father, Rashid Ahmed, an influential interventional radiologist who propelled the field in Pakistan.
iVascular has announced the initiation of Opal, the first-in-human study with the new embolic liquid Amber, based on a radiopaque biocompatible copolymer. Opal is a prospective, single-arm, multicentre study with a sample size of 70 patients requiring peripheral embolization. The study is a collaboration between 10 centres in Spain that specialise in embolization and will be led by Fernando Gómez (Hospital La Fe, Valencia, Spain).
Boston Scientific has announced it has entered into a definitive agreement to acquire Intera Oncology. Intera Oncology’s Intera 3000 hepatic artery infusion pump has been approved by the US Food and Drug Administration (FDA) and is used to administer hepatic artery infusion (HAI) therapy to treat tumours in the liver primarily caused by metastatic colorectal cancer.
Where is liquid biopsy today? Bruno Damascelli, Vladimira Tichà, Giancarlo Beltramo, Alberto Gramaglia and Gianluigi Patelli write on the complexities and challenges of the procedure as it gains ground among select interventional radiologists.
Medtronic has announced new, long-term data from the SPYRAL HTN-ON MED clinical trial that showed subjects who underwent radiofrequency renal denervation with the Symplicity Spyral renal denervation system had significantly greater reductions in 24-hr ambulatory systolic blood pressure, and office-based systolic blood pressure compared to sham patients at two years.
In a paper published last month in the journal CardioVascular and Interventional Radiology (CVIR), Matthew Lukies and colleagues from Alfred Health in Melbourne, Australia have released data collected from their institution giving visibility to the clinical interventional radiology (IR) service that they state has gone largely unnoticed.
Interventional radiology (IR) was officially recognised as a primary medical specialty in the USA by the American Board of Medical Specialties (ABMS) in 2012. This marked a significant milestone for the field, which had previously been considered a subspecialty of diagnostic radiology (DR). With 12 years of specialty distinction, Interventional News spoke to Parag Patel (Medical College of Wisconsin, Milwaukee, USA) who debriefed on their progress so far.
Presented today, late-breaking data from the second year of the LIFE-BTK clinical trial demonstrate the long-term effectiveness of the US Food and Drug Administration (FDA)-approved Esprit BTK everolimus-eluting resorbable scaffold system (Abbott Vascular) in patients with the most severe form of below-the-knee (BTK) peripheral arterial disease (PAD). The data show that the Esprit BTK offers sustained benefits over balloon angioplasty with fewer repeat procedures at two years.
Fluidx Medical has announced that the first patient has been treated in the GPX investigational device exception (IDE) prospective multinational clinical trial. The GPX embolic device was successfully used in a portal vein embolization procedure in preparation for hepatic resection.
AngioDynamics has announced that it has received US Food and Drug Administration (FDA) 510(k) clearance for the NanoKnife system for prostate tissue ablation.
The company received clearance for the NanoKnife System for prostate tissue ablation following the completion of the pivotal PRESERVE clinical study and submission of results to the US FDA in September. The study evaluated the safety and effectiveness of the system for ablating prostate tissue in patients with intermediate-risk prostate cancer (PCa). Conducted in collaboration with the Society of Urologic Oncology Clinical Trials Consortium (SUO-CTC), Preserve enrolled 121 patients across 17 clinical sites.
“We are incredibly proud to receive US FDA clearance for the NanoKnife system’s use in prostate tissue,” said Jim Clemmer, president and chief executive officer of AngioDynamics. “This milestone is the first step in recognising our vision to become the standard, function-preserving treatment for men with prostate tumours. The NanoKnife System minimises the life-altering complications often associated with traditional treatments by selectively targeting prostate tissue while preserving critical functions. As we expand our global footprint and increase access to our technology, we are launching comprehensive education and awareness campaigns to empower physicians with hands-on training and clinical support while engaging patients through innovative outreach initiatives.”
Clemmer added: “These efforts are designed to accelerate the adoption of the NanoKnife System, redefine the standard of care for prostate health, and deliver treatment outcomes that patients and physicians need. AngioDynamics is committed to driving meaningful impact through this revolutionary technology, providing new hope to patients and improved quality of life.”
The Preserve clinical study met its primary effectiveness endpoint demonstrating the performance of the NanoKnife System for the ablation of prostate tissue in patients with intermediate-risk PCa. At 12-months post-procedure, 84% of men were free from in-field, clinically significant disease. In addition, the study demonstrated strong quality-of-life outcomes with short-term urinary continence being preserved (96.6% at baseline, 95.4% at 12-months) and the ability to maintain erections sufficient for intercourse only decreasing 9% compared to baseline (80.7% to 71.7%).
The study’s results validated the robust safety and clinical efficacy profile of the NanoKnife System, reinforcing findings from more than 32 clinical studies performed around the world involving over 2,600 patients.
Prostate cancer is the second most common cancer in men worldwide, with approximately 1.5 million new cases diagnosed annually. Many of these patients seek alternatives to radical procedures that can lead to significant, long-term urological side effects. The NanoKnife system is the first non-thermal, radiation-free, ablation technology designed to treat prostate tissue by using irreversible electroporation (IRE) technology, offering patients a minimally invasive option for prostate treatment.
The NanoKnife system delivers an alternative to conventional radical surgery or radiotherapy, which often results in significant dysfunction in urinary continence and erectile potency. With its non-thermal approach, the system is engineered to preserve vital structures inside and outside the prostate, offering patients improved outcomes, reduced recovery times, and enhanced quality of life.
The Society of Interventional Radiology (SIR) has announced that Charles E Ray Jr (University of Utah School of Medicine, Salt Lake City, USA), past president of SIR, and Brian F Funaki (The University of Chicago Medical Center, Chicago, USA), past chair of the SIR annual scientific meeting, have been selected as the incoming co-editors-in-chief of SIR’s flagship publication, the Journal of Vascular and Interventional Radiology (JVIR).
This editorship represents the first time in JVIR history that the role will be shared between two editors-in-chief. Ray and Funaki will officially begin their roles in January 2026, as outgoing editor-in-chief Daniel Y Sze (Stanford University, Stanford, USA) concludes his term of visionary leadership for the journal.
“Our wide-ranging search yielded a robust pool of applicants with a clear vision for solidifying JVIR as the home of interventional radiology research, and we are pleased that Ray and Funaki have agreed to join forces to provide their expertise and insights as the co-editors-in-chief of JVIR,” said Alda L Tam (MD Anderson Cancer Center, Houston, USA) chair of the search committee and immediate past president of SIR. “This co-editorship will allow JVIR to continue its 34-year tradition of publishing gold-standard interventional radiology research, while also accommodating a growing number of submissions each year.”
“JVIR has long stood at the pinnacle of interventional radiology research publishing and, together, Funaki and I look forward to identifying and publishing the work that will be most impactful to improving patient care over time,” said Ray.
“Interventional radiology has always been on the leading edge of innovation in medicine, and this new co-editorship will help us define that leading edge of the best research the specialty has to offer, in formats that have proven most valuable to the community,” said Funaki.
SIR thanks Sze for his transformative leadership and the JVIR editor-in-chief search committee for its time and dedication.
Cook Medical has announced a strategic investment in the urology space via Zenflow, a medical device company developing a minimally invasive treatment for urinary obstruction caused by enlarged prostate, or benign prostatic hyperplasia (BPH).
“This investment reflects our confidence in the future of Zenflow and the Spring System technology. Zenflow is aligned with our core focus of developing minimally invasive technologies that restore flow,” said DJ Sirota, senior vice president of Cook Medical’s MedSurg division. “This type of agreement is yet another proof point to how Cook is changing to focus on our future as product innovators.”
With funding led by Cook, Zenflow closed an US$24 million series C financing round last month and included participation from existing investors Invus Opportunities, F-Prime Capital, Medical Technology Venture Partners and others.
Funds will be used to support the company’s pre-market approval (PMA) submission as well as to prepare for commercialisation in order to set the stage for US Food and Drug Administration (FDA) approval of its Spring System, a minimally invasive treatment option for patients who suffer debilitating symptoms due to an enlarged prostate. The Spring System relies on a small spring-like coil to prop open the urethra, restoring its normal function while preserving the natural anatomy.
IceCure Medical has today announced interim results from the company’s Icesecret study of cryoablation for patients with small renal masses who cannot be offered kidney preserving surgery. Data were presented on at the Israeli Urological Association conference (2–5 December, 2024, Eilat, Israel). These data were delivered by Keren Boguslavsky (Bnai Zion Medical Center, Haifa, Israel).
Results were reported at a mean follow-up period of 36 months for 111 patients with 117 lesions. Boguslavsky reported that, in 91 patients (approximately 82%), no tumour recurrence was observed. Following an additional cryoablation procedure for the same tumour in 13 patients, the success rate for the overall population was 83.8%, with a mean follow-up time of 39.6 months. In patients without a history of kidney cancer with one tumour <3cm, the success rate was 88.7%.
Freezing of the renal tumour—with a safety margin of 0.5cm—was achieved in 95.6% of the procedures demonstrating high efficacy in cases without anatomic limitation for ice ball creation.
Four procedure-related serious adverse events were reported, three of which were mild and treated conservatively. One severe complication was observed seven months after the cryoablation procedure. Renal function was preserved on an average basis across the patient cohort, with no significant change in creatinine and haemoglobin levels compared to baseline, the authors have stated.
The procedure time, relative to the standard of care as supported by and documented in medical literature, was approximately 25 minutes.
“The ability to offer cryoablation for kidney cancer is a large unmet need, particularly in patients who are ineligible for kidney preserving surgery. We are very pleased that Icesecret’s latest interim results present ProSense as a safe and effective option for these patients. These results are particularly important since ProSense is already approved for the as a cryosurgical tool in the destruction of malignant and benign tumours of the kidney in key markets including the USA and Europe,” stated IceCure’s chief executive officer, Eyal Shamir.
In a recent press release the company state that, according to the American Journal of Roentgenology, small renal masses, which may be malignant or benign tumours in the kidney, have been increasing in incidence over the past two decades. According to the American Cancer Society, in 2024, in the USA, an estimated 81,610 new cases of kidney cancer will have been diagnosed, with approximately 14,390 dying from the disease. Globally, there were more than 434,000 new cases of kidney cancer in 2022 and about 156,000 deaths according to World Cancer Research Fund International.
Centerline Biomedical has announced that it has received the US Food and Drug Administration (FDA) 510(k) approval for its new Intra-Operative Positioning System (IOPS) guidewire handle.
The IOPS guidewire handle is a second-generation device and the most recent addition to the company’s patented IOPS technology portfolio.
It is designed for use with the company’s sensor IOPS guidewire and new Viewpoint catheter to support three-dimensional (3D) navigation of a patient’s vasculature.
When used together with the algorithms of the IOPS software, clinicians can visualise the device in real time, significantly reducing the dependence on fluoroscopy during procedures.
Centerline founder and chief technology officer Vikash Goel said: “Centerline began with a focus on directly addressing clinicians’ needs and we continue to evolve it based on our experience in the field. Clearance for the new IOPS Guidewire Handle comes on the hVieweels of the launch of our next-generation Viewpoint catheter and our sixth software release. I couldn’t be more thrilled with our innovative product development team as they continue to advance the IOPS platform.”
According to the company, clinicians depend on fluoroscopy or live X-ray during endovascular procedures, to visualise medical devices inside the body.
Centerline has said that its IOPS device prevents the need for prolonged fluoroscopy during endovascular procedures to ensure the safety of clinicians and patients.
IOPS enables multicolour 3D visualisation of the arteries and their branches before, during, and after stent graft placement. The device provides vascular mapping with colourful, 3D images showing the fine features of diseased arteries, which are not visible with traditional 2D grayscale X-ray fluoroscopy.
Furthermore, the new software features that are offered only through IOPS will help create and display 3D wireframe vessel models for procedure mapping, said Centerline.
The Society of Interventional Radiology (SIR) has announced that Eve Lee, executive director at the American Orthotic and Prosthetic Association (AOPA), will join the organisation on 27 January, 2025, as its new chief executive officer.
In this role, Lee will advance SIR’s advocacy, education and policy mission to strengthen and support the practice of interventional radiology (IR) and ensure patient access to minimally invasive, image-guided therapies. She will also work to advance the goals of SIR Foundation as they pertain to research and fundraising.
“I am thrilled and honoured to join SIR as it begins its 50th anniversary year,” said Lee, “I look forward to building upon SIR’s strong foundation of advocacy, education and research to ensure greater access to interventional radiology care around the world.”
At AOPA, Lee championed patient access to care, spearheaded evidence-based advocacy, formed strategic collaborations, fostered global outreach efforts and strengthened AOPA’s role as a leading voice in healthcare policy. Before AOPA, she led the Society for Healthcare Epidemiology of America (SHEA) as its executive director. Under her leadership, SHEA became a recognised leader in infection prevention and public health policy, collaborating with agencies like the Centers for Disease Control and Prevention and the Food and Drug Administration to tackle pressing healthcare challenges.
“We are excited to welcome Lee to SIR at this pivotal moment in our history,” said SIR president Robert J Lewandowski (Feinberg School of Medicine, Chicago, USA). “SIR’s leadership is confident her experience as a champion of patient access to care, evidence-based medicine and public health policy will help SIR reach new heights and make our next 50 years as transformative as the first.”
Lee holds an MBA from the University of Maryland Global Campus—an online public university—a certificate in higher education teaching from Harvard University and an undergraduate degree in political science from Randolph-Macon College, Ashland, USA.
Terumo Interventional Systems announces the launch and commercial availability of its NaviCross peripheral support catheter in the USA, further expanding the company’s radial-to-peripheral (R2P) portfolio.
The R2P NaviCross catheter is now available in a 200cm length and is a double-braided, stainless-steel construction engineered for trackability and torque control for lesion crossing in complex procedures, a press release states.
“Our customers have been asking for a longer length, high-performance NaviCross support catheter, and I am proud to say we answered the need by delivering R2P NaviCross to the market, further enhancing our radial-to-peripheral portfolio,” said Ghada Farah, division president, Terumo Interventional Systems. “R2P NaviCross solidifies Terumo’s leadership in radial access, particularly as the demand for procedures to treat peripheral artery disease (PAD) and critical limb ischaemia continues to rise.”
“With the 200cm length, the R2P NaviCross catheter provides physicians performing percutaneous transluminal endovascular procedures from the radial artery a valuable tool to enhance their ability to safely and efficiently complete more procedures from a radial approach,” said Michael J Martinelli, chief medical officer, Terumo Medical Corporation. “Additionally, the double-braided, stainless-steel design of the R2P NaviCross catheter makes it possible to access and cross simple-to-complex lesions above and below the knee.”
Delcath Systems has announced that the US Food and Drug Administration (FDA) has completed its 30-day review of the company’s investigational new drug (IND) application for a phase two clinical trial evaluating Hepzato in combination with standard of care for liver-dominant metastatic colorectal cancer (mCRC). With the US FDA’s review completion, Delcath Systems is now authorised to initiate patient enrolment, a press release states.
The trial will evaluate the safety and efficacy of Hepzato in combination with trifluridine-tipiracil and bevacizumab compared to trifluridine-tipiracil and bevacizumab alone in patients with liver-dominant mCRC receiving third-line treatment. Approximately 90 patients will be enrolled in the randomised controlled trial. The study will take place at more than 20 sites across the USA and Europe, with patient enrolment expected to begin in the second half of 2025. The trial’s primary endpoint, hepatic progression-free survival (hPFS), is anticipated to read out by the end of 2027, while overall survival (OS), a secondary endpoint, is expected in 2028.
The company estimates that the total addressable market for liver-dominant mCRC receiving third-line treatment is between 6,000 and 10,000 patients annually in the USA. This market includes patients who present with significant liver disease burden, with liver-dominant status determined through radiological and clinical criteria. By targeting this patient population, Delcath Systems aims to provide a novel treatment option for those with limited therapeutic alternatives.
“This phase two trial represents an exciting step forward in evaluating Hepzato as a treatment for patients with liver-dominant metastatic colorectal cancer,” said Gerard Michel, chief executive officer of Delcath Systems. “The study reflects our commitment to expand the potential applications of Hepzato beyond metastatic uveal melanoma, offering new hope to an additional group of patients with liver dominant cancers.”
Inari Medical has announced that it received national reimbursement approval from the Japanese Ministry of Health, Labor and Welfare (MHLW) for its ClotTriever thrombectomy system for deep vein thrombosis (DVT).
A recent press release states that, due to ClotTriever’s mechanism of action for wall-to-wall thrombus removal in patients suffering from DVT, the MHLW have created a new functional category that is separate from other catheter-based therapies. This new functional category comes with a reimbursement premium based on clinical data showing the system’s efficacy in removing various types of thrombi.
To facilitate commercialisation of the ClotTriever system in Japan, Inari has entered into a distribution agreement with Medikit, a vascular medical device manufacturer serving Japan, the USA and over 30 other countries worldwide. With this new partnership, Inari plans to accelerate initiation of its 100-patient post market surveillance study.
“MHLW’s approval of reimbursement for ClotTriever under a newly designated functional category marks a transformative milestone for Inari in Japan,” said Drew Hykes, chief executive officer of Inari. “This decision underscores the value of ClotTriever in addressing unmet clinical needs, and we are thrilled to collaborate with Medikit to bring this innovative solution to Japanese DVT patients, improving lives and advancing care in the near future. Over time, we look forward to bringing our broader portfolio of purpose-built tools to the Japanese market.”
The ClotTriever system is 510k-cleared by US Food and Drug Administration and CE-marked for treatment of DVT. More than 75,000 procedures have been conducted with ClotTriever globally. Recently, two-year outcomes were reported from the 500-patient ClotTriever CLOUT registry showing a strong safety profile, significant clot removal, and low rates of post-thrombotic syndrome.
FastWave Medical has announced the issuance of its sixth utility patent by the US Patent and Trademark Office (USPTO), the fourth patent the company has been granted this year.
FastWave Medical’s intravascular lithotripsy (IVL) systems are designed to address calcified arteries. Vessels burdened with calcium pose significant challenges in treating vascular blockages safely and efficiently.
FastWave aims to empower physicians with breakthrough IVL devices to navigate complex arterial disease more effectively, reduce complications, and enhance overall patient outcomes.
“IVL has become a go-to tool for calcium modification and vessel preparation in large part due to its ease of use. I’m particularly excited about the potential of FastWave’s IVL devices in critical areas like catheter deliverability and energy durability. These types of improvements will lead to a more reliable first-line approach to tackle challenging cases,” said Raj Dave, president of Cardiovascular Experts of Pennsylvania (Camp Hill, USA).
With physicians increasingly relying on IVL for complex cases of calcific artery disease, innovations like FastWave’s are crucial in improving outcomes and making a tangible difference among at-risk patient populations with peripheral and coronary blockages.
“Our sixth utility patent is another step forward in our mission of providing physicians with leading-edge IVL technology,” said Scott Nelson, co-founder and CEO of FastWave Medical. “Our approach to development is rooted in key feedback from interventionalists across the world and I’m really proud of the progress our stellar engineering team has made in such a short time.”
Viz.ai has announced new data supporting advancements in neurology and vascular care, with two studies—both set to be presented at the Radiological Society of North America (RSNA) annual meeting (1–5 December 2024, Chicago, USA)—showing positive outcomes and the real-world impact of the company’s artificial intelligence (AI)-based technologies in clinical practice for patients with cerebral aneurysms or abdominal aortic aneurysms (AAAs).
“An aneurysm, whether in the brain or aorta, is a serious condition that can be life-threatening, prompting quick action to be taken to prevent rupture and potentially fatal bleeding,” said Molly Madziva Taitt, vice president of global clinical affairs at Viz.ai. “These studies, using diverse, real-world patient data, show the potential of both Viz AAA and Viz Aneurysm to be effective and highly accurate tools that can assist with a radiologist’s ability to triage and monitor patients appropriately, possibly saving lives.”
The first study, titled “Performance and validation of a machine learning-based aneurysm detection tool in the clinical setting”, assessed the performance of Viz Aneurysm through a retrospective evaluation of 703 head computed tomography angiography (CTA) exams from University of California (UC) Irvine Health System (Orange, USA).
The Viz Aneurysm algorithm successfully detected positive aneurysm cases with a sensitivity of 96.6% and specificity of 98.1%. The overall positive predictive value (PPV) of Viz Aneurysm in this study was 82.4% and the negative predictive value (NPV) was 99.7%. Additionally, it was noted that eight cases were detected with multiple aneurysms and 21 cases with aneurysms <4mm, suggesting Viz Aneurysm may be used to detect and manage patients with a lower risk of rupture, according to a company press release.
“Our findings show that the Viz Aneurysm algorithm successfully detected most of the aneurysms in our clinical dataset and performed consistently across subset analyses,” said Jennifer Soun (UC Irvine School of Medicine, Orange, USA). “Viz Aneurysm’s high accuracy shows its potential use to help detect and manage aneurysms in patients.”
The second study, titled “Performance of AAA AI triage software on real-world patient data”, evaluated the performance of the Viz AAA algorithm across 341 CTA exams of the abdomen from Montefiore Health System (New York City, USA). In this retrospective analysis, the Viz AAA algorithm successfully detected positive aneurysm cases with a sensitivity greater than 85%—whether cases with graft repair were included (86.5%) or not (88.6%)—and specificity of 98.3%. Additionally, it was noted that 25 CTAs with AAA and graft repair were correctly identified as positive by the Viz AAA module.
“These data suggest that this AI triage tool is both highly sensitive and specific, indicating high reliability for cases determined as positive across our diverse patient scans,” said Matthew Lazarus (Montefiore Medical Center, New York City, USA). “We believe incorporation of Viz AAA may help radiologists and other clinicians positively identify patients with AAA and potentially facilitate optimal treatment, management and health outcomes.”
Fluidx Medical has announced that the first patient has been treated in the GPX investigational device exception (IDE) prospective multinational clinical trial.
The GPX embolic device was successfully used in a portal vein embolization procedure in preparation for hepatic resection.
“We are pleased with the complete vessel filling we observed,” said principal investigator Stephen Chen (MD Anderson Cancer Center, Houston, Texas). “GPX was easy to prepare, deliver, and use. We could see the material flow distally into the vessel segment, completely blocking blood flow to the target area. This was exactly what we were aiming for.”
The safety and effectiveness trial includes leading medical centres and investigators from the USA, Canada, and New Zealand.
“The GPX Embolic was designed without toxic solvents which can cause patient pain and require special storage, preparation, handling, and catheters to deliver,” said Russ Bjorklund, vice president, Fluidx Medical. “Clinicians need embolics that can be quickly prepared, delivered with ease, and occlude the target immediately. The GPX embolic checks these boxes making it an innovative and simple solution designed for effective vessel filling.”
Newly released six-month results from single-arm arteriovenous graft (AVG) cohort in the WAVE (Wrapsody arteriovenous access efficacy) trial showed target lesion and access circuit primary patency rates of nearly 82% and 68.8%, respectively.
The latest data on the Wrapsody cell-permeable endoprothesis (Merit Medical)for treatment of stenosis or occlusion within the dialysis access outflow circuit were revealed during the final day of the 2024 VEITHsymposium (19–23 November, New York, USA) by co-principal investigator Mahmood K Razavi (St. Joseph Heart & Vascular Center, Orange, USA). “In light of the historically low patency rates for AVG patients, the positive results from the AV graft arm of the WAVE trial are very encouraging for physicians who manage these patients,” he said.
The WAVE trial was designed to evaluate the efficacy and safety of the WRAPSODY endovascular stent graft across two cohorts: up to 244 AV fistula patients randomized 1:1 to either the Wrapsody device or percutaneous transluminal angioplasty, and the AVG cohort.
Wrapsody
The graft arm enrolled 112 patients across 43 international sites. Primary efficacy and safety endpoints were assessed by comparing actual rates for the device to performance goals for covered stents (efficacy: 60%; safety: 89%). Efficacy of the Wrapsody device was 81.4%–21.4 percentage points higher than the performance goal (p<0.0001). The proportion of graft patients who were free from an adverse event was higher than the safety performance (95.4% vs. 89%, p=0.0162).
“As you well know,” Razavi told VEITH 2024, “these types of numbers are somewhat unusual in this patient population, having this kind of patency.”
The historical controls were based in three prior stent graft studies, he explained, with patency ranging between 50–71% at six months.
The proportion of graft patients who were free from an adverse event was higher than the safety performance (95.4% vs. 89%, p=0.0162).
“The patency results from the WAVE trial are the highest that I have seen to date and are expected to meaningfully improve patients’ quality of life and vascular access survival,” said WAVE trial investigator Leonardo Harduin (Universidade Federal do Estado, Rio de Janeiro, Brazil). “These results will probably have a positive impact on costs related to the care of these patients.”
The device is being investigated in the USA under a US Food and Drug Administration (FDA) investigational device exemption (IDE)
A recent press release by IASIOS has stated that, as the first paediatric hospital to seek IASIOS accreditation, St. Jude is setting a new precedent in paediatric oncology and establishing a benchmark within the broader field of interventional oncology (IO), pushing the boundaries of cancer care for children.
IASIOS offers healthcare institutions a framework to standardise patient pathways and implement measurable quality standards. As IO becomes recognised as the fourth pillar of cancer treatment, alongside surgery, radiation, and systemic therapies, it is essential for hospitals providing IO services to adhere to rigorous guidelines to guarantee safe and effective treatments.
The IASIOS standards are based on the Cardiovascular and Interventional Radiological Society of Europe’s (CIRSE) Quality Assurance Guidelines for Interventional Oncology, endorsed by the European Cancer Organisation (ECO) and supported by over 40 international medical societies.
Michael Temple, director of interventional radiology in the diagnostic imaging department at St. Jude, leads the accreditation effort: “At St. Jude, we are focused on the development, assessment and promotion of paediatric interventional oncology procedures. Seeking IASIOS accreditation demonstrates to our young patients and their families, our commitment to providing the highest quality of clinical care.”
As an IASIOS enrolled centre, St. Jude joins a global community of IO centres dedicated to advancing and promoting IO practices. This international network allows member facilities to collaborate, share knowledge, and participate in exclusive events, seminars, and workshops, all while working to raise awareness about the benefits of IO among patients and medical providers.
Boston Scientific has announced it has entered into a definitive agreement to acquire Intera Oncology.
Intera Oncology’s Intera 3000 hepatic artery infusion pump has been approved by the US Food and Drug Administration (FDA) and is used to administer hepatic artery infusion (HAI) therapy to treat tumours in the liver primarily caused by metastatic colorectal cancer.
In patients who receive HAI therapy to treat their cancer, the Intera 3000 pump is implanted under the skin and a connected catheter is placed in the hepatic artery, which supplies the liver with oxygenated blood. The pump then provides a continuous flow of floxuridine directly into the liver to treat tumours that have metastasised, most commonly from the colon.
“Liver cancer is a leading cause of cancer-related death, and we are committed to providing meaningful solutions to safely and effectively treat various forms of this disease with minimal systemic side effects and improved outcomes for patients,” said Peter Pattison, president, interventional oncology and embolization at Boston Scientific. “Interest in HAI therapy has grown in the oncology community given improved techniques, positive clinical results and ongoing trials. We believe this acquisition will enable us to provide a more comprehensive set of solutions to physicians and their patients to treat both primary and metastatic forms of liver cancer.”
The Intera 3000 pump is the only constant flow implantable pump for HAI therapy approved in the USA, a recent press release states. The safety and effectiveness of the Intera 3000 pump is supported by data from randomised controlled trials demonstrating the clinical benefits of HAI therapy for patients with unresectable colorectal metastases to the liver, both prior to and following resection.
Data from these trials have highlighted that HAI therapy significantly improves tumour response, time to progression and overall survival compared to systemic chemotherapy, and that combining HAI with systemic chemotherapy may lead to extended survival and higher conversion-to-resection rates in both chemotherapy-naïve and previously treated patients, so says the company. Current phase 2 and 3 studies are exploring HAI therapy use in larger patient groups for first-line, second-line and post-surgery adjuvant treatments.
Interventional radiology (IR) was officially recognised as a primary medical specialty in the USA by the American Board of Medical Specialties (ABMS) in 2012. This marked a significant milestone for the field, which had previously been considered a subspecialty of diagnostic radiology (DR). With 12 years of specialty distinction, Interventional News spoke to Parag Patel (Medical College of Wisconsin, Milwaukee, USA) who debriefed on their progress so far.
In the decade that followed the ABMS distinction, the crucial development of new training pathways in the USA dedicated to both DR and IR was a highlight for Patel. In 2014, the Accreditation Council for Graduate Medical Education (ACGME) followed the ABMS distinction by approving a dedicated training pathway—the integrated IR residency—which replaced the traditional model of completing a DR residency followed by an IR fellowship. “This is a further commitment to clinical care for our patients as this was mandated within the training programmes,” Patel said.
“We now recruit the best and brightest senior medical students into IR. The talent pool is extraordinary and these will be our future leaders in the field.” In 2024, the results of the main residency match announced via the National Residency Matching Program (NRMP) found that that IR-integrated spaces were the fifth-highest percentage (91.4%) among positions filled with US seniors. Although falling short of the 100% match rate that was achieved in 2022 and 2023, nearly all available resident positions for DR (97.9%) and IR (98%) were filled in 2024.
“Furthermore, we have seen increased opportunities for specialty representation that would have otherwise been relinquished to DR alone. The American College of Radiology (ACR) and Radiological Society of North America (RSNA) represent DR, radiation oncology, and IR. However, it is highly unusual for DR to be asked to represent radiation oncology for any clinical committees or guideline development.”
Similarly, with the recognition of IR as a distinct specialty, Patel stated that it would hold that the specialty should be provided its own representation at these discussions when appropriate.
“For example, interventional radiology should not rely on diagnostic radiology colleagues to support therapeutic interventions within National Comprehensive Cancer Network [NCCN] guideline development. Interventional radiology is best suited to voice the role of minimally-invasive interventional therapies for patients that are most suitable.”
In 2023, Patel concluded his term as president of the Society of Interventional Radiology (SIR), having progressed along the four-year pathway through secretary, president-elect, president and past president roles. He commented that the growth of IR in the USA has informed the direction of the SIR, with distinct primary specialty recognition allowing the society to advocate for board certified interventional radiologists. “In doing so, we are able to support interventional radiologists to pursue credentialing and hospital privileges specifically for procedures that would have otherwise not been available to them.”
In this article, Bjoern Suckow (Dartmouth Health, Lebanon, USA) discusses the Allia IGS 7 (GE HealthCare) and its role within his daily practice, sharing how the system has “technologically revolutionised” the way he and his team plan, visualise and perform complex procedures.
Suckow’s hybrid operating room
Encompassing the entire gamut of vascular surgery, Suckow’s practice has a strong emphasis on aortic pathology and endovascular treatments. In this continually evolving field, safety and efficiency remain key challenges, and interventionists face difficulties managing radiation exposure, visualising complex anatomy, and integrating preoperative planning with intraoperative imaging. To address these hurdles, the Allia IGS 7 system has been deployed as an addition to a hybrid operating room (OR), which Suckow describes as enhancing procedural accuracy and safety by reducing radiation use and improving workflow continuity.
Radiation exposure to both medical teams and patients remains a significant challenge when performing endovascular procedures. Traditional imaging requires high doses of radiation to achieve clear visuals of challenging anatomy, especially when treating advanced vascular pathology. This increased exposure is a persistent concern in endovascular interventions, Suckow states, as treatment of advanced pathology requires improved visualisation and so is “tied” to a high radiation exposure.
The Allia IGS 7 system offers a solution by integrating features that enhance imaging without increasing radiation. During procedures, the system allows for a fusion overlay that aids in visualising anatomy, with reduced reliance on additional imaging.
With this integration, interventionists can plan, execute, and assess procedures within a single software environment, which “helps to streamline workflow, reduce the repetitive nature of what we do, and lower radiation exposure while improving visualisation,” Suckow says. Previously, he and his team would repeat imaging or fuse prior imaging to “see what we can see now [with Allia IGS 7]”, which would have increased radiation dose to the patient.
Allia IGS 7 integrates with GE HealthCare’s ASSIST application, using three-dimensional (3D) guidance for endovascular aneurysm repair (EVAR ASSIST), including the vessel outline, ostia contours and stored optimal angulations for device placement.1 Suckow notes that the integration of this software into the same workstation for both pre- and intra-operative planning has been “integral” in enabling more accurate measurements and visualisation through segmentation and 3D modelling.
“During the execution of the procedure, EVAR ASSIST is fundamental through its fusion overlay so I can clearly visualise what I’m doing,” Suckow adds. “It clarifies, enhances and magnifies, all while keeping radiation dose low.”
EVAR ASSIST
In postoperative assessment, Suckow notes that Allia IGS 7 allows for on-table cone beam computed-tomography (CBCT) imaging, enabling review of placement and integrity of vascular devices immediately following implantation. This removes the need for additional postoperative CT scans, reducing both patient radiation exposure and hospital costs, “eliminating the possibility for errors”, Suckow said. “We can send patients home without further imaging assessments.”
For lower limb procedures, extensive anatomical regions need to be visualised, yet this can often be challenging with a machine with a smaller visual field, Suckow describes. In these cases, manoeuvrability is essential, to move the machine around the patient, or the patient around the machine.
“Much of the work we do in lower extremities is hybrid, meaning we have open exposures or concomitant open surgeries. Having a machine where the footprint and the manoeuvrability allows us to work in a sterile field with minimal complexity to move around and see what we need to see is crucial,” Suckow states.
Innova Breeze
He points out that the Allia IGS 7’s ability to perform a bolus chase using Innova Breeze (GE HealthCare) facilitates a continuous view of the entire limb during contrast injections.2 This effectively reduces the need for additional imaging and contrast material. This feature, combined with its flexible manoeuvrability, Suckow details, supports the visualisation required for long, complex limb interventions. Additionally, this technology can be used to recall stored 2D image series to treat lesions without repeat imaging, so that Suckow and his team can quickly confirm location, making procedures “easier, saving time, and lowering radiation”, he reiterates.
Touching on the hybrid OR setup they have achieved at their centre, Suckow explains how their previous system was “cumbersome” when moving from endovascular to open surgery. “For open surgery we need lighting, and with a large ceiling-mounted machine, lighting is difficult, and you cannot achieve optimal visualisation. With Allia, the machine can move entirely out of the way,” Suckow says.
“Allia is rapidly moved in and out, and I can bring in all of the lighting and accessories for true open surgery in a heartbeat. On the flip side, if I’m doing general open surgery in that room and I suddenly need endovascular imaging assessment, I can—from the table side—move Allia, and it does not require any breaking of sterility or extra manpower. We can just move the machine in and utilise it at a drop level.”
Digital pen function
Suckow adds that post-hoc analysis can also be done on-table using the digital pen and Allia IGS 7 console.3 “If you remember back in the day when we would have a picture on our screen, we would come up with a dry erase marker and mark on the screen certain locations that are of interest—that’s a way of the past,” he said. With this technology, a 3D mark can be made, which, if the patient or machine is moved, will stay in place. These marks can also provide length and diameter measurements that are true to size, which Suckow can do “with the click of the mouse”, he adds. “It has become a central part of our workflow and I use it in every single case.”
In the future, Suckow hopes that incremental improvements to safety, ease of device implantation, and workflow can be made, goals toward which the Allia IGS 7 system steps in the right direction. Additionally, integrating emerging technologies, such as radiation-free visualisation through fibre optic or electromagnetic field-based techniques could push the Allia system to the forefront of hybrid OR technology.
In all, the Allia IGS 7 system represents a valuable step forward in hybrid OR settings, through its ability to “visualise, zoom, pan, digitally enhance, lower radiation, and fuse workflow planning”, Suckow highlights. “This technology has revolutionised how I approach these cases—I couldn’t perform to such a standard in any other OR.”
Disclaimer
Bjoern Suckow is a paid consultant for GE HealthCare and was compensated for participation in this article. The statements by Suckow described here are based on his own opinions and on results that were achieved in his unique setting. Since there is no ‘typical’ hospital and many variables exist, i.e. hospital size, case mix, etc. There can be no guarantee that other customers will achieve the same results.
1. EVAR Assist 2 solution includes FlightPlan for EVAR CT, EVARVision and requires AW workstation with Volume Viewer, Volume Viewer Innova, Volume Viewer Innova enhanced, VesselIQ Xpress, Autobone Xpress. These applications are sold separately.
2. Innova Breeze is an option. Requires AW workstation. Applicable to Innova, Allia portfolio of systems.
3. Digital Pen option requires AW workstation with Volume Viewer, Volume Viewer Innova and Volume Viewer Innova Enhanced, HeartVision2 or Vision2. These applications are sold separately.
Product may not be available in all countries and regions and cannot be placed on the market or put into service until it has been made to comply with all required regulatory authorisations. Refer to your sales representative for more information.
A retrospective, single-centre study has found that women more frequently experienced moderate to severe pain and required more analgesics for pain management when compared to men following percutaneous thermal liver ablation.
“The reasons why women and men experience different levels of pain are still an ongoing research topic,” write the study’s authors—led by Christiaan van der Leij (Maastricht University Medical Center, Maastricht, The Netherlands). Speaking to Interventional News, Robrecht Knapen (Maastricht University Medical Center, Maastricht, The Netherlands) stated that “sex hormones, genotype, and endogenous opioid function may all play a potential role in these differences in pain experiences,” however these variables have not been sufficiently borne out in clinical research to date.
Percutaneous radiofrequency (RFA) and microwave frequency (MWA) thermal liver ablation are minimally invasive treatment options for patients with hepatocellular carcinoma (HCC) or colorectal liver metastases (CRLM). The authors describe that, according to the Barcelona Clinic Liver Cancer (BCLC) prognosis and treatment strategy, very early stage and some early stage HCCs should be initially treated with thermal ablation. In patients with CRLM, liver surgery “remains the standard treatment”, van der Leijet al state, “however thermal ablation has been increasingly used over the last few years with low complication rates. With studies, like the COLLISION trial, indications for thermal liver ablation will likely increase in the future.”
Informing their present research, van der Leijet al note that approximately 10% of patients treated with thermal ablation develop moderate to severe acute post-procedural pain. “This rate is 30–80% following surgery,” the authors add. Despite treatment modality, ineffective post-procedural pain management can lead to “increased length of hospital stay, opioid use, delirium in elderly patients, and thromboembolic complications,” they describe. Ablative factors which predict pain following treatment have been speculated, such as ablation volume, increase aspartate aminotransferase levels, and tumour location, which van der Leij and colleagues aimed to better define.
Their retrospective, single-centre cohort study was carried out at Maastricht University Medical Center, in Maastricht, The Netherlands. A total of 183 patients were included and treated with percutaneous thermal liver ablation for primary or secondary liver tumours between January 2018 and May 2022. Patients included were ≥18 years and had a thermal liver ablation performed with computed tomography (CT) or ultrasound guidance.
All patients received imaging prior to treatment and were routinely checked by the anaesthesiologist. The authors explain that typically, thermal ablation is performed under procedural sedation (PSA) using propofol and an opioid, or, if the patient does not meet the criteria for this due to high body mass index (BMI), sleep apnoea, or a prior unsuccessful PSA, general anaesthesia is given. Regardless of anaesthesia technique, all patients received lidocaine or bupivacaine as supplementary locoregional anaesthesia before the ablation procedure, van der Leijet al state.
Clinical outcomes were the maximal numeric ranking scale (NRS) score, ranging from 0 (no pain) to 10 (maximal pain), at the recovery after ablation, the prevalence of moderate/severe post-procedural pain (defined as NRS score ≥4) at the recovery room, and the NRS score at arrival recovery.
Of the 183 patients included—of whom 67% were men—at baseline, men were older on average, had a higher BMI, suffered from more primary liver tumours, and had larger mean maximal lesion diameters. At recovery, women exhibited a higher average maximal pain intensity (3.88 vs. 2.73) and a higher prevalence of post-ablation pain (NRS 4–10) compared to men. Regression analyses with adjustments for baseline differences showed that women suffered more from post-procedural pain (59% vs. 35%; adjusted odds ratio [aOR]: 2.50, 95% confidence interval [CI]: 1.16–5.39), and needed analgesics more often at recovery (77% vs. 63%; aOR: 2.43, 95% CI: 1.07–5.48) compared to men.
No differences were seen in the length of stay at the recovery, duration of anaesthesia, procedure time, and complication rate. Location of the tumour (subcapsular or deep), total tumours per patient, and distinction between primary and secondary tumours had no influence on the NRS, write van der Leijet al.
The authors draw attention to several limitations of their study, firstly its single-centre design and retrospectively collected data with a subjective pain measurement. They note that anaesthesiologists were free to choose analgesics during the ablation procedure, which may have caused “inconsistent sedation levels”. However, comparable medications, dosage, and sedation technique were used in both groups, minimising this bias, the authors state.
van der Leij and colleagues state that, until patient and procedural factors which influence pain have been “thoroughly investigated, anaesthesia care providers need to consider post-procedural pain differences in women undergoing thermal liver ablation”. Concluding, they state that higher dosages of analgesics should be considered—possibly morphine acting opioids—to reduce post-procedural excessive pain.
A retrospective evaluation has found that more than a third of old strokes discovered via head computed tomography (CT) imaging are “unknown” to both patients and physicians. Capturing these data, the study authors hope to better pinpoint opportunities for secondary prevention.
The analysis—which was recently published in the Journal of the American College of Radiology (JACR)—was led by Carys L Kenny-Howell (Yale School of Medicine, New Haven, USA) et al. They write that the incidental discovery of previously unknown strokes through neuroimaging provides an opportunity to implement additional prevention measures which can reduce the risk of recurrent stroke by up to 80%.
“Secondary prevention could benefit 100,000–200,000 patients per year in the USA, based on trends in emergency department care,” the authors detail. In conducting their retrospective analysis, Kenny-Howell and colleagues included all adult patients (≥18 years) who had received head CT imaging at three emergency departments between July and December 2023. Old strokes on CT imaging were categorised as ‘previously known’ or ‘unknown’. Patient and imaging factors associated with unknown strokes were assessed via univariable regression, multivariable regression, and decision tree analysis.
Kenny-Howell et al identified 21,985 head CT cases. A total of 869 (4%) examinations demonstrated an old stroke (mean age, 74.4 years±14), of which 372 (43%; 1.7% of all CTs) were unknown. Through univariable analysis, they found that unknown strokes were associated with greater age (odds ratio [OR], 1.03; 95% confidence interval [CI]: 1.02–1.04; p<0.001), a single site of old stroke (OR, 2.7; 95% CI: 2.06–3.58; p<0.001), smaller strokes (OR, 1.8, 95% CI: 1.6–2, p<0.001) as well as gangliocapsular (OR, 2.8; 95% CI: 1.9–4; p<0.001) and cerebellar location (OR, 2.1; 95% CI: 1.4–3.2; p< 0.001).
Speaking to Interventional News on behalf of their research team, Long H Tu (Yale School of Medicine, New Haven, USA) commented: “We were surprised at how prevalent unknown strokes were, and the relatively large proportion among all old strokes in our study. This emphasised to us the importance of calling attention to these findings which radiologists often consider non-actionable or not significant because they are chronic. There seems to be an opportunity to improve care and secondary prevention for a lot of patients.”
A single-centre report of mid- to long-term outcomes following prostate artery embolization (PAE) in a large cohort has found that the treatment shows significant and sustained relief from lower urinary tract symptoms (LUTS) caused by benign prostatic hyperplasia (BPH).
In a paper published in the Journal of Interventional Radiology (JVIR), principal investigator Shivank Bhatia (Miller School of Medicine, Miami, USA) et al write that PAE has recently been recognised as a viable treatment for BPH, and has been included within the American Urological Association (AUA) treatment guidelines. Yet, despite its increasing recognition there is a scarcity of long-term research to support its efficacy.
Their study included 1,075 patients with moderate-to-severe LUTS or urinary retention who underwent PAE in the period between January 2014 and July 2023. Patients were assessed at one, three, six and 12 months post-PAE and then yearly thereafter. Bhatia and colleagues used several modes to assess patient progress, including: the International Prostate Symptom Score (IPSS), quality of life (QoL) score, International Index of Erectile Function Score (IIEF-5), prostate-specific antigen (PSA), prostate volume (PV), post-void residual (PVR), benign prostatic obstruction (BPO) medication usage, urinary catheter status, and further prostate interventions. In addition, adverse events were recorded using the Society of Interventional Radiology adverse event (SIR-AE) severity classification.
Mean follow-up was 458.4 days, and the average patient age was 70.4 years. Median prostate volume was reported as 107 grams, and median pre-procedure IPSS, QoL, IIEF-5 and PSA were 23 (18–28), 5 (4–6), 17 (10–21), and 4.7 (2.6–8), respectively. In the LUTS subgroup, at 1–3, 6–12 and 48–60 months, the median IPSS was 7 (4–12, p<0.001), 6 (3–11, p<0.001), and 9 (4–15, p<0.001). QoL scores were 2 (1–2, p<0.001), 1(0–2, p<0.001), 2 (0–3, p<0.001) at the same timepoints. Of patients in the urinary retention cohort, 119 (94%) out of 126 patients were catheter-free at the three-month follow-up.
Up to 60 months post-PAE, 90 patients required reintervention. Overall, 65.5% of patients were BPO-medication free at one year following initial PAE. In this cohort, 7% of patients with an SIR-AE severity score of severe, which included three patients with transient ischaemic-attacks, two with urosepsis (treated via inpatient setting with intravenous-antibiotics), and finally, two patients with prostate sloughing. All adverse events resolved without sequelae, state Bhatia et al.
In their large cohort with long-term longitudinal follow-up, the authors report the significant improvement in LUTS symptoms, highlighting that 94% of catheter-dependant patients at baseline becoming catheter-free at three months.
They state that PAE is validated as safe and effective for the treatment of BPH, and, given its “efficacy and favourable safety profile”, should be considered equal to traditional surgical treatments. Bhatia and colleagues add that PAE should be more broadly integrated within clinical practice as a standard option for BPH.
Sharing an update with Interventional News, consultant vascular radiologist Raghu Lakshminarayan (Hull University Teaching Hospital, Hull, UK) describes where interventional radiology (IR) stands within UK healthcare today.
The role of IR in patient care pathways and care delivery is gaining prominence in healthcare leadership across hospital trusts and primary care in the National Health Service (NHS). The speciality demonstrated its key role especially with an increase in day unit procedures benefitting patient care during the COVID-19 pandemic. The evolving nature of IR jobs, with greater emphasis on clinical responsibilities and patient involvement, highlights the challenges of operating solely within a diagnostic radiology environment. There is an increasing recognition of the need to establish IR as a distinct faculty within radiology to promote patient care. Dual certification in diagnostic radiology will enable interventional radiologists to integrate imaging expertise with clinical skills. Additionally, the interdisciplinary collaboration will provide opportunities to influence government policy for the Royal College of Radiologists (RCR).
Establishing a dedicated faculty of IR would enhance leadership allowing for establishment of IR clinical leads who can address budgetary concerns, equipment needs, and staffing requirements. This would reflect positively in the job plans of IR consultants with adequate time for clinic and inpatient responsibilities. Addressing the shortage of qualified IR professionals is essential to support any new training and faculty structures. Healthcare system constraints make it difficult to support dedicated IR training programmes with its own clinical responsibilities and on-call training. Developing a comprehensive IR curriculum would attract trainees to apply from a broader pool of medical graduates providing a structured dedicated run through programme which emphasises the clinical and patient management issues of IR.
Current awareness of IR is low amongst stakeholders, patients and the public in the UK. This creates challenges and barriers in ensuring consistency in the availability of, and access to, minimally invasive image-guided treatments across the healthcare landscape. The only way of changing this is to enable key decisions of IR to be taken by interventional radiologists. At local, regional and national levels, having interventional radiologists represent the speciality at NHS and government level is necessary to provide the right leadership framework to advance the speciality and optimise patient care. The ideal way to achieve progression would be for IR in the UK to have a faculty status within the RCR, which is a current matter of debate.
Raghu Lakshminarayanis a consultant vascular radiologist at Hull University Teaching Hospital, Hull, UK.
In a paper published last month in the journal CardioVascular and Interventional Radiology (CVIR), Matthew Lukies and colleagues from Alfred Health in Melbourne, Australia have released data collected from their institution giving visibility to the clinical interventional radiology (IR) service that they state has gone largely unnoticed. As IR has not yet achieved formal distinct speciality status in Australia or New Zealand, the authors sought to show IR’s increasing self-governance independent from diagnostic radiology (DR).
The authors write that providing optimal care for patients in IR is dependent on interventional radiologists’ adoption of clinical responsibility—from referral and clinical assessment, through to treatment, and follow-up care. Lukies et al state that clinical practice in IR enables the provision of a comprehensive service, helping to develop a “robust referral pathway” and provide optimal care for patients. They believe this keeps IR “relevant and competitive” among other interventional specialties who are performing endovascular and minimally invasive procedures.
Lukies and colleagues detail that the strategic direction of IR and DR have “diverged” in the recent past and note that the output of DR is increasingly benchmarked via relative value units and other metrics. Without distinct specialty status away from DR, IR sits within these datasets, they state, operating via an ancillary ‘service provision’ structure which has created “inherent problems for interventional radiologists”. This is partly due to the fact that the clinical aspects of IR work, which include ward rounds, ward consultations, preadmission assessments, and outpatient appointments, are not captured in traditional DR key performance metrics.
This has led to a perceived “imbalance” in work output between IR and DR, Lukies and colleague state, resulting in interventional radiologists feeling “pressured” to achieve particular levels of diagnostic output to the detriment of clinical IR practice.
To capture their own data to measure clinical IR output, Lukies et al created a searchable tag within their inpatient ward round and electronic medical record consultation notes. This tag could then be measured over a given time period and collated as a ‘clinical IR’ key performance indicator.
A ward consultation constituted a face-to-face, bedside review of an inpatient by one or more members of the IR team (consultant, fellow, and intern) including ward rounds and consultation referrals. Excluded from this data collection were outpatient clinic reviews, phone consults to patients or family members and discussions with other specialities regarding patients.
Between April and July 2024, the authors write that their IR service provided a total of 394 inpatient consultations—a mean of 4.7 ward consultations per day. They describe that their service is typically comprised of two to four interventional radiologists and one advanced training fellow each day. They utilise three angiography suites, and deal with admissions, discharges, referrals and consultations, as well as twice weekly outpatient clinics.
The authors presented these data to their DR colleagues—including direct managers—who were unaware that this work takes place. They stated, however, that they were appreciative of its “value in audit and role in governance changes for optimal patient care”.
Demonstrable of the importance of measuring clinical care in IR, Lukies et al write that giving visibility to the day-to-day workload of interventional radiologists outside of DR’s metrics is “critical” in providing optimal care and initiating workforce planning for the future. They state that the promotion of their clinical work through distinct performance indicators is an important component in assessing and thereby resourcing IR services.
“Clinical practice is the cornerstone of modern IR, and we must be provided with sufficient time, resources and workforce to ensure safe and high-quality clinical care for our patients,” Lukies and the research team add.
I became an interventional radiologist by accident. As a resident in cardiology, I had an unusual chief: he belonged to a new breed of cardiologists who did cardiac catheterisations and coronary angioplasties. When I expressed an interest in doing the same, he said: “This work is usually done by radiologists. I am the exception to the rule. Go to the Hammersmith Hospital and ask Robert Steiner, the professor of radiology, to train you.” Steiner said: “If you want me to teach you, you have to become a radiologist.” “Thank you, Professor,” I said. “You start on the first of October.” That was my job interview. How times have changed…
Act I: Interventional cardiology
During my basic training in radiology, I went to the cardiac lab, within the department of radiology, just to observe the work, in preparation for what I thought would be my future career. Steiner allowed cardiologists as well as radiologists to be trained in cardiac catheterisation and intervention. Although the radiologists had excellent technical skills, it was obvious to me that their role in this new discipline was destined to disappear. Why? Because they were interested mainly in the catheters and the pictures. They were happy for the cardiologists to monitor the electrophysiological parameters and, most importantly, to look after the patients. That battle was lost before it even started.
Act II: Peripheral vascular interventions
Hammersmith Hospital was the home of the emerging discipline of interventional radiology (IR). It was an exciting time, with such a dizzying number of developments in all organ systems that it was difficult to choose a focus. Some of the things we did would be illegal today, like drawing the shape of a plastic spiral biliary stent on the silver paper in a cigarette packet (no, not mine), having the device in my hand a week later, and implanting it across a malignant hilar stricture the following day. What one could do was limited only by the anatomy of the human body and imagination. There was no challenge to IR from any other discipline. But, having witnessed the loss of cardiac intervention, I was certain that Charles Dotter’s exhortation to ‘accept clinical responsibility’ was wise.
When I was appointed to the university chair of IR by the Senate of the University of London in 1992, I approached the Royal College of Radiologists (RCR) to encourage them to create a new method of training, distinct from that of diagnostic radiology (DR), that would allow future interventional radiologists to look after their own patients. A historic meeting of the three governing bodies of the college—the faculties of radiation oncology and radiology, and the RCR council—was convened by the president of the college, who was a radiation oncologist. I told them that devices called ‘aortic stent grafts’ would change the way peripheral vascular disease was managed and that radiologists had an opportunity to play a major role in this field, provided they were trained as clinicians rather than as imagers. The radiation oncologists understood and agreed. The radiologists didn’t. I was told that ‘teamwork is the way forward’, which was code for ‘others can look after the patients of interventional radiologists’. I allowed my frustration to show and said, ‘teamwork is the kiss of death’. What I meant was that ‘shared’ clinical responsibility is an illusion; either you are a fully-fledged clinician, or you are not. My retort was inelegant and ungracious, but it was correct. Much of vascular IR is now in the hands of vascular surgeons.
Act III: Interventional oncology (IO)
The encroachment on IO by other specialties is still patchy because, until recently, it has focused on palliation and the treatment of small tumours in patients who are not candidates for surgery. This is changing fast, as solid scientific evidence now supports the use of ablation as a primary treatment of small tumours in the kidney and the liver. As IO expands, surgeons will want to use its techniques to replace major surgery.
Several countries are trying to establish IR as a specialty separate from DR, following the example of the American Board of Radiology (ABR). This is necessary, but not sufficient. If IR is to thrive as an independent discipline, rather than just tick along as an optional extra to surgery and radiation therapy, its practitioners must be full-time clinicians. They must stop spending time reading diagnostic images other than those concerning the patients they treat. Even those studies must be formally reported by diagnostic radiologists rather than by interventional radiologists. This will not happen without radical changes to training and recruitment.
The future of IR will be decided by institutions such as the RCR, and its counterparts in other countries, which define the pattern of training and practice of their members. If such professional bodies want to retain IR, they must create a specialty that focuses on clinical and procedural training. Although the intimate understanding of radiological imaging is a vital aspect of the skillset of interventional radiologists, they should be able to use that knowledge to guide their interventions and to assess the results. True, full-time clinical practice in IR can become a reality only if dual certification stops. Such a specialty would attract trainees with a surgical mindset, who are understandably reluctant to spend several years away from clinical practice in diagnostic radiology learning to be imagers.
Will this happen? Well…anything is possible. But betting more than half a pint of beer on it might be a little too optimistic.
Andreas Adam is emeritus professor of interventional radiology at King’s College London, UK and joint editor-in-chief of Interventional News.
A study which benchmarked results from prospectively collected Vascular Quality Initiative (VQI) data for patients who have undergone peripheral vascular interventions (PVI) for chronic limb-threatening ischaemia (CLTI) has found that patients in Singapore “fared worse” than patients in the USA, despite comparable technical success rates. These results were published in the Journal of Vascular Surgery (JVS).
The retrospective review conducted by Joel Jia Yi Soon (Singapore General Hospital, Singapore) et al, used the Society for Vascular Surgery (SVS) VQI registry database from the first, and at present only, VQI centre in Asia. The researchers reviewed the database to identify patients with CLTI who underwent endovascular revascularisation between July 2019 and April 2024, comparing these data with those collected from participating centres in the USA.
A total of 2,862 procedures were identified from Singapore General Hospital (SGH) and were benchmarked against 129,347 procedures from 406 centres in the USA and Canada. The researchers note that the average age of patients in their cohort was younger than those in the USA, reported as 68.8 years versus 69.6 years. Their patient cohort also had significantly lower body mass index (BMI) and a lower proportion of patients with a history of smoking.
Soon et al state that their cohort had a higher burden of comorbidities, including diabetes mellitus, end-stage renal disease, and cardiac disease, and presented with advanced Wound, Ischemia, and Foot Infection (WIfI) stages. The investigators add that their patients had more heavily calcified and longer (14.8cm vs 6cm) diseased vessels with higher prevalence of multi-level (87% vs 54.6%), infrapopliteal (52.6% vs 38.9%) and inframalleolar (9.6% vs 2.4%) disease.
Technical success and symptom improvement between the SGH VQI centre and those in the USA were comparable, reported as 92.7% versus 93%, and 39.1% versus 40.4%, respectively. However, one-year mortality (28.9% vs. 25.1%) and major amputation rates (13.3% vs. 7.8%) were significantly higher in the Singapore cohort.
The authors note that although their patients had improved short-term outcomes despite more advanced disease and comorbidities, they experienced worse long-term outcomes. They call for further research to investigate the underlying causes of these discrepancies. The study highlights that since 2019 when SGH was enrolled in the PVI registry, they remain as the only VQI centre outside of North America. The authors emphasise that the majority of VQI data on CLTI is based on North American patients, limiting the generalisability of findings to Asian populations.
“Enrolment of our centre in the VQI registry has been tremendously helpful in improving our understanding and management of our patients with CLTI via the standardisation of data collection, reporting of post-procedural outcomes and allowing for benchmarking against centres from the rest of the world,” the investigators write.
They hypothesise that differences in patient characteristics, disease morphology, and treatment approaches may explain the varying clinical outcomes between Asian and North American patients with CLTI undergoing endovascular revascularisation. The authors conclude that their findings offer valuable insights into improving treatment outcomes for Asian patients with CLTI.
Titled ‘Let’s talk about the “C” words’, Trevor John Cleveland’s (University Hospitals Plymouth, Plymouth, UK) Graham Plant lecture at this year’s British Society of Interventional Radiology (BSIR) annual congress (6–8 November, Brighton, UK) tackled nationwide inconsistencies across patient consent and the provision of interventional radiology (IR) clinics.
“Consent has evolved and changed significantly over the last few years,” Cleveland began, stating that, in the UK, the General Medical Council (GMC) sets out Good Medical Practice (GMP) guidelines which govern principals, values, standards and delivery of care. “They are very clear that, when we deliver care, this should be in the best interest of the patient. This may be stating the obvious for most of you, but I feel this can be lost in some of the discussions. We must keep this at the forefront.”
The GMC also outlines duties which must be carried out by interventional radiologists, which includes supporting patients to make informed decisions. Cleveland described the difficulties that can arise when explaining often complex procedures to patients, particularly in an ageing population with “increasing levels of dementia and confusion”.
The guidelines also state that clinicians should refer to another suitably qualified practitioner when necessary, “an important thing to bear in mind—it works both ways,” he said. “It’s reasonable to have support from our clinical colleagues, and when they need our help and refer to us, we’re on an equal footing.”
Placing his talk within its legal context, Cleveland detailed the Montgomery Ruling, which “changed the legal standards for consent which clinicians are expected to deliver”. The Montgomery Ruling, or Montgomery vs Lanarkshire Health Board, was a 2015 UK Supreme Court case which found the latter liable for negligence following patient harm as a result of undisclosed procedural risks.
“This ruling focuses on the patient’s right to decide, making sure that they’re not passive in that decision-making. This is not the decision we make in a multidisciplinary team—the board can make a recommendation, or have a view—but ultimately, it’s the patient who decides,” said Cleveland.
Referring again to the GMC guidelines, Cleveland stated that interventional radiologists must endeavour to “find out what matters to patients and give them time to understand what they need to know—it’s not a two-minute job”. He added that patients need to be made aware of the expected benefits, but as importantly risks, no matter how unlikely. When providing this care, the GMC states that clinicians should accommodate the patient’s wish to record the conversation. Cleveland remarked that the potential for this recording to be played back may appear “slightly threatening”.
The speaker made clear that to gain informed patient consent the provision of dedicated time during IR clinics is necessary. “This all comes down to time with the patient,” he stated. “It’s near impossible to make an assessment of a patient’s capacity in a day ward with two or three other patients listening, using curtains for privacy.”
Cleveland moved on to detail the importance of pre- and post-procedure clinics. Pre-procedure clinics work to reassure patients and guarantee they have adequately consented to treatment going forward. Provided this time, Cleveland underlined how the IR team is able to unify and align on pre-assessment plans and any necessary repeat procedures.
“As IR has become involved with more complex treatment pathways—an example would be diabetic foot care—these clinics give us the chance to actually get the patient the appropriate investigation and treatment fairly rapidly,” said Cleveland.
He continued that post-procedure clinics are equally as important as pre-procedure, to monitor any issues or complications that may have arisen. “[Post-procedure clinics] also allow patients to feedback to you on whether they thought [the treatment] was a great idea or not, and whether you offered them something they wanted. Sometimes it isn’t and you learn what not to do going forward,” Cleveland shared.
He summarised that consent is “a process, and a potentially complicated one”, but if carried out correctly, patient expectations and experiences are invariably improved. Clinics are of two-fold importance, Cleveland continued. He said that they not only facilitate the proper collection of patient consent but position interventional radiologists as the “clinical team leaders” who are afforded key responsibility over their patients’ care.
Xeltis has today announced that the Center for Devices and Radiological Health (CDRH) of the US Food and Drug Administration (FDA) has granted aXess Breakthrough Device Designation status. aXess is Xeltis’ vascular access conduit, which enables the creation of a new, permanent, living vessel for haemodialysis vascular access.
Concurrently, following investigational device exemption (IDE) approval from the US FDA, the first patient in aXess’ US-staged pivotal trial has now been enrolled and by Karl Illig (FLOW Vascular Institute, Houston, USA), marking a significant clinical milestone for Xeltis.
According to the press release, this Breakthrough Device Designation acknowledges that aXess meets the necessary criteria for its proposed use as a vascular prosthesis, as well as the fact that it has the potential of providing a more effective treatment option for patients needing haemodialysis vascular access than current treatments. These benefits, Xeltis said, include the avoidance of frequent reinterventions and complications, such as infections, which are faced by renal disease patients. The designation grants Xeltis accelerated interactions with US FDA review teams, prioritised review, and special reimbursement consideration, positioning the company for enhanced market access and expediting commercialisation for patients in need.
Eliane Schutte, chief executive officer (CEO) of Xeltis commented: “We are in a transformative period for Xeltis, and this designation from the US FDA is great recognition of the potential importance of our highly novel technology. We are also extremely proud that the first patient in our US pivotal trial has now been treated, and this clinical achievement provides us with significant momentum as we advance towards commercialisation.”
Illig, site principal Investigator for aXess US pivotal trial, also shared his thoughts, stating: “aXess has the potential to be a truly ground-breaking advance in the vascular access field, as it enables the creation of a new, permanent, living vessel. We hope that its ability to avoid the frequent reinterventions and infections associated with current treatment options will make a major difference to patients and their care.”
John Lucas III (Greenwood Leflore Hospital, Greenwood, USA), national principal investigator for aXess US pivotal trial, added: “The US trial for aXess is an important step in assessing and validating the ability of this unique conduit to transform the field of vascular access. The 12-month data from the first-in-human study in Europe is extremely promising and I look forward to working on this next clinical stage in Xeltis’ journey.”
Strong clinical data for aXess will be presented during the VEITH Symposium (19-23 November, New York, USA). On 21 November, Frans Moll (University Medical Center Utrecht, Utrecht, The Netherlands) will present the full two-year clinical results for aXess, and on 23 November, Lucas III will present an update on the US IDE Pivotal Study for aXess.
GE HealthCare has announced the US Food and Drug Administration (FDA) 510(k) clearance for its Signa Magnus magnetic resonance imaging (MRI) scanner.
The 3-tesla (T) head-only scanner is designed to improve clinical imaging and neuroscience research, assisting in the detection of various oncological, neurological, and psychiatric conditions. Signa Magnus features a high-efficiency asymmetrical, gradient coil design. This design helps in achieving higher gradient performance with a reduced inner diameter, making it ideal for neuroimaging applications, a recent press release describes.
It also allows for better patient head access by shifting the gradient isocentre towards the edge of the coil. This eliminates shoulder width constraints and enables a gradient amplitude and slew rate that surpasses conventional whole-body MRI systems.
Signa Magnus’ precision enables advanced imaging methods, offering high-resolution and signal-to-noise ratio with brief scan times. Short scan times and improved gradient strengths contribute to enhanced spatial resolution and image clarity, which can lead to more accurate diagnoses.
The system’s HyperG gradient technology has performance levels of 300mT/m and 750T/m/s, allowing for faster image acquisition without increased power requirements.
Signa Magnus’ capabilities in visualising brain function, microstructure, and micro-vasculature are further improvised by oscillating gradient diffusion encoding technology which delivers cellularity contrast.
The system will be available for new installations and as an upgrade from compatible Signa premier systems, allowing existing facilities to adopt this advanced technology without significant infrastructure changes.
Four investigational Signa Magnus scanners are currently installed at institutions, including Walter Reed National Military Medical Center and the University of Iowa, among others in the USA.
GE HealthCare MRI applications platform and research technologies general manager Jason Polzin said: “Obtaining FDA clearance further validates our commitment to not only innovating but also delivering clinical technologies that have real-world impact.
With Signa Magnus, we are providing neuroradiologists and neuroscience researchers a tool that supports advanced imaging and biomarker research and discovery previously impossible on conventional systems. It is our intent to make Signa Magnus widely available as a fully cleared commercial product.”
Arsenal Medical today announced the initiation of the EMBO-02 clinical study of NeoCast in the treatment of chronic subdural haematomas (cSDHs). NeoCast is a first-of-its-kind, shear-responsive, non-adhesive, solvent-free, liquid embolic material designed for deep distal penetration, according to a press release from the company.
The EMBO-02 study is enrolling up to 10 subjects at three sites in Australia, and the first of these patients has been enrolled at Monash Health (Melbourne, Australia).
“We are encouraged by our experience with NeoCast in cSDH,” said Monash Health’s Lee-Anne Slater, the principal investigator of both the EMBO-01 and EMBO-02 trials. “The initial case was an excellent translation of middle meningeal [artery] embolisation [MMAe] from EMBO-01, which studied hypervascular brain tumours. NeoCast performed predictably throughout injection and provided robust distal occlusion, further demonstrating its unique properties, which sets it apart from current embolic products.
“Better performing, innovative solutions are needed to manage this significant neurovascular condition. We look forward to continuing enrolment in EMBO-02 and uncovering the potential for NeoCast for this population.”
Upma Sharma, president and chief executive officer (CEO) of Arsenal Medical, added: “Recent data suggest MMAe procedures for treating cSDH are estimated to rapidly increase in frequency and are expected to surpass those for large-vessel stroke. The launch of EMBO-02, our second study with NeoCast, is an important milestone for the company and a next step toward delivering a differentiated embolic solution. I am grateful to all of our clinical and scientific collaborators who are helping us to advance our next-generation embolic material—and, most importantly, the patients who participate in these important studies.”
EMBO-02 is an open-label, multicentre, prospective clinical trial intended to evaluate the early safety and feasibility of NeoCast to embolise target vessels of a subject’s MMA in order to treat cSDH, and potentially reduce haematoma recurrence. Its primary endpoints include: safety, defined as freedom from device-related disabling stroke or neurological death within 30 days of the embolisation procedure; and feasibility, defined as the successful injection of NeoCast into the MMA, resulting in complete occlusion at or distal to the point of embolysate injection.
Healionics Corporation has today announced that its STARgraft arteriovenous graft—which it states is designed to provide a safer and more reliable means of bloodstream access for kidney failure patients needing dialysis—has been granted Breakthrough Device designation by the US Food and Drug Administration (FDA).
The US FDA’s Breakthrough Devices Program aims to identify important new medical devices that provide more effective treatment of life-threatening and irreversibly debilitating conditions, and fast-tracks their regulatory review in order to provide timely access for patients and healthcare providers. This Breakthrough designation signifies US FDA acknowledgment that STARgraft clinical outcomes show evidence of significant advantages over existing alternatives for dialysis access. The benefits of receiving Breakthrough designation include expedited interactions with the US FDA regarding market clearance and with Medicare regarding potential added reimbursement for healthcare providers.
According to the press release issued earlier today, more than 550,000 people in the USA suffer from kidney failure and require frequent dialysis to filter waste from their blood. Current methods of creating and maintaining regular bloodstream access for dialysis, Healionics argues, are risky, unreliable and costly, driving a significant portion of the US$50 billion the USA spends each year to treat kidney failure. They added that an arteriovenous graft (AVG) is often implanted to create an access site with sufficient flow rate for dialysis, but existing grafts frequently fail due to occlusion and/or infection. Healionics’ innovative STARgraft arteriovenous graft, based on proprietary synthetic biomaterial technology, is designed to resist both problems.
Healionics chief executive officer (CEO) Mike Connolly shared his thoughts on this Breakthrough designation, stating: “US FDA recognition of STARgraft’s potential to significantly improve the standard of care and quality of life for dialysis patients is a major company milestone and validation of our team’s efforts.”
Where is liquid biopsy today? Bruno Damascelli, Vladimira Tichà, Giancarlo Beltramo, Alberto Gramaglia and Gianluigi Patelli write on the complexities and challenges of the procedure as it gains ground among select interventional radiologists.
Liquid biopsy is gaining momentum on its path toward clinical utility, but the current role of this important advance in oncology is difficult to pinpoint. While it is easy to obtain a blood sample, molecular analysis of tumour biomarkers is still remarkably complex. The aim is to identify the genetic mutations of cancer in the biological markers it releases into blood. The most widely used of these is circulating tumour DNA (ctDNA) which is released into circulation primarily through apoptosis and cell necrosis. In the blood, ctDNA is mixed with cell-free DNA (cfDNA) which is produced in larger quantities because of cell turnover in normal tissues. This means ctDNA must be separated by an extraction process, which is followed by genetic sequencing—known as next generation sequencing (NGS)—covering a variable number of genes chosen according to their frequency in tumours. The cases presented here used Guardant360 (Guardant Health) comprehensive genetic profiling which reports the amount of ctDNA as a percentage of cfDNA.
The greatest difficulty in molecular analysis is the scarcity of ctDNA detectable in the general circulation, which has given rise to various methods of obtaining a significant amount of this biomarker. The simplest method, investigated by us and confirmed by another research group, is to draw venous blood in proximity to the tumour site. Percutaneous venous catheterisation is part of the armamentarium of interventional radiologists and relies on their familiarity with navigating the vascular system under fluoroscopic guidance. Sampling sites can be chosen as dictated by the natural history of the disease, which includes both primary and metastatic sites.
Unlike tissue molecular diagnosis, which is inevitably restricted to a few sections, liquid biopsy provides a wider reflection of the tumour’s epigenetic heterogeneity. Other advantages of selective sampling compared with conventional peripheral sampling are that it avoids the ctDNA dilution that occurs in the general circulation, and it exploits the topographical contribution of lymphatic drainage, a leading route of cancer spread. Lymph from the left hemithorax, the entire abdomen and the lower limbs drains into the thoracic duct, which empties into the left venous angle. Sampling from this site can provide information about intra- and extra-peritoneal cancers. Lymph from the right hemithorax and part of the head and neck drains into lymphatic trunks that empty into the right venous angle, where venous sampling provides more effective molecular characterisation than peripheral sampling.
Liquid biopsy is beginning to be considered for use in diagnosis of lung nodules (Case one) for which no convenient solution is offered by imaging methods or percutaneous biopsy, which can prove inconclusive or unfeasible because of the associated risks.
Case one: Male, 76 years old. Spiculated lung nodule, 14mm (A) in the right lower lobe, ischaemic heart disease, respiratory failure. Liquid biopsy from the right subclavian vein (B, C) with a finding of pathogenic mutation CDH1. Surgical histological confirmation of minimally invasive adenocarcinoma.
Radiosurgery is increasingly used in cancer treatment, sometimes as the only option, with a consensus for its use in the absence of histological examination. Liquid biopsy can confirm the diagnosis and assess treatment response or resistance during follow-up. A liquid biopsy showing a mutation consistent with glial neoplasm (Case two) is decisive not only when histological diagnosis is not possible but also for monitoring treatment in the event of recurrence or progression. Molecular diagnosis has a higher success rate on cerebrospinal fluid than on peripheral blood but repeated lumbar puncture is not without risk for the patient. Retrograde percutaneous catheterisation of the jugular veins is an outpatient procedure known since its use in the diagnosis of pituitary tumours.
Case two: Female 60 years old. High-grade right frontal glioblastoma extending to the corpus callosum (A, B). Surgical histological confirmation but with negative tissue-based molecular testing. Pre-operative liquid biopsy from the right jugular vein (C) showing BRAF and PIK3CA mutations. Negative peripheral sample (D).
Another application of selective venous sampling is in ocular cancers. Uveal melanoma (Case three) can express mutations predicting disease evolution. Follow-up relies on abdominal ultrasound to detect hepatic metastases, which are invariably detected too late for effective treatment. Sampling from the jugular vein on the melanoma side allows molecular characterisation of the tumour, predicting its behaviour and guiding the use of new drugs with recent, promising results. Until now, this tumour has been treated with radiotherapy based on a diagnosis made with physical and radiological means applied to the intact eye.
Case three: Female, 83 years old. Uveal melanoma, left eye (A). Right transfemoral catheterisation of the left jugular vein (B, C) with finding of HNF1A mutation indicating a poor prognosis.
Prostate adenocarcinoma (Case four) affects 16% of the male population. Early diagnosis of this cancer has had a positive effect on survival but metastatic spread leads to a long-lasting deterioration in quality of life. Peripheral sampling or selective sampling from the hypogastric veins can provide timely detection of the somatic mutations involved in resistance to radiotherapy or androgen suppression, guiding appropriate personalised treatments.
Case four: Male, 63 years old. Operated prostate adenocarcinoma, Gleason grade 7 (3+4), PSA increase to 0.26 six years after surgery. PET PSMA (A, B) positive for right pelvic adenopathy. In the right hypogastric vein (C) we found ESR1, FGFR2 and MAP2K1 mutations. In the left (D) vein, mutations were FGFR2, MAP2K1 and RET. Pelvic radiotherapy is indicated.
Liquid biopsy is not yet recognised for its diagnostic accuracy, clinical utility and patient benefit, and few molecular tests are approved by regulatory bodies. While it is unrealistic to imagine that liquid biopsy could replace histological examination, it is nonetheless true that in monitoring the evolution of a tumour and its sensitivity or resistance to treatment, blood sampling is always possible, whereas tissue biopsy often is not.
References:
Tichà V., Patelli G., Basso G. et al, Case Report: Potential role of selective venous sampling for liquid biopsy in complex clinical settings: Three case presentations, Frontiers, https://doi:10.3389/fgene.2023.1065537.
Tamrazi A., Sundaresan S., Gulati A. et al, Endovascular image-guided sampling of tumour-draining veins provides an enriched source of oncological biomarkers, Frontiers, https://doi:10.3389/fonc.2023.916196.
Saife N. Lone, Sabah Nisar, Masoodi T. et al., Liquid biopsy: a step closer to transform diagnosis, prognosis and future of cancer treatments, Molecular Cancer, https://doi:10.1186/s12943-022-01543-7.
Bruno Damascelli is an interventional radiologist at Fondazione Falciani ONLUS, Milan, Italy.
Vladimira Tichà is an interventional radiologist at Fondazione Falciani ONLUS, Milan, Italy
Giancarlo Beltramo is head of radiosurgery at Centro Diagnostico Italiano, Milan, Italy.
Alberto Gramaglia is head of radiotherapy at Monza General Hospital, Monza, Italy.
Gianluigi Patelli is head of radiology at Casa di Cura San Francesco, Bergamo, Italy.
Tracing back his line to interventional radiology (IR), Muneeb Ahmed, interventional radiologist and the current president of the Society of Interventional Oncology (SIO), told Interventional News of how he followed in the footsteps of his father, Rashid Ahmed, an influential interventional radiologist who propelled the field in Pakistan. Guided to IR, Ahmed’s career has driven research and innovation, and, throughout his presidency, Ahmed has sought the global expansion of the interventional oncology (IO) community and furthered clinical discovery via SIO-led clinical trials. As his term concludes, he reflects on these accomplishments and his continued commitment to advancing the field of IO.
What attracted you to a career in IR?
I have known IR as a field from a young age, both with regards to its impact on patients, and to its novelty and innovation. My father, Rashid Ahmed, was an interventional radiologist who trained in the USA before moving back to Pakistan, his home country, to develop both diagnostic and interventional radiology as fields within that country. Throughout his 35-year career there, he introduced a multitude of new procedures and types of imaging studies in the country, established new training programmes, started a national radiology society and journal, trained several generations of diagnostic and interventional radiologists, and was ultimately recognised by the government for his service with one of the highest national civilian awards. All this while, he was passionate for learning new techniques, and happiest when he had performed a life-saving procedure on a patient. I remember watching him perform angiography and embolization, talking with him about his cases, and meeting his grateful patients. This passion for continuous learning in IR left a significant impression on me.
When I had the chance to work within IR, and more specifically interventional oncology (IO), I understood his excitement for the field. There were so many different procedures to learn, a wide range of diseases to understand, and the technological advances seemed endless. By the time I was deciding on fellowship, IR was the clear and only choice, and I haven’t looked back since. IR has fulfilled that promise, as I continue to be excited about where the field is going, and all of the new and innovative treatments that are being developed.
Who were your mentors throughout your career?
I have been fortunate to have had several important mentors who have provided very important opportunities, guidance, and support at critical steps in my career-to-date. The earliest was Melvin Clouse, a world-renowned interventional radiologist at Beth Israel Deaconess Medical Center (BIDMC) in Boston, USA, who involved me in summer research programmes as a medical student from Pakistan, and encouraged my interests in scientific research, and ultimately in radiology.
One of the key introductions he made was to a young Nahum Goldberg, who was just starting out as an attending consultant at BIDMC and doing innovative research in percutaneous tumour ablation with radiofrequency energy. From that point onwards, through a three-year post-doctoral research fellowship, and in the over 25 years since, we continued to work together on our shared research to advance the field of image-guided tumour ablation. Nahum has been my key mentor throughout this time, instilling a passion for research, providing advice at critical career decision points, and serving as a role model for how to build an academic career.
More recently, I have also benefited from mentors that I have met later in my career. Fred Lee shared his insights in leadership and entrepreneurship during my time as a division chief. Through my volunteerism with the SIO, I have also been able to follow amazing examples of societal leaders in Matt Callstrom and Bill Rilling, both of whom have provided me with valuable mentorship.
I have appreciated each of these mentors, and sought to emulate and honour their generosity by providing similar opportunities, support, and guidance to younger interventional radiologists who are trying to develop successful careers in IR.
Is there a memorable case that stands out to you?
Many years ago, I started treating a patient with metastatic renal cell cancer who had already survived six years following a nephrectomy and various immunotherapies. He stood out at the time for his positivity and enthusiasm for life, his desire to find the right balance between his quality of life and longevity, and his faith in and excitement for new and emerging therapies (he received interleukin therapy as part of early clinical trials in renal cell carcinoma). When I first met him, he had developed isolated metastases in his single kidney—for which I performed a successful cryoablation. Over the next eight years, I treated additional metastasis in his liver, lung, and adrenal gland—and we were able to keep his cancer at bay through intermittent IO therapies, including repeated ablation and embolization. He ultimately succumbed to his disease, but after living his life to the fullest and with happiness and excitement. When his family reflected on his experiences after he passed away, the thing that they were most thankful for from the various minimally-invasive treatment options that he received over the years, was that he always had hope. Hope, even near the end of life, is an important thing that IR often offers even when patients receive news that their cancer has progressed through other therapies. When I think about him, I remember that it’s important to appreciate what we can do for people’s happiness—the importance of kindness and empathy, and the value of IR done well on a patient’s life.
You have published several research papers in 2024. Which of your recent endeavours has been the most insightful?
I firmly believe that we need to advance IR through a multi-pronged research approach, developing early ideas, proving their clinical efficacy (starting with proof-of-concept studies and progressing through to robust prospective clinical trials), and then tackling barriers to widespread clinical implementation such as cost-effectiveness and utilization research, and then training the next generation of interventional radiologists. I am excited about all of the research projects coming out of the BIDMC IR team in recent years— tackling questions at each of the various phases I mentioned. If I had to pick, the work that my partner Jeff Weinstein and I are doing on studying an operator’s hand motion while doing IR procedures is very interesting, as it provides us with insight into how interventional radiologists learn. This work will hopefully provide objective measures to assess technical skill acquisition and design better training methods in IR.
Similarly, I am also excited about our recent study with percutaneous cryoablation for locally recurrent prostate cancer—Vijay Ramalingam et al in the Journal of Vascular and Interventional Radiology (JVIR) 2024—as this incorporates a computed-tomography (CT) guided approach to treating focal prostate bed cancer recurrences that can be expanded and used at many centres overcoming resource-limitations that are associated with previously reported magnetic resonance imaging (MRI) guidance based techniques. Focusing on ways to make IO therapies accessible to a wider range of patients is something that I am very passionate about.
As your presidency of the SIO comes to a close, what have been your greatest achievements?
Two years as SIO president has flown by! The society team, including all of the volunteers and the staff (under Jena Stack’s extremely capable leadership) continues to accomplish so much. I am very excited that we have gotten the ACCLAIM trial off the ground and well on its way to completion, and are now planning additional trials. We have expanded our society membership through key global partnerships and are continuing to build collaborations with other societies on joint projects. We have continued to develop and offer the highest calibre of meeting content— last year’s SIO 2024 annual meeting having been one of our most successful meetings yet, and we have an exciting programme planned for 2025. Our most recent SIO Masterclass in musculoskeletal IO, a unique hands-on immersion-style programme that we recently held here at BIDMC, was also exciting and very successful.
At the beginning of my presidency, a priority was to strengthen IO’s global voice. We have made a lot of progress towards this goal. One of our key objectives has been to implement a ‘big-tent’ philosophy within the SIO, and specifically that anyone involved in the IO space—whether performing IO or wanting to learn more about IO—has a place in our society. To this end, we have created global SIO chapters through partnerships with different societies around the world, including the Middle East, creation of our Asia-Oceanic chapter and most recently with creation of our Latin American chapter. This has led to closer collaboration in these regions, and a growth in the SIO’s membership to over 1,300 members worldwide.
Overall, I am most proud of the extremely energetic and growing group of volunteers that we are attracting to the SIO—without whom we would not be able to continue to advance the IO space on many fronts. Success begets success.
How is the ACCLAIM trial progressing?
I am very excited about the ACCLAIM trial— we are making great progress! Thanks goes to Constantinos T Sofocleous, the trial’s global principal investigator, all of the volunteers who are involved in the trial, and the SIO staff team that is overseeing trial operations. We have opened 10 international sites, and have already recruited over half of the necessary patients, ahead of our original schedule, and look to close out patient recruitment by the fall of 2025. This is a pivotal prospective study that incorporates formal ablation margin confirmation as the technical endpoint to performing ablation for colorectal liver metastases, and the successful completion will provide necessary evidence to help us establish use of margin confirmation as the standard of care when performing liver ablation. This is the first multi-industry supported trial in our space, and the first that the SIO has developed and initiated, so I am particularly proud that we have been able to execute this so well.
Have any recent research papers caught your attention in the last 12 months?
I am very excited about the recent presentation of the COLLISION trial—a phase three randomised multicentre study comparing surgical resection and percutaneous thermal ablation for small liver-only colorectal cancer metastases led by Martjin Meijerink and colleagues from Amsterdam University Medical Center. This study stands out to me for how well it was designed and executed, how it incorporated many of the lessons that we have learned about thermal ablation over the years, including the importance of achieving a documented appropriate ablation margin (>1cm for colorectal metastases), use of contrast-enhanced margin assessment, and re-ablating patients where an adequate ablative margin was not achieved. To me, this underscores how the IO community has grown in the field—implementing high-quality studies that prove that our therapies offer patients excellent outcomes in a safer and better tolerated manner. The study team is to be commended, and I look forward to reading the full published manuscript when it becomes available.
What are your hobbies and interests outside of medicine?
As I am originally from Karachi, Pakistan, I enjoy travelling to new places around the world. Some of my most enjoyable trips have been to the Mediterranean, Mallorca, and the Maldives. I enjoy reading and spending time with my family, including my wife, Susan, my two children, Saif and Sofia, and our two snowshoe cats.
Born and raised in Singapore, interventional radiologist Tay Kiang Hiong is professor and head of the department of vascular and interventional radiology at Singapore General Hospital and and president-elect of the Asia-Pacific Society of Interventional Radiology (ASPCVIR). After completing his medical and diagnostic radiological training in Singapore, Kiang Hiong trained at the University of British Columbia in Vancouver, Canada under the mentorship of Lindsay Machan. Reflecting on his training and career in conversation with Interventional News, Kiang Hiong talks about the past, the present and the future of interventional radiology (IR) in the Asia-Pacific region, imparting advice for trainees starting out.
IN: How was it starting a career in IR in Singapore?
Starting a career in IR in Singapore has been both exhilarating and challenging. Exhilarating because I started in the 1990s and 2000s where IR was experiencing rapid evolution and growth in Singapore. We had new devices or techniques emerge every few months and it was very gratifying to see IR procedures replacing traditional surgical treatments as the new standard of care. In many patients with dire conditions who are unfit for surgery, IR often is the last bastion that can save their lives. To this day, I feel very privileged to be an interventional radiologist.
However, it was also challenging as we are short of manpower. Especially in the early days, where the work hours were long, it was extremely hard to balance work and spending time with the family, not to mention research and teaching commitments limiting this quality time as well. As IR gained success, it attracted other specialists, leading to exhausting “turf wars”. Additionally, IR’s lack of public and physician awareness has limited referrals, though this is gradually improving through public campaigns and medical school education on IR.
IN: What are the key differences in IR practice between the Asia Pacific region and Europe?
It is not surprising that the IR practice is different in Asia Pacific and Europe due to differences and variations in healthcare infrastructure, patient demographics and disease prevalence, economic status and regulatory frameworks.
Healthcare infrastructure in the Asia-Pacific region varies greatly, from advanced systems (e.g. Japan, Singapore, South Korea, Australia) to developing countries with no access to advanced medical technologies. As a result, IR services and technologies differ significantly, with some countries having no IR presence. In less developed economies, IR is limited to basic procedures like biopsies and drainages due to cost constraints, while well-developed countries offer a full range of IR procedures, often reimbursable. Interventional oncology (IO) is common due to high rates of hepatocellular carcinoma (HCC), but endovascular interventions for peripheral vascular and aortic diseases are diminishing and limited to a few centres of excellence in our region as they are mostly handled by cardiologists or vascular surgeons currently.
With respect to IR training, the Asia Pacific region has fewer formalised and standardised IR training programmes. Some countries have established formal IR fellowships and specialised training pathways, but in many parts of our region, training is much less structured, with trainees often having to go abroad for fellowship training, often times in Europe or North America. In the future, the ASPCVIR aspire to implement a vehicle for IR training much like the European Board of Interventional Radiology (EBIR) certification, to standardise IR training and certification in our region.
IN: As president-elect of APSCVIR, what do you hope to achieve in your term?
I have been involved with the APSCVIR for many years. Before 2016, I sat in the executive committee for several years. After 2016, I was the secretary general for three terms under the newly registered society, and now I am the president elect. I have been in a very privileged position for many years now, with the ability to influence and shape some of the strategic directions for APSCVIR.
We formerly registered the society in 2016 because we wanted to do more than just organising a scientific meeting. IR education has always been the main focus of APSCVIR and we do this through our annual scientific meeting and outreach programme.
The outreach programme is a signature programme of our society. Led by Bien Soo Tan (Singapore General Hospital, Singapore) it is comprised of onsite lectures, workshops and live case demonstrations supplemented by webinars every two to three months. The faculty of the outreach programme are all volunteers who fund their own travel to do so, and faculty from the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and the Society of Interventional Radiology (SIR) are regularly invited to help out in these programmes. We are poised to expand this initiative to more countries.
The Japanese Society of Interventional Radiology (JSIR) recently offered their online journal InterVentional Radiology (IVR) to be the official journal of JSIR and APSCVIR. This opens up another avenue for IR education and research for our members which I hope to actively promote in the coming years.
Strengthening international collaboration with other IR organisations around the world, especially SIR and CIRSE remains our top priority. Other than knowledge and skills exchange at our respective annual meetings, we hope to collaborate in other areas like journal publishing, IR certification exams, advocacy for IR, online education platforms etc. Through these efforts, my colleagues and I in the executive board of APSCVIR hope to leave a lasting impact on the growth, accessibility, and quality of IR across the Asia-Pacific region.
IN: What advice can you give to interventional radiologists starting out in the Asia-Pacific region?
Starting out as an interventional radiologist in the Asia-Pacific region offers both exciting opportunities and unique challenges. The region’s diversity in healthcare systems, patient populations, and access to technology means that your path might vary depending on where you’re based. I have the following tips for new interventional radiologists in this dynamic environment:
Build a strong foundation in diagnostic radiology
A strong grasp of diagnostic radiology is essential for becoming an excellent interventional radiologist. Proficiency in imaging interpretation ensures precise planning and execution, while knowledge of cross-sectional anatomy is key for guiding complex interventions like tumour ablation and embolization.
Prioritise hands-on training
Hands-on experience across various IR subspecialties is crucial for working in diverse clinical settings. Pursue a formal IR fellowship at a reputable centre in Asia Pacific, Europe, or North America if possible. Also, attend workshops, conferences, and hands-on courses from organisations like APSCVIR, SIR, or CIRSE to refine your skills.
Adapt to local healthcare realities
IR resources vary greatly across the Asia-Pacific, and you may often work in resource-limited environments. Adapting to local healthcare infrastructure is key to success. Get involved in expanding IR services by demonstrating flexibility, leadership, and advocating its value to administrators and colleagues.
Stay current with technological advances
IR is closely linked to advances in imaging and device technology. Stay updated on innovations like robotic interventions, angio-computed tomography (CT), cone-beam CT, and new embolisation or ablation devices. Despite regional limitations, global resources such as online platforms, journals, and webinars can keep you informed about the latest techniques.
Focus on research and evidence-based practice
Research is critical to advancing the field of IR, and there is great potential for original research in the Asia-Pacific region, where unique patient demographics and disease profiles can yield valuable insights. Consider engaging in clinical trials or retrospective studies to contribute to the evidence base in IR.
Prioritise on patient-centred care
Many patients in the Asia-Pacific region may be unfamiliar with IR. Spend time educating patients about how IR can help them, the risks involved, and what to expect during recovery. Emphasise the importance of follow-up to ensure long-term success of procedures. Clear communication builds trust and improves patient outcomes.
Advocate for policy and reimbursement changes
In some Asia-Pacific countries, reimbursement for IR procedures is limited, and policies may not always reflect the cost-effectiveness of IR. Advocate for improved reimbursement models and integration of IR into national healthcare systems, emphasising the potential to reduce hospital stays, complications, and long-term costs.
Stay resilient and be ready for challenges
IR is evolving rapidly, requiring adaptability to new technologies, healthcare changes, and patient needs. Success in the Asia-Pacific region demands determination, adaptability, and continuous learning, with a focus on foundational skills, collaboration, and engagement with professional societies. By doing so you can make a lasting impact in your career and contribute to the growth of IR across the region.
Rush University System for Health has announced today that it has acquired Quantum Surgical’s Epione platform. Rush University Medical Center is among a select group of hospitals nationwide—and the first in the Midwest—to adopt this technology.
The Epione platform is a state-of-the-art robotic-assisted technology for interventional radiologists who perform percutaneous ablations of abdominal tumours, a minimally invasive treatment often used with curative intent. Epione supports physicians in planning the optimal targeting of a tumour and monitoring the patient’s position in real-time. The robotic arm uses this information to precisely position the physician’s instrumentation. This enables increased accuracy of the ablation procedure and allows for immediate confirmation if the tumour ablation was successful, a press release has stated.
“Rush’s interventional radiology programme is one of the best programmes in the country, excelling in clinical interventional care, education with one of the largest and most sought-after residency programmes, and robust research activities with multiple ongoing clinical trials,” says Bulent Arslan, director of vascular and interventional radiology (IR) at Rush.
“We are very happy to be first in the region to provide this new technology to our patients that will make their experience better, more efficient, and safer. Robotic systems have been in surgical care for many years and now are available for the interventional care of patients. We treat complex lesions throughout the body with ablative therapies, but it is not always easy to reach our targets, and there is some risk involved in the process.
Using Epione, we will be able to reach most locations with computerised guidance using patients’ existing computed tomography (CT) or magnetic resonance imaging (MRI) images relatively easily and with less risk. This is an evolution in cancer patient care, and we are excited to be the first in the Chicago area to offer it.”
While surgery may be an option for some, it often involves higher costs and longer hospital stays. Epione is a minimally invasive option for patients with small tumours.
“We are thrilled to celebrate this milestone as Quantum Surgical’s Epione platform arrives in the Midwest,” said Bertin Nahum, chief executive officer (CEO) and co-founder of Quantum Surgical. “We are excited to collaborate with the esteemed team at Rush University System for Health, as our mission is to ensure that as many cancer patients as possible can benefit from this minimally invasive technology.”
iVascular has announced the initiation of Opal, the first-in-human study with the new embolic liquid Amber, based on a radiopaque biocompatible copolymer. Opal is a prospective, single-arm, multicentre study with a sample size of 70 patients requiring peripheral embolization. The study is a collaboration between 10 centres in Spain that specialise in embolization and will be led by Fernando Gómez (Hospital La Fe, Valencia, Spain).
The main objective of the Opal study is to evaluate the safety and efficacy of Amber in vascular anomalies, haemorrhages, aneurysms, pseudoaneurysms, type II endoleaks, varicose veins, portal veins, hypervascular tumours, and pathological organs.
The results of the study will provide crucial data on the safety and efficacy of Amber, as determined by the rate of complete vascular occlusion in all the evaluated indications. Patients will be followed up at discharge and at one, three and six months after intervention. Throughout the study, Gómez, together with the clinical events committee (CEC) and the data safety monitoring board (DSMB), will ensure patient safety and the scientific integrity of the data obtained.
“The Opal study may be the first step towards changing the way embolization with liquid is performed. All of us who have been able to test Amber agree that beyond its excellent properties in terms of penetration and visualisation, it will increase safety in this type of treatment,’ says Gómez.
The iVascular research and development team assures that Amber has been designed to overcome the limitations of current embolic liquids, a recent press release states. “Achieving total control of the product together with a homogeneous and intrinsic visualisation, being a ready to use liquid, have been the main objectives of Amber’s design,” says Sofía Valle, project leader for the development of the embolic.
Andreas Mahnken (University Hospital Marburg, Marburg, Germany), distinguished interventional oncologist, educator and advocator for interventional radiology (IR) standardisation, dives into the most salient outcomes from the recent Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Clinical Practice Survey.
Interventional radiology—IR—has become a clinical discipline, with interventional radiologists ideally taking care of the entire patient pathway, from initial multidisciplinary tumour board (MDT) assessment to discharge and follow-up.1 The implementation of continuous quality improvement (QI) activities represents a major factor for high-quality provision of clinical care as well as patient safety.1-3 To what extent such activities as well as the use of patient safety checklists are currently undertaken by interventional radiologists was part of the recent CIRSE Clinical Practice Survey, conducted by the CIRSE Clinical Services in IR Task Force from November 2023 to January 2024.4-5 The findings of the survey will further feed into CIRSE’s activities supporting clinical practice building, quality management and patient safety in IR.
The CIRSE Clinical Practice Survey included 63 structured items addressing the areas of clinical practice training, infrastructure and personal experience as well as patient safety and continuous quality improvement. Eight items were dedicated to the latter two topics. The survey collected a total of 520 responses and was closed in January 2024.
The member survey, which was answered by interventional radiologists from Europe and beyond, showed encouraging results with over half of the respondents having an established clinical practice as well as direct patient access, taking primary responsibility for patient care. A total of 77.3% of respondents indicated the regular use of patient safety checklists (Figure 1), which is strongly encouraged by CIRSE, with a checklist dedicated to IR being available in multiple languages.
In terms of continuous quality improvement, 68.1% indicated that they perform dedicated quality improvement activities. These included recording morbidity and mortality data (70.9%), daily case discussion (68.1%) and MDT outcome (56.5%). In the open responses, respondents to this question indicated most frequently case discussions, education and certification, quality assurance registries or programmes, audits, checklists and team teachings as regular activities in their departments.
While the vast majority of responding interventional radiologists actively engage in continuous QI activities and the use of patient safety checklists, there is still room for improvement and the European IR community will take advantage of the survey results to further design tools that will help interventional radiologists engage in clinical practice activities and encourage dedicated IR quality improvement. As part of this process a clinical practice manual was developed and CIRSE actively supports quality-driven accreditation measures, such as the International Accreditation System for Interventional Oncology Services (IASIOS).1
The full results of the survey have been published in the journal CardioVascular and Interventional Radiology (CVIR) with Anthony Ryan (University Hospital Waterford, Waterford, Ireland) as lead author.4 A presentation on the results relating to quality improvement and patient safety was held at the CIRSE 2024 annual congress (14–18 September, Lisbon, Portugal) and is available in the CIRSE Library.5
References:
Mahnken, A.H., Boullosa Seoane, E., et al. CIRSE Clinical Practice Manual. Cardiovasc Intervent Radiol 44, 1323–1353 (2021). https://doi.org/10.1007/ s00270-021-02904-3.
Binkert, C.A. Fostering clinical practice in IR regardless of (sub) specialty status. CVIR Endovasc 6, 23 (2023). https://doi.org/10.1186/s42155-023- 00370-1.
Morgan, R., Haslam, P., et al. Provision of Interventional Radiology Services 2023. Cardiovasc Intervent Radiol 47, 3–25 (2024). https://doi. org/10.1007/s00270-023-03600-0.
Ryan, A.G., Slijepcevic, B., et al. Developing a Clinical Service in Interventional Radiology: Results from the 2024 CIRSE Clinical Practice Survey. Cardiovasc Intervent Radiol (2024), https://doi.org/10.1007/ s00270-024-03858-y.
CIRSE 2024 Book of Abstracts. Cardiovasc Intervent Radiol 47 (Suppl 7), 441–1880 (2024). https://doi. org/10.1007/s00270-024-03850-6.
Andreas Mahnken is an interventional radiologist and oncologist at the University of Marburg, Marburg, Germany.
A focus session dedicated to quality-of-life (QoL) outcomes in interventional oncology (IO) at this year’s Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14–18 September, Lisbon, Portugal) saw experts study the critical importance of patient-reported outcome measures (PROMs) and the growing recognition of these data as key indicators of procedural success in cancer care.
In conversation with Interventional News, Roberto Iezzi (Policlinico Universitario Fondazione Agostino Gemelli, Rome, Italy) extracted key points from his presentation. “The journey is becoming more important than the destination,” he stated, praising the range of effective interventions that have been developed in IO today. “The good news is that we have so many treatment options—the bad news is that we have so many treatment options,” Iezzi deliberated. “Tailored to each patient’s disease and comorbidities, approach to treatment can be more dynamic and the right selection is the most important part of our job”, he added.
Iezzi explained that, today, precision cancer care has come so far as to cure 50% of metastatic cancer cases and extend the life expectancy of the other 50%. He referenced a study published earlier this year by Wörns et al, in which the investigators interviewed patients with hepatocellular carcinoma (HCC) on their treatment goals. Patients described extending overall survival as their most important goal in early-stage HCC, whereas for advanced/unresectable disease, QoL and managing side effects became their key priority.
“Undeniable connection” between QoL and survival
In treating advanced disease, Iezzi described the creation of a new subgroup of ‘chronic’ cancer patients, in whom life-extending treatment is achieved, but quality of life is maintained in careful balance. “This is a future concept,” said Iezzi, teasing new research to be published this year in which he and his colleagues will investigate how much life is sacrificed by cancer patients due to life-extending treatments.
Recent research attempted to evaluate the effect of QoL improvement on patient outcome. Earlier this year, Balitsky et al’s systematic review and meta-analysis of PROMs across Medline and Embase databases suggested that integration of PROMs into treatment improved health-related quality of life (HRQoL) and the overall risk of mortality at 12 weeks. In their report, however, the authors note that improvements in HRQoL dropped off at the 24-week mark and showed no association at 48 weeks.
Their results suggest that QoL improvements could benefit patients in the early phase of treatment. Vlasios Sotirchos (Memorial Sloan Kettering Cancer Center, New York, USA), who presented on the immediate QoL impact that IO treatments have for liver cancer patients, stated that there is an “undeniable connection” between QoL and overall survival in general. He told Interventional News that this could be due to the development of patient-centred treatment plans adapted to individual patient needs reported via PROMs data collection at each patient visit, rather than taking a one-size-fits-all approach. By placing focus on the physical, emotional and social effects of cancer and its treatments, interventionists can help dispel distress and elevate QoL, which Sotirchos stated can be “extremely meaningful” in patients with with cancer at any stage.
A dynamic approach to QoL
Placing QoL at the centre of the algorithm, treatment takes customisable form in Iezzi’s view. “We can select the best multimodality approach—we know that ablation is better than surgery when considering quality of life, and that chemoembolization and radioembolization are better than systemic chemotherapy. This way, we can provide dynamic systemic and locoregional treatment and achieve quality-of-life improving strategies such as chemo-holidays, and then restart treatment with appropriate systemic intensification,” he stated.
Iezzi made clear that setting a well-planned, dynamic treatment plan in motion is all well and good, but without clear communication to manage patient expectations, the overall success of said procedures can be limited. He went on to expand on what defines curative or palliative treatment and the flexibility of these concepts.
“If a 50-year-old man is given 10 years, this is not a curative approach, but, if an 85-year-old man is also given 10 years, this would be considered curative despite the treatment modality. The term palliative has completely changed over the last ten years,” Iezzi said. “Previously, palliation was akin to ‘waiting for death’ whereas today, all treatments are considered palliative due to the dual goal of extending-life years and maintaining good quality of life.”
Addressing the psychological impact of a cancer diagnosis and subsequent treatment on the patient, Iezzi suggested that a psychoncologist should be inducted into the multidisciplinary team. He noted that discussion during the session at CIRSE turned to cultural differences in communication with cancer patients, noting that in Italy patient-physician communication styles are more indirect than those of Canadan interventionists—to which session moderator and native Canadian, Riad Salem (Northwestern University, Evanston, USA) agreed. Providing emotional support throughout the therapeutic process, the implementation of a psychoncologist in routine cancer care could help to standardise PROMs from country to country.
Disparities between countries worldwide are well-documented, Sotirchos added, stating that many patients have limited access to this level of treatment or can experience significant delays in receiving care. “Treatment access inequities impact QoL and addressing this issue should be a priority for healthcare systems,” he said.
Barriers to collecting QoL data Although research conducted by Basch et al found that obtaining PROMs data has a positive impact on the patient and therapy outcomes, the collection of said data has been shown to be burdensome for both patients and centres.
Presenting on why this is during the CIRSE session, Nathalie Kaufmann—chief operating officer and procurator at Next Research—highlighted that, in 10 years of experience conducting CIRSE research, limited staffing, logistical centre issues, and patient refusal and incapacity were detrimental to the collection of PROMs. While about 86% of hospitals participating in CIRSE research projects returned PROMs data overall, most of the questionnaires were completed at baseline visits before treatments and return rates declined thereafter.
She detailed their plan of launching an electronic PROMs questionnaire in 2017–2018 in the hope of improving questionnaire return rates. Despite a lengthy development process improving language functionalities and browser compatibility, no hospital used the online questionnaire throughout the time period.
Centres attributed this to average patient age, which was mid-60s—“this may have created a challenge”, Kaufmann said, however, looking back now, the electronic PROMs tool might not have simplified the data collection process sufficiently.
Today, Kaufmann added that technology and patients’ ability to navigate it has improved, and they intend on conducting a similar study in the near future.
Irrespective of how QoL data will be collected in future, it will remain an essential part of research in IR. In an ideal world, Kaufmann states that PROMs data would be used in routine clinical practice outside of research as well. Demonstrating the value of collecting QoL data during research projects is an important step in this direction.
“Through our research projects we’re sometimes working with centres that are collecting quality-of-life data for the first time and we are then helping to establish processes, such as, if they think their patient might be experiencing depression, how do they communicate with the patient and where can they refer them,” Kaufmann said. “Collecting this data is valuable to the patient and healthcare professional to improve communication between the two,” she added.
“Mandatory” QoL outcome measures in clinical trials
Later in his presentation, Iezzi drew attention to the European Society for Medical Oncology-Magnitude of Clinical Benefit Scale (ESMO-MCBS) grading system to assess the robustness for QoL research. In the introduction to the scale, the authors asserted that QoL—assessed with a validated tool—must be at least a secondary endpoint in future IO trials. Advocating for mandatory QoL questionnaires, Iezzi underlined that particularly in a non-curative setting, these assessments can aid multidisciplinary teams in selecting effective interventions. “It’s important we make patients aware of the real purpose, aim and outcomes of the procedures we are performing,” Iezzi added, so that patient and procedural goals align.
Sotirchos reflected that obtaining QoL metrics has a two-fold benefit for patients and interventionists, and will help to improve outcomes and healthcare policy decisions.
“Due to the multidimensional nature of QoL assessments, including several generic and disease-specific instruments, comparisons across studies can be very challenging,” he said. Yet, Sotirchos averred that, through the development of new technologies and the demonstrated value of recording PROMs to exemplify the benefit of IO procedures, the collection of this data must be prioritised in both clinical trials and routine periprocedural care.
Endologix has announced the final 36-month results from the DETOUR2 study—a prospective, single-arm, international, multicentre clinical evaluation of the novel Detour system for fully percutaneous femoropopliteal bypass procedures.
A press release details that the findings highlight the durable efficacy of the Detour system, which is comparable to open bypass with a synthetic graft. Additionally, the low rates of complications and deep vein thrombosis (DVT) demonstrate the favourable safety profile of this novel technique.
Endologix notes that the Detour system offers a unique approach to treating complex peripheral arterial disease (PAD), enabling physicians to percutaneously bypass lesions in the superficial femoral artery, by using stents routed through the femoral vein to restore blood flow to the leg. The Detour system is comprised of the Endocrossdevice and Torus stent grafts.
The 36-month results from the study were presented during a late-breaking clinical trials session at VIVA 2024 (3–6 November, Las Vegas, USA) by one of the study’s principal investigators, Sean Lyden (Cleveland Clinic, Cleveland, USA). “These extended results from the DETOUR2 study help continue to demonstrate using the Detour system is comparable to surgical bypass but without requiring general anaesthesia, which can come with additional complications and longer length of stay,” said Lyden.
“The 36-month data from the DETOUR2 study underscore the potential of the Detour system to significantly impact the treatment paradigm for long segment SFA disease,” said Matt Thompson, president and chief executive officer of Endologix. “We are confident in the Detour system’s ability to offer a less invasive, effective alternative for patients with challenging femoropopliteal lesions. As we move forward, our focus remains on ensuring optimal patient outcomes through rigorous training, ongoing data collection, and the PTAB-1 postmarket study to further validate these results in real-world settings.”
The DETOUR2 study enrolled 202 patients at 32 sites, and 200 patients were treated with the Detour system. The mean lesion length was 32.7cm, 96% were chronic total occlusions (CTO), and 70% were severely calcified.
The results presented highlight:
Freedom from clinically driven target lesion revascularisation was 66.8% through three years.
Primary patency was 58.2% through 36 months.
Clinical success, defined as improvement in at least one Rutherford category at 36 months, was 96.7%.
Freedom from symptomatic DVT was 95.9% at 36 months.
Freedom from major lower limb amputation was 98.5% at 36 months.
Shockwave Medical, part of Johnson & Johnson MedTech, has announced the first clinical outcomes associated with the Shockwave Javelin peripheral intravascular lithotripsy (IVL) catheter, a novel, non-balloon-based lithotripsy platform designed to modify calcium and cross extremely narrowed vessels in patients with peripheral arterial disease (PAD).
A press release notes that the 30-day results met both prespecified performance goals while showing a similar safety and effectiveness profile to balloon-based Shockwave IVL catheters. The results, which helped support US Food and Drug Administration (FDA) clearance of the technology last month, were presented as a late breaker at VIVA 2024 (3–6 November, Las Vegas, USA).
“The outcomes were exactly what we have come to expect from IVL studies—a strong safety profile with the low final residual stenosis that physicians would hope to achieve,” said JD Corl (The Christ Hospital, Cincinnati, USA), principal investigator of the FORWARD PAD study. “These initial data are promising and pave the way for a new approach to the application of Shockwave IVL in our peripheral practices. With technologies now suited to safely address both crossable and uncrossable lesions, IVL has a unique opportunity to play an increasingly important role in optimising outcomes for a wider set of patients with PAD.”
Corl reported at VIVA that the Shockwave Javelin peripheral IVL catheter met both prespecified safety and effectiveness endpoints, with a major adverse event rate of 1.1% at 30 days, and a technical acute procedural success rate of 99%. Additionally, at final angiography, angiographic complications were restricted to a single case of dissection with no reported perforations, abrupt vessel closure, distal embolisation or no-reflow.
The feasibility and investigational device exemption (IDE) studies of the Shockwave Javelin IVL catheter, MINI S and FORWARD PAD, respectively, were prospective, multicentre, single-arm, angiographic core-lab adjudicated studies with similar inclusion and exclusion criteria. The studies enrolled 90 patients with 103 heavily calcified, stenotic peripheral arterial lesions. The average lesion length was 77mm, and just under half of the target lesions were located below the knee, and over a third were chronic total occlusions.
“Recognising the risks that patients with difficult-to-cross lesions are exposed to with other treatment modalities, we’re extremely optimistic about the role that Shockwave Javelin could play in offering an effective alternative crossing and treatment tool with a strong safety profile,” said Nick West, chief medical officer at Shockwave Medical. “We look forward to learning more about the performance of the Shockwave Javelin IVL catheter as we add to the ongoing trial follow-up data with a limited market release of the device in the coming months.”
Bolt Medical has announced the completion and results of the RESTORE ATK and RESTORE BTK pivotal clinical trials investigating the company’s Bolt intravascular lithotripsy (IVL) above-the-knee (ATK) and below-the-knee (BTK) systems for the treatment of peripheral arterial disease (PAD) in patients with moderate to severe calcified lesions.
Thomas Zeller (University Heart Centre Freiburg-Bad Krozingen, Bad Krozingen, Germany) presented the data from both studies in a late-breaking clinical trials session at VIVA 2024 (3–6 November, Las Vegas, USA).
RESTORE ATK enrolled 95 patients in the prospective, single-arm trial designed to assess the safety and efficacy of the Bolt IVL system in the superficial femoral and popliteal arteries. The study was led by principal investigator Marianne Brodmann (Medical University of Graz, Graz, Austria).
The primary safety endpoint of the trial was freedom from major adverse events (MAE) within 30 days following the index procedure. The primary efficacy endpoint was procedural success, defined as residual diameter stenosis <50%. Through 30 days, there were no reports of MAE including severe dissection, perforation, or unplanned target limb major amputation and no clinically driven target lesion revascularisation supporting the achievement of both the primary safety and efficacy endpoints in the trial.
RESTORE BTK is a prospective, single-arm trial designed to assess the safety and efficacy of the Bolt IVL system in 20 enrolled patients with moderate to severe calcified infrapopliteal arteries. The study was conducted at three centres across Europe and led by principal investigator Michael Lichtenberg (Arnsberg Clinic, Arnsberg, Germany).
The primary safety endpoint of the trial was freedom from MAE within 30 days following the index procedure. The primary efficacy endpoint was procedural success, defined as acute reduction in percent diameter stenosis of the target lesion. Through 30 days, there were no reports of MAE including severe dissection, perforation, or unplanned target limb major amputation and no clinically driven target lesion revascularisation supporting the achievement of both the primary safety and efficacy endpoints in the trial.
“The patients treated in the RESTORE BTK trial presented challenges to traditional IVL therapy. The improved deliverability and crossability of the Bolt IVL catheter accessed complex lesions with ease. Moreover, the visible emitters on the Bolt IVL catheter provided me with the ability to directly focus acoustic energy on areas of persistent calcification,” said Lichtenberg in a Bolt Medical press release.
“The Bolt team is proud to accomplish these major clinical milestones with the completion of both the RESTORE ATK and RESTORE BTK pivotal trial,” said Keegan Harper, chief executive officer of Bolt Medical. “Bolt IVL is positioned to expand the peripheral market and advance patient care as the company plans regulatory submissions for both peripheral devices in the near future.”
Bolt Medical notes that the data presented at VIVA 2024 will be used to support US Food and Drug Administration (FDA) and CE mark regulatory submissions.
New research finds that genicular artery embolization (GAE) has a lasting benefit of up to two years for moderate to severe symptomatic knee osteoarthritis
Interview: Asia-Pacific Society of Interventional Radiology (ASPCVIR) president-elect Tay Kiang Hiong speaks on the future of interventional radiology (IR) in Singapore
Profile: Muneeb Ahmed (Boston, USA)
Various key updates from the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14–18 September, Lisbon, Portugal), including new data concerning percutaneous transluminal angioplasty (PTA) and a country-by-country analysis of carotid artery stenting (CAS) practice
New research finds that genicular artery embolization (GAE) has a lasting benefit of up to two years for moderate to severe symptomatic knee osteoarthritis
Interview: Asia-Pacific Society of Interventional Radiology (ASPCVIR) president-elect Tay Kiang Hiong speaks on the future of interventional radiology (IR) in Singapore
Profile: Muneeb Ahmed (Boston, USA)
Various key updates from the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14–18 September, Lisbon, Portugal), including new data concerning percutaneous transluminal angioplasty (PTA) and a country-by-country analysis of carotid artery stenting (CAS) practice
Presented today, late-breaking data from the second year of the LIFE-BTK clinical trial demonstrate the long-term effectiveness of the US Food and Drug Administration (FDA)-approved Esprit BTK everolimus-eluting resorbable scaffold system (Abbott Vascular) in patients with the most severe form of below-the-knee (BTK) peripheral arterial disease (PAD). The data show that the Esprit BTK offers sustained benefits over balloon angioplasty with fewer repeat procedures at two years.
The LIFE-BTK trial evaluated the Esprit BTK in more than 260 patients worldwide with BTK PAD, comparing treatment with the Abbott device to balloon angioplasty—the current standard of care. Following the presentation of one-year results at TCT 2023 (23–26 October, San Francisco, USA), two-year results were revealed during a late-breaking data session at VIVA 2024 (3–6 November, Las Vegas, USA).
“PAD is a dangerous condition that is complex to treat, with limited approved treatment options,” said Brian DeRubertis (New York Presbyterian–Weill Cornell Medical Center, New York, USA), presenter and one of the principal investigators for the trial, in a press release announcing the results. “Abbott’s Esprit BTK system offers a new option for treating people with the most severe forms of PAD, helping to heal blood flow and potentially salvage limbs.”
Results after two years of the LIFE-BTK clinical trial showed that 90.3% of patients in the Esprit BTK arm did not require a reintervention at 24 months. The trial also showed sustained efficacy at 24 months.
Furthermore, compared to balloon angioplasty, patients treated with Esprit BTK had significantly greater freedom from chronic limb-threatening ischaemia (CLTI), at 61.5% vs. 32.8%.
Additionally, at one year, the trial’s powered secondary endpoints revealed that Esprit BTK had a higher rate of reducing vessel re-narrowing (35.2% improvement) compared to balloon angioplasty.
Alongside the announcement of these results, Abbott also shared that it has launched the Esprit BTK post-approval study (PAS) to assess the continued safety and effectiveness of Esprit BTK in treating CLTI patients in a real-world setting. The first patient was enrolled by Bernardino L Rocha (SSM Health Heart & Vascular Care, Oklahoma City, USA).
The US Food and Drug Administration (FDA) has approved Akura Medical’s investigational device exemption (IDE) application to initiate the QUADRA-PE study evaluating the Katana thrombectomy system in patients with acute pulmonary embolism (PE).
The co-principal investigators of the pivotal study are Sanjum Sethi (Columbia University Medical Center, New York, USA) and Ann Gage (Tristar Centennial Medical Center, Nashville, USA).
“The IDE approval of QUADRA-PE marks a significant milestone in the company’s journey toward providing physicians with a next-generation solution for treating acute pulmonary embolism,” said Murali Srivathsa, president and CEO, Akura Medical. “We designed the Katana System based on extensive feedback from physicians who shared their need for a thrombectomy system that minimised the difficulty of getting to the clot, removed all types of clots without catheter clogging and provided greater procedural feedback. We look forward to working with our clinical investigators to demonstrate our system’s efficacy.”
The Katana System consists of a bidirectional, low-profile sheath designed to facilitate smoother navigation in complex vasculature and enable contrast injection without requiring catheter exchanges. It also features high velocity saline jets that are engineered to effectively break up clots independent of morphology and prevent catheter clogging for procedural efficiency and sensors that provide real-time pulmonary artery pressure data to provide insights into procedure progress.
QUADRA-PE is a multicentre, international trial designed to enrol up to 118 patients with clinically significant acute PE at up to 26 sites globally. The primary effectiveness endpoint is the reduction in right ventricular/left ventricular (RV/LV) ratio from baseline to 48 hours post-procedure as assessed by computed tomography (CT) angiography. The primary safety endpoint is the composite rate of major adverse events (MAEs) within 48 hours post-procedure.
Royal Philips has announced enrolment of the first patient in the US THOR IDE clinical trial, which will study an innovative combined laser atherectomy and intravascular lithotripsy (IVL) catheter.
Procedures that previously required the use of two different devices can now be performed in a single procedure using a single device, simplifying workflows and procedures and potentially reducing the risk and improving outcomes for patients who might otherwise face multiple complex interventions, Philips says in a press release.
The Cardiovascular Institute of the South in Louisiana recently completed the first case using the new laser catheter. The care team there successfully treated a 78-year-old male with peripheral vascular disease using the Philips device.
“Developing and driving clinical evidence is crucial to improving care and guiding the adoption of new technologies like the Philips laser atherectomy and lithotripsy system,” said Craig Walker and McCall Walker (both Cardiovascular Institute of the South, Louisiana, USA). “This trial will provide essential data to demonstrate how this combined approach can optimise procedural efficiency and patient outcomes in treating challenging calcified lesions.”
The goal of this pivotal study is to evaluate the safety and efficacy of using this unique laser device, integrating laser atherectomy and IVL in a single device to treat complex, calcified lesions in a single procedure for patients with peripheral artery disease (PAD), restoring blood flow to their legs.
The prospective, single-arm, multicentre study will enrol up to 155 patients at up to 30 sites in the USA. Conducted under an investigational device exemption (IDE) from the US Food and Drug Administration (FDA), it will assess the system’s safety and effectiveness in achieving procedural success with a low rate of complications.
The study’s primary endpoints include freedom from major adverse events (MAEs) such as mortality, unplanned amputations, and clinically driven target lesion revascularisation (CD-TLR) within 30 days (about four and a half weeks) of the procedure, as well as achieving less than or equal to 50% residual stenosis post-procedure. Patients will be followed for 12 months.
“This innovative approach to vessel preparation could improve patient outcomes while minimising the need for multiple therapies and interventions. That makes this an exciting innovation milestone as we enroll the first patient in this important US clinical trial,” said Elizabeth Genovese (University of Pennsylvania, Philadelphia, USA), co-principal investigator of the THOR trial at the Penn Advanced Limb Preservation Hospital. “Integrating atherectomy and intravascular lithotripsy into a single device has the potential to revolutionise the treatment of patients with complex femoropopliteal lesions associated with moderate to severe calcifications.”
Stacy Beske, business leader, Philips Image Guided Therapy Devices, added: “A result of Philips’ extensive in-house innovation and development capabilities, our combined laser atherectomy and intravascular lithotripsy device reflects our commitment to providing physicians with the tools they need to tackle complex vascular challenges more efficiently and effectively, potentially transforming treatment paradigms for peripheral artery disease. Philips is dedicated to clinically validating its innovations through rigorous trials and does so in collaboration with strong clinical partners.”
The Philips laser atherectomy and intravascular lithotripsy system is currently investigational and not yet commercially available anywhere in the world, including the USA.
In October, the most popular stories from Interventional News included a subanalysis of the ABRE trial results revealing obesity ‘paradox in post-venous stenting outcomes; renal denervation gains class IIb recommendation in European Society of Cardiology (ESC) guidelines; and a new randomised controlled trial framework is set to improve reporting after endovascular infrainguinal lower-limb interventions for peripheral arterial disease (PAD).
In a new global statement, aimed to set forth the essential elements of interventional radiology (IR) and continuing challenges facing the specialty, the Cardiovascular and Interventional Radiology Society of Europe (CIRSE) and the Society of Interventional Radiology (SIR) query: Have we reached the tipping point?
Following his statement titled ‘Paclitaxel meta-analyses in the lower limbs: Missing the trees for the forest’ published in the June issue of The Journal of Vascular and Interventional Radiology (JVIR), Konstantinos Katsanos (University Hospital Patras, Rio, Greece) imparts his final word on the paclitaxel controversy, surveying the key meta-analyses data that moved the needle.
Results from a subset analysis of the ABRE study have shown that patients in three out of the six World Health Organisation (WHO) body mass index (BMI) groups—‘pre-obesity’, ‘obesity class I’ and ‘obesity class II’—trended towards higher 36-month patency rates compared with the ‘normal weight’ group.
Medinol has announced the successful first-in-human implantation of the ChampioNIR drug-eluting peripheral stent by Gerard S Goh and Thodur Vasudevan of the Alfred Hospital in Melbourne, Australia.
A new deep vein thrombosis (DVT) diagnostic pathway incorporating non-expert artificial intelligence (AI)-guided compression ultrasound could reduce workload and costs for healthcare systems while providing a quicker diagnosis and improving patient care.
EMBLOK has announced that it has enrolled the first 50 patients in a clinical trial to evaluate the performance and treatment effect of its Emblok embolic protection system (EPS).
Argon Medical has announced the launch of the Intara introducer sheath and the TLAB transvenous liver biopsy system. The Intara introducer sheath is intended to maintain access to a patient’s peripheral or central vasculature (excluding coronary and neuro vasculature) to facilitate the introduction of therapeutic or diagnostic devices.
Microbot Medical has today announced that it has successfully completed enrolment and follow-up for all patients in its ACCESS-PVI human clinical trial. The company also announced that it is accelerating its go-to-market strategy.
Pilot testing has shown that a new framework—dubbed Endo-STAR—can be used to describe and standardise endovascular interventions for peripheral arterial disease (PAD) within a randomised controlled trial (RCT) protocol and monitor adherence to the protocol over the course of a trial. Ewa M Zywicka (University of Bristol Medical School, Bristol, UK) shared this conclusion during the Prize Session at the recent European Society for Vascular Surgery (ESVS) annual meeting (24–27 September, Kraków, Poland).
Eric Secemsky is lead investigator for the ELITE-BTK pivotal trial
R3 Vascular today announced that the US Food and Drug Administration (FDA) has granted investigational device exemption (IDE) approval to initiate its ELITE-BTK pivotal trial of the next-generation Magnitude drug-eluting bioresorbable scaffold for below-the-knee (BTK) peripheral arterial disease (PAD).
“We are pleased to have FDA approval for our ELITE-BTK pivotal trial, thus allowing enrolment to begin for our next-generation Magnitude scaffold. This will enable R3 Vascular to follow-up on our positive first-in-human RESOLV1 study data, which demonstrated excellent and promising results with 96% patency by DUS [Duplex ultrasound scanning] at six months,” said Christopher M Owens, president and chief executive officer of R3 Vascular. “Initiation of this trial will begin in Q1 2025 and will be conducted at up to 60 global clinical sites with 264 subjects, and upon favourable conclusion will allow the company to complete and pursue a PMA [premarket approval] application for Magnitude with the FDA.”
R3 Vascular notes that Magnitude is a next-generation bioresorbable scaffold with the potential to address one of the greatest needs for patients suffering from chronic limb-threatening ischaemia (CLTI) due to below-the-knee PAD.
“R3 Vascular’s novel bioresorbable scaffolds are made from a unique, ultra-high molecular weight polylactic acid polymer. This polymer, combined with the company’s scaffold design and proprietary processing technology allow the sirolimus-coated scaffolds to be thinner, stronger, and more flexible even at larger diameters and longer lengths,” a company press release reads. “R3 Vascular scaffolds are specifically engineered to ensure that they gradually and predictably absorb into the tissue, leaving nothing behind and enabling a more naturally functioning vessel.”
Eric Secemsky (Beth Israel Deaconess Medical Center, Boston, USA), lead investigator for the ELITE-BTK pivotal trial, said in the press release: “This is a much-anticipated trial given the advancements and advantages of this next-generation technology, which has the potential to transform the field of peripheral interventions. We look forward to evaluating the impact of Magnitude on patient outcomes and its ability to meet this growing clinical need.”
In May of 2024 R3 Vascular announced the closing of its US$87 million Series B financing round to support the ELITE-BTK IDE pivotal trial as well as additional research and development, global regulatory submissions, scale up of manufacturing processes, and initial commercialisation.
A retrospective economic analysis of the LIFE-BTK trial has demonstrated the one-year cost-effectiveness of an everolimus-eluting resorbable scaffold over angioplasty for the treatment of infrapopliteal artery disease, with investigators predicting more significant results in the longer term.
Sharing this finding at TCT 2024 (27–30 October, Washington, DC, USA), LIFE-BTK co-principal investigator Sahil Parikh (Columbia University Irving Medical Center, New York, USA) highlighted a “significant difference” in terms of one-year cost-effectiveness in favour of the Esprit BTK resorbable scaffold (Abbott Vascular) over angioplasty using a “relatively modest” willingness-to-pay threshold.
These data come one year after the presentation and simultaneous publication of first results from the LIFE-BTK trial, which enrolled 261 patients globally at 50 sites. The headline finding, Parikh summarised, was that 74.5% of the Esprit BTK group achieved a composite endpoint of limb salvage and primary patency versus 43.7% of the angioplasty group.
With these data in hand, the LIFE-BTK leading investigators—namely Parikh, Ramon Varcoe (Prince of Wales Hospital and University of New South Wales, Sydney, Australia) and Brian DeRubertis (New York Presbyterian–Weill Cornell Medical Center, New York, USA)—set out to perform a cost-effectiveness analysis.
The investigators considered the costs of index procedure and follow-up visits (inpatient, outpatient and office), as well as the incremental cost-effectiveness ratio (ICER)—defined as the difference in total costs divided by the difference in primary endpoint failure or clinically driven target lesion revascularisation (CD-TLR).
At TCT 2024, Parikh shared that index costs were not statistically significant between the Esprit BTK and angioplasty groups, and that follow-up costs were similarly well matched. “The total difference in costs was modest,” he said, citing a gap of less than US$2,000 between the two groups.
The presenter continued that, “using the most conservative delta between the two groups in terms of the primary efficacy endpoint at 365 days, not inclusive of the treatment window”, the Esprit BTK scaffold costs an additional US$7,086 per primary efficacy endpoint avoided.
This led Parikh to report that the Esprit BTK scaffold achieves a 64% probability of cost-effectiveness at a US$10,000 willingness-to-pay threshold compared to angioplasty. As a result of this, he averred: “The use of Esprit BTK at one year alone is likely to be cost effective.”
The presenter went on to note that that Esprit BTK scaffold costs an additional US$22,163 per CD-TLR avoided.
Parikh summarised that the Esprit BTK scaffold shows proven benefit in delaying the need for repeat revascularisation in patients with below-the-knee (BTK) disease and that cost-effectiveness is “likely to increase over time if the reduction of TLR remains consistent over time”.
Additionally, the presenter stressed that the Esprit BTK scaffold is the only US Food and Drug Administration-approved option for patients with chronic limb-threatening ischaemia (CLTI) and infrapopliteal artery disease.
Looking ahead, Parikh highlighted the upcoming presentation of two-year LIFE-BTK results, which DeRubertis is set to announce this week at VIVA 2024 (3–6 November, Las Vegas, USA).
TPT payment, which will be effective for up to three years beginning 1 January 2025, aims to support patient access to new and innovative technology.
Symplicity Spyral
Approved by the US Food and Drug Administration (FDA) in November 2023, Medtronic‘s Symplicity Spyral RDN system is a minimally invasive procedure that delivers radiofrequency energy to nerves near the kidneys that can become overactive and contribute to high blood pressure.
“Receiving TPT approval for our RDN catheter is an important milestone for the Symplicity blood pressure procedure, as it will enable greater patient access to a breakthrough treatment by reducing cost barriers for healthcare systems,” said Jason Weidman, senior vice president and president of the coronary and renal denervation business within the cardiovascular portfolio at Medtronic, in a company press release. “Very few technologies achieve this qualification, and the core goals of fostering innovation and increasing access mirror Medtronic’s desire to continue bringing Symplicity to even more patients suffering from uncontrolled high blood pressure. We look forward to continuing to work with CMS to establish coverage and expand patient access.”
Supporting TPT approval is the Medtronic SPYRAL HTN Global clinical programme, which the company claims is the most comprehensive clinical programme studying RDN in the presence and absence of medication, and in patients with both high and lower baseline cardiovascular risk.
Medtronic advises that the Symplicity Spyral RDN system is approved for commercial use in more than 75 countries around the world and is backed by experience in more than 25,000 patients treated globally with the Symplicity blood pressure procedure. The Symplicity Spyral RDN system is limited for investigational use in Japan.
Paradise
A press release from Recor Medical and its parent company, Otsuka Medical Devices, notes that the Paradise uRDN system is a first-of-its-kind ultrasound-based RDN technology designed to lower blood pressure by denervating the sympathetic nerves surrounding the renal arteries, reducing the overactivity that can lead to hypertension.
The release details that, in approving the TPT, CMS created a distinct device category and code (C1736: Catheter Renal Denervation, Ultrasound) for uRDN in recognition of the differentiated technology and procedure with the Paradise uRDN system.
“TPT for ultrasound renal denervation increases access to a proven device-based hypertension treatment option to patients who have been unable to achieve blood pressure control with lifestyle changes and medications alone,” said Lara Barghout, president and chief executive officer of Recor Medical, in the company’s press release. “The granting of TPT highlights the safety and efficacy of this breakthrough device, which together demonstrated that the Paradise uRDN system met the newness and significant clinical improvement criteria. By creating a distinct device category, CMS have also recognised that the Paradise uRDN system is a highly differentiated technology and that there are significant differences in comparison to other technologies available in the marketplace. This is a major step forward in the reimbursement available for the Paradise uRDN system, creating additional financial support for hospitals and physicians to provide this novel and effective therapy to their uncontrolled hypertension patients.”
Recor Medical advises that the FDA approved the Paradise uRDN system for the treatment of hypertension on 7 November 2023.
Medtronic has announced new, long-term data from the SPYRAL HTN-ON MED clinical trial that showed subjects who underwent radiofrequency renal denervation with the Symplicity Spyral renal denervation system had significantly greater reductions in 24-hr ambulatory systolic blood pressure, and office-based systolic blood pressure compared to sham patients at two years.
The data were presented at TCT 2024 (27–30 October, Washington, DC, USA) by David Kandzari (Piedmont Heart Institute, Atlanta, USA), principal investigator in the SPYRAL HTN-ON MED trial.
“These findings are a key step toward informing the medical community of the long-term effectiveness with radiofrequency renal denervation as a treatment for uncontrolled hypertension,” Kandzari was quoted as saying in a press release issued by Medtronic. “Importantly, at two years, we continue to see Symplicity is safe and consistent with clinically meaningful and significant blood pressure reductions. These data further substantiate sustained blood pressure reductions consistently observed in across the SPYRAL and Global Symplicity clinical programmes.”
At two years, the data showed significant group differences in 24-hr ambulatory systolic blood pressure and office-based systolic blood pressure in favour of renal denervation, despite significantly more medications detected in the sham group.
At 24 months ambulatory systolic blood pressure reduced by -12.1 mmHg in RDN group vs. -7mmHg in sham group (treatment difference: -5.7 mmHg; p=0.039), and office-based systolic blood pressure: -17.4 mmHg in the RDN group vs. -9.0 mmHg in the sham group (treatment difference: -8.7 mmHg; p=0.0034). Long-term safety with no confirmed renal artery stenosis greater than 70% in the Spyral group at two years
Medtronic intends to investigate multi-organ (hepatic artery and renal artery) denervation with the Symplicity Spyral catheter. The planned Global Pilot study, SPYRAL GEMINI, will investigate the safety and efficacy of the multi-organ ablation approach in uncontrolled hypertension patients who are both on and off medications.
The utilisation of Symplicity Spyral in the hepatic artery is investigational and not approved for use.
The company is also expanding the GSR-DEFINE clinical trial to sites in the USA. The GSR-DEFINE trial is an extension of the Global SYMPLICITY registry, and is a prospective, all-comer observational study in 251 sites across 55 countries, including 3,000 patients from the GSR study and enrolling up to an additional 2,000 patients globally.
Approved for commercial use in over 75 countries around the world, the Symplicity Spyral renal denervation system is currently limited to investigational use in Japan.
Surmodics has announced that early results of a subset of 60 real-world acute, subacute, and chronic limb ischaemia patients from its PROWL registry study were presented by Dean Ferrera (Powers Health, Munster, USA) atTCT 2024 (27–30 October, Washington, DC, USA).
PROWL is an open-label, retrospective, multicentre US registry of the Surmodics Pouncethrombectomy platform for the non-surgical removal of emboli and thrombi in the peripheral arterial vasculature.
A press release details that the registry is collecting real-world efficacy and safety outcomes data for endovascular interventions using the fully mechanical, non-aspiration-based Pounce platform for up to 500 patients at up to 30 sites.
The core lab-adjudicated study is enrolling all patients treated with the Pounce platform, including those with shortened life expectancy, history of cancer or COVID-19, and those with prior interventions to the target limb.
Ferrera, on behalf of the PROWL investigators including national co-principal investigators Sean Lyden (Cleveland Clinic, Cleveland, USA) and Joseph Campbell (OhioHealth, Columbus, USA) presented results from the infrainguinal PROWL subset.
All patients in the 60-patient subset analysis were treated with the Pounce thrombectomy system, indicated for use in peripheral arteries 3.5–6mm in diameter. The analysis examined patients with symptomatic native, infrainguinal vessels, followed through 30 days.
Surmodics reports that procedural success, defined as restoration of pulsatile flow in the target lesion(s) with or without adjunctive treatment (patient level success), was 90%; nearly all (96.8%) patients experienced final post-procedural TIPI (thrombo-aspiration in peripheral ischaemia) 2–3 blood flow restoration; and technical success, defined as restoration of blood flow to the target lesion(s) with <50% residual obstruction without the need to initiate catheter-directed therapies or to proceed to open surgery or other endovascular thrombectomy devices (lesion-level success), was 80.8%.
Furthermore, the company shares that 49 of the 60 patients (81.7%) received no further thromboemboli removal treatment within 30 days post Pounce system use and that product use was well tolerated, with only one patient (1.7%) experiencing device-related adverse events.
Surmodics notes that previous studies of aspiration thrombectomy for symptomatic limb ischaemia excluded patients with symptom duration greater than 14 days or patients whose thrombi or emboli were not fresh. In the 60-patient PROWL cohort, however, 60% of patients presented with acute (≤14 days) limb ischaemia, 16.7% with subacute (15–28 days) limb ischaemia, and nearly one in four (23.3%) presented with chronic (>28 days) limb ischaemia. Forty patients (66.7%) in the 60-patient cohort avoided an intensive care unit (ICU) admission, while 49 (81.7%) were discharged home.
“Although patients with limb ischaemia often seek care acutely, many patients present after experiencing symptoms for several days or weeks,” said Campbell. “As a result, operators are often challenged to remove clots of mixed morphology and chronicity, which may impact procedural success rates both with thrombolytic and primary aspiration strategies. These early PROWL results suggest that the Pounce thrombectomy system is effective as a standalone solution for removing acute-to-chronic clot in real-world clinical settings without use of adjunctive thrombolytics, aspiration devices, or surgery.”
He added: “In terms of healthcare resource utilisation, the high rate of ICU avoidance and discharge home in this very ill population is encouraging. We’re eagerly awaiting further results from this highly promising registry study.”
Data from the prospective, multicentre, investigator-initiated SIRONA randomised clinical trial demonstrated MagicTouch (Concept Medical) sirolimus-coated balloons to be noninferior compared to paclitaxel-coated balloons with regards to the primary safety and efficacy endpoints in patients with femoropopliteal artery disease. Findings were reported today at TCT 2024 (27–30 October, Washington, DC, USA).
Researchers aimed to determine if sirolimus-coated balloon angioplasty is noninferior to paclitaxel-coated balloon angioplasty. From April 2021 to September 2022, a total of 482 participants with Rutherford category 2–4 femoropopliteal artery disease were enrolled at 25 clinical sites in Germany and Austria. Patients were randomised 1:1 to receive angioplasty with either a sirolimus-coated balloon or a paclitaxel-coated balloon. Patient characteristics were similar between both groups.
The mean lesion length was 84 ± 61 mm. A total of 34% of the lesions were totally occluded and 29% were calcified according to Peripheral Arterial Calcium Scoring System (PACSS) grade four. Bailout stents were implanted in 22.8% of the sirolimus group and 20.3% of the paclitaxel group lesions (2.5% (95% confidence interval [CI]: -4.9% to 9.8%).
The rate of the primary efficacy endpoint of primary patency at 12 months was 73.8% in the sirolimus drug-coated ballon (DCB) group compared with 75.0% in the paclitaxel DCB group (-1.2% (-9.7% to 7.4%, p=0.022, non-inferiority). The rate of the composite primary safety outcome at 12 months of clinically driven target vessel revascularisation (cdTVR), major amputation, or death was 9.4% in the sirolimus DCB versus 7.3% in the paclitaxel DCB (2.1% (95% CI: -3.2% to 7.5%, p=0.003, non-inferiority). Functional outcomes were similar between the two groups.
“This head-to-head comparison of sirolimus-coated balloons with paclitaxel-coated balloons during angioplasty of the femoropopliteal artery shows comparable results between the two study groups,” said Ulf Teichgräber (University Hospital Jena, Jena, Germany). “Understanding the safety and efficacy of these two types of balloons, especially compared to one another, can help provide the best patient care possible.”
Findings from the first international randomised controlled trial (RCT) to compare patient outcomes following treatment with large-bore mechanical thrombectomy (LBMT) versus catheter-directed thrombolysis (CDT) for intermediate-risk pulmonary embolism (PE) found that LBMT is superior with respect to the hierarchically-tested aggregated outcome of all-cause mortality, intracranial haemorrhage, major bleeding, clinical deterioration and/or escalation to bailout therapy, and postprocedural intensive care unit (ICU) admission and length of stay.
Findings were reported today at TCT 2024 (27–30 October, Washington, DC, USA) the annual scientific symposium of the Cardiovascular Research Foundation (CRF). Results were also published simultaneously in Circulation.
Over the last decade, catheter-based interventions for intermediate- and high-risk PE, including catheter-directed thrombolysis (CDT) and large-bore mechanical thrombectomy (LBMT), have been adopted to avoid the bleeding risks of systemic thrombolysis. Observational studies of CDT and LBMT have separately reported positive outcomes but there are no prior RCTs directly comparing these two interventional strategies.
From February 2022 to February 2024, a total of 550 haemodynamically stable adults with acute PE, right ventricular dysfunction and at least one additional clinical risk factor for adverse outcomes who did not have absolute contraindications to thrombolytics were randomised in a 1:1 allocation to LBMT with the FlowTriever device (Inari Medical; n=274) or CDT (n=276). The trial was conducted at 57 sites in the USA, Germany and Switzerland. Follow-up was performed at 24-hours, discharge (or after seven days), and at 30-days.
The primary endpoint was a hierarchal win ratio of five outcomes including all-cause mortality, intracranial haemorrhage, major bleeding per International Society on Thrombosis and Haemostasi (ISTH) definition, clinical deterioration and/or escalation to bailout therapy, and postprocedural ICU admission and length of stay. These five outcomes were assessed at discharge or seven days post procedure, whichever came sooner. The primary endpoint favoured LBMT over CDT with a corresponding win ratio of 5.01 (95% confidence interval [CI]: 3.68–6.97, p<0.001).
Among the individual components of these, the rates of all-cause mortality, intracranial haemorrhage, and major bleeding were similar between groups. Less than half of LBMT patients were admitted to the ICU following the procedure compared with nearly all CDT patients (41.6% vs. 98.6%; p<0.001). Although this occurred infrequently, there was also a lower rate of clinical deterioration and/or escalation to bailout therapy with LBMT (1.8%) compared with CDT (5.4%, p=0.038).
At 24 hours, LBMT patients also showed greater improvement in several symptom scores. In addition, the total hospital stay was shorter with LBMT compared to CDT (4.5±2.8 vs. 5.3±3.9 overnights; p=0.002) and fewer LBMT patients were readmitted to the hospital within 30 days (3.2% vs. 7.9%; p=0.03). All-cause mortality within 30 days was similar between both groups (0.4% vs. 0.8%; p=0.62).
“The PEERLESS results represent the most robust evidence comparing two methods of intervention for pulmonary embolism to date,” said Wissam A Jaber (Emory University Hospital, Atlanta, USA). “LBMT was shown to be superior to CDT driven by significantly lower rates of clinical deterioration or escalation of therapy and ICU admission. LBMT was also associated with faster clinical and haemodynamic improvement at 24 hours, significantly shorter hospital stays, and fewer readmissions through 30 days.”
Cook Medical’s Zilver Vena venous self-expanding stent has shown high rates of patency sustained for three years, according to recently published data in the Journal of Vascular and InterventionalRadiology (JVIR). The patency results extended across all patient subgroups, and patients experienced improvements in clinical scoring as compared to baseline.
“We strive for predictable results and are committed to long-term clinical evidence,” said Alec Cerchiari, a director of product management for Cook Medical’s vascular division. “We also gather insights on how to make our products better and create new medical devices for the future. The results we got from the VIVO study confirmed the safety and effectiveness of our stent in a wide variety of patient types that hadn’t been studied in detail like this before.”
Key three-year study outcomes include:
Sustained patency through three years across all patient groups. The Kaplan-Meier estimates for patency by ultrasound at three years were:
90.3% for the overall patient cohort
100% for the non-thrombotic iliac vein lesion (NIVL) group
84% for the acute deep vein thrombosis (aDVT) group
86.1% for the post-thrombotic (PTS) group
Effectiveness was further demonstrated by sustained clinically-driven reintervention rates across all groups. The Kaplan-Meier estimates for clinically-driven reintervention at three years were:
92.6% for the overall patient cohort
100% for the NIVL group
92.1% for the aDVT group
87.1% for the PTS group
No stent fractures through three years, demonstrating stent durability
Positive clinical outcomes for patients which were sustained through three years, demonstrated by improvements in patient symptoms and venous disease scores compared to baseline, specifically scores for venous clinical severity score (VCSS), venous disability score (VDS), chronic venous insufficiency quality of life questionnaire (CIVIQ-20) and clinical, etiological, anatomic, pathophysiology (CEAP) clinical classification (CEAP C classification).
Jupiter Endovascular has announced that the first US patient has been treated in the SPIRARE II US pivotal study of the Vertex pulmonary embolectomy system featuring the company’s Endoportal control platform technology.
The Vertex system is designed to treat acute pulmonary embolism (PE) in an endovascular procedure offering an “unprecedented level of control and precision”, according to the company.
The first US case was performed at Staten Island University Hospital, Northwell Health (New York, USA) by Mitchell Weinberg and Vincent Gallo.
“The unique manoeuvrability of the large-bore Vertex endoportal device enabled us to easily navigate across multiple bends through the right heart and into the pulmonary arteries. Once in the pulmonary arteries, the technology allowed us to stabilise the endoportal device, creating a secure base for us to safely advance the aspiration catheter deep within the pulmonary vasculature and capture hard-to-reach thrombi. With Endoportal Control, we achieved an excellent procedural result with remarkable speed and ease, especially given that it was our first time using this technology,” said Weinberg.
“Navigating the pulmonary arteries can be challenging and often requires a complex trial-and-error approach involving multiple guidewires and ancillary devices in order to safely reach the target vessels. Using Endoportal Control with the Vertex system, we eliminated many of these extra steps and device exchanges, resulting in a much simpler procedure that allowed us to focus less on gaining vessel access and more on treating the patient. Our team is very excited to study this technology further, and I would like to thank Brandon Dilluvio on our team for his support in facilitating this first US procedure,” said Gallo.
SPIRARE II is a prospective, single-arm, multicentre pivotal trial that will enrol up to 145 patients with acute, intermediate-risk PE treated with the Vertex pulmonary embolectomy system at up to 25 US sites. Trial endpoints will characterise the procedural and clinical benefits of PE treatment with Endoportal Control using the Vertex system, across measures of safety, right heart function, and clinical improvement from the time of the procedure to 30 days post-procedure.
The company’s Endoportal Control platform technology integrated into the Vertex system is designed to bring greater ease and stability to a variety of catheter interventions, with the goal of enabling interventionalists to treat anatomical sites that they cannot safely or easily reach with a conventional endovascular approach. The endoportal device is delivered in a flexible, relaxed state over a guidewire to a target location in the vasculature, pressurized with saline to fix it in a stable position for therapeutic delivery, then relaxed again to navigate to another target location or for removal.
“Navigation challenges during endovascular procedures are often underappreciated and have led to under-adoption of life-saving procedures, such as pulmonary embolectomy. We have purpose-built our Endoportal Control technology to solve these issues and make important endovascular procedures accessible to more clinicians and their patients who can benefit from them,” said Carl J St Bernard, Jupiter Endovascular CEO. “This first case in the USA could not have gone better, and appears to validate the safety and performance we are seeing in our currently-enrolling European SPIRARE I study.”
Vesalio has announced the initiation of a prospective, single-arm, multicentre study supporting the recently launched pVasc thrombectomy system for non-surgically removing peripheral occlusions. This multidisciplinary clinical research initiative aims to collect real-world insights on the pVasc system in treating patients suffering from peripheral arterial disease (PAD) that may lead to acute limb ischaemia (ALI).
A press release notes that current thrombectomy tools encounter multiple challenges, including difficulty accessing smaller arteries, prolonged time to flow restoration, and the risk of distal embolisation. “The pVasc system, featuring next-generation Drop Zone technology and a unique, low-profile design, is specifically engineered to address these limitations,” the company states. “The pVasc study will generate vital real-world evidence to support the optimisation of revascularisation techniques and outcomes for patients with PAD-related conditions such as ALI.
Vesalio also shares that the company will be attending the TCT Conference (27–30 October, Washington DC, USA), VIVA (3–6 November, Las Vegas, USA), and VEITHsymposium (19–23 November, New York, USA) in the coming weeks.
“The recent launch of pVasc in the USA represents a major milestone in our commitment to innovating to improve patient outcomes in vascular occlusion,” said Steve Rybka, chief executive officer of Vesalio. “We expect the post-market collection of real-world data to further validate the capabilities of our technology in addressing the challenges of peripheral vascular disease. We continue to support physicians with both technology and data to achieve the best possible outcomes for their patients.”
Results from a subset analysis of the ABRE study have shown that patients in three out of the six World Health Organisation (WHO) body mass index (BMI) groups—‘pre-obesity’, ‘obesity class I’ and ‘obesity class II’—trended towards higher 36-month patency rates compared with the ‘normal weight’ group.
Erin Murphy (Atrium Health Sanger Heart and Vascular Institute, Charlotte, USA) shared this finding at the 2024 American Vein and Lymphatic Society (AVLS) annual congress (10–13 October, Chicago, USA), noting that further research on the topic is needed.
The ABRE study was designed to evaluate the safety and efficacy of the Abre venous self-expanding stent system (Medtronic) in patients with symptomatic iliofemoral venous outflow obstruction. A total of 200 patients with an average age of 51.5 years, average BMI of 29.5 and 66.5% of whom were female, were enrolled across 24 global study sites and followed for 36 months.
In her presentation at AVLS 2024—which earned the first-place Best in Show award at the meeting—Murphy detailed that the ABRE subanalysis sought to assess the impact of BMI on post-iliac vein stenting outcomes. Historically, she noted, obesity has been viewed as a potential hindrance to venous stenting, with expectations of poorer patient outcomes due to higher comorbidity risks.
For the subanalysis, patients were categorised by the six WHO BMI groups: ‘underweight’ (four patients; 2%), ‘normal weight’ (55 patients; 27%), ‘pre-obesity’ (50 patients; 25%), ‘obesity class I’ (51 patients; 26%), ‘obesity class II’ (22 patients; 11%), and ‘obesity class III’ (18 patients; 9%).
Murphy reported at AVLS 2024 that, with regard to revised venous clinical severity score (rVCSS) outcomes, the ‘pre-obesity’, ‘obesity class I’, ‘obesity class II’, and ‘obesity class III’ groups showed increasingly higher baseline scores compared to ‘underweight’ and ‘normal weight’ patients. After six months, the presenter added, improvement in rVCSS was constant across all BMI groups except for ‘underweight’.
Murphy also shared quality-of-life (QoL) results. The presenter detailed that, as BMI increases, the baseline VEINES-QoL scores worsen and that improvement in VEINES-QoL at six months is constant across all BMI groups except for ‘underweight’. BMI was not found to be a factor in VEINES-QoL change from baseline to six months, she continued.
Regarding primary patency, Murphy relayed that the ‘pre-obesity’, ‘obesity class I’, and ‘obesity class II’ groups “paradoxically” trended towards higher patency rates at month 36 compared to the ‘normal weight’ group. However, the presenter stressed that the 95% confidence intervals overlapped for all three groups and that the subgroups are small.
Finally, Murphy added that the ‘obesity class III’ group (BMI >40) had the lowest 36-month patency—which she said indicates potential higher risk in this group independent of disease cohort—and that there was no significant difference in underlying disease cohort across the BMI categories.
During a satellite symposium session dedicated to real cases and trial outcomes which was held at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14–18 September, Lisbon Portugal), experts presented compelling data from large registries and randomised controlled trials (RCTs) which suggest that the Eluvia drug-eluting stent (DES, Boston Scientific) should be preferred when treating the superficial femoral artery (SFA).
Giovanni Torsello
The Münster registry was led by Giovanni Torsello (St. Franziskus Hospital, Munster, Germany)—his son, Giovanni Federico Torsello (University Medical Center Göttingen, Göttingen, Germany) presented his research in his absence at the CIRSE annual congress.1 Torsello began by stating that the goal of real-world registries is to generate data which can be extrapolated to daily practice, considering all of the variables that are encountered day-to-day. To reflect this, the Münster registry assessed the performance of the Eluvia DES in long and complex femoropopliteal lesions, and assessed consecutive patients treated between 2016–2018 for stent primary patency.
The criteria for using the Eluvia DES, Torsello noted, was to treat recoil post-percutaneous transluminal angioplasty (PTA) or flow-limiting dissection post-PTA, labelling the registry the “bailout Eluvia DES study”. The likelihood of needing a bailout stent increases due to lesion length, chronic total occlusion (CTO) and calcification.
In the Münster all-comer cohort, 130 patients were enrolled totalling 137 lesions with a mean length of 194mm; 21% of included patients had a Rutherford classification of 5–6; 67% were identified as having a PACSS classification of 3 or 4; and 74% of patients had total occlusion of the SFA. Patients with Trans-Atlantic Inter-Society Consensus Document on Management of Peripheral Arterial Disease (TASC) A/B lesions and those with in-stent restenosis were excluded.
Key lessons from the Münster registry
Using a selection of cases which exemplify the Eluvia DES’s efficacy in a range of scenarios, Torsello pulled out key lessons from his experience treating long CTOs and displayed an exemplar case to depict this (Figure 1). He stated that a DES is necessary in these patients, as “if you don’t use a scaffold, you will not have mechanical stability—and if you use a scaffold without eluting an anti-restenotic drug, you will see in-stent restenosis”.
Figure 1: CTO of the SFA, wire cross and ballooning, dissection after dilatation. Eluvia was chosen as bailout stenting to guarantee acute and long-term results.
“What about calcium?” Torsello asked, moving on to show the “more difficult” calcification cases, which pose the added challenge of drug uptake and impaired expansion. He stated that, in these cases, often his team opt for upfront stenting of calcified occlusions paired with PTA to expand the DES. He added that short balloons should be used to exert more force in the segments which are heavily calcified and stenosed and promoted the use of a DES in this setting to benefit from lower rates of restenosis.
Taking what has been learnt and placing it within the context of the Münster registry, Torsello shared that the Eluvia DES showed 71% primary patency at two years, which increased to 78% if the entire lesion is covered by the DES, underlining its successful deployment in long lesions.
As published in the journal CardioVascular and Interventional Radiology (CVIR), the primary patency rate for the Eluvia DES was 65% at five years, with a clinically driven target lesion revascularisation (CD-TLR) and major amputation rate of 79% (Figure 2) and 96%, respectively.
Figure 2
Sustained high patency rates
“What we have seen is that you can successfully treat the SFA and downgrade patients’ disease with the Eluvia DES. What is important is a sustained high patency rate which we have achieved here, with results which are not unlike that of bypass but by endovascular means—it’s amazing to see,” Torsello commented.
Overall, he stated that the Eluvia DES offers a good bailout strategy in cases with a sub-optimal vessel preparation result such as dissection or recoil, or in complex lesions. In light of their long-term registry data, Torsello stated that he looks forward to the RCT data to come in this arena which he believes will bear out their outcomes and bolster Eluvia within the procedural standard.
Insights from SPORTS RCT support DES use in long, complex SFA lesions
Gunnar Tepe
“Truly long lesions have been underrepresented in randomised controlled trials [RCTs], so there were no definitive data on primary treatment strategy or decision making—the SPORTS trial was born out of limitation of current data on TASC C and D lesions for endovascular intervention”, were the opening statements of Gunnar Tepe (Klinikum Rosenheim, Rosenheim, Germany) who also presented during the satellite symposium session, sharing insights from the SPORTS RCT using the Eluvia drug-eluting stent (DES) in complex lesions.2
Initially, Tepe brought attention to the EMINENT and IMPERIAL (Boston Scientific) RCTs which each showed superior primary patency when using the Eluvia DES in the superficial femoral artery (SFA). The EMINENT trial—the largest RCT to compare drug-eluting to self-expanding bare metal stents— randomised 508 patients, and reported that Eluvia demonstrated superiority over bare metal stents, with a statistically significant primary patency of 85.4% versus 76.3% through to one year. The IMPERIAL trial, involving 465 randomised patients, compared the Eluvia DES to Zilver PTX (Cook Medical). At one year, the Eluvia device demonstrated a primary patency rate of 86.8%, compared to 77.5% for Zilver PTX. The longer sustained drug release from the Eluvia system was highlighted as a key differentiator.
SPORTS data updates DES patency
Tepe then situated the SPORTS RCT within the arena of other Eluvia trials, commenting that IMPERIAL and EMINENT were “early” explorations and concerned short lesions which minimised its broader application. Since then, these data have been updated with those gained from later trials, such as IMPERIAL Long and SPORTS, which have demonstrated the pertinency of the Eluvia DES in complex lesions while maintaining high patency rates.
The SPORTS RCT was a prospective, randomised, multicentre trial which compared the angiographic and clinical outcomes of TASC C/D lesions in the SFA after treatment with the Eluvia DES and the SeQuent Please OTW (BBraun) drug-coated balloon (DCB), or a bare nitinol stent. Tepe—the trial’s principal investigator—and colleagues enrolled 224 patients with a mean lesion length of 228mm and a Rutherford classification of 2–4; 69% of patients were identified as having a PACSS classification of 3/4 and 76% had total occlusion of the SFA.
At one year, concerning angiographic stenosis, the data revealed superior results for the Eluvia DES (Figure 3) when compared to the bare nitinol stent. The SeQuent DCB was non-inferior to the bare nitinol stent. Of their secondary endpoints, Tepe noted that late lumen loss at 12 months “differed significantly” between treatment groups, however the least loss was reported in the Eluvia DES group.
Figure 3
Tepe situated the SPORTS RCT among others that have investigated the use of non-drug-eluting stents, showing that patency rates decrease when these are used in longer lesions. “With the Eluvia DES we have a really good patency even in those long, hard-to-treat lesions,” he continued.
“The SPORTS RCT provided new data on primary strategies in TASC C/D lesions and confirmed the Eluvia DES as superior to operator ‘best choice’ bare metal stenting for full lesion coverage,” Tepe stated. He described how the use of a DCB with or without bailout spot stenting as a strategy was non-inferior to full lesion bare metal stenting, however long bare metal stent restenosis remains “problematic”. This, Tepe stated, is due to the price of target lesion revascularisation (TLR) which can cost more than 22,000 euro per procedure.3
He concluded his talk by asserting that further analysis is underway to investigate the “astonishing” number of TLRs and failures in the DCB group, to create core-lab adjudicated “failure modes” for each treatment strategy.
Which gaps should future data fill?
Following Tepe’s talk, session moderator Marianne Brodmann (Medical University of Graz, Graz, Austria) asked the presenters what data is still missing concerning treatment of the SFA and what is needed now to guide daily practice and build a treatment algorithm. Tepe highlighted vessel preparation and the lack of data there, and noted that data to determine which device is superior in this setting would be beneficial, but conduction a study on this would be “very difficult”.
Sabine Steiner (Medical University Leipzig, Leipzig, Germany)—who also presented insights from the BEST SFA trial cases during the session—answered next, agreeing that the heterogeneity of SFA lesions makes conducting clinical trials in this space near impossible. “We need extremely good registry data with core-lab adjudication from angiogram. This is a prerequisite, because we know what investigators are reporting is in part ‘wishful thinking’,” Steiner said. She stated that intravascular ultrasound (IVUS) might assist in this area in the future, to “truly see what has an impact on our outcomes”.
In his response to Brodmann’s question, Torsello emphasised post-interventional medication and the lack of uniformity in its usage. He stated that, although studies such as VOYAGER have provided data on this, its takeaways “don’t apply to every patient”. Additionally, Torsello stated that research concerning the profunda femoris artery would be interesting, which is an area often overlooked in studies concerning the common femoral artery.
In conclusion, the Münster registry and SPORTS RCT presented at CIRSE provide compelling evidence for the sustained efficacy of the Eluvia DES in treating long, complex SFA lesions. The high primary patency rates displayed in these trials underscore the effectiveness of this endovascular approach. The Eluvia DES has demonstrated its value as a reliable bailout strategy in challenging cases, particularly where vessel preparation is suboptimal. Looking ahead, further research, including further RCTs and improved real-world registry data, will be crucial in addressing current challenges, such as restenosis in bare metal stents and high TLR rates in DCB treatments.
References
Muenster: Stavroulakis, Konstantinos & Torsello, Giovanni & Bosiers, Michel & Argyriou, Angeliki& Tsilimparis, Nikolaos & Bisdas, Theodosios. (2021). 2-Year Outcomes of the Eluvia Drug-Eluting Stent for the Treatment of Complex Femoropopliteal Lesions. JACC: Cardiovascular Interventions. 14. 692-701.10.1016/j.jcin.2021.01.026.
Tepe, G. SPORTS Trial: Drug Eluting Stent or Primary Bare Nitinol Stent Application versus Drug Coated Balloons in Long SFA Lesions. Presented at TCT 24 Oct 2023.
Saratziset al. COST Analysis of Target Lesion Revascularisation in Patients With Femoropopliteal In-Stent Restenosis or Occlusion: The COSTLY-TLR Study. EurJ Vasc EndovascSurg. 2024 Feb 6:S1078-5884(24)00160-6. doi: 10.1016/j.ejvs.2024.02.001. Epub ahead of print. PMID: 38331163.
In a new global statement, aimed to set forth the essential elements of interventional radiology (IR) and continuing challenges facing the specialty, the Cardiovascular and Interventional Radiology Society of Europe (CIRSE) and the Society of Interventional Radiology (SIR) query: Have we reached the tipping point?
SIR and CIRSE first published a joint statement which sought to define IR in 2010, following the Royal College of Physicians and Surgeons of Canada’s denial of the Canadian Interventional Radiology Association’s request for official recognition. The motivation for the 2024 document was both to reflect on how far IR has come as a discipline and where it needs to go next. This updated statement, which was this week co-published in the journal CardioVascular and Interventional Radiology (CVIR) and Journal of Interventional Radiology (JVIR), was first presented during the Global IR Summit at the CIRSE Annual Congress (14–18 September, Lisbon, Portugal), and sparked talks over the desynchronised development of international IR.
The central tenet of the updated document is the uptake of clinical practice and longitudinal care in IR over the 15-year interim, as presented in the session by Parag Patel (Froedtert Hospital, Milwaukee, USA) and Robert Morgan (St George’s NHS Trust, London, UK). They outlined the areas that necessitated an update, which alongside increased clinical practice, include the recognition of longitudinal care of patients provided by IR in some countries, the need to promote subspeciality or specialty recognition, and the developments in certification over the last decade, particularly via the European Board of Interventional Radiology (EBIR). The increased commitment to diversity amongst interventional radiologists and overarching workforce developments, such as their increased presence on interdisciplinary boards, and the importance of IR-led clinical studies, were also covered.
The project for this updated global statement was launched during CIRSE 2022 and spearheaded by lead authors Morgan, Patel, Alda Tam (MD Anderson Cancer Center, Houston, USA), and Christoph Binkert (Medizinisch Radiologisches Institut, Zürich, Switzerland). At the time of print, the document has been circulated and endorsed by 47 national IR societies.
Morgan indicated that the statement is essentially a call to action to promote IR, especially in countries where interventional radiologists have limited resources to endorse their services. “Our global IR societies must collaborate closely to advance common strategic goals and must continue to promote the field of IR and the treatments we provide as first options for patients whenever appropriate.” Informing their understanding of geographical disparities across international IR training and practice, Morgan referenced a global survey of IR status carried out by the international division of the SIR, presented earlier in the session by Constantinos T Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA).
Expanding on why the survey was carried out, Sofocleous said that “the world is not equal, and IR services throughout are extremely different with many disparities”. The anonymous survey was distributed to members of global IR societies and investigated demographics, local/regional practice characteristics, and professional challenges and practice needs.
“Of our responders, 92% agreed that there is a great need to establish unified global IR training standard”, Sofocleous said. He described the shortage in dedicated IR training programmes in “most” regions worldwide, as well as a “pronounced” shortage in IR exposure in Africa, Asia and South America. He also highlighted the lack of IR teaching responsibilities in Africa, however, he noted that, “interestingly”, they were more prevalent in Europe when compared to the USA. Regarding IR practice, the investigators found that public awareness of IR services was a universal issue, showing “no difference” between Africa and the USA—the geographies at either end of the spectrum concerning IR infrastructure.
As Sofocleous stated during the session: “Public awareness is our greatest universal need, and this should drive our future investments. Establishing training programmes, providing access to online education and organising local IR conferences in Asia, South America and Africa are all key takeaways [from the survey].”
With the information gained through this endeavour, the subsequent Global IR Statement concludes that a ‘tipping point’ may in fact be reached in the next two decades, initiating the formal designation of IR as a distinct sub- or primary specialty worldwide. However, this goal can only be achieved through “close collaboration” between societies to promote IR as the first option for patients when appropriate.
Other lectures during the Global IR Summit delved deeper into the ideas at the core of the Global IR Statement. Binkert expanded on the idea of clinical service as the driving force behind the advancement of IR. “I think this is the most critical part,” he stated, “If we master clinical service, all of the other parts will naturally fall into place.”
Session co-moderator Alda Tam spoke about the paths taken in the USA in establishing IR as one of 39 distinct specialities: “In short, how we convinced the American Board of Medical Specialties [ABMS] was our argument that better trained interventional radiologists lead to better patient care.”
The talk then turned to monitoring and measuring the progress of IR in future, and how development can be captured worldwide. Sofocleous stated that attention should be paid to marketing IR, shifting focus from imaging-oriented to disease-oriented messaging—“to show what our field has to offer each disease type”. However, “we don’t have enough boots on the ground”, he added, explaining that, if this were not the case, the installation of an interventional radiologist among every panel that dictates disease-specific guidelines would be an ideal metric to mark IR’s international growth in the coming years.
Patel inserted that: “As a specialty that has organised ourselves, we need to take responsibility for the promotion of IR services. We must be more vocal as a field, enrol in more clinical trials, and be at the table when multidisciplinary guidelines are being brought about.”
Closing the session, Morgan stated that raising the profile of IR worldwide is a question that has “taxed people better than us for many, many years”. He stated that through continual idea-sharing in forums such as the Global IR Summit, headway can be made, and a feasible method of monitoring IR’s development can be established.
Pilot testing has shown that a new framework—dubbed Endo-STAR—can be used to describe and standardise endovascular interventions for peripheral arterial disease (PAD) within a randomised controlled trial (RCT) protocol and monitor adherence to the protocol over the course of a trial. Ewa M Zywicka (University of Bristol Medical School, Bristol, UK) shared this conclusion during the Prize Session at the recent European Society for Vascular Surgery (ESVS) annual meeting (24–27 September, Kraków, Poland).
Zywicka began by noting that rigorous evaluation of novel lower-limb endovascular interventions is “critically important” to ensure adoption of effective technologies and rejection of those that are ineffective or harmful.
The presenter continued that poor reporting of RCTs limits the evaluation of technologies for lower-limb endovascular interventions, highlighting a recent study in which more than half of RCTs did not adequately describe interventions, and almost 80% did not report any form of standardisation.
The aim of Zywicka and colleagues’ present study, therefore, was to develop a specific framework for describing and standardising endovascular lower-limb interventions within clinical trials.
Zywicka explained to the ESVS audience that the Endo-STAR framework was developed using qualitative research methodology and the Enhancing the Quality and Transparency of Health Research (EQUATOR) methodological framework. The presenter added that trial reports and associated protocols identified in a recent systematic review of endovascular infrainguinal lower-limb RCTs for PAD provided the data for developing the preliminary framework.
Going into more detail about the research methods used, Zywicka detailed that a framework approach to thematic analysis of qualitative data was employed to code and categorise text into steps and components of endovascular infrainguinal interventions.
Subsequently, focus groups were conducted with key international stakeholders such as clinical practitioners—namely vascular surgeons, interventional radiologists, angiologists and cardiologists—trialists, industry representatives and journal editors to refine the framework and consider clarity and feasibility issues. Zywicka noted that the framework was updated based on this feedback, and a consensus between stakeholders was reached via a modified Delphi-style questionnaire.
Finally, Zywicka shared, the framework was refined through cognitive interviews with trialists to test the real-world feasibility of using the Endo-STAR framework in contemporary endovascular RCTs. An online version of the Endo-STAR framework was developed to facilitate implementation and dissemination.
At ESVS, Zywicka informed attendees that the preliminary framework was developed after including data from 112 RCTs evaluating endovascular infrainguinal interventions for PAD.
Zywicka relayed that 24 key stakeholders participated in three focus groups, contributing to the refinement of the framework, and all 24 participants took part in the consensus questionnaire. After the first round of the questionnaire, the presenter continued, an agreement above 85% was reached for each framework section. Ten trialists involved in contemporary endovascular trials took part in pilottesting the framework.
Ultimately, Zywicka reported, the Endo-STAR framework was structured into six main sections: 1) expertise of the professional delivering the intervention, 2) setting/location of the intervention, 3) anaesthesia provided for the intervention, 4) imaging used at the time of the intervention, 5) intervention components: access, crossing the lesion, treating the lesion (including specific steps and details related to all currently available endovascular devices) and closure of the artery, and 6) pharmacological interventions.
In discussion time following Zywicka’s talk, jury member Jon Boyle (Cambridge University Hospitals NHS Foundation Trust, Cambridge, UK) asked how the framework might help in terms of monitoring long-term outcomes of endovascular interventions, to which the presenter responded: “What we are aiming to achieve with this framework is to know what has been done in a trial […] we expect that actually being able to know and clearly describe what was done in a trial can be used to easily compare trials and even potentially compare results in the long term as well.”
Amplitude Vascular Systems (AVS) recently announced that it has enrolled the first patient in its US pivotal trial for pulsatile intravascular lithotripsy (IVL) therapy.
A press release notes that the POWER PAD II clinical study will evaluate the safety and efficacy of AVS’s Pulse IVL system for the treatment of patients with moderate to severely calcified peripheral arterial disease (PAD). Nicolas W Shammas conducted the first case at UnityPoint Trinity Medical Center in Bettendorf, USA.
AVS received an investigational device exemption (IDE) from the US Food and Drug Administration (FDA) in June 2024 to begin POWER PAD II. The trial will enrol up to 120 patients who will be followed for up to six months at up to 20 US facilities.
“AVS is one of the first companies to conduct a peripheral intravascular lithotripsy pivotal IDE trial in the USA, and this patient is the first of many US patients who will benefit from our innovative technology,” said Elizabeth Galle, vice president of clinical affairs at AVS. “This marks our most significant clinical milestone to date as we approach FDA clearance and market availability for the Pulse IVL system. We are confident in our innovative technology, which is designed for easy delivery across complex calcified lesions and can reduce overall procedural costs.”
“UnityPoint Trinity Medical Center is proud to enrol the first patient in the POWER PAD II study and we are grateful for the opportunity to be the first hospital to treat a US patient with this innovative approach to intravascular lithotripsy. We found the device to be very deliverable and incredibly efficient at effectively modifying calcium and ultimately restoring blood flow to our patients’ vascular system,” said Shammas, who is also president and director of the Midwest Cardiovascular Research Foundation.
“By introducing a new, innovative treatment for calcified arterial disease, we can make a dramatic impact on patient lives and improve outcomes,” said Chris Metzger, national principal investigator of the POWER PAD II study. “The results of this US pivotal trial will pave the way for a new treatment option in an evolving and exciting area of medicine: IVL therapy.”
Microbot Medical has today announced that it has successfully completed enrolment and follow-up for all patients in its ACCESS-PVI human clinical trial.
The company also announced that it is accelerating its go-to-market strategy. It expects to begin building out the commercial infrastructure, including the hiring of a seasoned healthcare executive to lead its sales efforts, upon the US Food and Drug Administration (FDA) clearance, which is expected during the second quarter of 2025.
“We are very pleased with the performance of LIBERTY throughout the study,” commented Juan Diaz-Cartelle, chief medical officer at Microbot Medical. “We want to thank all our investigators for their enthusiastic commitment to the trial. We expect to share the results of the clinical trial with the medical community and the public at a conference in early 2025.”
“This is a monumental moment and a significant achievement for Microbot Medical,” commented Harel Gadot, chairman, chief executive officer and president. “The conclusion of the trial and physician feedback is an encouraging development, and our immediate task is to prepare and finalise the FDA 510(k) submission package so we can file it by the end of the year. Concurrently, we will deploy our go-to-market strategy and begin to build out a commercial infrastructure to ensure we are fully prepared to launch LIBERTY upon the FDA’s clearance, which we expect during 2Q 2025.”
ACCESS-PVI is a prospective, multicentre, single-arm, trial to evaluate the performance and safety of LIBERTY in human subjects undergoing peripheral vascular interventions. The trial will support the 510(k) submission to the FDA and subsequent commercialisation. The company wants to thank the patients, physicians and clinical sites for their participation in the trial.
Contego Medical today announced the US Food and Drug Administration’s (FDA) premarket approval (PMA) of the Neuroguard IEP system for carotid revascularisation.
The company shares in a press release that clinical studies of the Neuroguard IEP system, including the PERFORMANCE I trial and PERFORMANCE II investigational device exemption (IDE) trial, have consistently recorded unprecedented low event rates—zero major strokes, zero neurologic deaths, and zero stent thrombosis at 30 days and one year.
William Gray, system chief of the Division of Cardiovascular Diseases at Main Line Health (Wynnewood, USA) and co-national principal investigator of the PERFORMANCE II trial, said in the press release: “FDA approval confirms the results of the clinical studies. The innovative Neuroguard IEP system performs exceptionally well with the lowest one-year stroke rates ever shown for any type of carotid revascularisation, thereby establishing a new standard of care for meaningfully reducing the risk of procedural and long-term stroke among patients with carotid artery disease.”
The Neuroguard IEP system utilises Contego Medical’s Integrated Embolic Protection (IEP) technology, featuring a 40-micron filter integrated on a 6 French delivery catheter. The size of the integrated filter can be adjusted by the operator to custom fit each patient’s unique anatomy, and the pores on the filter are three to four times smaller than those on traditional filters, the company claims, improving protection against stroke and cognitive impairment. According to Conteo Medical, the newest generation closed cell stent is highly conformable and shows remarkable short- and long-term durability, with no thromboses, no clinically driven target lesion revascularisation, and very low restenosis rates at one year.
“This FDA approval is a huge step forward for Contego and for patient care. The Neuroguard IEP system transforms how we approach patients with carotid artery disease by addressing the specific threats of microembolisation while simultaneously reducing procedural steps, ensuring patients receive the highest level of protection throughout the procedure,” said Ravish Sachar, Contego Medical’s chief executive officer and founder. “The ongoing PERFORMANCE III trial is evaluating the Neuroguard IEP system with a next-generation direct transcarotid access and protection system, TCAR-IEP, to demonstrate advanced stroke protection regardless of vascular approach.”
In 2023, the Centers for Medicare and Medicaid Services (CMS) issued a national coverage decision significantly expanding coverage for percutaneous transluminal angioplasty (PTA) of the carotid artery concurrent with stenting performed with FDA-approved carotid stents and embolic protection devices. Contego Medical states that this decision and FDA approval of the Neuroguard IEP system positions the company for ongoing growth.
Penumbra has announced the completion of enrolment in its THUNDER investigational device exemption (IDE) clinical study for patients with acute ischaemic stroke.
THUNDER is evaluating the safety and efficacy of the company’s latest computer-assisted vacuum thrombectomy (CAVT) technology—the Penumbra system with Thunderbolt aspiration tubing—for the removal of blood clots in the brain. This multicentre, single-arm study is evaluating patients with acute ischaemic stroke secondary to intracranial large vessel occlusion (LVO) who are eligible for mechanical thrombectomy, and its primary efficacy endpoint includes revascularisation of the occluded target vessel immediately post-procedure.
“This critical milestone brings us another step closer to providing physicians with the latest technology for stroke management,” said Adam Elsesser, president and chief executive officer of Penumbra. “The THUNDER study will provide the dataset needed to evaluate Penumbra’s Thunderbolt technology and I am optimistic that we are at the dawn of a new era in stroke treatment.”
As stated in a press release, the Penumbra system with Thunderbolt aspiration tubing uses an advanced CAVT software algorithm to generate proprietary, modulated aspiration, reducing friction between the clot and reperfusion catheter, and facilitating a more rapid and complete removal of blood clots in the brain. Thunderbolt aspiration tubing has been designed for use with the Penumbra Engine and Red reperfusion catheters, the release adds.
Following his statement titled ‘Paclitaxel meta-analyses in the lower limbs: Missing the trees for the forest’ published in the June issue of The Journal of Vascular and Interventional Radiology (JVIR), Konstantinos Katsanos (University Hospital Patras, Rio, Greece) imparts his final word on the paclitaxel controversy, surveying the key meta-analyses data that moved the needle.
More than five years ago we documented an increased long-term risk of all-cause death with the use of paclitaxel-coated devices in the femoropopliteal artery that sparked an intense scientific debate and flurry of research articles pursing to elucidate the actual risk of death associated with such devices in the peripheral arteries.1 Of note, our findings were soon corroborated by an individual patient data (IPD) meta-analysis of US Food and Drug Administration (FDA)- regulated paclitaxel devices.2 However, several follow-up observational studies have failed to replicate the survival detriment in real-world cohorts and the latest version of a similar IPD meta-analysis with more complete follow-up has found no significant mortality risk.3 Consequently, several regulatory agencies have recently exonerated paclitaxel from the death stigma in the lower limbs.
Certainly, this remains one of the most puzzling scientific questions and one needs to carefully review the design and quality of enrolled studies, the dosage and pharmacokinetics of the devices tested, the patient case mix differences, and of course the rigour of the statistics methods employed in the analyses. For starters, cause-and-effect questions (i.e. does paclitaxel in the legs increase risk of patient death?) are best answered by appropriately designed randomised controlled trials (RCTs) alone that by design suffer from reduced confounding and other bias compared to observational studies. To build on this, a recently updated study-level summary of 27 studies with 5,502 patients produced a significant risk ratio of 1.28 (95% confidence interval [CI], 1.04–1.58; random effects model) at two years, contrary to the reassuring patient-level results of Parikh et al from 10 RCTs with 2,666 patients at 4.9 years (Hazard ratio [HR]: 1.14, 95% CI (0.93–1.40), frailty Cox model).3,4
From a critical perspective, the latter meta-analysis of industry-sponsored analyses are missing a significant number of studies from our original 2018 meta-analysis with selective inclusion of mostly low-dose trials.3 Figure shows a ChatGPT-powered visualisation of a stacked horizontal bar chart of sample size contrasting Parikh et al’s latest paper with the totality of RCT evidence presented in the Katsanos et al study. The chart illustrates proportionally the sample size of devices with different design/dosage that are distinguished by colour, including ZILVER-PTX stent, 2.0μg/mm² DCB, 3.0μg/mm² DCB, 3.5μg/mm² IN.PACT, and other (e.g. SWEDEPAD study). Apparently, the latest IPD analysis suffers from selection bias being dominated by the low-dose devices and missing a significant amount of evidence from the rest of the devices. Therefore, the original paclitaxel mortality signal has been obviously diluted, but most likely not invalidated.4
So, how can we consolidate our understanding so far of the relationship between paclitaxel in the lower limbs and potential risk of death, and what should be the next steps? Certainly, the subgroup of low-dose paclitaxel-coated balloons has appeared to be safe since our original meta-analysis, but the IPD data silo built by the industry (with the exception of Cook Medical) along with the complexity of paclitaxel chemistry, pharmacology and tissue bioavailability still precludes any definitive conclusions. In addition, upon observation of diverse treatment effects between trials and time periods, one also needs to consider patient case mix differences and changes in medical science and practice over time. Therefore, an informed patient and doctor’s decision remains the wisest choice as advocated by our teachers a long time ago.
References:
Katsanos K, Spiliopoulos S, Kitrou P, et al. Risk of Death Following Application of Paclitaxel-Coated Balloons and Stents in the Femoropopliteal Artery of the Leg: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Am Heart Assoc 2018; 7:e011245.
Rocha-Singh KJ, Duval S, Jaff MR, et al. Mortality and Paclitaxel-Coated Devices: An Individual Patient Data Meta-Analysis. Circulation 2020; 141:1859-1869.
Parikh SA, Schneider PA, Mullin CM, et al. Mortality in randomised controlled trials using paclitaxel-coated devices for femoropopliteal interventional procedures: an updated patient-level meta-analysis. The Lancet 2023; 402:1848-1856.
Katsanos K. Journal of Vascular & Interv Radiol Published:June 04, In press, 2024 DOI:https://doi. org/10.1016/j.jvir.2024.05.018.
Konstantinos Katsanos is a consultant vascular and interventional radiologist, specialising in endovascular, spine and oncology at the University Hosptial Patras, Rion, Greece.
EMBLOK has announced that it has enrolled the first 50 patients in a clinical trial to evaluate the performance and treatment effect of its Emblok embolic protection system (EPS).
Explosive growth in transcatheter aortic valve replacement (TAVR) volumes has been reported globally, with some growth rates >50-fold according to a report from the American Heart Association (AHA). The TAVR market is estimated to increase at a compound Annual Growth Rate (CAGR) of 14.1% over the next decade in the USA alone.
The company’s press release states that TAVR offers a less invasive option for aortic valve replacement in the heart. During the replacement of the aortic valve, small pieces of calcium or tissue can sometimes break off from the old valve. This debris, referred to as emboli, can travel through blood vessels to the brain, placing a patient at risk for stroke. An embolic protection device captures emboli and mitigates the risk of emboli breaking free, protecting other vital organs during TAVR procedures. EMBLOK’s EPS device aims to offer whole-body protection from debris captured during TAVR, reduce procedural complexity and improve patient safety.
“The enrolment of the 50th patient in our study for our novel whole-body embolic protection system is a major milestone for the advancement of safety in TAVR procedures,” said Brad Brown, chief executive officer of EMBLOK. “Our mission is to provide a breakthrough solution that enhances patient safety during this increasingly prevalent procedure. The early results have been very encouraging, and we’re optimistic about the potential of this technology to set a new standard in embolic protection.”
The multicentre, single-blind, randomised controlled trial, Evaluation of safety and effectiveness of the EMBLOK EPS during TAVR, will enrol up to 532 subjects between 18–90 years of age with aortic valve stenosis who are undergoing TAVR. The company is initiating additional clinical sites and plans to finish enrolment by Q3 2025. Hemal Gada (UPMC Heart and Vascular Institute in Central, Pennsylvania, USA) and William Merhi (Corewell Health, Michigan, USA) will be co-principal investigators of the trial.
“Embolic protection is crucial during TAVR procedures to safeguard patients from the risk of stroke and other serious complications caused by debris dislodged during the procedure,” said Gada. “By ensuring comprehensive protection, we can significantly improve outcomes and enhance both the short and long-term quality of life for those undergoing this life-saving treatment.”
Cardiovascular pathologist, Renu Virmani (CVPath Institute, Gaithersburg, USA) commented: “As the field of transcatheter aortic valve replacement continues to evolve, the importance of whole-body embolic protection has never been more critical. While current systems target cerebral protection, capturing and removing debris from the entire circulatory system offers a more comprehensive safeguard. Whole-body embolic protection represents the next frontier in ensuring patient safety by minimising the risk of complications that can arise from debris dislodgement during TAVR procedures.”
“We’re thrilled to announce the formation of our advisory board, bringing together renowned experts who will help guide us as we continue advancing this important work and bring it to market,” continued Brown. “We see significant opportunities to, most importantly, support physicians performing TAVR procedures in their effort to optimise patient care, as well as play an integral role in the burgeoning TAVR market. These esteemed healthcare professionals will be instrumental to achieving our goals.”
InspireMD has announced that the US Food and Drug Administration (FDA) approval of the company’s investigational device exemption (IDE) application to initiate the CGUARDIANS II pivotal study of its CGuard Prime 80cm carotid stent system during transcarotid artery revascularisation (TCAR) procedures.
In February 2024, InspireMD announced that professor of surgery and radiology Patrick Geraghty (Washington University School of Medicine, St. Louis, USA) and programme director and chief of vascular surgery Patrick Muck (Good Samaritan Hospital, Cincinnat, USA) have agreed to act as lead investigators for the trial.
Marvin Slosman, chief executive officer of InspireMD, stated: “The approval of our CGUARDIANS II IDE is an important milestone and a significant step forward in our mission to serve the broadest range of physician and patient needs with a comprehensive set of tools that can deliver our best-in-class carotid stent system, CGuard Prime, for both carotid artery stenting and TCAR procedures. The CGUARDIANS II study is intended to facilitate approval of the use of CGuard Prime in an optimised TCAR version and indication.”
“In parallel, we continue to advance development of our comprehensive next generation TCAR Neuroprotection System, SwitchGuard NPS. Each of these initiatives helps pave the way, once approved, for us to initiate commercial sales and strive for market leadership in the USA. Our mission to improve stroke prevention and carotid disease management with our CGuard platforms continues as we build our company toward US expansion and global success. Additionally, as we previously announced, we are thrilled to have Geraghty and Muck as co-principal investigators for the study, as well as a world class group of investigators committed to the trial’s success,” Slosman concluded.
Medinol has announced the successful first-in-human implantation of the ChampioNIR drug-eluting peripheral stent by Gerard S Goh and Thodur Vasudevan of the Alfred Hospital in Melbourne, Australia.
The ChampioNIR drug-eluting peripheral stent poses a transformational technology designed to improve patient outcomes and procedural success. In a first-of-its-kind hybrid mechanical design, radial support is provided by the metallic component of the stent, whereas longitudinal structure is provided by a bioresorbable polymeric mesh providing unsurpassed flexibility and long-term durability in even the most challenging anatomies. Furthermore, a unique drug-elution paradigm releases drug from the entire cylindrical area of the stent, drastically reducing diffusion distances and allowing, for the first time, therapeutic dosing of a large peripheral vessel with a ‘limus’ drug for an extended period of time.
“We were impressed with ChampioNIR’s deliverability and its straightforward deployment”, said Goh, head of interventional radiology at The Alfred Hospital. “The frictionless deployment mechanism made the precise positioning of the stent very straightforward.”
Yoram Richter, chief executive officer of Medinol, added: “Medinol is excited to bring to clinical practice the culmination of years of research and development into novel stent designs, tailor-made for unmet clinical challenges in vascular interventions,”
The CHAMPIONSHIP study will enrol a total of 30 patients across seven sites in Australia and the USA. Sahil Parikh (Columbia University Irving Medical Center, New York, USA) principal investigator of the CHAMPIONSHIP study commented: “The ChampioNIR stent represents a breakthrough in treatment for superficial femoral artery (SFA) lesions. I am excited to see this device come to life after years of development.”
A new deep vein thrombosis (DVT) diagnostic pathway incorporating non-expert artificial intelligence (AI)-guided compression ultrasound could reduce workload and costs for healthcare systems while providing a quicker diagnosis and improving patient care.
“The diagnosis of DVT in a tertiary setting is part of a complicated clinical pathway including clinical probability scoring, D-dimer testing and a full duplex scan, often leading to long waiting times,” Avgerinos—who is co-director of the Clinic of Vascular and Endovascular Surgery at Athens Medical Group and visiting professor of vascular surgery at the University of Athens in Greece—told Venous News ahead of the ESVS meeting. He added that the need to have trained radiologists or sonographers available 24/7 incurs high costs and represents a “suboptimal use of resources”.
The ThinkSono system, Avgerinos explained, is based on the point-of-care ultrasound concept and eliminates the need for an expert operator and the absolute need to perform a standard duplex. “It is an AI-based software that you can install on your cell phone or tablet and will guide a non-expert on how to perform a compression ultrasound using a wireless probe,” he continued.
In their pilot study of the ThinkSono system, Avgerinos and colleagues set out to evaluate its clinical utilisation in real-world practice—having previously demonstrated its ability to generate valid images—hoping to show that the system could spare the need for standard venous duplex.
The researchers prospectively enrolled 53 patients who were suspected to have a DVT. These patients underwent a ThinkSono scan, performed by a nurse or resident in the emergency room, with the resulting images then reviewed remotely by the on-call radiologist. D-dimer testing was also performed as a safety measure.
Avgerinos shared that all 53 scans generated were of appropriate quality to be read by the radiologist. “This is a great milestone for an AI technology in the hands of non-experts,” he told Venous News, going on to reveal that 89% of the scans were negative for DVT. The team managed to discharge one-third of the patients without performing any standard duplex scan, which Avgerinos commented represents significant cost and time savings.
Six out of eight suspected DVTs were confirmed on standard duplex to be real, with the ThinkSono technology not missing a diagnosis. “Interestingly enough,” Avgerinos added, “all positive D-dimer testing patients who had a negative ThinkSono scan were also eventually negative, indicating D-dimer has a very low specificity and is not really a powerful testing method to rule in DVT.”
ThinkSono software
Avgerinos continued that it took on average six and a half minutes in total for scan and review. The median length of time between scan and review was 30 minutes, although there was a wide variation in this figure. According to Avgerinos, this “reflects unoptimized hospital logistics—mainly the availability of the qualified clinician to review the data”. He clarified that the expert clinicians who took part in the pilot study were volunteers who had various other clinical lab duties, going on to suggest that careful resource planning or the use of dedicated reviewers could help to maximize the efficiency of the AI-assisted pathway.
Avgerinos summarized: “Our study demonstrated that in DVT diagnostic workflow, using AI and remote expert review could safely decrease the need for a full duplex ultrasound and even D-dimer testing for a significant proportion of the patients who are suspected to have a DVT in the emergency room.”
Looking ahead, he noted that a large trial is needed to validate the results of this pilot study, and that clinical commercialization will soon launch in the UK and Germany, while a Food and Drug Administration (FDA) trial is underway in the U.S.
Finally, Avgerinos considered the wider application of this technology. While the pilot study focused on tertiary centers, he hinted at its potential future use in community hospitals and ambulatory centers. “Not a lot of hospitals have radiologists who can perform standard duplex scans 24/7,” he said. “With this technology, patients would not need to travel to the reference centers. A nurse at the community hospital, a nurse at the GP’s office or at the ambulatory centre could perform the scan and an expert could review it remotely from the main hospital. The application eventually expands to any remote or rural underserved area, essentially democratizing ultrasound—anybody can do it, anywhere.”
Arrayus Technologies has announced the Health Canada approval for its magnetic resonance imaging (MRI)-guided focused ultrasound therapy system for uterine fibroid tissue ablation.
The approval follows the successful completion of a first-in-human clinical trial, offering healthcare providers in Canada a non-invasive treatment alternative for the gynaecological issue.
It uses high-precision acoustic energy to target and treat tissue deep within the body without incisions or the need for general anaesthesia.
The system is said to be equipped with the world’s first clinically available fully phased array. It also features treatment planning tools and real-time therapy monitoring. This allows clinicians to customise treatments to individual patient needs, ensuring accuracy and the safety of surrounding healthy tissue.
Arrayus chief executive officer James O’Reilly said: “I am incredibly proud of our team for achieving this monumental first milestone. Securing Health Canada approval marks a pivotal moment in the evolution of our technology but it’s only the beginning. Our platform has the potential to transform patient care across multiple medical specialities. We are committed to pushing the boundaries of medical innovation to reduce the burden on the healthcare system and improve patient outcomes worldwide.”
Arrayus is actively pursuing the expansion of its focused ultrasound platform, a recent press release states. Clinical trials are currently in progress to assess the system in various oncological treatments.
The company is collaborating with healthcare professionals, researchers, and industry partners to investigate potential applications in neurology and women’s health, among other areas.
The treatment—in which energy is targeted through a catheter to the renal nerves to modulate the sympathetic signalling between the kidneys and brain to reduce blood pressure—has been included with a class IIb level of recommendation for treating resistant hypertension in patients with uncontrolled blood pressure, despite the use of three or more blood pressure-lowering drugs.
Additionally, clinicians can consider the interventional treatment in patients with increased cardiovascular risk who have uncontrolled hypertension on fewer than three drugs.
In both instances the guidelines stipulate that the treatment is contingent on patients expressing a preference for renal denervation after a shared risk-benefit discussion and multidisciplinary assessment, and that the procedure is performed at a medium-to-high volume centre. Furthermore, the therapy is not recommended for patients with highly impaired renal function (eGFR <40mL/min/1.73m2) or secondary causes of hypertension.
During a question and answer session following the presentation of the new guidelines at the 2024 ESC congress (30 August–2 September, London, UK), co-chair of the writing committee that drafted the document, John William McEvoy (University of Galway School of Medicine, Galway, Ireland), explained why there is greater emphasis on additional pharmacological interventions—such as the diuretic medication spironolactone or beta blockers—ahead of the device-based treatment in the algorithm for treating resistant hypertension.
“We followed a policy that to meet a class I recommendation or a higher level, we would like to see evidence from trials not just showing a blood pressure-lowering effect but also an impact on outcomes,” McEvoy said. “When it comes to spironolactone and beta blockers, we felt there was sufficient evidence—it wasn’t always direct evidence in the context of resistant hypertension, but in other areas where these agents have shown benefit on cardiovascular disease outcomes.”
McEvoy said that evidence of the efficacy of renal denervation in improving cardiovascular outcomes, on top of its efficacy in reducing blood pressure, would dictate any future changes.
Demonstrating that reductions in blood pressure resulting from the use of renal denervation do lead to improvements in cardiovascular events would likely elevate the therapy within guidelines, Felix Mahfoud (Saarland University Hospital, Homburg, Germany) who has researched the technique extensively tells Cardiovascular News, but the practicalities of conducting such a trial make it unlikely.
“Both randomised controlled trials and real-world registries have demonstrated the blood pressure-lowering efficacy of renal denervation. It is highly likely that these reductions in blood pressure will translate into improved outcomes, including lower rates of stroke, myocardial infarction, heart failure, and other cardiovascular events,” he comments.
“However, from a purist research perspective, proving this association in a randomised controlled trial would be ideal, as it could eventually lead to a class I recommendation in guidelines. Conducting such an outcomes trial in renal denervation, however, would be challenging due to the need for a large sample size (>10,000 patients), long-term follow-up (five years), and the associated high costs.”
Elsewhere, the 2024 guidelines maintain an existing definition for ‘Hypertension’ as a blood pressure measuring ≥140/90mmHg, but introduce a new category of ‘Elevated blood pressure’ which is defined as 120–139/70–89mmHg. This new category is intended to facilitate consideration of more intensive blood pressure treatment targets among persons at increased risk for cardiovascular disease.
Another change sees the introduction of a new systolic blood pressure treatment target range of 120–129mmHg for most patients receiving blood pressure-lowering medication, with the proviso that the new target requires that treatment is well tolerated.
In part to accommodate this new more intensive systolic blood pressure treatment target range, the 2024 ESC guidelines provide stronger recommendations than prior guidelines for the use of out-of-office blood pressure measurements—including ambulatory blood pressure monitors and validated home blood pressure monitors.
The addition of renal denervation—having previously been confined to use solely in the setting of clinical trials—has been described by advocates of the technique as a big step forward for patients requiring additional options to control hypertension.
“Renal denervation has returned to the guidelines and is now recommended for patients with uncontrolled resistant hypertension, as well as for those who are unable or unwilling to tolerate antihypertensive medications”, comments Mahfoud. “This is reassuring news for both physicians and patients. The guidelines also suggest that renal denervation should be considered as an alternative or additive approach to lowering blood pressure, used in combination with lifestyle modifications and antihypertensive drugs.”
The statement was published in the journal Hypertension and recognises in particular that patients with uncontrolled hypertension, those with resistant hypertension or who have multiple medication intolerances, may be the most likely to benefit from the procedure, albeit with the caveat that further research is needed in areas such as patient selection and long-term efficacy.
“The AHA scientific statement presents an intensive review of trial evidence, followed by clinical considerations and practical recommendations for incorporating renal denervation into hypertension treatment programmes,” said Naomi Fisher (Harvard Medical School and Brigham and Women’s Hospital, Boston, USA), a co-author of the statement and consultant for Recor Medical, one of the two companies that has a renal denervation device approved for use by the US Food and Drug Administration (FDA).
“While more research is needed, most, but not all, of the new generation randomised renal denervation control trials reached their primary endpoint, and the procedure carries a favourable safety profile. The AHA statement serves an important role by illuminating renal denervation as a new treatment option for many patients with uncontrolled hypertension, particularly those with resistant hypertension or who are intolerant to multiple medications.”
The Intara introducer sheath is intended to maintain access to a patient’s peripheral or central vasculature (excluding coronary and neuro vasculature) to facilitate the introduction of therapeutic or diagnostic devices. The 10Fr sheath is resistant to kinking and it offers enhanced visibility to assist with the introduction, navigation, and delivery of devices for a variety of vascular procedures. Argon Medical anticipates the Intara introducer sheath will help facilitate the use of the company’s TLAB transvenous liver biopsy system and the Scorpion and Traveler portal vein access sets, as well as stents for the transjugular intrahepatic portosystemic shunt (TIPS) procedure, a recent press release states.
“The Intara introducer sheath is an upgrade to the current market options. It provides more resilience, ease of use, and safety throughout the TIPS procedure and stent placement,” said Dylan Suttle (Greensboro Radiology, Greensboro, USA).
The TLAB transvenous liver biopsy system is an expansion of Argon Medical’s TLAB transjugular liver biopsy system, adding US Food and Drug Administration (FDA)-clearance for a unique approach for collecting biopsy samples from the liver via access in the femoral vein. The system includes a novel tool that allows users to safely adjust the shape of the device to best suit a patient’s unique anatomy. The new addition is reinforced by a recent 500-patient retrospective review demonstrating the safety and efficacy of transfemoral transcaval liver biopsies versus the traditional transjugular approach. The authors of this review, including Jacob Cynamon (Montefiore Medical Center, New York, USA) found transfemoral transcaval liver biopsies had reduced complication rates with no hepatic injuries. Argon Medical designed the TLAB transvenous liver biopsy system in conjunction with patents licensed from Montefiore on which Cynamon is a primary inventor.
“The TLAB transvenous liver biopsy system approved for both transjugular and transfemoral use, offers an alternative femoral approach for physicians to achieve technical and histopathologic success while minimising procedural time and complications. With the transfemoral approach, we have seen the benefits first-hand and I believe this will be a positive step forward for patients and physicians performing liver biopsies,” said Cynamon.
“We are pleased to expand our liver management portfolio with the addition of the Intara introducer sheath and the TLAB transvenous liver biopsy system,” said George Leondis, president & chief executive officer, Argon Medical. “Our company is dedicated to applying innovation to improve the devices interventionalists use to diagnose and treat liver diseases. This is demonstrated by our cadence of new product introductions in this space.”
“Liver diseases (cirrhosis, hepatitis, and cancer) account for one out of every 25 deaths worldwide, illustrating the need for faster, easier, and more accurate diagnosis and treatment options. We listened to the advice of physician experts in this field to guide development of the Intara introducer sheath and the TLAB transvenous liver biopsy system. As we commercialise these new devices, we are excited to see their expertise translate into positive outcomes for interventionalists and the patients they serve,” said Tom Younker, senior vice president of Global Marketing, Argon Medical.
Surmodics has announced that it has received US Food and Drug Administration (FDA) 510(k) clearance for its Pounce XL thrombectomy system.
The Pounce XL thrombectomy system is indicated for the non-surgical removal of thrombi and emboli from the peripheral arterial vasculature in vessels 5.5–10mm in diameter, making it suitable for iliac, femoral, and other arteries within this range. The Pounce XL thrombectomy system dramatically increases the size range of the Pounce platform, which also includes the thrombectomy system, indicated for 3.5–6mm peripheral arteries, and the Pounce Low Profile (LP) thrombectomy system, indicated for 2–4mm peripheral arteries. The Pounce thrombectomy system and Pounce LP thrombectomy system were introduced in 2021 and 2024, respectively.
“Securing FDA clearance for Pounce XL is a major step forward in Surmodics’ pursuit of a complete mechanical thrombectomy solution for all peripheral arteries, notably critically ischemic lower extremity vessels,” said Gary Maharaj, president and chief executive officer of Surmodics. “The Pounce thrombectomy platform has already demonstrated its performance as a rapid, efficient solution for the removal of both acute and chronic thrombi and emboli in peripheral arteries without the use of thrombolytics. The addition of the Pounce XL thrombectomy system to our Pounce thrombectomy platform demonstrates our commitment to setting the pace and direction of innovation in this critical space.”
Maharaj added: “Critically ischaemic peripheral arteries often have older, organised clots that resist catheter-directed thrombolysis and aspiration thrombectomy. The Pounce thrombectomy platform allows physicians to rapidly restore blood flow regardless of clot morphology, which has the potential to reduce the need for follow-up procedures and additional thrombolytic therapy requiring intensive-care-unit admission.”
Surmodics expects to initiate limited market release for the Pounce XL thrombectomy system in the first half of 2025, with commercialisation planned following the completion of the limited market release.
B Braun has announced that the US Food and Drug Administration (FDA) has granted 510(k) clearance for the Introcan Safety 2 deep access intravenous (IV) catheter, the newest addition to the Introcan Safety 2 IV catheter portfolio.
The Introcan Safety 2 deep access IV catheter merges the trusted technologies of the original Introcan Safety 2 Multi-Access and Introcan Safety deep access catheters, offering clinicians an advanced solution that combines the strengths of both devices. This innovative catheter provides fully automatic passive safety needlestick protection and multi-access blood control in longer lengths and is designed to access deeper veins in patients with difficult vascular access and to achieve longer dwell times.
The Introcan Safety deep access IV catheter has been shown to increase peripheral intravenous catheter (PIVC) dwell times to approximately 5.7 days—compared to 3.8 days for standard long PIVCs—to help reduce PIVC restarts and help reduce escalation to more costly, invasive devices such as peripherally inserted central catheters (PICC). The multi-access blood control hub in the Introcan Safety 2 deep access PIVC is designed to minimise blood exposure and reduce the need for cleanup of blood throughout IV therapy, and there is no need to occlude the vessel during insertion or any time the hub is accessed.
“We are excited to broaden our Introcan Safety 2 IV catheter portfolio, allowing our customers to benefit from passive safety and blood exposure protection with deep access technology,” said Chad Laity, director of marketing, vascular access, IV systems and securement. “By offering a reliable solution for challenging cases, we aim to help improve patient outcomes and reduce the need for more complex procedures.”
Six-month results of the WRAPSODY Arteriovenous Access Efficacy (WAVE) pivotal trial have reported superior target lesion primary patency (TLPP) with Wrapsody (Merit Medical) cell-impermeable endoprosthesis (CIE) when compared to percutaneous transluminal angioplasty (PTA). These data were presented by Mahmood Razavi (St Joseph Heart & Vascular Center, Orange, USA) during a FIRST@CIRSE session at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14–18 September, Lisbon, Portugal).
Wrapsody was developed to aid physicians in treating patients with stenosis/occlusion in the vessels used for haemodialysis. Creation and maintenance of an arteriovenous fistula or graft (AVF/AVG) to achieve long term vascular access is required for patients undergoing haemodialysis, although progressive stenosis or occlusion can pose life-threatening consequences.
In 2021, clinical outcomes from the first-in-human trial of Wrapsody showed a 12-month TLPP rate of 84.6% and an access circuit primary patency (ACPP) of 65.9%. Building on these results, the WAVE trial was conducted to assess the outcome of Wrapsody endoprosthesis as compared to PTA in a large-scale study.
The prospective, randomised, multicentre study enrolled 245 patients with arteriovenous fistula (AVF) peripheral venous circuit outflow lesions requiring intervention from 43 international centres. Of this cohort, 122 patients were randomised to PTA and 123 to Wrapsody.
Their results showed that six-month patency was “significantly” higher for both TLPP (89.8% vs. 62.8%, p<0.0001) and ACPP (72.6% vs. 57.9%, p<0.015) in patients treated with Wrapsody when compared with patients randomised to PTA. Additionally, in a summary of safety events through 30 days post treatment, there was no significant difference between the groups with very low event rates in both. Freedom from 30-day safety event rate was 96.6% in the Wrapsody group versus 95% in the PTA group.
Speaking to Interventional News following his presentation, Razavi noted that Wrapsody’s superiority over PTA concerning ACPP is crucial, as this is a “critical” metric for physicians and patients when identifying the magnitude of an intervention’s benefit.
He continued, stating that: “While covered stents and drug-coated balloons have improved lesion patency in these patients, ACPP still remains a challenge. Results of this trial not only showed superiority of Wrapsody over angioplasty but also numerical improvement over prior technologies. This six-month analysis provides insight regarding Wrapsody’s anticipated long-term performance.”
The first report of six-month results from the SUCCESS PTA trial evaluating the Selution SLR (Cordis) drug-eluting balloon has shown that consistent haemodynamic, functional and clinical improvements were observed, associated with a 97.7% freedom from clinically-driven target lesion revascularisation (CD-TLR), which was reported as 97% for the chronic limb-threatening ischaemia (CLTI) subgroup.
The SUCCESS PTA trial enrolled 723 patients from 27 sites across Europe, Asia, and South America, primarily evaluating CD-TLR. Lichtenberg described the cohort’s Rutherford classification at baseline, noting that 74.2% of patients had claudication and 25.8% were identified as having CLTI.
Describing lesion characteristics of the full cohort, Lichtenberg pointed to the percentage of grade 3 and 4 lesions, which were 20% and 16.3%, respectively. He stated that bail-out stenting occurred in 32% of patients—the reasons for this being residual stenosis (47.5%), flow-limiting dissection (45.6%), and other factors (11.4%).
In the full cohort, the identified procedural and device success rate was 97.9% and 99%. In the claudication subgroup, device and procedural success was 99.2% and 98.3%, and 98.6% and 96.8% in the CLTI subgroup, respectively. Using a Kaplan-Meier curve, freedom from CD-TLR at 180 days was 97.7% across the full cohort—97.9% for the claudication subgroup and 97% for the CLTI subgroup.
The study’s major adverse event rate (MALE) composite endpoint—including severe limb ischaemia leading to an intervention on target limb or major vascular amputation—was 5.9% in the full cohort at six months, which translated to 4% and 12.2% in the claudication and CLTI subgroups, respectively. Overall, 85.4% of patients improved by least one Rutherford classification category.
In conversation with Interventional News at CIRSE 2024, Lichtenberg stated these results are “game changing” in the treatment of peripheral arterial disease (PAD) in patients with claudication and CLTI. He commented that these six-month results are encouraging and show a consistent improvement across a range of associated disease processes.
A new study shows that a minimally invasive treatment for osteoarthritis (OA) in the knees may have a lasting benefit of at least two years.
Published today in the Journal of Vascular and Interventional Radiology during Pain Awareness Month, the study of genicular artery embolization (GAE) followed 40 patients with moderate-to-severe symptomatic knee OA after their GAE treatment and measured pain scores throughout the 24-month study period. The patients were not candidates for total knee replacement.
“Knee osteoarthritis is a leading cause of adult disability and, until now, most minimally invasive treatment options have been proven to provide only short-term relief, measured in weeks or months,” said Siddharth A Padia (UCLA Health, Los Angeles, USA), the lead author of the study. “For patients who are not candidates for knee replacement surgery, our study shows that GAE provides durable benefit to many patients, measurable for up to two years, a great leap forward in offering this cohort lasting relief.”
OA was once considered just a “wear and tear” process, but there is increasing evidence that the growth of new, abnormal synovial blood vessels causes painful inflammation, greatly contributing to OA symptoms throughout the body. GAE targets this abnormal blood flow to reduce inflammation, quickly improving patients’ pain.
To deliver treatment, interventional radiologists create a pinhole-size incision in the hip and insert a small catheter into the arteries in the arthritic knee. They, then, inject tiny particles to normalize the blood supply to inflamed and painful areas of the knee. The outpatient procedure takes approximately one to two hours, followed by a two-hour recovery period.
For this prospective, single-arm study, researchers defined clinical success as a greater than 50% reduction in OA symptoms using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). A previous study of this cohort found that 25 of the patients (66%) reported improvement at one year. Of those 25, 18 patients (72%) have since reported continued relief of symptoms at two years. Overall, 18 of the original 38 patients (47%) who remained in the study throughout the two-year follow up period reported a greater than 50% reduction in OA symptoms over the two years. No long-term adverse effects were reported.
“GAE is a promising therapeutic option for patients with osteoarthritis in the knee, allowing patients to return to their normal activities without lengthy recovery times,” said Padia. “We believe further investigation with larger cohorts and randomised controls should be conducted so we can validate these findings, refine patient selection and optimise the management of OA related knee pain.”
Jupiter Endovascular has announced that the first two patients have been treated in SPIRARE I, a multicentre study of the Vertex pulmonary embolectomy system using the company’s Endoportal Control platform technology.
The Vertex system is designed to treat acute pulmonary embolism (PE) in an endovascular procedure. The successful first two cases were performed at St John Paul II Hospital in Krakow, Poland, a cardiothoracic specialist centre affiliated with the Jagiellonian University, by study investigators Grzegorz Kopec, Jakub Stepniewski and Krzysztof Bartus.
“In these first cases, the Vertex system was successful in safely navigating through the right heart and into the pulmonary vasculature, facilitating an efficient and effective pulmonary embolectomy with no safety issues,” said Kopec, who is the head of the team for the diagnosis and treatment of pulmonary circulatory diseases at St John Paul II Hospital. “The patients’ clinical condition and haemodynamics improved on the table during the procedure, and postoperative imaging showed noticeable improvements in right heart function.”
“Controlling interventional devices within the pulmonary arterial tree when treating patients with intermediate-risk and high-risk PE can be challenging with today’s commercially available technology,” said Stepniewski, the Pulmonary Embolism Response Team (PERT) coordinator at St John Paul II Hospital. “The endoportal technology enabled the large-bore Vertex system to remain stable in tachypneic patients, allowing us to quickly access and revascularise multiple areas of the pulmonary vasculature in a controlled manner when facing a high degree of cardiorespiratory movement.”
“I was pleasantly surprised that the endoportal technology provided a level of control similar to what I experience in an open surgical embolectomy, with the added ability to directly access a much wider range of vessels,” said Bartus, professor of medicine at the Jagiellonian University, St John Paul II Hospital. “My team and I are very excited about studying a new technology with the potential to give us greater stability and control when treating pulmonary embolism, which may have a positive impact on patient outcomes. As a principal investigator of this study, I want to thank the Jupiter Endovascular team, Professors Boguslaw Kapelak, Jacek Legutko, and Piotr Podolec from our hospital, and director of the hospital Doctor Grzegorz Fitas, for their help and support in this first-in-human clinical trial.”
SPIRARE I is a prospective, single-arm, multicentre study enrolling patients with acute, intermediate-risk PE treated with the Vertex pulmonary embolectomy system.
In addition to St John Paul II Hospital, the Medical University of Vienna is planned to be a second study site, with Irene Lang serving as the principal investigator for that site.
Trial endpoints will characterise the procedural and clinical benefits of PE treatment with Endoportal Control using the Vertex system, across measures of safety, right heart function, and clinical improvement from the time of the procedure to 30 days post-procedure.
The company’s Endoportal Control platform technology integrated into the Vertex system is designed to bring greater stability to a variety of catheter interventions, with the goal of enabling interventionalists to treat anatomical sites that they cannot safely or easily reach with a conventional endovascular approach, Jupiter Endovascular says in a press release. The endoportal device is delivered in a flexible, relaxed state over a guidewire to a target location in the vasculature, pressurised with saline to fix it in a stable position for therapeutic delivery, then relaxed again to navigate to another target location or for removal.
“We are delighted with the performance of our technology in these first two cases, demonstrating safe access and the ability to bring a high degree of precision and control to the successful treatment of these patients with intermediate-risk pulmonary embolism,” said Carl J St Bernard, Jupiter Endovascular CEO. “As the first step in our SPIRARE clinical program, we look forward to validating these positive results more broadly in this study and in the upcoming SPIRARE II pivotal trial, as well as to expanding the potential benefits of our Endoportal Control platform technology to additional clinical areas where we intend to improve the lives and well-being of many patients.”
Royal Philips today announced the introduction of the 160cm US Food and Drug Administration (FDA)-approved version of its LumiGuide endovascular navigation wire. This enhanced LumiGuide guidewire, which utilises the company’s Fiber Optic RealShape (FORS) technology, was used for the first time on a patient by Carlos Timaran (UT Southwestern Medical Center, Dallas, USA). He used the technology during a complex aortic aneurysm repair operation, marking the 1000th patient treated milestone using FORS since its first clinical use in 2020.
A press release notes that the introduction of a longer FORS-enabled LumiGuide navigation wire enables US clinicians to visualise a broader range of catheters and expands usage of this technology to patients in the USA treated in centres equipped with LumiGuide.
“The new enhanced Philips LumiGuide navigation guidewire represents a significant leap forward in endovascular surgery, offering unprecedented 3D visualisation and precision during complex procedures,” said Timaran. “As the first to use this guidewire for a complex aortic repair, I experienced firsthand its potential to revolutionise how we approach minimally invasive vascular interventions. The patient who underwent this groundbreaking procedure is doing well, further validating the efficacy of this innovative technology.”
Philips shares that LumiGuide—powered by the company’s FORS technology—allows clinicians to see their guidewires and catheters in 3D and colour as they manipulate them inside the patient’s body, from any angle, in real-time, and with minimal radiation. The company adds that its FORS technology simplifies navigation in tortuous vessels.
Using this advanced technology, research published in the Journal of Vascular Surgery and from Philips shows that complex cases such as aortic repair procedures can be done 37% faster and use 70% less X-ray imaging during the process.
Providing greater reach and enhanced catheter loading possibilities than the company’s existing 120cm (47 inch) guidewire, Philips claims that its new 160cm (63 inch) LumiGuide wire enables US physicians to experience 3D device guidance with more catheters than before, enabling use of the technology for more patients and procedures.
“LumiGuide unlocks the colour visualisation of wires, catheters, and patient anatomies in 3D from any angle, including simultaneous angles to generate ‘virtual biplane’ images. Combined with device navigation viewed from angles physically unachievable using conventional C-arm systems, it has already been shown to improve workflows, reduce procedure times, and decrease patient and staff radiation dose,” said Atul Gupta, chief medical officer for diagnosis and treatment at Philips and a practicing interventional radiologist.
Philips advises that LumiGuide integrates seamlessly into the company’s image-guided therapy system, Azurion, allowing its use alongside preoperative cross-sectional imaging.
Merit Medical has today announced positive six-month findings from the randomised arteriovenous (AV) fistula arm of its Wrapsody Arteriovenous Access Efficacy (WAVE) pivotal trial. The data were shown at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE: 14–18 September, Lisbon, Portugal) during a FIRST@CIRSE presentation.
Wrapsody is a cell-impermeable endoprosthesis which is intended to extend long-term vessel patency in dialysis patients. Many patients undergoing dialysis rely on a vascular access site created in the arm called an AV fistula. The maintenance of adequate blood flow through this site is crucial for patient survival.
The AV fistula arm of the WAVE trial enrolled 245 patients at 43 sites. Patients were randomised 1:1 to Wrapsody or percutaneous transluminal angioplasty (PTA). Target lesion primary patency in patients treated with Wrapsody was 27 percentage points higher than patients in the PTA cohort (89.8% vs. 62.8%, p<0.0001). The proportion of patients who experienced an adverse event was similar between cohorts.
“The superiority of the six-month efficacy data is compelling and provides clinicians the chance to evaluate how Wrapsody can help us prolong the vascular access of our patients. Wrapsody should be the new standard of care for these patients,” said Mahmood K Razavi (St. Joseph Heart and Vascular Center, Orange, USA), co-principal investigator of the WAVE trial. “Meeting with colleagues at CIRSE to discuss the AV fistula arm of the WAVE study was the first of what we hope to be many productive discussions,” said Robert G Jones (Queen Elizabeth Hospital Birmingham, Birmingham, UK), and co-principal investigator of the WAVE study. “The potential for Wrapsody to help us safely extend vascular access for our patients is a vital component of care.”
“The data release of positive findings from the randomised AV fistula arm of the WAVE study marks a major milestone for Merit,” said Fred P Lampropoulos, Merit’s chairman and chief executive officer (CEO). “This is an important next step in our continued efforts to seek ways to improve care for patients requiring haemodialysis treatment.”
The Merit Wrapsody Cell-Impermeable endoprosthesis is not approved or available for commercial distribution in the USA and may not be approved or available for sale or use in other countries. In the USA, the device is being used under an Investigational Device Exemption (IDE) from the US Food and Drug Administration (FDA). Findings from the WAVE study expand on results from the first-in-human study (Wrapsody FIRST) and support the Premarket Approval (PMA) application to the US FDA for commercial use in the USA. The device is available in Brazil and in the European Union.
Sirtex Medical has today announced that it has received certification according to European medical device regulation (MDR) 2017/745 for SIR-Spheres Y90 resin microspheres and its delivery systems, paving the way for the European launch of the SIROS delivery system.
The MDR places greater emphasis on patient safety measures, risk management, post-market surveillance, and comprehensive data collection for medical devices seeking European market access.
“Patient health and safety are always at the forefront of our work. That is why we are particularly proud to receive EU MDR certification for SIR-Spheres Y90 resin microspheres and its delivery systems, including SIROS. This achievement underscores our commitment to delivering innovative products responsibly and ethically,” said Matt Schmidt, chief executive officer of Sirtex Medical. “With the expansion of SIROS outside of the USA, interventional radiologists in Europe now have an additional option to support patients battling metastatic colorectal cancer (mCRC) and unresectable hepatocellular carcinoma (HCC). This milestone reflects the outstanding efforts of our team, the rapid growth of our business, and the groundbreaking interventional oncology solutions we have developed.”
The SIROS delivery system offers an intuitive, visual, and adaptable solution for physicians to administer SIR-Spheres to liver cancer patients. Its easy-to-use design along with controlled administration provides physicians confidence in the Y90 delivery, states a recent press release published by the company.
“As an interventional radiologist, I am excited about the future use of the SIROS Delivery System,” shared Thomas Helmberger (München Klinik Bogenhausen, Munich, Germany). “This device has an intuitive design and a precise control that will facilitate the administration of SIR-Spheres Y90 resin microspheres, and I am looking forward to incorporating it into my practice.”
Shockwave Medical, part of Johnson & Johnson MedTech, has announced the full US launch of its Shockwave E8 peripheral intravascular lithotripsy (IVL) catheter, following clearance by the US Food and Drug Administration (FDA).
“Shockwave’s newest peripheral catheter offers significant improvements that will help physicians refine their treatment algorithm and better support challenging patients with heavily calcified disease,” said Venita Chandra, vascular surgeon and clinical associate professor, Division of Vascular Surgery, Stanford Health Care (Stanford, USA). “The catheter’s ability to treat long lesions and its extended reach enable safe and effective treatment of some of our most difficult-to-treat patients, including those with CLTI, a complicated and severe disease state with a high mortality rate.”
Shockwave Medical claims that, with four hundred pulses delivered twice per second, and eight emitters across an 80mm balloon, Shockwave E8 can treat longer lesions more efficiently. Additionally, with an increased catheter working length of 150cm, physicians can extend their IVL treatment to reach below-the-knee and very distal lesions. Combined with Shockwave L6, Shockwave M5+, and Shockwave S4 IVL catheters, the company notes that the addition of Shockwave E8 offers physicians a complete IVL portfolio to treat challenging calcified lesions across the entire peripheral anatomy.
“Shockwave E8 represents our commitment to physician-guided innovation while maintaining the simplicity and effectiveness of our IVL technology,” said Isaac Zacharias, president, Shockwave Medical. “We have received very positive physician feedback on Shockwave E8 and look forward to establishing it as our new workhorse peripheral IVL catheter for physicians addressing challenging calcium above and below the knee.”
Argon Medical has today announced the launch of the CLEANER Vac thrombectomy system for the removal of blood clot from the peripheral venous vasculature.
The Cleaner Vac thrombectomy system is a disposable, large-bore aspiration system designed to quickly and effectively remove blood clot, also known as thrombus, from vessels with restricted blood flow. In a recent press release, the company states that the device enables physicians to manually control powered aspiration, enabling procedures with precise clot removal that may minimise vessel damage and reduce blood loss.
“Removing thrombus from the venous anatomy can be very challenging depending on the patient’s condition. Interventionalists need a simple and intuitive tool that allows them to easily navigate through the vasculature to the treatment area and control the removal of any obstructive thrombus. The streamlined design of the Cleaner Vac enables easy assembly, quick navigation, and efficient treatment, making it a welcomed treatment option for patients with this disease state.” said Fakhir Elmasri (Lakeland Vascular Institute in Lakeland, USA). Elmasri was the first physician in the USA to treat a patient with the Cleaner Vac system.
“We are committed to advancing healthcare and we are excited to deliver the newest thrombectomy solution to interventionalists who prioritise efficient, successful outcomes for their patients. The Cleaner Vac thrombectomy system is a testament to our dedication to improving treatment for this disease state, and we are confident this device will easily integrate into the current standard of care,” said George Leondis, president & chief executive officer at Argon Medical.
“Nearly 900,000 people in the USA are diagnosed with problematic blood clots in the venous system, every year, leading to between 60,000 and 100,000 deaths annually. The Cleaner Vac thrombectomy system offers physicians more control to remove those clots and the streamlined design can simplify traditionally complex procedures,” said Tom Younker, senior vice president of global marketing at Argon Medical.
The Cleaner Vac thrombectomy system is currently available in the USA.
Penumbra today announced it has secured CE mark in Europe for two computer-assisted vacuum thrombectomy (CAVT) technologies—Lightning Flash 2.0 and Lightning Bolt 7.
“Based on outcomes from our clinical trials and from physicians using our devices globally, our CAVT technologies have greatly improved our ability to rapidly and safely remove clot in the vascular system,” said James F Benenati, chief medical officer at Penumbra. “With quicker procedures and more efficient clot removal, we have improved outcomes while demonstrating a high level of safety. As adoption of thrombectomy becomes more widespread, Lightning Flash 2.0 and Lightning Bolt 7 will provide physicians in Europe with the confidence that CAVT is a valuable first-line option to manage conditions such as pulmonary embolism (PE), venous thrombosis, and acute limb ischaemia (ALI).”
A press release details that Penumbra’s Lightning products will be the only CAVT systems available in Europe.
Lightning Flash 2.0
According to Penumbra, Lightning Flash 2.0 is the most advanced mechanical thrombectomy system on the market to address venous and pulmonary thrombus. It features Penumbra’s Lightning Intelligent Aspiration technology with the latest dual clot detection algorithms, using both pressure and flow-based processes to detect blood clot and blood flow.
The Lightning Flash 2.0 catheter is made with MaxID hypotube technology, allowing an inner diameter similar to large-bore catheters while maintaining a lower profile and a soft, atraumatic tip design. It is designed to help remove blood clots with speed, safety and simplicity, Penumbra notes, allowing physicians to better navigate the body’s complex anatomy and deliver high power aspiration for clot removal with minimal blood loss.
Additionally, Lightning Flash 2.0 has streamlined audio-visual feedback, which Penumbra states enables physicians to have a better understanding of what is occurring at the tip of the catheter during a procedure.
“We have utilised Penumbra’s aspiration technology since the introduction of the first-generation Indigo system, witnessing significant advancements with each new iteration,” said Nils Kucher, director of the Department of Angiology at University Hospital Zurich (Zurich, Switzerland).
“Our team has experience with the 12Fr system for acute venous thrombosis, and with this latest advancement, we are hopeful that the procedures will be even more efficient for PE and venous thrombosis as we have received positive feedback from colleagues in the USA.”
“We are eagerly anticipating the opportunity to use the new Lightning Flash 2.0 system, as it promises aspiration capabilities to address large clot burden quickly and has the potential to minimise blood loss,” said Stefano Barco, Department of Angiology at University Hospital Zurich.
Lightning Bolt 7
Penumbra claims that Lightning Bolt 7 is the most powerful arterial thrombectomy system on the market. Lightning Bolt 7 introduces a new method for removing blood clots—modulated aspiration—which pairs Penumbra’s Lightning Intelligent Aspiration technology with an advanced microprocessor algorithm. When used together, Lightning Bolt 7 is designed to enhance the ability to rapidly remove large, fibrous blood clots in the arteries with minimal blood loss, addressing conditions such as ALI, hibernating thrombus and visceral occlusions.
Lightning Bolt 7 is engineered to detect the difference between blood clot and blood flow. Additionally, it is designed to break the friction between the catheter and clot by having the computer algorithms rapidly modulate aspiration to quickly fatigue the thrombus and remove the clot from the arteries. This facilitates maximum vacuum force at the catheter tip for optimal, rapid ingestion of blood clots.
“In my opinion, computer-assisted thrombus removal is the future of arterial clot management and offers the promise of peak procedural efficiency that was not previously available to endovascular specialists,” said Gianmarco de Donato, chief of the Vascular Surgery Unit at University Hospital of Siena (Siena, Italy). “Our ability to rapidly revascularise vessels with minimal blood loss is crucial for achieving optimal patient outcomes.”
Lightning Flash 2.0 and Lightning Bolt 7 come on the heels of Penumbra recently receiving CE mark for five of its stroke reperfusion and access catheters, expanding both its neuro and vascular portfolios in Europe.
Immunophotonics has announced a collaboration with The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) around a phase 2/3 clinical trial.
The trial is designed in collaboration with a Steering Committee nominated by CIRSE and managed by CIRSE’s contract research organisation, Next Research. This trial, entitled INJECTABL-3, will be a clinical trial conducted in two phases and is expected to enrol an estimated 300–500 patients in a randomised, controlled study in the USA and Europe. This pivotal trial will evaluate the safety and efficacy of Immunophotonics’s lead clinical asset, IP-001, in combination with ablation treatments in key indications where tumour ablation is the current standard of care.
Philippe L Pereira (SLK-Kliniken, Stuttgart, Germany)—incoming president of CIRSE, commented: “The collaboration between Immunophotonics, CIRSE, and Next Research highlights the importance of multidisciplinary partnerships in advancing major medical breakthroughs for patients in need. Tumour recurrence following radical tumour ablation is a major unmet medical need, and Immunophotonics’s novel approach is not only practical for clinicians and patients, but early data indicates it has tremendous promise.”
“This partnership signifies an important step in advancing the emerging field of interventional immuno-oncology,” remarked Nathalie Kaufmann, chief operating officer at Next Research. “It’s just the start, and we look forward to combining the expertise of our organisations to advancing the potential of IP-001.”
Uwe Martens (SLK-Clinics Heilbronn, Heilbronn, Germany) and future principal investigator of the INJECTABL-3 study, stated, “We are looking forward to playing a part in the INJECTABL-3 trial and seeing the potential for IP-001 to become a game-changing treatment option for patients that receive tumour ablation. Early data demonstrates tolerability of the investigational product along with promise in terms of IP-001’s ability to drive abscopal effects. This type of immune-mediated response could be quite beneficial for patients, and therefore it will be important to conduct this clinical trial.”
“Immunophotonics is dedicated to transforming routine tumour destruction techniques, such as ablation, into something much more powerful for patients,” said Lu Alleruzzo, chief executive officer and co-founder of Immunophotonics. “Ablation will liberate tumour information that IP-001 will use to drive a systemic tumour specific immune response. Our clinical data thus far demonstrates the potential of our technology, and we are thrilled to be collaborating with the global clinical experts at CIRSE and Next Research on INJECTABL-3. I believe that together we will forever change the way cancer is treated.”
Microvention, a wholly owned subsidiary of Terumo Corporation, has today announced its official rebranding to Terumo Neuro, effective immediately.
This name change signifies a new chapter in the company’s evolution while maintaining its unwavering commitment to the creation and commercialisation of groundbreaking innovations in neurovascular care, as stated in a press release.
Founded in 1997 and acquired by Terumo Corporation in 2006, Microvention has been at the forefront of developing technologies that support neurovascular surgeons in preserving and restoring brain health. As Terumo Neuro, the company is poised to continue its legacy of innovation with an enhanced focus on driving impactful growth and leveraging Terumo’s global resources and reputation, the release continues.
Carsten Schroeder, president and chief executive officer of Terumo Neuro, commented on the rebranding: “This transformation reflects our growth as a company and Terumo’s confidence in our future. For eighteen years, we have maintained independent branding as Microvention and now, as Terumo Neuro, we’re combining the best of Microvention with the full strength and support of the Terumo family. Our culture, speed of innovation, focus on game-changing technologies, and close collaboration with physicians, will remain unchanged.
“What will evolve is a deeper partnership with Terumo, a new visual brand, and a more defined brand identity under our new name and slogan—‘Terumo Neuro: game-changing impact’. Our strategy is expanding beyond our core focus on haemorrhagic and ischaemic stroke and access solutions to encompass the neurovascular patient care continuum.”
As Terumo Neuro, the company will continue its close collaboration with leading physicians worldwide, translating clinical insights into technologies that enhance patient outcomes. Schroeder has also emphasised that the company’s DNA remains rooted in innovation for ischaemic stroke, haemorrhagic stroke, and access, while expanding into broader areas of neurovascular care.
FlowPhysix, formerly known as Expanse ICE, has announced a strategic partnership with 3comma Medical who will serve as their international commercial partner for their FlowRunner aspiration thrombectomy system.
This partnership between FlowPhysix and 3comma will provide physicians outside of the USA access to new standards in thrombectomy technology, enabling FlowPhysix to focus on US commercialisation.
3comma managing partner and former vice president of Penumbra, Marc Paris, believes the FlowRunner system will make an immediate impact in the peripheral thrombectomy segment. “We can rapidly activate our established international commercial infrastructure to accelerate adoption of the FlowRunner system. We are confident that FlowPhysix will be the next major disruptor in the global thrombectomy market and we are excited to be part of this endeavour,” Paris said.
The FlowRunner system overcomes the characteristic vacuum decay that limits conventional aspiration catheters by leveraging FlowPhysix proprietary technology. The aspiration catheter is advanced through an aspiration sheath and out of a distal valve, to directly apply full and undecayed aspiration force to the thrombus. The catheter is then retracted back into the aspiration sheath. This process of extension and retraction of the aspiration catheter is then repeated to fully aspirate the clot. In each cycle, segments of thrombus are sheared and efficiently evacuated through the catheter via an integrated saline flush. The device has shown to successfully remove a broad range and large volumes of thrombi and effectively restore blood flow.
“Our game-changing technology has the potential to alter the current standard of care for thrombectomy. This partnership provides FlowPhysix expanded reach in delivering our unique solutions to patients worldwide. We strongly believe that 3comma’s proven leadership and deep expertise will drive commercial success internationally and increase shareholder value for the company,” said Jeff Hopkins, chief executive officer of FlowPhysix.
A recent analysis of deep venous stent placement has determined that the procedure is safe with low rates of major complications. Published in the journal CardioVascular and Interventional Radiology, the researcher team, led by Doireann P Joyce (Galway University Hospital, Galway, Ireland), state that responsibility is placed on the operator to be aware of the risks associated with deep venous stenting, although rare, so that fully informed consent can be obtained from the patient.
In their introduction, the authors describe the development of deep venous stenting into a primary treatment modality for venous obstruction across recent decades. Largely, reported complications rates are low, and are typically based on patient case reports and single-centre cohorts, which limits the broader applicability of collected data.
Aimed to determine the incidence of major complications associated with iliocaval and iliofemoral stent placement, Joyce et al collected data from three tertiary deep venous referral centres between January 2014 and September 2023. Their focus was on major complications which included: death, major bleeding requiring transfusion, massive pulmonary embolism, any complication that required endovascular or open surgical intervention, vessel rupture, acute kidney injury requiring dialysis, stent crushing, fracture, migration, involution or erosion.
Within the nine-year study period, 1,814 patients were treated for acute or chronic deep venous pathology. Concerning the venous pathology of their cohort, 44 patients were identified as having post-thrombotic syndrome; nine with acute deep vein thrombosis (DVT); six with May-Thurner lesions with DVT; and two with phlegmasia cerulea dolens. Among these patients, 61—3.3%—experienced a major stent-related complication, the most frequent of which was reported to be stent crushing (29.5%), followed by stent fracture (16.4%) and erosion of the stent through the vessel wall (13.1%). The authors note that death was a rare event (0.2%).
“Interventionists performing these procedures must be aware of the occurrence of complications associated with stent placement to counsel patients adequately and promote avoidance through optimal procedural approach,” Joyce and colleagues write.
Speaking to Venous News, Joyce commented: “This paper, highlighting the low rate of major complications associated with deep venous stenting, is timely given the increasing number of these procedures being performed worldwide. It is essential that interventionalists remain cognisant of potential risks and audit their own outcomes at regular intervals in order to ensure compliance with international best practice.”
“When providing a 24/7 interventional radiology [IR] trauma service, sometimes our procedures are expected to be concluded in few minutes. That’s why it’s important that we approach patients with a clear strategy,” said Anna Maria Ierardi (University of Milan, Milan, Italy), speaking to Interventional Newsahead of her presentation titled Minimal IR “survival kit” within trauma care.
Ierardi’s talk will appear during the Trauma team and the role of IR session at this year’s Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual scientific congress (14–18 September, Lisbon, Portugal). Setting out her objectives, Ierardi described what variables contribute to a successful IR trauma service.
“Our team is often faced with unpredictable situations in which time is crucial,” she detailed. “For us, it’s mandatory to have every tool available in order to choose the most suitable technique and to go with what we are most comfortable with.” Among the devices used in this setting, Ierardi defined what is needed to perform resuscitative endovascular balloon occlusion of the aorta (REBOA)—a procedure for patients with life-threatening bleeding not responding to resuscitative manoeuvres.
“A REBOA kit includes a needle, a sheath, guidewire, and balloon. In my opinion, to perform REBOA in a trauma setting, it should be a requirement to be able to get the access with ultrasound guidance,” Ierardi said. “You are faced with the most unstable and shocked patients without arterial pulses, so it’s important to be familiar with ultrasound guidance.”
In modern hospitals, the hybrid trauma room is equipped with a sliding computed tomography (CT) scanner—a feature which she stated is becoming more widespread across European and international centres. “This is the ideal situation,” she explained, “with this set up, specialists don’t need to move the patient for a CT, so when the patient arrives, they do not need to be mobilised until treatment is concluded, when they are then transferred to the intensive care unit”.
Another crucial aspect of the IR trauma team is cooperation between personnel, Ierardi shared. She believes that cooperation between trained interventional radiologists who usually work together on both elective and trauma cases makes a successful team. “It’s so that they know each other and are confident that they work in an effective and complementary way. Good results are dependent on the team being tight-knit.”
Ierardi went on to describe the differences in skillset between interventional radiologists who deal with elective cases and those who deal with trauma patients, stating that the latter, in her opinion, must be “very experienced”. “A good background— equating to long-term experience as an interventional radiologist—should translate well to the fast-paced environment that trauma care demands,” she added.
During her presentation, Ierardi will describe memorable cases from her centre that exemplify the scenarios her IR trauma team often encounter. Reflecting on how these cases went, Ierardi shared that often, cases that occur during the night are harder to manage.
“A big problem in this setting is that interventional radiologists are usually on call during the night. During the day, when all specialists are on-site, we can all be a part of the decision-making process along with orthopaedics, surgeons and anaesthesiologists,” Ierardi said. However, during the night or over the weekend, interventional radiologists are usually called in and must travel to the hospital when the diagnosis is already finalised and the indication for embolization has been determined by specialists. In most cases, the result is that the delivery of treatment is inevitably delayed, she said.
In setting out the “modern reality” of the IR trauma setting and the crucial elements that make up a 24/7 service, Ierardi invites all attendees to map their teams’ successes and failures to outline where improvements can be implemented to better approach the most critical of cases.
Taking place at the 2024 Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14–18 September, Lisbon, Portugal) the Women in Interventional Radiology (IR) focus session will include a brand-new forum. Taking place on Saturday afternoon, the inaugural Women in IR workshop: ‘Influencing with authenticity and assurance’ wants attendees to leave with actionable strategies to gain confidence at work. Speaking to Interventional News, Alex Barnacle (Great Ormond Street Hospital, London, UK) tells of what may be holding female interventional radiologists back, and the soft and hard skills needed to lead a room and command attention.
IN: What is the purpose of the Women in IR workshop and the new format?
The annual Women in IR session that is part of the CIRSE programme every year is always a big success, but we were keen to add something more for 2024. This year, the CIRSE meeting will include a focused workshop for mid-career female consultants in IR led by a wonderful leadership coach, Sarah Perugia. Sarah is well known to many of us in the leadership space. She brings expertise in working with diverse teams and women in leadership from around the world. Her focus is on empowering leaders to advance their careers, build confidence, enhance their performance in the workplace and ultimately to flourish and thrive.
During the two-and-a-half-hour workshop, Perugia will help participants to explore their mindset at work and reflect on how they present themselves in both clinical situations and during meetings or presentations. She will provide tips and tricks to help women gain confidence in order to lead with assurance, yet stay true to themselves. There will be opportunities for the workshop delegates to present topics to each other, discuss what might be holding them back in their career journeys and reflect on new ways to approach the challenges every single one of us face at work, male or female. By limiting this workshop to a small number of delegates and allowing plenty of time to explore these themes in depth, we hope to give participants a unique space to focus on themselves and their careers in a way that is almost never afforded them in their busy everyday lives.
This Saturday afternoon workshop will follow on very well from the morning plenary session which will focus on three different aspects of how women can be at our best in the workplace. Sarah will join a group of female interventional radiologists on stage in the morning to look at the role of mindset in shaping success in the workplace, building resilience in high-stress environments and the role of non-verbal communication.
IN: In the promotional video for the Women in IR session at CIRSE this year, Perugia explains that female body language and outward femininity makes it harder to “tell the story of power”—do you feel that femininity cannot be synonymous with power and leadership in IR?
We all know that we should be confident in being who we are and as feminine as we want to be, but it is something that many women in a male-dominated environment struggle with. Each of us need to find our own way to do it, and different people will do it in different ways. Some women are naturally more feminine in their style or their outlook than others, but it is something that I think preys on some people’s minds, especially early in a career when interventional radiologists are working to establish their credibility and figuring out how to express their professional expertise and fit in with a team.
All of this is often an unspoken thing, too. When I ask female colleagues about this, they often admit to concerns about feeling less equal than others in the workplace or about how to express themselves confidently at work without being labelled as aggressive or ‘bossy’. But there are very few forums that provide space for us to have these honest conversations or explore solutions. In the workshop, Sarah will look at all this in detail. I think it will be really valuable, because women rarely get the opportunity to deeply reflect on these things. I suspect that we often do ourselves a disservice by being uncertain in knowing how to project ourselves in the workplace and thinking we may be open to judgement. And for whatever reasons, men seem to struggle with this less often, though it is by no means a female-only problem.
IN: The sessions are geared toward mid-career interventional radiologists. Why is this and do you think early-career interventional radiologists would also benefit from this training?
We suspect that today’s mid-career consultants have probably never had any opportunities for this kind of training, it just doesn’t come up. Leadership and coaching themes are becoming more of a thing for junior doctors coming up through the ranks, and there are various mentor schemes available for younger doctors. So there are a few forums where some of these valuable conversations are taking place for our future IRs and that is wonderful. But when I was training, there was never a focus on these aspects of building a successful career. I know many women who are mid-career and who feel stuck, who wish that they could be on stage speaking at CIRSE, who wish they could be become a principal investigator on a research study, who wish that they could put themselves forward for a committee or a writing group, but just don’t feel that they have the confidence or the ability to do that.
It’s those women that I am interested in right now. CIRSE has a huge group of highly talented females who are out there doing really amazing work already, but their expertise may be under-recognised at national and regional levels because they do not put themselves forward. They remain very hesitant at taking that next step. And we see evidence of this quite often, we don’t always get a yes from women when we encourage them to step up to these roles. I know there are many, many reasons for that and some of it may well be work commitments as well as family life, but there is also a confidence issue that underlies it in many cases. We want those women to be flourishing in their careers to the best of their ability and recognised for being IR experts. So that’s what we are trying to achieve by providing these building blocks for them.
IN: You have gathered applications for the workshops, asking potential attendees what they would like to take from the forum. Can you share what some of the most common responses have been?
We had so many honest and open responses. Many attendees hope to gain a better understanding of how their body language changes how they are perceived by others and how they can express themselves with greater confidence at work. Frequently, responders reported that they feel unseen in the workplace, one woman sharing that patients often assume her to be a technician or nurse when male counterparts are in the room. Others have said that, although they are confident in their knowledge, transmitting this with confidence to colleagues and patients can be difficult, and they are concerned that this then lessens the importance of their viewpoint; this can be critical in emergency clinical scenarios. Several said they wanted to feel more self-assured when presenting and wanted to gain the confidence to push themselves forward for new roles. To address these concerns, we hope to provide the workshop attendees with constructive, actionable ways to project themselves with more self-assurance, increase their influence in the workplace and work towards building the careers they dream of.
In this short video, Michael Kostrzewa (Baden, Switzerland) and Rashid Akhtar (London, UK) discuss the latest approaches to the treatment of acute pulmonary embolism (PE) and deep vein thrombosis (DVT) using mechanical thrombectomy.
They examine which patients are eligible for this treatment based on current guidelines and physician experience. If you’d like to learn more, join Kostrzewa and Akhtar at the INARI Symposium at CIRSE 2024 on Sunday 15 September at 13:00 (Auditorium 2).
This video, intended for readers outside the USA, is sponsored by Inari Medical.
Jessica K Stewart (University of California, Los Angeles, Los Angeles, USA) shares what is currently known about reproductive outcomes following uterine artery embolization (UAE) through recent exemplar studies.
Understanding the impact that UAE for the treatment of symptomatic uterine fibroids may have on future reproductive outcomes is essential in helping patients choose a treatment that aligns with their goals. Though data regarding these outcomes is limited, several studies have provided information that might be useful in counselling patients considering UAE who have not yet completed their families.
A randomised controlled trial (RCT) by Maskova J Mara (Charles University, Prague, Czech Republic) et al compared reproductive outcomes between women undergoing myomectomy or UAE for uterine fibroids.1 In this study, more women undergoing myomectomy attempted to conceive compared to those undergoing UAE (40 vs. 26). There were significant differences in reproductive outcomes in favour of myomectomy, including a pregnancy rate of 78% vs. 50%, a delivery rate of 48% vs. 19%, and an abortion rate of 64% vs. 23%. This study was limited by small numbers, follow-up time, loss to follow-up, potential lack of generalisability, and lack of information about any fertility treatments utilised. The randomised trial of treating fibroids with embolization or myomectomy to measure the effect on quality of life (FEMME), led by Isaac Manyonda (St George’s University Hospital, London, UK), included reproductive outcomes as a secondary endpoint and found a pregnancy rate of 15% after UAE vs. 6% after myomectomy, but was also limited by small sample size.2 These conflicting RCT results underscore the need for additional investigation of the factors impacting reproductive outcomes.
One interesting recent study focused on ovarian function after UAE, and the impact that protective coiling might have on pregnancy rates.Their results found that 108 of 398 patients undergoing UAE had a “dangerous utero-ovarian anastomosis”, of which 33 underwent protective coil embolization. In patients desiring pregnancy, this occurred at a rate of 0.95 with ovarian protection versus 0.61 without ovarian protection (p=0.001), and remained significant when adjusting for age.3 Another study found that of five out of six women with increased follicle-stimulating hormone (FSH) levels after UAE had type IB or III utero-ovarian anastomoses, while none of the 21 women undergoing protective coiling for these anastomoses developed ovarian failure.4 These studies suggest that changes in technique could mitigate effects of UAE on ovarian function, which may impact fertility.
There are several challenges in attempting to design RCTs or large registry to evaluate reproductive outcomes in patients undergoing UAE. Enrolment is unlikely to be achievable, given that most women seeking pregnancy are counselled to undergo myomectomy based on the existing, low-quality data. Alternative approaches to studying reproductive outcomes should be considered in the future, such as studies of proxy metrics of fertility that could provide information to patients and physicians that would be valuable in shared medical decision making.
References:
Mara, Maskova J, Fucikova Z et al. Midterm clinical and first reproductive results of a randomized controlled trial comparing uterine fibroid embolization and myomectomy. Cardiovascular and Interventional Radiology. 2008 Jan;31:73-85.
Daniels J, Middleton LJ et al. Uterine artery embolization or myomectomy for women with uterine fibroids: Four-year follow-up of a randomised controlled trial. European J Obstet & Gynecol and Reproductive Biology: X. 2022 Jan 1;13:100139.
Serres-Cousine O, Kuijper FM et al. Clinical investigation of fertility after uterine artery embolization. Am J Obstet Gynecol. 2021 Oct;225(4):403.e1-403.e22. doi: 10.1016/j. ajog.2021.05.033. Epub 2021 May 29.
Sheikh GT, Najafi A, et al. Angiographic Detection of Utero-Ovarian Anastomosis and Influence on Ovarian Function After Uterine Artery Embolization. Cardiovasc Intervent Radiol. 2020 Feb;43(2):231-237. doi:10.1007 s00270-019-02305-7. Epub 2019 Sep 17.
Jessica K Stewart is an assistant professor of interventional radiology at the University of California, Los Angeles, Los Angeles, USA.
In August, the most popular stories from Interventional News included a feature on renal denervation and the techniques’ unexpected reappearance; a study which reveals an unforeseen neuropsychological effect following genicular artery embolization (GAE) for osteoarthritis; and a long-term Medicare study which uncovers a critical need for value-based care concerning peripheral vascular interventions (PVIs).
SonoVascular has announced the successful initiation of its first-in-human study (FIH) of the company’s SonoThrombectomy system, an ultrasound-facilitated, thrombolytic-enhanced platform that utilises multiple mechanisms of action to treat patients with venous thromboembolism (VTE). The catheter-based system combines microbubble-mediated cavitation with low-dose thrombolytic delivery to treat clots with no blood loss.
The US Food and Drug Administration (FDA) has issued a Class I recall—the most serious type—for Inari Medical‘s ClotTriever XL, 30mm device due to reports of patient injury, and death from device entrapment and pulmonary emboli (PE).
In a paper published in the July 2024 issue of the Journal of Hypertension, Andrew Sharp (University Hospital of Wales and Cardiff University, Cardiff, UK) et al reviewed 16 randomised controlled trials to assess the evidence of renal denervation’s (RDN) efficacy, concluding that, in uncontrolled arterial hypertension, RDN leads to a consistent reduction in blood pressure.
Continuing to divide opinion, as industry-led data regarding renal denervation emerge to show that the technique can provide a significant reduction in blood pressure long-term, some clinicians remain dubious.
Jupiter Endovascular has announced that the US Food and Drug Administration (FDA) has approved its investigational device exemption (IDE) application for the SPIRARE II US pivotal study. The pivotal trial will study the Vertex pulmonary embolectomy system, which incorporates Jupiter’s Endoportal Control platform technology into endovascular procedures intended to treat acute pulmonary embolism (PE).
A new study has determined genicular artery embolization (GAE) to be a “safe intervention” for mild knee osteoarthritis (OA), showing a sustained benefit at two years. Published in the journal CardioVascular and Interventional Radiology, the authors state that the “learning curve” reflected in their technical success rates uncovers the “complexities” behind the safe and successful performance of GAE.
In a new post-hoc analysis of the Lutonix (BD) arteriovenous (AV) global registry using investigational device exemption (IDE) criteria, Dimitrios Karnabatidis (Patras University Hospital, Patras, Greece) reports the “highest” six-month target lesion primary patency (TLPP) to date when evaluated through IDE criteria, presented at the Endo Vascular Access (EVA) meeting (14-15 June, Patras, Greece).
A newly published US Medicare cohort study illuminates trends and factors associated with peripheral vascular interventions (PVIs)—including a sharp rise in the use of ambulatory surgical centres (ASCs) and office-based laboratories (OBLs) for treatment—from 2011 to 2022.
In a session titled ‘Bariatric embolization: Is it the end or a new resurgence?’ at the Global Embolization Oncology Symposium Technologies (GEST) annual conference (16–19 May, New York, USA), Clifford Weiss (Johns Hopkins University, Baltimore, USA) made a case for “his future” and the future of bariatric embolization, providing the capability to “do surgery without doing surgery” to treat a highly comorbid patient population suffering with obesity.
An analysis of data collected on interventional radiology (IR) practice in the UK has shown an increasing trend in the number and complexity of procedures between 2017 and 2021, despite an imbalance in provision and demand of IR services, as well as a “striking” lack of records regarding safety and service-cost data.
In their introduction, researchers led by Mo Hamady (Imperial College London, London, UK) state that demand for IR services has been driven by the evolution of technology and clinical knowledge as well as an expanding range of treatments. However, the Royal College of Radiologists commented that the expansion of IR has not met anticipated rates due to a shortage in consultants, nurse and radiographer support, as well as inpatient and day beds.
“To help improve the future provision of IR services, we need to understand the current demand as well as a shortfall in the resources dedicated to provide 24/7 IR services nationally and regional variations in IR provision,” the authors write. Currently, there is no comprehensive data collection protocol to outline the number and type of IR procedures carried out in the UK, and limited data are available on IR facilities and workforce within National Health Service (NHS) trusts.
To remedy this lack, Hamady et al used the 2000 Freedom of Information Act to obtain data regarding IR procedures carried out in radiology departments only at NHS trusts in England and Wales between 2017 and 2021. This included IR workforce and facility information, number of IR consultants, nurses, trainees, angiographic suites and day-case units; analyses of procedure complexity and frequency by region.
Vascular procedures included those for which the basis of the procedure was mainly endovascular, such as angiogram, angioplasty, vascular stents, embolization, and thrombolysis. Non-vascular procedures included those for which an endovascular approach was not necessary, including ultrasound-guided biopsies and aspirations, nephrostomy, tumour ablation and vertebroplasty.
A total of 1,3400,352 IR procedures were analysed from 116 NHS trusts between 2017 and 2021. Throughout this period, the number of IR procedures increased from 256,592 to 292,030 procedures per year, respectively. A decrease in procedure numbers was observed in 2020—falling to 232,202 in correlation with the COVID-19 pandemic—but rose by 20.5% in 2021.
Over the five-year period, there were significantly more intermediate and complex IR procedures performed. Intermediate procedures were defined as a day or inpatient case of up to one hour using local anaesthetic with or without moderate sedation, the procedure must involve more than one type of equipment with an average cost of up to £500 and post-operative monitoring of at least two hours must be carried out.
Between 2017 to 2021, a total of 423,235 vascular and 917,117 non-vascular procedures were performed across the trusts. In 2021, across 118 trusts, there were a total of 561 IR consultants, 982 IR nurses, and 103 IR trainees. The authors comment that, in this analysis, they confirm the demand and utilisation of IR services has increased despite a “major” shortage in workforce, which no doubt has caused widespread burnout among UK interventional radiologists.
The authors add that a “postcode lottery” became clear in their analysis of IR procedures and number of consultants per region, highlighting the difficulty in maintaining IR services in certain areas of the UK.
“The main way to understand the need to achieve a standard level of IR service provision across the UK, monitor the quality of care and identify areas of cost saving is through a robust and centralised data registry,” the authors state. Previously, there has been “useful but limited” efforts to collected data on IR applications by the British Society of Interventional Radiology (BSIR) inferior vena cava registry and iliac angioplasty and stent registry, Hamady et al state.
Hamady and colleagues assert that a revision of services is needed and should include on-call provision and a broader national registry by the Royal College of Radiologists. They note that their analysis, although a start, was limited by NHS trusts’ limited resource to capture data and the subjectivity of criteria for the complexity of procedures. The research team state that “centralised and harmonised” data collection of IR procedures is key to better understand the scope of IR services, and to better understand pitfalls and assess training opportunities.
Sabine Steiner (University of Leipzig, Leipzig, Germany) took to the podium at this year’s Leipzig Interventional Course (LINC 2024; 28–31 May, Leipzig, Germany) to share, for the first time, two-year data from the BEST SFA randomised controlled trial (RCT) and final, five-year results from the COMPARE study.
BEST SFA
Steiner first revealed the latest findings from BEST SFA. By way of background to the trial, the presenter highlighted a discrepancy between the available evidence—which she noted focuses mainly on single devices and short- and intermediate-length lesions— and the “much more complex” superficial femoral artery (SFA) disease requiring the use of multiple devices that clinicians face on a day-to-day basis.
“The additive value of adjunctive therapy is unclear,” Steiner pointed out. As a result, she and colleagues sought to run an exploratory pilot study comparing strategies rather than single devices in very complex, real-world SFA lesions without restricting the use of adjunctive devices. “Actually,” the presenter highlighted, “we were encouraging the use of these devices for vessel preparation.”
In the investigator-initiated, industry-independent BEST SFA RCT, 120 patients with Rutherford category 2–4 disease were randomised in a 1:1 fashion to either a stent-preferred or a stent-avoiding treatment strategy. Steiner informed the LINC audience that both strategies had to be feasible according to the operator.
With regard to lesion characteristics, Steiner underscored the complex nature of the SFA disease treated in the study. The mean length of the included lesions was 18–19cm and around 80% were chronic total occlusions (CTOs).
At two-year follow-up, Steiner reported a freedom from clinically driven target lesion revascularisation (CD-TLR) rate of 84% in the stent-preferred group and a 78% rate in the stent-avoiding group. There were no major amputations during this time period.
“We had a high bailout stenting rate and high rates of residual stenosis, which might explain a relatively significant loss of patency at two years,” the presenter continued. “However, the freedom from TLR rates are really promising, and we will continue to follow these patients.”
COMPARE
Later in the same session, Steiner shared final, five-year results from the COMPARE study.
“The COMPARE RCT has quite a unique study design,” the presenter began, noting that this was the first head-to-head investigation of two drugcoated balloons: one with a lower dose of paclitaxel (Ranger; Boston Scientific) and another with a higher dose (IN.PACT Admiral; Medtronic).
The study had a non-inferiority design, enrolling 414 patients with femoropopliteal lesions who were stratified for lesion length—up to 10cm, 10–20cm and 20–30cm, with a third of the patient population in each group. The patients were randomised 1:1 to treatment with either the ‘low-dose’ or ‘high-dose’ DCB.
“Non-inferiority was met for both the primary efficacy and safety endpoints,” Steiner informed the LINC audience, recalling data presented at LINC 2020.
Moving on to the new, five-year results, Steiner reported: “We do not see a significant signal for a difference between these balloons and we have a freedom from TLR rate of around 67% for the lowdose group and about 75% for the high-dose group after five years of follow-up.”
Furthermore, Steiner shared that short lesions (up to 10cm) “did very well,” stabilising earlier on with respect to CD-TLR and with a freedom from TLR rate of 80–85% at five years.
The presenter outlined “a similar picture” with lesions of 10–20cm in length, pointing out a stabilisation of reintervention after two years and a freedom from TLR rate of around 66–75% at five years.
With regard to long lesions, Steiner underlined the fact that there were more reinterventions in this group, adding that more than half of these lesions were free from CD-TLR at the five-year time point.
Finally, closing her presentation, Steiner shared that no signal for increased mortality or amputations were seen in either group.
Vesalio announces the US commercialisation of pVasc thrombectomy system for non-surgically removing peripheral occlusions.
A recent press release outlined that pVasc targets the full range of emboli from soft acute clots to fibrin-rich, calcified ones. The company states that their Drop Zone technology traps, retains and securely removes thrombus to restore flow in patients suffering from acute limb ischaemia and other conditions related to peripheral artery disease (PAD).
“Given the complicated health history of patients with acute limb ischaemia, physicians often face the challenge of delivering devices through highly diseased arteries and working in small, stenotic vessels,” noted Frank Arko (Sanger Heart and Vascular Institute, Charlotte, USA). He adds that “pVasc has a low profile and excellent deliverability, making it an especially valuable tool when access is difficult or when working in arteries below the knee.”
“I have achieved highly positive results with pVasc in challenging cases that range from organised emboli in the tibialis, to emboli in the brachial and distal ulnar artery,” said Nick Abedi (Fayette Surgical Associates, Lexington, USA). “pVasc has helped my patients avoid open surgery on multiple occasions, becoming an invaluable tool in my practice.”
pVasc is indicated for arteries from 2–6mm in diameter, typically located below the knee, in the femoropopliteal, the mesenteric, the upper extremities, and a few other locations. Comprised of a self-expanding nitinol structure on a pusher wire, pVasc provides a versatile tool with no need for capital equipment, the company states.
“PAD is a common disease that can lead to devastating consequences. With the pVasc thrombectomy system, physicians now have access to a critical tool to help their patients,” stated Vesalio chief executive officer Steve Rybka. “We received extremely encouraging early feedback on pVasc’s ease of use and efficacy in cases with challenging clots. At Vesalio, we remain steadfast in our commitment to provide innovative technologies to physicians treating vascular occlusions.”
Vascular interventional radiologist Maria Antonella Ruffino (Interventional Radiology, IIMSI, Ente Ospedaliero Cantonale, Lugano, Switzerland) discusses her experience from the “men’s world” of endovascular interventions, sharing insights from her innovative career with Interventional News.
Tracking her experiences from training to be a surgeon, to working alongside pioneers of vascular interventional radiology, Ruffino describes the challenges women have faced and still face, and calls for broader opportunities to be offered to women in the field. She believes: “You can be a good doctor or a bad doctor, but not because you are a man or a woman” and seeks to encourage more individuals to join the specialty.
In 2023, the Society of Interventional Radiology (SIR) Foundation awarded the percutaneous cholangiopancreatoscopy (PCPS) registry the largest grant to date to investigate the use and role of cholangioscopy in the treatment of gallbladder and biliary tree lesions with the goal of removing indwelling drainage catheters quickly, treating biliary stones and diagnosing and treating strictures. Although cholangioscopes are not new and have been used for decades during gastrointestinal interventions and by a small number of interventional radiology (IR) practices, recent advancements in technology have begun to make new of old, drawing scopes to the forefront of a novel era of biliary intervention.
Harjit Singh
“Percutaneous biliary endoscopy has come to the procedural forefront in the past five years,” said Harjit Singh (Johns Hopkins University, Baltimore, USA), lead researcher for the PCPS registry, when speaking to Interventional News. “Prior to that time, only a few large academic centres were performing the procedure.” Since the early 1990s, laparoscopic cholecystectomy has typically been the gold standard for patients with symptomatic gallstones, which involves the surgical removal of a diseased gallbladder. However, when considered in an aging, increasingly comorbid, and so surgically unsuitable patient population, this treatment option is unviable. For these patients, percutaneous drains can be inserted into the gallbladder, but these require regular changing. Cholangioscopy can improve the efficiency of such procedures and the patient’s quality of life (QOL).
Percutaneous cholangioscopy is a minimally invasive procedure used to diagnose and treat conditions affecting the biliary tree and gallbladder. This typically involves the insertion of a flexible endoscope into the biliary system, enabling visualisation of the gallbladder lumen or bile ducts for the removal of stones, to place stents, treat strictures or perform biopsies. When the biliary tree/gallbladder cannot be approached endoscopically, percutaneous access with the placement of a drainage catheter is usually the first step. For choledocholithiasis and cholelithiasis, percutaneous scope-directed lithotripsy with fragment removal is increasingly being used as an effective minimally invasive option.
Although a smattering of medium-sized studies have evaluated the effectiveness of cholangioscopy and eventual tube removal, no large studies have been conducted to date. In 2022, to begin filling these gaps in understanding, Singh led the SIR Foundation research consensus panel, identifying crucial priorities regarding percutaneous image- and cholangioscopy-guided procedures for biliary and gallbladder diseases.
“Bringing together experts who have performed cholangioscopy was critical,” he commented. They identified three key areas of future research: the treatment of benign biliary strictures, the evaluation and treatment of intrahepatic cholangiocarcinoma (IHCC), and cholelithiasis/ choledocholithiasis in patients not suitable for surgery. Based on the response the panel received, Singh and his team determined that a multisite registry would be the best vehicle to collect these data and—with the sponsorship of the SIR Foundation—have enrolled close to 500 patients.
Hugh McGregor
Moving beyond specialised academic centres, Singh stated that percutaneous cholangioscopy’s maturation can be attributed to the technological advancements of recent years. Sharing his experience, Hugh McGregor (University of Washington Medical Center, Seattle, USA) explained that the broader market availability of smaller, disposable scopes “lowered the barrier to entry”, making the procedure more accessible to IR teams. Previously, clinicians would need to buy a reusable endoscopic system or borrow one from another speciality, creating “challenges” for various reasons, he added. “There is definitely a learning curve—it’s a new modality that interventional radiologists don’t typically come across. We’re used to looking at X-rays in real time, not videoscopic images,” McGregor said.
McGregor’s own research has focused on gallbladder cryoablation, having conducted a first-in-human trial in 2020 which found the modality to be a promising alternative to long-term cholecystostomy tube drainage for the treatment of cholecystitis in non-operative patients. “When you look at devitalisation of the gallbladder, there was a lot of work done in the 1970s and 1980s, but there seemed to be a gap in the 1990s into the 2000s, perhaps due to the advent of laparoscopic cholecystectomy becoming the absolute standard, despite still being a fairly morbid operation in some patient groups.”
McGregor noted however that the clinical problem has begun to resurface once more, defined by an aging population with increasingly complex comorbidities. To meet this need, investment in scope technology applied to minimally invasive IR techniques is increasing. “The growth in the number of patients we’re seeing is outpacing the number of doctors we’re gaining, which has driven speciality crossover and collaboration, each coming toward the centre to act as proceduralists,” McGregor said.
Peter Mueller
Peter Mueller (Massachusetts General Hospital, Boston, USA) backed the motion for multidisciplinary collaboration, identifying intensivists, surgeons, interventional radiologists and gastroenterologists as key players in the management of these patients. “Collaboration is extremely important,” Mueller said. “Some people worry about losing their turf, but this is one area that any specialty would be apprehensive to take on. Treatment options for patients with biliary/ gallbladder diseases have little to no long-term data or evidence, but at our hospital we can confidently say that percutaneous cholangiopancreatoscopy to place a drainage catheter is very effective.”
Mueller reiterates that data must be sought, particularly for the sake of patient QOL metrics; “the five-year survival of these patients may not be great, but what about the two-year survival rates—did they get cholecystitis again? Did their stents become clogged?” he said. “In fact, I’m going to go to my old hospital next week and encourage the team to look at this.”
John Smirniotopoulos
“Quality of life is the most underrated metric in IR,” Mueller continued. “It’s all in the decision making, the talking to the family and in the follow-up.” Today, patients are more autonomous during treatment decision-making conversations. John Smirniotopoulos (MedStar Washington Hospital Center, Washington DC, USA) shared that, at his centre, “a new subset” of patients has emerged, self-referring from across the country and internationally for biliary colic secondary stones. In doing so, these patients elect to avoid surgery and undergo organ sparing gallstone removal via percutaneous cholangiscopy.
From a research perspective, Smirniotopoulos stated that the efficacy of such a procedure still needs “bearing out”, and that stone recurrence should also be an area of particular interest. McGregor also touched on recurrence rates, stating that: “increasing the body of literature is going to be important here. If it turns out that 100% of patients will experience stone recurrence at five years, that changes the treatment equation and there may be an argument for a higher-risk cholecystectomy upfront, but we just don’t know yet.”
Primed to bolster or bin scope-directed biliary intervention, Singh et al’s forthcoming registry data are hoped to equip IR with a “whole new set of tools for the diagnosis and treatment of biliary tract disease,” said Singh. “Using what I expect to be proven [via the PCPS registry data], through an adjunctive set of tools, we can accelerate the process of diagnosis and treatment of biliary pathology such as stones, strictures and obstruction.” Singh hopes that subsequently, a “new treatment algorithm” can begin, providing an alternative to the “long, tedious and financially burdensome” treatment algorithms that are available now for these patients and their families currently.
Rendering of HistoSonics treatment head demonstrating histotripsy delivery and targeted destruction of liver tissue
HistoSonics has announced the company’s initial partnership in Asia with Hong Kong University receiving their first histotripsy system following a donation from the Li Ka Shing Foundation.
The foundation, led by its founder Li Ka-shing, is a global philanthropic organisation with a focused effort in Hong Kong, and is responsible to date for over HK$30 billion in projects involving education, medical services, charity, and anti-poverty programmes, a recent press release states.
As part of the foundation’s focus on bringing innovative medical advancements to Hong Kong, the foundation provided the capital to acquire two initial histotripsy systems to the leading public hospitals in Hong Kong, one each to the University of Hong Kong and the Chinese University of Hong Kong. The Chinese University of Hong Kong will receive the second histotripsy system early next year to complete the initial gift from Li.
“We could not be more excited to partner with these two prestigious university hospitals to be the first in Hong Kong to offer our novel therapy to their patients,” said Mike Blue, HistoSonics chief executive officer (CEO) and president.
Histotripsy is a novel form of focused ultrasound that uses high amplitude, very short pulses to create a “bubble cloud” that is designed to mechanically destroy and liquefy targeted liver tumours. These bubble clouds form and collapse in microseconds, creating mechanical forces strong enough to destroy tissue at cellular and sub-cellular levels in a non-invasive and non-thermal method. Histotripsy offers an alternative for patients with liver tumours to avoid certain side effects like surgical site infections, bleeding, and radiation toxicity common to other treatments such as surgery and radiation therapy.
The company believes that the novel mechanism of action of their proprietary technology may provide significant advantages to patients, including the ability of the treatment site to recover and resorb quickly. Li commented that “treating tumours using the HistoSonics histotripsy system by forming microbubbles is fascinating,” and believes medical research and innovation can bring hope and economic prospects to the city.
Experts in liver treatment from the University of Hong Kong and the Chinese University of Hong Kong recently underwent training at HistoSonics headquarters in Minneapolis, USA, and expect to begin treating patients as early as this week. “We could not be more excited to partner with these two prestigious university hospitals to be the first in Hong Kong to offer our novel therapy to their patients,” said Blue. “Unfortunately, Asia carries a substantial proportion of the world’s population suffering from diseases that cause liver tumours and based on the experiences from our US launch we are confident that we can begin to make an immediate impact on the quality of life of many of the patients who need it most in this region. We are very grateful for the foundation’s very generous gift and Li’s personal interest in helping patients in Hong Kong,” added Blue. Both Hong Kong-based hospitals will be eligible to enrol patients in HistoSonics’ prospective study and post market clinical programme, called BOOMBOX, which aims to collect data across a broad number of clinical use cases, and liver tumour pathologies, observing the use of histotripsy across all stages of liver disease.
The Edison histotripsy system is indicated for the non-invasive destruction of liver tumours, including unresectable liver tumours, using a non-thermal, mechanical process of focused ultrasound.
The Auryon atherectomy system uses solid-state laser technology to treat PAD lesions and occlusions. A press release notes that Auryon is the first laser atherectomy system to efficiently treat lesions of any type, length, or location (above and below the knee), with minimal impact on vessel walls.
“The CE mark approval of the Auryon system is a significant milestone that underscores our commitment to bringing safe and effective solutions to healthcare professionals treating peripheral arterial disease,” said Laura Piccinini, AngioDynamics senior vice president and general manager of endovascular therapies and international. “This approval validates the clinical value of the Auryon system and allows us to expand our presence in Europe, as the prevalence of PAD continues to grow across the region. We are committed to supporting physicians with innovative technologies that empower them to deliver the best possible care when treating some of the most challenging cases of this disease.”
AngioDynamics states that the Auryon atherectomy system, which received US Food and Drug Administration (FDA) 510(k) clearance in 2020, has treated over 50,000 patients in the USA. The recent CE mark approval now provides patients with PAD in the European Union access to the Auryon system’s laser platform.
The technology underlying the Auryon atherectomy system has been shown in clinical studies to be effective in treating lesions ranging from soft plaque to severely calcified, a press release reports. The system uses a 355nm wavelength laser platform, enabling the use of short UV laser pulses with targeted biological reactions that are effective in treating PAD while minimising the risk of perforation and preserving the ability to vaporise lesions without thermal ablation.
The press release continues that the Auryon atherectomy system features aspiration and off-set capability in certain catheter sizes, allowing clinicians to address the risk of embolisation and to treat all lesion types, while answering a need for non-surgical intervention options for PAD, including ISR, and CLTI.
Nicolas Shammas and the Midwest Cardiovascular Research Foundation (Davenport, USA) have published a prospective, multicentre, single-arm investigation examining the use of the Auryon laser system in patients with below-the-knee CLTI. The study demonstrated that the Auryon laser system effectively reduced residual stenosis to ≤30% in the majority of patients post-treatment, without any cases of target lesion revascularisation.
The recently published PATHFINDER registry further supports these findings, showing no flow-limiting dissections and significant improvement in ankle-brachial index (ABI), Rutherford classification, and Walking Impairment Questionnaires at both six and 12 months in a real-world clinical setting.
These results add to a growing body of evidence indicating that the Auryon laser system is a safe and effective treatment option for a wide range of complex patients with PAD.
Matteo Tozzi (Varese, Italy) recently spoke to Vascular News about the role of drug-coated balloons (DCBs) in vascular access.
The full professor of vascular surgery at the University of Insubria started the use of Aperto® OTW DCB by Cardionovum® in his vascular access practice over 10 years ago and will publish his experience with more than 600 DCBs.
While the efficacy of DCBs has been proven to be superior to that of plain balloon angioplasty for these patients, there is limited data on their economic benefit. To rectify this, Tozzi noted that he has started a collaboration that aims to assess the cost benefit of DCBs in the vascular access failure population using the data coming from his study named Aperto 600. He described the preliminary results from this as “incredible”.
Tozzi concluded that, in his opinion, DCBs should now be viewed as a “first-line” treatment for stenosis and vascular access failure in haemodialysis patients.
Sonio has today announced the official approval by the French Ministry of the Economy and Finance of the complete acquisition of shares by Samsung.
The deal closes following the company’s second wave of US Food and Drug Administration (FDA) clearance in 2024 and with Sonio reporting and workflow solution operating in multiple sites across the USA.
“Alongside Samsung Medison, we are excited to make significant strides in the maternal care industry. In addition, Sonio plans to continue to advance medical reporting technology and diagnostic software globally, including for underserved areas in healthcare” says Cecile Brosset, chief executive officer (CEO) and co-founder of Sonio.
Established in 2020, Sonio has developed a reporting and workflow solution powered by artificial intelligence (AI) for obstetrics and gynaecology ultrasound that assists clinicians in the evaluation and documentation of ultrasound exams.
Samsung Medison CEO Kyu Tae Yoo said: “With the workforce shortages affecting the global healthcare industry, the real-time ultrasound exam guidance and quality assurance developed by Sonio is becoming more relevant to ensure high quality care. We look forward to combining Sonio’s and Samsung’s advanced engineering to enhance our ultrasound roadmap and introduce next generation AI technologies to the market. We will focus on innovations designed to enhance exam quality, efficiency, and ultimately improve patient care.”
“We are committed to support all healthcare providers and patients as we pursue our mission of providing equal access to high-end technology and quality maternal healthcare globally,” commented Brosset.
Updating on a previous meta-analysis, new data which pooled survival estimates of patients undergoing transarterial radioembolization (TARE) has shown the treatment to be a valid option for unresectable intrahepatic cholangiocarcinoma (ICCA), particularly if the patient is naïve to previous treatments. These results were recently published in the journal Cardiovascular and Interventional Radiology (CVIR).
Lead researchers Maria Adriana Cocozza and Elton Dajti (both IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy) note that this update was based on a prior 2017 meta-analysis from the same study group which included nine studies, and revealed encouraging results for ICCA patients undergoing TARE. This preliminary evaluation identified one, two and three-year survival rates to be 55.7%, 33.1% and 20.2%, respectively.
The authors note that, although the results were promising, studies have since emerged which have bolstered these findings—notably, Julien Edeline (Centre Eugène Marquis, Rennes, France) et al’s 2020 trial on the combined benefit of TARE plus chemotherapy in unresectable ICCA. Despite these compelling data, Cocozza and Braccischi observe that the role of locoregional therapies in the guidelines remains “unclear” and recommendations for their use are weak, as emphasised by the 2023 European Association for the Study of the Liver (EASL) update.
To provide a “benchmark” for survival rates following treatment with TARE for patients with ICCA, the authors identified 27 studies which included 1,365 patients. The mean patient age in this cohort was 64 years and 49% of patients were male. Concerning tumour characteristics, 48% of tumours were bilobar and 54% of tumours were multifocal. Extrahepatic disease—mainly consisting of lymph node metastases—presented in 36% of patients. Importantly, the rate of patients who were naïve to previous treatment was 25%, while 49% received concomitant chemotherapy.
The main result was that at one-, two- and three-year intervals, survival estimates were identified as 53%, 27% and 17%, respectively, with a mean survival of 15.8 months following TARE, and 24 months after diagnosis. As heterogeneity was high between the included studies, the authors conducted a meta-regression analyses of study and patient characteristics.
The authors identified that previous treatment naiveté was the “sole pre-treatment determinant of survival”, stating that the predicted one-, two- and three-year survival rates were 70%, 45%, and 36% in treatment-naïve patients, and 44%, 18%, and 7% in patients who had received previous treatments. The mean survival for treatment-naïve ICCA patients was 19.7 months and 12.2 months for non-naïve patients.
Further, in a secondary evaluation, the authors observed tumour response through computed tomography (CT) and magnetic resonance imaging (MRI) according to RECIST 1.1 and modified RECIST (mRECIST) in 20 and four studies respectively.
The proportion of patients who achieved objective response according to RECIST 1.1 criteria was 19.6% and were associated with improved one-year survival at meta-regression analysis. In responders, the precited one-, two- and three-year survival rates were 83%, 51%, and 37% respectively, and mean survival was 23.8 months. In non-responders, these rates fell to 43%, 18%, and 8% and the precited mean survival was 11.6 months.
According to mRECIST criteria, the summary proportion of patients that achieved objective tumour response was 67%, and this was associated with a one-year increase in survival. The precited one-, two- and three-year survival rates in responders was observed as 81%, 63%, and 57%, with a mean survival of 20.1 months. Survival rates for non-responders was identified as 16%, 0%, and 0%, with a mean survival of 4.8 months.
The authors also calculated the rate of successful downstaging to surgery which was 0% in many studies, but this figure ranged between 3% and 54% in other series. However, they state that at meta-regression analysis, the increasing proportion of patients who were successfully downstaged to surgery positively correlated with increased survival, with a predicted mean survival of 34.8 months.
The authors comment that TARE shows promise as a “transformative” treatment for ICCA, potentially downstaging tumours to enable resection and increase survival. However, the success of downstaging varies significantly in their analysis, due to the high heterogeneity among the baseline clinical and tumoral features in the included studies.
“This [heterogeneity] likely mirrors the inherent diversity within the group of patients subjected to various previous treatments, encompassing surgical interventions, locoregional therapies, and the number of failed chemotherapy lines, among other factors,” the authors write. Ultimately, this diversity poses a challenge when interpreting the long-term outcomes of TARE across studies, limiting the likelihood of their uptake in the current guidelines. To this, the authors state that further research must refine patient categorisation to address these limitations, but they maintain that their present analysis provides “new possibilities” for managing inoperable ICCA.
Left to right: Michael Kostrzewa and Rashid Akhtar
Evaluating the current standard of care for the management of acute pulmonary embolism (PE) and deep vein thrombosis (DVT), Michael Kostrzewa (Cantonal Hospital Baden, Baden, Switzerland) and Rashid Akhtar (Barts Health NHS Trust, London, UK) discuss the efficacy of mechanical thrombectomy and its expanding application.
Until today, mortality rates for PE remain unacceptably high, sitting between 6–15% for intermediate-high risk and 25–50% in high-risk patients. A similar trend can be observed in patients with DVT, where residual thrombus after treatment can cause long-term issues, with approximately 50% of patients developing post-thrombotic syndrome (PTS) as a result. Standard treatment for PE has typically involved thrombolysis, and for DVT, anticoagulation. However, via technological advances, a better understanding of the importance of new predictors in choosing the right treatment option, and the availability of new tools have begun to shift the focus towards interventional management.
“There are several reasons why we are increasingly intervening on PE and DVT. We have previously never been able to fully extract the clot and characterise its type, l et alone describe the efficacy of tissue plasminogen activator (tPA) on collagen-rich thrombus. Would that clot have been completely dissolved?” Akhtar said. “With the updated toolkits that are now available, such as the FlowTriever® or ClotTriever® systems (Inari Medical) for venous thrombectomy in PE and DVT respectively, it makes treatment more approachable,” Kostrzewa added. In his opinion, these technologies, paired with the positive clinical data and growing evidence, provide treating physicians with the necessary confidence of a reliable and predictable outcome.
ClotTriever: for wall to-wall mechanical thrombectomyFlowTriever: designed for lytic-free thrombectomy
At present, data from the FLASH and FLAME registries—which collected data on the use of mechanical thrombectomy with the FlowTriever system for the treatment of acute PE—have shown low rates of all-cause mortality at 30-day follow-up and significantly lower rates of in-hospital adverse events. Similarly in the treatment of DVT with the ClotTriever system, the CLOUT registry shows safety and effectiveness of wall-to-wall thrombus removal, with 93% of patients having no or mild symptoms of post-thrombotic syndrome (PTS) symptoms at two years.
“There’s still a lot to be done,” Kostrzewa said, “but we have good evidence at present and there is very exciting data to come, with the DEFIANCE trial for DVT and the PEERLESS II trial for intermediate-high risk PE patients, as it is often difficult to decide between conservative or interventional treatment. These results will hopefully bring clarity and change the guidelines.”
Touching on the current guidelines and changing the status quo, Kostrzewa believes that awareness is a prevailing issue, which, in his experience, has prevented him and his colleagues from using new and more effective treatment strategies, and has led to a reduced influence on guidelines. “We need to build awareness to change guidelines,” he said, “but I do believe that awareness is changing in the venous thromboembolism [VTE] space, both among the treaters and the non-interventional stakeholders [NISH]. It is all about building an effective and efficient team.”
In Akhtar’s experience, the frequency of mechanical thrombectomy procedures he performs is increasing. “We are in a unique era with the right devices and evolving guidelines, and we are no longer ignoring the mortality figures for PE patients or the prolonged complications that DVT patients face.” Importantly, updates to the European Society of Cardiology (ESC) Guidelines for the diagnosis and management of acute pulmonary embolism from 2019 on mechanical thrombectomy were “a step in the right direction” for Akhtar, helping his team to better assess patients and decide on an informed treatment pathway.
In his institution, he explains, admitted patients are typically administered low molecular weight heparin. Treatment is escalated towards intervention, if the patient shows signs of deterioration within 24–48 hours. They consider factors such as the ratio between right and left ventricle (RV/LV ratio), lactate levels, clot burden and concomitant DVT—all these parameters are essential in their interdisciplinary case discussions and the decision-making process, also known as PE response team (PERT) meetings.
“In the treatment of PE and DVT treatment, interventional radiologists can take the clinical lead, because we see many of these patients and are experts in this field,” Akhtar said. “In my practice, I review patients pre- and post-intervention. You’re getting a DVT procedure with ClotTriever device done within the hour, which is swift and not tedious.” By integrating devices such as the FlowTriever into clinical practice, interventionalists can improve procedural efficiency, Akhtar explained: “It’s useful for interventionalists to do both DVT and PE treatments—I often use the FlowTriever device in DVT interventions. I encourage offering both PE and DVT treatment, as the procedures are straightforward for experienced interventional radiologists. Plus, it’s rewarding. I find that both PE and DVT interventions have renewed my job satisfaction,” he shared.
Kostrzewa points out that the lack of clear guidelines in DVT is a major challenge for referring physicians, as it is not always easy to differentiate between patients who will benefit from interventional treatment and those for whom it is not indicated. “As clinicians, we now have a better understanding of both conditions and what can happen with these patients in the long term. We also have better tools for PE and DVT to safely and efficiently remove thrombus in the lungs and lower extremities,” he states. “Still, we rely on referring physicians to ensure that all VTE patients who are eligible for mechanical thrombectomy, receive this treatment.”.
In Akhtar’s view, a multidisciplinary approach is key to provide PE and DVT patients with optimal care, as interventional techniques such as mechanical thrombectomy shift to become commonplace. Akhtar and Kostrzewa agree mechanical thrombectomy is a game changer in the minimally invasive treatment of PE and DVT, rapidly restoring blood flow and reducing associated risks. Advances in technology, along with further studies, is expected to establish mechanical thrombectomy as a key tool in the management of venous thromboembolic disease, which is expected to be reflected in the future guidelines for the treatment of PE and DVT.
At this year’s Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14–18 September, Lisbon, Portugal) Inari Medical will be hosting a hands-on workshop on Saturday 14 September, demonstrating the FlowTriever and ClotTriever systems. In addition— on Sunday 15 September—an expert panel will be exploring the impact of mechanical thrombectomy in the management of venous thromboembolism at the 1pm Symposium in Auditorium 2.
The CLEANER Rotational Thrombectomy system (Argon Medical) used for arteriovenous fistula and grafts seeks to provide interventionalists with an all-in-one tool to treat a range of percutaneous thrombectomy cases. This is according to general surgeon Jason Beaver (Surgery Center South, Dothan, USA) and interventional radiologist Amr Elsaadany (Barts Health NHS Trust, London, UK), who discuss their experiences macerating organised or difficult-to-access thrombus with the device.
The CLEANER device is indicated for the mechanical declotting of native vessel dialysis fistulae, synthetic dialysis access grafts, and peripheral vasculature. Additionally, the device can be used for controlled and selective infusion of physician-specified fluids in the peripheral vasculature. It works via a self-sizing sinusoidal wire that rotates at 4,000 rpm, breaking apart wall-adherent thrombus. This design creates a fluid vortex that forces clot burden to macerate into small particles without causing endothelial damage and has had proven success in patients with pseudoaneurysms and stents .
Procedurally, Elsaadany notes that one of the most “challenging” elements of native AV fistula treatment is the tortuosity of the vessel—especially with long-standing fistulas with aneurysmal dilatation. He adds that challenges also arise due to pseudoaneurysms, as these can often contain thrombi of different ages, from acute to sub-acute and chronic.
“That’s why you need a powerful machine. I usually perform the entire procedure under ultrasound, and, using the CLEANER device, you can massage or compress the rotational wire against the vessel wall,” Elsaadany says. “With its adaptive function, you can ensure that you are going from wall to wall, taking the entire thrombus.”
Cleaner 15
For Beaver, the adaptability of the system is a key benefit. He believes CLEANER’s self-sizing ability is invaluable when macerating thrombus from a native fistula. Eliminating this thrombus can be challenging, as an inflammatory response can be triggered when the vein clots, creating a more organised, rubbery, defined clot. With the CLEANER device, labelling it the ‘Keep it Cleaner’ system, Beaver asserts that the “appropriately aggressive” rotational function allows for safe and effective thrombus maceration in the first instance. “With other devices, the fistula can often re-clot sooner,” he says.
“The CLEANER device helps you get a large percentage of the clot out quickly, re-establishing flow,” Beaver adds. In doing so, he has seen fewer patients needing a secondary thrombectomy two or three days following the initial procedure. This, he believes, is the effect of the CLEANER device, which provides “more comprehensive clot clearance from the access.”
Continuing, Elsaadany and Beaver agree that macerating clot efficiently minimises procedural time. “Having used several mechanical thrombectomy devices,” Elsaadany states, “the CLEANER device has provided the most efficiency. Graft cases should not take more than 20–30 minutes. Having a patient in your angio suite for over an hour will restrict the number of patients you can treat daily. The CLEANER device, in my experience, provides a higher level of efficiency.”
Particularly in dialysis patients, Beaver notes that streamlining procedures with the CLEANER system is important to minimise time “on the table” and decrease the disruption to the patient’s regularly scheduled treatment and their daily lives. “The device helps to improve procedure times,” he says. “I’m big on not keeping these dialysis patients on the table longer than they need to be, and I can usually do a straightforward declot in around 10–15 minutes. Efficiency-wise, the CLEANER device helps tremendously.”
Selecting patients for mechanical thrombectomy can be complex. Beaver points out, “Often we are working with a patient population that is very frail, with several comorbidities.” For this reason, complication rates are paramount when selecting a device. For difficult cases, such as those involving large, dilated fistulas, Beaver explains that he first injects alteplase to dissolve some of the clot before using the CLEANER device to ensure a more successful outcome.
Elsaadany agrees that careful patient selection is necessary when planning a mechanical thrombectomy. He details that, when using a thrombolytic agent, the three-way infusion port of the CLEANER device effectively delivers the injection to the patient. Alternatively, Elsaadany highlights his recent experience using the device without a thrombolytic agent in cases where it may be risky, noting that these procedures have been successful.
“Before choosing the most appropriate equipment for a procedure and patient, you will ask yourself— which tool has the potential to cause the fewest complications?” Elsaadany says. In his experience, the CLEANER device has reduced side-effects in his patients undergoing thrombectomy, mainly due to its “atraumatic” tip and rotational wire. “There’s no risk for any perforation or injury to the vessel wall as it macerates the thrombus into minute parts, which also means there is little to no concern about pulmonary embolism [PE],” Elsaadany states.
Citing the risk of PE, Beaver underlines the importance of macerating the entire clot while reducing procedure time to improve patient outcomes. He states this can be helped by combining visualisation techniques with the CLEANER device during thrombectomy procedures. The system’s compatibility with the latest imaging and fluoroscopy technology allows visualisation of the thrombus and surrounding vasculature in real time to ensure interventionalists can make informed decisions and monitor the procedure’s progress. “If you’re de-clotting an access in which you aren’t sure which side is the venous and which is the arterial,” he details, “you can go across with the CLEANER device, inject some contrast and figure out which side you are on—that’s a nice bonus.”
Summing up, Elsaadany reflects that: “The dialysis fistula is the lifeline of chronic kidney disease patients. We need equipment that is fast, efficient, and powerful and that reduces clot recurrence rates which I have seen with the CLEANER device.” To this, Beaver agrees, noting that since moving to CLEANER, he has provided safer and more effective treatment, seeing fewer patients returning re-clotted for a repeat procedure. Using CLEANER for a “multitude” of thrombectomy cases, Beaver attests to the device’s “versatility across a spectrum of indications” and ability to optimise mechanical thrombectomy procedures for the benefit of patients and physicians.
References:
Vega, F. Safety Comparison of Cleaner™ Rotational Thrombectomy System Versus Arrow PTDTM in Native Vessel. San Carlos, CA: Isis Services, LLC; 2010.
Webb A, Zacharias K, et al. Dialysis Shunt Thrombectomy Utilizing a Rotational Thrombectomy Device in Patients with Pseudoaneurysms. The Arab Journal of Interventional Radiology. 2020;4(02):87-91. https://doi. org/10.1055/s-0041-1729018).https://doi.org/10.1055/s-0041-1729018).
This advertorial is sponsored by Sirtex Medical,is only available in selected countries and geographies.
Macarena Rodríguez-Fraile and Irene Bargellini
The SUMM90YT conference (23 February, Frankfurt, Germany)—hosted by Sirtex—gathered leading experts in selective internal radiation therapy (SIRT) utilising SIR-Spheres Y-90 resin microspheres (Sirtex Medical). The conference facilitated discussion and debate on the appropriate selection of patients with unresectable hepatocellular carcinoma (HCC) and metastatic liver tumours from primary colorectal cancer (mCRC) refractory to or intolerant of chemotherapy, as well as the latest technical advancements in the field.
Organised into three distinct sessions— SIRT in HCC, SIRT in mCRC, and key technical considerations—the SUMM90YT programme fostered dialogue through a modelled multidisciplinary tumour board. Speaking to Interventional News, moderator Macarena Rodríguez-Fraile, nuclear medicine physician (Clínica Universidad de Navarra, Pamplona, Spain) and speaker Irene Bargellini, interventional radiologist (Cuneo Hospital, Cuneo, Italy) reflect on their key takeaways from the conference.
The day’s first session was dedicated to HCC, as speakers including surgeon Claire Goumard (University Hospital Pitié Salpêtrière, Paris, France), surgeon Pietro Addeo (Hôpital de Hautepierre, Strasbourg, France), radiation oncologist Maria Hawkins (University College Hospital, London, UK), Bargellini herself, and others, described what is known to date regarding research and treatment options. Predominantly, speakers used patient cases to illustrate the use of SIRT for bridging or downstaging to transplantation and downsizing to resection, inducing contralateral hypertrophy, and explored the potential of combining SIRT with systemic therapies.
In this segment, Bargellini presented on the applicability of SIRT for intermediate to advanced stage HCC. “Thanks to the refinement of indications and the development of personalised dosimetry, SIRT has become a highly appealing and potentially curative treatment across all stages of the Barcelona Clinic Liver Cancer (BCLC) staging system for HCC, evidence showing most benefits in early-stage HCC, in patients with single lesions, to the advanced stage, in patients with portal vein tumour thrombosis,” she told Interventional News. Bargellini added that the speakers in the morning session suitably described the “value in downsizing tumours with SIRT or to induce contralateral hypertrophy—which is now fully demonstrated—making it a valid tool to convert patients to surgery”.
In agreement with Bargellini, Rodríguez-Fraile detailed the “progressive expansion” of SIRT from advanced HCC to earlier stages, through its potential to reclassify disease status. “Growing evidence of the benefits of using SIRT as a facilitator of surgery were shown during SUMM90YT. This was either to reduce tumour size for resection or to bridge/downstage for liver transplant, allowing for surgery that was initially inadvisable. SIRT can also be performed to increase the future liver remnant evaluating the biology of the tumour through the “test of time”, she said.
“Numerous trials and recent prospective registries from the USA and Europe—namely, RESiN (Radiation-emitting SIR-Speres in non-resectable liver tumor) and CIRT (CIRSE registry for SIR-Spheres therapy)—have demonstrated the safety and efficacy of SIRT with Y-90 resin microspheres in HCC patients,” Rodríguez-Fraile conveyed. “Speakers looked at the real-world evidence gained in these registries and concluded that SIRT is a safe and effective bridging therapy.”
Clinical characteristics must define multidisciplinary decision-making
In the programme segment which followed, speakers including medical oncologist Elena Elez (Vall d’Hebron University Hospital, Barcelona, Spain), interventional radiologist Franco Orsi (European Institute of Oncology, Milan, Italy) and surgeon Simeon Ruiter (University Medical Center Groningen, Groningen, The Netherlands), among others, introduced SIRT for chemo-intolerant or -refractory mCRC patients.
Here, the multidisciplinary panel and audience-member participants concluded that SIRT “can have a role” in controlling mCRC in advanced settings, Rodríguez-Fraile explained, as SIRT can be used to enable surgery through contralateral hypertrophy induction or by applying radiation segmentectomy. “Consensus was made that SIRT can be used to maximise metastases control to improve progression-free survival and overall survival, as well as for chemotherapy breaks, and chemo-intolerant patients,” she said.
“Although we still need better designed and well-conducted clinical trials,” Bargellini said, “there is clear evidence that SIRT is safe and effective for mCRC and should be a part of our armamentarium, and that came across at SUMM90YT.” Expanding on this conclusion, she detailed how speakers in this session exemplified how radiation segmentectomy is able to induce a “complete and durable” response in patients who are unfit for surgery or excluded from ablation, and further, how radiation lobectomy may play a role as a conversion strategy in unresectable patients.
Overall, Bargellini stated that to be “actively integrated” into the modern therapeutic landscape for mCRC, “adequate patient selection needs to be mandatory to avoid unwanted toxicities and futile treatments”. In Rodríguez-Fraile’s recollection, this was a central takeaway of the session, the multidisciplinary panel placing emphasis on decerning clinical characteristics when selecting appropriate patients for treatment. She emphasised however, that patient selection can be optimised through tailored profiles A, B and C. Patients in these profile groups she described as: chemo-intolerant with desire for more quality of life (QoL) (A), chemo-refractory, but willing to undergo treatment (B), and aggressive liver-dominant disease with poor prognosis (C).
Summarising the panel’s thoughts, Rodríguez-Fraile noted that patient and tumour features—including tumour biology, personalised dosimetry and patient preference—should be considered above all when considering SIRT for mCRC.
Technical advancements in personalised dosimetry
In the final session of the day, speakers including nuclear medicine physician Michael Kreißl (Universitätsklinikum Magdeburg, Magdeburg, Germany), interventional radiologist Manuel González-Leyte Hospital General Universitario Gregorio Marañon, Madrid, Spain), and interventional radiologist Roberto Iezzi (Policlinico Universitario Fondazione Agostino Gemelli, Rome, Italy) provided various insights into the technical facets of SIRT, offering practical guidance on optimal usage strategies.
Rodríguez-Fraile recalled how prominent focus was placed on dosimetry and microsphere distribution. She explained that microsphere distribution is not only related to blood flow and parameters that the interventional radiologist has control over, such as injection velocity, or type of catheter used, but also to the number of microspheres injected and the specific activity per sphere.
“It has been demonstrated that microsphere distribution has a direct impact on dosimetry such as radiobiological effect, e.g. toxicity and efficacy,” she said. To achieve this flexibility, Rodríguez-Fraile noted that the FLEXdose Delivery programme by Sirtex enables modulation of microsphere properties (number of microspheres and specific activity per sphere) and can facilitate tailored, patient-specific treatments.
“Depending on the goal of the treatment, the volume of the liver to be treated, and the tumoral characteristics (vascularity, size, volume), it is possible to use a different day of calibration vials to maximise the effect. For example, for the same prescribed activity, as the precalibration day increases, the activity per sphere is greater and the number of spheres to be injected will be smaller. This type of vial can be especially useful in selective treatments, as it reduces the risk of reflux and allows greater activity to be administered,” Rodríguez-Fraile explained.
The importance of the work-up phase to precisely plan each treatment was foregrounded at during the session, Bargellini noted. “Today, we know that personalised dosimetry, based on tumour type, extension and treatment goal, is key to achieve high local control and reduce hepatotoxicity.”
“Discussion at SUMM90YT called for a standardised and streamlined workflow, which has been seen through the flexibility of SIR-Spheres in sparing time by exploiting the potential of single-day or single-stay procedures, while better tailoring our treatments to each patients’ clinical and anatomical conditions.”
Processing points given throughout SUMM90YT, Rodríguez-Fraile believes the future of SIRT will be defined by personalisation, combining optimal clinically informed selection of patients with targeted dosimetry-driven treatments. For Bargellini, a central takeaway for the future was the “strong potential synergistic effect” between SIRT and immunotherapy, the integration of which will be better understood via the results of ongoing studies, she states.
As these promising applications develop through research, Bargellini believes that implementation of a standardised treatment protocol for SIRT is required to reach landmarks in its use, to increase safety and efficacy, and to broaden the number of centres that have access to this technology.
“For us, the main clinical objective is accuracy. Precision is key for interventional radiology [IR] procedures,” said Lambros Tselikas** (Gustave Roussy, Villejuif, France), who discussed how he and his team have leveraged cone-beam computed tomography (CBCT)-guided navigation to elevate their procedural efficiency.
CBCT-guided percutaneous procedures have gained prominence over the last decade across interventional oncology, radiology and pain management. Real-time CBCT imaging is used to guide the insertion of needles and other instruments to target specific regions of the body, with applications ranging from biopsies and drainages, to the delivery of treatments such as cryoablation.
In Lambros’s practice, procedures that involve the placement of a needle tend to be more technically challenging, more specifically when the needle trajectory is angulated and deep, which is increasingly the case for bone procedures. Most commonly, Lambros and his team perform diagnostic and therapeutic interventions using the Alia IGS 7(1) for augmented imaging, in combination with the Imactis Navigation system—both developed by GE HealthCare—to plan and navigate the patient’s anatomy during percutaneous procedures.
One of the key benefits of CBCT-guided procedures is their ability to provide detailed, cross-sectional images of internal structures. This capability allows for precise navigation to the area of interest, reducing the risk of complications and improving overall procedural outcomes.
The Imactis Navigation system collects detailed CBCT images to create a virtual, three-dimensional model of the patient’s anatomy. The system uses electromagnetic navigation to increase the accuracy of procedures ensuring that clinicians can navigate complex anatomies while avoiding critical structures and organs.
“What I find interesting when using the Imactis system with the addition of CBCT is, due to the wide bore, you can very easily jump from one modality to another,” he detailed. In practice, Lambros is able to plan the trajectory of the needle on the initial CBCT scan while the patient’s arms are down, and then precisely choose the entry point using Imactis. This way, Lambros and his team can view the virtual anatomical mapping alongside the real-time control images to proceed with absolute confidence.
“We know based on our clinical experience that a good entry point can really make the difference, especially for a tricky case—with Imactis, this is a huge advantage,” Lambros said. “Then, following the needle insertion, we can continue using our advanced guidance tools such a Needle ASSIST(2) (GE HealthCare) which can help to reduce dose and increase the number of patients we can treat. The key benefit of using Imactis Navigation for CBCT with the GE HealthCare Angio system, is to bring together complementary navigation and guidance tools in an easy-to-use, versatile manner, to make difficult cases easy.”
Although centres today seek to offer the highest-quality treatment to their patients, investment in new technologies can appear unattainable due to cost-efficiency and time to installation. GE HealthCare interventional chief executive officer Arnaud Marie told Interventional News hat he heeded this challenge, and explained that their vision for Imactis was to be able to “integrate with already available CT-scanners and innovations emerging from start-ups, academics and other large companies, so we can leverage our ecosystem to seamlessly provide the best-in-class solution”. With this ethos in mind, Marie explained how GE HealthCare has collaborated with companies such as Centerline Biomedical—a provider of X-ray navigation technology—to help to bring beneficial solutions to market.
To Marie, IR is a dynamic field defined by exponential growth in clinical advancement, exemplifying this through the development of genicular artery embolization (GAE) and musculoskeletal (MSK) interventions. In response to these leaps, new navigation software using X-ray and electromagnetic energy, as well as robotic elements has rapidly evolved.
“My vision is that there will be a convergence of technologies to provide integrated systems that will enable delivery of these procedures in a much more predictive, democratised and safer way for both for the patient and the interventionalist through reducing exposure to radiation.”
Marie shared that their intent is to initiate a “strong step toward automisation”, using the Imactis CT-Navigation system in collaboration with “several” companies who specialise in robotics. He believes that “lighter, portable and flexible” robotic technology can achieve improved needle placement in combination with GE HealthCare’s navigation software, producing an all-in-one solution.
While maintaining quality of care, Imactis CT-Navigation is aimed to give interventional radiologists better control over patient care. As minimally invasive procedures become more frequently used for a wider range of patient cases, Marie believes this technology can provide confidence of care, making complex procedures accessible to more clinicians while maintaining quality of care.
In early 2023, GE HealthCare acquired Imactis—a France-based company developing ergonomic stereotactic needle guidance through CT-navigation and CBCT-navigation—which the company states is a part of a broader strategy to improve the workflow of interventional radiologists and become standard of care. The Imactis CT-Navigation system, which includes an integrated workstation, guidance software, and disposable procedure kit, is currently approved under the European Union’s Medical Devices Regulation (MDR).
Disclaimer:
*IMACTIS CT-Navigation is CE Marked and US Food and Drug Administration (FDA) approved. IMACTIS CBCT-Navigation is CE Marked but not yet FDA approved and is not available for sale in the USA. IMACTIS Navigation may not be available in all countries. Refer to your sales representative for more information.
**Tselikas Lambros is a paid consultant for GE HealthCare and was compensated for participation in this article. The statements by Lambros described here are based on his own opinions and on results that were achieved in his unique setting. Since there is no “typical” hospital and many variables exist, i.e. hospital size, case mix, etc. there can be no guarantee that other customers will achieve the same results.
IGS 7 refers to Discovery IGS 7 and Allia IGS 7 system.
Needle ASSIST solution includes TrackVision 2, stereo 3D and requires AW workstation with Volume Viewer, Volume Viewer Innova. These applications are sold separately.
Social support is thought to bolster cardiovascular health by facilitating health-promoting behaviours and acting as a buffer against the impacts of stress on the heart. A team led by Santiago Callegari of the Yale Department of Internal Medicine (Yale University, New Haven, USA) used questionnaires to assess perceived social support (ENRICHD Social Support Inventory), PAD-specific health status (Peripheral Artery Disease Questionnaire), and general health status (EuroQOL Visual Analog Scale) for 949 patients at baseline and 12 months later.
For the 18.2% of respondents reporting low social support, researchers found scores more than seven points lower on average on both the Peripheral Artery Disease Questionnaire and the EuroQOL Visual Analog Scale, indicating significantly poorer outcomes in PAD-specific and general health metrics. The association between low social support and poorer outcomes remained strong even when adjusting for factors including stress, depression, and socioeconomic status.
The research team says their work highlights the importance of psychosocial factors, like social support and depression, in the treatment of cardiovascular disease. “The focus has been on specific devices to open blockages or do bypasses,” says corresponding author Carlos Mena-Hurtado, associate professor of medicine (cardiology) at Yale. “This study shows that it is time to see patients with PAD in a multidimensional way, such that a multidisciplinary team needs to get involved in their management.”
The European Society of Cardiology (ESC) has today published its 2024 guidelines for the management of peripheral arterial and aortic diseases (PAAD), evaluating these vascular conditions together as part of the same cardiovascular system.
The guidelines are aimed at cardiologists, but were coordinated for alignment with guidelines for surgeons by the European Association for Cardio-Thoracic Surgery (EACTS) and endorsed by the European Reference Network on Rare Multisystemic Vascular Diseases (VASCERN) and the European Society of Vascular Medicine (ESVM).
“These updated guidelines have been introduced now due to significant advancements and shifts in our understanding and management of aortic and peripheral arterial diseases (PAD), including new treatment modalities, since the last guidelines were published in 2014 and 2017, respectively,” says ESC guidelines co-chair Jose Fernando Rodriguez Palomares (University Hospital Vall d’Hebron, Barcelona, Spain).
“The decision to integrate these guidelines is based on several key factors. The aorta and peripheral arteries are integral components of the same arterial system. Disorders in one part of this system often have implications for the other,” adds co-chair Lucia Mazzolai (Lausanne University Hospital, Lausanne, Switzerland. “Combining the guidelines provides consistent and standardised recommendations for the management of arterial diseases as a whole. This ensures that patients receive cohesive and coordinated care across different vascular conditions, reducing fragmentation and improving overall treatment outcomes.”
An ESC press release notes that PAAD is estimated to affect around 113 million people aged 40 and over globally, of whom nearly half (43%) are in low- and middle-income countries. The global prevalence is 1.5% and increases with age, affecting 15–20% of those aged 70 years and over and 20–30% of those aged 80 years and older. Prevalence increased by 72% from 1990 to 2019, despite the global population growing only 45%.
The authors say the most important recommendations in the new 2024 guidelines are those addressing the chronic nature of PAAD, the importance of screening, and the necessity of comprehensive treatment strategies—and awareness that this a chronic disease that needs lifetime follow-up.
“A significant proportion of patients are asymptomatic and therefore PAAD screening is crucial, based on age, the presence of cardiovascular risk factors, family history and/or presence of syndromic features. PAAD diagnosis can be easily achieved with a non-interventional vascular test/imaging,” says Rodriguez Palomares. The guidelines highlight that optimal pharmacological treatment (antithrombotic, lipid-lowering, antihypertensive, antidiabetic) and emphasis on exercise and lifestyle changes are mandatory and effective in reducing burden of disease. Patients with PAAD have a very high cardiovascular risk and require optimal management of risk factors such as hypertension, hyperlipidaemia, and diabetes to prevent serious complications.
Finally, the authors emphasise gender aspects and that PAAD comprises chronic diseases requiring continued attention. They conclude: “PAAD is a chronic disease necessitating lifelong follow-up by vascular specialists, cardiologists, and a multidisciplinary team. Women often present with atypical or asymptomatic disease, warranting special attention during screening. Exercise and lifestyle changes are crucial before considering interventional management in chronic PAAD.”
Jupiter Endovascular has announced that the US Food and Drug Administration (FDA) has approved its investigational device exemption (IDE) application for the SPIRARE II US pivotal study. The pivotal trial will study the Vertex pulmonary embolectomy system, which incorporates Jupiter’s Endoportal Control platform technology into endovascular procedures intended to treat acute pulmonary embolism (PE).
Endoportal Control is designed to bring these benefits to a variety of catheter interventions, with the goal of enabling interventionalists to deliver treatment to anatomical sites that they cannot safely or easily reach with a conventional endovascular approach. The endoportal device is delivered in a relaxed state over a guidewire to the target location in the vasculature, pressurised with saline to fix it in a stable position for therapeutic delivery, then relaxed again to navigate to another target location or for removal.
SPIRARE II is a prospective, single-arm, multicentre pivotal trial that will enrol up to 145 patients with acute, intermediate-risk PE treated with the Vertex PE system at up to 25 US sites, a recent press release states. Trial endpoints will characterise the procedural and clinical benefits of PE treatment with Endoportal Control using the Vertex system, across measures of safety, right heart function, and clinical improvement from the time of the procedure to 30 days post-procedure. SPIRARE II is part of Jupiter Endovascular’s SPIRARE clinical program, which also includes the SPIRARE I clinical study evaluating the Vertex system at up to two sites in Europe.
“One of the remaining challenges in treating PE is the ability to safely navigate through the right heart and into multiple areas of the pulmonary vasculature. The act of placing stiff interventional devices across the right heart may add stress to a strained right ventricle, and today’s catheters can become difficult to purposefully control beyond the main pulmonary arteries,” saidCatalin Toma, director of Interventional Cardiology for the Heart and Vascular Institute at the University of Pittsburgh Medical Center (UPMC) and national co-principal investigator for the SPIRARE II trial. “These risks pose a barrier to the widespread adoption of large-bore catheter therapies for PE, creating the need for a procedural system that can safely access the pulmonary arteries with increased control.”
“In open surgery, we have the benefit of being able to directly visualise the anatomy and the instruments with which we are working. This provides surgeons with an excellent level of control and precision,” saidJoshua Goldberg, surgical director of the Structural Heart Surgery Program at Weill Cornell Medical Center in New York and national co-principal investigator of SPIRARE II. “A percutaneous embolectomy system that can provide interventionalists with the control and stability we enjoy in surgery holds the potential to dramatically improve procedural safety, efficacy, and efficiency.”
“We are excited about FDA approval of the first pivotal study of a system leveraging our Endoportal Control platform technology. In the more than 25 animal studies conducted to-date with the technology, it has demonstrated safe and easy navigation through the heart and vasculature, and effective delivery of test interventions,” said Carl J St Bernard, Jupiter Endovascular CEO. “Endoportal Control has the potential to meaningfully improve many endovascular procedures while enabling entirely new therapies. Our Vertex system for pulmonary embolectomy is the first of what we intend to be a portfolio of our own interventional procedure systems incorporating Endoportal Control to treat a variety of cardiovascular conditions that affect millions of patients worldwide.”
Copyspace design of hope amid the gloom concept, a bright exit door in dark room, the light at the end of the tunnel
“Dombrowski finally determined that the rupture had happened in the pancreatic branch of the inferior pancreatic-duodenal arcade, a minor and rarely problematic artery. All that remained was to run a catheter down the artery and embolize it with a series of coils that are left in place to create a massive blood clot. A guide catheter was advanced to the site of the occlusion in the celiac. Dombrowski forced his way through the blockage, to reach the rupture.”
Sebastian Junger
This extract, taken from his latest book, In My Time of Dying, Sebastian Junger—acclaimed journalist and best-selling author of The Perfect Storm—exemplifies a visceral departure from his usual exploration of conflict and war. Here, he offers a sobering first-person account of his near-death experience and the interventional radiological treatment that saved his life.
Philip Dombrowski
In stark contrast to the gravity of Junger’s experience, to Phillip Dombrowski (Cape Cod Hospital, Hyannis, USA)—the interventional radiologist who treated Junger—these events were somewhat routine. Yet, when told from the perspective of the patient on the table, the pioneering interventional techniques used to treat critical conditions such as Junger’s are brought to life. Speaking to Interventional News, Dombrowski recounted the incident.
“It was during the beginning of the COVID-19 pandemic, and I got a call for our interventional service for a late-50-year-old male with a ruptured aneurysm in his pancreatic artery. Haemodynamically, he was in a very guarded condition in terms of his blood pressure, and I had been given prior warning as he was being resuscitated in the emergency room at that time.
We were still perplexed over the source of his bleeding, and a computed-tomography [CT] scan was ordered which ultimately showed that he was bleeding from the bed of the pancreas and had a large intraperitoneal haematoma. I got a call from Dan Gorin, the vascular surgeon on call, and Steve Kohler, the emergency room physician, who felt he was not a good candidate for surgical exploration. We considered approaching this from an intravascular standpoint, and when we were able to isolate the area from the CT scan, the issue appeared to be a pseudo-aneurysm occurring from the pancreatic or duodenal artery that supplies the pancreas. We determined that an endovascular approach would be best to try to embolize or block the aneurysm.”
Dombrowski noted that this type of aneurysm is rare, accounting for only 2% of all visceral artery aneurysm cases and carries a mortality rate of between 20–30%.
“After resuscitation, his vital signs had improved and so we were using what we call conscious sedation which means the patient is in a semi-awake state. I know that Junger has spoken on being awake for different parts of the procedure and could hear and was aware of what was happening. It’s interesting to read.”
“I was very worried that I had died but didn’t know I had, and was some kind of spirit—I know how crazy this sounds”—Sebastian Junger
Junger describes how, during his treatment, he was visited by his deceased father who invited him to join him. He recounts that this is the last thing he remembered before coming to the following day in the intensive care unit. This ordeal prompted him to research the IR techniques that prevented his death and provoked his near-death experience. Junger began reviewing medical literature and interviewing retired interventionists, seeking a better understanding of what had happened.
In conversation with Interventional News, Junger shared that he was “strongly averse” to literature on near-death experiences for a long time. “It’s hard overstate how psychologically debilitating this was for many months afterwards. I was very worried, against all evidence, that I could develop another aneurysm very quickly that would rupture and kill me. I was very worried that I had died but didn’t know I had, and was some kind of spirit—I know how crazy this sounds—” Junger explained.
“Apparently, this kind of derealisation is a well-known consequence of near-death experiences. A mass was later detected against my pancreas, which was clearly the remnants of the haematoma, and was tested as a possible tumour. That, of course, was absolutely terrifying. The testing went on for months and wound up with a recommendation of surgery ‘just to make sure’. This process was frankly far more traumatic than the original aneurysm rupture and really should be guarded against. I opted against surgery, and I am fine.”
Junger stated that, following his treatment, he experienced mild radiation burns on his back—“an unavoidable consequence of saving my life”. Although rare, he highlighted how important information sharing is on radiation exposure and the associated risk of cancer. “The vast majority of survivors are going to be externally grateful to the doctors for saving their lives, but still deeply traumatised by the events. This leaves them wide open to paranoid fears about their health that only full, open conversations can alleviate.”
In Nantucket last month, Dombrowski and his family attended Junger’s talk on his experience, meeting for the first time since his treatment. For Junger, this meeting was emotional, describing Dombrowski as a “sweet, compassionate and humble man, and an unbelievably skilled interventionist”.
“Everyone in the audience knew that they could have been me in the IR suite that day. After the talk, Dombrowski and I hugged and chatted for a bit. It brought the entire terrifying ordeal full circle and allowed for a bit of closure,” Junger said.
Reflecting on Junger’s near-death experience, Dombrowski admitted that he doesn’t necessarily believe in life after death. “I tend to approach things in a very scientific way and need some proof before believing. But there are situations that have occurred that make you wonder if there is something beyond what we can understand or grasp.”
Yet—suspending his disbelief—Dombrowski anecdotally shared how he came to realise that he was the interventionist described in Junger’s book.
“I got a message from Michael Hallisey saying ‘Good job—I’ll call you in two hours’. Hallisey is an interventional radiologist I’ve known for 30 years. We were at the forefront of training in the 1970s and 80s—it was a relatively new profession, and we would both call to discuss cases and bounce ideas off each other. Hallisey told me that he had recently seen the New York Times article about Junger’s experience and was heading to his book signing in Atlanta and had listened to his talk, not realising that I was the one who had performed the procedure until after. He called me on his drive home.
The fact that we have known one another and collaborated for years—and Hallisey had even published a paper on the specific aneurysm Junger experienced 20 years earlier—makes me think there is probably more out there in space than we realise, something pulling the strings.”
“It’s a boy’s club. If the only examples of success are men, it becomes harder for women to envision themselves in those positions.” These were the words of Miyuki Sone (National Cancer Center, Tokyo, Japan)—head of interventional radiology (IR) and consultant radiologist—during her honorary lecture at the Global Embolization Oncology Symposium Technologies (GEST) annual conference (16–19 May, New York, USA).
Sone’s talk covered a plethora of issues faced by women in IR, including visibility and social and cultural barriers. Speaking to Interventional News following her lecture, Sone first and foremostly emphasised empathy in the IR suite.
“Women are more capable of empathy than men,” Sone explained, describing the 2023 report published in Nature which found women to be superior to men in displaying empathy and compassion, but found men and women equal when expressing theory of mind— the inference of others’ emotional status. “If you include women in your IR team, you can build an empathetic environment which is translated to the patients,” Sone said. “This nurturing environment is crucial for the development and retention of talent, particularly in women who may face unique challenges in their career.”
Recruiting women to the team however remains Sone’s initial challenge. In her talk, she shared data from a 2019 survey carried out by the Japanese Society of Interventional Radiology (JSIR) which compared membership, leadership, and mentorship with that of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE). Of the 304 women who were members of JSIR, 63 responded—79% of whom did not hold a leadership position and 55% reported having a mentor, of which 88% stated that their mentor was male.
These numbers have remained low, Sone reporting that in 2023, only 40% of Japan’s new medical students were women, and further, only 13% of those with JSIR membership were women. “When women see other women thriving in IR, they can envision themselves in those roles,” she said. “We need to promote a self-reinforcing cycle where more women are encouraged to join and excel in the field.”
However, women who have gone into IR in Japan report high job satisfaction, Sone stated, having conducted another survey to measure this regardless of gender. Receiving 901 responses from a total of 2,824 recipients, 56% reported high job satisfaction, which was positively associated with a higher number of IR procedures and negatively associated with salary, overtime and the absence of an “IkuBoss”—a person who manages the working environment and supports work-life balance.
“My young colleagues have a different mind as they are of another generation,” Sone explained. “They care more about their family and believe that if they are not happy, the patient can’t be happy. It’s my belief that happiness should come from both work and private life, so I always tell my colleagues: ‘your life and your family are your first priority—if you want to go early to take care of your children or go out and enjoy a concert, just manage your time and we can manage the team together.”
To her point on time management, Sone then used the 2017 paper titled ‘Women’s challenges in IR: #ILookLikeAnIR’ as an example of the positive retentive outcomes that occur when work-life balance is prioritised. The paper discussed the six-strong team of women interventional radiologists at Memorial Sloan Ketting Cancer Center in New York, USA, who organise their team according to preferred working hours. Their team channels add-on inpatient cases to prespecified rooms, ensuring that colleagues who require a scheduled finish are able to leave on time, enhancing the quality of life of their male and female colleagues.
Through her honorary lecture, Sone highlighted the crucial “drivers of change” that will be led by “individuals, allies, sponsors, institutions and through organisation structures”.
“I was fortunate to have the opportunity to speak at GEST particularly on the topic of women in IR. The conference organisers were early adopters in terms of diversity and inclusion. It was excellent to connect with people around the world and talk about strategies to increase the number of women in our field.”
SonoVascular has announced the successful initiation of its first-in-human study (FIH) of the company’s SonoThrombectomy system, an ultrasound-facilitated, thrombolytic-enhanced platform that utilises multiple mechanisms of action to treat patients with venous thromboembolism (VTE). The catheter-based system combines microbubble-mediated cavitation with low-dose thrombolytic delivery to treat clots with no blood loss.
The FIH case was completed at the Hospital Dipreca in Santiago, Chile, under the supervision of vascular surgeon Manuel Espíndola, principal investigator (PI) at the site, with the assistance of Albrecht Krämer, also a vascular surgeon and the study PI. The clinical team successfully used SonoThrombectomy to treat deep vein thrombosis (DVT) involving the common and external iliac veins, SonoVascular reported in a press release.
“We were extremely pleased to perform the first clinical case using the SonoThrombectomy system,” said Espíndola. “The Resonator catheter performed exceptionally well, successfully and very quickly removing the thrombus and, most importantly, without the typical blood loss commonly seen in mechanical thrombectomy procedures. The patient was discharged from the hospital within 48 hours and is now at home, asymptomatic and recovering well.”
“The SonoThrombectomy system was effective at reducing thrombus burden while preserving vessel walls due to its unique and gentle approach,” added Krämer. “It is exciting that we achieved such a comprehensive result on the table with a very low dose of thrombolytic.”
The US Food and Drug Administration (FDA) has issued a Class I recall—the most serious type—for Inari Medical‘s ClotTriever XL, 30mm device due to reports of patient injury, and death from device entrapment and pulmonary emboli (PE).
The device remains on the market with updated instructions for use (IFU), with all devices and lot numbers with labelled dates prior to 1 August affected. The FDA recall was categorised as a “correction,” addressing a problem with a medical device in the place where it is used or sold rather than removing it from the market.
There have been four reported injuries and six reports of death, the FDA noted. The serious adverse events occurred in patients who had the ClotTriever catheter inserted through the jugular vein; thrombus that is fibrotic, organised and/or adherent; clot formed by tumour cells; and extremely large clot that cannot be removed in pieces.
On 19 July 2024, Inari sent all affected customers an Urgent Medical Device Labeling Correction letter covering IFU updates, recommending that they view the letter and updates, then share it with any relevant personnel and/or device users; share this information with any organisation where the ClotTriever XL catheter may have been transferred; and complete the Customer Acknowledgement Reply Form as soon as possible.
The FDA recommended that, based on its review of the reported adverse events, users consider the device to be contraindicated for the removal of fibrous, firmly adherent or calcified material, and be aware that the use of a clot capture device—for example an embolic protection device—”has not yet been demonstrated to be effective in the venous vasculature.”
The FDA noted in the recall that US customers with questions about the recall should contact their local Inari sales representative, Inari Customer Care at 877-923-4747, or its quality department at [email protected].
Chidubem Ugwueze (Oregon Health & Science University, Portland, USA) provides an update on the current state of play concerning interventional radiology (IR) equipment and training in low and middle-income countries (LMICs).
Developing an equitable supply chain for IR equipment is essential for training and encouraging interventional radiologists in LMICs, especially in Sub-Saharan Africa. The need for IR training programmes in LMICs has long been acknowledged. Over the past five to ten years, various training initiatives have emerged to address this need. Despite the nascent growth of IR training programmes in the region, local manufacturing of IR devices is clearly non-existent, and direct supply chains are scarce. The graduates of these programmes then find themselves in settings where they cannot fully utilise the range of skills which they have acquired from their training. This is particularly true for clinicians returning to their practice in the public teaching hospitals following completion of their training. One such programme is the two-year IR fellowship in Lagos, Nigeria.
Established through a tripartite partnership between RAD-AID International, University College Hospital (UCH) in Ibadan, and IRDOCNIGERIA, this programme aims to leverage the growing clinical IR practice in the private sector and to transfer this clinical expertise to clinicians in public teaching hospitals. IRDOCNIGERIA, led by Hammed Ninalowo, is a private IR practice in Lagos offering interventional and neurointerventional services.
From left to right: Hammed Ninalowo, Peter Adenigba, Chidubem Ugwueze
In addition to excellent clinical training, further honed by working as an IR attending at a tertiary hospital system in the USA, Ninalowo’s success in creating a clinical service which is suitable as a training programme is based on creation of a reliable supply chain for necessary consumables to utilise the capital imaging equipment instalments already made by hospitals in the private sector. This strategic approach, detailed in an Journal of the American College of Radiology (JACR) article titled ‘Developing a supply chain for interventional radiology consumable equipment in a lower middle-income country: A strategic approach’, includes leveraging clinical expertise, focusing initially on elective cases, adopting a ‘just in case’ bulk procurement model, fostering self-sustaining investment, and collaborating with multiple hospitals.
The wide range of clinical services offered by IRDOCNIGERIA made the practice an ideal partner for an in-country IR fellowship programme, which aims to train senior registrars or junior consultants from teaching hospitals who pledge to return to their teaching hospitals to build IR practice and train residents. The first trainee, Peter Adenigba from UCH in Ibadan, completed his fellowship in June 2024, having performed up to 936 interventions on 821 patients. He now faces the daunting challenge of securing consumables for his new clinical practice. This is not a problem unique to Adenigba. There is a new generation of IR trainees across LMICs who have put in the hard work to become trained, with the goal of training future generations, only to find themselves struggling to obtain the required support to achieve this.
Possible avenues of support include national governmental investment in the capital equipment required to grow an IR practice in public institutions and the support of industry to make consumable devices more easily accessible to these burgeoning IR pioneers like Adenigba. The aim of this article is to add to the voices advocating for industry investment in device registration, partnership with local distributors, and eventual local manufacturing of equipment in LMICs. This is an investment that is bound to be mutually beneficial for industry and the growing practice of IR in LMICs.
Chidubem Ugwueze is an associate professor of interventional radiology at the Dotter Institute of Oregon Health and Sciences University in Portland, USA.
In a session titled ‘Bariatric embolization: Is it the end or a new resurgence?’ at the Global Embolization Oncology Symposium Technologies (GEST) annual conference (16–19 May, New York, USA), Clifford Weiss (Johns Hopkins University, Baltimore, USA) made a case for “his future” and the future of bariatric embolization, providing the capability to “do surgery without doing surgery” to treat a highly comorbid patient population suffering with obesity.
First, placing emphasis on the severity of the obesity crisis in the USA, Weiss relayed that a dataset collected by Nima Hafezi-Nejad (Johns Hopkins University, Baltimore, USA) et al, found that 22 states reported an obesity prevalence of over 35%. However, he noted that the comorbid nature of obesity, which causes sleep apnoea, cancer, pancreatitis, diabetes, heart disease, and suicide and depression, is fundamentally “what kills”.
“Minority populations in particular are heavily hit by this disease. We also know that annually, there’s an aggregate of US$260 billion spent on obesity and obesity-related illnesses in the USA. This is a deadly disease causing significant excess mortality annually. We need effective treatment options and I think we can all agree with that,” Weiss stated.
He explained that treatments for obesity are most effective and show the highest mortality signal improvement when sought intentionally, “in other words, you don’t seek to lose weight because you’re sick—this is the argument for why we need patients to be healthier and thinner. It’s not to look better at the beach, but it’s to be clinically healthy”.
Treatments can range from extreme, such as surgery, which is the “least accepted but the most effective”, he stated, to lifestyle modification. His focus, however, is on the pharmacotherapy treatments which sit in the middle and include interventional radiology and gastroenterology devices.
When performing bariatric artery embolization (BAE), the targeted intra-arterial therapy delivers the embolic to the gastric fundus, defunctionalising it and causing a mechanical shift which affects ghrelin-producing cells, or hunger-stimulating hormones, Weiss described. “We down-regulate these cells, turning them off rather than cutting them out.”
Weiss went on to provide an update on the ongoing BAE of Arteries with Imaging Visible Embolics (BEATLES) trial—of which he is principal investigator. He detailed that participants with a body mass index (BMI) of ≥40kg/m2 with no other comorbid conditions underwent BAE with 300–500μm Embospheres (Merit Medical), which at six months, show a 7.6% weight loss or a 60% excess weight loss.
“What we’re doing in this trial is looking at whether this is fat loss or muscle loss, and multi-compartment [magnetic resonance imaging] MRI shows that we were losing subcutaneous fat and liver fat, while muscle volume remains steady,” he said. Their six-month results also show “soft signs” of improvement, such as cardiovascular markers, changes in hunger and quality-of-life scores, each showing statistically significant values post-BAE.
Regardless of his allegiance to BAE, Weiss stated that the current US investment in anti-obesity medications (AOMs)—such as Ozempic (Novo Nordisk)—is valuable. “I didn’t want to avoid this. We have really good drugs on the market right now that are getting an easy 15–20% weight loss, so is there relevance to [BAE] still?”
In Weiss’ belief, BAE still provides a crucial and relevant benefit to this patient population as medication persistence—which is a prevailing issue with AOMs—can be avoided.
“When you take these medications away, the benefits go away with them, almost back to baseline. The current AOM guidelines state that these are lifetime medications, yet that’s a problem—many patients don’t qualify and adherence can be as low as 27% after the initial weight loss. So, can we have a combination strategy to mitigate recidivism and dependence on medication?”
Finalising his talk, Weiss advocated for the cost-effectiveness and efficacy of combined pharmacotherapy and embolization, for the dual benefit of patients as well as national and international healthcare systems.
One-year limb salvage and quality of life (QoL) data from the STRIDE study, showing that frontline use of Penumbra’s Indigo system for patients with lower extremity acute limb ischaemia (LE-ALI) is safe and effective, has been published in theJournal of Vascular Surgery. Results were presented at the Vascular Annual Meeting (VAM 2024; 19–22 June, Chicago, USA).
One-year outcomes include: 88.5% target limb salvage rate and 12% mortality rate at 365 days, and overall improvement in QoL, as measured by the VascuQoL-6 questionnaire, from baseline to one year follow-up.
The latest results build on evidence from the initial publication of 30-day STRIDE data, in which the primary endpoint, target limb salvage, was achieved in 98% of patients. The Indigo system was able to achieve these high rates of limb salvage and low rate of mortality with median device time of 22 minutes.
“The latest STRIDE data continue to demonstrate the use of Penumbra’s Indigo aspiration system to address LE-ALI results in excellent outcomes, including high target limb salvage rates and quality of life,” said Thomas Maldonado (New York University of Langone Health, New York, USA), national principal investigator of the STRIDE study. “The data is promising in that it underscores the significant benefits of continuous aspiration to remove thrombus and should be considered a frontline treatment for LE-ALI.”
STRIDE was a multicentere, prospective, single-arm, observational study that enrolled 119 patients across 16 sites in the USA and Europe. The study, which completed follow-up in October 2023, was designed to assess safety and efficacy of mechanical thrombectomy using the Indigo aspiration system in patients with LE-ALI. Secondary endpoints at 365 days included target limb salvage and mortality. Additionally, the VascuQoL-6 questionnaire, developed for evaluating patient-centred QoL outcomes for peripheral arterial disease, was assessed at baseline and follow-up through 365 days.
ALI, a sudden lack of blood flow to a limb, is associated with a high risk of amputation and death. Early diagnosis and intervention are crucial to improving patient outcomes and preserving limb function. Penumbra’s Indigo aspiration system is a minimally invasive continuous aspiration device that is designed to quickly remove emboli and thrombi from vessels of the peripheral arterial and venous systems.
“Yes, we know that gelatin sponge works, but I believe that these are vital data to show that what we do is safe and effective, and to guide regulatory approval not only in Australia, but internationally,” said Warren Clements (Alfred Health, Melbourne, Australia), presenting preliminary efficacy results using EmboCube (Merit Medical) embolization gelatin to control haemorrhage.
Clements shared these results at The European Conference on Embolotherapy (ET) annual meeting (1–4 June, Vienna, Austria), ahead of a further data release at the Cardiovascular and Interventional Society of Europe (CIRSE) annual congress (14–18 September, Lisbon, Portugal).
“We know that uncontrolled bleeding is a leading cause of preventable death following trauma, and embolization has become an important facet of the management of haemorrhage in this space,” Clements stated. He described that, over the last 10 years, open surgery has been common in these patients, but now a “shift” toward endovascular techniques is taking place.
Charting the course of gelatin embolization, Clements highlighted that this technique was reportedly first used in 1967. “Why are we doing a study looking at gelatin when we know it works?” he asked the ET audience. In response, he explained that, often in interventional radiology (IR), clinicians adopt a technique that works and begin using it without gaining the “right data” to prove why.
“What happens is jurisdictional and regulatory bodies then step in,” Clements said. In Australia, Gelfoam sponge (Pfizer) is currently off-label for endovascular use following an embargo that was placed in May 2021, previously, Gelfoam was favoured for gelatin embolization procedures.
Clements et al, in the introduction to their study, note that this embargo did not reflect Australian IR user experience, which largely believed Gelfoam to be a “highly effective” live-saving tool. Providing evidence for their experience, Clements outlined their multicentre, prospective cohort study which enrolled 100 patients experiencing haemorrhage. Their primary endpoints were defined as safety—the absence of unanticipated serious adverse device-related effects within 24 hours, and effectiveness— technical success and clinical success, or the cessation of bleeding within 24 hours post-procedure.
In this patient population, the mean age was 56 years, and 48 patients were reported to be taking anticoagulants or antiplatelets. Clements stated that the vessels treated were significantly heterogenous, pointing out that the hepatic artery, uterine artery and pelvic artery were among the most commonly treated.
Technical success was achieved in all patients with no complications recorded with the use of gelatin. Clinical success was reported as 98% due to two patients requiring repeat intervention. Additionally, he noted a 7% rate of all-cause mortality, which, when considered in this patient population which experience multi- system trauma including neurological trauma, a 7% rate of mortality—a rate lower than general pelvic trauma management—is a “good rate”, Clements said.
Clements underlined that gelatin foam is safe and effective, despite this being somewhat known already. However, in collecting these “vital” data he hopes to guide regulatory approval in Australia to prevent future embargoes being placed which restrict clinicians access efficacious tools.
A new research letter underscores the need to improve long-term survival following lower extremity revascularisation for chronic limb-threatening ischaemia (CLTI), setting out a randomised controlled trial to examine the impact of coronary artery ischaemia testing in these patients.
The letter, authored by Dainis Krievins (Pauls Stradins Clinical University Hospital, Riga, Latvia), Andrejs Erglis (University of Latvia, Riga, Latvia) and HeartFlow’s senior advisor for medical affairs, Christopher K Zarins, was recently published online ahead of print in the European Journal of Vascular and Endovascular Surgery (EJVES).
Krievins and colleagues first detail that patients undergoing lower extremity revascularisation for CLTI or claudication have “poor” long-term survival due to co-existing coronary artery disease (CAD), which they note is “often asymptomatic, undiagnosed and undertreated”.
Diving into the available data on the topic, Krievins et al highlight an “alarmingly high” mortality rate in these patients that is evident throughout the literature. They state, for example, that the recent BASIL-2 and BEST-CLI randomised controlled trials reported a five-year mortality rate for patients with CLTI that exceeded 50% and was three times higher than the risk of amputation. They also note a 10–12% annual mortality rate following lower extremity revascularisation in studies including both patients with CLTI and those with claudication—namely SWEDEPAD, SAFE-PAD and VQI Vision.
The authors point out that the mortality rate in these patients is not only high, but has remained unchanged over the past 40 years, contrasting a “marked decline” in the mortality rate among patients with symptomatic CAD in association with coronary revascularisation as a mainstay of treatment. Current annual mortality for patients with CAD is only 1–2%, the researchers point out, as per the ISCHEMIA, FAME 2 and SCOT-HEART trials.
Krievins and colleagues state that guidelines recommend no cardiac testing of patients without cardiac symptoms prior to vascular surgery procedures, despite patients with PAD with combined CAD having “invariably worse outcomes”.
Against this backdrop, Krievins et al detail that they have embarked on a multicentre, randomised clinical trial to determine whether non-invasive diagnosis of silent coronary ischaemia together with ischaemia-targeted coronary revascularisation can improve the outcome of patients following lower extremity revascularisation.
The SCOREPAD (Selective coronary revascularisation in peripheral artery disease patients after lower extremity revascularisation) trial, will enrol up to 600 patients with CLTI or severe claudication and no known CAD after successful open or endovascular lower extremity revascularisation, Krievins and colleagues share in EJVES. The patients will be randomised to either coronary computed tomography angiography (CTA) plus computed tomography-derived fractional flow reserve (FFRCT; HeartFlow) with ischaemia-targeted coronary revascularisation in addition to best medical therapy (BMT) or BMT alone with no elective coronary revascularisation, which they note is the current guideline-directed standard of care.
The primary endpoint of the trial is a composite of cardiac death, myocardial infarction (MI) and urgent (unplanned) coronary revascularisation during twoyear follow-up, the authors detail. Extended followup will continue out to five years.
“Patient enrolment began in February 2024 and more than 80 patients have been randomised so far,” Krievins et al report in EJVES, who go on to say that the trial is seeking to include up to 10 additional sites in Europe and the USA.
In a paper published in the July 2024 issue of the Journal of Hypertension, Andrew Sharp (University Hospital of Wales and Cardiff University, Cardiff, UK) et al reviewed 16 randomised controlled trials to assess the evidence of renal denervation’s (RDN) efficacy, concluding that, in uncontrolled arterial hypertension, RDN leads to a consistent reduction in blood pressure.
Up until now however, RDN had been effectively abandoned, largely due to the influential 2014 SYMPLICITY HTN-3 (Renal denervation in patients with uncontrolled hypertension) trial which found no significant difference between RDN and sham control groups at six-month follow-up. Yet—perhaps supplying the spark for RDN’s revival—in 2022, the Medtronic-sponsored trial published three-year follow-up data which showed that RDN provided a sustained blood pressure reduction benefit for those patients, with the first-generation single-electrode technology.
In Franz Messerlli’s (Saint Luke’s Roosevelt Hospital, New York, USA) view, there are still two groups despite the emerging data—the enthusiasts and the sceptics. “In recent meta-analyses—such as Sharp et al’s—we see a fall of 3.6mm of mercury [mmHg], and
Franz Messerli
to many of us, this is simply not sufficient to justify an invasive procedure.”
Although, in an accompanying commentary to Sharp and colleagues’ research titled ‘Why the lack of enthusiasm for renal denervation?’ in the July issue of the Journal of Hypertension, Messerli asserts that the authors “correctly conclude” that RDN leads to consistent blood pressure lowering. Messerli however, took issue with the authors’ statement that the reduction of systolic blood pressure of 2mmHg was associated with a 10% reduction in stroke mortality in a middle-aged population, which references the 2002 Sarah Lewington (Nuffield Department of Population Health, Oxford, UK) et al study of age-specific relevance of usual blood pressure to vascular mortality.
“This is a wishful misinterpretation of the Lewington [et al] data,” Messerli writes, “all too commonly misused for marketing drugs with paltry antihypertensive efficacy.” He believes that, due to hypertension’s prevalence as one of the most common cardiovascular diseases worldwide, it has therefore become “a money-making” procedure. “You can simply assume that without industry support, RDN would not survive,” Messerli said. He continued, describing a term he has coined as ‘gizmo idolatry’, stating that the treatment of hypertension—a disease that has been around for centuries—is “absolutely boring”, but with the development of a new device, “there is a new kid on the block—a gizmo”. In his opinion, following this excitement drawn up by recent meta-analyses concerning RDN, clinicians will realise that there is “very little reason” to use the technique except in “selected patients, few and far in between”.
Hypertension leads to stroke, heart attack, heart failure, kidney damage, and several other health problems, particularly in an aging population. As set out in Dena Ettehad (University College London, London, UK) et al’s 2016 data in The Lancet, a reduction of 10mmHg in systolic blood pressure is associated with substantial risk reductions: 28% for heart failure, 27% for stroke, 17% for coronary disease, 5% for chronic kidney failure, and 13% for mortality. Although RDN is commonly believed to reduce blood pressure to the equivalent of one antihypertensive drug, the minimally-invasive procedure can reduce the issue of non-adherence to medication, as often patients are required to take anywhere from one to three types of medication daily.
Mahmood Razavi
Mahmood Razavi (Providence St. Joseph Hospital, Orange, USA) commented that compliance with this level of medication is challenging for most. “No one likes to get up every day and take one, two or three medications multiple times daily,” he stated. On top of this, he noted that hypertensive patients will likely have other medical conditions that they will also be taking medication for. He explained that the idea behind RDN was to replace medication with a single procedure, to reduce the frequency or dosage of medication a patient must take, or to treat patients who cannot tolerate antihypertensive drugs.
The incidence of non-adherence to antihypertensive medication could be why the early randomised RDN studies like SYMPLICITY HTN-3 were negative, Razavi stated. “Patient selection is key—this could have been due to patients who were non-compliant with medication and once entered into the trial, received treatment and therefore their blood pressure dropped.” Despite this, Razavi recounted that, of the patients that his centre enrolled into SYMPLICITY HTN-3, they reported “very positive outcomes”, having observed that even in patients on three antihypertensive medications, blood pressure was reduced by 20mmHg following RDN.
Since then, several second-generation RDN trials using multielectrode technology and adjacent ultrasound techniques have been reported to cause a significant reduction in blood pressure compared to sham control groups. Presenting at the 2024 Charing Cross (CX) International Symposium (23–25 April, London, UK), Neelan Das (East Kent Hospitals University NHS Foundation Trust, London, UK)— presenting in a session dedicated to the developing evidence in support of RDN’s return—exemplified the 2023 RADIANCE II trial results as proof of this fact.
Neelan Das
Das described the study as the largest trial to compare ultrasound RDN to a sham control. The trial highlighted the statistically significant improvement in blood pressure in patients who were taken off antihypertensive medication for four weeks, with a sustained benefit at night to prevent the deleterious effects of nocturnal hypertension. In November 2023, the Paradise (Recor Medical) RDN system used in the RADIANCE II trial was approved by the US Food and Drug Administration (FDA), followed closely by the Symplicity Spyral RDN system (Medtronic) in the same month.
Then, Das detailed the current European Society of Hypertension (ESH) and UK National Institute of Clinical Excellence (NICE) guidance which suggests RDN should only be used in patients who have resistant hypertension, are intolerant to medications, or are on fewer than three medications. This guidance, however, contrasts the findings of the RADIANCE II trial, he stated, which provided a significant reduction in blood pressure “overall, even without antihypertensives”. “I do believe that there is a role for RDN in this difficult-to-treat group,” he concluded.
Lindsay Machan
Lindsay Machan (The University of British Columbia, Vancouver, Canada) also presented in the CX 2024 session, and stated: “Looking at the historic headlines, everybody here would think this is a dead technology and assume that it shouldn’t resurface— why is it alive again? The answer is new information. We have new information for physicians who treat hypertension—of the 116 million adults in the USA with hypertension, less than half are controlled and this rate of control is falling off. Nobody entirely understands why.”
However, with the advent of this new information, access to RDN remains a challenge in locations worldwide. As Razavi highlighted, difficulties have arisen when seeking reimbursement—“although two devices are approved by the US FDA, we cannot offer them to our patients as there is no reimbursement from Medicare or from private insurance companies. This means patients realistically have no access to the technique.”
RDN continues to divide opinion. As industry-led data emerge to show that the technique can provide a significant reduction in blood pressure long-term, some clinicians remain dubious. “We need more refinement that correlates various physiological characteristics with outcomes— without refinement which tells us who will benefit from which type of technology, we won’t know who needs RDN. But, we are learning and progressing, and over the next several years we will know who responds best,” Razavi said.
A newly published US Medicare cohort study illuminates trends and factors associated with peripheral vascular interventions (PVIs)—including a sharp rise in the use of ambulatory surgical centres (ASCs) and office-based laboratories (OBLs) for treatment—from 2011 to 2022.
In the Journal of the American Heart Association (JAHA), first author Chen Dun, senior author Caitlin Hicks (both Johns Hopkins University School of Medicine, Baltimore, USA) and colleagues write that while previous cross-sectional studies have identified wide practice pattern variations in the use of PVI for the treatment of claudication, there is a paucity of data on longitudinal practice patterns. Against this backdrop, the investigators set out to describe the temporal trends and charges associated with PVI use for claudication over the past 12 years in the USA.
Dun et al conducted a retrospective analysis using 100% Medicare feefor- service claims data to identify all patients who underwent a PVI for claudication between January 2011 and December 2022. The researchers evaluated trends in utilisation and Medicare-allowed charges of PVI according to anatomic level, procedure type, and intervention settings using generalised linear models. They used multinomial logistic regressions to evaluate factors associated with different levels and types of PVI.
Overall, Dun and colleagues identified 599,197 PVIs performed for claudication. They report in JAHA that the proportional use of tibial PVI increased 1% per year and atherectomy increased by 1.6% per year over the study period.
Furthermore, they highlight that the proportion of PVIs performed in ASCs and OBLs grew at 4% per year from 12.4% in 2011 to 55.7% in 2022, and that total Medicare-allowed charges increased by US$11,980,035 per year.
Finally, the authors share that multinomial logistic regression identified “significant” associations between race and ethnicity and treatment setting with use of both atherectomy and tibial PVI.
In the conclusion of their findings, Dun et al summarise that the use of tibial PVI and atherectomy for the treatment of claudication has increased “dramatically” in the past decade “despite poor evidence supporting their efficacy, especially long term”. They stress that this trend is most notable in ASC and OBL settings and among non-white patients and has been associated with a “significant” increase in healthcare expenditures over time.
Dun and colleagues note that—to the best of their knowledge—this study is the most up-to-date analysis describing the use of PVI for claudication using longitudinal, nationally representative data.
The authors also acknowledge “several” limitations to their research, including the fact that their results are based on Medicare beneficiaries primarily aged 65 years and older who “might not be representative of the overall US population with claudication”. In addition, they recognise the downsides of administrative data, underscoring a possibility that patients they identified as having claudication had more advanced peripheral arterial disease and were misclassified. They also highlight the possibility that some of the trends they report “are related to an ageing population with an increased prevalence of risk factors, rather than practice-specific changes alone”.
Despite these limitations, Dun et al write as a closing statement that their results highlight “a critical need to improve the delivery of equitable, evidence-based and value-based care for the treatment of claudication”.
NOTE: This video is ONLY available to watch in selected countries and geographies
Bulent Arslan (Chicago, USA) explores why interventional radiologists. interventional cardiologists and vascular surgeons should consider the Laguna Clot Retriever and Malibu Aspiration Catheter to experience its benefits when performing peripheral vascular thrombectomy. This device is exclusively distributed in the USA by Varian Medical Systems, Inc.
He describes how the device adapts to remove acute, subacute and chronic clots—the latter of which can be the most problematic. When dealing with these older clots, he believes that timely aspiration and clot retrieval are essential, due to the dual effect of the Laguna clot retriever and Malibu aspiration catheter. This can aid procedural efficiency.
Arslan explains why he favours the device for subacute and large clots that require the most prompt treatment and, as the device is available in a wide range of sizes, how it can also be safely across different clot morphologies and vessel sizes.
“We can treat all of the clot, from the heart down to the popliteal level with this device”, Arslan says.
A new study has determined genicular artery embolization (GAE) to be a “safe intervention” for mild knee osteoarthritis (OA), showing a sustained benefit at two years. Published in the journal CardioVascular and Interventional Radiology, the authors state that the “learning curve” reflected in their technical success rates uncovers the “complexities” behind the safe and successful performance of GAE.
The study, titled Genicular artery embolization in patients with osteoarthritis of the knee (GENESIS) and led by Mark Little (Royal Berkshire NHS Foundation Trust, Reading, UK) et al, is a National Institute for Health and Care Research (NIRH) portfolio single-centre prospective trial which recruited patients presenting to the orthopaedic department at Royal Berkshire Hospital in Reading. Patients were aged 45 years or older with mild-to-moderate knee OA, defined as Kellegren-Lawrence grade 1–3, who had experienced pain for more than six months despite conservative management.
Little et al enrolled 46 patients with a median age of 60 years, performing GAE using 100–300μm Embosphere (Merit Medical) permanent particles diluted in 20ml (300mg/ml) iodinated contrast (Iomeron). Technical success—defined as embolization of the targeted genicular artery—was achieved in 40 patients (87%) and mean visual analogue scale (VAS) improved from 58.63 (standard deviation [SD] 20.57, 95% confidence interval [CI] 52.7–65.5) at baseline to 37.7 at two years.
The authors also assessed knee injury and osteoarthritis outcome score (KOOS) which they state showed significant improvement at six weeks, three months, one- and two- year timepoints, with associated reductions in analgesia usage. Concerning complications following GAE, Little and colleagues observed a self-limiting groin haematoma and a single case of deep vein thrombosis due to immobilisation, which they say highlights the importance of early mobilisation post GAE.
Further, Little et al detail that nine patients underwent total knee replacement following GAE but when followed up post-surgery, no intraprocedural issues or adverse events were experienced by the operating surgeons or the patient. “This provides further support for the procedure’s utility in those with mild-moderate disease,” the authors state, “as it appears that embolization can be utilised in this cohort without being prohibitive of further surgical intervention in cases of disease progression.”
The authors also carried out functional magnetic resonance imaging (MRI) and psychometric assessments, observing an “unexpected” correlation between baseline catastrophising—maladaptive pain cognitions—and greater reduction in pain post GAE. The authors note that these findings may suggest that patients who catastrophise at baseline experience a bi-fold improvement.
“The neurological data suggest that those who catastrophise at baseline are associated with higher functional connectivity between pain modulatory and processing regions of the brain, perhaps representative of frequent dependency on pain modulation. These patients could be benefitting from a successful reduction in nociceptive signalling via embolization and an overreliance on pain modulatory circuitry.”
Remarking on the operator learning curve visible in their technical success data, the authors identify that a “thorough knowledge” of genicular vascular anatomy, including a “myriad” of anastomoses and non-target tissues supplied by these vessels, is crucial to obtain good technical outcomes. They explain that improved anatomical understanding and the application of intraprocedural cross-sectional imaging has enabled GAE to be undertaken in more complex cases today.
Of their limitations, the authors highlight their small sample size, the lack of an experimental control group and note a placebo effect which “requires consideration” when evaluating modes of treating pain. Going forward, the team detail the GENESIS 2 randomised sham-controlled trial which will consider the placebo effect “inherent with GAE”. Little et al note that they are currently recruiting patients for this study and hope to build on experiences gained from the current work.
In a new post-hoc analysis of the Lutonix (BD) arteriovenous (AV) global registry using investigational device exemption (IDE) criteria, Dimitrios Karnabatidis (Patras University Hospital, Patras, Greece) reports the “highest” six-month target lesion primary patency (TLPP) to date when evaluated through IDE criteria, presented at the Endo Vascular Access (EVA) meeting (14-15 June, Patras, Greece).
As part of a post-approval study mandated by the US Food and Drug Administration (FDA), the Lutonix AV global registry assessed the safety and clinical benefit of the Lutonix drug-coated balloon (DCB) catheter for the treatment of dysfunctional AV fistulae (AVF) and grafts (AVG) located in the arm. The real-world, multicentre, prospective study enrolled 320 patients from 12 countries across Europe and Asia—the largest DCB arm to date— Karnabatidis told EVA delegates.
At six months, the primary safety endpoint defined as freedom from serious adverse events was reported as 95.5%, while TLPP was 73.9% and access circuit primary patency (ACPP) was 71%. TLPP for stenosis of AVFs was 78.1%.
Karnabatidis then went on to question how key IDE exclusion criteria would affect these results, detailing which variables would affect the patient population. These variables include:
Lesions of >80mm
Lesions outside the range of 4–12mm
>30% residual stenosis
Previous graft
In-stent restenosis
Central veins as target lesions
Karnabatidis and his team also identified thrombosis at index as a potential exclusory variable, comparing this to the IN.PACT IDE trial which also excluded patients with current or previous thrombosis events. Other key exclusions include the presence of a stent in the target or secondary lesion, or if more than two secondary lesions are in circuit, however Karnabatidis specified that if a single patent stent is in circuit this was allowed.
Using IDE exclusion criteria to better understand the Lutonix registry results, Karnabatidis stated that the primary safety endpoint of freedom from access circuit-related serious adverse events was 94.9% at 30 days. Concerning the registry’s efficacy endpoint, TLPP was 85.1% at 180 days—the “highest” reported when compared with the original dataset. Karnabatidis concluded that often DCB trials are impacted by procedural variables such as inflation time, variations in dose when delivering drugs and excipients and patient population differences. For these reasons, it is challenging to compare DCB trials, he said, underscoring the importance of future randomised controlled trials in this area.
As a champion of innovation and forward movement in his chosen field of interventional radiology (IR), Patrick Haage’s career is no less a reflection of this ideology. With an interest in vascular access, state-of-the-art imaging technologies and artificial intelligence (AI), Haage’s research throughout his career has looked to steer many domains toward progress. Haage is also active in education on a national and international level through leadership roles within multiple scientific conferences and as a founding member of the European Board of Interventional Radiology (EBIR). Set to receive the Distinguished Fellow award at this year’s Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14– 18 September, Lisbon, Portugal), Haage speaks to Interventional Newsto share key moments from his career so far.
What attracted you to a career in IR?
During my medical studies, I developed an interest in less invasive surgical procedures that enable substantial interventions through small incisions. Simultaneously, I was deeply impressed by the scope of radiology as a field and its potential for interdisciplinary and multidisciplinary collaboration. As a radiologist, one has the unique ability to both diagnose a disease and offer therapeutic interventions. The opportunities presented by this discipline appeared to be the ideal path forward for me at that time, and I am happy to affirm today that it was indeed the correct decision. In my view, interventional radiology (IR) offers an unparalleled blend of innovation, technology, patient care, problem-solving, diversity, and constant advancement.
Who were your mentors?
Throughout the years, professor Rolf W Günther, former chairman of radiology at the Rheinisch-Westfälische Technische Hochschule (RWTH) Aachen University in Aachen, Germany, has been a mentor of mine, having previously been my academic teacher and later friend. Professor Dierk Vorwerk Klinikum Ingolstadt in Ingolstadt, Germany, who is the former head of IR at RWTH Aachen University who also supported me in my clinical and scientific development from day one.
Could you describe a particularly memorable case of yours?
There are many cases that have stayed in my memory. Every single event, whether positive or negative, has contributed to my development. The combination of these experiences has shaped me into the person I am today.
I have been very fortunate to never have permanently harmed a patient due to an avoidable complication over all these years, even in difficult situations that I encountered for the first time. Therefore, every procedure that I was allowed to perform as lead interventional radiologist for the first time was memorable—my first dialysis patient, my first gastrointestinal bleed, my first cava filter, my first thrombectomy, my first transjugular intrahepatic portosystemic shunt.
I also had the great fortune to be the first interventional radiologist in Aachen to insert an aortic prosthesis endovascularly. In collaboration with vascular surgeons at my centre, we spent a long morning in the angiosuite successfully inserting this prosthesis. I am still amazed at how confidently the team and I took on this challenge. This is not only a matter of attitude but perhaps also the privilege of the young.
Having been involved in several CIRSE committees for many years, how has the programme adapted to scientific innovation and what key developments stick out in your memory of previous congresses?
CIRSE has a long tradition of adapting its programmes to scientific innovation by incorporating the latest advancements in IR and related fields into its congresses and events. This includes hot-topic symposia, hands-on workshops, and presentations on emerging technologies, techniques, and research in the field.
Key developments that stick out in my memory from previous CIRSE congresses include the introduction of ever-new minimally-invasive procedures, paired with advancements in imaging technologies, breakthroughs in the treatment of emergency, tumour and paediatric conditions. Particularly exciting has been the implementation of prostatic artery embolization and more recently musculoskeletal embolization and its direct impact on patient well-being.
The integration of artificial intelligence (AI) and machine learning in IR practices will significantly impact the way interventional radiologists diagnose and treat patients. I believe that this technology will ultimately lead to improved outcomes, time and money savings and improved patient care. In the end however, the patient-doctor relationship will remain as an non-negotiable part of the diagnostic, and especially therapeutic, road to restitution.
As one of the founding members of EBIR, how important is the standardisation of education for IR and how do you feel the EBIR examination has influenced IR practice?
Ensuring that practitioners of IR possess the required knowledge and skills to deliver top-notch patient care is essential. EBIR plays a vital role in this process by establishing educational standards, creating curricula, and conducting examinations to evaluate the proficiency of IR specialists. Since 2010, the EBIR exam has had a hugely beneficial impact on IR practice in various ways. Firstly, it guarantees a consistent level of knowledge and expertise among IR specialists, throughout not only Europe, but worldwide, fostering uniformity and excellence in patient care. Secondly, the exam promotes ongoing learning and professional growth among interventional radiologists as we strive to meet the high standards set by the EBIR. Additionally, the EBIR exam offers a respected credential that showcases the proficiency and competency of IR specialists to patients and other healthcare professionals. This has boosted the reputation of IR as a specialised field within radiology and attracts talented individuals to pursue a career in IR.
Overall, the standardisation of education through the EBIR exam has positively influenced IR practice by campaigning for excellence, ensuring know-how, and elevating the overall standard of care provided to patients. The newly established European Certification for Endovascular Specialists (EBIR ES) serves as a validation of an interventional radiologists’ knowledge, experience, and competency in performing complex endovascular procedures, and thus not only enhances our credibility and reputation, but also radically increases our visibility for patients, colleagues, and healthcare institutions.
You are also a co-founder of the European Conference on Embolotherapy (ET) conference which just recently commenced. What were the priorities of this year’s meeting and were there any particularly exciting data releases?
Founded by Christoph Binkert in 2019— with a little help from myself —ET is typically focused on in-depth discussion of the latest research findings, advancements in embolization procedures, updates on imaging technologies for embolotherapy, and the management of complex cases using embolization techniques.
At the 2024 ET meeting in Vienna, some of the data releases and presentations included new research on the efficacy of embolization procedures, advancements in imaging technologies for embolotherapy, and updates on the management of complex cases using embolization techniques. Some of the main foci this year were the treatment of haemorrhoids, lymphatics, endoleaks and musculoskeletal pathologies. The newly added “deep-dive” sessions intensified the teaching and learning aspect for attendees.
Several of your recent research papers have considered the place of AI and machine learning in IR. How do you feel these technologies will interact with IR in the future? Should interventional radiologists have any reservations in embracing this technology?
AI and machine learning have the potential to greatly impact our field by improving efficiency, accuracy, and outcomes. These technologies can help in image interpretation, treatment planning, and decision-making. In the future, AI algorithms and machine learning should play a significant role in IR by automating routine tasks, assisting in complex procedures, and providing personalised treatment options. Interventional radiologists should not have reservations in embracing AI and machine learning technology. Instead, they should see it as a tool that can enhance and improve their existing skills. Nevertheless, it is important for interventional radiologists to receive proper training on how to effectively integrate these technologies into their practice. Plus, they should also be aware of the limitations and potential biases of AI algorithms, and use them as a supplement to their own expertise rather than a replacement.
With decades of experience in IR education, what, in your opinion, is the most underserved/underresearched area of IR?
Generally, I find the development of our community and society in the last 20 years as breathtakingly positive. Interventional radiologists are constantly reinventing themselves by opening up multiple intelligent and less invasive treatment possibilities that are beneficial to the patient. If I should name one area I find underserved and in need of more attention it is paediatric IR.
Paediatric patients have unique anatomical and physiological considerations that require specialised care and tailored interventions. As of now, there is a limited amount of research and few dedicated training programmes focused on paediatric IR compared with adult programmes. In my years as scientific programme committee member and chairman I have tried to push paediatric IR training into attention. This development should be continued.
What piece of advice would you give to early-career interventional radiologists today?
As I’ve mentioned, IR is rapidly evolving. Thus, focus on continuous learning and professional development is key. Actively attend national and international conferences and workshops. Pursue additional training and certifications and advance your skills. Engage in research and academic activities, publish scientific papers and present your work at conferences to contribute to the advancement of IR. This will give you the benefit of expanding your network. Seek mentorship and guidance as you navigate your early career. Finally, always welcome innovation and technology, stay ever curious so that you can deliver cutting-edge care to your patients. Don’t let yourself be changed, be part of the change.
What are your interests and hobbies outside of your career?
Outside of my work I enjoy spending time with my family (my two sons Noah and Jona, and wife Nadja) or my friends. I like to travel, particularly to Asia and Korea. I also enjoy sports such as skiing or tennis, and driving fast cars—or old ones, (Porsche 911, Volkswagen Beetle)—and going to big events, such as rock concerts and soccer games.
Findings from a post-hoc analysis of Lutonix arteriovenous (AV) global registry data
Interview with Philip Dombrowski (Cape Cod Hospital, Hyannis, USA), the interventional radiologist who saved Sebastian Junger—journalist and author of The Perfect Storm—from a rare pancreatic aneurysm
Findings from a post-hoc analysis of Lutonix arteriovenous (AV) global registry data
Interview with Philip Dombrowski (Cape Cod Hospital, Hyannis, USA), the interventional radiologist who saved Sebastian Junger—journalist and author of The Perfect Storm—from a rare pancreatic aneurysm
Updated findings from the COLLISION and CROSSFIRE trials
BioCardia has submitted a 510(k) for approval of its patented Morph DNA steerable introducer sheath to the US Food and Drug Administration (FDA).
This product family is intended to provide a pathway through which medical instruments, such as balloon dilatation catheters, guidewires, or other therapeutic devices, may be introduced into the peripheral vasculature or chambers and coronary vasculature of the heart.
The filing for approval of this product family follows the FDA approval of BioCardia’s Helix biotherapeutic delivery Morph DNA guide system and its Avance transseptal steerable introducer, both of which incorporate Morph DNA technology.
Morph DNA designs enable the tensioning elements in the catheter to rotate around the catheter shaft, allowing consistent catheter performance in any direction, BioCardia said in a press release. The DNA name reflects this design, as these tensioning elements appear as a double helix like that in a strand of DNA. This design is intended to enable smooth navigation and prevent “whip,” when the build-up of mechanical forces in the device causes a catheter to suddenly jump from one orientation to another.
According to BioCardia, the market for this product family is measured in millions of procedures per year, including cardiac interventions such as structural heart procedures and electrophysiology procedures, peripheral vascular interventions including renal interventions, endovascular aortic repair, and carotid artery interventions. The product family approval is intended to span the range of sizes and lengths to accommodate many of these procedures.
“All of the biotherapeutic interventions we support for treatment of heart failure, refractory angina, and acute myocardial infarction are expected to utilise this same introducer technology platform,” said Peter Altman, BioCardia’s president and chief executive officer. “This submission for approval of the Morph DNA Steerable Introducer Sheath product family for broader clinical usage in other complex clinical procedures is in line with our mission to enable and advance therapeutic solutions for cardiovascular and pulmonary diseases.”
China’s National Medical Products Administration (NMPA) has granted a Class III Medical Devices Certificate of Registration for the msRDN radiofrequency renal denervation system (SyMap Medical).
The msRDN system consists of a disposable renal artery radiofrequency ablation catheter, a console with both electronic stimulation and radiofrequency ablation function.
According to SyMap Medical, the system can accurately map the renal nerve sites to selectively denervate renal sympathetic nerves, and has a good match with the anatomical shape of the renal artery with additional flexible manipulability, guiding function, contrast injection, stimulation/mapping, temperature-controlled ablation and manual irrigation. Thus, the system can provide real-time feedback before, during and after a renal denervation procedure in order to achieve selective ablation of renal sympathetic nerves.
The safety and efficacy of the msRDN system for treating patients with uncontrolled hypertension have been demonstrated by the SMART trial, which was led by Huo Yong (Peking University First Hospital, Beijing, China), Ge Junbo (Zhongshan Hospital, Fudan, China) and Sun Ningling (Peking University People’s Hospital, Beijing, China). The msRDN therapy achieved the goals of reducing the drug burden of hypertension patients and controlling office systolic blood pressure <140mmHg, with only four targeted ablations per renal main artery. The results have been published in The Lancet/eClinicalMedicine.
NMPA described the msRDN system as, “the world’s first renal artery radiofrequency ablation product that can map renal nerves, can provide accurate ablation positions for renal sympathetic denervation, and can also provide effective feedback during and after the procedure to examine the immediate effect of renal sympathetic denervation, meeting the needs of renal denervation in clinical practice.”
Centerline Biomedical has announced that the Intra-Operative Positioning System (IOPS) Viewpoint Catheter has received US Food and Drug Administration (FDA) 510(k) clearance. The Viewpoint Catheter is the most recent addition to the company’s patented IOPS portfolio.
Viewpoint Catheter, a low profile 6Fr catheter, is designed for precision access to provide three-dimensional (3D) navigation feedback to clinicians. When Viewpoint Catheters are used in combination with the proprietary algorithms of the IOPS software, clinicians can clearly visualise endovascular tools in real-time and reduce their dependency on fluoroscopy systems. The result is state of the art image-guided, real-time navigation designed to revolutionise the way endovascular procedures are performed. This is achieved while reducing exposure to harmful radiation emitted from the X-ray fluoroscopy systems that are typically used to see vessels during these procedures.
“Development of our second-generation portfolio for IOPS has been the top priority for Centerline Biomedical. Viewpoint Catheters were developed with input from leading clinicians to best meet their procedure needs,” said Gulam Khan, chief executive officer of Centerline Biomedical. “Our company continues to re-envision the field of endovascular interventions, developing technologies designed with the express purpose of improving outcomes for both providers and patients.”
Gravity Medical Technology has announced the launch of its next-generation stroke treatment devices: the Neutron aspiration catheter and the Supernova stent retriever. Early adoption has demonstrated the successful treatment of more than 60 patients worldwide, according to a company press release.
“Team Gravity is attempting to address one of the most important public health challenges of this generation,” said Dileep Yavagal (University of Miami, Miami, USA), principal investigator of the GRASSROOT trial.
“Gravity’s life-saving technology has demonstrated its ability to remove clots from the brain, which brings a much-needed technology to the rest of the world,” added Tudor Jovin (Cooper University, Camden, USA).
Leveraging advanced artificial intelligence (AI)-assisted computer simulation, Gravity claims to be at the forefront of developing next-generation devices that enhance effectiveness in treating stroke patients across various pathologies, making them substantially more accessible globally.
The Supernova stent retriever’s innovative design enhances the capture and removal of hard fibrin-rich (white) clots, which tend to present more in non-Caucasian populations. The Neutron aspiration catheter, with its enhanced kink resistance, ensures consistent aspiration power to effectively remove blood clots.
The release goes on to note that the Supernova device has shown clinically successful results in the GRASSROOT trial, presented at the iCURE/World Live Neurovascular Conference (WLNC) meeting (8–10 May, Istanbul, Turkey) earlier this year. The Supernova has demonstrated a high rate of first-pass successful recanalisation as well as achieving highly favourable revascularisation outcomes, according to Gravity.
“Stroke remains a leading cause of death and disability worldwide, and current technologies are not accessible to many patients in need,” said Gravity chief executive officer Kunakorn Atchaneeyasakul.
Gravity states that it aims to bridge this gap by bringing cutting-edge stroke treatment technologies to patients across the globe.
Both Supernova and Neutron have received approval from the Thai Food and Drug Administration (FDA) and are undergoing further clinical trials globally to validate their effectiveness and safety across diverse populations.
CALCIO is a prospective, observational cohort study that is collecting real-world data on the use of intravascular lithotripsy (IVL) with the Shockwave Medical IVL system (Shockwave Medical) to disrupt vascular calcifications in patients with CLTI. The study was initiated and is co-chaired by Raman Uberoi (The John Radcliffe Hospital, Oxford, UK), Peter Reimer (Municipal Clinic Karlsruhe, Karlsruhe, Germany) and Christoph Binkert (MRI Bahnhof Oerlikon, Zurich, Switzerland).
Once patient enrolment is complete, an additional two years will be dedicated to the collection of patient follow-up data to ensure the study meets its objectives. Currently, there are several sites enrolled from Germany and the UK. More centres from Germany, the UK, France, Austria, Italy, Greece and Canada are in the recruitment process and are expected to join soon.
Next Research, CIRSE’s contract research organisation (CRO), is the administrator of CALCIO and is managing the study on a day-to-day basis, the press release states. Their team asked the CALCIO initiators and principal investigators to share their thoughts on the study’s significance, their experiences so far, and the importance of generating more clinical evidence. They also encouraged other centres to participate in this research effort.
Binkert shared: “I think CALCIO is an important registry because it collects real-world data on a very severe problem, as patients with CLTI need to get revascularisation and if they have very calcified arteries, this is a big challenge and the current evidence is not sufficient.”
Reimer said: “As interventional radiologists, we should learn to collect outcome data that looks at the long-term prognosis of patients. This is exactly what we will do with the CALCIO study. We’ll look at the amputation rate and wound healing through the use of IVL. That is why we should all try to enrol as many patients as possible in the CALCIO study.”
Joo-Young Chun, principal investigator (St. George’s University Hospital, England, UK), highlighted what makes CALCIO so special: “I am very excited to be part of the study. What makes CALCIO quite unique is that it takes real-world patients with very wide inclusion criteria and very few exclusion criteria. I am also happy that the outcome measures are clinically focused. We are talking about CLTI patients, so these are patients with the risk of losing their legs, and we are looking at wound healing and also amputation-free survival. We are not necessarily focusing on how the lesion performs with IVL, but on how the patient does. Another exceptional thing about CALCIO is that we are looking at quality of life, which is quite unusual in such studies, and it would be very interesting to see how patients perceive their treatment and how it is affecting their quality of life.”
Raghuram Lakshminarayan (Hull University Teaching Hospital, England, UK) principal investigator, emphasised the significance of addressing calcification: “Calcification is a huge problem for the medical community, especially with peripheral arterial disease. We saw this in the pulmonary system, and we now realise that this is a major issue in peripheral arterial disease, and IVL has come as a new technique in order to try to deal with this problem of calcification in peripheral arteries. CIRSE has set up this unique registry to look at exactly how IVL is going to work over a period of time. There have been a lot of studies, but we want to have a large population to look at over a long period of time for us to get to the bottom of how IVL modifies calcium and the outcomes when we treat these patients. CALCIO is a great registry, and I think you should add every patient with CLTI to this study!”
In July, the most popular stories from Interventional News included a survey highlighting a significant lack of awareness among women surrounding uterine artery fibroid treatment options; outcomes of a secondary investigational device exemption (IDE) analysis of the aVeNEW trial data; results from the EMBO-01 trial as presented at 2024 Society of NeuroInterventional Surgery (SNIS) annual meeting and several more.
Following her presentation on uterine artery embolization (UAE) for fibroids at the Global Embolisation Oncology Symposium Technologies (GEST; 16–19 May, New York, USA), Abeer AlDhawi (Riyadh, Saudi Arabia), describes the “significant relief” that can be provided to patients through this minimally invasive procedure.
A recent survey conducted by The Harris Poll on behalf of the Society of Interventional Radiology (SIR) has revealed that more than half (53%) of women diagnosed with uterine fibroids were primarily offered a hysterectomy. In contrast, fewer than 20% were presented with less invasive alternatives such as over-the-counter non-steroidal anti-inflammatory drugs (NSAIDs; 19%), uterine fibroid embolization (UFE; 17%), oral contraceptives (17%), and endometrial ablation (17%).
At the recent Endo Vascular Access (EVA) meeting (14–15 June, Patras, Greece), Ziv Haskal (University of Virginia School of Medicine, Charlottesville, USA) spoke to Timothy Clark (Perelman School of Medicine at the University of Pennsylvania, Philadelphia, USA) about what they referred to as the “gold rush” of thrombectomy devices for large-calibre blood vessels.
Microbot Medical has announced that Baptist Hospital of Miami, USA—which includes Miami Cardiac & Vascular Institute and Miami Cancer Institute—has completed its first clinical procedure in a patient utilising the Liberty endovascular robotic surgical system.
“Study design is critically important when interpreting outcomes,” said Bart Dolmatch (Mountain View Hospital, Mountain View, USA) in his evaluation of the “disconnect” between target lesion primary patency (TLPP) and access circuit primary patency (ACPP) analysing AVeNEW study data at this year’s Endo Vascular Access (EVA) meeting (14–15 June, Patras, Greece).
Arsenal Medical has announced that NeoCast—a first-of-its-kind, shear-responsive liquid embolic material designed for deep distal penetration—met its primary feasibility and safety endpoints in the open-label, multicentre, prospective EMBO-01 clinical trial. These data were presented earlier today at the 2024 Society of NeuroInterventional Surgery (SNIS) annual meeting (22–26 July, Colorado Springs, USA).
A recent study suggests that endovascular treatment of the common femoral artery (CFA) is associated with an increased rate of long-term CFA-specific reintervention, regardless of indication. Nicholas Wells, a medical student at Yale School of Medicine in New Haven, USA, presented this and other key findings from a tertiary care centre analysis of open and endovascular treatment of the CFA at the 2024 Vascular Annual Meeting (VAM; 19–22 June, Chicago, USA).
Inspire Medical Systems has secured the CE mark certification for full-body magnetic resonance imaging (MRI) compatibility for its Inspire IV neurostimulator device under the European Union’s (EU) medical device regulation (MDR).
The procedure was performed by Peter Stratil (RIA Endovascular, Denver, USA) and, according to the company, marks a significant advancement in minimally invasive interventions for UAE.
A press release notes that XO Cath, engineered with a laser-cut metal hypotube, was designed to provide optimal pushability and torque control in tortuous and distal vasculature. The recent case displayed the capabilities of these design features and expanded the potential for optimising radial access procedures, the release continues.
In addition to strong pushability and trackability, Transit Scientific shares that the 2F XO Cath offers an inner lumen size of 0.021”, providing high-quality imaging and allowing for broad embolic compatibility without sacrificing a low profile.
Stratil’s recent procedure utilising XO Cath 2F 021” lumen with a bern-shaped tip in a UAE procedure demonstrated the microcatheter’s performance via transradial access, without the need for a supporting catheter. Transit Scientific states that this feature can be especially valuable when treating patients with small or delicate radial vasculature where a support catheter may create procedural complications or patient harm.
Navigating from the left forearm through the aorta, into the left iliac artery, and the left uterine artery, XO Cath provided strong pushability and torque responsiveness, the company reports. It adds that the catheter provided high-quality imaging and successful embolic sphere delivery for successful treatment.
Commenting on the procedure, Stratil remarked: “The torquability and pushability of XO Cath were impressive, especially without the use of a base catheter. It tracked very nicely over the guidewire to the treatment site. Additionally, I was able to achieve very good injection through this 2F, 0.021” lumen microcatheter.”
Transit Scientific’s president and CEO commented: “The successful application of XO Cath via radial access without a support catheter underscores its versatility and potential to optimise patient care in a wide range of interventional procedures. Transit Scientific remains committed to driving innovation in the field of endovascular interventions, empowering clinicians like Dr Stratil with transformative technologies.”
The company advises that its XO Cath microcatheter is available in both 2F 0.021” inner diameter for use with standard 0.014” and 0.018” guidewires, and 2.6F 0.027” inner diameter for use with standard 0.014”, 0.018”, and 0.021” guidewires. Both microcatheters are offered with either a straight or bern-shaped tip and are available in 90cm, 110cm, 130cm, 150cm, 175cm, and the class-leading 220cm working lengths for radial access procedures.
Recor Medical's Paradise ultrasound renal denervation system
Recor Medical’s Paradise ultrasound renal denervation system
The first patients in the USA have been treated in Recor Medical’s Global Paradise System US Post Approval Study (US GPS), a real-world study gathering data on the long-term safety and effectiveness of ultrasound renal denervation.
Antonio Gutierrez is the primary study investigator at Durham VA Medical Center (Durham, USA), the first US site in the study to enrol and treat patients.
The study will focus on gathering real-world safety and effectiveness data over five years from up to 1,000 patients, collaborating with research centres to help advance diversity and health equity within clinical trials.
Building upon the substantial clinical data generated to-date, which led to US Food and Drug Administration (FDA) approval of the Paradise system in November of 2023, the study will collect data on patients who undergo treatment with the Paradise system.
The study seeks to enrol patients from historically underserved populations in clinical trials, including racially diverse groups, women, and the elderly, along with those having significant comorbidities like chronic kidney disease and diabetes.
Patients will be asked to measure their blood pressure throughout the study, including measuring blood pressure out of the clinic setting using a home monitoring device provided by the study. Participants will also be asked about their quality of life, health, sleep and emotions. Additional demographic data, medical history and socio-economic data may also be collected.
“New therapies to lower blood pressure are desperately needed. Following a rigorous set of randomised clinical trials, each one demonstrating that ultrasound renal denervation is a safe and effective treatment for hypertension, we enter the next stage with great excitement,” said study principal investigator Naomi Fisher (Harvard Medical School, Cambridge, USA and Brigham and Women’s Hospital, Boston, USA). “These milestone treatments mark the beginning of a critical extension—using ultrasound renal denervation in the real world, focusing especially on patients who have been underrepresented in trials to date.”
Recor Medical’s Paradise uRDN system is an ultrasound-based renal denervation technology designed to lower blood pressure by denervating overactive sympathetic nerves surrounding the renal arteries in patients whose hypertension is not controlled by medications alone.
“The launch of the US GPS study for the Paradise ultrasound renal denervation system is an important step in collecting real-world data on the blood pressure lowering impact ultrasound renal denervation can provide,” said Recor president and CEO Lara Barghout. “Patients with uncontrolled hypertension face potentially catastrophic chronic diseases, and new solutions are vital to help them achieve blood pressure control and realise a healthier future. We are proud to be providing this opportunity to Veterans in the US, and we hope to make a meaningful impact on their lives.”
“The US GPS study will build upon the wealth of clinical evidence Recor has generated to show the continued safety and efficacy of the Paradise ultrasound renal denervation system in a real-world setting,” added Recor’s chief clinical officer Helen Reeve-Stoffer. “Long-term data on the safety and durability of ultrasound renal denervation will help further reinforce the impact the therapy can have in lowering blood pressure, and how it can be an important option in the fight to control hypertension.”
“Study design is critically important when interpreting outcomes,” said Bart Dolmatch (Mountain View Hospital, Mountain View, USA) in his evaluation of the “disconnect” between target lesion primary patency (TLPP) and access circuit primary patency (ACPP) analysing AVeNEW study data at this year’s Endo Vascular Access (EVA) meeting (14–15 June, Patras, Greece).
AVeNEW, a prospective and randomised study, compared outcomes using the Covera (BD) vascular covered stent versus percutaneous transluminal angioplasty (PTA) for the treatment of stenotic lesions in the venous outflow of upper-extremity arteriovenous fistulas (AVFs). Composed of 280 patients enrolled at 24 sites in the USA, Europe, Australia, and New Zealand, 142 patients were randomised to treatment with Covera and 138 patients to PTA.
Alongside criteria stipulating that enrolled patients have a 50% or greater target stenosis and evidence of dysfunction, Dolmatch noted that non-target stenoses were also allowed, but could only be treated with PTA. Primary outcomes were 30-day safety and six-month TLPP, powered to test whether TLPP after covered-stent placement was superior to PTA alone. Twelve-month TLPP and six-month ACPP were also evaluated while additional clinical outcomes were observed through to two years.
Dolmatch stated that their results showed comparable and non-inferior safety for the PTA group compared to the group treated with the covered stent, while the covered stent group had superior TLPP and fewer target-lesion reinterventions through to 24 months. In terms of efficacy, he added that they saw a “very significant” improvement of TLPP for the covered stent group, which was 30% more than TLPP for the PTA group at six months. “However, that’s the target lesion,” he said, stating that when they looked at circuit patency, it appeared to be numerically better for patients who received the covered stent, but not statistically superior.
“So you have to wonder, why was TLPP superior, yet ACPP was not statistically better for the covered stent group?” Answering this question, Dolmatch suggested that the answer is largely related to the study protocol which allowed enrolment of patients with non-target stenoses that were found in roughly one third of all patients enrolled in the AVeNEW trial. Per protocol, non-target stenoses could only be treated with angioplasty. While this reduced primary circuit patency for both groups, there were randomly more non-target stenoses in the covered stent group. Frequent and early recurrence of non-target stenoses after PTA led to a disproportionally greater loss of circuit patency in the Covera group, even though the target treatment site had better patency with the covered stent.
“By allowing enrolment of patients with non-target stenoses treated only with angioplasty, ACPP was reduced in both groups,” Dolmatch concluded. In the Covera group, more patients were had non-target stenoses treated with PTA, which had a greater impact on ACPP when compared ACPP for the angioplasty group. He added that, although circuit patency was numerically greater for the Covera group, it did not reach statistical significance due to the “random and disproportionately higher number of non-target stenoses in the covered stent group”.
He offered pros and cons for including patients with secondary stenoses in this type of randomized, prospective clinical trial. By including patients with non-target stenoses the AVeNEW study was closer to a “real-world” experience since many dysfunctional AVFs will often have more than one stenosis. Furthermore, faster enrolment was possible by including patients with non-target stenoses. But the downside was that primary circuit patency was more quickly lost due to non-target stenosis even though the target lesion had superior outcome with the covered stent.
Exploring how this study could have been designed to better address the impact of target lesion treatment upon circuit patency, Dolmatch first suggested simply not including patients with non-target stenoses. Alternatively—and perhaps more realistically—he recommended treating both target and non-target stenoses with the mode the patient was randomised to, PTA or covered stent.
Dolmatch reiterated the importance of study design when interpreting outcomes, and believes that the markedly improved TLPP with the covered stent reiterates the benefit using covered stents in AV access circuits. He concluded by stating that more data is on the way, with results from the post-approval AVeNEW study of 100 consecutive patients treated with the Covera covered stent to be presented at this year’s Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress (14–18 September, Lisbon, Portugal).
Arsenal Medical has announced that NeoCast—a first-of-its-kind, shear-responsive liquid embolic material designed for deep distal penetration—met its primary feasibility and safety endpoints in the open-label, multicentre, prospective EMBO-01 clinical trial. These data were presented earlier today at the 2024 Society of NeuroInterventional Surgery (SNIS) annual meeting (22–26 July, Colorado Springs, USA).
“NeoCast has the potential to be a gamechanger for liquid embolics,” said Lee-Anne Slater (Monash Health, Melbourne, Australia), the principal investigator for the EMBO-01 trial who presented findings at SNIS 2024. “The product was easy to handle and performed consistently and reproducibly during injection while providing excellent visibility during and post-procedure, unlike currently available options. Early results show that NeoCast has the potential to fill a treatment gap with a tool that’s straightforward for clinicians to use and will ultimately benefit patients; I am encouraged by its possibilities in other middle meningeal artery indications.”
An Arsenal press release states that NeoCast “stands alone” in clinically demonstrating predictable and well-controlled vascular occlusion. The late-breaking data presented today, according to Arsenal, are further bolstered by an additional presentation highlighting preclinical study results showing that it occluded approximately five times more vessel branches with improved radiopacity, compared to the market-leading liquid embolic, in swine kidneys. The company describes NeoCast as a next-generation, solvent-free, non-adhesive liquid embolic that can enable the significant distal penetration of hypervascular brain tumours.
“These emerging preclinical and clinical data are exciting, as they clearly demonstrate the potential for NeoCast to be an optimal liquid embolic agent for the treatment of neurovascular conditions that require distal penetration of the targeted vasculature,” said EMBO-01 medical monitor Dave Fiorella (Stony Brook University Medical Center, Stony Brook, USA). “Middle meningeal artery embolisation for the treatment of chronic subdural haematoma [cSDH] is the application that immediately comes to mind. The existing clinical data have suggested that distal penetration into the meningeal circulation is associated with faster and more complete cSDH resolution. Moreover, this agent has the additional advantage of not incorporating an inflammatory solvent or inducing a thermal reaction upon polymerisation. This characteristic should allow NeoCast embolisation procedures to be carried out under conscious sedation rather than general anaesthesia in many or most patients, as we would expect that the agent would not create any pain or discomfort during the infusion.”
“This is an important milestone in the clinical development of NeoCast as a differentiated solution for middle meningeal artery embolisation and other conditions where deep distal penetration is beneficial,” added Upma Sharma, chief executive officer and president of Arsenal. “NeoCast is making the leap from legacy products that utilise technology developed decades ago. We appreciate Dr Slater and our other clinical investigators; their commitment and hard work have been crucial to this first experience.”
Imperative Care has announced that late-breaking data from the Imperative trial were presented recently at the ongoing Society of NeuroInterventional Surgery (SNIS) annual meeting (22–26 July, Colorado Springs, USA). The prospective, multicentre clinical trial evaluated the clinical benefits of the Zoom reperfusion system, including aspiration with 0.088-inch catheters, for the treatment of ischaemic stroke.
The aforementioned data were presented by William Mack (University of Southern California, Los Angeles, USA), co-principal investigator of the Imperative trial.
“The observed data showed all three prespecified performance goals were met,” said Mack. “These data suggest a lower rate of rescue therapy than prior thrombectomy trials, and may demonstrate that intracranial positioning of a super-large-bore catheter could influence or reduce the need for stent retrieval rescue therapy as well as decrease costs. Additionally, the very low rate of symptomatic intracranial haemorrhage coupled with high rates of reperfusion are promising. I look forward to the potential implications for my practice and the patients I treat.”
The Imperative trial evaluated 260 patients who met inclusion and exclusion criteria and were treated across 26 US institutions from October 2021 to March 2024. Prespecified performance goals were established in conjunction with the US Food and Drug Administration (FDA) and 254 patients completed follow-up at 90 days.
Results from the trial demonstrated that the core-lab adjudicated rate of modified thrombolysis in cerebral infarction (mTICI) ≥2b reperfusion within ≤3 passes—without the use of any additional thrombectomy devices as rescue therapy—was achieved in 82.2% of patients (213/259). According to Imperative, this is similar to prior trials used to support US FDA 510(k) clearance for reperfusion indications (82.4%; 1,832/2,246). In addition, stent retrieval rescue therapy was used to achieve mTICI ≥2b reperfusion in only 5.5% of cases (13/238).
Data also showed that the median time from groin puncture to mTICI ≥2b reperfusion using the Zoom reperfusion system was 19 minutes. Additionally, the core-lab adjudicated rate of symptomatic intracranial haemorrhage was 2.3% (6/260), which is lower than the rate of prior trials (4.7%; 116/1,777), and the rate of independently adjudicated dissection and vessel perforation was 1.2% (3/260), which is similar to prior trials (1.3%; 14/933).
“We are pleased with the preliminary results of the Imperative trial,” said Fred Khosravi, chairman and chief executive officer of Imperative. “Our mission to elevate care for patients suffering from stroke and other devastating vascular diseases extends beyond the operating room. We are happy to advance the field through our commitment to validating our innovations with robust clinical data.”
“At Imperative Care, we are focused on developing technologies designed for intracranial access, with the goal of enabling physicians to perform better procedures with faster clot removal using fewer devices, as demonstrated in previous clinical studies of the Zoom stroke solution—and now further supported by initial findings from the Imperative trial,” added Ariel Sutton, general manager of Imperative’s Stroke business. “These data suggest this approach is poised to be better across a number of endpoints. We look forward to our continued efforts to elevate stroke care through our sustained commitment to clinical evidence and meaningful innovation with the goal of improving patient outcomes.”
MicroVention has announced the recently published results of the CLinical EValuation of WEB 17 Device in Intracranial Aneurysms (CLEVER) one year effectiveness results for ruptured and unruptured aneurysms. The CLEVER study was a multicentre, prospective study evaluating the WEB 17 system in ruptured and unruptured aneurysms to understand the safety and effectiveness of the newest and smallest WEB system.
The study comprised of 163 patients across 17 European centres with results concluding that WEB 17 is just as safe and effective as previous WEB generations with a low complication rate and no rebleeds at 30 days and one year. The adequate occlusion rate was 86.5% for ruptured aneurysms (73.1% complete occlusion) and 82.4% for unruptured aneurysms (57.1% complete occlusion) at one year follow up. The results of the CLEVER study demonstrate that the WEB 17 system maintains the same efficacy as previous generations of WEB.
Laurent Spelle (Paris Sud University, Paris, France), a contributor from the CLEVER study made the following comments about the WEB technology and the clinical data supporting it: “One-year angiographic results of CLEVER show excellent complete occlusion rates at one year in the population of wide-neck bifurcation aneurysms treated with WEB 17,” said Spelle.
Adam Arthur (The University of Tennessee Health Science Center, Memphis, USA) principal investigator for the WEB-IT Trial, which was the US investigational device exemption (IDE) study to support WEB premarket approval (PMA) in the USA, also commented: “WEB has changed my practice and set a new standard for safety in the treatment of cerebral aneurysms,” said Arthur.
“MicroVention’s WEB aneurysm embolization system is now the most studied intrasaccular device available today, underscoring our commitment to physicians and patients alike to provide innovative, advanced medical device technology coupled with long-term safety and effectiveness,” said Carsten Schroeder, president and CEO, MicroVention. “With over 10,000 units sold in the USA, WEB advances treatment of wide-neck bifurcation aneurysms with one intrasaccular device – clinically proven one and done treatment. We will continue to work side-by-side with leading physicians around the world to identify the evolving needs in patient care, and then transform those insights into innovative technologies that help to save patient lives.”
iVascular has announced that “outstanding” results from the SOL Japan study were recently presented at the Japan Endovascular Treatment (JET) conference (14–16 June, Fukuoka, Japan).
SOL Japan is a clinical trial aimed at evaluating the efficacy and safety of the Luminor 18 drug-coated balloon (DCB) in treating femoropopliteal arteries within the Japanese population.
A press release notes that this pivotal study marks a significant milestone for the Luminor DCB in Japan. The trial has been conducted in collaboration with Medico’s Hirata, a company from Japan that iVascular states has vast experience and knowledge of medical devices.
The SOL Japan study, under the guidance of principal investigator Yoshimitsu Soga from Kokura Memorial Hospital (Kitakyushu, Japan), is a prospective, multicentre, single-arm trial. A total of 122 patients were enrolled, with 57.4% of the participants being diabetic. The study focused on femoropopliteal lesions, presenting a mean lesion length of 11cm.
Key findings from the 12-month follow-up of the SOL Japan study include a primary patency rate of 94.9% and a freedom from target lesion revascularisation rate of 99.2%. In addition, only one patient required revascularisation within the first year.
According to iVascular, these results underscore the high efficacy of Luminor DCB, with only one patient needing reintervention over the course of one year. This confirms that Luminor DCB’s TransferTech coating technology makes the difference, the company adds, making it a top-class therapeutic option for femoropopliteal lesions. iVascular advises that TransferTech is last-generation nanotechnology that ensures minimal drug loss during navigation, fast and high drug transfer, and long retention time.
“Luminor DCB has showcased extraordinary performance in the SOL Japan study, significantly benefiting patients,” Soga stated in a press release. “The data reflect a major advancement in our ability to provide a safe and effective treatment with very low reintervention rate.”
Inspire Medical Systems has secured the CE mark certification for full-body magnetic resonance imaging (MRI) compatibility for its Inspire IV neurostimulator device under the European Union’s (EU) medical device regulation (MDR).
This approval extends the use of Inspire therapy beyond the previously allowed head, neck, and extremity MRI scans. The CE mark approval retroactively applies to all patients implanted with the Inspire IV neurostimulator since 2018. This advancement ensures that these patients can now safely undergo full-body MRI scans, the recent press release details.
Inspire chairman and chief executive officer Tim Herbert said: “Expanding compatible use to include full-body MRI is a significant milestone in our effort to bring Inspire to more obstructive sleep apnoea (OSA) patients who struggle with CPAP [continuous positive airway pressure]. Providing the full range of scan options enables us to better help all current and future patients with their imaging needs.
“This full-body MRI compatibility has been an important benefit for patients in the USA for the past two years, and this new approval will provide the same positive benefit for patients in Europe going forward.”
Inspire Europe managing director and executive vice-president Andreas Henke said: “Until now, concern over future access to MRI had been a barrier for some patients considering Inspire therapy. Compatibility with this important diagnostic tool will provide peace of mind for current and future Inspire patients.”
The therapy is said to be the first and only US Food and Drug Administration (FDA)-approved neurostimulation technology designed to provide a safe treatment for moderate to severe OSA.
GE HealthCare has agreed to acquire the British medical device company Intelligent Ultrasound Group’s clinical artificial intelligence (AI) software unit for up to US$51m.
GE HealthCare intends to integrate Intelligent’s solutions into its ultrasound portfolio. The deal follows GE HealthCare’s acquisition of Caption Health last year and is expected to be closed in quarter four of 2024.
GE HealthCare president and ultrasound and image-guided therapies chief executive officer Phil Rackliffe said: “We are pleased to bring innovative technology from Intelligent Ultrasound into GE HealthCare’s ultrasound portfolio, allowing us to fully integrate these solutions into our systems. This technology and the experts who developed it will help enhance our portfolio of AI-enabled devices and accelerate our pace of development of next-generation AI tools.”
Intelligent Ultrasound has developed the ScanNav Assist AI technology, which powers its SonoLystlive and SonoLyst X/IR solutions. Both solutions are available on GE HealthCare’s Voluson Expert and Voluson Signature ultrasound devices, while SonoLyst is also featured on its Voluson SWIFT.
Intelligent Ultrasound chief operating officer Nick Sleep said: “I really believe that we are at the start of a wave of AI making a profound difference to medical imaging, and especially ultrasound. “Becoming part of the GE HealthCare family will help speed the adoption of this technology and make ultrasound even easier for customers to use.”
Imperative Care has announced US Food and Drug Administration (FDA) 510(k) clearance of its Zoom 6Fr insert catheters, the company’s latest innovation in elevating stroke care and—as stated in an Imperative press release—the first insert catheters developed specifically for ischaemic stroke procedures. The company also recently announced the successful completion of the first case with the Zoom 6Fr insert catheters, which was performed by Dana Tomalty at Huntsville Hospital in Huntsville, USA.
Based on physician feedback, the new Zoom 6Fr insert catheters were developed to be more supportive, more ‘torque-able’ and longer than current vessel selection devices, and are offered in three stroke-specific shapes. These features are designed for faster vessel selection and “uncompromised delivery” of Imperative’s comprehensive 0.088-inch intracranial access technologies—Zoom 88, Zoom 88 Support and Zoom RDL—to the intracranial anatomy.
“Insert catheters used for stroke today are diagnostic catheters that were designed for cardiovascular access more than 30 years ago,” said Ariel Sutton, general manager of Imperative’s Stroke Business. “The Zoom 6Fr insert catheters bring physicians the modern-day tools and technologies that will allow them the opportunity to best care for their patients, bridging the innovation gap of 30 years to today’s standards for stroke treatment. We are deeply committed to working closely with physicians to identify critical gaps in stroke care and providing innovative solutions that bring meaningful benefits to their patients. The introduction of the Zoom 6Fr insert catheters demonstrates our core tenet of clinical partnership, which puts the perspectives of front-line physicians at the centre of our research and development process.”
The Zoom 6Fr insert catheter portfolio consists of the Zoom SIM, Zoom VRT and Zoom VTK technologies—all, according to Imperative, unique in their shape, construction and length, with the goal of helping physicians achieve faster and more reliable intracranial access in a wide range of patient anatomies.
In the first case performed by Tomalty, the Zoom SIM insert catheter was used to quickly select the target vessel and provide 0.088-inch intracranial access from the femoral artery with Zoom 88 in a patient with a challenging anatomy and distal left M2 occlusion. The Zoom SIM provided added stability to navigate Zoom 88 far into the brain and access the clot more quickly. Tomalty then used both Zoom 71 and Zoom 35 to aspirate and remove the clot in only 10 minutes from puncture to reperfusion, resulting in a complete thrombolysis in cerebral infarction (TICI) 3 revascularisation.
“In my experience, navigating the aortic arch can pose a significant challenge in patients with more tortuous anatomy,” Tomalty said. “Due to the unique design and capabilities of the Zoom 6Fr insert catheters, I believe the use of these technologies will help mitigate this challenge and take minutes off my stroke thrombectomy times, allowing me to get the clot out faster.”
At the recent Endo Vascular Access (EVA) meeting (14–15 June, Patras, Greece), Ziv Haskal (University of Virginia School of Medicine, Charlottesville, USA) spoke to Timothy Clark (Perelman School of Medicine at the University of Pennsylvania, Philadelphia, USA) about what they referred to as the “gold rush” of thrombectomy devices for large-calibre blood vessels.
Haskal: Is this truly the “gold rush” in thrombectomy devices?Or does this landscape hold no promise?
Clark: There is no question that the portion of patients who are treated with thrombectomy is a small fraction of the number of patients presenting with deep vein thrombosis (DVT). There are differing estimates—we are currently treating somewhere between 4–12% of DVT patients with thrombectomy—you can look at the data and think that that is appropriate, or you can think that that is vastly underutilising endovascular therapy. In the USA, there is only the Acute venous thrombosis: Thrombus removal with adjunctive catheter-directed thrombolysis (ATTRACT) trial that has level one data, and the ATTRACT trial used a semi-quantitative primary endpoint that the US Food and Drug Administration (FDA) required the investigators to use. So, the Villalta score—like all these symptom severity scores—is semi-quantitative at best, and is still a relatively crude metric to assess and compare outcomes, but it is among the best we have.
Haskal: Clinicians like yourself have been pushing to treat patients with lysis well before ATTRACT. Has the expanded recognition of thrombectomy driven individuals to design devices that make money?
Clark: There is no question that there has been a huge surge in the number of dedicated thrombectomy systems and devices in the last several years, and that’s just the tip of the iceberg. There are many more technologies that are in various phases of development and stages of regulatory approval. Now we are going to have a plethora of devices which will make it difficult to choose. The ATTRACT trial had two devices—AngioJet (Boston Scientific) and Trellis (Covidien; now Medtronic)— one of which is no longer in the market and the other is rumoured to being “sun-setted” by the manufacturer at some point in the future. When this happens, we will have no devices that have withstood the rigours of an investigator-initiated randomised trial, and so this leaves us trying to understand where these currently available and emerging systems fit into providing a treatment solution that doesn’t require an intensive care unit (ICU) bed, transfusion for blood loss, or lytics and the resultant need to escalate the level of care and deal with lytic-related complications. So, we all can agree on the attributes of what a perfect device should do.
Haskal: Cost is a fundamental question here, given the extraordinarily high price of these class of devices. Out of cheaper, faster, and safer, we may be able to do safer and faster. What are your thoughts?
Clark: There have been some medical economic estimates that show that the expensive thrombectomy systems are still cost-effective by reducing length of hospital stay and mitigating, or avoiding altogether, the need for expensive ICU stays. Twenty years ago, it wasn’t uncommon for us to perform venous thrombolysis for DVT and require 72–96 hours of urokinase infusions in the intensive care unit, then also have to transfuse the patient if they had blood loss and manage the puncture site haematomas that would occur.
Haskal:For a long time, clinicians still could not get massive pulmonary embolism (PE) patients treated routinely. Now it is more widespread, there is some cost sensitivity to that, but some still struggle with the idea of 18Fr or larger for leg DVT. Is that a concern, or do you see peripheral devices “amping up” to work with smaller catheters?
Clark: I can remember back when certain vena cava filters were being selected by interventionalists because “it goes through a 7Fr or 6Fr delivery system and I don’t want to put that big 8Fr device in”. Now, endovascular clinicians think nothing of putting in a 13Fr, 16Fr, and even larger devices through the popliteal, femoral and jugular veins. Some people are using a pre-close suture technique to get haemostasis. Others are putting in purse string sutures, holding pressure and hoping that that is going to work—and it typically does. I agree there has been an arms race of sorts in PE treatment with progressive escalation of catheter size. You have one vendor that now is up to 16Fr, another goes up to 24Fr, and newer systems are also very large. There seems to be almost no limit. You can also look to the structural heart field where there are trans-venous structural heart systems that go through a 30-French sheath. So perhaps the PE thrombectomy systems have the capacity to get even bigger providing they can safely traverse the right heart into the pulmonary arteries.
Haskal: Do you think it is beneficial to move towards devices that have mechanical actuators and energy-based systems that might be able to increase efficacy and perhaps reduce blood loss, rather than plain old suction?
Clark: With suction, you are limited because you cannot change physics. If your system is an aspiration system, and the tip of the device becomes occluded by impacted clot, there’s just no longer going to be any movement of the clot. You can’t overcome the force.
Haskal:There is only so much, as you say, that you can do due to physics. We need to see devices that move beyond that. Do you see that lying in the long grass out there for us?
Clark: Yes, I see that. I think the other thing that’s not talked about in this post-pandemic world, is that many practices struggle from staffing shortages. There’s a nursing shortage, and a technologist shortage. In the USA, many large health systems and hospitals are, at the present time, financially underwater. Among the most precious commodities we have is time. For example, PE cases aren’t something we schedule. They are add-on cases done urgently and/or emergently as additions to our already busy schedules. So, if you’re incorporating DVT thrombectomy into your already busy interventional practice, when you bring a patient into the interventional suite for a DVT thrombectomy and you don’t know if that procedure is going to take an hour, two hours, or three hours, that becomes a problem. It becomes a huge problem for workflow and staffing demands. As these technologies evolve, if there are systems that can improve procedural efficiency and enable you to basically predict—with a high degree of certainty—whether you’re going to be able to get that patient’s clot out and flow restored in under an hour with little to no blood loss, then these will be incredibly beneficial.
Haskal:Coming full circle, do you feel that this gold rush is because of data that’s arisen from the PE intervention world? There is certainly a lot of interest in mechanical or mechanical-assisted thrombectomy. What are your projections here?
Clark: What informs what clinicians are using frequently is what they are most familiar with. They get comfortable with a system, they learn its little nuances, they figure out workarounds for limitations of that system and they tolerate those limitations. We all have our go-to systems that we use for certain disease states. I think that is true with DVT and PE, and I think on the educational front—the awareness front—or you could also say the sales and marketing front, certain stakeholders are looking well beyond the interventional suite to other points-of-contact in the care cycle for a patient with DVT and say “how can we make other people aware of these catheter-directed therapeutic options?” They are looking to get in front of the decision-makers, whether they are in the emergency room (ER), in the ICU, or on other parts of the front line of people who are seeing DVT and PE, where they can be very influential in determining whether or not a patient is going to end up seeing an interventionist.
Transit Scientific announces the successful clinical deployment of XO Cath, an embolic delivery microcatheter intended for interventional procedures.
Richard Saxon (North County Radiology Associates, San Diego, USA), performed the inaugural procedure utilising the XO Cath 2.0Fr 130cm microcatheter with a Bern-shaped tip. The prostatic artery embolization (PAE) case involving significant vessel tortuosity demonstrated the microcatheter’s capabilities, a recent press release states, specifically its manoeuvrability while navigating tortuous anatomy.
Saxon accessed the treatment site from the right femoral artery, beginning in the left prostatic artery where he deployed 100 to 300, and 300 to 500um microspheres and then tracked XO Cath to a wedged position. After treating the left prostatic artery, he navigated to the right side through a 5Fr support catheter and finished treatment on the second side.
Saxon commented on the procedure: “The pushability, visibility, and trackability of the XO Cath were notable, enabling precise manoeuvrability even in challenging anatomical conditions. It tracked incredibly well around tight turns and bends, allowing for distal and precise embolic delivery. In addition, the microcatheter’s luminal size allows for strong injection rates and high-quality imaging.”
Jennifer Arnold, president and CEO of Transit Scientific commented: “The successful debut of XO Cath in its inaugural procedure underscores its potential to redefine the standards of care in interventional radiology and interventional oncology. Transit Scientific remains committed to advancing medical innovation and aims to empower clinicians worldwide with transformative technologies like XO Cath.”
Microbot Medical has announced that Baptist Hospital of Miami, USA—which includes Miami Cardiac & Vascular Institute and Miami Cancer Institute—has completed its first clinical procedure in a patient utilising the Liberty endovascular robotic surgical system.
The clinical case was performed shortly after last week’s announcement regarding the participation of Baptist Hospital of Miami as a clinical trial site. Baptist Hospital is the second clinical site to perform a clinical procedure, following the announcement earlier this week of the first clinical case at Brigham & Women’s Hospital in Boston, USA.
The principal investigator at Baptist Hospital of Miami is Ripal Gandhi who performed this clinical case. The trial is part of the investigational device exemption (IDE) for Liberty, and the company expects its results will support the future submission to the US Food and Drug Administration (USA) and subsequent commercialisation.
“We are very excited to have a hospital of the calibre of Baptist Hospital of Miami performing clinical cases. It is very encouraging to see the progress of our clinical study, as within a couple of weeks we now have two sites actively enrolling patients,” commented Harel Gadot, CEO, president and chairman of Microbot Medical.
A recent survey conducted by The Harris Poll on behalf of the Society of Interventional Radiology (SIR) has revealed that more than half (53%) of women diagnosed with uterine fibroids were primarily offered a hysterectomy. In contrast, fewer than 20% were presented with less invasive alternatives such as over-the-counter non-steroidal anti-inflammatory drugs (NSAIDs; 19%), uterine fibroid embolization (UFE; 17%), oral contraceptives (17%), and endometrial ablation (17%). Additionally, 17% of women surveyed “mistakenly” believe that hysterectomy is the only available treatment, a misconception held by over 27% of women aged 18–34.
The survey highlights a “significant lack of awareness” among women regarding uterine fibroids. Approximately 72% of women are unaware of their risk for developing fibroids, despite up to 77% of adult women developing them at some point in their lifetime. The incidence of fibroids is notably higher among women of colour, with Black women experiencing the highest rates.
John C Lipman (Atlanta Fibroid Center, Smyrna, USA)—advisor for the report—emphasised the importance of informing women about all available treatment options. He noted that the survey results indicate a gap in education, as minimally invasive treatments like UFE are not being consistently offered. Lipman criticised the tendency to prioritise surgical options over minimally invasive ones.
“The survey findings, coupled with the low number of women who were offered a minimally invasive treatment like UFE, indicate that women are not being given all of the information they need to make their own healthcare decisions,” said Lipman. “Not offering minimally invasive treatments like UFE in addition to the surgical treatment options is a significant oversight. Women need to be informed about the complete range of options available for treating their uterine fibroids; not just the surgical options as is most commonly done by gynaecologists.”
The survey included over 1,000 women in the USA, including those diagnosed with uterine fibroids, and are part of the report titled ‘The fibroid fix: What women need to know’ which serves as a resource to inform women about minimally invasive treatment options for uterine fibroids.
UFE is a minimally invasive, image-guided, non-surgical, outpatient treatment that is performed by an interventional radiologist. The treatment is often just as effective as other uterine fibroid treatments and doesn’t require the complete removal of the uterus. Even though several studies have noted the long-term efficacy of UFE, this survey shows that women are not learning about UFE from their doctors. Among women who have heard of or are familiar with UFE, only two in five (40%) first heard or learned about the procedure from a healthcare provider.
The survey also found significant gaps in awareness across different demographics. More than half of women aged 18–34 (56%) and 35–44 (51%) reported being unfamiliar with uterine fibroids. Among Hispanic women, 50% were unaware of fibroids, compared to 37% of Black women. Furthermore, 22% of Hispanic women and 36% of Black women incorrectly believe that they are not at risk for developing fibroids, despite being two and three times more common in these groups, respectively. Furthermore, the survey showed that in women with uterine fibroids who are seeking treatment, 48% prioritised prevention of recurrence and 46% proven effectiveness.
“The survey noted deep disparities in awareness and access regarding fibroids and fibroid treatments among Black and Hispanic women, who have a higher risk factor for developing uterine fibroids,” said Robert J Lewandowski (Northwestern Medicine Feinberg School of Medicine, Chicago, USA), president of the SIR. “The data serve as a guiding light for improving physician and patient educational efforts on various treatments to ensure all women, regardless of background, are informed about their risks and the full range of treatment options available.”
UFE involves inserting a thin catheter into an artery and guiding it to the fibroid’s blood supply. Small particles are released to block the blood vessels, causing the fibroid to shrink and die. Most patients can leave the hospital the same day and resume normal activities within a week. Studies show that nearly 90% of UFE patients experience significant or complete symptom resolution.
“Women suffering from fibroids are often given only one treatment option by their gynaecologist—hysterectomy—without being informed of less invasive treatments, like UFE,” said Lipman. “Many patients don’t want a hysterectomy and they’re left to suffer in silence, even though their lives could be transformed back to normal if they only knew about UFE.”
Avicenna.AI has received Medical Device Regulation (MDR) certification for five of its algorithms from British Standards Institution (BSI) Medical Devices—a development that means the company’s product portfolio is fully compliant with the European Union’s (EU) MDR 2017/745, which is now mandatory for medical device companies wanting to provide solutions in Europe.
As a press release from Avicenna.AI notes, the MDR was introduced to update the EU’s regulations for medical devices, addressing safety issues and the recent emergence of artificial intelligence (AI) tools and software as a medical device (SaMD), which did not exist when the old regulations were created. Ensuring MDR compliance is a critical component of obtaining and maintaining CE-mark status, allowing a device to be freely traded in the EU, the release adds.
Compared to the previous Medical Device Directive (MDD), the MDR has a wider scope and more stringent requirements. It emphasises clinical evaluation, post-market surveillance, device traceability, rigorous technical documentation, and risk management, according to Avicenna.AI. These measures aim to enhance patient safety and ensure high standards for medical devices, including AI and software-based solutions.
Avicenna.AI’s products have been certified as Class IIb medical devices, which require a high level of clinical validation. The certified products include the company’s suite of AI tools for neurovascular conditions, as well as its suite of algorithms for vascular conditions.
“Obtaining MDR certification is a significant milestone for Avicenna.AI,” said Stéphane Berger, regulatory manager at Avicenna.AI. “It demonstrates our commitment to meeting the highest standards of medical device safety and performance. This certification not only reinforces our dedication to compliance but also assures our customers of the quality and reliability of our AI product portfolio.”
The company’s newly MDR-certified AI tools include algorithms for intracranial haemorrhage (CINA-ICH), large vessel occlusion (CINA-LVO), quantification of stroke severity (CINA-ASPECTS), aortic dissection (CINA-AD), pulmonary embolism (CINA-PE), and opportunistic cases of pulmonary embolism (CINA-iPE). All of these products are CE-marked as well as being US Food and Drug Administration (FDA)-cleared, the release states.
“Crucially, despite the differences in SaMD regulatory requirements between authorities in the USA and Europe, we are consistently achieving both FDA and CE-mark clearance for our AI products,” Berger added.
Avicenna.AI claims that all of its AI tools are seamlessly integrated into radiologists’ clinical workflow, automatically triggering and reporting algorithm results through the systems already used by clinicians.
A recent press release has stated that this marks a significant milestone, highlighting their adherence to the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Standards of Quality Assurance in Interventional Oncology, a set of standards supported by 42 national and international societies, including the European Cancer Association.
The Hôpitaux Universitaires de Strasbourg was among the early adopters of the IASIOS programme, becoming the second facility in the world to achieve IASIOS Accreditation in April 2020. Their consistent maintenance of high standards and dedication to patient care has now culminated in achieving IASIOS’s highest distinction, the centre of excellence seal. This designation required the centre to meet rigorous international standards that exceed the core criteria for interventional oncology (IO) services.
The team at the Hôpitaux Universitaires de Strasbourg has demonstrated exceptional commitment to quality patient care, facility development, and the advancement of IO as a discipline. IASIOS states that the organisation is proud to celebrate this global milestone with the hospital team and acknowledges their significant contribution to setting new benchmarks in IO patient care.
Chairman of radiology and nuclear medicine at the Hôpitaux Universitaires de Strasbourg, Afshin Gangi comments: “Through IASIOS, we were able to assess our department from the top down and recognise our strengths and weaknesses. This deep analysis resulted in a comprehensive improvement of patient services and safety and allowed us to provide standardised, yet personalised, treatment to each of our patients. I would like to highlight the contributions of our entire team—the interventional radiologists, nurses, radiographers, supervisors, quality control team, secretaries, and hygiene team—towards achieving and upholding the highest standards of care in IO.”
Following her presentation on uterine artery embolization (UAE) for fibroids at the Global Embolisation Oncology Symposium Technologies (GEST; 16–19 May, New York, USA), Abeer AlDhawi (Riyadh, Saudi Arabia), describes the “significant relief” that can be provided to patients through this minimally invasive procedure.
AlDhawi details that they observed the highest success rates among younger female patients with initially small fibroid masses found at the uterine cervix.
She advocates for further UAE research, placing emphasis on the need for long-term efficacy data. Through this, interventional radiologists will be able to gain a better understanding of fibroid recurrence rates following embolization and can develop “better criteria for patient selection and lead to more personalised and effective treatment plans”.
A recent study suggests that endovascular treatment of the common femoral artery (CFA) is associated with an increased rate of long-term CFA-specific reintervention, regardless of indication. Nicholas Wells, a medical student at Yale School of Medicine in New Haven, USA, presented this and other key findings from a tertiary care centre analysis of open and endovascular treatment of the CFA at the 2024 Vascular Annual Meeting (VAM; 19–22 June, Chicago, USA).
“The CFA is a common site of disease in patients with peripheral arterial disease,” Wells began. He noted that endarterectomy is seen as the gold standard of treatment, with primary patency rates “often surpassing 95% at five years” and evidence of “excellent long-term durability as far out as eight years.”
The objective of the study, Wells shared, was to compare open and endovascular treatment of the CFA with a focus on reinterventions and major adverse limb events.
This was a retrospective study of all revascularisations involving the CFA, including repeated reinterventions, conducted at a single centre between 2013 and 2020. “These procedures were performed by various specialists, including vascular surgeons, interventional radiologists and interventional cardiologists,” Wells detailed, adding that the researchers used standard comparative statistics and stratified their analysis by indication—claudication versus chronic limb-threatening ischemia (CLTI).
The researchers found that, from their database of 1,954 patients, 23% were treated for the CFA at least once and 15% of all individual revascularisations involved the CFA.
“Patients with claudication were more likely to be treated initially with endovascular therapy, at 57%, and those with CLTI were more likely to be treated with open surgery, at 60%,” Wells added.
The presenter reported that approximately one-third of the open surgery group underwent extended CFA endarterectomy involving the external iliac arteries, superficial femoral artery, and profunda femoral arteries, and about one-third underwent a concomitant ipsilateral bypass.
He also noted that approximately half of the patients in the endovascular group underwent concomitant endovascular revascularisation of the distal femoropopliteal region.
In the perioperative period, Wells shared that open surgery was associated with an increased rate of bleeding and wound infection, while endovascular therapy was associated with shorter mean length of hospital stay. Perioperative major amputation and mortality were below 1% in both groups.
“For claudication, endovascular therapy led to an increased rate of CFA-specific reintervention in the long term—35% compared to just 21% of those initially treated with open surgery,” Wells revealed.
“Additionally,” he continued, “15% of those who initially received endovascular treatment required eventual conversion to endarterectomy of the CFA, while only 5% of those who were initially treated with open surgery required a redo open CFA with endarterectomy.”
The researchers observed similar outcomes in the CLTI group, where 33% of initial endovascular recipients required eventual CFA reintervention compared to 21% of those initially treated with open surgery. Conversion to endarterectomy was not found to be significant in this subgroup.
“The take-home message here was that endovascular therapy led to higher rates of CFA reintervention in the long term and that for claudicants, conversion to endarterectomy was more common following endovascular therapy than redo endarterectomy,” the presenter told VAM attendees.
After a median follow-up time of three to four years, major amputation, major adverse limb events and mortality were not found to be different.
Furthermore, major adverse limb events-free survival—which was defined as time to either reintervention to any artery, major amputation or death—was not found to be significantly different between treatment approaches in either subgroup.
Senior author Cassius Iyad Ochoa Chaar, associate professor at Yale School of Medicine, told Vascular News that the anatomy of the CFA is “very peculiar,” and that the extent of the disease treated was not accounted for in this analysis. “Our future work will focus on studying the anatomy of the atherosclerosis affecting the CFA to better understand which lesions are best treated with which strategy of revascularisation,” he commented.
In June, the most popular stories from Interventional News included new data from the C-GUARDIANS pivotal investigational device exemption (IDE) trial; positive 12-month results from the Selution SFA Japan trial; and a range of industry updates.
Boston Scientific has announced that it has entered into a definitive agreement to acquire Silk Road Medical, a medical device company involved in producing products to be deployed during transcarotid artery revascularisation (TCAR). The purchase price is US$27.50 per share, reflecting an enterprise value of approximately US$1.16 billion.
A study conducted by the Harvey L Neiman Health Policy Institute (HPI) has identified a large percentage of unidentified interventional radiologists ‘hidden’ within Medicare data. The research has uncovered a previously unforeseen trapdoor, in which self-designated specialty in Medicare claims data have proven to be an “inadequate selection method” resulting in the omittance of practicing interventional radiologists from records.
Cook Medical have announced that Beacon tip sizing catheters are now available in the USA and Canada. The Beacon catheter is available in a variety of lengths and tip configurations, a recent press release adds.
Xeltis has announced that it has gained approval from the US Food and Drug Administration (FDA) for an investigational device exemption (IDE) submission to begin enrolling patients into a pivotal study for aXess.
New data from the C-GUARDIANS pivotal investigational device exemption (IDE) trial support consideration of carotid artery stenting (CAS) with the CGuard embolic prevention stent system (EPS; InspireMD) as a “frontline therapeutic option for appropriate patients being considered for carotid revascularisation”. This is according to lead investigator Chris Metzger (OhioHealth, Columbus, USA), who presented one-year results from the trial at the Leipzig Interventional Course (LINC) 2024 (28–31 May, Leipzig, Germany).
Medical Templates has announced that they have received US Food and Drug Administration (FDA) clearance for their Cube Navigator software for planning of percutaneous, computed tomography (CT)-guided interventions.
Cordis has announced positive 24-month results from the Selution SFA Japan trial. The prospective, multicentre, single arm trial is designed to assess the safety and efficacy of Selution SLR drug-eluting balloon (DEB) for the endovascular therapy of de novo and non-stented restenotic lesions in the superficial femoral artery (SFA) and the popliteal artery (PA). The findings were presented at the Japan Endovascular Treatment (JET) conference (14–16 June, Fukuoka, Japan).
Penumbra has announced that it has received CE mark approval and so has initiated the European launch of BMX81 and BMX96, devices which are designed for neurovascular management of ischaemic and haemorrhagic stroke.
Amplitude Vascular Systems (AVS) announced today that it has received an investigational device exemption (IDE) from the US Food and Drug Administration (FDA) to begin its pivotal trial for pulsatile intravascular lithotripsy (IVL) therapy.
Johnson & Johnson today announced it has completed its acquisition of Shockwave Medical. Shockwave is now part of Johnson & Johnson and will operate as a business unit within Johnson & Johnson MedTech.
Cordis has announced positive 24-month results from the Selution SFA Japan trial. The prospective, multicentre, single arm trial is designed to assess the safety and efficacy of Selution SLR drug-eluting balloon (DEB) for the endovascular therapy of de novo and non-stented restenotic lesions in the superficial femoral artery (SFA) and the popliteal artery (PA). The findings were presented at the Japan Endovascular Treatment (JET) conference (14–16 June, Fukuoka, Japan).
“The Selution SLR DEB outcomes demonstrate patient benefits that are sustained out to 24 months and can match proven paclitaxel DCB performance in a complex patient population,” said Osamu Iida (Osaka Police Hospital, Osaka, Japan). “These are promising results that build confidence in Limus drug-eluting balloons being a safe and effective option for SFA treatment while avoiding any paclitaxel related concerns.”
The long-term follow-up of Selution SLR DEB confirmed efficient sirolimus drug transfer and retention with safety and efficacy sustained through 24 months in a complex population that included 60.3% diabetics, mean lesion length of 127mm, 17.2% total occlusions, and 47.8% involvement of the popliteal. At 24 months, Selution SLR DEB delivered primary patency of 83.0% and 94.5% freedom from clinically-driven target lesion revascularisation (CD-TLR).
“The Selution SFA Japan trial continues to build confidence in the Selution SLR DEB technology. The Selution SLR DEB delivers some of the highest patency rates amongst SFA paclitaxel DCB studies and differentiates from other Limus-based devices. The ability to achieve durable clinical results in a challenging patient population provides clinicians a solution that will offer value to real world patients” said George Adams, chief medical officer at Cordis. We are excited for the evolution of patient care and to be leading that journey by expanding access to Selution SLR DEB.”
Cordis add that the Selution SFA Japan trial is one of four randomised controlled trials and one real world registry data sets currently underway across coronary, SFA and below-the-knee (BTK) arteries.
Penumbra has announced that it has received CE mark approval and so has initiated the European launch of BMX81 and BMX96, devices which are designed for neurovascular management of ischaemic and haemorrhagic stroke.
This announcement further expands the company’s neuro portfolio in Europe, following the news in early May when Penumbra launched three new RED reperfusion catheters (RED 43, RED 72 with SENDit technology, and RED 78).
“Physicians in Europe now have more options to serve their patients using our expanded portfolio. With five innovative devices introduced in Europe in a matter of months, our dedication to improving stroke care enables us to provide physicians with customised stroke solutions,” said Joan Kristensen, head of the Europe, Middle East and Africa region for Penumbra.
Unlike traditional access catheters, Penumbra’s BMX81 and BMX96 are made using laser-cut stainless steel hypotube technology, offering stability and trackability. They are designed to allow physicians to navigate the brain’s complex anatomy and can be used from either a femoral or radial access approach (i.e. via groin or wrist). The stainless steel hypotube also allows for a larger inner diameter while maintaining a lower outer diameter without compromising support. This expands intraprocedural options in both ischaemic and haemorrhagic stroke.
“I need to be able to trust that my access catheters can provide the stability that I need. The new BMX catheters promise excellent support. With their expanded inner diameters, I will be able to increase therapeutic options for my patients, especially when going radial,” said Markus Holtmannspötter, (Klinikum Nürnberg, Nürnberg, Germany).
With 20 years of experience optimising science-based aspiration thrombectomy (S-BAT), Penumbra’s catheters are engineered with the latest technology in trackability and aspiration to address a wide range of large vessel occlusions and to navigate the challenging vasculature of the brain.
Boston Scientific has announced that it has entered into a definitive agreement to acquire Silk Road Medical, a medical device company involved in producing products to be deployed during transcarotid artery revascularisation (TCAR). The purchase price is US$27.50 per share, reflecting an enterprise value of approximately US$1.16 billion.
“The TCAR platform developed by Silk Road Medical is a notable advancement in the field of vascular medicine, which has revolutionised stroke prevention and the treatment of carotid artery disease,” said Cat Jennings, president, vascular, peripheral interventions, at Boston Scientific. “We believe the addition of this clinically differentiated technology to our vascular portfolio demonstrates our continued commitment to provide meaningful innovation for physicians who care for patients with peripheral vascular disease.”
The TCAR system gained US Food and Drug Administration (FDA) approval in 2015 and is supported by several clinical studies demonstrating a reduced risk of stroke and other complications associated with traditional open surgery. The products sold by Silk Road Medical are the only devices commercially available for use during the TCAR procedure.
Boston Scientific expects to complete the transaction in the second half of 2024, subject to customary closing conditions. Silk Road Medical has guided to net revenue of approximately US$194–198 million in 2024, representing 10–12% growth over the prior fiscal year. The impact to Boston Scientific adjusted earnings per share is expected to be immaterial in 2024 and 2025, and accretive thereafter.
Xeltis has announced that it has gained approval from the US Food and Drug Administration (FDA) for an investigational device exemption (IDE) submission to begin enrolling patients into a pivotal study for aXess.
aXess is a restorative conduit that enables the creation of a new, permanent, living vessel for haemodialysis vascular access, combining the safety and patency of an arteriovenous fistula (AVF), with the speed to treatment of an arteriovenous graft (AVG) a recent press release has stated. The aXess vascular access conduit is said to offer an improved dialysis patient experience and avoids the frequent reinterventions and complications, such as infections, faced by many renal disease patients.
Xeltis’ implants platform is an important development in vascular replacement technology as, over time, its implants are gradually replaced by the patients’ own living healthy tissue. Xeltis’ novel technology has already treated over 100 patients across different clinical trials.
Eliane Schutte, chief executive officer, Xeltis commented: “We have already shownIDE outstanding 12-month data from our first-in-human study in Europe and are looking forward to starting this pivotal trial in the USA. We are very proud of the potential for aXess to transform the field of vascular access by stopping the cycle of interventions and infections and bringing our unique restorative solution to haemodialysis patients worldwide.”
Paulo Neves, chief medical officer, Xeltis said: “Our focus is on improving the outcomes for patients on dialysis. aXess offers this potential through its avoidance of the reinterventions and complications associated with other vascular access solutions. This pivotal study is important in assessing and demonstrating this and marks a significant milestone in our clinical strategy in the US.”
The US-based pivotal trial follows 12-month data from the first-in-human trial in Europe in comparison to haemodialysis vascular access solutions. aXess is also undergoing an EU pivotal trial, recruiting up to 110 patients in nine European countries.
Medical Templates has announced that they have received US Food and Drug Administration (FDA) clearance for their Cube Navigator software for planning of percutaneous, computed tomography (CT)-guided interventions.
Part of the Cube Navigation System, the computer vision-enabled software pairs with Medical Templates’ proprietary hardware, a needle guide in the form of a Cube, as an alternative to free-hand navigation as well as capital-intensive solutions such as robots. With adoption rapidly expanding in Europe, the FDA clearance dovetails with the launch of the product in the US market.
Navigation is gaining importance in the field of interventional radiology (IR), mainly driven by expanding treatment options in oncology and improved patient outcomes through the use of minimally-invasive procedures, the press release states. Smaller targets, more complex access routes, and time and personnel constraints have all contributed to the increased adoption of CT navigation systems.
“Market pressures are pushing physicians to perform increasingly complex procedures, while reimbursement continues to be a driving force in determining which tools are used during interventions. The Cube Navigation System was designed to provide accurate navigation at a reasonable price point, without compromising on workflow complexity or speed,” says CEO Anika Uhde. “Centres in Europe have been enthusiastic about our solution because of its ease of use and incredibly fast onboarding. They see an improvement almost immediately.”
A recent study published in the Journal of Vascular and Interventional Radiology (JVIR) found that punctures performed with the Cube Navigation System were more than 4x closer to the target on the initial puncture (2.5mm ± 1.2mm vs. FHM 12.1mm ± 7.7mm), had significantly more accurate final needle locations (3.8 mm ± 1.3 mm vs. FHM 6.7 mm ± 4.5 mm, p=0.004), and were significantly faster (263.1s ± 84.4s vs. FHM 411.2s ± 141.0s, p<0.001). Further studies on accuracy and speed are currently being carried out in Switzerland and Germany.
Vicente Riambau (Barcelona, Spain) describes the unique features and improvements of the iCover balloon expandable covered stent, notably its low profile, radiopaque markers, and total encapsulation with polytetrafluoroethylene (ePTFE), which give the device an edge over its competitors and make it his “first choice.”
Riambau also reflects on how iVascular’s vertical integration, by which the company manufactures all product components such as plastic tubes, balloons and stents, allows freedom from supply chain difficulties. This is important, he says, to maintain high quality for every single step during the manufacture of key parts.
Amplitude Vascular Systems (AVS) announced today that it has received an investigational device exemption (IDE) from the US Food and Drug Administration (FDA) to begin its pivotal trial for pulsatile intravascular lithotripsy (IVL) therapy.
The POWER-PAD-II clinical study will evaluate the safety and efficacy of AVS’s Pulse IVL system for the treatment of patients with severely calcified peripheral arterial disease (PAD) in the USA.
POWER-PAD-II will enrol up to 120 patients who will be followed for up to six months. This new trial follows the success of POWER-PAD-I, which was presented by Jon George (Pennsylvania Hospital, Philadelphia, USA) at TCT 2023 (23–27 October, San Francisco, USA). POWER-PAD-I demonstrated clear benefits to patients with calcific femoropopliteal arteries, including reduced leg pain, increased blood flow and improved ability to walk.
“We are proud to be one of the first companies to conduct a peripheral intravascular lithotripsy pivotal IDE trial in the USA,” said Mark Toland, chairman of the board of AVS. “The IDE approval marks our most significant clinical milestone to date as we approach FDA clearance and market availability for the Pulse IVL system, which is designed to easily deliver therapy across complex calcified lesions and reduce overall procedural costs.”
“By introducing a new, innovative treatment for calcified arterial disease, we can make a dramatic impact on patient lives and improve outcomes,” said Chris Metzger (OhioHealth, Columbus, USA), national principal investigator of the POWER-PAD-II study. “The results of our pivotal trial will pave the way for a new treatment option in an evolving and exciting area of medicine: IVL therapy.”
In May, the most popular stories from Interventional News included a recent investigation into ChatGPT and patient perception of interventional radiology (IR); interventional radiologists speak on their experience of private practice in the Middle East and North Africa (MENA) region; and scientific reports from the European Conference of Interventional Oncology (ECIO) annual meeting (28 April–1 May 2024, Palma de Mallorca, Spain).
Preliminary results from the largest global liver venous deprivation (LVD) registry—EuroLVD—confirms “high” hypertrophy and kinetic growth rate and “very low” rate of post-hepatectomy liver failure (PHLF), demonstrating the “safety” of LVD over portal vein embolization (PVE) in a real-world, multicentre setting.
During the Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA), interventional radiology (IR) societies from nations worldwide sat around a table to consider the status of IR in their geographies. The Global Society Summit—the first meeting of its kind—heard international IR leaders discuss and define common challenges, to track a path for multinational collaboration and sustain a unified voice for IR in an increasingly competitive global healthcare environment.
Using Chat generative pre-trained transformer (GPT) to understand the public perception of interventional radiology (IR), Chloe Cross (Icahn School of Medicine at Mount Sinai, New York, USA) and colleagues presented new data which provide “exciting” insights into how and when IR is suggested for treatment for patients using artificial intelligence (AI).
Merit Medical Systems, a global leader of healthcare technology, has announced US Food and Drug Administration (FDA) 510(k) clearance for its Siege vascular plug. Merit also announced the launch of its Bearing non-spherical polyvinyl alcohol (nsPVA) Express prefilled syringe in the USA and Australia.
AngioDynamics has announced European CE mark approval of the AlphaVac F1885 system for the non-surgical removal of thrombi or emboli from the pulmonary arteries and for the treatment of pulmonary embolism (PE).
Jack Jennings is a professor of radiology and chief of musculoskeletal radiology for Mallinckrodt Institute of Radiology (MIR) at Washington University School of Medicine in St Louis, USA. Best known for his innovation in musculoskeletal and spine interventions, Jennings is no stranger to blending niches, combining skills gained from his experiences in interventional radiology (IR), neuroradiology, and musculoskeletal radiology for a range of tumours in the bone, spine and soft tissue.
Interventional radiologists Mohammed Almoaiqel (King Abdulaziz Medical City, Riyadh, Saudi Arabia), Karim Abd El Tawab (Ain Shams University Hospitals, Cairo, Egypt) and Mohammad Al-Twalah (Dawali Clinic, Riyadh, Saudi Arabia) speak to Interventional News about the pros and cons of private practice in the Middle East and North Africa (MENA) region, surveying the spectrum of opportunities and challenges faced by interventionists today.
Fluidx Medical Technology has announced that the US Food and Drug Administration (FDA) has granted investigational device exemption (IDE) approval to initiate the GPX embolic device pivotal clinical trial. The objective of this trial will be to evaluate the safety and effectiveness of the GPX embolic device.
Etienne Garin (Centre Eugene Marquis, Rennes, France), presenting results from an ad-hoc interim analysis of the PROACTIF trial data, reported that “appropriately selected” patients who received transarterial radioembolization (TARE) with yttrium-90 (Y90) glass microspheres within a “personalised treatment plan” for primary and metastatic liver tumours—including intrahepatic cholangiocarcinoma (ICC)—achieved “long survival” and had a “low adverse event rate”.
Late-breaking data from the ENGULF trial showed that a novel dual-action thrombectomy device was effective and safe in treating acute pulmonary embolism (PE). The safety and effectiveness results were presented today as late-breaking science at the Society for Cardiovascular Angiography & Interventions (SCAI) 2024 Scientific Sessions and simultaneously published in JSCAI.
New data from the C-GUARDIANS pivotal investigational device exemption (IDE) trial support consideration of carotid artery stenting (CAS) with the CGuard embolic prevention stent system (EPS; InspireMD) as a “frontline therapeutic option for appropriate patients being considered for carotid revascularisation”. This is according to lead investigator Chris Metzger (OhioHealth, Columbus, USA), who presented one-year results from the trial at the Leipzig Interventional Course (LINC) 2024 (28–31 May, Leipzig, Germany).
Metzger detailed that this was a prospective, multicentre, international, single-arm clinical trial comparing the primary endpoint to a performance goal derived from the literature.
The objective was to evaluate the safety an efficacy of the CGuard in the treatment of carotid artery stenosis in symptomatic and asymptomatic patients at high risk for carotid endarterectomy (CEA) undergoing CAS.
From July 2021 to June 2023, 316 patients were prospectively enrolled in the study at 24 sites across the USA and Europe.
The primary endpoint of the trial was a composite of: (1) incidence of major adverse events including death (all-cause mortality), any stroke, or myocardial infarction (DSMI) through 30-days post index procedure, or (2) ipsilateral stroke from day 31 to day 365 post-procedure.
Metzger revealed at LINC 2024 that stenting with the CGuard in patients with carotid artery stenosis and at high risk for CEA had a primary endpoint event rate of 1.95%, from procedure through one-year follow-up.
The presenter commented that the data are consistent with previously published European data.
“We are very excited that the one-year carefully adjudicated C-GUARDIANS data confirm the extremely low rates of stoke, death, myocardial infarction, and target vessel revascularisation in this prospective trial of high-CEA-risk patients with obstructive carotid disease, including 25% who were symptomatic,” Metzger stated in an InspireMD press release announcing the results. “These data confirm the potential ‘neuroprotective properties’ of this unique MicroNet technology, offering an outstanding frontline option to consider for each patient with obstructive carotid artery disease.”
A study conducted by the Harvey L Neiman Health Policy Institute (HPI) has identified a large percentage of unidentified interventional radiologists ‘hidden’ within Medicare data. The research has uncovered a previously unforeseen trapdoor, in which self-designated specialty in Medicare claims data have proven to be an “inadequate selection method” resulting in the omittance of practicing interventional radiologists from records.
Mikki D Waid (Harvey L Neiman Health Research Policy Institute, Reston, Virginia) and colleagues reference interventional radiology (IR) as arguably one of the most poorly understood fields of medicine in the introduction to their research. They assert that the overlap in services across radiology has created a “challenge” for identifying interventional radiologists.
The authors note that definitions of IR to date have been “insufficient” for identifying “replicable samples of interventional radiologists for research”. Additionally, they posit that the self-designated physician specialty found in Medicare data—which are typically derived from the Medicare Provider Enrolment, Chain, and Ownership System (PECOS)— have been shown to be “unreliable” and does not accurately represent the true level of self-described interventionists when compared with physicians’ own websites.
“This research does not attempt to make a judgement on which radiologists should be considered interventional radiologists,” Waid and colleagues underline. Rather, their research sought to identify if interventional radiologists are accurately represented in the available data.
The primary sources for their analysis were the 2015–2019 Centres for Medicare and Medicaid Services (CMS) Provider and Payment Utilization and Payment Data Physician and Other Supplier Public Use File (PUF), and 2015–2019 data from Optum’s de-identified Clinformatics Data Mart (CDM) database.
The PUF provides physician-level data including gender, self-designated specialty, state, zip code of practice, and counts and payments by service performed. The CDM database includes full patient-level medical claims data from approximately 20 million members enrolled in commercial and Medicare Advantage plans.
To identify practicing interventional radiologists within PUF and CDM data, Waid et al looked at the number of procedures that were billed as IR-related treatment and rank-ordered radiologists IR-related work as a percent of total-billed work relative value units (wRVUs). Characteristics were analysed at various threshold percentages. The authors also note that external validation used Medicare records with the Society of Interventional Radiology (SIR) membership records.
Their results show that, of the 37,131 unique radiologists, in the Medicare data, 8,010 (21.6% of total unique self-designated diagnostic radiologists and interventional radiologists), 3,572 (9.6%), and 2,060 (5.5%) met the 10%, 50%, and 90% thresholds, respectively. Above a 10% IR-work threshold only 24% of selected practicing interventional radiologists were designated as such in the data; above 50% and 90% thresholds, percentages rose to 42% and 48%, respectively. The average IR-related work (surgical, invasive, and evaluation and management services) reported among practicing interventionists was 45, 84 and 96% of total wRVUs, for the 10, 50 and 90% thresholds. Pulling key takeaways from their results, the authors highlight that in both datasets, most practicing interventional radiologists at all IR-work levels up to 95% were designated as diagnostic radiologists in the source data. They contend that, even at the highest levels of IR-related work effort, no more than 47.6% of interventional radiologists are “appropriately” self-designated in the Medicare sample.
Furthermore, Waid et al identified characteristics that were associated with “greater likelihood” of being a practising interventional radiologist. Among these characteristics were male sex, fewer years since training, practicing in a metropolitan area, and employment within a “smaller” practice. The authors opine that future research exploring the “relationships between workforce, practice, system, and community factors” to understand the fundamental IR workforce dynamics could illuminate “factors that predict patient access to IR services”.
The fluidity of IR in definition and the pervasive overlap of its services has created statistical invisibility for practicing interventional radiologists, the authors salient conclusions assert. “Physicians’ self-designation could vary over time—defined as diagnostic one year and interventional the next. They also do not necessarily always define themselves. Their institution or billing provider may take on this power, particularly in the PECOS system,” the authors state.
“There is an absence of an available gold standard for assigning specialty that reflects both training and medical practice,” Waid and colleagues pose. “Identifying IR physicians in claims data poses a challenge that hinders the progress and comparability of research to broadly characterise and measure the value of this important independent medical specialty.” The authors conclusions demonstrate a need for better representation and definition of IR and call for improved selection method to avoid the omittance of “the majority” of practicing interventional radiologists.
Cook Medical have announced that Beacon tip sizing catheters are now available in the USA and Canada. The Beacon catheter is available in a variety of lengths and tip configurations, a recent press release adds.
The Beacon catheter is used in angiographic procedures, diagnostic procedures and vascular interventions to make sure medical devices are sized correctly. These catheters are uniquely designed to help physicians correctly size devices, such as grafts, stents and balloons, to identify the best size of product to use for an individual patient’s situation. Sizing catheters also help to measure lesions accurately under fluoroscopy.
Cook is offering the Beacon tip sizing catheter in 14 sizes so physicians have catheters for a wide variety of procedures. The Beacon tip sizing catheter is available in centimetre, cava and white sizing configurations, as well as in pigtail, varrel contralateral flush (VCF) and straight tip shapes. All tip configurations are radiopaque for high visibility under fluoroscopy.
“This catheter complements and enhances our portfolio of vessel sizing products. Cook’s portfolio is uniquely positioned to support interventional procedures from initial access throughout the intervention,” said Remco Van der Meel, director of product management for Cook’s interventional specialty. “This sizing tool is an instrumental device during aortic interventions, a space where Cook is dedicated to. By offering our premium, accurate, gold-banded sizing catheters again, we are continuing to expand our ‘access and target’ portfolio to support complex interventions.”
Johnson & Johnson today announced it has completed its acquisition of Shockwave Medical. Shockwave is now part of Johnson & Johnson and will operate as a business unit within Johnson & Johnson MedTech.
Joaquin Duato, chairman and chief executive officer of Johnson & Johnson, said: “Through Innovative Medicine and MedTech, Johnson & Johnson is transforming the trajectory of cardiovascular disease, one of the leading causes of death globally. We are delighted to welcome the Shockwave team to Johnson & Johnson and look forward to bringing their innovative IVL technology to more patients around the world.”
Tim Schmid, executive vice president and worldwide chairman of Johnson & Johnson MedTech, said: “Completing this acquisition is a significant milestone in the expansion of our leadership position in the medtech industry. Shockwave’s differentiated solutions and robust pipeline represent an exciting opportunity for Johnson & Johnson MedTech to bring more innovations to patients in one of the largest areas of unmet medical need. We are excited to begin collaborating directly with the Shockwave team and look forward to a bright future together.”
A press release notes that Shockwave offers the first and only commercially available intravascular lithotripsy (IVL) platform for coronary artery disease (CAD) and peripheral arterial disease (PAD) and complements Johnson & Johnson’s leading positions in heart recovery (Abiomed) and electrophysiology (Biosense Webster) to make it a category leader in four of the largest and highest-growth medtech markets within cardiovascular intervention.
Shockwave is ultimately expected to become Johnson & Johnson MedTech’s thirteenth priority platform, as defined by annual sales of at least US$1 billion. The transaction is expected to accelerate revenue growth for both Johnson & Johnson and Johnson & Johnson MedTech. Johnson & Johnson expects the transaction to be accretive to operating margin, but considering the impact of financing costs, is expected to dilute adjusted earnings per share by approximately US$0.10 in 2024 and approximately US$0.17 in 2025.
In connection with the completion of the transaction, Shockwave’s common stock ceased trading on NASDAQ.
FastWave Medical has announced the 30-day results of its first-in-human (FIH) study using the company’s differentiated peripheral intravascular lithotripsy (IVL) technology.
This was a prospective, single-arm study to assess the safety and feasibility of the FastWave IVL system in patients with peripheral arterial disease affecting the superficial femoral artery (SFA) and popliteal artery with moderate to severe calcium. Principal investigators Miguel Montero-Baker (HOPE Vascular & Podiatry Clinic, Houston, USA), and Venkatesh Ramaiah (HonorHealth Vascular Group and Pulse Cardiovascular Institute, Scottsdale, USA), successfully conducted the procedures in collaboration with the hosting investigator, Antonio Muñoa (San Lucas Hospital, Chiapas, Mexico).
Eight patients with moderate to severe calcified occlusions in the superficial femoral artery (SFA) and popliteal arteries were successfully treated, providing encouraging evidence supporting the early safety and feasibility of the FastWave IVL system, the recent press release states.
Of the company’s key procedural findings, they reported 100% procedural success, no peri-procedural adverse events, and 5.9% mean residual diameter stenosis post-therapy. Reporting their 30-day results, FastWave also shared that no major adverse events were observed, they identified 100% patency, <2.4 peak systolic velocity ratio (PSVR), no revascularisations, walking impairment questionnaire (WIQ) scores showed improved walking distance and speed, and stair-climbing ability, and finally, ankle-brachial index (ABI) improved from baseline 0.56 to 0.89 at 30 days noting enhanced blood flow.
Montero-Baker approved these results, stating: “The overall improvement in the patients treated in the FastWave FIH study is really encouraging and provides compelling evidence supporting the feasibility and safety of the FastWave IVL system for further evaluation in a larger patient population in the USA.”
Ramaiah added: “I am impressed by the performance of the FastWave peripheral IVL catheter—it’s both highly deliverable and easy to use. Achieving a 94% mean residual diameter stenosis reduction at the end of the procedure is equally impressive and the 30-day follow-up results reinforce the initial procedure’s success.”
Scott Nelson, co-founder and CEO of FastWave Medical, shared his excitement: “The procedural data from the initial intervention and the 30-day results reinforce our confidence in the FastWave IVL system’s potential to pave the way for a peripheral pivotal trial in the USA. On behalf of the rest of our team, I’d like to express our sincere gratitude to the principal investigators for their exceptional clinical work and collaboration with the FastWave team in sharing these 30-day data.”
Terumo Europe recently shared that a positive guidance has been published by the National Institute for Health and Care Excellence (NICE) stating that selective internal radiation therapy (SIRT) is now recommended to be used for the treatment of neuroendocrine tumors with liver metastasis (NELM).
According to a Terumo press release, this is a key milestone as it expands the existing treatment options (surgery, percutaneous ablation, systemic therapies, peptide receptor radionuclide therapy [PRRT] and other intra-arterial therapies) for the treatment of patients with NELM.
The NICE guidance describes SIRT as a tool to reduce tumour size within the liver, slow local tumour growth or control a collection of symptoms caused by some neuroendocrine tumours that release hormones. SIRT can be preceded or followed by other treatments such as PRRT and it can be repeated over time. The committee stated that SIRT is likely to be better tolerated than other intra-arterial therapies, because SIRT relies on radiation rather than an embolic effect to kill the tumour cells.
This guidance is part of NICE’s interventional procedure programme, which considers whether interventional procedures (e.g. SIRT) are safe and work well enough for wider use in the National Health Service (NHS). A comprehensive review of the literature and consultations with clinical experts and patient representatives informed the decision of the committee.
This is a positive endorsement for the safety and efficacy of SIRT and a complement to the 2020 European Society for Medical Oncology (ESMO) guidelines for gastroenteropancreatic neuroendocrine neoplasms in which locoregional therapies (including SIRT) have been recommended for tumour shrinkage and for symptoms control in patients with NELM suffering from carcinoid syndrome (flushing and/or diarrhoea). The European Neuroendocrine Tumor Society (ENETS) guidance (2022) also mentions that SIRT can be considered as a therapeutic option for patients with NELM with carcinoid syndrome.
The positive impact on the quality of life of the NELM patient has been described in the NICE report. It was reported from a patient that nearly two months after the treatment, tiredness subsided and he began to enjoy normal activities and hobbies again, slowly returning to his old self.
Terumo notes that QuiremScout (Holmium-166 microspheres) and QuiremSpheres (Holmium-166 microspheres) as components of the Holmium Platform can be used for an individualised treatment approach (work-up and therapy) of patients with NELM.
Publications by Braat et al (2020) and Ebbers et al (2022) concerning the HEPAR PLuS study concluded that QuiremSpheres microspheres are effective with an acceptable safety profile after initial peptide receptor radionuclide therapy (PRRT) for patients with bulky NELM.
Another recent publication by RamdHani et al (2024) demonstrated a clear dose-response relationship in patients with NELM treated by QuiremSpheres. More specifically, achieving a tumor dose ≥120Gy provides the highest likelihood (90%) for obtaining a response based on a retrospective analysis of QuiremSpheres use in real-world practice.
Nabil Kibriya (King’s College Hospital, London, UK) remarked on the guidance: “SIRT provides a minimally invasive treatment option for patients with metastatic neuroendocrine tumors (mNETs) of the liver, offering precise targeting of tumour cells while sparing healthy tissue. This approach has demonstrated significant tumour response rates and prolonged progression-free survival, leading to improved outcomes and quality of life for individuals with mNETs. Additionally, SIRT can be combined with other therapies, enhancing its effectiveness in managing advanced diseases and providing hope for patients facing this challenging condition. This specific NICE guidance can help us to receive UK reimbursement soon and therefore get wider access of this treatment modality for our patients.”
A single-centre, retrospective review has reported 13-year data confirming cryoablation as a “highly effective” treatment modality for solitary T1a renal cell carcinoma (RCC) with low complication and recurrence rates.
Interventional radiology fellow Ahmed Awad (The University of Texas MD Anderson Cancer Center, Houston, USA) presented these data at the recent Global Embolisation Oncology Symposium Technologies (GEST; 16–19 May, New York, USA). Cryoablation has emerged as an “attractive treatment option” for small renal masses, Awad stated, due to “favourable” intermediate- and long-term outcomes and its subsequent inclusion in the National Comprehensive Cancer Network (NCCN) guidelines alongside thermal ablation techniques.
Investigating the long-term experiences of their centre, Awad described their review, which regarded adult patients with a confirmed histopathology of solitary RCC with tumours of less than 4cm who received percutaneous cryoablation between January 2008 and December 2021. Exclusion criteria included patients with a prior history of RCC, patients with RCC metastases at the time of ablation or patients found to have multiple renal metastases at the time of the procedure.
Awad noted that overall survival, local recurrence-free survival, disease-free survival, metastases-free survival, and cancer-specific-free survival were each measured in this cohort.
Of the 86 patients included in their cohort, 57 were male and 29 were female. The median age in this population was 69 years and the median size of RCCs treated was reported as 2.7cm. The most common subtype of RCC was clear cell carcinoma, making up 63% of patients, and 4.6% of patients had a grade 3 or higher complication rate, which Awad defined as the requirement of any kind of intervention.
The median overall survival rate following cryoablation was 10.3 years. At five year follow-up, overall survival was 69%; “this stems from the fact that 60% of our population has another primary malignancy which confounded their overall survival”, Award reported. Local recurrence-free survival was 93.5%, five and 10 years disease-free survival was 91% and 84% at follow-up, respectively, and median disease-free survival was 7.8 years. Additionally, both metastases-free and cancer-specific-free survival were 100% at 10 years.
“Our results show that cryoablation is highly effective in treating T1a RCC. Our continued collection of long term follow-up data will favour additional quality and survival outcomes,” Awad said. “Cryoablation provides us the ability to visualise the ablation zone and the opportunity for a more controlled and confident approach both when planning and executing the procedure.”
Following the presentation, session moderator Bradford Wood (NIH Center for Interventional Oncology, Bethesda, USA) commended Awad and his team at MD Anderson for their research efforts, stating that theirs is one of the “greatest experiences” of the use of cryoablation for T1a RCC to date. He added that “caveats” in the most recent NCCN guidelines “keep [interventional radiologists] out of the mix and keep patients from hearing that [cryoablation] is an option”, so congratulated Awad on the addition of their data to the growing body of evidence which supports the use of cryoablation in this pathology.
Interventional radiologists Mohammed Almoaiqel (King Abdulaziz Medical City, Riyadh, Saudi Arabia), Karim Abd El Tawab (Ain Shams University Hospitals, Cairo, Egypt) and Mohammad Al-Twalah (Dawali Clinic, Riyadh, Saudi Arabia) speak to Interventional News about the pros and cons of private practice in the Middle East and North Africa (MENA) region, surveying the spectrum of opportunities and challenges faced by interventionists today.
The significant traction of interventional radiology (IR) as a specialised field has been marked on a global scale in recent years. For interventionists in the MENA region, demand for IR’s minimally invasive procedures has steadily increased year on year with growing awareness of its benefits for a range of indications. Although public healthcare systems in the MENA region have traditionally been the primary providers of interventional treatments, a tangible uptick in private healthcare institutions—or office-based labs (OBLs)—has been observed.
In Almoaiqel’s view, private practice runs alongside his role at the government hospital in Riyadh, which means that from 8am–5pm he can be found at the hospital, and from 5–9pm he covers a private IR clinic. In his OBL setting, he is able to perform “pure, elective IR procedures” such as embolization— including prostate artery embolization (PAE) and uterine artery embolization (UAE)—as well as vascular procedures via their diabetic foot service. He stated that around 30–40% of interventional radiologists in his region also work in both settings.
“It gives us freedom—freedom to see more patients and practice IR,” Almoaiqel said, commenting on the clinical autonomy that private practice has afforded him. In many countries worldwide, IR’s distinction from diagnostic radiology (DR) or radiology is still being forged, which equally applies to the MENA region. As Abd El Tawab added, most interventionists that open OBLs still perform DR procedures alongside IR, and the number of “true IR” clinics are still few.
The prevalence of these catch-all clinics, Abd El Tawab pointed out, may be in part due to the competitive nature of private practice IR in Egypt, where he practises. “No one will refer to us—no urologist, gynaecologist, or surgeon will send patients to us. All patients are self-referred, so we have to recruit them,” he stated.
Karim Abd El Tawab
Due to the increasingly saturated market, establishing a reputable presence to recruit patients has equated to marketing initiatives, with OBLs differentiating their services via social media advertisements. In Egypt, medical advertising is legal, which means Abd El Tawab’s private practice runs Facebook ads to reach patients—“they see the ads, they come, and they are convinced”, he said.
To Al-Twalah, the age of social media advertising in private practice IR has been “very challenging”, particularly in Riyadh. “People have moved online, they’re watching videos on TikTok and Instagram and you have to be there to be seen—it’s not us, but we have a team for that. We have daily challenges with this.”
Viewing social media as a double-edged sword, Almoaiqel attested to the benefit of educational campaigns which have been furthering the reach of IR, and what their procedures can do. Erecting a booth near their private clinic, his team have distributed brochures in the past, in order to spread awareness of IR treatments in their community.
“It’s a slow process,” Almoaiqel said, “but our community awareness must be improved—many women are not aware of fibroid embolization as a non-surgical alternative option, and our rate of amputation for diabetic foot is very high. We could save those feet and limbs by doing endovascular procedures.”
However, caseloads in public hospitals remain high, all three speakers asserted. Despite the lack of visibility of IR procedures, interventionists are experiencing long wait times and convoluted patient access. For this reason, Almoaiqel detailed his governments initiative to “relieve pressure” on public hospitals and insurance companies. He said that they have “facilitated investment” into private practice, “simplifying the opening of new facilities”. This support for OBLs also relieves pressure on the government to pay for the health sector, he continued.
Yet, as the government “injects support” into private practice, Almoaiqel said, challenges arise as “most patients are not insured, and they have to pay from their own pocket—this is a limitation”. He added that IR procedures are not cheap, some even working out to be more expensive than surgical procedures, via the specialist materials and technology that are required. “This limits us to patients who are able to pay,” he said. Abd El Tawab added that, in Egypt, patients’ insurance often “covers everything or nothing”, highlighting a discrepancy between funding and insurance coverage, which may be blocking patient access to private IR treatment.
Mohammad Al-Twalah
Historically, private practice has provided interventional radiologists with a higher earning potential compared to that of public hospitals. Yet, in Al-Twalah’s experience, the value in switching to private practice came from being “able to do what you want to do”. “Life is short—your work has to be enjoyable for both you and the patient, and in a good setting with a focused team.” Often private practices have a condensed, multidisciplinary team working under “one umbrella”, which Almoaiqel believes is the key to “long-term success” in private practice.
“In our clinic we have phlebologists, interventional radiologists, vascular surgeons and a podiatrist. In supporting each other to forward this vision for IR, the continuity of care we can achieve for patients is limitless,” Almoaiqel said.
AngioDynamics, a leading medical technology company focused on restoring healthy blood flow in the body’s vascular system, has announced European CE mark approval of the AlphaVac F1885 system for the non-surgical removal of thrombi or emboli from the pulmonary arteries and for the treatment of pulmonary embolism (PE).
“The CE mark represents a major step forward in enhancing patient care and safety for endovascular therapies in the EU, a market with a higher prevalence of PE when compared to the USA,” said Laura Piccinini, AngioDynamics senior vice president/general manager, Endovascular Therapies and International. “This designation allows us to broaden our reach and provide innovative solutions to more healthcare professionals treating patients diagnosed with PE—on an increasingly global scale.”
An estimated 435,000 PE events occur each year in the six largest European Union (EU) countries. Compared to the USA, the prevalence of PE is higher for those patients admitted to the emergency department in Europe, and European patients also had higher acuity and worse outcomes.
The CE mark for the AlphaVac F1885 system expands treatment options for healthcare professionals in the EU by offering a tool that helps reduce thrombus burden and improve right ventricular function in patients with PE, the recent press release states.
In December 2023, AngioDynamics announced the completion of patient enrolment in its US-based Acute Pulmonary Embolism Extraction Trial with the AlphaVac System (APEX-AV) study, a single-arm Investigational Device Exemption (IDE) study that enrolled 122 patients with confirmed acute, intermediate-risk PE across 25 hospital-based sites to assess the AlphaVac F1885 System for the treatment of PE.
The APEX-AV trial showed a mean decrease in the RV/LV ratio from baseline to 48 hours post-procedure of 0.45 (significantly greater than the pre-defined performance goal of 0.12 (p<0.001) and a major adverse event (MAE) rate of 4.1% (significantly lower than the pre-defined performance goal of 25% (p<0.001). The study also showed a 35.5% mean reduction in clot burden from baseline to 48 hours post-procedure and a mean procedure time of 37.2 minutes.
The JACC paper is the work of the American College of Cardiology (ACC), the American Heart Association (AHA) and nine other societies including the Society for Vascular Surgery (SVS) and the Society of Interventional Radiology (SIR).
Authored by cardiologist and writing committee chair Heather L Gornik (University Hospitals Harrington Heart & Vascular Institute, Cleveland, USA) and colleagues, the 2024 guidance aimed to advise clinicians on the treatment of patients with lower extremity PAD across its multiple clinical presentation subsets—asymptomatic, chronic symptomatic, CLTI, and acute limb ischaemia (ALI). The document represents an update to the 2016 AHA/ACC guidelines on PAD.
Among a list of key take-home messages from the guidance, Gornik et al highlight that health disparities in PAD “must be addressed at the individual and population levels,” recommending that interventions be “coordinated between multiple stakeholders across the cardiovascular community and public health infrastructure.”
Recommendations regarding medical therapy are also underlined, with the writing committee advising that rivaroxaban (2.5mg twice daily) combined with low-dose aspirin (91mg) “is effective to prevent major adverse cardiovascular events and major adverse limb events in patients with PAD who are not at increased risk of bleeding.”
Furthermore, structured exercise is labelled a “core component” of care for patients with PAD, and the writing committee states that revascularisation—whether endovascular, surgical, or hybrid—“should be used to prevent limb loss in those with chronic limb-threatening ischaemia and can be used to improve QoL [quality of life] and functional status in patients with claudication not responsive to medical therapy and structured exercise.”
The guidelines continue that foot care is “crucial” for patients with PAD across all clinical subsets and that podiatrists and other specialists with expertise in foot care, wound-healing therapies, and foot surgery “are important members of the multispecialty care team.”
Finally, the guidelines mention the PAD National Action Plan, which, the authors write, outlines six strategic goals to improve awareness, detection, and treatment of PAD nationwide. “Implementation of this action plan is recognised as a top advocacy priority by the writing committee,” the JACC paper reads.
Majorie van Helvert (University of Twente, Enschede, The Netherlands) and Michel Reijnen (Rijnstate Hospital, Arnhem, The Netherlands) are currently conducting research on ultrafast contrast-enhanced ultrasound blood flow quantification in peripheral arterial disease (PAD) patients after endovascular treatment. Early findings show that the new technique could offer an innovative imaging alternative.
Vascular News recently spoke with both van Helvert and Reijnen, and they went into more detail about their findings. Traditionally, conventional ultrasound systems are used in the diagnostic work-flow of PAD. These systems have limited temporal resolution which is typically capped out at 10–100 frames per second. However, with the novel technique that Reijnen and van Helvert used, they were able to increase that framerate to thousands or even tens of thousands of frames per second. This may be necessary to adequately quantify very high velocities and short-lived flow disturbances, for instance, in and around stenoses.
“Within that technique we use a new type of ultrasound transmissions, which is called plane wave ultrasound,” Reijnen explained. “When you look at regular ultrasound, and its image reconstruction, it’s done line-by-line. So, they make the image in separate lines, and all these lines are combined into one image. With plane wave, all transducer elements are simultaneously active in transmit and receive, thus you construct the image in one go. That enables you to get much more frames per second.”
Besides the increased framerate, the team also used contrast microbubbles. For this purpose an IV [intravenous drip] needs to be inserted to allow for contrast administration prior to the ultrasound acquisitions. “Once we use the ultrasound, these contrast microbubbles make sure that the echogenicity of the blood is enhanced,” van Helvert said. “Next to that, they can be used as tracer particles; that is really the basis for this technique in deeper structures, like the iliac arteries. When we’re looking at more superficial arteries, we don’t really need the contrast as we can perform our analysis based on the bloodspeckle signal itself.”
Reijnen explained that, when you look at anatomy, you are going to mostly use computed tomography (CT) angiography or magnetic resonance imaging (MRI). “Those are the two most important modalities,” Reijnen said. “When we look at functional imaging, there’s mostly duplex ultrasound. A duplex ultrasound is a regular ultrasound combined with doppler. It gives us flow velocities in one direction, generally in the middle of the vessel.”
He continued by saying that there are some drawbacks to duplex ultrasound, next to the aforementioned temporal resolution. “One of them is that it’s only in one directional. Also it requires a beam-to-flow angle correction which makes it highly operator dependent.”
While MRI technologies offer acceptable imaging, there are still some drawbacks to that as well. Namely, Reijnen explains, it’s time consuming, expensive, and the fact that multiple cardiac cycles are combined during image reconstruction may filter out important diagnostic information. “Another important drawback for example,” Reijnen said, “when there are stents, metal and MR is not a good combination. So, there may be disturbances because of the material of the stent.”
Once the images from the ultrafast contrastenhanced ultrasound have been compiled, the more technical aspect comes into play. In order to determine blood flow patterns, the recorded images from the contrast-enhanced ultrasound are divided into different sub-windows. An algorithm then registered how the microbubbles moved across the images.
“We calculate a cross correlation, and the peak in this cross correlation defines the most probable movement that these microbubbles made between two consecutive images that we captured,” van Helvert stated. “Combined with the time in between the frames, we can calculate a velocity vector per sub-window.”
After the images are captured, they must be filtered to see the microbubble contrast compared to the tissue clutter. The thousands of images that the team captures through ultrasound and thereafter analyse, allows them to build a velocity vector field over time. However, one unfortunate downside of this is that the images and the velocity vector field are still twodimensional compared to the three-dimensional flow characteristics.
“But, the upside of this technique compared, for instance, to MRI-based flow imaging, is that we measure a couple of cardiac cycles and its proven feasible inside stents.. So, it does provide added information in that sense,” van Helvert explained.
Reijnen went into more detail. “We can really track these bubbles during the cardiac cycle, and we can assess different patterns from that. So, we can see recirculations, we can see stasis of blood, we can see forward flow and backflow. We can also see that there is difference in blood flow at the anterior wall and the dorsal wall of the blood vessel where there a re bifurcations.”
“What we’re aiming for is, at least my view on things, that in an early disease stage you can do such measurements reliably and minimally invasive to assess if patients have favorable or unfavorable blood flow with respect to disease progression,” van Helvert said.
As for the next steps, Reijnen noted: “At this stage we’re looking at the technique itself, so we’re looking at which parameters can we reliably derive. How can we standardise them and how can we quantify them? And when we’ve done that, then we can do clinical studies in which we start to look at the predictive value of each of them.”
“There’s a lot of steps ahead of us,” van Helvert told us. “We’re in the very first stage.”
Post-embolization angiogram of the GPX embolic device filling a pelvic tumour (as featured on the cover of Journal of Vascular and Interventional Radiology, February 2024)
Fluidx Medical Technology has announced that the US Food and Drug Administration (FDA) has granted investigational device exemption (IDE) approval to initiate the GPX embolic device pivotal clinical trial. The objective of this trial will be to evaluate the safety and effectiveness of the GPX embolic device.
Embolization is a minimally invasive catheter-based procedure that blocks blood flow to targeted blood vessels and organs, the recent press release explains. Over US$3.5 billion per year is spent on embolic devices to treat tumours, internal bleeding, aneurysms, fistula, uterine fibroids, prostates, malformations, neurovascular bleeding, and other conditions throughout the body, but these devices can be difficult to prepare and deliver.
“The GPX Embolic Device will fill a void in our toolbox,” said Michael Darcy (Washington University, St Louis, USA) and past president of the Society of Interventional Radiology (SIR). “Its simplicity, visibility, and distal reach will allow us to achieve deep tumour occlusion independent of delivery technique.”
As many as twenty medical centres across the USA, Canada, and New Zealand will participate in the study, which will begin enrolling shortly.
“This study will further expand on the positive results we saw in our recent multicentre clinical trial,” stated Libble Ginster, president and CEO of Fluidx Medical Technology. “Clinicians need more solutions to meet diverse patient needs.” The results of that trial were recently published in the Journal of Vascular and Interventional Radiology (JVIR). In that trial, the GPX embolic device achieved 100% technical success and high usability scores from physicians for ease of preparation, deliverability, and visibility.
New two-year follow-up data from the BIOMAG-I first-in-human trial confirms a reliable and predictable long-term safety profile for Freesolve, the third-generation resorbable magnesium scaffold (RMS), establishing it as a true alternative to contemporary drug-eluting stents (DES). The results were presented by Michael Haude (Rheinland Klinikum, Neuss, Germany) at the 2024 EuroPCR conference (14–17 May, Paris, France).
At the 24-month follow-up, the incidence of target lesion failure (TLF) was 3.5% alongside a corresponding 3.5% incidence of target lesion revascularisation (TLR) compares favourably with various second-generation DES. No cases of myocardial infarction (MI), cardiac death, or definite/probable scaffold thrombosis were reported.
“At this two-year time point, the Freesolve RMS with its new Magnesium alloy which allows for increased radial strength, showed again excellent clinical and safety,” said Haude. “With this highly competitive device, we’re advancing towards a randomised trial BIOMAG-II to compare the advantages of a fully resorbable implant to a permanent DES that remains in the artery indefinitely.”
The initial findings from the BIOMAG-I study one year follow-up revealed excellent late lumen loss outcomes at both six and 12 months. Additionally it confirmed that the Freesolve RMS achieves complete absorption within 12 months post-implantation as a result of its proprietary BIOmag magnesium alloy.
“The new outcomes from the BIOMAG-I trial highlight a very promising future for the era of metallic resorbable magnesium scaffolds,” said Georg Nollert, vice president medical affairs, vascular intervention at BIOTRONIK. “This strengthens our dedication to innovate and progress through the Freesolve RMS technology, while continuously building strong clinical evidence to ultimately enable the optimal outcomes for patients.”
Additionally, the BIOMAG-II trial has started and is a prospective, international, multi-centre randomised-controlled study aiming to evaluate the safety and clinical performance of the new-generation Freesolve RMS, compared to a contemporary DES. The first patient has already been enrolled at the University Hospital Geneva in Switzerland. The study is primarily evaluating the TLF rate over a 12-month period with consecutive follow-ups.
FastWave Medical has been issued its fifth utility patent by the United States Patent and Trademark Office (USPTO), a press release reveals.
“FastWave’s IVL [intravascular lithotripsy] systems have been designed with physician input to deliver meaningful improvements for the management of calcific disease, which is one of the most difficult challenges we face in treating blood flow-limiting vascular blockages,” said Peter Schneider (University of California San Francisco, San Francisco, USA). “I am excited to witness FastWave’s team making tremendous advancements with their IVL technology, supported by a growing IP portfolio.”
According to a company press release, the newly granted patent bolsters the innovative design of Fastwave’s next-generation IVL platform, aimed at overcoming challenges associated with treating calcified arteries in patients with occlusive vascular disease. By developing advanced lithotripsy platforms, FastWave aims to address gaps in existing IVL options while enhancing ease of use and patient safety, thereby reducing procedural complications.
“This issuance of FastWave‘s fifth patent from the USPTO marks another milestone for our company and demonstrates clear progress with our unique IVL portfolio,” commented Scott Nelson, co-founder and chief executive officer of FastWave Medical. “The FastWave team highly values the collaboration with our medical advisors, translating real-world insights into compelling clinical solutions for the benefit of physicians and their patients.”
In one presentation, late-breaking data showed that endovascular therapy results in a one-third reduction in post-procedural complications for women with PAD, while another demonstrated that women and Asian Americans are less likely to undergo endovascular revascularisation for PAD compared to men and other races.
According to a SCAI press release announcing the results from these studies, PAD contributes to 400 amputations performed each day, with additional data highlighting a disproportional impact on underserved communities.
In addition, the release highlights a December 2023 American College of Cardiology (ACC) statement showing that data from up to 20 years ago highlighted racial and sex-specific disparities in treatment for PAD. “This underscores the need for more recent information on how PAD treatment impacts genders and races (medication, lifestyle changes, angioplasty and stent placement, or bypass surgery),” the SCAI press release reads.
“PAD is a prevalent and debilitating disease with serious consequences, especially for advanced cases that may have progressed due to lack of treatment, which is something that many clinicians are seeing in their patients today. Evidence-based data on treatment outcomes for all are critically important for individualised care,” said SCAI president George D Dangas (Icahn School of Medicine at Mount Sinai, New York, USA). “SCAI and its PAD Pulse Alliance partners have worked to close these gaps through the Get a Pulse on PAD campaign, which kicked off this year with resources for physicians and patients.”
At SCAI, one late-breaking presentation showed data supporting the effectiveness and safety of endovascular therapy with stent implantation as an alternative to bypass surgery in both women and men with PAD.
A literature search identified six randomised controlled trials comparing endovascular therapy with stent implantation (bare-metal, drug-eluting, or covered stent) versus bypass surgery with vein or prosthetic material in patients with symptomatic PAD involving the femoropopliteal segment. The primary endpoint was major adverse limb events (MALE), a composite of all-cause death, major amputation, or reintervention of the target limb. Other endpoints included amputation-free survival (AFS), the individual components of MALE, and primary patency. Early complications were defined as a composite of any bleeding, infection, or all-cause death within 30 days of the procedure.
Of 639 patients investigated, 185 (29.0%) were female. Baseline and procedural characteristics were comparable between patients randomised to endovascular therapy versus bypass surgery. At two years, there was no significant difference in the incidence of MALE between endovascular therapy and bypass surgery in women (40.6% vs. 42.1%, p=0.764; hazard ratio [HR] 0.93) and men (39.7% vs 34.4%, p=0.963; HR 0.98). Similarly, there were no differences in amputation-free survival (AFS), individual components of MALE and primary patency between endovascular therapy and bypass surgery regardless of sex. Endovascular therapy compared to bypass surgery was associated with a significantly lower rate of early complications at 30 days (8.7% vs. 25.96%, p=0.002 in women and 5.9% vs. 21.5%, p<0.001 in men) and significantly shorter hospital stay in both women and men (3.7±5.7 vs. 7.2±4.3 days, p<0.001 and 2.8±3.2 vs. 7.4±5.1, p<0.001).
“While the findings of the study are of value considering the scarce data on PAD treatment in women, they are also a strong reminder that we must do better in enrolling women in PAD trials. Women remain underrepresented in PAD trials and concerted efforts are warranted to achieve adequate representation of women to improve our understanding of the disease and its management in both women and men,” said Serdar Farhan (Icahn School of Medicine at Mount Sinai, New York, USA), lead author of the study. “Early diagnosis and guideline-directed medical therapy are key to improving outcomes of any treatment strategy for PAD.”
Another study presented at SCAI showed that women and Asian Americans are less likely to undergo endovascular revascularisation.
In this analysis, Bayesian machine learning-augmented propensity score translational (BAM-PS) statistics with multivariable regression was conducted for the largest US all-payor inpatient dataset, the National Inpatient Sample (NIS), from 2016 to 2020.
Of 148,755,036 adult hospitalisations, there were 17,173,000 (11.54%) with PAD, of whom 680,025 (3.96%) underwent inpatient endovascular revascularisation. Endovascular revascularisation prevalence increased steadily (0.46% to 0.49%, p <0.001). In BAM-PS multivariable regression adjusting for several clinical and demographic variables, female sex (odds ratio [OR] 0.54) and Asian versus Caucasian race (OR 0.66) significantly decreased the odds of endovascular revascularisation. Medicare versus commercial insurance (OR 1.17) significantly increased the odds of endovascular revascularisation (p<0.001). There were no significant differences in endovascular revascularisation mortality and cost when analysed by sex, race, and income (p>0.05 for all).
“Although not surprising, it is frustrating to see women and Asian Americans are less likely to undergo procedures that may prevent amputations or even death,” said Awad Javaid (University of Nevada, Las Vegas, USA), lead author of the study. “The results reinforce the need to change current practice by using a more inclusive and multidisciplinary approach to peripheral arterial disease interventions.”
Reflow Medical has announced completion of enrolment in the DEEPER REVEAL clinical trial to evaluate the Reflow Spur stent.
The company notes in a press release that the Spur—designated a Breakthrough Device by the US Food and Drug Administration (FDA)—is a unique clinical solution intended to provide stent-like results while leaving no metal behind. The study enrolled 130 patients in over 35 clinical centres in the USA.
“The steady rate of enrolment, along with the level of support from so many centres, has been impressive. The response reflects the huge unmet need for treatment options for CLTI [chronic limb-threatening ischaemia],” said S Jay Mathews (Bradenton Cardiology/Manatee Memorial Hospital, Bradenton, USA), one of the lead principal investigators (PIs). He continued: “We’re looking forward to next steps in working with the FDA to bring this technology to our patients.”
Mahmood K Razavi (St Joseph Heart & Vascular Center, Orange, USA), one of the lead PIs, commented: “As a physician who has worked with Reflow, I have followed the clinical data generated from the EU trials, which are very promising. I’m looking forward to seeing the final clinical data from the DEEPER REVEAL trial.”
The prospective, single-arm, multicentre study will examine the efficacy and safety of the Spur stent for the treatment of vascular lesions in the infrapopliteal arteries below the knee. A novel device intended for use in patients with CLTI, this retrievable scaffold therapy (RST) features a retrievable stent with radially self-expanding spikes that treat the diseased vessel wall without leaving anything behind.
Merit Medical Systems, a global leader of healthcare technology, has announced US Food and Drug Administration (FDA) 510(k) clearance for its Siege vascular plug. Merit also announced the launch of its Bearing non-spherical polyvinyl alcohol (nsPVA) Express prefilled syringe in the USA and Australia.
The latest additions to Merit’s embolics portfolio, Siege vascularplug and Bearing nsPVA Express, complement a comprehensive offering of microsphere, particle, and gelatine foam products supported by a range of microcatheters, guide wires, and other enabling devices.
Embolization is a minimally-invasive procedure where physicians implant devices or materials to occlude blood vessels or abnormal vascular channels. It may be used to stop bleeding or to block the flow of blood to a tumour or abnormal area of tissue. Embolization has made remarkable advances in recent years, becoming a widely adopted treatment option, the recent Merit press release states.
The Siege vascular plug has a highly deliverable, recapturable design that enables precise placement. The nitinol self-expanding plug achieves vessel occlusion within 1.3 minutes. Available in three sizes, Siege treats peripheral arteries 1.5mm to 6mm in diameter. All sizes of the Siege vascular plug are delivered with a microcatheter.
“The Siege Vascular Plug will be a valuable addition to my clinical practice. A plug with rapid occlusion, precise placement, and microcatheter compatibility is important to me,” said Gary Siskin (Albany Medical Center, Albany, USA), paid consultant of Merit.
The newly launched Bearing nsPVA Express is a 20mL, vacuum-sealed syringe prefilled with Merit-manufactured Bearing nsPVA embolization particles. Bearing nsPVA embolization particles are small, irregularly shaped, biocompatible, hydrophilic, and non-resorbable particles available in multiple sizes (45-1180µm). The preloaded syringe offers convenience and ease of use that can save clinicians’ time and minimise product waste. In hands-on testing, 100% of clinicians found the Bearing nsPVA Express to be easily incorporated into a procedure, and 75% said it was easier to use than the vial product.
“Bearing nsPVA Express streamlines embolization procedures. It eliminates a number of steps involved in using PVA in a vial,” said Jafar Golzarian, founder of Northstar Vascular and Interventional in Golden Valley, USA. “Unlike vial products, it’s ready to use, enabling interventional radiologists to focus on the procedure.”
As part of its commitment to innovation, education, and research in embolotherapy, Merit will participate in the 18th Annual Global Embolization Oncology Symposium Technologies (GEST) annual meeting (16–19 May, 2024, New York City, USA). In addition to introducing the Siege Vascular Plug and Bearing nsPVA Express, Merit will be exhibiting other embolic product solutions, including Embosphere microspheres, EmboCube embolization gelatine, and Torpedo gelatine foam. Merit will also feature the SwiftNINJA steerable microcatheter and the longer-length Merit Maestro microcatheter; both delivery systems are ideal for radial procedures.
Physicians can try these products through hands-on workshops held at the Merit booth. GEST attendees will also have access to Merit’s simulator for added prostatic artery embolization and uterine fibroid embolization experience involving Embosphere microspheres and other Merit devices.
“Merit is a leader in embolotherapy,” said Fred P Lampropoulos, Merit chairman and chief executive officer. “Through continued investment in new product solutions, we have developed a strong record of delivering meaningful innovation, new indications, and portfolio extensions designed to meet the needs of our healthcare partners. We look forward to demonstrating this excellence at GEST, showcasing the ways we help physicians deliver a better patient experience.”
Experience wall-to-wall thrombectomy in action with Manuela Konert from Leipzig, Germany! In this brief video, Konert walks through a deep vein thrombosis (DVT) case step by step using the ClotTriever system, providing valuable clinical insights along the way. Highlighting the safety and efficiency of wall-to-wall thrombectomy, Konert invites vascular specialists to join the discussion on DVT treatment at INARI’s symposium during the LINC 2024 (29th May at 12:45, Main Arena 2).
This video was filmed by Inari Medical and is being sponsored for distribution in association with Vascular News, Interventional News and Venous News. Biba Medical bears no responsibility for the assets used in the production of this video.
At this year’s Society of Interventional Oncology (SIO) annual conference (25–29 January, Long Beach, USA), Dimitrios Filippiadis (Athens, Greece) moderated and presented in a session focused on palliative interventions, an area of rising interest within interventional oncology (IO). Filippiadis is an associate professor of diagnostic and interventional radiology (IR) at the National and Kapodistrian University of Athens, whose practice centres on musculoskeletal (MSK) and oncologic interventions, and cancer pain management. Catching up with Interventional News, he gives an update on palliative care as it stands today, the treatments that work, and the broader significance of palliation in light of a global opioid crisis.
IN: What were the key takeaways from your presentation and the overall session at SIO?
My talk in this palliative session focused on injections for cancer patients, so the main focus was pain reduction, mobility improvement, and improvement of life-quality in cancer patients. The fact is that, currently, there is a very high percentage of cancer patients that experience pain. Almost 80% of patients will experience pain during the course of their disease, and the vast majority of these patients are not adequately treated for their pain today. Therefore, this is a very large patient pool that we need to help.
Specifically for nerves, we can inject a wide variety of different agents, ranging from corticosteroids, local anaesthetics, alcohol of phenol, and rarely, hyaluronate acid derivatives for intra-articular injections. For example, you have a patient who is suffering either from degenerative disease in the spine or from metastases in the spine, and the result is neuralgia going all the way down to the lower extremities. To help these patients, you can inject corticosteroids with local anaesthetic. If you want something more permanent, you can perform neurolysis. An alternative to that is temperature mediated neurolysis—which will use radiofrequency or cryoneurolysis—in order to destroy the nerves. When you are performing any type of neurolysis, you interrupt the pain signals from the periphery to the brain, providing the patient with immediate pain relief, which complements life quality improvement.
Let’s take, for example, pancreatic cancer—in the guidelines, neurolysis of coeliac plexus or splanchnic nerves is included for the management of pancreatic cancer-related pain. In the National Comprehensive Cancer Network (NCCN) guidelines from 2021, and in the revised version of 2023, IO techniques including injections, neurolysis, augmentation techniques and ablation, are included for the management of adult cancer pain. For too many years, myself and my colleagues believed that pain palliation is an extra fourth step in the well-known analgesic ladder from the World Health Organisation (WHO). But right now, everybody’s convinced that our techniques—IO percutaneous, minimally invasive techniques—are not an extra fourth step, but actually an intermediate step which should be performed before switching from weak to strong opioids. Thus, the earlier we perform this kind of therapeutic approach, the better the result we are seeing. By doing so, we can significantly reduce strong opioid administration and we can positively impact the global opioid overdose crisis.
IN: How significant is palliative care to your oncology practice?
Palliative care is a major part of our everyday clinical practice. In my hospital, we have weekly multidisciplinary board meetings to discuss pain management, which are held separately from the multidisciplinary team (MDT) tumour board meetings.
We have orthopaedic surgeons and neurosurgeons, medical and radiation oncologists, anaesthesiologists, interventional oncologists, and we speak about different cases with a clear focus on pain management. Therefore, for the last three years that we have been holding these meetings, running palliative procedures has become around 50% of our everyday clinical practice. There is also a wide variety of techniques that we can offer; as well as neurolysis, we offer ablation, vertebral augmentation, or bone augmentation techniques. For patients with lytic spinal or peripheral skeletal metastasis, which cause pain and mobility impairment, we can offer percutaneous ablation, which can result in both local tumour control, prolonged overall survival, and pain reduction followed during the same session by an augmentation technique for structural support.
Additionally, one of the greatest advantages of our percutaneous or transarterial approaches is that they can be combined in a single session. A patient can visit the hospital once and receive ablation, plus structural augmentation, and maybe transarterial embolization—whenever it’s necessary. This is not only beneficial for the patient, but for the hospital and its finances as well.
IN: What influences your judgement when deciding on a pain management pathway?
Following our weekly MDT meetings to decide which therapy should be performed, we consult with the patient to clearly explain what their expectations should be. Expectations differ case by case—you can have a patient with less extensive disease and the goal could be a combination of local tumour control, plus symptomatology improvement. You can have patients who have extensive metastatic disease and the goal there is to first identify the source of pain and treat it. In these cases, you will offer improvement of the symptomatology in terms of pain reduction and mobility improvement. And last but not least, you also have cancer patients who have been treated, but they’re suffering from pain as an adverse event of the treatment. For example, you can have breast cancer patients who have undergone mastectomy, or patients with lung cancer, who have undergone thoracotomy and, respectively, these patients after surgical operation might suffer from post-mastectomy or post-thoracotomy pain syndrome. We also help these patients with neurolysis by taking out specific nerves for each case.
Looking past pain, you can have patients suffering from other symptoms, such as breast cancer patients with hot flashes, or patients with abdominal malignancy that suffer from nausea or vomiting. Cryoneurolysis of specific nerve targets in specific cases can also help in improvement and resolution of these symptoms as well.
IN: Is every interventional oncologist equipped to provide pain palliation? What soft/hard skills are required to perform these techniques?
This is the million dollar question. As interventional oncologists, we are clinicians, we are fully fledged clinicians. And we should start by explaining to everybody that we are treating the patient and not the images. There is a long list of clinical skills that are required to first decide on the correct therapy and then perform this treatment. Interventional oncologists should be able to consult with the patient, analyse the medical and clinical record, see the list of drugs the patient is taking, identify the source of pain, the source of symptomatology in general—and this will happen if you combine clinical and physical examination with evaluation of the diagnostic imaging.
Once we have this ability—and trust me, interventional oncologists, we do have these abilities because we were trained for that—we can proceed for selection of an appropriate therapeutic technique. I strongly believe that interventional oncologists should be involved in the decision-making process, simply because we know better than anybody else, the advantages and disadvantages of our therapeutic approaches, and therefore we can offer an optimal utilisation of these therapies.
We should also be involved in the follow-up of the patient—in pain, I explain it to my patients through an example of an onion. There are lots of large layers on the outside which cover the smaller layers inside. When you remove these outer layers, you must check to see what effect this has had on the inner portion. Which is to say we should follow up with the patient to see whether additional treatments are necessary. In the era of personalised medicine, it’s not who owns the patient, but who is clinically responsible for a specific section of their disease.
Major interest in palliative treatments in IO has spiked in the last five to 10 years. This may perhaps be due to the opioid crisis, as previously mentioned, but also due to its inclusion in the 2019 NCCN guidelines. I have participated in a group of authors who published a paper in 2019 which has been referenced in The NCCN Adult Cancer Pain Guidelines. Pain has also had a major impact on cancer patients, and it can drive them away from systemic and local therapies. If you have a patient who is in pain, it’s not possible to expect them to sit still on the table during chemotherapy. So being able to offer them pain reduction is of utmost importance, and it has positive implications on many levels.
Late-breaking data from the ENGULF trial showed that a novel dual-action thrombectomy device was effective and safe in treating acute pulmonary embolism (PE). The safety and effectiveness results were presented today as late-breaking science at the Society for Cardiovascular Angiography & Interventions (SCAI) 2024 Scientific Sessions and simultaneously published in JSCAI.
PE is a serious cardiovascular event where a blood clot causes issues with blood flow and oxygen levels in the lungs. It can be life-threatening, with up to 30% of individuals dying within one month of diagnosis. Despite recent advances in therapeutic options, PE still carries a high risk of mortality and morbidity with few US Food & Drug Administration (FDA) -cleared thrombectomy catheters available to physicians.
The ENGULF trial is a prospective, single-arm, first-in-human, safety and feasibility study evaluating a novel embolectomy catheter system for the treatment of acute PE with a steerable and expandable funnel and an internal agitator, the Hēlo PE thrombectomy system. Patients underwent a pre- and 48-hour post-procedural computed tomography (CT) scan. The primary efficacy outcome was the percent difference in the pre-to-post procedural right ventricle–to–left ventricle (RV/LV) ratios. The primary and secondary safety outcomes were all-cause mortality, major life-threatening bleeding, device-related serious adverse events, pulmonary or cardiac injury, and clinical decompensation at 48 hours and 30 days post-procedure.
All 25 patients from eight centers underwent successful embolectomy. The mean RV/LV ratio was 1.53±0.27 at baseline and 1.15±0.18 at 48 hours post-procedure (23.2%±12.81% change). Of note, there were no major adverse events at 48 hours and no deaths at 30 days.
“Although more rigorous studies are needed, RV/LV ratio is the most important predictor of dysfunction and adverse outcomes in acute PE, and it is exciting to see that the RV/LV ratio reduction was just as much as other FDA-approved devices on the market without any large safety concerns in a new first-in-human device,” said Tai Kobayashi, assistant professor of Clinical Medicine at Penn Medicine, and lead author of the study. “This technology represents the marriage between large and small-bore embolectomy, which allows for operators to travel through the heart with a smaller catheter but expand a larger funnel that matches the size of the large bore catheters – leaving a smaller footprint and lowering the risk of hemodynamic impact for the patient.”
“For the field of interventional PE therapies to fully reach its promise, continued innovation is needed to optimize our procedural workflows across the wide array of patients affected by this disease,” said Jay Giri, director of the Cardiovascular Catheterization Laboratories at the Hospital of the University of Pennsylvania in Philadelphia, USA, senior author of the study, and national principal investigator of the study. “The ENGULF trial is an important step in this process, demonstrating that a novel, purpose-built PE thrombectomy catheter can achieve excellent results even among its earliest users.”
New data from the REAL-PE analysis investigated catheter-based pulmonary embolism (PE) treatment, showing women and Black people were less frequently treated with minimally invasive therapy compared to men or non-Black patients. The late-breaking results were presented today at the Society for Cardiovascular Angiography & Interventions (SCAI) 2024 Scientific Sessions.
REAL-PE analyzed data from patients within the Truveta database diagnosed with PE and treated with USCDT or MT for PE. Patient characteristics including race, ethnicity, age, sex, comorbidities, and prior diagnoses were assessed to investigate their association with the type of treatment used. Of the more than 430,000 patients diagnosed with PE, about 2,000 patients analyzed were treated with one of the invasive therapies. Women or Black patients were less frequently treated with invasive therapy than men or non-Black patients. Moreover, women more than men and white people more than Black people had higher bleeding rates.
“Although this data demonstrates the value of real-world data in the assessments of new technologies in which randomized data are not always available, there is still work that needs to be done to evaluate the current utilization of advanced therapies for PE in underrepresented patient populations,” said Sahil A. Parikh, MD, Associate Professor of Medicine, Columbia University Irving Medical Center in New York City, and lead author of the study. “Evaluating care disparities in real clinical practices is key to addressing the existing barrier and improving patient outcomes.”
Results from Acute Pulmonary Embolism Extraction Trial with the AlphaVac System (APEX-AX) finds significant improvement in right ventricle function and minimal major adverse events.
New data from APEX-AV demonstrated that catheter-directed mechanical thrombectomy is safe and effective in patients with acute intermediate-risk pulmonary embolism (PE) with significant improvement in the right ventricle (RV) function and minimal major adverse events. The safety and efficacy results from the prospective trial were presented today as late-breaking science at the Society for Cardiovascular Angiography & Interventions (SCAI) 2024 Scientific Sessions.
The APEX-AV trial is a prospective, single-arm, multicenter investigational device exemption trial in which patients with acute intermediate-risk PE were treated with the AlphaVac F1885 aspiration system. The primary efficacy endpoint was a change in the right ventricle-to-left ventricle (RV/LV) ratio from baseline to 48 hours post-procedure on core lab–adjudicated computed tomography angiography. The primary safety endpoint was a composite of 48 hours post-procedure major adverse events: device-related death, major bleeding, and device-related serious adverse events.
Among the 122 patients treated at 25 U.S. sites, the average reduction in the RV/LV ratio was 0.45 with a 35.5% mean percentage reduction in the overall clot burden from the baseline at 48 hours post-procedure. Five patients had major adverse events within the 48-hour visit and no death was reported. Lastly, procedural times were short with a mean procedural time of 37.2 ± 17.7 minutes.
“Pulmonary emboli can be extremely dangerous and require effective and prompt action,” said William Brent Keeling, MD, Associate Professor at the Emory School of Medicine in Atlanta, Georgia, and lead author of the study. “Catheter-directed mechanical thrombectomy using a new aspiration system can achieve excellent thrombus removal with a wonderful safety profile, thus enabling more tools in our armamentarium for the treatment of acute PE.”
Using Chat generative pre-trained transformer (GPT) to understand the public perception of interventional radiology (IR), Chloe Cross (Icahn School of Medicine at Mount Sinai, New York, USA) and colleagues presented new data which provide “exciting” insights into how and when IR is suggested for treatment for patients using artificial intelligence (AI).
Cross et al detailed their study titled ‘Settling turf wars: When does ChatGPT refer you to an interventional radiologist?’ at the Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA), in a session dedicated to emerging technologies within IR.
Developed by OpenAI, ChatGPT is a conversational AI-based chatbot which provides answers to questions or prompts. “Although it’s not specifically designed for medicine,” Cross explained, “many patients are using ChatGPT for medical decision-making—similar to how patients use WebMD. Our purpose was to understand public perception of IR and when IR treatments are offered.”
Cross and colleagues developed a standardised prompt that reflected a realistic patient query, adhering to a ‘I have a disease process, what type of doctors can treat this?’ formula. The researchers created a list of disease processes in various systems treated by IR which were selected from a literature review. Each prompt was repeated three times and then the number of times IR was suggested and an average rank was recorded.
Their results showed that ChatGPT mentioned IR in 51 (73.9%) of 69 prompts, with an average rank of 3.3. Of all the disease states, IR was consistently ranked first for stroke angiography and splenic artery aneurysm embolization. Cross offered that for the splenic artery, this result may be due to the level of literature published on this diagnosis in IR. “We are pretty much the only ones who are doing splenic artery aneurysms in the recent past, so you can see where this result is coming from. It speaks to the importance of having our name in new searches published in these realms.”
Their data, however, showed that IR was not suggested for the treatment of pulmonary embolism (PE) or image-guided bone biopsy, and was only suggested once for the treatment of benign prostatic hyperplasia. Interestingly, Cross added that IR was only mentioned once and ranked far behind other specialties for image-guided percutaneous ablation of renal carcinoma, a treatment frequently performed by interventional radiologists.
“It’s important to note that IR was cited for the treatment of many diseases, which is quite exciting. This may help to improve patient awareness of IR, especially for referrals,” said Cross. Yet, she stated that these data indicate a “need for more public outreach” concerning the disease processes such as PE where IR was not indicated.
One limitation of their study was that they do not know the “inner workings” of ChatGPT, Cross relayed, so any conclusions drawn may be speculative. There is also little understanding of how patients are interacting with the technology as it is still relatively new.
“New versions of these large language models are coming out constantly. We may see changes in the generative answers that we obtain from this research, however for now, ChatGPT can help us understand public perception of IR and we are being suggested for many diseases we are able to treat, so that is very exciting,” Cross told attendees. She concluded that future research should explore ChatGPT’s role in medicine in order to better understand how the patient pathway to IR can be expedited through this new technology.
Today, Penumbra announced the launch of its Midway 43 and Midway 62 delivery catheters, which are designed to provide ideal tracking and a stable platform to support the delivery of various embolisation therapies in the neurovasculature. This news came on the same day that the company also announced the CE-mark certification and European launch of three of its reperfusion catheters for acute ischaemic stroke: Red 43, Red 72 with Sendit technology, and Red 78.
Based on the company’s Red catheter technology, Penumbra describes its newly launched Midway intermediate catheters as a “significant advancement” in the intermediate access device market—which has seen “minimal innovation over the last decade”.
“The field of neuroendovascular surgery continues to evolve and expand in both scope and expectations of efficacy, creating increasing demands for technical efficiency and safety,” said John Chaloupka (Mount Sinai Medical Center, Miami, USA). “This trend is taking operators into more challenging technical scenarios, such as microcatheterisation into far distal target lesions, tortuous intracranial vasculature, and unfavourable aortic arch/neck anatomy. As such, use of so-called ‘intermediate access guiding catheters’ has become an important technological requirement towards achieving these goals. Penumbra’s portfolio of Midway intermediate catheters now provides us with highly engineered technology that provides an optimal balance of support and trackability in a wide range of applications.”
Compatible with Penumbra’s Benchmark 71, BMX 81 and BMX 96 access systems, the new Midway catheters are engineered to enable the precise delivery of distal microcatheters, embolisation coils, intrasaccular devices, and flow diverters, according to a company press release. For each therapeutic approach, the release continues, Midway catheters are designed to provide a critical balance between trackability and support, which is achieved through their advanced catheter design, full-length polytetrafluoroethylene (PTFE) liner, and distal hydrophilic coating.
“The innovative design of the new Midway intermediate catheters incorporates Penumbra’s advanced Red catheter technology, providing physicians with optimal support,” said James Benenati, chief medical officer at Penumbra. “With these solutions, clinicians can expect unparalleled performance and reliability, ultimately leading to better patient outcomes.”
In addition, Penumbra claims in a second recent press release that the launch of its Red 43, Red 72 with Sendit technology and Red 78 products in Europe will expand the company’s neurovascular offerings designed for acute ischaemic stroke.
“I’m thoroughly impressed with the currently available Red aspiration catheters’ precision in navigating and removing clots,” said Levansri Makalanda (Barts Health NHS Trust, London, UK). “I’m eagerly anticipating the Red 43, Red 72 Sendit and Red 78, which promise to enhance both the reach and efficiency of clot extraction.”
Optimising science-based aspiration thrombectomy (S-BAT), these devices are engineered with the latest technology in trackability and aspiration to address a wide range of large vessel occlusions, the release adds. The Red catheters feature Redglide technology, which enhances the trackability of the catheters as they navigate the challenging vasculature of the brain—and, additionally, Penumbra says these catheters have a full-length PTFE liner designed to maintain their true lumen size under a powerful vacuum, further maximising aspiration efficiency.
“Penumbra’s latest innovations offer physicians more options to provide care to their patients, regardless of the clot location,” said Joan Kristensen, head of the Europe, Middle East and Africa region for Penumbra. “Our focus is on pioneering technology and expanding access to these innovations with a goal of advancing the delivery of patient care in Europe, and improving patient outcomes.”
Etienne Garin (Centre Eugene Marquis, Rennes, France), presenting results from an ad-hoc interim analysis of the PROACTIF trial data, reported that “appropriately selected” patients who received transarterial radioembolization (TARE) with yttrium-90 (Y90) glass microspheres within a “personalised treatment plan” for primary and metastatic liver tumours—including intrahepatic cholangiocarcinoma (ICC)—achieved “long survival” and had a “low adverse event rate”.
Sharing these findings at the European Conference of Interventional Oncology (ECIO) annual meeting (28 April–1 May 2024, Palma de Mallorca, Spain) during the Best of ECIO session, Garin detailed the aims of the PROACTIF (Prospective post-approval multi-centre, open-label, non-interventional registry study to evaluate effectiveness of TheraSphere [Boston Scientific] in clinical practice in France) registry—the “largest Y90 registry in liver cancer” to date, he stated. Selecting ICC patients only, amounting to 168 of the 1,088 patients included in the registry, Garin and his team obtained real-world effectiveness, quality-of-life and safety data using TheraSphere Y90 microspheres, primarily measuring overall survival. Secondary endpoints were defined as adverse events and serious adverse reactions.
Garin then gave an overview of key characteristics of their patient cohort. He highlighted that: 52.4% of patients identified in this subgroup were female; median age was 69 years; 57.1% were marked as 0 using the Eastern Cooperative Oncology Group (ECOG) performance status scale; 31.5% had associated liver fibrosis/cirrhosis; and mean index lesion length was 70.7mm. Prior to Y90 treatment, 48.8% were treatment naïve and 37.5% had previous treatment (systemic, n=56; locoregional, n=6; liver surgery, n=10). Personalised treatments comprised of multicompartment dosimetry (63.1%); ultra-selective or selective treatment (53.6%); and repeat treatments—two (23.2%) or three (1.2%).
At a median follow-up of 18.2 months, Garin stated that median overall survival was 18.1 months, which he commented is an “interesting result in this cohort of non-resectable ICC patients”. Adverse events were experienced by 14 patients, and 13 patients had serious adverse reactions—10 device- or procedure-related and four hepatobiliary-related.
“This ad-hoc analysis demonstrates that TARE—when used in personalised treatment, including multicompartment dosimetry and repeat treatments, results in a favourable risk-benefit profile with long survival and low adverse event rates,” Garin said. Closing his talk, Garin added that the final results for the PROACTIF study are set to be released in 2025.
This advertorial, sponsored by Varian, is only available in selected countries and geographies.
In the realm of interventional radiology (IR), technological advancements and innovation are continuously reshaping the landscape of patient care. This has become more evident in recent years in the field of ablation, which has long been a staple for a range of oncologic and interventional treatments. As technology continues to evolve, however, so too does the need to refresh the ablation space to keep pace with innovation and patient-specific needs.
Microwave ablation (MWA) has emerged as an effective treatment modality for hepatocellular carcinoma (HCC) and metastatic liver cancer (mCRC), and as a promising alternative to surgery for in selected patients. However, as MWA assumes a more prominent role in treating primary and metastatic liver cancers, there is a concurrent need for an update in technologies that reflect the advancements that have been made in improving procedural predictability and outcomes.
Imaging and therapeutic advancement
One of the key areas driving the need for advancements is the significant progress in therapeutic and imaging technologies. These advancements have enabled medical professionals to target and treat abnormal tissue with improved accuracy, minimising damage to surrounding healthy tissue and improving patient outcomes.
With the current technologies, physicians can face challenges ablating large tumours that require the use of more than one probe. This can result in overlapping ablation zones, creating procedural complexity, as well as necessitating extensive planning to ensure the best positioning of probes to treat the patient with confidence. The ability to consistently predict and plan what is needed for individual patients is essential. When planning, parameters that need to be considered can include temperature, power, or number of probes, which are all necessary factors to gain a real-time, accurate understanding of the ablation zone.
To meet expectations of interventionalists today, ablative technologies should incorporate continuous registration capabilities throughout the procedure to ensure precise localisation of the patient’s anatomy. As physicians ablate, the initial target may become obscured, making accurate targeting difficult. With current tools that cannot always guarantee repeatability, interventionalists must have extensive experience to achieve consistent accuracy.
The ongoing Ablation with Confirmation of Colorectal Liver Metastases (ACCLAIM) prospective trial for MWA as definitive local tumour control (local cure), seeks to confirm the importance of ablative technologies, and the potential of MWA to treat metastases that can be ablated with sufficient margins. Led by Constantinos T Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA) et al, the researchers hypothesise that MWA of colorectal liver metastases (CLMs) of ≤2.5cm with confirmation of an ablation margin over 5mm, will achieve definitive local tumour control (local cure) with minimal morbidity. Currently, this international study is enrolling subjects with one to three CLMs using any United States Food and Drug Administration (FDA)-cleared or CE-marked MWA device. The procedure will be performed with the intent to create a minimum margin of ablation of 5mm, ideally ≥10mm from the edge of the target tumour to the ablation periphery. Minimum margin size will then be assessed immediately after MWA using an FDA cleared image-processing software to provide a three-dimensional (3D) assessment of the ablation zone and margin.
“If someone is doing liver tumour ablation, they should be doing margin confirmation in some way, shape or form, 100% of the time, to ensure good clinical outcomes. Newer technologies will make it better for physicians not doing it every day to achieve this,” said William Rilling (Medical College of Wisconsin, Milwaukee, USA) and ACCLAIM investigator during a recent interview featured on VISion—Varian’s blog about breakthroughs, resources, and expert insights for IR professionals.
The ACCLAIM trial seeks to affirm the importance of margin confirmation and pre and postprocedural imaging, driving a much-needed update in technologies that are utilised for MWA. Co-sponsored by Varian, the trial reflects Varian’s commitment to advancing procedural efficiency to support interventional radiologists in the future.
New groundbreaking technology
At the recent Society of Interventional Radiology (SIR) annual meeting (23–28 March, Salt Lake City, USA), Varian announced its newest ablation technology. The IntelliBlate MWA system* by Varian, a Siemens Healthineers company, combines microwave technology with advanced imaging capabilities.
Aiming to meet elevated levels of performance required to achieve optimal patient outcomes, IntelliBlate MWA system allows clinicians to tailor treatment plans to each patient’s unique anatomy and pathology. With its real-time monitoring and feedback capabilities, the system provides visual and audible cues to streamline setup and interaction for the clinician.
“This is a tangible result of our synergy and collaboration with Siemens Healthineers— IntelliBlate [is] the cornerstone of a future-focused integrated imaging and treatment ecosystem from a single provider,” said Frank Facchini, president of Varian Interventional Solutions during the unveiling of the system.
The IntelliBlate system
The system also includes the Ximitry* probe, which is comprised of a laser alignment disc, LED status indicator, fixed burn centre with symmetrical ablation zone growth pattern, and intuitive temperature sensors. Varian believes that a single Ximitry probe can be used for large ablation zones, sparing healthy tissue and providing consistent control across diverse tissue types, leading to optimal treatment outcomes while minimising the risk of complications.
The IntelliBlate system also integrates with the myAblation Guide* software and is further complemented by the myNeedle Companion workflow, which is available on select Siemens Healthineers imaging systems. This enables healthcare providers who use a range of systems to seamlessly transition their ablation practice to align with the most recent innovations.
Next-generation microwave ablation
The need to advance the ablation space is apparent. Due to the rapid advancements in both therapy and imaging technologies, interventionalists and innovators alike strive to provide patients with the best possible care. The IntelliBlate MWA system has the potential to reshape the landscape of ablation therapy and to provide better procedural control for physicians.
“Our dedication to understanding the performance of our new microwave ablation system goes beyond conventional preclinical research. We have invested significantly in gathering comprehensive data across various tissue types, including perfused tissues. This extensive preclinical testing has provided robust insights that we believe truly distinguish our next-generation microwave system,” says Theresa Caridi, director of medical affairs at Varian Interventional Solutions.
In summary, with the latest addition to Varian’s arsenal of tools soon to be available, innovative solutions aimed at improving predictability and planning when providing ablative therapies are on the horizon. Among the evolving technologies, the IntelliBlate MWA system is noteworthy for its potential to influence the direction of ablation therapy, with the goal of pursuing improved outcomes in this patient population.
References:
Han Y, Zhao W, Wu M, Qian Y. Efficacy and safety of single- and multiple-antenna microwave ablation for the treatment of hepatocellular carcinoma and liver metastases: A systematic review and network meta-analysis. Medicine (Baltimore). 2022 Dec 23;101(51):e32304. doi: 10.1097/ MD.0000000000032304. PMID: 36595779; PMCID: PMC9794220.
Dou Z, Lu F, Ren L, Song X, Li B, Li X. Efficacy and safety of microwave ablation and radiofrequency ablation in the treatment of hepatocellular carcinoma: A systematic review and meta-analysis. Medicine (Baltimore). 2022 Jul 29;101(30):e29321. doi: 10.1097/MD.0000000000029321. PMID: 35905207; PMCID: PMC9333547.
Tang Y, Zhong H, Wang Y, Wu J, Zheng J. Efficacy of microwave ablation versus radiofrequency ablation in the treatment of colorectal liver metastases: A systematic review and meta-analysis. Clin Res Hepatol Gastroenterol. 2023 Aug;47(7):102182. doi: 10.1016/j.clinre.2023.102182. Epub 2023 Jul 20. PMID: 37479137.
Benson AB, D’Angelica MI, Abbott DE, et al. Hepatobiliary Cancers, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2021;19(5):541-565. Published 2021 May 1. doi:10.6004/ jnccn.2021.0022
This four-page supplement shares insights given by key opinion leaders in selective internal radiation therapy (SIRT) using SIR-Spheres Y-90 resin microspheres (Sirtex Medical). Taking place at the SUMM90YT conference (23 February, Frankfurt, Germany), hosted by Sirtex, the meeting featured multidisciplinary discussion and debate on patient selection in hepatocellular carcinoma (HCC) and metastatic liver tumours from primary colorectal cancer (mCRC) refractory to or intolerant of chemotherapy, and technical advancements to date.
Global network connection. World map point and line composition concept of global business. Vector Illustration
Left to right: Alda Tam, Constantinos Sofocleous, Robert Morgan, Hiroshi Kondo, Parag Patel, Denis Szejnfeld, Christoph Binkert
During the Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA), interventional radiology (IR) societies from nations worldwide sat around a table to consider the status of IR in their geographies. The Global Society Summit—the first meeting of its kind—heard international IR leaders discuss and define common challenges, to track a path for multinational collaboration and sustain a unified voice for IR in an increasingly competitive global healthcare environment.
Thirteen panellists in attendance, representing IR societies from every global continent, stood and updated the room on the status of IR in their country. “It’s heartening to hear that many of our challenges and thought processes are very similar worldwide,” said Alda Tam (MD Anderson Cancer Center, Houston, USA), SIR president and co-coordinator of the summit. Although at different stages down the path to subspecialty and specialty status, each society reported strikingly similar challenges, namely the recognition of the importance of clinical care in IR, difficulties with standardisation and training, practice economics and specialty distinction.
The IR clinical practice model was first to be dissected by the panel. SIR international division councillor and panel moderator Constantinos T Sofocleous (Weill Cornell Medical College Memorial Sloan-Kettering Cancer Center, New York, USA) began by discussing the value of routine outpatient IR clinical practice with longitudinal care for patients. Taking a poll, the majority of the panel agreed on the value of IR clinics and indicated that they offer this service.
“I think that in the USA,” said Parag Patel (Medical College of Wisconsin, Milwaukee, USA) following this poll, “one of the critical aspects for our recognition as a specialty and from other specialties was the recognition that we take care of patients with the diseases that we manage.” Until the American Board of Medical Specialties recognised the important role that interventional radiologists play in the “longitudinal management of disease going forward”, he said, there was “no path to specialty”. However, he added that a young trainee who wants to take care of patients and do procedures will likely pursue an IR-dedicated training pathway that “involves or invokes” clinical practice as “mandatory”, Patel noted. This, however, is a highly streamlined training modality that is not frequently offered worldwide.
Adding to this point, Robert Lookstein (Icahn School of Medicine at Mount Sinai, New York, USA) noted that these direct training pathways are “critical to the success of [IR] at a global level”. Yet, in an effort to “refocus”, he shared data from a survey his centre carried out which asked US IR chiefs or clinical leads whether or not they provide outpatient clinical services. They found that 76% said yes and 24% said no, and these figures were similar when the same question was asked for inpatient services. “I share these because there are clearly opportunities for improvement, to meet the goal that we’re all stiving for here. We all want IR to have a singular focus on longitudinal clinical care to achieve clinical excellence. Is the distribution of clinical services similar in other countries?” Lookstein asked.
“In Europe, I think that the numbers are much lower,” said Christoph Binkert (Kantonsspital, Winterthur, Switzerland), “but heterogeneity is much higher, not just across Europe but even within my country.” Although Binkert noted that Switzerland is not entirely representative of Europe, he explained that outpatient clinics have become the norm. “All of the big players do it—if you’re not offering outpatient clinical care, patients will not come to you.”
In the UK, Robert Morgan (St George’s Hospital NHS Foundation Trust, London, UK)—British Society of Interventional Radiology (BSIR) president and co-coordinator of the summit—shared that being given “permission” to provide outpatient clinics is not always given in UK hospitals for interventional radiologists. He believes that there is “much to be done” to increase recognition by UK Hospital Trusts of dedicated, protected time, within work hours to see patients before procedures and at follow up in outpatient clinics.
In Denis Szejnfeld’s (Certa Hospital, São Paulo, Brazil) view, issues arise as interventional radiologists often do not specialise early in training. Confirming this statement, Ethel Rivas Zuleta (Universidad Dr José Matías Delgado, La Libertad, El Salvador) commented that in Latin America, graduates must choose between two paths early in their training—private practice or institutional national practice, also referred to as academic hospitals, which leaves little room for deviation.
In other nations worldwide, training can be limited due to a lack of resources, as audience member Chidubem Ugwueze (Icahn School of Medicine at Mount Sinai, New York, USA) conveyed. Addressing the panel, he explained his involvement with a training programme in Nigeria which provides a well-rounded IR course preparing trainees for the European Board of Interventional Radiology (EBIR) examination.
He referenced one of his trainees who he says has all of the clinical requirements he would need to pass the EBIR examination—this is not the issue in these African nations, he said. “The biggest obstacle is that trainees can have all of the technical skills to do the procedures, but they don’t have reliable access to the devices needed to perform these,” Ugwueze said. “I see a lot of big names in this room who can move mountains and change these circumstances. I also see people who have already solved these problems elsewhere—how would you go about changing this?” he asked.
In response to Ugwueze, interventional radiologist Sangjoon Park (Seoul National University Hospital, Seoul, South Korea) shared his experience in Ethiopia and recounted difficulties in transporting enough lipiodol to the centre there. Park averred that trainee interventional radiologists there should not be trained in these procedures if they have no access to the devices/therapeutic agents. “Bottom line, there’s some things that you can do and some things that you can’t—so you have to decide on what procedures you can do to the best of your ability.”
“I did not want to touch on the lack of materials,” Rivas Zuleta commented. “Coming from Latin America, these disparities are ingrained, and what we must focus on is these materials come from companies who earn millions of dollars/euros in Europe and the USA. They aren’t going to give us free products, so we have to focus on what we can do.”
Referencing a previous session that day—Extreme IR—Rivas Zuleta noted that her first thoughts were “oh my god, what an expensive case”. In this session, one particular case reported the use of 12 coils for a single patient. “All I was thinking was, ‘I wouldn’t be able to use coils for the rest of the year’. Coming from relatively low-income countries means that we have to focus on what procedures are possible for us,” she said.
Another voice from the audience was past president of the Society of Interventional Radiology (SIR) Brian Stainken—interventional radiologist and current co-editor-in-chief of Interventional News—who stated he was “a little disappointed” more speakers had not addressed a glaringly obvious issue. “I’m old enough now to know it’s all about the dollars. Practice economics is something that isn’t much talked about on the international stage but it’s very real. There are lots of reasons given to why these medical device companies aren’t selling in these countries, but the big one is there’s no market. There’s no market because the market hasn’t been made.”
Wael Saad (University of Utah, Salt Lake City, USA)—representing the Society of African Interventional Radiology and Endovascular Therapy (SAFIRE)—responded that each society can help to “push in the right direction” in terms of moving mountains for countries requiring resources. “It’s very impactful for physicians in Africa to be able to help patients in need with minimal equipment and there is a lot of need there. An advantage of progressing from behind is that you learn from others’ mistakes and misfortunes,” Saad added.
Closing the summit, Morgan asked the panel how they believe the forum should go forward, to which Patel added that, yes, although their needs are varied, how can they “identify and prioritise support needed in each region?” Patel continued that the forum is intended to be a “continued effort in partnership with SIR and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE)”, holding global summits at each of their respective meetings to “continue conversations, identify society needs and maintain collaboration to elevate IR, so that it is recognised universally as a distinct specialty that can provide exquisite care”. Sofocleous indicated that on behalf of SIR alongside Patel and Morgan, the summit will prioritise the described international IR needs for the next agenda to be discussed at CIRSE 2024 (14–18 September, Lisbon, Portugal). The coordinators stated that this inaugural summit is the “first of many” that will help to empower local interventional radiologists. In doing so, they hope to join international forces to increase IR outreach in each corner of the globe.
In April, the most popular stories from Interventional News included highlight research from the Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA); Andrew Holden (Auckland City Hospital; University of Auckland, Auckland, New Zealand) shares his thoughts on the paclitaxel mortality controversy ahead of the Charing Cross (CX) Symposium 2024 (23–25 April, London, UK); and new research which finds early DAPT, statin therapy and stent patency are among predictors of good post-thrombectomy outcomes, among several others.
AngioDynamics has announced that the US Food and Drug Administration (FDA) has cleared the AlphaVac F1885 system for the treatment of pulmonary embolism (PE), enhancing its utility in critical medical scenarios such as PE.
The EMBOLIZE trial, a prospective, randomised controlled trial—the first of its kind—was recently launched at the Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA), and seeks to investigate the effects of ovarian vein embolization (OVE) and pelvic vein embolization in reducing symptoms in women experiencing chronic pelvic pain due to pelvic venous disease (PeVD).
Hotly debated across SIO annual conference programme, speakers took to the stage to contest the survival of transarterial chemoembolization (TACE) in the age of yttrium-90 (Y90) transarterial radioembolization (TARE) and immunotherapy, their compelling arguments making some audience members “more confused and others happy”.
The Society of Interventional Radiology (SIR) Foundation, The VIVA Foundation and Penumbra, today announced the launch of the EMBOLIZE trial, a first-of-its-kind prospective, randomised controlled trial studying the effects of ovarian vein embolization (OVE) and pelvic vein embolization in reducing pain in women experiencing chronic pelvic pain due to pelvic venous disease (PeVD).
Bien Soo Tan is a senior consultant at the Department of Vascular and Interventional Radiology (IR) at Singapore General Hospital (SGH). Following his recent acceptance of the Society of Interventional Radiology (SIR) Gold Medal award, Tan speaks to Interventional News about his achievements to date.
Cerenovus, part of Johnson & Johnson MedTech, has today announced the launch of Cereglide 71 aspiration catheter in Europe, an aspiration catheter equipped with TruCourse technology, indicated for the revascularisation of patients suffering from acute ischemic stroke.
New research to be presented at the Society of Interventional Radiology (SIR) annual scientific meeting has found early intervention with uterine artery embolization (UAE) can help women avoid hysterectomy due to severe bleeding after childbirth.
“These will be important, salutary lessons. Should a controversy arise again involving a proven efficacious therapy, we now know that stopping access to that therapy may result in unwanted and unexpected negative effects on patient care.” These are the preluding thoughts of Andrew Holden (Auckland City Hospital; University of Auckland, Auckland, New Zealand)—one of the Charing Cross (CX) Symposium 2024 (23–25 April, London, UK) co-chairs—ahead of this year’s meeting, referencing the paclitaxel mortality controversy.
An analysis involving some 300 patients with anterior-circulation acute ischaemic strokes caused by tandem lesions has determined a number of factors that may be predictive of good clinical outcomes at three months following an endovascular mechanical thrombectomy procedure.
This year’s Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA) gave recognition to select abstracts during the closing plenary session. Introduced by SIR 2024 programme chair Bulent Arslan (Rush University, Chicago, USA), who commended the “strong” and “compelling” presentations, speakers offered data which challenge preconceptions about disease states and treatment strategies.
As a member of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) social media subcommittee, Evgenia Efthymiou (University of Athens, Athens, Greece) expands on the importance of visibility and the valuable interventional initiatives that can be achieved online.
The advent of social media has generally transformed the healthcare landscape, facilitating communication, collaboration, education, and patient-centred care. Interventional radiology (IR), a technologically driven specialty, inevitably experiences the impact of platforms like X, LinkedIn, Facebook and Instagram. Past research has shown a significant increase in the adoption of social media within the radiology community,1 while a recent Australian study showed that the majority of interventional radiologists use at least one social media account.2
Sharing educational content, such as intriguing cases and innovative approaches to complex clinical scenarios, is among the most prevalent and efficient use of social media within the IR community.3 Εvery post with a popular hashtag could be widely shared and may commence a vivid discussion regarding technical details, risk of complications and postoperative care etc.
Educational posts are shared not only among qualified interventional radiologists, but also between medical students and residents. It is essential to highlight the role of social media in early medical education, as nowadays, multiple accounts are available on X (@ETF_IRtrainees, @IR_Juniors) along with Instagram and Facebook accounts and groups, which provide a wealth of images and case-based discussions about IR. The importance of social media use in early medical education and during residency could be easily addressed, by observing the constant increase of followers across various accounts as well as the increasing frequency of reposted content.
Social media serves as a crucial platform for mentoring and motivating medical students and young interventional radiologists. Presently, numerous accounts are accessible, providing students, prospective residents, and fellows with insights into the daily experiences of IR and the training programmes available. These accounts may belong to societies and training centres, but they can also be managed by current trainees and interventional radiologists, who—in a more direct and personal manner— share insights into their training journey and the challenges they face.
Besides educational purposes, social media facilitates communication and interaction, allowing active participation in online discussions. These interactions are instrumental in developing a professional network and can enhance one’s career by creating opportunities for collaboration. Platforms like LinkedIn or ResearchGate showcase individuals’ curriculum vitae (CV) and research interests, facilitating recruitment efforts and enabling participation in multicentre research projects. It has also been proven, that sharing research via social media is linked with higher citation rates.4 In addition to personal accounts, radiology departments, journals and radiology professional societies use social media platforms for research dissemination.
Social media can also raise awareness among other medical professionals and patients, advocating for the important role of IR in modern medicine. It highlights the availability of alternative minimally invasive treatments and showcases the positive impact IR procedures can have on patients’ lives.
A primary concern regarding the use of social media in healthcare is the potential breach of patient confidentiality, which can occur easily. Discussing specific procedural details or complex and rare cases could compromise patient privacy. Additionally, social media platforms do not undergo the rigorous peer review process of scholarly articles, making them susceptible to misinformation. Therefore, each post should undergo further personal review before dissemination. Lastly, maintaining professionalism consistently in all interactions is crucial, as misunderstandings can easily occur.
To sum up, social media has become an indispensable aspect of the contemporary world, including within IR, providing a multitude of opportunities such as promoting medical education, fostering career development, facilitating networking, and disseminating research, among others. As we expand our presence on social media, the field of IR will have greater influence in the swiftly changing medical environment.
References:
Patel SS, Hawkins CM, et al. Professional social networking in radiology: Who is there and what are they doing?. Acad Radiol. 2017;24(5):574-579. doi:10.1016/j.acra.2016.09.026
Wang MT, Foo M, Maingard J, et al. Social media in interventional radiology. J Med Imaging Radiat Oncol. 2021;65(2):182-187. doi:10.1111/1754-9485.13142
Kassin MT, Ukeh I, Bunch PM, Sabri SS. Social media considerations for the interventional radiologist. Radiographics. 2022;42(6):E165-E166. doi:10.1148/ rg.220157
Widmer RJ, Mandrekar J, Ward A, et al. Effect of promotion via social media on access of articles in an academic medical journal: A randomized controlled trial. Acad Med. 2019;94(10):1546-1553. doi:10.1097/ ACM.0000000000002811
Evgenia Efthymiou is an interventional radiologist at the Attikon University Hospital, Athens, Greece.
Jack Jennings is a professor of radiology and chief of musculoskeletal radiology for Mallinckrodt Institute of Radiology (MIR) at Washington University School of Medicine in St Louis, USA. Best known for his innovation in musculoskeletal and spine interventions, Jennings is no stranger to blending niches, combining skills gained from his experiences in interventional radiology (IR), neuroradiology, and musculoskeletal radiology for a range of tumours in the bone, spine and soft tissue.
What attracted you to a career in IR?
Since I was young, I always wanted to be a doctor and do something with my hands in medicine. I spent a lot of time in the operating room with a neurosurgeon friend of my family, so I naturally had neurosurgery as my chosen pathway. This trajectory was modified late in medical school based on the wisdom and advice of my mentors Don Hilbelink, my doctorate advisor, and Reed Murtagh (both University of South Florida, Tampa, USA) a neuroradiologist. I was introduced to radiology and IR concurrently, though a quick last-minute pivot resulted in me matching to a radiology residency.
Who were your mentors?
At MIR, I was fortunate to work under internationally respected pioneer in musculoskeletal (MSK) radiology and interventions, Louis Gilula, who sadly passed away in 2014. Lou pushed me as a resident and fellow to meet and spend time with Afshin Gangi and Matt Callstrom who both blazed the trail for MSK interventional oncology (IO). I was fortunate and able to go to Strasbourg, France at the beginning of my career and spend time with Afshin and his team. This was my introduction to advanced bone and soft tissue ablations, including the treatment of spine metastases. Matt Callstrom was very instrumental in MIR developing a bone ablation practice over 15 years ago and guided me through the process. His direction was invaluable. He helped us navigate the reimbursement and third-party payer issues in an era before there were current procedural terminology (CPT) codes for the majority of the ablation procedures we were doing. I am forever grateful for all of their guidance, mentorship, and very close friendship.
The ability to combine imaging with cancer-related treatments has been the perfect blend for my career satisfaction. IR is always developing new procedural techniques, ablation and procedural devices, imaging guidance, and ablation evaluation/ confirmation. This allows us to have a very close relationship with industry and work with research and development teams in the creation of therapeutic devices for the treatment of cancer. This relationship and the overlapping goals we share, has fostered many wonderful mentors and friends.
I have been blessed with incredible mentors at every step of this journey. Having one great mentor in your career is a blessing but to have as many as I’ve had is beyond words. Maybe it speaks of how much guidance I need i.e. too much. I have such gratitude for all of them and I would encourage early career physicians to reach out and find a mentor or two. This is the beauty of societies such as the Society of Interventional Oncology (SIO), the American Society of Spine Radiology (ASSR), the Society of Interventional Radiology (SIR) and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), as they all have programmes and mechanisms for students to early IR/IO to meet with programme/society faculty and/ or be involved with the mentor programmes. These relationships that you will develop with mentors, colleagues and being involved in societies, will give a dimension and satisfaction to your career that goes beyond the everyday grind.
Could you describe a particularly memorable case of yours?
My most memorable case was my first cryoablation case. Lou had a case involving metastatic thyroid cancer to the bone with lesions increasing in size, and he convinced myself—a fellow at the time—and Daniel Wessell, first-year faculty, to do the first bone cryoablations at MIR. Talk about pressure! We did six lesions that day, which took us nearly 12 hours (obviously very novice and very slow) and let’s just say my scrubs were drenched; however, it was the nidus for us to begin to build what is now a very robust ablation practice.
You formed a multidisciplinary metastatic spine working group (MMSWG) in 2014 that led to published recommendations for the treatment of metastatic spine disease. What are the most important factors when devising recommendations?
The MMSWG came about by the efforts of radiation oncologist Cliff Robinson (Washington University in St Louis, St Louis, USA), Bob Poser, vice president of Global Spinal Therapies at Merit Medical, and myself. This group was made up of radiation, surgical and medical oncologists and interventional radiologists from institutions from the USA and Europe. We used level-one evidence and recommendations available at the time to develop a treatment algorithm for patients with spine metastatic disease. This included an in-person, day-long roundtable discussion, presentations of the evidence and formulation of the treatment pathways for various scenarios of spine metastatic disease. To this day, we follow this algorithm and even updated it a few years ago with a follow-up manuscript as we learned that, as an institution, we were more aggressive and had promising results when operating on patients with metastatic spinal cord compression.
What is the most exciting development in the musculoskeletal interventional arena in the last five years?
MSK IR has gone from being a niche subset of IR 15 years ago with only a few people in the audience at scientific meetings—by few I mean the speakers mostly attending each other’s talks—to a rapidly advancing field with ever increasing adoption, hands-on courses all over the world, and positively affecting the lives of many cancer patients with osseous metastatic disease. Cancer patients are living much longer and many will have bone metastases. Our mission is to educate and train as many IR physicians as possible in these procedures so that they can offer them in their practice.
As previous president of the ASSR, what was your experience holding this post?
This society has been so kind to me and took me in as a young attending and really an outcast i.e. MSK radiologist in a neuroradiology society! The mentorship and career fostering by this society, including past presidents Josh Hirsch (Massachusetts General Hospital, Boston, USA), Allan Brook (Montefiore Medical Center, New York, USA), Bassem Georgey (University of California San Diego, La Jolla, USA), and Adam Flanders (Thomas Jefferson University Hospital, Philadelphia, USA) was incredible, and I am very appreciative of them. This society is unique in that it focuses on diagnostic and interventional spine treatment, and it has greatly impacted the advancement of spine procedures from adoption to reimbursement. The rebirth of its workshop has been an over-the-top success with attendees and with our industry partners. This synergy has led to its success and I am sure this will continue for many more years.
Currently, you are treasurer of the SIO. How did you become involved with the society and what does your current role entail?
SIO has really been one of the greatest highlights in my career as it has made great strides in solidifying IO as the fourth pillar of oncologic treatment of cancer patients. Very similar to ASSR, I am blessed that this group has allowed me to be involved in this journey for the advancement of IO patient care. Being on the board and executive committee has allowed me to work with the incredible team of interventional physicians including Muneeb Ahmed (Beth Israel Deaconess Medical Center, Boston, USA), Matt Callstrom (Mayo Clinic, Rochester, USA), Bill Rilling (Medical College of Wisconsin, Milwaukee, USA), Alexis Kelekis (National and Kapodistrian University of Athens, Athens, Greece), Sean Tutton (University of California San Diego, La Jolla, USA), and Michael Soulen (University of Pennsylvania Health System, Philadelphia, USA) who continue to mentor and educate me.
As this society continues to grow and as more society-sponsored trials and educational efforts go forward, the immediate and future financial stability becomes more complex and requires much accountability. Working closely with SIO staff and the finance committee, we are focusing on developing a very solid financial foundation. I have learned much throughout this process and it could not be done without the support of our SIO team led by Jena Stack.
Yours was recently the first US hospital to be accredited with the International Accreditation System for Interventional Oncology Services (IASIOS). How will this benefit your practice?
With the rapid growth, depth and breadth of IO, having a baseline accreditation such as IASIOS for quality and safety will ultimately result in greater uniformity and validity making us all better at caring for patients. I am very thankful to Andreas Adam (King’s College London, London, UK), Liz Kenny (Royal Brisbane and Women’s Hospital, Queensland, Australia) and CIRSE for all of their help with this process and their continued support. Our quality and safety office was very excited to be a part of IASIOS. The application process educated us on some deficiencies and we have already begun making modifications in our patient workflow.
What is the most exciting development in IO at present?
IO is rapidly growing in its scientific advancements and multidisciplinary adoption. The increased presence in the National Comprehensive Cancer Network (NCCN) guidelines and multidisciplinary tumour boards will allow for broader adoption and knowledge to the other oncology specialties who are not aware of what IR can offer. Likewise, the study and use of combined therapies including ablation and immunotherapy and radiation therapy will continue to advance the treatment of patients especially in those who have failed multiple lines of treatment. These collaborative efforts will surely lead to better patient care.
What is the greatest challenge facing interventional radiologists today?
The rapid growth of IO comes with a responsibility to be able to provide these services to as many individuals as possible across this world—we need growth beyond the walls of ‘ivory towers’. We will need to continue to train and educate more individuals, both residents and those already in practice, to go out and provide these services and to emphasise the importance of a multidisciplinary approach to cancer care. This is a very exciting time for IR and IO, but we must continue the education, training, and scientific pursuits to make a solid pillar in cancer treatment. We also must continue to educate our insurance companies and third-party payers of the advances that have been made and their scientific legitimacy to mitigate this being a barrier for patient treatment.
What are your hobbies and interests outside of medicine?
I have nine children (seven biologic and two step), and we are very sports-driven family— sports such as basketball, hockey, football, volleyball, and soccer. Nearly every second of my free time is filled with my family. The only exception is that I run/workout every morning. We also like to travel. My wife French so we like to go to France every summer and we travel frequently throughout Europe.
Preliminary results from the largest global liver venous deprivation (LVD) registry—EuroLVD—confirms “high” hypertrophy and kinetic growth rate and “very low” rate of post-hepatectomy liver failure (PHLF), demonstrating the “safety” of LVD over portal vein embolization (PVE) in a real-world, multicentre setting. These data were presented during a scientific session at the European Conference of Interventional Oncology (ECIO) annual meeting (28 April–1 May 2024, Palma de Mallorca, Spain).
EuroLVD is an initiative that has been set up between interventional radiology and hepatobiliary surgery groups in Lausanne to collect information about LVD. “It’s almost copy and pasting what has been done for the associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) technique,” lead investigator—and previous chairman of ECIO—Alban Denys (Centre Hospitalier Universitaire Vaudois [CHUV], Lausanne, Switzerland) told Interventional News.
ALPPS is a surgical technique that combines transection of liver parenchyma and the ligation of the portal vein to the diseased liver. It allows higher, “more efficient” degrees of hypertrophy of the future liver remnant (FLR) in a short time, Denys explained. However, studies have shown a high rate of morbidity and mortality associated with the procedure, such as the 2020 single-centre study conducted by Kosuke Kobayashi (University of Lausanne, Lausanne, Switzerland) which confirmed the superiority of liver venous deprivation (LVD) over portal vein embolization (PVE) alone, inducing faster hypotrophy of the future liver remnant.
“As more groups worldwide use this technique,” Denys said, “a more systematic exploration, including randomised controlled trials of multiple centres and registries of cases are paramount to confirm the efficiency of LVD compared to other techniques such as PVE or Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS), the latter being associated with severe morbidity and mortality.”
In total, Denys et al identified 216 patients from centres in Switzerland, France, the USA, and the UK, the majority of whom had had a previous diagnosis of colorectal cancer or chloangiocarcinoma. Concerning procedural characteristics for LVD, Denys outlined that average procedure duration was 130 minutes and noted 6.5% rate of complication, including two pleural effusions or reports of chest pains. Median FLR and standardised FLR ratios prior to LVD were 35% and 32%, respectively. Following LVD, median FLR and standardised FLR “significantly increased” to 48% and 44%, corresponding to a median kinetic growth rate of 3.4% per week. Denys also noted that the median delay between LVD and surgery was 41 days.
Hepatectomy was performed in 160 patients—85 hepatectomies, 65 extended right hepatectomies, seven extended left hepatectomies and 3 other resections. He noted that 77 (48%) of patients experienced post-operative complications and five (3%) developed postoperative liver failure.
Presenting these data at ECIO, Denys confirmed that: “EuroLVD demonstrates the safety of LVD in a large real-world multicentre setting—hypertrophy and kinetic growth rate are high and the PHLF rate is very low. It is our approach that, the more liver you leave in place, the easier it is for surgery, for recovery and the shorter the stay in the intensive care unit.”
“I think this could impact the clinical practice of centres that are still not convinced on LVD,” Denys continued. “Our main messaging is to not be afraid to start. It’s a safe procedure, it’s not very complex and it enables better outcomes from your patient, so don’t be afraid to go for it—and even participate in the EuroLVD registry if you do implement the procedure.”
“The idea of LVD is to be more efficient than PVE but less morbid and with a lower mortality than ALPPS,” said Denys. In his team’s view, striking this balance may provide a “significant benefit” in terms of hypertrophy of the left lobe of the liver when resection of the right lobe is necessary, but the left lobe is “too small”, without additional morbidity/ mortality.
“The technique has only been invented a few years ago however, so there is not much depth in the literature,” he added. Aside from Kobayashi et al’s monocentric retrospective analysis, Denys noted that there are “almost no prospective data”, which led his team to build their comprehensive registry.
“The results are quite positive,” Denys commented. He explained that his teams’ intention is to provide this initial detail and subsequently subdivide their cohort by disease groups based on liver function characteristics recorded before patients underwent LVD. In doing so, Denys and his team will seek answers to questions, such as—is the liver normal? Has the patient received chemotherapy? Is it a cholestatic liver? Is it a cirrhotic liver? In asking these questions, they aim to define how LVD works in various groups.
“Ultimately, we have confirmed the previous monocentric studies which have provided optimistic data that have informed our present registry,” Denys said. “There is already a very positive signal supporting LVD and its superiority over PVE for every single patient.”
Looking to the future, Denys noted that observing marginal indications for liver preparation techniques, such as LVD and PVE, will be “very interesting” when they are able to analyse the final data of their registry.
“When your left liver lobe volume is at its limit, what preparation technique should you decide to go with, if at all? What do you get in terms of results? If you are able to shorten hospital stay and reduce morbidity, that’s very interesting information. There’s also room for expanding the indication for liver preparation techniques to broader indication criteria, as the technique has very low morbidity and this is what we want to confirm—the more liver you leave in place after surgery, the better the patient outcome in the post-operative period.” This, he stated, may be due to faster recovery time and less complications—all endpoints that he anticipates can be achieved with LVD, or at least this is what his team are seeing “at the moment”.
Finally, Denys added that interventionists should not be “afraid” to use LVD and hopes that any centre which begins to deploy the technique may consider becoming involved in the registry. His presentation of their preliminary data at ECIO is aimed to not only provide a small glance into the significance of their long-term data, but also to publicise their registry so that they might “gather even more patients”, bolstering final conclusions to be released in the summer.
Eric J Keller and Tauqir Rana discuss a session at the Pan Arab Interventional Radiologists Society Pan Arab (PAIRS) annual congress (10–13 February, 2024, Dubai, United Arab Emirates) featured the first session on ethics in IR in the region, discussing issues such as futility, surrogate decision-making, and conflicts of interest.
The session stimulated a lively discussion and highlighted important cultural differences, which can shape these challenging issues faced in IR practice.
Futility was the first issue raised. Interventional radiologists often care for critically ill patients and can be faced with requests for procedures that offer little chance of benefit. Common examples include gastrostomy tubes in patients with severe dementia or numerous biliary drains for patients with advanced cancer and malignant biliary obstruction. Advance care planning and partnerships with palliative care can be helpful in navigating these requests. Perceptions of value, risks, and preferences vary widely, so it is important when faced with these requests to understand the patient’s and family’s goals of care and values to differentiate palliative from futile care.1
The talk then transitioned to consent and surrogate decision-making. The audience raised questions about family requesting that elderly patients not be told about their terminal diagnosis and how to facilitate informed consent when patients and family defer to whatever the doctor thinks is best in certain cultures. The modern ideal of consent has moved away from paternalism (what the doctor orders) as well as deferring solely to patient autonomy (whatever the patient/ family wants). Rather, we are challenged to facilitate shared decision making where we respect patients’ preferences and encourage their involvement in the decision-making process but also offer recommendations and guidance as content experts.2 Patients have a right to know/make decisions about their care, but they also have the right to defer to others to make decisions on their behalf, and this preference should be respected.
The audience was then asked about requiring suspension of Do Not Resuscitate (DNR) and Do Not Intubate (DNI) orders to have an IR procedure. American surgical and anaesthesia guidelines have recommended against requiring suspension for procedures, advising that code status should instead be rediscussed. Yet, a study3 of IR practices in the USA found that about a third of practices require the patient to be full code for IR procedures. Most participants agreed with required suspension, noting that their anaesthesiologists (and selves) want the ability to resuscitate their patient if something happens intraoperatively.
The final questions raised involved conflicts of interest and relationships with industry. Conflicts of interest (COIs) are a natural part of professional life and are not always financial. The issue is not necessarily to the existence of conflicting interests or relationships with industry, but the potential bias caused by these relationships. Interventional radiologists’ relationship with industry is viewed as invaluable, but the question becomes how can we effectively manage bias associated with these valuable relationships? Improving disclosure of potential bias is likely the most practical solution. For example, a recent study found 0% disclosure of relevant financial COIs among social media posts.4
The PAIRS 2024 Applied Ethics in IR session was critical in initiating these key conversations across the world of IR. We hope to continue raising important issues facing our specialty to develop practical strategies and tools to help navigate them across cultures.
References:
H D Rockwell, et al. Utilisation of Goals of Care Discussions and Palliative Care Prior to Image-Guided Procedures Near The End of Life. Clinical Radiology. 2022 Feb 14; 10.1016/j.crad.2022.01.050.
Tia Forsman, et al. Consent in Interventional Radiology—How Can We Make It Better? Canadian Association of Radiologists Journal. 2022 May 25; 10.1177/08465371221101625
Eric D Cyphers, et al. Required Suspension of Do Not Resuscitate and/or Do Not Intubate Orders in Interventional Radiology: A Survey of Prevalence and Practices. Journal of Vascular and Interventional Radiology. 2022 Dec 20; 10.1016/j.jvir.2022.12.032.
Thomas Webb, et al. The Prevalence of Financial Conflict of Interest Disclosures by Endovascular Specialists on X (Twitter). Journal of Vascular and Interventional Radiology. 2024 March 19; 10.1016/j. jvir.2024.03.017
Tauqir Rana is a consultant interventional radiologist at King Faisal Specialist Hospital, Riyadh, Saudi Arabia and Eric J Keller is a senior IR resident at Stanford Health Care, Stanford, USA.
The unique dual-lumen design creates the patented Surge Aspiration technology, a novel type of cyclic aspiration at the distal end of the catheter.
Ice aspiration system
Expanse Ice recently announced that its Ice aspiration system has received 510(k) clearance from the US Food and Drug Administration (FDA).
A press release notes that the Ice system is specifically designed to address the complex challenges associated with peripheral thrombectomies.
Eitan Konstantino, a serial entrepreneur in the vascular device field, is the driving force behind Expanse Ice. “We’ve engineered the Ice catheter system to harness the aspiration power typical of a large bore catheter, but within the slender profile of a much smaller device,” Konstantino said.
“It is clear this device was built with physicians in mind. It aims to address some of the biggest issues we see regularly. The device was designed and built with a strong understanding of foundational physics that leaves me optimistic for its success,” said Michael Lichtenberg, chief medical officer of angiology at the Vascular Center Clinic in Arnsberg, Germany.
“I am looking forward to being among the first users of the Expanse Ice system. Its ability to offer powerful clot removal in a compact size is an intriguing proposition that could significantly enhance our ability to meet patient needs more effectively and improve treatment outcomes in peripheral vascular disease,” said Aravinda Nanjundappa, director of peripheral vascular interventions at the Cleveland Clinic in Cleveland, USA.
“The thrombectomy market is witnessing robust growth and the approval of the Ice system comes at an auspicious time. It is cutting-edge technology in an underpenetrated market,” said Shlomi Nachman, former Johnson & Johnson Company group chairman of cardiovascular and specialty solutions and vision.
Abbott has announced that the US Food and Drug Administration (FDA) has approved the Esprit BTK everolimus-eluting resorbable scaffold system (Esprit BTK system), a breakthrough innovation for people with chronic limb-threatening ischemia (CLTI) below-the-knee (BTK).
The Esprit BTK System is designed to keep arteries open and deliver a drug (everolimus) to support vessel healing prior to completely dissolving.
Until today, there were no stents or drug-coated balloons approved for use below the knee in the USA. The standard of care has been balloon angioplasty, which relies on a small balloon delivered via a catheter to the blockage to compress it against the arterial wall, opening the vessel and restoring blood flow. However, blockages treated only with balloon angioplasty have poor short- and long-term results, and in many instances the vessels become blocked again, requiring additional treatment.
The Esprit BTK system is a first-of-its-kind dissolvable stent and is comprised of material similar to dissolving sutures. The device is implanted during a catheter-based minimally invasive procedure via a small incision in the leg. Once the blockage is open, the Esprit BTK scaffold helps heal the vessel and provides support for approximately three years until the vessel is strong enough to remain open on its own.
“The FDA approval of Abbott’s Esprit BTK System marks a significant milestone in our fight against peripheral artery disease below the knee and should usher in a new era of improved outcomes for people worldwide,” said Sahil A Parikh, (Columbia University Irving Medical Center, New York, USA) and one of the principal investigators of the LIFE-BTK trial. “By introducing a treatment option that is superior to balloon angioplasty, Abbott is changing the landscape of CLTI therapy.”
The LIFE-BTK trial, which evaluated Abbott’s Esprit BTK system, was presented in October 2023 as a late-breaking clinical trial at the 35th Transcatheter Cardiovascular Therapeutics (TCT) conference (23–26 October, San Francisco, USA) and simultaneously published in the New England Journal of Medicine. The results of the trial demonstrated that the Esprit BTK System reduces disease progression and helps improve medical outcomes compared to balloon angioplasty, the current standard of care.
“At Abbott, we’ve recognized the significant burden of disease and limited treatment options available for people living with the most severe form of peripheral arterial disease (PAD). That’s why we’re revolutionising treatments with resorbable scaffold technology below the knee,” said Julie Tyler, senior vice president of Abbott’s vascular business. “Our resorbable program is focused on meeting unmet needs in the peripheral anatomy to help people live better and fuller lives.”
Provisio Medical has announced US Food and Drug Administration (FDA) 510(k) clearance of the Provisio sonic lumen tomography (SLT) intravascular ultrasound (IVUS) system.
According to a press release, SLT technology addresses a critical unmet need for vascular specialists by providing automatic, real-time, accurate, numeric measurements of the flow lumen of blood vessels without the complexities of image interpretation.
Provisio Medical states that its catheter is the world’s first integrated intravascular imaging and support crossing catheter and enables vessel lumen measurement and visualisation simultaneously with guidewire support and delivery of radiopaque contrast agents.
It has been demonstrated repeatedly that the current standard-of-care of using angiographic information by itself is insufficient to accurately assess vessel size in the approximately 20 million people in the USA with peripheral vascular disease, the company notes. It goes on to say that the use of intravascular imaging has been shown to improve accuracy of vessel sizing and thereby improve clinical outcomes.
By incorporating its technology into a front-line support crossing catheter, Provisio claims to simplify the acquisition and presentation of vessel sizing data without changing the physician’s workflow, while potentially reducing the time for data acquisition, use of contrast media, and exposure to radiation.
“Clinical outcomes in peripheral vascular disease have consistently been shown to benefit from accurate intravascular measurements, yet adoption has been limited by the additional procedure time and training required to interpret images” noted S Eric Ryan, chief executive officer. “Thanks to the ease-of-use of SLT IVUS, which can be incorporated more efficiently in the peripheral vascular workflow, we believe there is the possibility of increased adoption and therefore improved outcomes for many more patients with potentially devastating peripheral vascular disease.”
The Provisio SLT IVUS system consists of the SLT IVUS P1 system and the SLT IVUS support crossing catheter. The SLT IVUS support crossing catheter is an over-the-wire IVUS catheter with an ultrasound transducer array at the distal end that also functions as a support crossing catheter. The information from the ultrasound signal is used similarly to sonar technology to measure vessel dimensions in real-time and visualise the peripheral vessel’s flow lumen.
In the UK National Institute for Health and Care Research (NIHR) Health Technology Assessment (HTA)-funded BASIL-3 randomised controlled trial (RCT), neither drug-coated balloon (DCB) angioplasty with or without bare metal stent nor drug-eluting stent (DES), when used in the femoropopliteal segment, conferred a hypothesised clinical benefit over femoropopliteal plain balloon angioplasty with or without bare metal stent.
In addition, it was found that DCB with or without bare metal stent is unlikely to be cost-effective at the UK National Health Service (NHS) National Institute for Health and Care Excellence (NICE) willing-to-pay threshold. DES, on the other hand, is potentially cost-effective at this threshold.
Andrew Bradbury (Birmingham, United Kingdom) and the BASIL-3 team of triallists shared this and other key findings on Tuesday afternoon, addressing the question of which endovascular strategy is best in the femoropopliteal segment. The investigators presented—for the very first time—the results of this long-awaited, only completed, fully publicly funded RCT in the space.
“This was a pragmatic, ‘real-world’ UK trial whose outcomes are likely to be a realistic representation of what can be reasonably achieved across the NHS,” Bradbury shared during the session.
Following an introduction to the trial from Bradbury, Lewis Meecham (Cardiff, Wales) shared evidence for paclitaxel DCB and DES in chronic limb-threatening ischaemia (CLTI) before BASIL-3; Matthew Popplewell (Birmingham, United Kingdom) put the trial into context, speaking specifically about the BASIL Prospective Cohort Study (PCS); and Gareth Bate (Birmingham, United Kingdom) and Jack Hall (Birmingham, United Kingdom) shared BASIL-3 clinical and statistical methodology, respectively.
Against this backdrop, Catherine Moakes (Birmingham, United Kingdom) reported clinical results of the BASIL-3 trial.
Between 29 January 2016 and 26 August 2021, the trial enrolled 481 patients, with 160 randomised to plain balloon angioplasty with or without bare metal stent, 161 to DCB with or without bare metal stent, and 160 to DES.
In the intention-to-treat analysis, Moakes revealed that 54 (34%) patients in the plain balloon angioplasty group met the primary endpoint of amputation-free survival (AFS), defined as the time to major (above-the-ankle) amputation of the index limb or death from any cause, compared to 64 (40%) in the DCB arm and 66 (42%) in the DES arm.
In a per-protocol analysis of only adherent participants, Moakes reported that 49/140 (35%) patients in the plain balloon angioplasty group met the AFS endpoint, compared to 48/122 (39%) in the DCB group and 47/118 (40%) in the DES group.
The research group also shared health economic outcomes. In a cost-utility analysis, Jesse Kigozi (Birmingham, United Kingdom) outlined that DCB angioplasty with or without bare metal stent when compared to plain balloon angioplasty with or without bare metal stent was less costly by £-250.71 and less effective by -0.007 quality-adjusted life years (QALYs).
Kigozi then shared health economic results comparing the DES group versus plain balloon angioplasty. In the cost-utility analysis, the differences observed in the costs and outcomes between DES and plain balloon angioplasty with or without bare metal stent[1]first strategies were minimal, he reported.
However, Kigozi added that DES was the dominant strategy because, when compared to plain balloon angioplasty with or without bare metal stent, DES was less costly by £-724 and resulted in additional 0.048 QALY.
Kigozi summarised that there were minimal incremental differences in costs and outcomes in terms of QALYs out to two years and amputation-free life years out to seven years when the DCB with or without bare metal stent or the DES-first revascularisation strategies were compared to the plain balloon angioplasty with or without bare metal stent-first strategy in the cost-utility and cost-effectiveness analysis.
Kigozi said that, while there is uncertainty overall, the results show DCB is unlikely to be cost-effective when compared to plain balloon angioplasty, while DES is potentially cost-effective when compared to plain balloon angioplasty. He added that these findings were generally consistent over different scenarios and analyses and across different patient subgroups.
Finally, Bradbury summed up the main findings and underscored limitations, take-home messages, and further research.
He stressed that the trial’s power exceeds 90%, with more than the 291 required primary outcomes observed. Bradbury added that follow-up was long and better than anticipated, with only seven patients withdrawing prior to the primary endpoint. Cause of death was available for all deceased patients, he continued, adding also that most (35) UK vascular units randomised patients.
Bradbury also outlined some potential limitations of the trial, highlighting among these the effects of the “Katsanos pause”— referring to the fallout from the controversial 2018 meta-analysis on paclitaxel-coated devices—and the effects of COVID-19.
Discussion following the presentations included examination of the choice of AFS as the primary endpoint.
William Gray (Philadelphia, United States) asked, for example, why AFS was chosen versus another endpoint like major amputation “given the dominance of death” in this patient population.
Bradbury responded that there was a lot of support in the UK for AFS. “I’m not saying it’s the only endpoint, but it’s the one that we’ve chosen, and it runs through all three BASIL trials rightly or wrongly,” he said. “In BASIL-1 and BASIL-2, we have actually found that the biggest difference between the two groups is mortality and not amputation rate.”
Michael Conte (San Francisco, United States) added that there have now been three BASIL trials, but not one has shown a difference in limb outcomes. “While I recognise that AFS is a critical endpoint, I think the way in which you’ve powered it doesn’t take into account that death is a noise and the outcome in the limb is what you’re actually looking to differentiate.”
CX co-chair Andrew Holden (Auckland, New Zealand), who co-moderated the session, asked Bradbury what should be taken away from these trial results in 2024. “We would like to have had a more clear-cut result,” he admitted. “Maybe over the next few days, weeks, months, as we digest it, as the publications come out and as we present more data, people will begin to think about what it means for their practice, in their country, in their healthcare system.”
L to r: Robert Shahverdyan, Matteo Tozzi, Robert Jones, Leonardo Harduin, Andrew Holden and Ellen Dillavou
A first-time presentation of five-year data from the IN.PACT AV Access study evaluating the IN.PACT AV (Medtronic) drug-coated balloon (DCB) today led principal investigator and CX co-chair Andrew Holden (Auckland, New Zealand) to conclude that “we know which DCB to use” now. However, discussions during the morning’s Vascular Access Masterclass did raise several other questions that are yet to be answered conclusively.
With IN.PACT AV Access having demonstrated superior outcomes at three years with the IN.PACT AV DCB versus plain balloon angioplasty for dialysis access—as per a presentation from Holden at last year’s CX Symposium—the speaker initially noted that it is currently the only randomised pivotal study to have produced “consistent and sustained clinical benefit” with an arteriovenous fistula (AVF) treatment device at such a long-term follow-up.
According to Holden, 98 patients—57 in the DCB group and 41 in the standard percutaneous transluminal angioplasty (PTA) group—had follow-up data available at five years. He reported an all-cause mortality rate (post vital status update) of 41% and 46.5%, respectively, across these two groups, describing these figures as “comparable”. Holden highlighted the fact that both of these figures are significantly lower than a 60.4% five-year mortality rate among US haemodialysis patients derived from the United States Renal Data System (USRDS).
“Durable, long-term data suggest the use of IN.PACT AV DCB as a standard of care for AVF maintenance in patients with ESKD [end-stage kidney disease],” Holden concluded, also remarking that “we now know which DCB to use”, and reporting that the device is enabling prolonged time to reintervention in dialysis access patients.
These findings may—in Holden’s view, at least—have drawn a line under debates over the optimal DCB in dialysis intervention, but further discussions throughout the Vascular Access Masterclass revealed several other areas yet to be fully addressed. The first of two controversies tackled within the session alluded to the fact that, despite recommendations in the 2019 update to the Kidney Disease Outcomes Quality Initiative (KDOQI) Clinical Practice Guideline for Vascular Access, ‘we don’t know what the right access, at the right time, for the right patient, is’.
Presentations here saw Maarten Snoeijs (Maastricht, Netherlands) assert that “access registries are not adequate, currently”; Karen Stevenson (Glasgow, United Kingdom) highlight the need for ‘minimally disruptive vascular access’ owing to the immense burden experienced by dialysis patients; and David Kingsmore (Glasgow, United Kingdom) advocate arteriovenous grafts (AVGs) over AVFs, drawing dissent from Robert Shahverdyan (Hamburg, Germany). A somewhat more positive outlook was conveyed via a presentation from Koen van der Bogt (Leiden, Netherlands), who updated delegates on progress towards developing a ‘dynamic AVF’ that is able to normalise flow rates between dialysis sessions, thus reducing patients’ cardiac burden. While this project remains in its infancy, CX Executive Board member Nicholas Inston (Birmingham, United Kingdom) described the concept as “really innovative and futuristic”.
Following this, speakers debated a highly contentious notion: ‘endoAVFs are a failed experiment’. Tobias Steinke (Dusseldorf, Germany) and Shannon Thomas (Sydney, Australia) delivered arguments favouring this statement, with the former emphasising that device-created fistulas have demonstrated some success in specialised centres but these results are unlikely to be replicable in the ‘real world’, and the latter positing that better surgical fistulas—not endoAVFs—hold the key to truly solving existing vascular access challenges.
Meanwhile, Shahverdyan and Monnie Wasse (Chicago, United States) were in opposition to these viewpoints, with both primarily focusing their arguments on positive data produced on the Ellipsys (Medtronic) and WavelinQ (BD) systems. Shahverdyan also noted that endoAVFs are “a complementary addition, not a replacement” for surgical fistulas. Wasse pointed to the high technical success rates observed with endoAVFs, also averring that they are already part of the current standard of care and should now be incorporated into clinical guidelines.
Both sides garnered considerable support, but pro-endoAVF arguments accrued marginally more support, with an audience poll revealing that 54% of those in attendance disagreed with the suggestion that endovascular fistulas are a ‘failed experiment’. CX Executive Board member Kate Steiner (Stevenage, United Kingdom) weighed in on these discussions, noting that “it would be impossible to take [endoAVFs] away now”—especially given the number of patients she sees who would not be able to receive a fistula if only surgical options were available. Inston dubbed the session and voting result as “fascinating”, predicting that such debates are likely to rage on for several years.
Penumbra has announced the US Food and Drug Administration (FDA) clearance and launch of Lightning Flash2, the next generation computer assisted vacuum thrombectomy (CAVT) system to remove venous thrombus and treat pulmonary embolism (PE), a press release states.
Lightning Flash 2 features advanced Lightning Flash algorithms, designed for increased speed and sensitivity to thrombus and blood flow. These new features combined with Penumbra’s novel catheter technology allow physicians to better navigate the body’s complex anatomy and deliver high power for clot removal with possible minimal blood loss.
“Based on what we’ve seen in the initial launch, Lightning Flash 2 has significantly improved procedure time by shortening the aspiration time. It has also shown reductions in blood removed during aspiration. These advantages can improve patient safety, provide better outcomes for the patients, and streamline efficiency for physicians treating the patients,” said James F Benenati, chief medical officer at Penumbra. “As adoption of thrombectomy becomes more widespread, Lightning Flash 2 will provide physicians with the confidence that CAVT is a valuable frontline option.”
With streamlined audio-visual feedback, Lightning Flash 2 enables physicians to have a better understanding of what is occurring at the tip of the catheter during a procedure, the press release details. This enhanced feedback loop results in a more intuitive thrombus removal experience for the physician.
“Lightning Flash 2 now combines an optimally sized catheter with the latest algorithm technology designed to more efficiently remove blood clots while maintaining a high level of safety,” said Adam Elsesser, president and chief executive officer of Penumbra. “Our ongoing innovation around CAVT underscores our commitment to advancing patient care so that more patients suffering from these complicated conditions can benefit from this advanced therapy.”
Lightning Flash 2 is part of Penumbra’s Indigo system with Lightning portfolio. The company’s Lightning products are the only computer assisted mechanical thrombectomy systems currently available in the US and early clinical data has demonstrated improvement in patient clinical outcomes and quality of life.
“Unfortunately, we are doing worse for our patients today,” were the sobering thoughts of Eric Secemsky (Beth Israel Deaconess Medical Center, Boston, USA) during a late-breaking presentation at the Charing Cross (CX) Symposium 2024 (23–25 April, London, UK). Among several presentations on paclitaxel safety, he reported that: yes, the meta-analysis and regulatory body restrictions on paclitaxel-coated devices did cause harm through the relegation of patients to the “less durable” conventional device treatment, increasing the incidence of adverse events post-revascularisation.
In a session focused on reaching resolution on the paclitaxel controversy, early presentations given by Thomas Zeller (Bad Krozingen, Germany) and Peter Schneider (San Francisco, United States)—concerning paclitaxel-coated balloon safety in femoropopliteal occlusive disease and paclitaxel mortality across randomised controlled trials—established the “lack” of paclitaxel-coated device mortality risk in the most recent available data.
Secemsky, who presented next, gave a brief timeline of the rise and fall of paclitaxel-coated devices showing their sharp decline in use following the Konstantinos Katsanos (Patras, Greece) et al meta-analysis which reported an increased mortality risk, and the subsequent regulatory restrictions. Previously, paclitaxel devices—driven by drug-coated balloons (DCB)—were the preferred treatment for femoropopliteal intervention for peripheral arterial disease (PAD) in the United States.
Using both Medicare data and the IQVIA: Medical Device Supply Audit database, Secemsky and colleagues looked at paclitaxel device use in US hospitals between Q3 2013 and Q3 2023. He reported that, following the pivotal Katsanos et al meta-analysis, DCB and drug-eluting stent (DES) use did not recover to pre-meta-analysis levels until Q3 2023—a period of four and a half years—showing the close “parallel” trajectory between device use and emerging data, Secemsky said. The speaker also highlighted the “shrunken” downward trend in the overall femoropopliteal procedural counts in the US following the controversy, despite PAD-related amputations remaining “stable” in the same period.
Then, Secemsky and colleagues followed 275,009 Medicare beneficiaries who underwent femoropopliteal intervention, comparing the risk of major amputation and death in the period prior to and following the paclitaxel controversy. Risk of amputation or death was reported in 40.4% and 43.2% of patients in the pre- and post-paclitaxel period, respectively. Secemsky also reported a 43.9% risk of major amputation and death in the post-COVID-19 period, establishing that risks following femoropopliteal intervention were “not driven by COVID-19 alone”, he said.
“Global restrictions on paclitaxel device use relegated thousands of patients to conventional device treatment,” said Secemsky. “The use of a less durable treatment increases the possibility of more frequent repeat interventions, the associated risks of re-intervention and the economic burden of performing these procedures.”
Although the meta-analysis and regulatory body restrictions on paclitaxel devices caused harm, Secemsky—flipping the coin—stated that it “also did good” by reiterating the need for better clinical trial practices and complete study participant follow up.
“The paclitaxel controversy not only instigated interest in non-paclitaxel therapies such as sirolimus-based treatments, but it also demonstrated that the vascular community could quickly band together to address a dispute, and particularly displayed the collaborative nature of US Food and Drug Administration (FDA) who ensured regulatory concerns were addressed,” Secemsky finalised. “These lessons can help guide the vascular community through the next controversy and to further develop evidence to shape clinical practice.”
The discussion was then opened to the FDA and UK Medicines and Healthcare products Regulatory Agency (MHRA) to provide a conclusive perspective on the matter. Representing the FDA, Ariel Ash-Shakoor (Washington, United States) began by tracing the course of the regulatory bodies’ communication to present day. Ash-Shakoor stated that, based on the “totality of available evidence” the FDA has determined that the data do not support an excess mortality risk for paclitaxel-coated devices. However, current FDA guidance when using paclitaxel-coated devices includes, but is not limited to, routine monitoring and optimal medical therapy.
Ash-Shakoor noted that lessons can be learned from the paclitaxel mortality controversy, including the importance of long-term follow up, pre-specified plans concerning missing data, and proactive patient monitoring to ensure “complete” reporting.
Providing the perspective of the MHRA, Alexander McLaren (London, United Kingdom) confirmed that no increased risk in mortality with paclitaxel-coated devices has been observed in their review of available randomised controlled trial data.
“Looking back with a critical eye to our own management of the long-running complex topic, I do feel the MHRA response was swift and decisive with the establishment and advice that we received by the expert advisory group,” McLaren stated. In his view, as “quality, robust data were slow to emerge”, delays in decision-making were inevitable. However, taking what has been learnt forward, McLaren said that the MHRA intends on improving pre-market clinical investigation and ensuring studies are “sufficiently powered and supported” to collect real-world follow-up data.
Showcasing cutting-edge applications of robotics in interventional radiology (IR), presenters at the Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA) delivered results from a range of pioneering studies.
First to the podium was Christopher Bailey (Johns Hopkins University School of Medicine, Baltimore, USA) whose team demonstrated “breakthrough capabilities” in fabricating soft robotic microcatheters capable of steering and navigating through “small, complex, tortuous and/or delicate” vasculature.
Bailey and his team went about creating a strategy for fabricating microfluidic multilumen tubing to serve as the microcatheter tubing, employing two-photon direct laser writing (DLW) for three-dimensional (3D) printing of soft microrobotic actuators with submicron-scale resolutions.
Subsequently, they produced multilumen tubing with an outer diameter of roughly 2.1Fr and inner microfluidic channels enabling actuation of 0.21Fr in diameter. The 3D microprinted soft robotic unidirectional microcatheter tip is fluidically sealed to a microfluidic chip and is capable of achieving deflection angles of greater than 115 degrees and burst pressures larger than 600kPa, Bailey explained.
Transarterial interventions are routine in IR, the speaker noted; however, in geometrically complex anatomy, interventionists can face an inability to effectively manoeuvre microcatheters/guidewires, causing a “substantial everyday challenge”.
“By uniting these strategies,” Bailey said, “a new class of microcatheter can be created that overcomes manoeuvrability deficits, which can cause unsuccessful catheterisation” and can minimise risk of complications in arterial interventions.
Bailey indicated that their microcatheter shows the “unique additive micromanufacturing techniques” that can serve as the “basis for future multidirectional designs and innovations”. Ultimately, their team hope to expand catheter-based procedures and improve procedural success rates.
“High technical success” with robotic percutaneous bone biopsy
Next, Agnieszka Witkowska (Rhode Island Medical Imaging, Providence, USA) presented high technical success and diagnostic yield, with reduced complications, for percutaneous computed tomography-guided bone biopsy using a patient-mounted robot.
Witkowska explained that their study sought to evaluate the feasibility of a robotic system with steering capabilities in patients with cancer. Including 40 consecutive biopsies in 39 outpatients, their retrospective observational study looked at biopsies that were performed in the pelvis, spine, ribs, shoulder, femur, and sternum. The median size of lesions was 26mm and lesion characteristics biopsied included 14 lytic (35%), 16 mixed (40%), and 10 sclerotic (25%). Witkowska outlined that, for mixed and sclerotic lesions, needles were manually exchanged over a Kirschner wire prior to drilling for lesion access.
Delivering their results, Witkowska stated that they achieved 100% technical success, with a mean trajectory length of 55.5mm. She noted that intermediary checkpoints were utilised in eight biopsies, but overall, procedure time was kept “low”.
Demonstrating this, she detailed that median time to needle insertion from skin to target was 19 seconds, time from first to final scan was 21 minutes, procedure time was 30 minutes and dose length product and effective dose were 536.6mGycm and 7.1 millisievert, respectively. Continuing, she noted that the diagnostic yield was 72.5% for cancer in this cohort.
The EMBOLIZE trial, a prospective, randomised controlled trial—the first of its kind—was recently launched at the Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA), and seeks to investigate the effects of ovarian vein embolization (OVE) and pelvic vein embolization in reducing symptoms in women experiencing chronic pelvic pain due to pelvic venous disease (PeVD).
The trial is a multisociety collaboration between SIR Foundation and The VIVA Foundation, in partnership with Penumbra, and will be led by Ronald S Winokur (Weill Cornell Medicine, New York, USA) and Gloria Salazar (The University of North Carolina, Chapel Hill, USA).
PeVD occurs when enlarged veins develop in the pelvis surrounding the uterus or ovaries, which can lead to severe chronic pelvic pain. Speaking to Interventional News, SIR Foundation chair and member of The VIVA Foundation board of directors Maureen P Kohi (The University of North Carolina, Chapel Hill, USA) referenced a call to action from the World Health Organization (WHO), which looked at global data citing pelvic pain as a central manifestation of the disease in women.
Maureen Kohi
“The main treatment that we’ve been offering is OVE, and we know that the data show a substantial improvement in chronic pain, but we’ve not been able to produce high-quality evidence to support that treatment option. Not only for the scientific community but also to our payers. Many women do not have insurance coverage for this procedure,” said Kohi. In women, these veins can be difficult to see and feel, Neil Mansho Khilnani (Weill Cornell Medicine, New York, USA)—a member of the EMBOLIZE steering committee—explained, which has driven “scepticism” over diagnosing and treating the pain. “The payers also hear this scepticism and jump on that as an opportunity to reduce expenses to their budget.”
The study investigators are seeking women over the age of 18 who have dilated uterine, ovarian or pelvic veins that are causing chronic pain. To determine efficacy, the study will compare changes in the patients’ pain scores on a visual analogue scale from four weeks before treatment through six months post-treatment to evaluate the outcome of vein-directed intervention for venous-origin chronic pelvic pain. Investigators will also evaluate other quality-of-life improvements, improvements in the pelvic vein varices, and changes in pain medication usage.
Neil M Khilnani
“Pain is a tricky thing to quantify as there are many variables,” commented Khilnani. “The impact of pain is more important because pain doesn’t just cause pain, it interferes with your life, how many days you’re with your spouse, missing work or how much you are able to do things in your life that are important to you.” To ensure the quality of patient-reported outcomes, the investigators will conduct cognitive interviews to get an accurate “picture” of how pain is affecting the patient.
Gloria Salazar
Salazar is confident that due to the large size of the centres from which the investigators will draw participants, enrolment should begin quickly. “Referral will not be a problem. A problem will be selecting appropriate patients for this study. We have evidence for the role of venous compression in this patient population and so we have specific criteria in terms of evaluating the ovarian minimalisation outcomes,” she said.
The investigators added that, in the setting of challenges in gaining reimbursement for this procedure, the EMBOLIZE trial is actively encouraging providers to refer potential participants who they cannot treat. “It’s in our best interest to broaden the conversation to touch patients who might be looking for treatment as both arms of the study are fully funded,” Khilnani stated, explaining that participants in the untreated arm will eventually receive treatment after six months.
The multi-society partnership with Penumbra is hoped to expand the reach of the trial to give many women in pain the opportunity to participate. “Patients with pelvic venous disease have few treatment options available to them,” said James F Benenati, chief medical officer at Penumbra. “Dedicated to advancing innovative therapies that address a significant unmet need, Penumbra’s support of this study will help provide clear evidence of the benefits of OVE and pelvic vein embolization to help patients worldwide.”
“These will be important, salutary lessons. Should a controversy arise again involving a proven efficacious therapy, we now know that stopping access to that therapy may result in unwanted and unexpected negative effects on patient care.” These are the preluding thoughts of Andrew Holden (Auckland City Hospital; University of Auckland, Auckland, New Zealand)—one of the Charing Cross (CX) Symposium 2024 (23–25 April, London, UK) co-chairs—ahead of this year’s meeting, referencing the paclitaxel mortality controversy. Here, Holden sets sights on the unmissable peripheral arterial programme, which will tackle global controversies and host heated debates.
“The peripheral arterial programme is jam-packed with controversy this year— controversy being the theme for CX 2024,” says Holden, highlighting this fact by noting that the first session will address paclitaxel mortality. The paclitaxel mortality controversy in peripheral arterial disease (PAD) will be punctuated by a late-breaking presentation from Eric Secemsky (Beth Israel Deaconess Medical Center, Boston, USA), who plans to examine whether the meta-analysis and subsequent regulatory body restrictions on paclitaxel caused harm.
“Although the original paclitaxel mortality controversy did not make sense in terms of causation theories, it was appropriate to take this report very seriously. However, in many geographies this resulted in stopping a therapy that had been shown to be more effective and durable than our non-drug-coated strategies,” details Holden. “An important question that hasn’t been addressed to date is when depriving patients of a more effective treatment modality, were we causing patients harm? With the benefit of hindsight, can we learn important lessons regarding this?”
“Hopefully we will provide the final chapter of this controversy. We have key opinion leaders presenting new data, and some input from regulators such as the US Food and Drug Administration (FDA) and the UK Medicines and Healthcare products Regulatory Agency (MHRA),” Holden says. “I’m very grateful to Eric and his group for providing additional data to allow us, for the first time, to dive into this issue.”
Holden notes that during this session, speakers and audience members will have the opportunity to ask the regulators what their thoughts are with regard to the removal of access to paclitaxel-coated devices and the duration of time it has taken to have these therapies reinstated.
“When depriving patients of a more effective treatment modality, were we causing patients harm?”
Paclitaxel-coated devices also feature in later sessions, Holden contributes, commenting that the ‘Paclitaxel and sirolimus-coated balloons in the femoropopliteal arteries’ session will end with a debate, which asks if “following the FDA announcement, do paclitaxel-coated devices now beat limus-coated devices”. He adds that drug-coated technologies will be of “great interest” at this year’s CX Symposium and will provide delegates with the opportunity to share their thoughts and experiences.
“Promising” future for bioresorbable scaffolds in the tibial arteries
Later in the peripheral programme, speakers will turn to bioresorbable scaffolds in the tibial arteries. Brian DeRubertis (Weill Cornell Medicine, New York, USA) will present late-breaking data in the LIFE-BTK clinical trial evaluating the safety and efficacy of the everolimus-eluting Esprit below-the-knee (BTK) system (Abbott) in chronic limb-threatening ischaemia (CLTI) patients with infrapopliteal artery disease.
“Bioresorbable scaffolds have been the holy grail for lower limb arterial interventions for many years,” Holden details. He draws attention to the high percentage of cases that require a scaffold due to issues such as dissection and recoil after angioplasty, but also the long-term negative effects of metal stents when placed in the tibial arteries.
“We’ve looked for a bioresorbable scaffold that works in the acute phase, but then dissolves with time and allows arterial structure and physiology to be restored. Many trials have failed both above and below the knee,” he says. However, following the LIFE-BTK trial results in 2023, which showed a statistically significant benefit for primary bioresorbable scaffolds, Holden believes this year’s CX is positioned well for a “timely deep dive” into the subject and “promising” emergent technologies.
Inaugural Roger M Greenhalgh late-breaking trials session
On both Tuesday 23 and Wednesday 24 April at CX 2024 the inaugural Roger M Greenhalgh late-breaking trials sessions will take place. “I believe Professor Greenhalgh would be very proud of the late-breaking trial sessions we are hosting in the peripheral arterial space at CX 2024,” says Holden.
At a glance, he highlights that deep venous arterialisation is a topic of “growing interest” that will feature in this session. He states the session will provide an opportunity for attendees to evaluate where this new technology may sit within physicians’ current armamentarium, particularly in patients with advanced CLTI. New data from the CLARITY trial will be presented by Anahita Dua (Massachusetts General Hospital, Boston, USA), evaluating transcatheter arterialisation of deep veins for no-option CLTI.
Holden also places focus on the six-month SHOCC study data, which will be presented by Athanasios Saratzis (University of Leicester, Leicester, UK). The trial analysed the Shockwave lithotripsy device (Shockwave Medical) for patients with PAD and will produce new data during Wednesday’s Roger M Greenhalgh late-breaking trials session. This data, Holden shares, will shed light on the device’s “effectiveness” at the trial’s UK centre.
CLTI and imaging modalities
Elsewhere in the peripheral programme, Holden highlights the comprehensive coverage of CLTI trials—including updates from BEST-CLI and the BASIL-3 podium first—and points toward the imaging modalities session.
“One of the big challenges with imaging and CLTI is trying to identify the patients who are going to respond to revascularisation. We know that CLTI patients often have a multifactorial cause for their disease in addition to their macrovascular arterial disease. In many cases, we can spend a lot of time revascularising patients who don’t benefit so we need to get a better idea of favourable responders,” says Holden.
Holden restates the importance of pre-procedural and intra-procedural imaging, which will be explored during this session, enabling physicians to get to grips with new technologies to assist in measuring when a therapeutic endpoint has been reached during a revascularisation procedure”.
“Imaging and CLTI is an expanding and very important topic that we’re going to certainly delve into on the Thursday [25 April] of CX 2024,” he adds.
Great debates in the peripheral arterial programme
The CX 2024 peripheral programme will also play host to a variety of controversial debates including paclitaxel versus limus-coated devices, and bypass versus endovascular surgery, affording CX delegates the opportunity to cast their votes. Aptly devised, the debates in the peripheral arterial programme are centred on controversial topics and are hoped to spark lively discussion. To this end, Holden believes that they will “drive consensus and effectively further the conversation” surrounding these complex treatment modalities.
FastWave Medical has announced the issuance of its fourth utility patent by the United States Patent and Trademark Office (USPTO) for its laser-intravascular lithotripsy (IVL) platform.
William Nicholson (Emory Healthcare, Atlanta, USA), one of FastWave Medical’s physician advisors, expressed his excitement about the potential for the company’s laser-IVL system, stating: “FastWave’s novel approach has enormous potential to leapfrog today’s IVL technology with durable, fast, and consistent laser energy. It also enables FastWave’s team of engineers to develop an ultra-sleek balloon catheter, overcoming the challenges of existing IVL options in reaching and crossing diseased vessels.”
Millions of people worldwide have occlusive arterial disease that is further complicated by the presence of calcium, leading to increased morbidity and mortality.
FastWave’s differentiated laser-IVL system aims to address hurdles associated with treating calcified arteries. Through its advanced lithotripsy technology, FastWave aims to solve the gaps with current IVL solutions while improving ease of use and patient safety by reducing procedural complications.
“It’s a very exciting time for FastWave and the field of IVL to further enable physicians to optimise procedural outcomes for their patients,” said co-founder and CEO of FastWave Medical, Scott Nelson. “Our growing IP portfolio is a key asset and catalyst to advance IVL technology with novel energy sources and design elements that can expand its use for more patients. I am excited and proud of the FastWave team for their dedication to power innovation that enhances clinical outcomes.”
Top stories from this year’s Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA)
Interview with Dimitrios Filippiadis (National and Kapodistrian University of
Athens, Athens, Greece) on adult pain palliation in cancer care
A first look at global liver venous deprivation (LVD) registry data to be presented at the upcoming European Conference of Interventional Oncology (ECIO) annual congress (28 April–1 May 2024)
Top stories from this year’s Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA)
Interview with Dimitrios Filippiadis (National and Kapodistrian University of
Athens, Athens, Greece) on adult pain palliation in cancer care
A first look at global liver venous deprivation (LVD) registry data to be presented at the upcoming European Conference of Interventional Oncology (ECIO) annual congress (28 April–1 May 2024)
This year’s Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA) gave recognition to select abstracts during the closing plenary session. Introduced by SIR 2024 programme chair Bulent Arslan (Rush University, Chicago, USA), who commended the “strong” and “compelling” presentations, speakers offered data which challenge preconceptions about disease states and treatment strategies.
Abin Sajan
Abin Sajan (Columbia Irving Medical Center, New York, USA), presenting first, relayed the team’s evaluation of the long-term efficacy of haemorrhoid artery embolization (HAE) in patients with symptomatic haemorrhoids.
Providing initial background, Sajan noted that haemorrhoid disease affects between 5–10% of the general population and is the third most common outpatient gastrointestinal diagnosis. Current treatment options, he outlined, range from least to most invasive, including lifestyle modifications, office-based procedures such as rubber-band ligation, and lastly surgical haemorrhoidectomy. Sajan explained however that office-based procedures currently have recurrence rates as high as 40–50%.
With intent to confirm the effectiveness of HAE, Sajan then described his team’s retrospective, single-centre study of 221 patients—“the largest sample size to date”, the speaker noted. All patients had symptomatic internal haemorrhoids and were observed over the course of two years between August 2021 and April 2023. Their cohort, comprised of 115 males and 106 females, had an average age of 57.1 years and an average haemorrhoid grade (HG) of 2.1. Patient symptoms ranged from less than five years to more than 20 years, which truly “shows the disease burden of this population”, Sajan said.
After undergoing embolization of the abnormal vascular blush at the haemorrhoidal cushion, patients were evaluated at baseline, 1–, 3–, and 6–12 months for haemorrhoid-related pain (HRP), haemorrhoidal symptoms score (HSS), quality of life (QoL), French bleeding score (FBS), and HG.
Here, Sajan detailed their results, stating that for “every single outcome measure was significant across every single timepoint”. Technical success was achieved in 100% of cases and a 90% clinical success was also reported, with 21 patients requiring repeat embolization. 19 out of the 21 patients had a middle-rectal artery supply which was embolized.
“Haemorrhoidal artery embolization is an effective and durable treatment option for haemorrhagic disease with a very low risk profile,” he summarised. “Next steps will include a comparison to standard treatments such as rubber-band ligation.” Finally, Sajan asserted that the current evidence is sufficient to place HAE within the treatment algorithm for symptomatic haemorrhoid treatment.
Novel ex vivo human liver for microwave ablation research
Carlos B Ortiz
Following Sajan, Carlos B Ortiz (University of Texas Health Centre at San Antonio, San Antonio, USA) discussed the novel creation of dual-perfused ex-vivo human liver models for the investigation of microwave ablation (MWA).
In collaboration with local transplant surgeons and the Texas Organ Sharing Alliance (TOSA), Ortiz and his team gained research consent and received human research livers from deceased organ donors using standard surgical and transplant preservation techniques. He described that a fluoroscopic compatible ex vivo dual arterial and portal perfusion system was used to perfuse and oxygenate the organ. MWA was performed using a 2.45GHz system (Angiodynamics) at 140 Watts for six minutes followed by placement of a spinal needle to mark the trajectory of the probe. MWA zones were segmented along the MWA trajectory to obtain maximal short axis diameter (SAD) and long axis diameter (LAD) measurements. Ellipsoid volume and sphericity were then calculated.
Receiving a total of 12 livers, seven underwent “successful” perfusion and MWA procedures, with an average cold ischaemic time of 76.8 hours. Continuous bile production was observed in five perfused livers, including the two cirrhotic livers, while average oxygen consumption was 11.4 + 8.3mL/ min. No bile production was noted in livers with >60 hours cold ischaemic time. Comparing perfused and non-perfused MWA, Ortiz expanded that perfused resulted in significantly smaller MWA dimensions than nonperfused ablations, with a difference of approximately 28%. Additionally, in a sub-analysis, the speaker described a “statistically significant increase” in perfused MWA zones in livers with steatosis compared to those with cirrhosis.
“We report the successful creation of a dual-perfused human liver model,” Ortiz continued, “this model can produce the heat-sink effect and enable the study of different tissue types.”
Breast cancer recurrence after cryoablation
Jolie Jean
Jolie Jean (Weill Cornell Department of Radiology, New York, USA) was next to present, addressing breast cancer recurrence after cryoablation. Giving brief context, Jean outlined that the National Comprehensive Cancer Network (NCCN) in the USA set guidelines in which surgery is the “cornerstone for locoregional control” of breast cancer. “Presenting a unique challenge,” she said, “are women who are poor surgical candidates or who refuse surgery.”
Breast cryoablation has been studied in recent clinical trials which have demonstrated its effectiveness in low-risk cancers less than 1.5cm, Jean said. Due to a “paucity” in literature, Jean’s team set out to evaluate breast cancer recurrence after cryoablation in a broader range of cancer subtypes a and sizes, who were poor surgical candidates or refused surgery.
Their single institution retrospective study included 60 patients with an average age of 75. Of these patients, 48 had invasive ductal carcinoma (IDC), five with invasive lobular carcinoma, and seven who had other histology. Tumour size ranged from (0.3-9cm), with average size of 2.5cm±1.8cm. Jean stated that a multi-probe approach was taken for tumours greater than 1.4cm with a series of freeze-thaw cycles to achieve a 1cm margin.
“All procedures were well tolerated,” Jean described for attendees, noting that “minimal or no” sedation was used based on patient preference. Following the procedure, patients were imaged using mammography and ultrasound, which at a median follow-up of 16 months, showed a recurrence rate of 10% (six patients).
Patients with poorly differentiated disease had higher risk of recurrence, while invasive lobular carcinoma status, oestrogen/progesterone receptor status and triple-negative breast cancer (TNBC) status did not contribute to the risk. Jean added that tumour size did not differ between recurrence and nonrecurrence groups.
“To date, this is the largest single-institution retrospective experience describing recurrence rates after cryoablation of primary breast cancer. Our study demonstrates that cryoablation can be performed effectively in patients with large tumours using a multi-probe approach,” Jean summarised, adding that they hope this research and prior studies will “pave the way” for US Food and Drug Administration approval and insurance reimbursement.
Radiofrequency ablation for intrahepatic cholangiocarcinoma
Qian Yu
Qian Yu (University of Chicago, Chicago, USA) was next to the podium, describing a 20-year analysis of radiofrequency ablation for intrahepatic cholangiocarcinoma (iCCA). In this “rare but very aggressive” indication, Yu began, the majority of tumours are not resectable at the time of diagnosis, and following resection, recurrence can be high.
Data on this topic are “sparse”, thereby, through using the Surveillance, Epidemiology, and End Results (SEER) database from 2000–2020, the researchers extracted data from approximately 27% of the US population diagnosed with cancer, evaluating trends in survival among iCCA patients undergoing thermal ablation. For a total of 192 patients, the median overall survival (OS) in these data was 28 months, with one, three, and five-year OS of 79.3%, 35.8%, and 19.8%, respectively. Looking closely at the data, Yu noted that patient survival increased after 2010, and that “as expected”, tumour burden correlated with survival.
“The survival curve of local disease appears better than extrahepatic disease,” Yu said, with tumours of less than 3cm demonstrating better survival than larger tumours. For patients with tumours of less than 3cm, survival was reported as an “impressive” 49 months, Yu detailed. “This tells us that ablation can be effective in carefully selected patients.” Yet, there is still a need for high-level evidence, Yu stated, drawing attention to the size of their cohort despite the 20-year time range. “It is beyond a single-centre’s ability to gather a homogenous, yet large enough sample size—future institutional collaboration is key for this research to move forward,” Yu finalised.
Cerenovus, part of Johnson & Johnson MedTech, has today announced the launch of Cereglide 71 aspiration catheter in Europe, an aspiration catheter equipped with TruCourse technology, indicated for the revascularisation of patients suffering from acute ischemic stroke.
Cereglide 71 aspiration catheter is the latest innovation in a planned Cereglide family of catheters to join the Cerenovus stroke solutions portfolio. Cereglide 71 is optimised for effective, direct aspiration of blood clots and for the delivery of compatible stent retrievers, including the EMBOTRAP III revascularisation device and Cerenovus NIMBUS geometric clot extractor, into the neurovasculature.
“The Cereglide 71 aspiration catheter using TruCourse technology represents a great advancement in acute ischaemic stroke treatment,” said Mark Dickinson, worldwide president, Cerenovus. “It provides physicians with a greater level of flexibility while offering reliable trackability, durable delivery, and versatility for both direct aspiration and stent-retriever use.”
Acute ischaemic strokes account for 85% of all strokes in Europe. By utilising aspiration catheters during thrombectomy procedures, physicians can restore blood flow in the brain by directly withdrawing a blood clot or using the catheter in combination with a stent retriever. However, in up to nearly 50% of cases, challenging anatomical features are present that can impact access to the clot, procedure time, recanalisation success, and clinical outcomes.
The TruCourse technology used in the Cereglide 71 aspiration catheter increases flexibility of the device, which is designed to deliver smoother navigation and access to clots, even in challenging anatomical conditions. This provides physicians with optimal compatibility, durable delivery, and reliable trackability during thrombectomy procedures, the press release states.
“The introduction of the Cereglide 71 aspiration catheter in Europe is an important step in endovascular thrombectomy, as it allows swift targeted clot access and removal during stroke treatment,” said Kyriakos Lobotesis (Imperial College London, London, UK). “With Cereglide 71 aspiration catheter, we can now access occlusion sites and aspirate clots more rapidly and efficiently, maintaining a smooth interaction with stent retrievers when used in co-aspiration. This leads to the prompt restoration of blood flow in the patient’s brain, which has the potential to save more lives and improve long-term clinical outcomes.”
Devices within the Cerenovus stoke solutions portfolio are developed using Cerenovus’ stroke science insights from its Neuro Thromboembolic Initiative (NTI). The results are products that have been tested in models that simulate real-world scenarios and seek to further address clinical unmet needs. The Cereglide 71 aspiration catheter will be included in the next phase of the CERENOVUS EXCELLENT Registry, a real-world registry focused on studying stroke-inducing blood clot removal by mechanical thrombectomy.
Speaking on behalf of ‘IR Bites’—a group whose mission is to raise the baseline public understanding and level of education on interventional radiology (IR)—medical student Milindu Wickramarachchi details their aims, the importance of elevating knowledge of IR and a pragmatic guide to running educational workshops.
IR among medical students, doctors, healthcare staff and the general public is very much a foreign field. As a medical student myself, the only hint of IR provided by Cambridge Medical School is showing the odd digital-subtraction-angiogram in passing during a lecture.
Personally, I think this is unacceptable. As technology has developed from the age of Charles Dotter, IR has had an exponential increase in its use in modern healthcare—from the simple yet elegant angioplasty to the excruciatingly detailed work of brain aneurysm coiling. This has not, however, been matched with an exponential increase in awareness of IR. By enabling further education on IR, we can foster innovation through collaboration of different specialities with radiology colleagues, enabling development of new techniques and breakthroughs in patient care.
If we are to increase interest and awareness of IR as a specialty, and its role in modern healthcare, drastic steps need to be taken to educate medical students, doctors, healthcare staff and the public.
Fostering awareness through an environment of learning and collaboration, we propose the introduction of new ‘IR Bites’ workshops—IR themed workshops held locally by people in the field, with the aim of raising the baseline public and medical understanding and level of education on IR.
The impetus for launching IR Bites workshops stems from a recognised need for targeted and accessible educational opportunities in IR. These workshops aim to bridge the gap between theoretical knowledge and practical application, offering a unique blend of lectures by professionals in the field and hands-on experiences with cutting-edge equipment that caters to the diverse learning preferences of participants.
Chris Grieco
Having carried out two of these workshops in 2023, head organiser and creator of IR Bites, Chris Grieco (Cambridge University Hospital, Cambridge, UK) has received overwhelmingly positive feedback. Participants reported:
Improved theoretical understanding of IR and how it relates to modern healthcare
Increased exposure to IR as a specialty
Increased understanding of the career path in IR
An increased need for their medical school to educate on IR
That they are likely to consider IR as their future career
All the points mentioned above are exciting future prospects for Interventional Radiology as a specialty, especially due to the critical shortage of interventional radiologists and training bottle-necks we are currently experiencing.
We propose a template for these events, such that they can be reproduced at any hospital/trust throughout the UK or abroad.
10 Step Guide: How To Run An IR Bites Workshop
Book a room and set the date: The first crucial step is to secure a venue and schedule the workshop, recognising that the date is pivotal for event progression.
Create a poster: Use design tools like Canva to craft an engaging poster, facilitating effective promotion through various channels.
Build industry contacts and secure sponsorship: Attend IR events, connect with professionals in-person and virtually through social media like LinkedIn and X. Leverage industry contacts to enhance workshop quality and visibility. Engage industry representatives to sponsor refreshments. We recommend pizza. Our speakers and delegates like pizza.
Identify speakers: Personally approach speakers, we suggest two consultants and one registrar each to give a 15 minute talk, to ensure varied perspectives and allows for a diverse question and answer session.
Finalise the agenda and plan the venue layout: Structure the workshop with a well-defined agenda, balancing informative talks with hands-on sessions. Strategically plan the workshop space, accommodating seating arrangements and industry demo setups, then distribute this so industry helpers can adequately prepare their logistics.
Streamline event registration: Utilise platforms like MedAll for seamless event registration, pre/post questions, and certificate distribution. This also allows for hybrid events with both local in-person and virtual attendees from around the world.
Implement marketing strategies: Employ diverse marketing strategies, including emails, newsletters, social media posts and posters with QR codes.
Coordinate pizza logistics: The most important step! One week before the event, confirm pizza orders and ensure industry confirmations to avoid disappointment. Check with the food policy with the venue.
Collect training kit: Check with industry representatives what kit they are bringing and source additional expired or training kit from your local IR department with permission from the charge nurse and lead doctor from the department. Photograph the borrowed kit before moving it so you can return it all exactly as you found it.
Prepare for Dropouts: Anticipate last-minute changes by maintaining a reserve list of attendees, speakers, and industry representatives.
Bonus Tip: Under Promise, overdeliver: Enjoy the workshop, savour the pizza, document attendance, and encourage immediate feedback using QR codes for a more impactful experience.
By following the above template, these events can be easily facilitated throughout different healthcare settings around the world. Medical students and doctors, healthcare staff and the public can be educated further about Interventional Radiology.
Along with the success of our previous two workshops (held in Taunton and Cambridge, UK), we are eager to improve on the format of these workshops. One major roadblock we faced was the lack of availability for the online participants to engage in the hands-on workshops. This could be improved by having a dedicated specialist talking through the equipment and doing a demonstration on camera (either pre-recorded or live). Another suggestion we received was having an ‘icebreaker’ where the leaders of the workshop could bust some myths the audience had about IR as a specialty. By acting on these points, we can hopefully increase the reach of courses in the future.
We aim to expand our reach of the IR Bites Network and hold courses across the UK and further afield with the next full day IR Bites Workshop scheduled for Thursday 6 June 2024 in Cambridge, UK. As IR Bites Workshops continue to evolve and grow, their impact on shaping the future of IR education and awareness is undeniable. If you want to be involved in organising an IR Bites workshop local to you or just stay up to date with future IR Bites Workshops scan the QR code to join our community and groups on WhatsApp: https://chat.whatsapp.com/CwUWim9JxIG62myRc7M59s
Milindu Wickramarachchi is a Year 5 Medical Student at University of Cambridge who recently attended an IR Bites Workshop and here shares his thoughts and reflections. The workshop event was organised by Chris Grieco with help from colleagues within the Radiology Department and industry partner representatives.
Bien Soo Tan is a senior consultant at the Department of Vascular and Interventional Radiology (IR) at Singapore General Hospital (SGH). Following his recent acceptance of the Society of Interventional Radiology (SIR) Gold Medal award, Tan speaks to Interventional News about his achievements to date.
IN: Throughout your career you have won several awards and will now accept the SIR Gold Medal Award. What does winning these awards mean to you?
I am very honoured and humbled to have been presented with these prestigious awards over the course of my career so far. I view these awards as a testament to the good work and high standards of IR practised in my department in SGH, in my country, Singapore, and in the Asia-Pacific region. The practice of IR is a team game, and I would not have been able to make any significant contributions without the help of many colleagues in the various institutions and organisations who I have worked with. I would also like to acknowledge the key roles my many mentors have played in my career. These awards are also a reflection of their achievements.
IN: You are past president for the Asia-Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR) among other leadership positions. How important is outreach and education for IR in the Asia-Pacific region?
Today, the standard of IR in the Asia-Pacific region varies widely throughout. We have many centres of excellence across the region, but unfortunately even more regions where there is no access to IR expertise. Education is key to addressing disparity. The APSCVIR is striving to be the driving force for IR education in the Asia-Pacific region. I am privileged to be part of the APSCVIR outreach initiative. This initiative commenced in 2016 with in-person IR workshops where APSCVIR faculty volunteered to teach in multi-year IR educational programmes in countries of need. It is important that outreach programmes are not one-off events but continuous programmes working hand-in-hand with host member IR societies. The APSCVIR outreach programme unfortunately ground to a halt during the COVID-19 pandemic. However, we soon realised the potential of virtual education and established a series of IR webinars that achieved even greater reach.
Last year, we resumed our in-person outreach programmes, and the plan moving forward is to have a hybrid of in-person teaching in targeted countries while continuing virtual webinars, which reach a wider audience.
IN: You have played a pivotal role in the expansion and modernisation of SGH’s IR department. What has been a standout achievement for your centre?
The contributions towards building our hospital’s department of vascular and IR must be attributed to all IR staff at SGH, which includes our radiographers, nurses, ancillary and support staff, and doctors. We are very proud that today, we are a standalone IR department providing a comprehensive range of IR services. We strive to be an IR centre of excellence, embracing both a high standard of clinical service as well as an academic practice. The strongest attribute we have is that despite being a large organisation, everyone pulls together to work as a team, in the interest of our patients. This is in keeping with our institution’s motto ‘Patients at the heart of all we do’.
IN: What is the current status of IR in South-East Asia? Where will IR go next in your region?
IR has grown tremendously in South-East Asia over the past decade, but there continues to be many regions and countries where access to IR services is not easily available.
I see continued growth in IR, with the clinical practice of IR being developed more robustly in this region. That means that radiologists have to care for and manage patients pre and post procedure, and not just be technicians performing procedures. I am optimistic that where IR is less developed, the timelines for catching up will be shortened. IR techniques are minimally invasive and work well for patients, and eventually patients will demand for the right to access IR services.
In the next five years, IR must embrace value-based care, as there is intense competition with increasing options in healthcare. For IR to grow, we must continue to collect the data and build the evidence for our techniques, as well as prove that our techniques are cost effective.
Johnson & Johnson is to acquire Shockwave Medical, it has been announced today.
Under the terms of the transaction, Johnson & Johnson will acquire all outstanding shares of Shockwave for US$335.00 per share in cash, corresponding to an enterprise value of approximately $13.1 billion including cash acquired. The transaction was approved by both companies’ boards of directors.
The acquisition of Shockwave further extends Johnson & Johnson MedTech’s position in cardiovascular intervention and accelerates its shift into higher-growth markets, Johnson & Johnson said in a press release. The acquisition will expand Johnson & Johnson’s medtech cardiovascular portfolio into coronary artery disease (CAD) and peripheral artery disease (PAD).
The transaction follows Johnson & Johnson MedTech’s acquisitions of Abiomed, a leader in heart recovery, and more recently Laminar, an innovator in left atrial appendage elimination for patients with non-valvular atrial fibrillation (AF). These
Shockwave is a provider of intravascular lithotripsy (IVL) technology for the treatment of calcified CAD and PAD. IVL is a minimally invasive, catheter-based treatment for calcified arterial lesions, which can reduce blood flow and cause pain or heart attack. IVL
In addition to its IVL platform, Shockwave also recently acquired Neovasc, developer of the the Reducer system, a novel product focused on symptom relief of refractory angina. The Reducer system is currently undergoing clinical studies in the USA and is CE marked in the European Union and the United Kingdom.
Joaquin Duato, chairman and chief executive Officer of Johnson & Johnson, said: “With our focus on innovative medicine and medtech, Johnson & Johnson has a long history of tackling cardiovascular disease—the leading cause of death globally. The acquisition of Shockwave and its leading IVL technology provides a unique opportunity to accelerate our impact in cardiovascular intervention and drive greater value for patients, shareholders and health systems.”
Tim Schmid, executive vice president and worldwide chairman of Johnson & Johnson MedTech, said: “Shockwave offers a truly differentiated opportunity to further enhance our leadership position in medtech, expand into additional high-growth segments, and ultimately transform the future of cardiovascular treatment. Shockwave’s IVL technology for treating CAD and PAD, and its strong pipeline, are in a class of their own. We look forward to bringing Shockwave’s solutions into Johnson & Johnson MedTech and the hands of more physicians around the world.”
“Shockwave has transformed the treatment of complex calcified arterial disease through the pioneering development of intravascular lithotripsy, and it is our mission to make this remarkable technology available to patients worldwide,” said Doug Godshall, president and CEO of Shockwave. “As part of a larger, more diverse organisation, with broad expertise and a core focus on improving patient outcomes, we are confident we will be able to further solidify IVL as the global standard of care for patients.
“I am deeply grateful to our team members and colleagues whose efforts have made today’s milestone possible; their accomplishments and passion have been extraordinary. I could not think of a better partner and home than Johnson & Johnson as the Shockwave team prepares to write its next exciting chapter.”
Dated 11 October 2023, the US Centers for Medicare & Medicaid Services (CMS) recently finalised its decision regarding National Coverage Determination (NCD) 20.7 for carotid artery stenting (CAS), confirming coverage expansion. Previously, patients were only eligible for CAS through clinical trials or if they were high-surgical-risk individuals. The decision made by the CMS removes several facility standards and approval requirements, as well as leaving coverage for any CAS procedure not described in the NCD to Medicare Administrative Contractor (MAC) discretion.
Previously, the CMS required facilities to hold an accreditation certification as a condition of reimbursement for CAS procedures. This meant that centres must meet a minimum standard for a range of criteria, self-attesting quality in areas such as staffing, equipment status, device inventory and facility infrastructure. Sceptical about the scope and diligence of the CMS’ accreditation requirements, David Sacks (Reading Hospital, West Reading, USA), past president of the Intersocietal Accreditation Commission (IAC) CAS board and a representative of the Society of Interventional Radiology (SIR), worked with stakeholders from professional societies to develop the IAC Carotid Artery Stenting accreditation programme, which began accrediting CAS facilities in 2011.
“Accreditation has two main purposes,” said Sacks, “one is that it provides guidelines for facilities to do a good job, know what best practices are, and fulfil recommendations. Second, it provides some degree of assurance to patients and insurance companies that patients are getting care that meets a particular benchmark—both of those have value”. Yet, he noted that some facilities see accreditation personified as “a policeman”, viewing the process as “unpleasant and usually not well-accepted”, rather than seeing accreditation as a means to provide “tools” to help organisations achieve better patient outcomes.
In the early days of CAS—around 2007—Sacks detailed that there was concern among specialties and societies that the procedure may be “abused” by providers with “unbridled enthusiasm” despite poor outcomes at that time. “Many of us felt that accreditation could be a useful tool for reigning in some of this enthusiasm and allow patients to get good care. There was no accrediting organisation that focused on [CAS], so I organised multiple conference calls among various societies to see how we could move forward.”
Engaging multiple societies, Sacks and colleagues agreed that a multispecialty, multisociety accreditation programme would be effective. Representatives from the American Academy of Neurology (AAN), American Association of Neurological Surgeons/Congress of Neurological Surgeons (AANS/ CNS) Cerebrovascular Section, American Association of Physics in Medicine (AAPM), Neurocritical Care Society (NCS), Society for Vascular Medicine (SVM), Society for Vascular Surgery (SVS), the SIR, Society of NeuroInterventional Surgery (SNIS), and the Society of Vascular and Interventional Neurology (SVIN), and later joined by the Society of Cardiovascular Angiography and Interventions (SCAI) “took off their societal hats to work together” to create the programme. Sacks averred that their end product—the IAC CAS accreditation programme— upholds “good processes of care via a thorough history”, requiring facilities to provide detailed logs of CAS procedures and periodical case reviews.
Following the launch of the IAC CAS programme, Sacks stated how they had hoped the CMS would defer to them for CAS accreditation. “Medicare in the USA requires facilities to be accredited to be reimbursed for CAS, but their accreditation system was pretty much just attestation, stating ‘we do good work’ and Medicare saying ‘OK’. We were hopeful that they would defer to us, but they never did.”
Aimed to reveal the distinction between IAC-accredited and non-accredited facilities certified by the CMS with CAS best practices, Sacks et al conducted an exploratory study in 2019. Their results demonstrated that IAC-accredited facilities are more likely to “follow best-practices, use quantitative tools to select appropriate patients, and quantitatively measure patient-centred clinical outcomes”, although the authors acknowledge the limitation of the study’s small sample size.
In Sacks et al’s discussion of their results, they aver that CMS-certified facilities “may not necessarily comply with process measures”, determining the value indicated by having an “external entity audit facilities” and provide “oversight to ensure best practices”. In a separate article analysing cases submitted for accreditation 90% of CAS asymptomatic cases and 28% of symptomatic stenosis did not meet CMS requirements for stenosis severity. Accredited facilities were found to have had significantly better compliance. Sacks and colleagues subsequently communicated these results with the CMS, however CMS decided to remove several training requirements and quality assurance measures, allowing centres to self-monitor procedural standards for CAS.
Casting a realistic eye toward the near future, Sacks stated that he is uncertain of whether facilities will choose to become accredited for CAS: “There could be many facilities who say ‘we are going to get into this and we want to be the best—what tools are available?’ Those folks might seek us out and apply for accreditation the same way people hire consultants to help them do a better job. Consultants aren’t mandatory, but they are a resource. We are hoping with the expected increase in the number of carotid artery stenting procedures and the number of facilities offering [CAS], that there will be an interest in using the IAC as a resource to improve and maintain quality of care.”
The IAC CAS accreditation is available both in the USA and internationally.
AngioDynamics, a leading and transformative medical technology company focused on restoring healthy blood flow in the body’s vascular system, expanding cancer treatment options and improving patient quality of life, today announced that the US Food and Drug Administration (FDA) has cleared the AlphaVac F1885 system for the treatment of pulmonary embolism (PE), enhancing its utility in critical medical scenarios such as PE.
The expanded FDA indication allows for the utilisation of the AlphaVac F1885 system for the treatment of PE, which broadens the applicability of the AlphaVac F1885 system in the non-surgical removal of thrombi or emboli from the venous vasculature. The indication expands treatment options for patients with PE, reducing thrombus burden and improving right ventricular function.
“FDA clearance marks a significant advancement in patient care and safety. This milestone underscores our commitment to merging physician-centric design with patient outcome-driven solutions,” said Juan Carlos Serna, AngioDynamics senior vice president of scientific and clinical affairs. “In addition to meeting our primary endpoints, the trial also showed a meaningful, favourable reduction in clot burden, ultimately improving patient outcomes.”
In December 2023, AngioDynamics announced the completion of patient enrolment in its Acute pulmonary embolism extraction trial with the AlphaVac system (APEX-AV) study, a single-arm Investigational Device Exemption study that enrolled 122 patients with confirmed acute, intermediate-risk PE across 25 hospital-based sites in the USA to assess the AlphaVac F18 system for the treatment of PE.
The APEX-AV study was initiated in partnership with the widely respected Pulmonary Embolism Response Team (PERT) consortium and led by co-principal investigators William Brent Keeling (Emory University School of Medicine, Atlanta, USA) and immediate past president pf the PERT consortium and Mona Ranade (University of California Los Angeles, Los Angeles, USA).
“The addition of the AlphaVac system in the mechanical thrombectomy world is a critical step forward in the treatment of PE patients,” said Keeling. “The rapid patient enrolment and the excellent safety and efficacy outcomes from the APEX-AV study validate the need for such technologies to be part of the PE treatment algorithm.”
The primary efficacy endpoint of the APEX-AV Study was the reduction in RV/LV ratio between baseline and 48 hours post-procedure. The primary safety endpoint was the rate of major adverse events (MAEs), including events such as major bleeding and serious device-related clinical deterioration, pulmonary vascular injury, and cardiac injury, within the first 48 hours. Patients were followed for 30 days post-index procedure.
“The 510(k) clearance of the AlphaVac system represents an important milestone towards the treatment of PE,” said Ranade. “The data from the APEX-AV study showed a significant improvement in the RV function and a rapid resolution of clot burden in the pulmonary arteries.”
The APEX-AV study showed a mean decrease in the RV/LV ratio from baseline to 48 hours post-procedure of 0.45 (significantly greater than the pre-defined performance goal of 0.12 (p < 0.001) and a MAEs rate of 4.1% (significantly lower than the pre-defined performance goal of 25% (p < 0.001). The study also showed a 35.5% mean reduction in clot burden from baseline to 48 hours post-procedure.
“Catheter-based therapies are becoming a major tool in the PE space,” said John M Moriarty (University of California Los Angeles, Los Angeles, USA), president-elect of the PERT consortium. “With a handle that can limit blood loss and a true large bore cannula with a 33Fr funnel, I expect the AlphaVac system to play a crucial role in the treatment of PE.”
Silk Road Medical has announced the launch of its Enroute transcarotid neuroprotection system Plus (NPS Plus), which the company describes as a key component of its transcarotid artery revascularisation (TCAR) portfolio.
As per a Silk Road press release, this next-generation device builds upon the prior Enroute transcarotid neuroprotection system to deliver smoother arterial sheath insertion, greater flow precision, and a simplified prep experience for surgical teams—all while maintaining “unparalleled” neuroprotection during the TCAR procedure.
“With the launch of the NPS Plus, we’re thrilled to empower our TCAR-trained physicians with a solution that addresses their insights and feedback to further strengthen and streamline the TCAR procedure,” said Chas McKhann, chief executive officer of Silk Road. “Our focus on new product innovation reflects our ongoing commitment to leadership in the treatment of carotid disease.”
The release goes on to state that TCAR combines direct carotid artery access with robust blood flow reversal, providing neuroprotection akin to open surgical techniques in a less invasive, more patient-friendly approach to treating carotid artery disease. During TCAR, the surgical team inserts a tube-like sheath into the carotid artery and connects it to the Enroute neuroprotection system, which temporarily reverses blood flow. The system filters potentially dangerous debris from the blood to reduce intraprocedural stroke risk while the team uses a TCAR-specific balloon and stent to open the artery, and contain the carotid artery disease.
TCAR delivers periprocedural stroke rates of less than 1% and a better patient recovery experience than open surgery, according to Silk Road.
“Silk Road Medical’s responsiveness to our feedback has provided us with better procedure predictability and a more streamlined workflow for our entire surgical team,” stated Brian Peterson (St Luke’s Heart and Vascular Institute, St Louis, USA). “With over 500 TCAR procedures performed by our team, we view TCAR as a first-line treatment option for carotid disease and we’re excited about what these improvements mean for patient care.”
Debates will shed new light on controversies in the treatment of aortic disease at the 2024 Charing Cross (CX) Symposium, alongside practical sessions with a focus on techniques and technologies in both aortic endovascular and open surgical repair.
Running over the full three days of the symposium, the comprehensive aortic programme at CX 2024 opens with aortic techniques and technologies on day one, followed by a full day focused on aortic arch and thoracic aortic controversies, and finishing with sessions covering juxtarenal and abdominal aortic aneurysm controversies, alongside advanced imaging and radiation reduction on the final day.
CX has a three-year cycle of raising vascular and endovascular controversies in order to challenge the available evidence and to be able to reach a consensus after discussion with an expert audience. “It is a controversies year, so the focus will be on debate,” says CX Executive Board member Tilo Kölbel (University Heart Center Hamburg, Hamburg, Germany).
The treatment of uncomplicated acute type B aortic dissection will be the subject of a great debate during Wednesday’s thoracic aortic controversies session, during which Kevin Mani (Uppsala University, Uppsala, Sweden) and Hence Verhagen (Erasmus Medical Center, Rotterdam, The Netherlands) will put forward their case that best medical treatment remains the standard of care, whilst Christoph Nienaber (Royal Brompton & Harefield Hospitals, London, UK) and Firas Mussa (McGovern Medical School, Houston, Texas) put forward the counter argument.
Gustavo Oderich (University of Texas Health, Houston, USA) and Eric Verhoeven (Paracelsus Medical University, Nuremberg, Germany) will debate the use of self-expandable covered stents versus balloon-expandable stent grafts in branched endovascular aortic repair later that day.
“It is of great interest to the community to understand the pros and cons for the use of balloon- versus self-expandable stents in branched repair,” says Kölbel of the significance of this debate. “Branched aortic repair is being done in increasing numbers, with more off-the-shelf devices being available for use in North America and in Europe. There are basically two different schools in vascular surgery. One uses balloon-expandable stents, which may be less flexible, and one uses self-expandable stents, which are more difficult to use because they need more profile.”
This session will also see Martin Austermann (St Franziskus-Hospital, Münster, Germany) and Nikolaos Tsilimparis (Ludwig-Maximilians University Hospital, Munich, Germany) trade views on the justification for prophylactic spinal drainage for thoracoabdominal endovascular repair.
“Spinal cord ischaemia is the most devastating outcome of complex aortic repair,” comments Kölbel. “One of the best ways to prevent that from happening is spinal drainage and it has been a recommended part of guidelines for many years. Recent guidelines have downgraded that recommendation, indicating that there is more controversy over whether the downsides and complications of spinal drainage still allow for prophylactic use.”
Polling at the end of each debate will give a clear indication as to where the CX community stands on each of these issues.
Alongside these sessions, Tuesday’s techniques and technologies session will focus on specific techniques in open and endovascular repair. Highlights include an edited case, presented by Oderich, which will cover transcatheter septotomy in chronic aortic dissection.
A podium first presentation—one of many to feature throughout the three-day aortic programme—during Thursday’s advanced imaging and reducing radiation session will explore how operator position influences radiation dose.
In March, the most popular stories from Interventional News included reports from the Society of Interventional Oncology (SIO) annual meeting (25–29 January 2024, Long Beach, USA); upcoming research to be presented at the Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA); among several more.
Sirtex Medical, a manufacturer of interventional treatment solutions, announced today the appointment of Matt Schmidt as chief executive officer and board of directors member, effective March 25, 2024.
A recent study published in the journal CardioVascular and Interventional Radiology has found conservative management may be efficacious in patients with spontaneous retroperitoneal haemorrhage (SRH), with added variable success seen after embolization in a more unstable patient group.
Hotly debated across SIO annual conference programme, speakers took to the stage to contest the survival of transarterial chemoembolization (TACE) in the age of yttrium-90 (Y90) transarterial radioembolization (TARE) and immunotherapy, their compelling arguments making some audience members “more confused and others happy”.
The Society of Interventional Radiology (SIR) Foundation, The VIVA Foundation and Penumbra, today announced the launch of the EMBOLIZE trial, a first-of-its-kind prospective, randomised controlled trial studying the effects of ovarian vein embolization (OVE) and pelvic vein embolization in reducing pain in women experiencing chronic pelvic pain due to pelvic venous disease (PeVD).
BD has announced the enrolment of the first patient in the AGILITY investigational device exemption (IDE) study, which will assess the safety and effectiveness of the BD vascular covered stent for the treatment of peripheral arterial disease (PAD).
Set to be presented at the upcoming Society of Interventional Radiology (SIR) annual scientific meeting, an anticipated late-breaking analysis of the BEST-CLI (Best endovascular versus best surgical therapy in patients with critical limb ischaemia) trial will expose the cause and significant impact that endovascular technical failure (ETF) had on patient outcomes.
New research to be presented at the Society of Interventional Radiology (SIR) annual scientific meeting has found early intervention with uterine artery embolization (UAE) can help women avoid hysterectomy due to severe bleeding after childbirth.
Cryoablation—minimally-invasive technique that uses ice to freeze and destroy small, cancerous tumours—has now been proven effective for breast cancer patients with large tumours, providing a new treatment path for those who are not candidates for surgery, according to new research to be presented at the Society of Interventional Radiology (SIR) annual scientific meeting.
The Society of Interventional Oncology (SIO) announces the European Institute of Oncology (IEO) in Milan, Italy, as the next European site approved for enrolment and activated for the society’s primary clinical trial, Ablation with Confirmation of Colorectal Liver Metastases (ACCLAIM) prospective trial for microwave ablation as a local cure.
Getinge and Cook Medical today announced an exclusive sales and distribution agreement for the iCast covered stent system, which recently received US Food and Drug Administration premarket approval for the treatment of symptomatic iliac arterial occlusive disease.
During the Society of Interventional Radiology (SIR) 2024 annual meeting (23–28 March, Salt Lake City, USA), newly presented data from a subgroup analysis of the STRIDE study showed that Penumbra’s Indigo aspiration system used in a single session without the need for overnight tissue plasminogen activator (tPA) is safe and effective for patients with lower extremity acute limb ischaemia (ALI).
“Although the use of tPA following aspiration thrombectomy with [the] Indigo system was not limited during the STRIDE study, the majority of patients did not receive it and still experienced excellent outcomes,” said STRIDE investigator Jayer Chung (Baylor College of Medicine, Houston, USA).
“These findings demonstrate that the use of aspiration mechanical thrombectomy, without overnight tPA, yields high procedural success, low complication rates, and high target limb salvage rates in [lower extremity] ALI.”
A press release details that, although widely used, there are many complications associated with tPA and other clot-busting drugs. In the case of the overnight lytic group, tPA was also associated with an increased need for intensive care unit (ICU) monitoring as shown by the higher median length of ICU stay among those patients.
“The high risk of associated major bleeding is a notable limitation of thrombolytics as an intervention across many disease states, and [lower extremity] ALI is no exception,” said Thomas Maldonado (New York University of Langone Health, New York, USA), national principal investigator of the STRIDE study. “The data show that aspiration mechanical thrombectomy is a safe and effective minimally invasive procedure, which may offer an option to eliminate thrombolytic use for some patients.”
STRIDE is an international, prospective, single-arm, multicentre, observational study of patients with lower extremity ALI and using the Indigo aspiration system as a frontline intervention. The latest findings include:
No significant differences were detected between patients who received overnight tPA and those who did not for target limb salvage rate at 30 days, patency at 30 days and 30-day mortality.
ICU resource utilisation was significantly lower in single-session Indigo patients.
Penumbra notes that ALI is associated with a high risk of amputation and death. Studies have shown that ALI patients treated with catheter-directed thrombolysis often risk further vascular complications, such as major bleeding.
An analysis involving some 300 patients with anterior-circulation acute ischaemic strokes caused by tandem lesions has determined a number of factors that may be predictive of good clinical outcomes at three months following an endovascular mechanical thrombectomy procedure. Said factors include admission glycaemia; initiating dual antiplatelet therapy (DAPT) and statin therapy within 12 and 24 hours, respectively, post-procedure; and stent patency within the first 30 days.
Writing in CardioVascular and Interventional Radiology (CVIR), Daniel Šaňák (University Medical School and University Hospital Olomouc, Olomouc, Czech Republic) and colleagues note that these predictors of positive post-thrombectomy outcomes were present in their study “beside the generally known ones”.
“However,” the authors add, “it remains unclear whether early start of DAPT and statin therapy after [mechanical thrombectomy] could be affected by the preceding early neurological worsening followed with or without sICH [symptomatic intracranial haemorrhage] in some patients. Thus, a further large prospective study is needed.”
Initially averring that tandem lesions in the anterior circulation currently represent a “clinical challenge” in stroke thrombectomy treatment, Šaňák and colleagues attempted to assess potential predictors of good clinical outcomes in these patients via the multicentre, retrospective ASCENT study.
In ASCENT, a ‘good’ three-month outcome was defined as a score of 0–2 on the modified Rankin scale (mRS), while successful recanalisation was defined as a score of 2b–3 on the thrombolysis in cerebral infarction (TICI) scale. SICH was assessed using Safe implementation of thrombolysis in stroke-monitoring study (SITS-MOST) criteria. In addition, logistic regression analysis was used to evaluate possible predictors of mRS 0–2, with adjustment for potential confounders.
Ultimately, a total of 300 patients with a median National Institutes of Health stroke scale (NIHSS) score of 17—of whom 68.7% were male and who had a mean age of 67.3 years—were analysed in the study. Šaňák and colleagues note that recanalisation was achieved in 290 patients (96.7%), and 176 (58.7%) had an mRS score of 0–2.
Besides the more well-known predictors of post-thrombectomy outcomes, including age, NIHSS on admission, and sICH, the researchers identified that the following, less established factors were also present in ASCENT: lower admission glycaemia (p=0.005; odds ratio [OR], 0.884); stent patency within the first 30 days after thrombectomy (p=0.0003; OR, 0.219); DAPT started within 12 hours after thrombectomy (p<0.0001; OR, 5.006); and statin therapy started within 24 hours after thrombectomy (p<0.0001; OR, 5.558).
Prior to concluding, Šaňák and colleagues do acknowledge multiple limitations of their study, including its retrospective design and lack of central, blinded assessment of imaging findings. They also note that thrombectomy-related strategies—including carotid artery stenting (CAS), periprocedural antiplatelet regimen and postprocedural management—were not standardised or unified across all participating centres, and the possibility that these differences may have impacted their results cannot be excluded.
In addition, they state that the fact some patients did not receive DAPT due to early neurological worsening and/or presence of ICH on computed tomography (CT) imaging performed earlier than the first 12 hours after thrombectomy may limit the interpretation of their findings. However, no association between starting DAPT early and sICH occurrence was found in the study, they add.
I believe medicine is an art not a science. WH Auden said it was the art of wooing nature not the science of healing. We practice an artisanal craft, having become attuned to the patient’s needs and woes, using expensive complex technology to be minimally invasive. The devices and technologies we use today have been created by less than 3% of our colleagues. I know this because when I was running the annual Society of Interventional Radiology (SIR) meeting in 2010 I took the membership of the society—6,000 doctors—and cross-referenced their names with patent filings at the US and European patent offices. Of this survey, 447 people held 2,500 patents or patent filings.
I repeated this work in 2020. I have longitudinal data on a cohort of inventors over time. We built social network maps of the inventors and identified those who invented during residency, fellowship and in their staff positions. Peak creativity for most interventional radiologists occurs during their fellowship. That’s when they perfect their skills, they work with mentors, they find their voice and culture as physicians, and they are challenged by impossible cases. It’s the impossible cases, which we do not decline to attempt to fix, that result in the creation of new devices and techniques.
The focus is traditionally on new device development, intellectual property, on royalties exits and initial public offerings (IPOs). That is misplaced. Let’s be clear that invention may be a technique not a device, and it may be shared by word of mouth and example for publication without there ever being any financial reward.
I interviewed many SIR inventors, and as in other fields, I found that the driving force for most was regret. People like us lie awake at night perseverating over bad outcomes and think of ways we could have done the procedure differently. Throughout medical history this is the case. Laser Greenfield developed his vena cava filter after a patient with multiple leg fractures had died from pulmonary embolism. He lamented about this in a bar with his friend who worked in the oil and gas industry. His friend told him of a filtering system used in pipes which Greenfield applied to the inferior vena cava. Harvey Cushing developed the intraoperative anaesthesia record after a patient he was sedating with chloroform died in his arms. Andreas Grüntzig, the inventor of the coronary angioplasty balloon, and many others were driven by grief from bad outcomes to develop better devices.
What became clear from analysis of the 2020 social network maps was that key institutions played a major role in enabling trainees to express their creativity through device development. These institutions are the classic ones, the inner-city hospitals of last resort, the major training programmes across the USA and Europe. Those inevitably are the locations or cultures that have developed the supports for this creativity. They can expedite and enable our trainees to succeed in new device development. The halos of those institutions’ open doors with industry that would be regrettably shut if you were training in a smaller, less globally relevant institution.
I developed my Murphy vertebroplasty needles while a fellow at the University of Geneva working with Professor Daniel Rufenacht. He told me I was going to be the vertebroplasty person. I didn’t want to do that but when I began to do those procedures I realised how inadequate the equipment was. Daniel opened the door for me with industry which gave me access to a catalogue of tools and devices. I was able to pick and choose and create better needles, better injectors and better cements for vertebroplasty. Great mentors create those opportunities. I try to do that for my trainees today. Some are incredibly talented. That talent is like the rare earth elements in the periodic table that creates the future of interventional radiology. Talented residents and fellows need to be nurtured, enabled and opportunities created for them. That is the critical part of our role as teachers.
Kieran Murphy is vice chair and vice chief of radiology and medical imaging at the University of Toronto, in Toronto, Canada.
The International Accreditation System for Interventional Oncology Services (IASIOS) is the world’s first accreditation programme focused exclusively on standardising interventional oncology (IO) care, redefining the rapidly evolving field. Reporting record growth exceeding 150% in 2023, IASIOS recently announced their first accredited facility in the USA, a significant milestone which marked its expansion to a new and major corner of the international IO community.
Jack Jennings
“It’s accreditation and unification,” said Jack Jennings on behalf of the newly accredited Mallinckrodt Institute of Radiology (MIR) at Washington University in St Louis, USA. Embarking on their IASIOS accreditation process, Jennings and his team were driven by the opportunity to strengthen bonds with the physicians of IASIOS’ international network. This “alliance”, and mutual dedication to improving quality and safety in IO, is more relevant today than ever, Jennings conveyed, as the specialty does the groundwork for the “steep and rapid incline” of IO procedures in this booming faction of interventional radiology (IR).
In a comment to Interventional News, chair of the IASIOS supervisory board Andreas Adam (Kings College London, London, UK) shared that the global nature of IASIOS is one of its greatest strengths, as it emphasises certain universal concepts such as IRs looking after their own patients. Remarking on the recent USA accreditation, Adam stated that MIR’s enrolment is a “major milestone” in IASIOS’ history. “The USA is the birthplace of IR and the largest provider of IR services. We are delighted to welcome the MIR, as its accreditation is a perfect demonstration of the universality of the principles on which IASIOS is founded.”
A world-first accreditation programme
IASIOS is the world’s first accreditation system focused solely on upholding quality assurance for minimally-invasive treatments for cancer. Due to the continued growth and recognition of IO as a key clinical discipline and the fourth pillar of cancer care, consensus has dictated that centres providing IO treatments must adhere to robust guidelines to ensure a universally high standard of care. During its conception, the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) lifted the current quality assurance standards for radiation oncology—developed by The Royal Australian and New Zealand College of Radiologists (RANZCR)—as a template which was well aligned with the practice of IO.
The fruits of this labour—the CIRSE Standards of Quality Assurance in Interventional Oncology—establishes a “gold standard” in patient care and safeguarding in IO. Yet, as RANZCR president at the time and current steering board member of IASIOS Liz Kenny (Royal Brisbane and Women’s Hospital, Herston, Queensland Australia) noted, IO is “still a
very young speciality and in many countries faces obstacles that other clinical disciplines have already overcome”.
For this reason, Kenny alongside CIRSE, spearheaded the development of the tiered accreditation system—IASIOS— to “distinguish between ‘core criteria’ i.e., those considered necessary to provide safe patient care, and ‘extended criteria’, which are more aspirational and considered the ideal”, which Kenny and IASIOS chief operations officer Mardis Karlsdottir, outlined in a recent article published in the Journal of Medical Imaging and Radiation Oncology.
The Standards of Quality Assurance in Interventional Oncology that form the foundation of IASIOS has since gained global support from over 40 national and international radiology and interventional radiology societies, drawing the discipline together in a “unified front”, Kenny and Mardis state, and this comes at an opportune moment.
In the house of IR—and an integral section of it—IO is embarking on a parallel path to greater recognition internationally, which is developing apace alongside novel innovations and technological advancements in the field. For Jennings, installing a “baseline accreditation” sets a background for quality and safety among the rapid growth of IO therapies, such as immunotherapy. “It’s great to have an overarching accreditation process to know that we’re not going rogue, or cowboy-esque; to bring greater uniformity, credibility and validity to the specialty on both sides of the pond,” Jennings explained.
David Breen
“The truth is that [IO] has become a bit of an innovative Wild West,” said David Breen (University Hospital Southampton, Southampton, UK), resonating with Jennings while speaking on behalf of his IASIOS-accredited centre. IO sits within a “rapidly developing and complex therapeutic arena” he explained, stating that IASIOS, alongside CIRSE, has arrived at a critical time in the development of IO. “In a number of areas an individual’s cancer care pathway is set to become more complex, with increasingly significant contributions from IO. It’s important that IASIOS now begins to set agreed international standards and expectations of practising units. This will help IO develop in an organised fashion and realise its full potential.”
By surveying accredited facilities, recognition for IO varies geographically, but this remains a challenge which IASIOS intends to rectify across the globe. For Jennings in the USA, following the American Board of Medical Specialties (ABMS) recognition of IR as a primary specialty in 2012, quality and safety measures have “not been geared at [IO], which is seen as a subset of [IR’s] quality and safety”. In gaining IASIOS accreditation at his institution, Jennings hopes to lead the way for other interventional oncology facilities in the USA to follow suit, giving the specialty better footing—“a lot of people are talking about this” he said, suggesting that IASIOS accreditation has a “larger overall message” of awareness raising.
Connecting international centres
Murat Dökdök
IASIOS accreditation for Murat Dökdök (Anadolu Medical Centre, Gebze, Turkey) has enabled his centre to look at IO procedures specifically, to “define the processes that are crucial in maintaining best medical practice”. As day-to-day interventional procedures are “complex to interpret”, he detailed, a clear benefit of IASIOS is its ability to “instil trust” and promote confidence for patients and physicians alike. Dökdök also expressed the importance of bolstering IO through IASIOS’ global network, noting that “collaboration among accredited centres from various countries can foster international research projects, joint training programmes and cross-border healthcare initiatives”.
Mark Burgmans
In The Netherlands, Mark Burgmans (Leiden University Medical Centre, Leiden, The Netherlands) agrees that IASIOS accreditation has made it “easier to reach out to other centres and share experiences” in order to “overcome hurdles” in the field. Yet, he maintained that the collection of robust data via randomised controlled trials in IO can be “difficult or impossible”. He furthered that real-world data and registries should be used to reinforce recognition for IO, as they have already found “convincing evidence of the efficacy and effectiveness of IO therapies”.
“Healthcare is facing tremendous challenges,” Burgmans continued, identifying rising staff shortages and financial constraints occurring amid increasing demand for care. “IO is part of the solution—it offers effective therapies at lower costs and shorter hospital stays,” said Burgmans, advocating for “investment” in IO today, confident that this investment will return in the future, in part facilitated by IASIOS. “IASIOS will help to convince policy makers, health authorities, funding agencies, and board directors that IO is a safe bet”.
“We are close,” Breen added, “but healthcare commissioners and patients still need awareness of IO’s major, yet still potential, contribution to cancer treatment”. Concurrent to Burgmans, Breen believes that high-quality adoption of IO will be achieved through “highly-literate lobbying” with interventional oncologists placed on guideline panels. This is particularly crucial in the context of technological advancements, as Breen stated that IASIOS will bring “structure to IO provision before there is haphazard, poor-quality adoption by other services”.
Rodrigo Gobbo
For Rodrigo Gobbo (Hospital Albert Einstein, São Paulo, Brazil) IASIOS has allowed of applying to become his centre to “stay abreast” of technological advancements, seeing their clinicians gain “comprehensive training” and maintain “consistent high-quality outcomes” for patients. “The accreditation acts as a guide for navigating the dynamic landscape of IO,” Gobbo said, underlining the adaptive nature of the IASIOS which ensures accredited centres “remain at the forefront of innovation to benefit both patients and clinicians alike”.
Gaining momentum
IASIOS’s global expansion is evident; with their most recent accreditation in the USA, sights are set on connecting more global facilities with their IO network. Championing excellence in oncological treatments, IASIOS’ objectives are “not just checkboxes” as chief operations officer Mardis conveyed, but rather “milestones in our collective journey towards excellence in IO”. “Our vision extends beyond accreditation, to a collaborative community that accelerates IO development and enhances global access to IO care. In 10 years, IASIOS aspires to be a central hub where IO practitioners contribute to and benefit from benchmarking, workshops and knowledge exchange, ensuring excellence in patient care on a global scale.”
IASIOS is no doubt gaining international momentum in its pursuit of a worldwide standard for the highest quality of care for patients with cancer. Creating a unified voice for the furtherment of IO, IASIOS continues to report a growing community with centres throughout Asia, Australia, Europe, the Middle East, North America, and South America.
In a recent interview, Marie Josee van Rijn from Rotterdam, the Netherlands and Emma Wilton from Oxford, UK, provided insight into the transformative power of interventional approaches in the treatment of DVT. They also set the stage for the upcoming INARI Symposium at CX 2024, where they will focus on the critical importance of clot removal and its profound impact on the lives of patients with iliofemoral DVT.
Both van Rijn and Wilton agree that mechanical thrombectomy has enabled their centers to achieve an optimal patient pathway by providing interventionalists with a wider treatment window. ” It doesn’t really matter if the clot is two, six or eight weeks old, you can still intervene with ClotTriever. If you only had thrombolysis as a treatment option, that would matter and your therapy would fail”.
To learn more about INARI’s Symposium at CX 2024 click here.
This video was filmed by Inari Medical and is being sponsored for distribution in association with Vascular News, Interventional News and Venous News. Biba Medical bears no responsibility for the assets used in the production of this video.
Medical imaging artificial intelligence (AI) company Avicenna.AI have today announced that it has received 510(k) clearance from the US Food and Drug Administration (FDA) for its CINA-iPE and CINA-ASPECTS products. Using a combination of deep learning and machine learning technologies, the company develops AI solutions that automatically detect and prioritise life-threatening conditions, assess them for severity, and subsequently notify clinicians.
Addressing the serious issue of delayed and missed findings in diagnostic imaging, CINA-iPE is an AI-powered tool that detects incidental pulmonary embolism (PE) during routine computed-tomography scans. Unsuspected PE is a common finding in routine CT scans of the chest, but as little as 25% of emboli are reported during the initial interpretation, the press release explains. This is particularly relevant in the cancer patient population, where pulmonary embolism is a significant cause of mortality.
The CINA-iPE algorithm identifies lung blood clots detected during routine CT scans for entirely different health conditions. Scan types may include full-body scans, scans of the chest, abdomen, and pelvis, and scans of the thoracic area along with the abdomen and pelvis. The tool was validated on 381 CT scans (performed for other clinical indications than for PE evaluation) acquired on 39 different scanner models from five leading manufacturers, achieving excellent sensitivity and specificity.
“From day one, we have been committed to validating our AI tools on every type of CT scanner,” said Yasmina Chaibi, clinical affairs manager, Avicenna.AI. “In our validation studies, CINA-iPE achieved excellent sensitivity and specificity, demonstrating its ability to provide effective prioritisation and triage on routine CT scans performed for other clinical indications than pulmonary embolism suspicion.”
CINA-ASPECTS is an AI tool for stroke severity assessment, automatically processing non-contrast CT scans and calculating the “ASPECT” score, a topographic scoring system used to quantify the severity of a stroke from a CT scan of the brain. The tool computes a heat map indicating the probability of hypodensity and sulcal effacement in the brain, displays a list of infarcted regions, and provides CT images corrected from tilt to easily compare the right and left hemisphere.
“The validations and multi-reader-multi-case studies we conducted highlighted that CINA-ASPECTS not only obtained outstanding standalone performance, but also demonstrated that its adjunctive use significantly improved clinicians’ accuracy in the assessment of ASPECTS regions, compared to the conventional use of National Center for Competency Testing (NCCT) images alone,” added Chaibi.
CINA-ASPECTS is the first FDA-cleared tool from Avicenna.AI in the category of computer-aided diagnosis (CADx), which means it goes beyond identifying abnormalities in scans to provide an assessment of the severity of a condition.
“We are delighted to launch CINA-ASPECTS to the US market, marking a significant milestone as our first CADx product receives FDA clearance,” said Stéphane Berger, regulatory and quality manager. “We take pride in being at the forefront of CADx solutions, being the first AI company supported by thorough clinical validation and a rich repository of real-world clinical data, which ensures compatibility across all manufacturers and platforms.”
CINA-iPE and CINA-ASPECTS are the latest tools from Avicenna.AI to secure FDA clearance, joining its AI solutions for medical emergencies, including automatic detection of intracranial haemorrhage (CINA-ICH), large vessel occlusion (CINA-LVO), aortic dissection (CINA-AD), PE (CINA-PE) from CT-scan imaging.
“After a long journey of dedication and perseverance, we are thrilled to announce the FDA clearance of not one, but two of our groundbreaking products,” said Cyril Di Grandi, co-founder and CEO of Avicenna.AI. “The clearance of CINA-iPE and CINA-ASPECTS marks a significant milestone in our mission to strive for excellence in advancing patient care. These achievements stand as a testament to the unwavering commitment of our team.”
Getinge and Cook Medical today announced an exclusive sales and distribution agreement for the iCast covered stent system, which recently received US Food and Drug Administration premarket approval for the treatment of symptomatic iliac arterial occlusive disease.
Cook Medical will assume sales, marketing and distribution rights for the product in the USA over the coming months. The iCast covered stent system will continue to be manufactured by Atrium Medical Corporation (Merrimack, USA), which is part of Getinge.
“This agreement with Cook Medical ensures that the iCast covered stent system will reach the optimum number of patients who will benefit from it in the USA,” said Patricia Fitch, president of Getinge in North America.
“This product fills the need of a covered stent in our vascular portfolio with a proven technology. iCast has five-year data aligned with our commitment to long-term clinical evidence and predictable results for [peripheral arterial disease] therapies,” said Mark Breedlove, senior vice president of Cook Medical’s vascular division.
Cook and Getinge continue to collaborate in other strategic areas, also partnering to complete the PRESERVE-Zenith branch endovascular graft-iliac bifurcation investigational device exemption (IDE) study with five-year follow-up. The purpose of this study was to evaluate the safety and effectiveness of the Zenith device in combination with the iCast covered stent in patients requiring treatment of aortoiliac and iliac aneurysms.
At the Charing Cross (CX) Symposium 2024 (23–25 April, London, UK), Andrew Bradbury (University of Birmingham, Birmingham, UK) and the BASIL-3 team of triallists will address the pressing question of which endovascular strategy wins in the disputed femoropopliteal segment. The investigators will be presenting—for the very first time—the results of this long-awaited, only completed, fully publicly funded randomised controlled trial (RCT) in the space.
The BASIL-3 team will reveal clinical and cost-effectiveness data comparing three alternative femoropopliteal endovascular revascularisation strategies—plain balloon angioplasty with or without bail-out bare metal stent, drug-coated balloon with or without bail-out bare metal stent, and drug-eluting stent— for the management of severe limb ischaemia (chronic limb-threatening ischaemia [CLTI]).
“They’re actually very different technologies,” Bradbury points out to Vascular News ahead of CX 2024. “So, when we set up BASIL-3, we thought it was very important to have a three-arm trial so that we could compare these three different endovascular strategies. And, we’ve been able to do that; we’ve recruited to target, observed more than the required number of primary endpoints and that gives us at least 90% power. We have very complete, virtually 100%, follow-up data on the primary outcome, which is amputation-free survival. So, we think they’re good-quality data.”
“It’s a very controversial area,” Bradbury opines, making the BASIL-3 first-time data presentations an apt centrepiece for this year’s controversies-focused meeting.
“Although these drug devices have been in practice for probably 15 years now and certainly the last 10 years, it’s been a rocky road for them,” Bradbury explains, citing the paclitaxel mortality debate sparked by the 2018 meta-analysis from Katsanos et al as some important context to the trial. The publication directly affected the progress of BASIL-3, halting proceedings for many months.
“There were concerns around what appeared to be excess mortality across a wide range of industry-funded trials at two and five years, and it’s taken a long-time to resolve that,” Bradbury remarks, providing a brief summary of the six-year saga that a separate session at CX 2024 will address in detail. He references recent reversals of paclitaxel safety warnings by both the US Food and Drug Administration (FDA) and subsequently the UK Medicines and Healthcare products Regulatory Agency (MHRA) that have, “to a great extent”, put any concerns “in the rearview mirror”.
Some of the data being presented at CX 2024 will illuminate the cost effectiveness of the three strategies being compared. Bradbury underlines the “very complicated” nature of health economics and details what the investigators have looked for in BASIL-3. “There’s a close relationship between number of days spent in hospital an overall cost,” he says. “So, if you have a procedure that’s more expensive but reduces the length of the index admission and also subsequent readmissions—because a lot of these patients come back into hospital—that saving, in days in hospital and further interventions, could easily wipe out even quite a large excess of increased cost from the procedure, which in this case being three endovascular strategies would be the device costs.”
Bradbury also considers the global landscape of endovascular care. He underlines variation and unpredictability in endovascular practice across the world, highlighting a need for concrete data in the field.
“Sometimes what you hear at meetings is not really what happens day to day in various vascular centres,” Bradbury points out. The BEST-CLI study, for example, published in the New England Journal of Medicine in 2022, showed a benefit of vein bypass over endovascular in cohort one. “But if you look at the data,” he says, “only half of the patients who were put into the endovascular group actually received a drug device.” This, Bradbury points out, is much lower than might be expected for USA-based practice.
In BASIL-2, on the other hand, which was presented at CX 2023 and simultaneously published in The Lancet, around a third of the patients in the endovascular group had a drug device. “That’s higher than I expected,” he comments.
“It’s really interesting to look at what is custom and practice at the moment in different countries and I think it’s quite difficult to know what that it,” Bradbury highlights.
New data set to aid endovascular decision making
“We think you’ll find the data that we present on clinical effectiveness and also cost-effectiveness very interesting, whatever your views at the moment on the role of these drug devices in the management of CLTI,” Bradbury remarks of the forthcoming presentations. “We very much hope that these new Level 1 data will be of great interest to the Charing Cross audience and help people make decisions in their everyday practice.”
The BASIL-3 podium first is set to take place at 16:10 on Tuesday 23 April as part of the peripheral arterial controversies programme’s inaugural Roger M Greenhalgh late-breaking trials session.
The Society of Interventional Radiology (SIR) Foundation, The VIVA Foundation and Penumbra, today announced the launch of the EMBOLIZE trial, a first-of-its-kind prospective, randomised controlled trial studying the effects of ovarian vein embolization (OVE) and pelvic vein embolization in reducing pain in women experiencing chronic pelvic pain due to pelvic venous disease (PeVD).
“Women living with pelvic pain often suffer in silence because of a lack of awareness of pelvic venous disease and the minimally invasive treatment options available,” said SIR Foundation Chair Maureen P Kohi (The University of North Carolina, Chapel Hill, USA) a member of The VIVA Foundation board of directors and an interventional radiologist and chair of the department of radiology. “This study will solidify the role of OVE in the treatment of women experiencing pain from pelvic venous disease and will also provide evidence needed to ensure insurance coverage for these treatments.”
This trial is a multi-society collaboration between SIR Foundation and The VIVA Foundation, in partnership with Penumbra. An investigator-initiated clinical trial, EMBOLIZE will be led by Ronald S Winokur Weill Cornell Medicine, New York, USA) and Gloria Salazar (The University of North Carolina, Chapel Hill, USA), associate professor of radiology. Both will serve as the national co-principal investigators.
The study investigators are seeking women over the age 18 who have dilated uterine, ovarian vein or pelvic veins that are causing chronic pain. To determine efficacy, the study will compare changes in the patients’ pain scores on a visual analogue scale from four weeks before treatment through six months post-treatment to evaluate the outcome of vein-directed intervention for venous origin chronic pelvic pain. Investigators will also evaluate other quality of life improvements, improvements in the pelvic vein varices, and changes in pain medication usage.
PeVD occurs when enlarged veins develop in the pelvis surrounding the uterus or ovaries. This can lead to severe chronic pelvic pain. PeVD usually affects women who have previously been pregnant and have experienced a backup of blood flow in the ovarian and pelvic veins much like varicose veins in the legs.
“Patients with pelvic venous disease have few treatment options available to them,” said James F Benenati, chief medical officer at Penumbra. “Dedicated to advancing innovative therapies that address a significant unmet need, Penumbra’s support of this study will help provide clear evidence of the benefits of OVE and PVE to help patients worldwide.”
Sirtex Medical, a manufacturer of interventional treatment solutions, announced today the appointment of Matt Schmidt as chief executive officer and board of directors member, effective March 25, 2024.
Since joining Sirtex in 2023, Schmidt has been an integral part of the company’s executive leadership team, collaborating with senior leaders and shareholders to set corporate strategy, accelerate organisational performance, deliver strong results and build a winning culture, a press release states.
“I am confident Matt will advance Sirtex’s vision of providing minimally invasive cancer and embolization therapies to more patients around the globe,” said Weikun Tang, chairman of Grand Pharmaceutical Group. “Matt’s performance-driven leadership capabilities, as well as his commitment to partner with physicians to provide patients with innovative solutions, positions him as the right person to lead Sirtex into its next phase of growth. We are excited to work closely with Matt as Sirtex continues to create value for patients, physicians, employees and shareholders.”
With 20 years of industry experience and expertise, Schmidt joined Sirtex as executive vice president of global sales in February 2023 and was subsequently promoted to chief commercial officer in August. He has previously held leadership positions at Abbott Vascular, including divisional vice president, where he was responsible for leading the company’s US coronary interventional cardiology device business, overseeing sales, marketing, commercial excellence and customer engagement. Prior to that role, Schmidt was divisional vice president and general manager for Abbott’s vascular business in Japan. He earned an MBA from the University of Michigan and a bachelor’s degree in accounting from Goshen College in Indiana.
“I am optimistic about the future and honoured to lead the Sirtex team during this exciting time in company history, especially given some of the transformative solutions we have brought to market over the last year,” said Schmidt. “We are a patient-centred organisation with talented employees who are dedicated to improving lives. I am very much looking forward to what we will achieve together.”
New research to be presented at the Society of Interventional Radiology (SIR) annual scientific meeting (23–27 March, Salt Lake City, USA) has found early intervention with uterine artery embolization (UAE) can help women avoid hysterectomy due to severe bleeding after childbirth.
“These findings are important and may help more women avoid hysterectomy and other very serious complications of uncontrolled haemorrhage,” said lead author Younes Jahangiri (Michigan State University, East Lansing, USA), a resident interventional/diagnostic radiologist. “As the medical community looks for ways to provide better care for women to address maternal health and peri-partum care, this is one more option on the table that could help many women.”
The study was a retrospective review of 66 patients with a median age of 31 who underwent UAE for uncontrolled postpartum haemorrhage at a single, high-volume medical centre between 2014–2022. UAE successfully controlled postpartum haemorrhaging in 62 of the 66 patients (94%). Four patients required hysterectomies to stop the bleeding, all of whom lost at least 2,400ml blood prior to presentation for UAE and symptoms of diffuse intravascular coagulopathy, a clotting abnormality that can happen after large-volume haemorrhage due to rapid consumption of clotting factors.
Postpartum haemorrhage is a rare, but can be a potentially deadly complication of childbirth. To stop it, obstetricians will initially use conservative approaches to replace the lost blood or to promote clotting. If these measures are insufficient, hysterectomy is usually performed. Alternatively, interventional radiologists can be brought in to perform UAE, injecting tiny particles into the arteries that supply blood to the uterus using fluoroscopic imaging guidance. Once placed in the arteries, the particles temporarily block blood flow to stem uterine bleeding.
“Based on these findings, we would encourage obstetricians to involve interventional radiologists early, to be ready to perform UAE if more conservative approaches are not managing postpartum haemorrhage,” said senior author James Morrison (Michigan State University, East Lansing, USA).
Researchers in this study found a 36% incidence of post-embolization syndrome, which presents with abdominal pain and flu-like symptoms. The study found that it was more likely to occur in patients who experienced greater blood loss before embolization.
Jahangiri, Morrison and their colleagues plan to expand their research to include multiple institutions and ultimately to conduct a prospective study that examines longer-term outcomes of UAE.
A minimally invasive treatment using MRI and transurethral ultrasound instead of surgery or radiation is effective in treating prostate cancer, according to new research presented at the Society of Interventional Radiology (SIR) annual scientific meeting (23–27 March, Salt Lake City, USA).
The traditional treatment options of radiation or surgery often come with a risk of side effects, including urinary incontinence and erectile dysfunction that cause significant morbidity and adverse lifestyle effects. Researchers said that some patients now have a durable alternative for whole-gland treatment with magnetic resonance imaging (MRI) guided transurethral ultrasound ablation (TULSA) that does not preclude future treatment with surgery or radiation.
“The success of TULSA represents a revolution in whole-gland treatment for prostate cancer,” said lead author Steven S Raman (University of California, Los Angeles, USA). “Prostate cancer is the most common form of cancer in men, affecting one in eight men in their lifetimes. We have more research to do, but if validated, TULSA has the potential to change the standard of care for thousands of men.”
In the TULSA procedure, a small catheter-like device is inserted through the urethra into the prostate. Once there, MRI is used to guide precise positioning of 10 therapeutic ultrasound elements into the prostate. MR thermometry is used to monitor the tissue while heating to more than 55 degrees within the prostate and limiting heat to the sensitive nerves surrounding the prostate as the device rotates around the entire gland. The procedure can be performed in an outpatient or in-patient facility under general or spinal anaesthesia in two to three hours.
According to Raman this image-guided therapy: “maximises our ability to kill cancer cells while minimising collateral damage to the prostate to achieve the ultimate trifecta in prostate cancer treatment—full local cancer control while maintaining urinary continence and potency. The latter are the complications of most prostate cancer therapies that patients hate and often result from a lack of precision in treatment monitoring.”
In the prospective observational study, participants showed improvement in the reduction of the presence of cancer, prostate size and prostate-specific antigen levels (PSA), which are markers for cancer. Cancer was undetectable on follow up biopsy by 76% at one year after TULSA with a decrease in median prostate volume by 92% within one year and a decrease in PSA from 6.3ng/ml to 0.63ng/ml at five years.
TULSA had a very favourable side-effect profile compared to alternative surgical, radiation and thermal therapy showing that, up to five years, 92% of patients recovered continence and 87% preserved erectile function. During the study, 115 men were enrolled across 13 sites in five countries. Of those treated, 25 men received follow up conventional treatment with surgery or radiation because of residual or new tumours. Through this process, researchers learned the early predictors of TULSA failure related to calcifications between the urethra and prostate cancer and better monitoring of prostate swelling, targeting and misalignment, leading to improved detection and management of these preventable errors during the procedure.
Raman noted that the study affirms that interventional radiologists now have a meaningful role in detection and management of prostate cancer care as they already had in other types of cancer, such as lung, kidney and liver cancers. He said interventional radiologists expertise in imaging and image-guided procedures and experience with ablation make them a critical part of the prostate cancer care team.
The research into TULSA’s effectiveness continues with the CAPTAIN trial, a randomised control trial comparing TULSA with radical prostatectomy.
Cryoablation—minimally-invasive technique that uses ice to freeze and destroy small, cancerous tumours—has now been proven effective for breast cancer patients with large tumours, providing a new treatment path for those who are not candidates for surgery, according to new research to be presented at the Society of Interventional Radiology (SIR) annual scientific meeting (23–27 March, Salt Lake City, USA).
“For patients who have larger tumours but can’t undergo surgery, this approach could be more effective than the current standard of care for patients who are not surgical candidates,” said Yolanda Bryce (Sloan Kettering Cancer Center, New York, USA). “When treated with only radiation and hormonal therapy, tumours will eventually return. So, the fact that we saw only a 10% recurrence rate in our study is incredibly promising.”
Cryoablation uses imaging guidance such as ultrasound or computed tomography (CT) scan to locate tumours. An interventional radiologist will then insert small, needle-like probes into the breast to create an ice ball that surrounds the tumour, killing the cancer cells. When combined with hormonal therapy and radiation, patients can have nearly 100% of their tumours destroyed. If the tumours do grow, patients can be treated with cryoablation multiple times to control growth. The treatment has been successfully used to treat tumours smaller than 1.5cm, but its effectiveness on larger tumours was not extensively demonstrated until now.
This retrospective study assessed outcomes for 60 patients who underwent cryoablation because they were not candidates for surgery or refused surgery after consultation with a breast surgeon due to age, cardiac issues, hypertension, or currently undergoing chemotherapy for another cancer. Their tumour sizes ranged from 0.3—9cm with an average size of 2.5cm. Patients with tumours larger than 1.4cm were treated with multiple probes (one probe placement for each centimetre of disease). In a follow-up after 16 months, the recurrence rate was just 10%.
“Surgery is still the best option for tumour removal, but there are thousands of women who, for various reasons, cannot have surgery,” said Bryce. “We are optimistic that this can give more women hope on their treatment journeys.”
The procedures were performed with local anaesthesia or minimal sedation, depending on the eligibility and preference of the patient. The freeze-thaw cycle started with 5–10 minutes of freezing, followed by 5–8 minutes of passive thaw, and then 5–10 minutes freezing at 100% intensity. Patients were able to go home on the same day, following the treatment.
The researchers will continue to follow the patient cohort to collect data on long-term effectiveness and to better understand the impact that adjuvant (e.g. hormone therapy and radiation) therapies combined with cryoablation can have on this patient population.
Hans-Henning Eckstein, the vascular surgeon who played a leading role in the SPACE and SPACE 2 randomised controlled trials on the treatment of carotid stenosis and founder of the Munich Vascular Conference (MAC), died on 24 February at the age of 68. Colleagues have paid tribute to an “excellent doctor, outstanding researcher and university professor” as well as a “bridge-builder between vascular surgery and neurology”.
Eckstein had been chair and professor of the Department of Vascular and Endovascular Surgery at the University Hospital Rechts der Isar of the Technical University of Munich (Munich, Germany) and was widely recognised for advancing research and knowledge in the field of vascular surgery. He was awarded an honorary doctorate from the Medical Faculty of the University of Larissa (Larissa, Greece) in 2017 and, since 2019, had also been a visiting professor at the Medical School of Pittsburgh (Pittsburgh, USA) and Stanford University (Stanford, USA).
After studying medicine at Ruprecht-Karls University Heidelberg (Heidelberg, Germany), Eckstein completed his PhD in 1986 and two years later acquired his postdoctoral teaching qualification in Heidelberg.
From 1999 until 2003, Eckstein was medical director of the Clinic for Vascular Surgery at Ludwigsburg Hospital (Ludwigsburg, Germany). In 2004, he became director of the Department of Vascular Surgery at the University Hospital “Rechts der Isar” of the Technical University of Munich and five years later was appointed the first holder of the newly created chair for vascular and endovascular surgery at the university—a role he held until his retirement in 2023.
A statement on the Technical University of Munich’s website mourning the loss of Eckstein reflects on his impact at the institution: “Prof Eckstein made the clinic known far beyond the borders of Munich and developed it into a leading centre and attraction for patients with vascular diseases.”
Eckstein played a leading role in research including randomised controlled trials on symptomatic and asymptomatic carotid stenosis, which—a statement on the European Stroke Organisation (ESO) website reads—made him “well-known” in vascular neurology. He was co-chair of the steering committee of SPACE and SPACE 2, representing vascular surgery in both multicentre trials.
Furthermore, Eckstein was heavily involved in the creation of international guidelines in his field, including the German S3 guideline for the diagnosis, therapy, and follow-up care of patients with carotid stenosis and the ESO guideline for carotid stenosis.
Eckstein’s involvement in professional organisations included his 2009–2010 presidency of the German Society of Vascular Surgery and Vascular Medicine (DGG), and his editorship of the journal Gefässchirurgie (Vascular Surgery).
Eckstein was also involved in vascular education and founded the Munich Vascular Conference (MAC). The 12th iteration of this event took place in December 2023 and received international attention.
Several colleagues have paid tribute to Eckstein and highlighted his legacy in the fields of vascular surgery and neurology. “We are deeply saddened by the death of Prof Eckstein,” a statement on the Technical University of Munich’s website reads. “With Prof Eckstein we are losing an extremely committed colleague and excellent doctor, outstanding researcher and university professor.”
Eckstein is also remembered in a statement on the ESO website, with Werner Hacke, senior professor of neurology at Ruprecht-Karls University of Heidelberg, and Peter Ringleb, academic researcher at the University Hospital Heidelberg (Heidelberg, Germany) stating: “In Hans-Henning Eckstein we have lost an extremely dedicated colleague and excellent physician, an outstanding researcher, university lecturer, bridge-builder between vascular surgery and neurology, and a friend.”
Biotronik has been granted Breakthrough Device designation (BDD) from the US Food and Drug Administration (FDA) for the Freesolve below-the-knee (BTK) resorbable magnesium scaffold (RMS).
To qualify for a Breakthrough Device designation, a device technology must address an unmet need and show that it has the potential to provide for more effective treatment of life-threatening diseases or irreversibly debilitating conditions. The goal of the programme is to provide patients and clinicians with timely access to these breakthrough treatments by accelerating their development, assessment and review while maintaining regulatory standards for pre-market approval.
A press release notes that the newly CE-launched Freesolve RMS for coronary artery lesions, based on the Biomag magnesium alloy and the proven Orsiro drug-eluting stent (DES) coating technology, provides safety, improved deliverability, and optimal performance and vessel support during and after implantation. It has shown 99.6% degradation of magnesium observed 12 months after implantation in coronary arteries, the release details.
These characteristics of the Freesolve RMS may be of particular value in BTK interventions, where vessel scaffolding is desired in the short-term to resist vessel recoil, yet ultimately leave the vessel implant-free.
“Biotronik’s focus on vascular interventional excellence is evident in our strategic investments and persistent dedication to innovation”, said Jörg Pochert, president of Vascular Intervention at Biotronik. “Our efforts to expand therapeutic possibilities, underlined by the introduction of the Freesolve RMS for coronary artery disease treatment, will continue in the BTK indication with this groundbreaking innovation.”
“This Breakthrough Device designation for the Freesolve RMS for BTK treatment is a significant milestone in advancing treatment options. Biotronik is committed to design our products to enhance the lives of patients,” stated Ryan Walters, US president at Biotronik. “Our next generation RMS represents a leap forward over existing resorbable technology, incorporating technical innovations intended to address physicians’ needs and optimise outcomes for patients suffering from CLTI.”
Set to be presented at the upcoming Society of Interventional Radiology (SIR) annual scientific meeting (23–28 March, Salt Lake City, USA), an anticipated late-breaking analysis of the BEST-CLI (Best endovascular versus best surgical therapy in patients with critical limb ischaemia) trial will expose the cause and significant impact that endovascular technical failure (ETF) had on patient outcomes. In doing so, the investigators hope to provide a granular, contextual understanding of why these failures happen in real-world practice.
Published in 2022, the BEST-CLI trial results found surgical intervention superior to endovascular revascularisation. Split into two cohorts based on the availability of suitable single segment greater saphenous vein (SSGSV) for bypass, BEST-CLI enrolees were randomised in a 1:1 fashion to either surgery with SSGSV bypass or endovascular treatment (cohort 1), or surgery with an alternate bypass conduit or endovascular treatment (cohort 2). Enrolment criteria required reasonable surgical risk and anatomy suitable for both bypass and endovascular treatment. The results showed that technical success was 98.3% vs. 84.7% for cohort 1, and 100% versus 80.6% in cohort 2, respectively.
Technical failure rates in both cohorts markedly contributed to the difference in outcome between surgery and endovascular outcomes in both groups, but the reason these failures occurred was unclear. This formed the basis for Richard Powell (Dartmouth Hitchcock Medical Center, Lebanon, USA) et al’s analysis which sought to evaluate the causes and impacts of ETF on outcomes.
Richard Powell
Powell, speaking to Interventional News, explains that the BEST-CLI findings offered a close-to-accurate representation of real-world endovascular treatment experience. “If you look at a lot of studies carried out by industry there are very low rates of technical failure, as lower-risk patients are often cherry-picked for enrolment meaning biased results,” Powell states. However, in extracting causal factors of ETF from the BEST-CLI data, Powell et al have drawn conclusions which will “[confirm] suspicions” about industry-run studies in this arena.
In their analysis, Powell and colleagues analysed the causes for ETF in both cohorts, the impact on major adverse limb events (MALE), above ankle amputation, death and major adverse cardiovascular events (MACE: defined as myocardial infarction, stroke and serious cardiovascular adverse events). ETF was defined as the inability to successfully complete the initial endovascular procedure.
John Kaufman
“We approached this with an open mind,” details co-investigator John Kaufman (Oregon Health and Science University [OHSU] in Portland, USA). “We were interested that proximal SFA [superficial femoral artery] occlusion, which was such an influential determinant, and that failure to cross the lesion was far more common than dissection, residual stenosis, or distal embolization as a failure mode.”
The investigators also analysed lesion location, which Powell highlights as a strength of their trial. In determining this, he hopes that granular predictions can be developed for patients that are less likely to achieve technical success, to map potential failure modes for each specific case.
Kaufman suspects there will be great interest in their findings set to be presented at highly-anticipated SIR 2024 in Salt Lake City, USA, due to the significant influence ETF had on outcomes in the BEST-CLI dataset, and on real-world endovascular practice. He adds that their results will likely stimulate even more questions in an attempt to elucidate the reasons for ETF even further. “We anticipate some difficult and maybe even some sceptical audience questions at the SIR annual meeting” he speculates.
Taking this in stride, Kaufman views that this is all an essential part of science and important research, but there are questions that they will not be able to answer yet, such as the morphology of uncrossable occlusions that cause ETF. “We don’t yet know whether these are flush or heavily calcified, nor the specifics of the techniques used to attempt to cross the lesions. I think we all approach occlusions with a measure of respect, and these results support that.”
Ahead of the presentation of their results, USA, Kaufman hopes to shed some light on the context for why ETF happens in order to help provide guidance when evaluating patients, and point to areas of improvement and innovation in endovascular procedures. In using the BEST-CLI data for their current research, Powell adds that credit is due to the three principal investigators—Matthew Menard (Brigham and Women’s Hospital, Boston, USA), Kenneth Rosenfield (Massachusetts General Hospital, Boston, USA), and Alik Farber (Boston Medical Center, Boston, USA)—who accomplished a “huge undertaking” with a highly comorbid and sick patient population, which produced valuable, real-world data for the betterment of endovascular treatment.
With more than 35 years of tenure at the University of California, San Diego (UCSD) School of Medicine, Anne Roberts retired in 2022 and is a USCD distinguished professor of radiology, emeritus. Having held numerous leadership positions, the development of her self-titled catheter for uterine artery embolization, and now, her most recent gold medal from the Radiological Society of North America (RSNA), Interventional News interviewed Roberts to survey her key moments from a trailblazing career in interventional radiology (IR).
I don’t think that anybody goes into their career with the idea that they’re going to win a gold medal of any kind, but the medals are a lovely recognition that I made some contributions to the field. In a way, [the awards] are all tied together because I had been involved in leadership positions with each society during times of development. For example, I had been president of the SIR and then was in leadership with the ACR when the idea of IR becoming a separate specialty arose, and I helped support this, despite the ACR not being initially too enthusiastic. The RSNA Gold Medal was probably also partially in recognition of my involvement in the push toward an IR primary specialty. At the end of the day, the main thing that awards do is say, well, you got involved, you helped, you did something, and some people recognised your work. I’m incredibly fortunate to be recognised since there are so many people who are involved in multiple societies that improve the specialty.
IN: Early in your career you took a sabbatical with the US Food and Drug Administration (FDA) and the Center for Devices and Radiological Health (CDRH). How did your experience influence your IR practice and why did you specifically become involved?
The reason I got involved with the US FDA was because I was eligible for a sabbatical and I knew I wasn’t going to write a book. At the time there was a huge hue and cry about how IR devices weren’t being approved and that it was the FDA’s fault. This was a part of the reason I wanted to get involved, I was going to fix the FDA—talk about hubris. So, I got involved with the CDRH and it was my job to be a reviewer.
I discovered the reason devices weren’t getting through was because interventional radiologists were doing a very poor job of running their studies. They would enrol patients, some would be randomised but then the patients would be off protocol—it was sort of the Wild West, there just weren’t good data to support the FDA’s protocol. I think we’ve gotten better; we have learned a lot about running clinical trials, we’re certainly better than we were.
IN: You were at involved in advancing uterine fibroid embolization and the development of the Roberts Uterine Catheter (RUC)—what did this process look like?
When I was a fellow as Massachusetts General Hospital, Arthur Waltman took several of us to a medical device company to see the manufacturing process, and I watched the Birds Nest filter (Cook Medical) be made—by workers who were soldering the wires, making them all by hand—and I was blown away by that. I realised there was an industry out there that made things to specifications.
When uterine artery embolization came along, a lot of people were using the Waltman loop. I learnt the technique from Arthur but we were using a larger, thicker catheter, and it would tend to hold its shape. I had tried to do this with smaller catheters but the loop tended to unloop, and I couldn’t get it to do what I wanted—I guess that was one of my failures as one of Arthur’s trainees!
So, I approached a manufacturer and said: I want a 5Fr catheter that has a long extra limb and I want it tapered down to a 4Fr so that it’s easier to get into the uterine artery. I want a marker put on the apex so that I can tell when I have got it over the bifurcation so it’s ready to reform. They made it and then they put my name on it.
I didn’t ask them to do that, and I don’t get anything for it. People have said ‘Oh boy, you could’ve made a lot of money’, all I wanted was for people to have something useful. It’s kind of sad that it’s become very difficult to get innovative things made, everybody is very risk averse and understandably so, but it has moved away from the individual being able to design something, and toward company development.
IN: You have previously served as president of the SIR, vice-president of the ACR. Across these appointments what has been your greatest achievement?
The fact that I became president of SIR is probably my greatest accomplishment. I was very young when I became president and there weren’t many women in the society. Arina Van Breda (Sentara Northern Virginia Medical Center, Woodbridge, USA) was the first woman who was president in 1992–3 and she did a great job and was a terrific role model. This was a time of significant change, the society was opening up and some of the old guard weren’t too happy about that, but there were other members that knew this is where we should be going.
IN: You have been involved in several training programmes in Africa—what would you say are the priorities when it comes to making sure interventional radiologists-in-the-making receive the highest standard of training possible?
In Africa, training programmes can be difficult to set up due to the infrastructure of many of these countries. Electricity was a huge problem, for all kinds of medical equipment, but particularly for IR equipment—you can’t have the power suddenly going out. It’s also incredibly hard for them to access IR training, since it is so hands-on—the USA isn’t accepting short-term hands-on trainees from foreign countries, and it’s become difficult to find training in programmes in Europe and Asia.
What is needed is someone like me who’s retired—more or less—and put us someplace for several months at a time. In this way, the people in the community can become trained, and be trained on the problems that are present in their community, with the equipment they have available to them.
IN: What has been your experience as a woman in the field of interventional radiology?
The great thing was at the beginning I never had to wait for a bathroom. Today, it’s unfortunate that many women are worried about going into IR, I think this is misplaced. There are great women in IR and I trained in a place where there were many women doing IR. I never felt that I couldn’t be an interventional radiologist, but there has been discrimination. I once called to apply for a private practice job and introduced myself, and this guy says to me ‘We’ve never hired a woman. We’ll never hire a woman and we’re not interested’. So, there were hurdles along the way.
IN: Where does IR go next? What one innovation do you see for the field in the next five years?
I’m not a very good prognosticator. Five to ten years ago if you spoke about radioembolization I would have said, what’s that? Things have changed a lot over my career, and will continue to change. I’m not smart enough to think that I know—or maybe I’m smart knowing that I don’t know.
Innovation has always driven IR, that’s what we do and it’s what drives the field forward. It’s important that we have people who have a desire for innovation and see IR as a place where this can be done. I don’t know where IR is going to go, but wherever it is, it’s going to be great.
In a session dedicated to neonate, infant and paediatric interventional radiology (IR), Hisham Alshehri (King Abdulaziz University, Jeddah, Saudi Arabia) gave a talk at the Pan Arab Interventional Radiology (PAIRS) annual congress (10–13 February, 2024, Dubai, United Arab Emirates) on the wide range of conditions that botulinum toxins (Botox) can treat.
First, explaining its mechanism of action, Alshehri detailed that Botox works by blocking the release of acetylcholine at the level of the neuromuscular junction, resulting in the relaxation of local muscles within two weeks of treatment. The injection effects typically last between three to six months.
The speaker detailed however that interventional radiologists should act with “careful consideration” when deciding dose for paediatric patients. “Botox affects children in a different way when compared with adults,” Alshehri explained, using hypertonia—a condition in which there is too much muscle tone which stiffens the arms, legs or neck, making them difficult to move—as an example. For patients with this condition, the underlying hypertonic disorder is superimposed onto two unique processes of childhood growth and development in contrast to adults.
Looking at appropriate dosage for paediatric patients, Alshehri noted that the total maximum body dose per visit must not exceed 12 units per kg or 400 units total, and the maximum volume per site should not exceed 0.5ml, except for certain cases that may require more.
Alshehri then discussed the niche indications that have shown to benefit from Botox treatment, such as upper and lower limb spasticity in children with cerebral palsy, congenital muscular torticollis, sialorrhea and brachial plexus palsy. The toxin can be used in all ages, but early research carried out by Barry Rawicki (Monash Medical Centre, Clayton, Australia) et al suggests a better response in children younger than eight years old.
Then, drawing the PAIRS 2024 audience’s attention to the current safety status of Botox treatment in paediatric patients, Alshehri detailed that serious side effects have been observed to date. These can include fever, muscle weakness, swallowing and respiratory difficulties, seizures, or death. Between 2006 and 2018 the US Food and Drug Administration (FDA) Adverse Event Reporting System recorded 51 cases of adverse reactions associated with Botox injections to children 17 years of age and younger.
However, he added that research in this area is still in its infancy. A meta-analysis carried out by Jean- Sébastien Bourseul et al found that, in 437 children who received Botox injections for musculoskeletal conditions, no severe side effects were reported. In another study by the same author, they found that in 74 infants younger than two years old who received Botox for spasticity, there was a 3.6% incidence of mild side effects in patients younger than one year and a 6.5% incidence in infants between one and two years old.
Surveying these results, Alshehri pointed out that there is no international consensus for the use of Botox in paediatric patients younger than two years of age. Due to the safety and effectiveness of this treatment however, Botox can be used off-label as an adjuvant to physical therapy and surgery in moderate to severe cases.
He concluded that many of these musculoskeletal conditions come with permanent sequelae causing a “high level” of disability. Botox for the treatment of these paediatric patients offers a minimally invasive means of providing relief and preventing long-term disability. Concluding, he asserted that interventional radiologists should use tools such as ultrasound to increase the effectiveness and accuracy of Botox treatments, to crucially minimise adverse events.
“Is more research needed in the world of filters? Yes, but is more research needed to determine whether the class itself is safe? No.” Charting the recent history of inferior vena cava (IVC) filters through the PRESERVE trial (Predicting the safety and effectiveness of inferior vena cava filters), principal investigator Matthew Johnson (Indiana University, Indianapolis, USA) speaks to Interventional News on the ins and outs of filter removal.
“Hundreds of thousands of patients with venous thromboembolism [VTE] had filters placed, yet clearly there was an incidence of filter-related complications, such as breaks or perforations.” Johnson began by discussing the rationale behind PRESERVE, recounting the “maelstrom of concern” that was raised in 2010 following the US Food and Drug Administration (FDA) warning letter. The letter stated that all “implanting physicians and clinicians responsible for the ongoing care of patients with retrievable IVC filters should consider removing the filters as soon as protection from pulmonary embolism [PE] is no longer needed”.
Sparking “multidistrict litigation” against filter manufacturers in the USA, Johnson stated that there was a “huge lack of understanding” over the role of IVC filters as they relate to VTE. This, in part, may have been due to opaque definitions of VTE which, “for example, could be a sub-centimetre gastrocnemius clot below the knee or the entire vena cava could be occluded causing massive symptoms”, he explained. “Our definitions made it difficult for us to evaluate things, because we weren’t exactly sure what the extent of disease was and how filters should be used in these populations.”
Primarily used to prevent deep vein blood clots from developing into PE, the patient population privy to this procedure is “incredibly variable” in Johnson’s experience. IVC filters are often placed in patients “immediately following trauma, as a preoperative measure in cancer patients, or for prophylaxis—which is another entirely complicated thing, placing a filter in a patient without VTE”.
In clinical practice, filters are most commonly placed in people who cannot be anticoagulated; randomised trials have sought to evaluate filter efficacy in patients who have received concomitant anticoagulation, because randomising patients who can be anticoagulated to a filter or no treatment is unethical, Jonson explained. PRESERVE—a large multicentre prospective trial without a control group but with predetermined imaging and clinical outcome evaluations—was performed to obtain the best ethical data.
Originally PRESERVE had been incited by a US FDA warning letter—“which scared people”, Johnson recalled—and which brought the Society of Interventional Radiology (SIR) and Society for Vascular Surgery (SVS) together, putting themselves forward to evaluate the safety and efficacy of IVC filters from the seven manufacturers who marketed filters in the USA.
Conducted at 54 sites in the USA between 10 October, 2015 and 31 March, 2019, Johnson et al identified 1,421 patients who had a filter implanted—1,019 of patients had existing deep vein thrombosis (DVT) or PE. Their results met primary safety and effectiveness endpoints, with investigators reporting that procedural adverse events were “uncommon” and there was a “low incidence” of clinically-significant PEs.
The investigators note that a “high rate” (44.5%) of filters were removed in this cohort and the reported low rate of adverse events was perhaps due to the “mandates for noting a plan for [IVC filter] removal at the time of placement”, accompanied by frequent follow-up. Supplying a conclusory suggestion, Johnson et al believe that, when planning IVC filter placement, physicians should consider when the device should be removed, and patients should be followed closely in the interim.
“We should—all of us who place filters—view planning a patient’s treatment pathway as a central tenet of providing comprehensive, filter-inclusive care. In today’s world you cannot place a filter and just leave it. That’s not good medicine,” Johnson said. Having demonstrated the correlation between retrieval planning and survival rate through PRESERVE, Johnson’s central takeaway is: “at the time of placement, have a plan for removal”, although he understands that that is “much easier said than done—people’s states change all the time, operation dates change, contraindications change”.
“We’re not going to do better than PRESERVE,” Johnson said, but more is yet to be done to “optimise patient care” in this population. “Newer devices are being developed, however more research is needed to evaluate a device that may be less likely to poke out of the vena cava, or is easier to remove, or may even dissolve,” said Johnson, who maintained that innovation for better outcomes in these patients will prevail through future research efforts.
Interventional radiologists Thomas Albrecht (Vivantes Clinic Neukölln, Berlin, Germany) and Roberto Iezzi (Policlinico Universitario Fondazione Agostino Gemelli, Rome, Italy) share their experience performing transarterial chemoembolization with degradable starch microspheres (DSM-TACE) using EmboCept S DSM 50 μm (Magle Group). Indicated for liver cancer treatment including hepatocellular carcinoma (HCC) and liver metastases from colorectal cancer (mCRC), and lung tumours, they detail how this invaluable “tool in [their] toolbox” has expanded effective options for interventionists to provide better patient care.
EmboCept S DSM 50 μm is an adjuvant in the intra-arterial treatment of inoperable liver and lung tumours in combination with cytostatic agents. Using microspheres of roughly 50 μm in size and with a half-life of approximately 35 minutes, EmboCept S DSM 50 μm can be used for super-selective treatments of single segments and selective targeting of one liver lobe to treat multifocal tumors.
EmboCept S DSM 50 μm in the landscape of TACE
Thomas Albrecht
EmboCept S DSM 50 μm DSM-TACE sits alongside drug-eluting bead transarterial chemoembolization (DEB-TACE), and conventional transarterial chemoembolization (cTACE), as a viable treatment option for patients with liver tumours. However, due to its unique degradable quality, EmboCept S DSM 50 μm can be used in a wider breadth of patients with varying levels of disease as Albrecht elaborates: “We use EmboCept S DSM 50 μm mainly in patients with multifocal or multisegmental disease, which is predominantly HCC in our practice, because you can treat patients with a high degree of efficacy and low toxicity.”
The degradable mechanism of action characteristic of EmboCept S DSM 50 μm allows for “transient” ischaemia, Albrecht states, detailing that this significantly decreases sides effects and improves the therapeutic effect. He adds that, during treatment, prolonged ischaemia has the potential to produce toxicity which can cause post-embolization syndrome and subsequently trigger loss of liver function. With EmboCept S DSM 50 μm however, the risk of these occurrences is “much less marked, if not minimal”, he says, providing a “much improved” safety profile, even when used in more extensive disease—“although we treat a larger proportion of the liver, it’s still better tolerated than other techniques”.
Treatment strategy
Roberto Iezzi
For Iezzi, the degradable characteristic of EmboCept S DSM 50 μm is also a notable benefit, enabling revascularisations “without concern over occlusion or collateralisation from a material point of view”. For mCRC, the ability to repeatedly perform treatment is key, as chemoembolization is often combined with irinotecan, which requires repeated activation by a healthy liver, he outlines.
“When providing care for mCRC, we need to apply a lobar approach, which involves a total of two treatments per lobe—or four treatments if it’s a bilobar procedure—performed with a delay of two to three weeks. It’s essential that we have the ability to perform repeated treatments within a very short period of time.”
In Iezzi’s view, the possibility to combine EmboCept S DSM 50 μm with various drugs, such as doxorubicin or epirubicin, which are also commonly used, is invaluable. “We are experiencing great results and its potential to be combined with other drugs [opens] the door for the treatment of new indications. Not only HCC or mCRC, but also cholangiocarcinoma and other liver metastasis, from pulmonary or gastrointestinal to gynaecological tumours,” he says.
“It’s a local treatment option for patients with advanced multifocal disease,” Albrecht states, expanding on the potential application of EmboCept S DSM 50 μm for a range of indications. “These patients would often not be treated with other types of TACE and they are being treated with radioembolization less often,” he says. Causing “minimal toxicity”, Albrecht conveys that EmboCept S DSM 50 μm is an “extremely well-tolerated” treatment option with very few side effects, making the procedure tolerable to patients at a wider range of disease level.
Evidenced clinical performance of EmboCept S DSM 50 μm
Informing their assertions, Iezzi and Albrecht worked side-by-side to conduct the largest retrospective European multicentre study, which scrutinised the safety and efficacy of DSM-TACE for advanced stage HCC in patients for whom were ineligible for other standard therapies or for whom these had failed . Their results were published in 2021 in the journal Cancers.
Led by Johannes M Ludwig (University Duisburg- Essen, Essen, Germany), the investigators identified 121 patients from three European centres. To be treated with DSM-TACE, patients were required to have had unresectable HCC with specific inclusion criteria between institutions. In Berlin, patients with a Barcelona Clinic Liver Cancer (BCLC) stage of C and D were deemed eligible; in Rome, patients with BCLC B refractory to TACE or stage C, those with a Child-Pugh class of A or B and those with an Eastern Cooperative Oncology Group (ECOG) status of between 0–1; in Essen, patients not suitable for ablation, transplantation, conventional TACE, radioembolization, or systemic therapy with kinase inhibitors, and an ECOG status of between 0–2.
They documented that the overall tumour burden in this population was high, with bilobar disease in 63.6%, >3 HCC nodules in 61.2%, and vascular invasion in 26.4%. Yet, their results showed that patients survived a median of 15.5 months with a median time of 9.5 months to tumour progression, and a 83.2% disease control rate. Additionally, they found that patients who survived longer had lesions of ≤10cm, the involvement of a single liver lobe, a lower Child-Pugh class and BCLC stage, and the absence of vascular invasion or of extrahepatic metastases.
In summary of their results, the investigators asserted that DSM-TACE using EmboCept S DSM 50 μm particles is a “veritable treatment option” for all unresectable HCC patients with high/diffuse tumour burden, “where other treatments fail or cannot be offered due to contraindications”.
The future of DSM-TACE with EmboCept S DSM 50 μm
For now, Albrecht says that he would like to see more interventionists using the technique, and to continue disseminating knowledge about its benefits to the wider community, with the approach still somewhat “unknown” in many countries. “For healthcare professionals, it’s an attractive option to be able to offer patients,” underlining how the effective treatment is also “relatively simple”.
Returning to the patient, Iezzi highlights that DSM-TACE using EmboCept S DSM 50 μm represents another treatment option for those in whom options may be limited. “It’s characterised by a high level of comfort for the patient,” he continues, “and it could be combined with a transradial approach”. In Iezzi’s belief, the demonstrable efficacy and safety of EmboCept S DSM 50 μm in liver tumours can “open the door” to future “outpatient and ambulatory care. The patient could be dismissed from hospital six hours after treatment” he adds, with the aim of offering effective and comfortable treatment options for patients.
Embo ASSIST AI
helps interventional
radiologists to develop embolization practice in OBLs
This advertorial is sponsored by GE HealthCare.
Jason Brower
“Our practice has embraced the concept of artificial intelligence [AI] as a tool that improves physician performance for better outcomes—placing patients at the centre of the equation,” shares Jayson S Brower, interventional radiologist and president of Inland Imaging in Spokane, USA. Translating treatment from a hospital setting to an office-based lab (OBL), Brower describes their unique setup using GE HealthCare’s Embo ASSIST AI software, which he claims streamlines procedures and ensures cost-effectiveness when treating increasingly complex cases in an outpatient interventional setting.
Opening their outpatient interventional radiology (IR) clinic during COVID-19, Brower and colleagues’ initial aims were to sustain treatment of immunosuppressed patients—often those attending for oncology procedures—while reducing exposure to illnesses found in hospitals. Hospitals in the USA, Brower points out, are “cash strapped”, meaning equipment can often be “outdated”. Shifting away from the traditional hospital setting, outpatient treatment centres, or OBLs, have become more common in the USA in recent years. As Brower explains, “it has been a bit of a journey— we opened in 2019 after planning for about a year and half to two years prior to that. If you rewind all the way to 2017, there were maybe a handful of OBLs in the country—it was really a novel concept”.
As a champion for the OBL model, Brower believes that the translation of treatment to an outpatient environment is the “next best evolution in patient care, primarily due to the cost, quality and patient experience”, he asserts. “Outpatients can be seen on a timely basis—if we say we will treat you at 9am, we are going to treat you at 9am. Whereas, when you come to the hospital, emergencies arise, thereby delaying scheduled procedures.” Opening their OBL to ensure patients can receive timely, efficient treatment, Brower was confident that patients were going to have “the same great quality [treatment] by our team, with significantly less cost to the system”, a benefit which is then passed on to the patient. “Those were the elements that really motivated us to start pushing this down the path,” he says.
Brower and his team opted for the latest generation of imaging equipment, “opening the door for us to improve patient experience, with less radiation and overall improved patient experience” he says. Choosing GE HealthCare’s “exceptional” equipment for their interventional suite, Brower and his team’s focus was on their “strong” concurrent alignment on AI as a tool that aims to improve patient care, which formed the foundations of their current collboration. Brower states that the incorporation of Embo ASSIST AI into their practice has proven to “tangibly benefit both the physician and the patient” in both diagnostic and interventional settings.
Embo ASSIST AI helps interventional radiologists to develop embolization practice in OBLs
After setting up their outpatient interventional suite, Brower tells Interventional News, their team’s focus on how best to integrate AI with their practice continued. “We invested in the software and software upgrades alongside the evolution of the technology, such as the Liver ASSIST Virtual Parenchyma [GE HealthCare] solution, which we have incorporated into our practice.”
In helping to reduce procedure times, Brower defines the “spill-over” benefits, such as reduced sedation and radiation, which also come with using the Embo ASSIST AI solution. However, his team will “continue to evaluate emerging AI tools to determine their value to patients”.
“There are many tools out there,” Brower explains, “but the question is does it bring value or is it just a flashy, ‘Hey, we can do this’, type of situation—it must bring value and then it must be applicable and reproducible.” Often performing liver-directed therapies such as Y90, Brower highlights the “highly reliable” Embo ASSIST AI, which has enabled his team to simplify procedural workflow and improve mapping via its three-dimensional (3D)-augmented image visualisation.
Facilitated by the software’s augmented imaging capabilities, Brower and his team are of the belief that AI will only “continue to improve and grow” as one of the “primary tenets” on opening their OBL.
Arnaud Marie
With this, Arnaud Marie, GE HealthCare CEO and general manager of interventional image-guided systems agrees, saying “nothing will be untouched by AI”. Speaking to Interventional News, Marie sets out the company’s three-fold intent with the development of Embo ASSIST AI. First, by enabling augmented imaging to support embolization strategy planning, the technology allows users to simulate injection points, visualising arterial details. Designed to automatically track vessel pathways to anticipate navigation challenges, Marie asserts that interventional radiologists can “[define] the impact of any decision they make, to decide what treatments are best and to guide them during procedures”.
“The second element is to drive workflow efficiency—how can we eliminate steps during procedures? How can we make it as simple and as intuitive as possible?” Marie expands that a key focus in developing the technology was to remove “unnecessary” procedural touchpoints or clicks. Embo ASSIST AI does this by exporting automatically segmented vessels and landmarks of potential embolization points for augmented 3D fusion guidance. Then, interventionists are able to overlay this information via live fluoroscopy on the frontal or lateral plane. Previously, several steps were necessary to segment vessels to remove pollution from the 3D model Marie describes. Now however, “there are no steps, there is almost nothing to do”, he says.
Marie then defines the third tenet that shaped the development of Embo ASSIST AI—to provide integrated patient care—and explains how the software brings together the “silos” which he states make up healthcare. By speeding up data consolidation, Marie hopes the AI technology can “link those different silos—from the doctor, the technician, the nurses—through information sharing, to revolutionise” the patient care pathway. Throughout this process, Marie states that the company’s overarching refrain was to ask: How can it be summarised? How can it be accelerated? “We are all patients, or have been patients,” he states. “We want interventionists to have access to the best data and tools.”
Embo ASSIST AI’s imaging potential is of central importance to Brower, who describes the “community benefit” patients in Spokane have gained when attending their OBL clinic and imaging centre, which is operated with their joint venture partner Providence Healthcare.
“As imaging volumes continue to grow and have increased from 6 to 9% just through organic growth over the past year, then spin off from just diagnostic, to interventional, OBL practice should mirror that,” Brower says, highlighting their ability to consult and treat patients more efficiently today.
“Change is not easy,” Marie comments, commending OBLs like Brower’s that are successfully modifying their practice while “demonstrating how Embo ASSIST AI may enable a reduction of procedural time for interventionists, enabling them to solve problems that could not previously be solved”. Brower believes that their OBL has “removed some of the politics”, creating a space where doctors from “any group, practice, or hospital setting can feel comfortable sending patients”. Although “biased”, Brower believes that they provide the “best patient care” in their market, working to ensure their “reputation and service stays intact—it all comes back to the patient”.
In light of increasing demands, Brower is in agreement with Marie, that “the simple fact is AI will continue to play a major role in what we do across the board, but particularly in imaging—I would imagine that the role of AI is only going to increase within our specialty”. Installing Embo ASSIST AI has been “pivotal” in getting their OBL to where it is now, Brower avers, “they have been fantastic, their equipment in my mind is exceptional—I am a firm believer that [OBL clinics] are the best way to treat patients”.
*Disclaimer: Jayson Brower is not a paid consultant for GE HealthCare. The statements made by Jayson Brower described here are based on his own opinions and on results that were achieved in his unique setting.
Embo ASSIST AI solution includes FlightPlan for embolization and requires AW workstation with Volume Viewer, Volume Viewer Innova, Vision 2, VesselIQ Xpress, Autobone Xpress. These applications are sold seperatley and may not be available in all countries.
A large, single-centre analysis has found that, despite parity between the two procedures in terms of perioperative clinical outcomes, carotid endarterectomy (CEA) was associated with a reduced rate of late stroke/death compared to transcarotid artery revascularisation (TCAR).
Writing in the Journal of Vascular Surgery (JVS), Ali AbuRahma (Charleston Area Medical Center/West Virginia University, Charleston, USA) and colleagues also conclude that CEA produced a marginally lower rate of restenosis ≥80% at two years—although this difference did not reach statistical significance.
The authors initially note that multiple registry studies—primarily ones conducted within the Society for Vascular Surgery’s (SVS) Vascular Quality Initiative (VQI)—have compared early outcomes, and outcomes up to one year, between TCAR, CEA and carotid artery stenting (CAS). However, no large, single-centre studies have reported on late clinical outcomes between these procedures and, as such, they conducted a retrospective analysis comparing intermediate outcomes with TCAR versus CEA.
Their study analysed data collected from the TCAR Surveillance Project on patients at the Charleston Area Medical Center, with these data being compared and subsequently propensity matched against patients undergoing CEA. Patients in both groups were treated by the same providers across the same time period, the authors note.
The primary outcome of the analysis was a combination of perioperative stroke/death and late stroke/death rates, while secondary outcomes included combined stroke/death/myocardial infarction (MI), cranial nerve injury (CNI), and bleeding. Kaplan-Meier analyses were used to estimate patients’ freedom from stroke, stroke/death, and also rates of restenosis ≥50% and ≥80%.
Across 637 patients, a total of 646 procedures (404 CEAs and 242 TCARs) were analysed, with AbuRahma and colleagues finding no significant differences in indications for carotid intervention between these two groups—although TCAR patients had more high-risk criteria including hypertension, coronary artery disease, congestive heart failure, and renal failure.
The authors report that there was no significant difference between CEA and TCAR in terms of the rates of 30-day perioperative stroke (1% vs. 2%, respectively), stroke/death (1% vs. 3%), or major haematoma (2% vs. 2%). However, the rate of early CNI was found to be significantly higher with CEA (5%) versus TCAR (1%; p=0.0138). In addition, late follow-up analyses at two years revealed results favouring CEA over TCAR, as the former produced lower rates of stroke (1% vs. 4%, respectively; p=0.0273), stroke/death (8% vs. 15%; p=0.008), and restenosis ≥80% (0.5% vs. 3%; p=0.0139).
AbuRahma and colleagues’ propensity-matched analysis, under which 242 CEAs and 242 TCARs were included, found broadly similar perioperative outcomes regarding stroke rate (CEA, 1% vs. TCAR, 2%), stroke/death rate (CEA, 2% vs. TCAR, 3%) and CNI rate (CEA, 3% vs. TCAR, 1%). Once again, however, their later follow-up analysis generally favoured CEA, as demonstrated by a rate of stroke of 1%—compared to 4% with TCAR (p=0.0615)—and a rate of stroke/death of 8%—compared to 15% with TCAR (p=0.0345).
Finally, the authors also note a marginally smaller difference in the occurrence of restenosis ≥80% following propensity matching, as compared to their regular analysis, with rates of 0.9% associated with CEA versus 3% with TCAR (p=0.099). This difference was not deemed statistically significant, they add, and rates of restenosis ≥50% were not statistically significantly different between the two procedures either.
“In propensity-matched analysis, both CEA and TCAR have similar perioperative clinical outcomes. However, CEA was superior to TCAR for the rates of late stroke/death and had somewhat lower rates of ≥80% restenosis at two years,” AbuRahma told NeuroNews, outlining the salient message from the paper. “The type of intervention, CEA versus TCAR, should depend on risk stratification—anatomical and/or physiological.”
Switzerland-based startup firm Nanoflex Robotics has announced that it recently installed its first remote-ready robotics system for neurovascular procedures at the Jacobs Institute (Buffalo, USA).
The Nanoflex Robotics system uses a compact magnetic field generator and a navigation control unit to guide ultra-flexible devices through the body for a range of complex vascular interventions, as per a company press release. This technology allows physicians to directly control, bend and guide the tip of the guidewire through the body’s vasculature, enabling them to conduct procedures “at the bedside, or thousands of miles away”.
The company’s first target application is to make remote mechanical thrombectomies a reality for acute ischaemic stroke patients, the release continues. By reducing the need for interhospital transfers, the hope is that this will shorten the time to reperfusion and potentially better preserve a patient’s quality of life.
“We are thrilled to collaborate with the esteemed Jacobs Institute in New York for the first installation of our robotics system,” said Matt Curran, chief executive officer of Nanoflex Robotics. “We believe remote robotics has the potential to transform surgical outcomes and benefit patients by enabling greater and earlier access to critical treatments.”
The company’s remote-ready robotics system will be enabled for usability testing, in-vivo studies, and training, at the Jacobs Institute. Furthermore, due to growing clinician interest in the system, it will also serve as a site for physician demonstrations, the release adds.
“Robotic neurovascular intervention is undoubtably the future. We are delighted to work with Nanoflex Robotics to prove this concept,” said Adnan Siddiqui (University at Buffalo, Buffalo, USA), chief executive officer and chief medical officer of the Jacobs Institute.
The installation of Nanoflex Robotics’ first remote robotics system comes shortly after the company received an ISO 13485 certification for its quality management system in designing and manufacturing remote robotic devices for endovascular interventions, the release also notes.
Riad Salem (Northwestern University, Chicago, USA) began by iterating that TACE will undoubtedly remain the global standard in terms of availability and feasibility. A better, “spicier” question, he posed, is what happens when both TACE and Y90 are widely available. “In reality TACE is already being replaced by Y90, based on curative data and therapeutic narratives,” Salem averred.
Despite his pro-Y90 position, Salem acknowledged that he is a “big fan” of TACE and has conducted the two largest TACE trials for hepatocellular carcinoma (HCC) in the USA—the first in 2010, and the second in 2016, evaluating response, toxicity and overall survival of TACE for HCC—alongside his mentor Michael Soulen (Abramson Cancer Center, Philadelphia, USA).
Yet, aside from his own contributions to the literature, Salem scrutinised the level of data that has solidified TACE in practice today, regarding the two seminal 2002 trials which found TACE to be beneficial in patients with limited disease and without portal vein thrombosis (PVT), when compared to no treatment in a small sample size randomised controlled trial (RCT). However, when compared to larger analyses of Y90, Salem highlighted that Y90 outperforms chemoembolization in four variables, namely: reproducibility/standardisation, precision, intentional threshold dosimetry, and clinical benefit.
A new narrative
Presenting data from individual cases of his colleagues and well-known trials to date, Salem attested to the “compelling” narrative that is being created by Y90, that provides high-risk patients with the same survival rates as low-risk patients, as well as improvements in quality-of-life measurements. “Who cares about quality of life?” he asked the audience. “Patients care about quality of life. They want to feel good, they want fewer treatments, they don’t want to feel sick”.
“You have the Swiss army knife of locoregional therapy. That’s the way I see it”, Salem continued, asserting that when reviewing the “scorecard”, Y90 far outperforms chemoembolization in areas such as downstaging, bridging, PVT management and immune therapies, but lacks the global accessibility of chemoembolization due to the greater infrastructure needs of a Y90 programme.
With a focus on patient experience, Salem wrapped up his presentation with a frank appeal to the “pragmatists” in the audience. He called to those that “actually have to talk to patients and manage humans” in the hopes that his argument has resonated, while acknowledging the “purists”, who must have had “little-to-no interest” in his point of view. To the latter he remarked “I wish you well and good luck”, but concluded that he is optimistic about how Y90— building upon what has been learned through TACE—is creating new treatment paradigms to improve cancer care.
Key trials backing TACE
Next, moderator Sarah White (Medical College of Wisconsin, Wauwatosa, USA) invited Soulen to the podium to “slap his mentee” and present in favour of TACE’s survival in the age of radioembolization and immunotherapy.
Michael Soulen
Sparing no time, Soulen prefaced his presentation with a direct response to this question, and remarked: “Hell yeah, [TACE] is still the only evidence-based treatment in the space for unresectable hepatocellular carcinoma [HCC]”. Yet he spoke of the lack of a comprehensive regulatory pathway for procedures and for medical devices, which enter clinical practice without compelling evidence. “This is the Achilles’ heel of interventional radiology [IR]” Soulen said, in contrast to the highly regulated phase 3 trials involving thousands of patients that must be carried out for anti-cancer drugs to gain approval.
Referencing new data however, Soulen contended that there are level 1 data indicating that TACE works and level 1 data that Y90 does not in unresectable disease; notably the RCT of TACE +/- brivanib which prospectively analysed >500 TACE patients, the Japanese-Korean cooperative group study of TACE for HCC, and the Precision Italia trials, all of which showed two to three-year median overall survival after TACE versus the universally negative RCT’s for TARE.
Yet, he maintained that Y90 does have a valuable role in a curative intent setting. Published in January 2024, he offered the updated analysis of the DOSISPHERE-01 trial which evaluated overall survival using Y90 microspheres in patients with inoperable locally advanced HCC. Principal investigator Etienne Garin (Rennes 2 University, Rennes, France) et al reported that, at long-term follow up, a meaningful improvement in overall survival was sustained after applying personalised dosimetry in patients who were successfully downstaged and resected, but consistent with prior studies that showed no survival benefit in unresectable patients.
Soulen then postulated on whether immunotherapy will change the landscape, considering the positive immunostimulatory effects of embolization using a large series of matched cohort studies from the 1970s concerning patients with Stage 4 renal cell carcinoma who had nephrectomy—“and there weren’t any good drugs back then”, he added.
Additionally, looking at the recent release of EMERALD-1 data, Soulen asserted that the benefits of combining of TACE and immunotherapy are apparent. “We now have data showing better outcomes with the combination— so where’s the data for radiation and immunomodulation?” Posing this rhetorical question in front of a slide that read ‘crickets chirping’, Soulen finalised his claim, acknowledging that there are trials coming in this area with much still yet to be learned.
Mechanistic data are crucial
Rony Avritscher
With a focus on immunotherapy, Rony Avritscher (MD Anderson Cancer Center, Houston, USA) spoke next, and first pointed out the lack of mechanistic data offered by Salem and Soulen. He noted that collecting standardised data for interventional oncology (IO) therapies is one of the “biggest challenges” interventional oncologists face, due to the complex nature of their procedures and equipment, as well as the specialists needed to a dminister treatments.
Without crucial mechanistic and therapy standardisation, scalability for IO procedures will continue to be an area of “struggle” Avritscher claimed, placing the field at a “disadvantage”. In order to make these gains, the speaker stated that the development of tools which include innovative technologies such as artificial intelligence (AI) should be sought, with the capability of prescribing dose for complex tumours.
Following Avritscher’s position on gaining better data, the panel were then invited to discuss; Salem first stated that new ways of collecting meaningful analyses must be devised, as RCTs—although ideal—are not constructive or representative of most of the procedures carried out in clinics. Developing this point, Soulen reiterated the difficulty they face in gaining data for both devices and drugs, and how making headway with the former is one of the “biggest challenge[s] in IR”. “We have no data because our devices don’t have to have data to be sold, and the companies won’t pay for trials because they don’t have to”.
With the information they have now, Soulen added, there will never have been a situation where TARE will replace TACE. As every patient is fundamentally different, individualised treatment is key. “It’s not a black and white decision in everyday life,” he contended, “there are other clinical factors besides their cancer and you’re going to initialise your care using whichever tool in your toolbox is suited to that so that [the patient] can have the best quality of life and outcomes can be improved”.
Avritscher added that even different types of embolization procedures have “fundamentally different” effects on the human body which the community must seek to understand in order to pinpoint which patients would benefit from what combination of agents to specialise their care. Avritscher averred however that the only way this can be achieved on IO’s “turf” is to invest in basic science and translational studies looking at patient subsets and their molecular profiles.
The three speakers agreed that every treatment option to their disposal is valuable. To Soulen, these options give patients agency to select a route that best suits them in terms of quality of life: “TACE is quick and sick, Y90 is slow and glow. They work similarly well and some patients want the slow, gentle route, because they don’t want to be sick, but others say ‘No, I want this tumour dead tomorrow’ and will tolerate the subsequent sickness.”
Wrapping up, White asked the room to raise their hands if their institution offers and performs TACE or Y90, showing a visibly divided audience. Of the panel’s most salient conclusory points, consensus on TACE versus TARE may never be reached for good reason, so that case-by-case the most applicable treatment can be deployed for individual patient needs. Reaching agreement on this, Salem resolved that rather than focus being placed on one winning out over the other, attention should be paid to the new narrative that is being created by Y90 that is crucially expanding the dialogue for IO treatment.
In a roundtable dedicated to comparing training pathways for interventional radiology (IR) in Saudi Arabia, the Middle East and North Africa (MENA), Europe and North America, discussion levelled on the challenges faced by many and heard first-hand experiences of trainees around the globe.
Presenting first on the Sunday of the Pan Arab Interventional Radiology (PAIRS) annual congress (10–13 February, 2024, Dubai, United Arab Emirates), Raman Uberoi (The John Radcliffe Hospital, Oxford, UK) elaborated that interventional radiologists are image-guided surgeons, and on the critical nature of IR assessment worldwide. He noted that in the past, interventional radiologists have no or very minimal exposure to IR in the early years of their training, and have no formal assessment in the quality of training they receive to confirm that they have achieved basic core competencies in IR. “Patients would be shocked if surgeons had no assessment in place to prove their core skills.”
In Europe, Uberoi’s work with the European Board of Interventional Radiology (EBIR) to consolidate a comprehensive examination for training IRs was aimed at “evolving the way [interventional radiologists] work and train, focusing on the critical core skills that future interventionists will need”.
Abdulkader Alkenawi (King Abdulaziz Medical City, Jeddah, Saudi Arabia) explained that the bodies which determine the IR curriculum and examination are entirely separate in Saudi Arabia, but the parties frequently come together to ensure what trainees are being taught aligns with their assessment.
Although important, assessment can only take trainees so far, one audience member stated. He provided that his centre in Jordan sees very limited numbers of complex cases, and queried whether trainees would be accepted to facilities such as Alkenawi’s so that they may gain exposure to a broader range of pathologies. To this, Alkenawi explained that due to Visa constraints and a consistently significant workload for their small IR team this is not yet a possibility, but hopes that in the future they may begin accepting trainees from other countries.
Mamoon H Al-Omari (King Abdullah University Hospital, Ar Ramtha, Jordan) then went on to describe how IR is still yet to be included within diagnostic radiology (DR) training today. At his hospital, those who are interested in IR can take one to two months elective training; however, he stressed the lack of exposure to IR for most trainees generally.
Sparking contention, attendees and speakers turned to IR’s position within the house of DR. Saher Sabri (MedStar Georgetown University Hospital, Washington, DC, USA) asked the audience whether an IR-only residency would be attractive, including one/ two years IR training and a year or so training in DR, but would certify trainees in IR alone.
Taking stock of hands raised, Sabri concluded that most would prefer dual certification and when asked why, an audience member said that this is beneficial as trainees would have something to show for the significant portion of time spent training in DR.
Another audience member opined however, that if IR was selected from the off, there would be more dedicated interventional radiologists who could create better recognition for the specialty. They stated that maintaining a qualification in DR when training in IR acts as a ‘safety net’, enabling trainees to have a field to fall back on, negatively affecting the growth of IR. Yet, another audience member viewed the ‘plan B’ quality of dual certification as positive, and explained that with limited jobs in the MENA region, having the ability to do both DR and IR procedures places interventionists in a better position to secure a place in a competitive job market.
“It’s not an easy path doing IR,” Alkenawi said, airing his concerns that IR has lost “too many battles” with other specialties to date, which Uberoi consolidated, noting the difficulties interventionists can encounter if they are “at the whim” of referring specialities. Sabri, however, in attempts to “uplift a little bit”, brought the discussion back to the positive practice models that are already in action for many centres, to which Alkenawi agreed that IR as a field has shown its capability to adapt to challenges.
Uberoi concluded that “the future is bright, but we must think in a radically different way. The next generation can hold the future of IR in their hands, which will mean [they] must grapple with these issues now, talk to [their] trainers and develop [themselves].”
Alda Tam is an interventional radiologist and professor at the University of Texas MD Anderson Cancer Center in Houston, USA, and is current president for the Society of Interventional Radiology (SIR). As an active and prolific researcher, Tam speaks to Interventional News about the trajectory of her career, maintaining her practice alongside her involvement with clinical trials, her development of clinical practice guidelines and more recent app development.
What attracted you to a career in interventional radiology (IR)?
Third year medical school came with the task of having to choose a future career and I had to decide whether I would be more interested in using my hands and operating (surgical specialty) or seeing patients and engaging in cerebral work (medical specialty). With an undergraduate degree in neuroscience and leaning towards surgery, I thought about neurosurgery and signed up for a summer research internship, complete with shadowing in the operating room. During one of the cases, I remember seeing brain tissue in the Yankauer suction and tubing and thought “I don’t know about this…maybe there’s something out there with more finesse?” During my radiology rotation, one of the faculty suggested I check out IR since they knew my affinity for surgery. It only took a few assignments in the IR suite to realise this was it for me; the complexities of surgery with the finesse I desired. That’s how I ended up entering the field.
Who were your mentors?
I completed my radiology residency at the University of Southern California (USC) and had an awesome team of IR mentors: Sue Hanks, Vicki Marx, Michael Katz (all Keck Medicine of USC, Los Angeles, USA), and Donald Harrell (Mammoth Hospital, Mammoth Lakes, USA). I witnessed a high-functioning team delivering top notch care while having fun doing so, and thought that I could see myself in a career like that. During my fellowship at MD Anderson, I continued to find guidance from Marshall Hicks, Michael Wallace, Sanjay Gupta, and Steve McRae (all University of Texas MD Anderson Cancer Center, Housten, USA). They gave me my first job, and the rest is history. As my network has grown over time, there are many colleagues, friends, and peers—too many to name—who I continue to rely on for counsel and support. I only hope that I can serve in a similar manner to future interventional radiologists.
What led you to oncology? Was it always your intention to specialise there?
Becoming an interventional oncologist was pure serendipity! My husband is a medical oncologist and the years of training for internal medicine/oncology and radiology were not perfectly aligned. He was matched to Houston first and I joined him there after finishing my final year at USC. But I then finished my fellowship first and started my faculty position at MD Anderson while he was in his last year of training. Then we both ended up staying and we’ve been Houstonians for almost 20 years.
Could you describe a particularly memorable case of yours?
I’ll always remember my first case as a solo operator. I was the second year resident on-call and had been given the go-ahead to start the case by my attending, who was finishing up in the other room. Although it is what most interventional radiologists would consider a bread and butter case—a 65-year-old man in urosepsis, complete with hypotension and tachycardia, from ureteral obstruction related to stone disease, needing a nephrostomy tube—it was definitely an exciting yet nerve racking moment for me because once the patient was prepped and draped, we got word that there had been a hold up in the other room and my attending said, “start if you feel comfortable but if not, you can wait”. In all honesty, I would have preferred to wait, but the patient’s vital signs were not good and getting worse, so I made the decision to act and put in the nephrostomy tube. I will never forget the support of the seasoned radiologist technologist and nurse team who encouraged me and got me through the case. The patient defervesced after the pus in the collecting system was drained, was discharged out of the intensive care unit to a regular floor, and then subsequently home. As I realised what could be done with a needle and wire, this case became one of the moments that cemented my decision to specialise in IR.
What are some of the challenges which face interventional radiologists providing cancer treatment today?
Awareness and access. We continue to face the challenge of physicians and patients being unaware of the value IR can add to oncology care across the spectrum of diagnosis, local treatment, and palliation. That’s why it is key for us to emphasise the importance of IR research and IR-driven clinical trials to obtain the data that will permit the inclusion of our therapies into treatment guidelines. This would ensure that patients can be presented with all the available treatment options. We also have a challenge with patient access to IR. In the USA, approximately 30% of the country’s population do not have access to an interventional radiologist in their state (Ahmad Y et al). When you scale this concept, I suspect that there are many cancer patients globally who could benefit from the treatments that IR has to offer, if only their access to IR care could be improved.
Your largest body of work regards biopsies in oncology clinical trials. How important is biopsy acquisition?
This body of research has led to efforts to standardise biopsy acquisition within the National Cancer Institute Clinical Trials Network (ETCTN). The difference between a biopsy for clinical care and a biopsy for research purposes is that oftentimes, a patient enrolled in a clinical trial that requires a research biopsy that may derive no direct benefit. Working at MD Anderson in the mid-2000s, we began to see an increase in the number of clinical trials that were incorporating research biopsies into their trial design and also realised that more tissue was usually needed to meet the goals of a research biopsy. This naturally brought up questions about how to optimise biopsy yield to inform trial endpoints while at the same time protecting patients from undue adverse events. Our collaborative group of medical oncologists, pathologists, and interventional radiologists at MD Anderson have performed research in this area.
In one early study, we examined transparency, meaning how the risks and adverse events associated with biopsies in clinical trials are discussed within informed consent. We reviewed the IR database to identify all therapeutic clinical trials in which image-guided research biopsies were performed from 1 January, 2005, to 1 October, 2010. Among 57 clinical trials, 67% contained at least one mandatory biopsy. Most of the studies failed to convey the risks and benefits of research biopsies in study protocol and informed consent. We also evaluated how often the biopsy results of clinical trials are reported. We searched ClinicalTrials.gov for trials in oncology with completion dates between 1 January, 2000, and 1 January, 2015, with endpoint category terms including biopsy, biopsies, or tissue.
Among 301 trials, only 50.8% reported any biopsy-related results. In a similar analysis of 866 research biopsies performed across 46 clinical trials, 61% of trials did not report results from research biopsies. From an ethics perspective, questions arose about subjecting patients to unnecessary procedures with limited scientific gain and so the American Society of Clinical Oncology (ASCO) put together an ethical framework regarding the inclusion of biopsies in clinical trials. The ethical framework addresses three main areas: how to maximise the scientific utility associated with biopsies, how to minimise the participant risk, and how to improve oversight of the process. To help patients and clinical trialists determine whether a research biopsy fulfils the goal of having an overall favourable risk-benefit ratio—and therefore meets ethical justification—the framework explicitly defines the scientific contribution to be expected from a biopsy, categorises participant risk, and outlines when mandatory biopsy may be justified. As a result, the research led to the adoption of standard operation procedures for biopsy acquisition within the National Cancer Institute Clinical Trials Network (ETCTN). The idea is that by providing “best practice” guidance, we will minimise the number of patients who undergo unnecessary or non-diagnostic research biopsies as part of their participation in a clinical trial.
What do you hope to achieve as SIR president?
As SIR is a big organisation, I think it’s important that the president not necessarily have a personal agenda but rather, that the executive leadership works cohesively towards multi-year strategies that will drive forward initiatives for the society and specialty. As we begin to celebrate 50 years as a society in 2024, many of the initiatives in the past several years have been focused on establishing a foundation to allow us to be able to compete as a primary medical specialty. Examples of this include the integration of the clinical specialty councils into the governance structure which allows for the voices of our key opinion leaders to be heard and participate in strategic decision-making; the variety of educational products, including the launch of SIR Edge, a new fall 2024 meeting offering; and the ongoing website and user digital experience update. I hope by the end of my time in leadership, I will have contributed to significant infrastructure changes that will set IR and SIR up for success in the coming years.
“We continue to face the challenge of physicians and patients being unaware of the value IR can add to oncology care across the spectrum.”
What was the rationale behind the creation of the SIR Guidelines app?
I became the standards division counsellor for the SIR in 2017, which is how I got involved in the creation of clinical practice guidelines. I’m really proud of the work that committee achieved because, together, we moved the Society to develop the National Academy of Medicine—compliant clinical practice guidelines—and SIR may very well be the first radiology society in the world to do so. This is tremendously important because we’re still jockeying for position on where IR falls in medical treatment algorithms and the acceptance of IR therapies. For us to be viewed as legitimate and competitive as a primary specialty, we needed to put our data through the same methodological scrutiny that is considered the industry gold standard. This was a big step for us in terms of the maturation of the Society and the specialty.
Our first clinical practice guideline was on inferior vena cava filters in the treatment of patients with venous thromboembolic disease. When you read this guideline, you’ll see that it’s different in the sense that it’s question-based with a literature search specific to that question and provides a recommendation that weighs out benefit and harm. Leading the Guidelines Committee was a professional and personal growth experience for me and one of the most rewarding leadership/volunteering experiences I’ve had.
I was also able to work with residents from University of California San Diego, San Diego, USA and some of our early career section members to develop and launch the SIR Guidelines mobile app, which is now used worldwide.We have been downloaded in more than 130 countries and have over 17.5K users! The app gives clinicians point of care access to periprocedural anticoagulation and antibiotic management recommendations for each IR procedure. It returns the information a clinician needs to make a decision in about eight seconds. Ultimately, the guidelines app helps to disseminate information for practice guidance and can help with the adoption and adherence to evidenced-based recommendations.
What are your hobbies and interests outside of medicine?
I enjoy spending time with my family and travelling. We have been to many national parks and we like to hike—some of our more memorable hikes have been Angel’s Landing (Zion National Park) and Half Dome (Yosemite National Park). We are off to Banff this summer. I also like to read, particularly Japanese and Scandinavian murder mysteries, and continue to think about completing another half marathon.
FastWave Medical, a clinical-stage medical device company developing intravascular lithotripsy (IVL) technology, has announced the issuance of its third utility patent by the United States Patent and Trademark Office (USPTO).
The newly granted patent supports the differentiated design of FastWave’s next-generation IVL system, which aims to address challenges associated with treating calcified arteries in patients with occlusive vascular disease, a condition affecting millions of people worldwide. By developing advanced lithotripsy platforms, FastWave aims to solve the gaps with existing IVL technology while improving ease of use and patient safety by reducing procedural complications.
Silk Road Medical has announced the launch of its tapered Enroute transcarotid stent system to hospitals in the USA, expanding upon the company’s prior Enroute transcarotid stent system and offering additional configurations to better tailor the transcarotid artery revascularisation (TCAR) procedure to patient anatomy.
“The new tapered stent is a welcome addition to my TCAR toolkit, further differentiating the company’s core product offering,” said Joseph Lombardi (Cooper University Health Care, Camden, USA). “The Enroute stent has always provided comprehensive lesion coverage and durable procedural outcomes, but I now have more options to customise treatment to each patient’s anatomy.”
“As pioneers in stroke prevention, our product development efforts are focused on extending our lead in the minimally invasive treatment of carotid artery disease,” said Chas McKhann, chief executive officer of Silk Road. “New tapered configurations for our Enroute transcarotid stent system build upon the robust portfolio of Silk Road’s carotid solutions. We are pleased to bring this portfolio expansion to market as part of our commitment to offering a diverse toolkit for physicians, allowing them to address individual patient anatomy.”
TCAR is a minimally invasive surgical procedure designed to provide best-in-class stroke protection while minimising adverse events in patients requiring treatment for carotid artery stenosis.
The Enroute transcarotid stent system is the only commercially available transcarotid stent system indicated for patients at high risk and standard risk for adverse events from carotid endarterectomy (CEA), as per a Silk Road press release. It features an optimised cell design balancing lesion coverage and anatomical conformability for long-term plaque stabilisation—and was purpose-built for TCAR, with a short delivery system for ergonomic and precise stent delivery.
The Society of Interventional Oncology (SIO) announces the European Institute of Oncology (IEO) in Milan, Italy, as the next European site approved for enrolment and activated for the society’s primary clinical trial, Ablation with Confirmation of Colorectal Liver Metastases (ACCLAIM) prospective trial for microwave ablation as a local cure.
Principal investigator at the study site, Franco Orsi and co-investigator Paolo Della Vigna were recently approved as the eighth site overall, and third European site, activated in the ACCLAIM trial.
In this multicentre, international trial, SIO proposes to establish microwave ablation (MWA) as the preferred treatment option for selected colorectal liver metastases that can be ablated with sufficient margins. The study is the first global, prospective trial to use an objective and reproducible technical outcome in its study design, which SIO believes will drive important changes to future treatment guidelines.
The study will incorporate software to assess the ablation zone and margins and determine if achieving complete margins during an ablation equates to procedural success, where the primary outcome is local disease progression at two-years post-ablation.
Constantinos T Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA) is the global principal investigator for the study. “We are excited and pleased to share the opening of Orsi’s site,” said Sofocleous. “We look forward to announcing our remaining sites in Europe as they are approved for enrolment to begin.”
Participants of the ACCLAIM trial will be patients with a diagnosis of colorectal cancer liver metastases. MWA will be performed using an FDA-cleared, commercially available MWA system and using margin confirmation (visualisation) software. Upon its launch, the ACCLAIM study is expected to have a three year enrolment period with 330 tumours treated (approximately 275 subjects) across ten sites in the US and Europe.
This trial is funded collectively through grants from Boston Scientific, NeuWave Medical, Varian, and Siemens Healthineers.
BD has announced the enrolment of the first patient in the AGILITY investigational device exemption (IDE) study, which will assess the safety and effectiveness of the BD vascular covered stent for the treatment of peripheral arterial disease (PAD).
The investigational vascular covered stent is a self-expanding, low-profile, polytetrafluoroethylene encapsulated nitinol implant. It is deployed from a delivery system that provides controlled stent release.
“When we’re addressing advanced PAD, a self-expanding covered stent can play an important role,” said Sean Lyden (Cleveland Clinic, Cleveland, USA) national principal investigator of the study. “We need a stent that can track to the lesion, opposes the vessel wall and ultimately provides long-term durability. We’re excited to see how this technology performs.”
According to BD, the global, prospective, multicentre, single-arm, non-randomised AGILITY clinical study will include 315 patients at up to 40 clinical study sites across the USA, Europe, Australia and New Zealand. Follow-up for all treated patients will be performed at various points after treatment—starting at one month and ending at 36 months.
“There continues to be significant unmet needs in the treatment of PAD patients,” said Tim Hug, vice president and general manager at BD Peripheral Intervention. “We are excited to have initiated this study and evaluate the treatment benefits of this potentially differentiated technology. This stent could give interventionalists an important new solution in the fight against PAD, expand our portfolio and enable us to better serve our customers and the patients they treat.”
The first patient in the AGILITY study was enrolled at Trinity Medical Center in Bettendorf, USA by Nicolas Shammas, interventional cardiologist and founder and president of the Midwest Cardiovascular Research Foundation.
Shape Memory Medical has announced that it has completed $38 million in Series C financing, which has been led by Earlybird Venture Capital, along with participation from both new and existing investors.
Shape Memory stated in a press release that its proprietary shape memory polymer is a low-density, porous embolic material that is crimped for catheter delivery. According to this press release, it is also self-expanding upon contact with blood for rapid conversion to organised thrombus. It is the company’s hope that this new technology will offer unique properties, including vascular space-filling, radiolucency, low radial force, and stimulation of the immune response and healing system.
Shape Memory also recently announced that the US Food and Drug Administration (FDA) granted the company an investigational device exemption (IDE), which will allow it to begin a prospective, multicentre, randomised, open-label trial to determine the safety and effectiveness of the Impede-FX RapidFill device in improving abdominal aortic aneurysm (AAA) sac behaviour, when used with elective endovascular aneurysm repair (EVAR).
Ted Ruppel, chief executive officer and president of Shape Memory Medical said that “with this financing, we are well positioned to accelerate the clinical and market development of shape memory polymer technology for aortic and peripheral vascular markets”. Ruppel continued, adding that “the funds will support the execution of the AAA-SHAPE pivotal trial, a randomised controlled study comparing EVAR plus sac management with Impede-FX RapidFill to stand-alone EVAR. The funding will also support the research and development of our product pipeline, and the expansion of sales and marketing strategies to address the increasing demand for our commercially available Impede embolisation plug family of devices”.
Thom Rasche, partner at Earlybird Venture Capital and Shape Memory Medical board member added to Ruppel’s statement, commenting that “Shape Memory Medical’s approach to embolisation is highly differentiated. At Earlybird Health, we support companies with breakthrough technologies and robust, positive patient outcomes. With 35 million people worldwide affected by AAA, leading to 150,000–200,000 annual deaths due to rupture, Shape Memory Medical’s innovative concepts for managing aortic aneurysms have the potential to be transformative in treating this condition.”
A recent study published in the journal CardioVascular and Interventional Radiology has found conservative management may be efficacious in patients with spontaneous retroperitoneal haemorrhage (SRH), with added variable success seen after embolization in a more unstable patient group.
The single-centre retrospective case-control study of patients with SRH included patients who were treated conservatively or with embolization. Enrolled patients aged ≥18 years were identified from computed-tomography (CT) imaging reports which stated a diagnosis of SRH or similar, with images reviewed for confirmation. Exclusion criteria were outlined as recent trauma, surgery, retroperitoneal vascular line insertion and other non-spontaneous aetiology.
Corresponding author Warren Clements (The Alfred Hospital, Melbourne, Australia) and colleagues identified a total of 54 patients who were predominantly anticoagulated (74%), male (72%), older adults (mean age of 69 years), with active haemorrhage on CT-scan (52%).
Overall mortality in this patient cohort was 15%, however clinical success was more likely with conservative management over embolization; all-cause, uncontrolled primary bleeding mortality was higher with embolization. However, embolized patients more commonly had active bleeding, shock, and higher blood transfusion volumes.
In their discussion of the results, Clements et al. note that, while most patients treated conservatively were haemodynamically stable, conservative treatment was successful in 13.2% of unstable groups, 100% of whom were taking therapeutic anticoagulants.
“These findings suggest that embolization in SRH may be best reserved for patients with ongoing bleeding despite adequate reversal of anticoagulation agents, or patients who were not anticoagulated to begin with and are haemodynamically unstable,” the authors state.
Of their study’s limitations, the investigators note that their groups were not congruent—embolized patients were more likely to have been unstable and/or have received high blood resuscitation volume, and were not matched even after propensity score matching, particularly regarding blood transfusion volume. Furthermore, they add that underlying coagulopathy, which has been shown to develop in the setting of major blood loss, likely contributed to the lower success rate in the embolization group.
They also underline that patients with SRH are typically older adults who come with a broader range of significant comorbidities. Due to this, Clements et al add that it can often be difficult to determine a precise cause of death, which perhaps explains variations in mortality attributable to SRH in contemporary published literature.
Although more research is needed in this area to confirm the effectiveness of conservative management of SRH, the authors highlight that their results—alongside the findings of other recent studies—show that mortality in SRH is high, and goals of treatment should include addressing the coagulopathy, and not just arrest of haemorrhage, in this patient population.
Endologix has announced the initiation of the Percutaneous transmural arterial bypass (PTAB)1 postmarket study. This study marks the beginning of a comprehensive postmarket study aimed at evaluating the real-world performance of the Detour system in patients undergoing treatment for long complex superficial femoral artery (SFA) disease.
The study will leverage the Vascular Quality Initiative (VQI) registry infrastructure developed and supported by the Society for Vascular Surgery Patient Safety Organization (SVS PSO), a company press release notes.
The PTAB1 postmarket study evaluates the Detour system’s performance in patients with very long (TASC D) SFA lesions. The study plans to enrol up to 450 patients, with a focus on including at least 200 women and also features an imaging substudy. Recruitment will involve up to 200 sites, with five-year follow-up.
“The initiation of the PTAB1 postmarket study represents a pivotal moment in our ongoing commitment to advance the treatment of complex peripheral arterial disease [PAD]. Through this study, we aim to further validate the Detour system’s innovative approach to overcoming complex PAD challenges,” expressed Matt Thompson, president and CEO of Endologix.
Thomas Maldonado
Thomas S Maldonado, the Schwartz-Buckley endowed professor of surgery in the Vascular Division at New York University Langone Medical Center (New York City, USA), underscored the significance of being the inaugural site to enrol a PTAB patient: “Our privilege of enrolling the first patient in the PTAB1 postmarket study underscores our commitment to advancing patient care in complex PAD. The Detour system offers a glimpse into a future where minimally invasive treatments could redefine our approach to extensive SFA lesions. We are optimistic about the contributions this study will make towards evolving patient treatment paradigms.”
In the final months of 2023, the Addenbrooke Hospital in Cambridge, UK, were reported as the first UK National Health Service (NHS) facility to deploy artificial intelligence (AI) during thermal ablation of liver tumours. Speaking to Interventional News, consultant radiologist Nadeem Shaida shares how the technology has enabled his team to bypass the “Achilles’ heel of liver tumour ablation” and treat tumours with better precision to ultimately reduce recurrence.
IN: The Addenbrooke Charitable Trust supporters donated the £200,000 thermal ablation machine to your hospital—how did this come about?
Liver ablation as a treatment option has grown in popularity following its incorporation into all major national and international guidelines for treatment of liver cancers such as cellular carcinomas, or hepatocellular carcinoma (HCC), but also for tumours that have spread to the liver from elsewhere, typically the colon.
We’ve been doing liver ablation here for many years—coming on 20 years in fact. Over this period, we found that demand for our services continued to rise, and we were being increasingly asked to do cases that we couldn’t do with our conventional means either via ultrasound or with a free-hand computed-tomography (CT) scan to guide the needle. This was due to poor image quality and/or obscuration of the tumour because of its location.
We had to find a solution because liver ablation works very well, and in looking for one we came across navigation. Essentially, navigation segments the tumour via markers on the skin which guides the needle. With this it became easy to do the cases we previously couldn’t such as high lesions near the dome of the liver.
IN: How has the addition of AI changed your practice?
It has helped us get around the Achilles’ heel of liver ablation. If you follow these patients up long enough, quite a number of them will recur and this is mainly because you haven’t ablated all of the tumour in the first sitting. To prevent this, you have to ablate the tumour, but also a safety margin around the tumour, which is where AI comes in.
AI has increased the accuracy of tumour segmentation, meaning patients are much more likely to be rid of the entire tumour in the first instance and have no chance of recurrence. Evidence for this is still emerging however, but there are promising data already which suggest AI-driven segmentation leads to better outcomes and lower recurrence rates.
IN: Are there any drawbacks to the use of AI technology to ablate liver tumours?
Yes. Quite often with AI segmentation it will tell you that you probably haven’t burned enough, and this can be quite a leap of faith for an operator, particularly if they’ve come from an ultrasound background where they put the needle in, burn, fire and forget. We need to see clinical data validating how accurate post-ablation measurements are when using AI and whether following these leads to improvements in long-term survival.
IN: In your opinion, what will the trajectory of AI look like within interventional radiology of the near future?
Ours is a technology-driven industry and we’re seeing a symbiosis between AI and systems we currently use through innovations in stereotactic navigation and robotics. So, I expect to see that develop and come to fruition—which we have already seen in some regards.
Expect to start seeing technology suggest to you, rather than you picking, the trajectory at the beginning of a case. AI won’t however eclipse the human element of healthcare and radiology, which is to understand the clinical processes and patient factors. Although when you look at HCC, with the variety of treatment options—embolization, radioembolization, chemoembolization, surgery, drugs, ablation—I do think in the future we may see patient selection become more driven by AI.
TriSalus Life Sciences, an oncology company integrating delivery technology with immunotherapy in the treatment of patients with liver and pancreatic tumours, today announced the publication in Current Medical Research and Opinion—a manuscript detailing a real-world study of the use of the pressure-enabled drug delivery (PEDD) method with the TriNav device for transarterial chemoembolization (TACE) and transarterial radioembolization (TARE) in patients with hepatocellular carcinoma (HCC) and liver metastases.
The data presented in this study captured real-world safety and clinical outcomes data for TriNav in its launch phase, utilising a large, 300 million patient dataset covering 98% of payers in the US. These data provide valuable insights into the important benefits of this technology that would otherwise take many years to accumulate through alternative approaches using clinical trials. Key findings include that TriNav patients, despite a higher baseline disease burden and clinical complexity, showed overall clinical results comparable to patients with lower disease burden.
The study also revealed that, in TACE procedures, interventional radiologists could deliver more of the chemotherapeutic agent to the tumour when using TriNav vs. the amount delivered using standard catheters, a critical treatment goal. In a matched cohort comparison, TriNav patients had fewer 30-day inpatient visits post-procedure, than non-TriNav patients.
TriNav HCC patients were more likely to have a post-procedure liver transplant in a matched cohort comparison. TriNav TARE patients with liver metastases had fewer clinical complications post-procedure vs. non-TriNav patients in a matched cohort comparison. Additionally, TriNav TARE patients with liver metastases had lower rates of post-procedure fatigue vs. non-TriNav patients.
These study data demonstrate that TriNav is preferentially selected to treat patients with a higher burden of disease than patients treated with standard catheters, yet these patients show similar results post-treatment compared to patients with a lower disease burden. TriNav patients showed trends toward better outcomes in matched cohort comparisons, including an increased rate of liver transplants.
“Analyses of real-world data are critical to obtaining a holistic understanding of the benefits of treatment with TriNav. The ability of the PEDD method to impact more complex patients when compared to standard-of-care drug delivery systems is potentially game-changing and brings us closer to addressing the limitations of current treatment options for HCC and other liver cancer patients,” said Mary Szela, chief executive officer of TriSalus.
“This important, peer-reviewed, real-world study speaks to our commitment to improve patient care and outcomes. These data, together with the recent, new Centers for Medicare and Medicaid (CMS) Healthcare Common Procedure Coding System (HCPCS) code effective as of this year, are a testament to TriNav’s continued emergence as a potentially best-in-class and cost-effective drug delivery method for patients with liver and pancreatic tumours.”
“These new population-based findings resonate well with previously published clinical studies that indicate PEDD improves therapeutic uptake, accuracy of therapeutic delivery, and clinical outcomes in liver cancer patients. The ability of the TriNav’s SmartValve to favourably modulate drug delivery pressure and flow within target blood vessels gives liver cancer patients, even those with major medical comorbidities and large tumour burdens, the opportunity to achieve better outcomes,” said Steven C Katz, chief medical officer at TriSalus. “This large sample size study underscores the particular benefits of the TriNav device compared to standard drug delivery systems.”
Royal Philips has announced the launch of their image-guided therapy mobile C-arm system 9000—Zenition 90 Motorized, designed to help surgeons deliver high-quality care to more patients at the European Congress of Radiology (ECR) annual meeting (February 28–3 March, 2024, Vienna, Austria).
The new mobile C-arm with expanded capabilities is designed to meet complex vascular needs and a range of clinical procedures such as cardiac interventions, pain management and urology. Zenition 90 Motorized will be commercially available from the second quarter of 2024.
In a recent press release, Philips has stated that the Zenition 90 Motorized is an intuitive C-arm that allows the surgeon to control it from the table-side with user-friendly controls and time-saving features, giving surgeons greater flexibility and independence. It delivers state-of-the-art image quality for the most challenging procedures and is designed to meet complex vascular needs. The system allows greater clinical efficiency thanks to its automated workflows, the image controls via the Touch Screen Module and the advanced software solutions.
“During complex procedures, it’s vital to be able to rely on surgical imaging systems. As surgeons navigate their way through challenging vasculature, the priority is to quickly visualise small anatomical details while limiting contrast use and X-ray dose,” said Mark Stoffels, business leader Philips image-guided therapy systems. “The new Zenition 90 Motorized empowers medical teams to confidently perform a wide range of interventions while achieving the best possible outcome for their patients.”
The launch of the Zenition 90 Motorized follows the recent launch of the Philips Zenition 30 C-arm, and is the latest device in the renewed portfolio of the company’s Zenition C-arm systems.
Philips have added that data collected from usability studies from clinicians in Europe and the USA show that the Zenition 90 Motorized performs beneficially in simulated environments. Their results showed that 100% of users found that, with the table side operator function, they have complete control over C-arm movements, and 97% reported that workflow features such as automatic vascular outlining will help save time during procedures.
As part of its stated commitment to sustainability and providing customers with responsible choices, Philips has also leveraged its EcoDesign process for the Zenition 90 Motorized to improve product life by 25% and power efficiency by 13%.
Fujifilm is set to unveil new mammography technology, Amulet Sophinity, at the European Congress of Radiology (ECR) annual meeting (February 28–3 March, 2024, Vienna, Austria). This technology aims at improving accuracy and ease in the diagnosis of breast cancer and offers patient comfort without reducing image quality, a press release states.
Amulet Sophinity is a digital mammography system that offers low dose, high-image quality, and improved workflow with artificial intelligence (AI) technology. The technology uses a pixel size of 50 µm and supports dual angle tomosynthesis with an improved sharp image reconstruction for better calcification, providing images focused on structures, further facilitating observation of lesions that are difficult to detect due to overlapping mammary gland structures.
Furthermore, the Amulet Sophinity digital mammography system is equipped with the projection function using AI, which can map the skin lines and nipple positions extracted from the previous mammography image. These are then projected onto the table surface as a guide to the same positioning as in the previous mammography image. This allows the radiographer to position the breast with reference to the projected skin line and nipple position, making it possible to take images that can be compared with previous images.
In addition, the design and functions are designed to be gentle to the examinee. The curved shape that conforms to the shape of the body is provided in the front of the detector to relieve tightness during examinations, and the Comfort Comp automatic pressure reduction control function, which aims to reduce pain during breast compression, is provided as standard, the press release describes.
Last year, Fujifilm Europe announced the separation of its medical systems from the wider imaging and materials business and merging it with its Fujifilm Healthcare Europe entity (former Hitachi Medical Systems Europe) to focus on providing med-tech solutions.
Masaharu Fukumoto, Managing Director, Fujifilm Healthcare Europe, said: “We’re delighted to be launching the Amulet Sophinity digital mammography system at ECR 2024, where we are showcasing our pioneering, comprehensive and innovative med-tech solutions. Amulet Sophinity digital mammography system is not just a product, it’s a platform that will house all mammographic techniques in one place. This is the first chapter of the new platform, which can ensure that patients have the clarity of confidence in their diagnosis”
Cook Medical, a global medical device manufacturer, has partnered with Bedal International, a company specialising in catheter securement devices marketed under the brand FlexGRIP. FlexGRIP devices are now available as an addition to Cook’s portfolio of percutaneous drainage products to improve patient comfort and experience during treatment.
As a result of the collaboration, FlexGRIP catheter securement devices are now available to Cook customers in Europe, Canada and the USA. Using this device helps to reduce the risk of dislodgement, infection and kinking of the catheter. Bedal’s proprietary air-pillow technology ensures secure catheter stabilisation in addition to comfort and ease of use and allows the patient more freedom of movement.
Alexander Van Damme, CEO of Bedal International, expressed excitement about the partnership, stating: “We are thrilled to partner with Cook Medical to bring the FlexGRIP catheter securement device worldwide. This collaboration represents a synergistic union of expertise, innovation, and commitment to advancing medical solutions.”
“When patients are treated with Cook catheters, we think about the patient’s whole experience. That means not just the outcome—it also means we think about how comfortable the patient is during treatment,” said Remco Van der Meel, director of product management for Cook’s Interventional specialty. “The FlexGRIP device is the perfect complement to Cook’s comprehensive portfolio of percutaneous drainage products. This well-designed and secure fixation device will help promote better outcomes and improve patient experiences, and we’re excited to have this product as an option available to all Cook customers who are using our percutaneous drainage products.”
Phillips’ LumiGuide ‘human GPS’ technology is now available to specialised hospitals in Europe and the USA. LumiGuide uses light reflected along an optical fibre inside a guidewire to generate three-dimensional (3D), high-resolution, colour images of devices including catheters inside a patient’s body in real time, from multiple angles and views.
LumiGuide, powered by Fiber Optic RealShape (FORS) technology, enables doctors to navigate through blood vessels using light, instead of X-ray. “[It’s] one of the most exciting changes that we’ve seen with imaging certainly throughout my career,” said Andres Schanzer (UMass Memorial Medical Center, Worcester, USA). In late 2023, LumiGuide was used for the first time to treat patients in Maastricht University Medical Center in the Netherlands, closely followed by the University of Alabama at Birmingham in the USA.
Developed in close collaboration with clinical partners, LumiGuide is made available, in first instance, to aortic centres of excellence that perform complex aortic repairs in the USA and Europe, a press release states.
LumiGuide’s radiation-free technology offers benefits for complex aortic procedures, removing physicians reliance on X-ray. With physicians tackling increasingly complex endovascular cases—such as aortic aneurysm repair—procedures can take significantly more time, resulting in a higher radiation dose for patients and clinicians.
LumiGuide uses light reflected along an optical fibre inside a guidewire to generate 3D, high-resolution, colour images of devices, including off-the-shelf catheters, inside a patient’s body in real time, from any angle and in multiple views. This means that physicians know which direction their device is facing and can see where they need to go. This navigation can be done all without X-ray.
“If we can see more, we can proceed more quickly and more confidently,” said Atul Gupta, chief medical officer for image-guided therapy and precision diagnosis at Philips and practicing interventional radiologist. “In effect, LumiGuide is a 3D human GPS system powered by light.”
Following a limited release to nine aortic centres, more than 900 patients have undergone procedures, with one site conducting a historic cohort comparison showing a 37% reduction in complex aortic procedure time, and a 56% reduction in radiation exposure (DAP) compared to X-ray.
Geert Willem Schurink, (Maastricht University Medical Center, Maastricht, The Netherlands) who performed the first surgical procedure with LumiGuide, said: “This artificial intelligence-based semi-automatic registration is very quick and accurate, even in the presence of stent grafts. Especially, if there is a need to re-register the device being guided in the patient’s body during the procedure, it is extremely helpful.”
Live guidance of a thrombectomy procedure performed with Philips Azurion
Endovascular Engineering, a medical device company involved with clot removal technologies for venous thromboembolism (VTE), has announced the enrolment and treatment of the first patient in the pivotal phase of its ENGULF US clinical trial.
This IDE trial will further evaluate the safety and efficacy of the Hēlo pulmonary embolism (PE) thrombectomy system, a first-of-its-kind technology, for the treatment of PE. This initial treatment, led by Malcolm Foster (Tennova Turkey Creek Medical Center, Farragut, USA) represents a step forward on the path to introducing the Hēlo PE system to the US market.
Enrolment of the first patient in the ENGULF pivotal cohort follows the completion of the 25-patient feasibility phase of the study. All patients in the pivotal trial will be treated with the latest version of the Hēlo PE thrombectomy system, equipped with a new accessory device designed to optimise clot engagement and blood loss management. “The integration of this new feature into the Hēlo system marks an impressive advancement, providing invaluable feedback that supports safe navigation for engaging target clot and helps to minimise blood loss throughout thrombectomy procedures,” noted Foster.
Mike Rosenthal, CEO of Endovascular Engineering, emphasised the importance of initiating the ENGULF pivotal IDE trial stating, “This first procedure represents a critical milestone for our company as the ENGULF trial is a reflection of our commitment to advancing the field of thrombectomy and has been initiated ahead of schedule.” Through clinical collaborations with leading medical institutions and clinicians like Foster, Endovascular Engineering remains committed to improving patient outcomes and revolutionizing thrombectomy treatment.
Cagent Vascular has announced a series C financing close in excess of US$30 million. US Venture Partners (USVP) led the round. Participation included new investor Blue Ridge Medical and existing investors, including Sectoral Asset Management.
“We are pleased with the significant investment from US Venture Partners and other new and existing investors. To date, we estimate that over 10,000 Serranator PTA [percutaneous transluminal angioplasty] serration balloon catheters (Serranator) have been used to treat those suffering from peripheral arterial disease (PAD). This infusion of capital will increase our commercial reach, helping to provide greater access for healthcare providers and their patients,” stated Carol A Burns, CEO.
USVP is a Silicon Valley venture capital firm based in Menlo Park, USA. “At US Venture Partners, we understand the challenges facing PAD patients and are keenly aware of the need for innovation for this vulnerable patient population. As we reviewed the impressive clinical data and spoke to physicians about their patient outcomes, it was clear that serration angioplasty is truly innovative. This was further underscored by the strong early commercial success driven by the exceptional team at Cagent Vascular,” said Casey Tansey, general partner, US Venture Partners.
A press release details that the Serranator has received US Food and Drug Administration (FDA) 510k clearance and is intended for dilatation of lesions in the iliac, femoral, iliofemoral, popliteal and infrapopliteal arteries for the treatment of obstructive lesions of native or synthetic arteriovenous dialysis fistulae. The product is currently being sold in the USA. The Serranator device also has CE mark and limited distribution in Europe.
IsomAb Ltd,a UK-based biotechnology company, has announced the closing of a £7.5 million (approximately US$9.4 million) seed financing round, led by Broadview Ventures, with further backing from existing investor, SCVC and participation from MEIF Proof of Concept & Early Stage Fund, which is managed by Mercia Ventures and part of the Midlands Engine Investment Fund (MEIF).
Founded in 2022, IsomAb is developing isoform-specific disease modifying antibody treatments for serious and life-threatening diseases with an initial focus on peripheral ischaemia. The seed funding round enables the company to advance the pre-clinical development of its lead antibody, ISM-001.
Jackie Turnbull, CEO of IsomAb, commented: “IsomAb’s lead programme targeting VEGF-A165b aims to treat peripheral arterial disease (PAD) in the large proportion of patients with concomitant metabolic syndrome and type 2 diabetes. We are delighted to have attracted a group of high-quality investors to support the early development of our novel programme toward CTA filing to enter the clinic.”
Benjamin Kreitman, principal at Broadview Ventures, said: “Peripheral arterial disease remains a significant unmet medical need worldwide, and the development of novel treatments to alleviate ischaemia could improve clinical care for millions of patients. As Broadview’s investment strategy is focused on the improvement of human health in the areas of cardiovascular disease and stroke, we are delighted to accelerate this highly innovative approach to treat peripheral arterial disease.”
SCVC managing partner, Harry Destecroix said: “We have been an investor in IsomAb since its incorporation and we are delighted to now be working with Broadview Ventures to take this technology to the clinic. There is enormous impact potential for patients aligning to a key area of SCVC’s mission: the advancement of human health.”
Hannah Tapsell Chapman of Mercia Ventures added: “IsomAb offers a fresh approach to the treatment of vascular disease. Although the initial focus will be on treating diabetics, research shows high levels of VEGF-A165b are also linked to increased risk of heart attack and stroke in non-diabetics, so it could have much wider applications. The funding will enable the team to progress the development of the lead compound ISM-001 towards human clinical trials.”
The MEIF is supported financially by the European Union using funding from the European Regional Development Fund (ERDF) as part of the European Structural and Investment Funds Growth Programme 2014–2020 and the European Investment Bank.
Efemoral Medical today announced that the US Food and Drug Administration (FDA) has granted its novel Efemoral vascular scaffold system (EVSS) Breakthrough Device status for the treatment of de novo or restenotic lesions of the infrapopliteal arteries in patients with chronic limb-threatening ischaemia (CLTI).
A press release states the EVSS offers a new approach to treating peripheral arterial occlusive disease by addressing the specific anatomic challenges and complex biomechanics of patients with athero-occlusive disease in the leg. Using multiple, serial, intravascular scaffolds, the patented FlexStep technology combines flexibility with support to open clogged vessels and sustain healthy blood flow while accommodating tortuosity and skeletal movement.
Formulated with sirolimus antiproliferative drug elution, the bioresorbable scaffolds restore normal vessel diameter at the time of the procedure, deliver therapeutic benefits across all lesion lengths and morphologies, and maintain durable patency while leaving no permanent implant behind. The device designed for femoropopliteal intervention is currently being tested in a first-in-human trial, EFEMORAL I, in investigative sites in New Zealand and Australia. Encouraged by the early clinical results, Efemoral Medical is now developing an additional device for treating infrapopliteal arteries in patients with CLTI.
“Diseased human arteries are most simply, reliably, and successfully treated with drug-eluting, balloon-expandable stents,” said Lewis B Schwartz, co-founder and CMO of Efemoral Medical. “However,” he continued, “it is extremely challenging to implant these permanent devices in the long and twisting arteries of the lower extremities. The EVSS uses a unique design of alternating, dissolvable, drug-eluting scaffolds that, for the first time, allows the long arteries of the legs to be treated with the same, effective, drug-eluting technology proven to be successful in multiple other vascular beds.”
The Breakthrough Devices programme is reserved for novel medical technologies that potentially provide for more effective diagnosis and/or treatment of life-threatening or irreversibly debilitating diseases. It is intended for patients to enjoy more timely access to novel devices by expediting their development, assessment, and review.
“Peripheral arterial occlusive disease has a significant negative impact on the health of as many as 20 million Americans,” said Christopher Haig, co-founder and CEO of Efemoral Medical. “It is especially devastating for those 10% of patients suffering from its most severe form, CLTI. We are extremely gratified that the FDA has recognised the potential of the EVSS to benefit these patients by granting Breakthrough Device status to our device.”
Sensome has announced enrolment of the first patients into a feasibility clinical study using the Clotild smart guidewire in peripheral artery disease (PAD). Clotild was designated a breakthrough medical device for use in brain arteries by the US Food and Drug Administration (FDA) in 2021.
The clinical trial, named SEPARATE, is designed to assess the artificial intelligence (AI)-powered Clotild sensor’s capability to detect various characteristics of blood vessel blockages in PAD patients. The first five patients have been enrolled at AZ Sint-Blasius Hospital in Dendermonde, Belgium, and preliminary results are anticipated in mid-2024.
A key focus of the SEPARATE clinical trial—according to a Sensome press release—is to evaluate the Clotild sensor’s capacity in differentiating between soft and friable “fresh” clots, and organised “old” clots. This critical information empowers physicians to select the most suitable endovascular therapeutic approach, thereby mitigating complications, avoiding embolisation, and enhancing long-term treatment outcomes, the release adds.
“Understanding the makeup of a total occlusion in peripheral artery disease is essential to choose an adequate treatment approach to ensure lower complication rates and more durable long-term outcomes in this complex group of vascular patients,” said Koen Deloose (AZ Sint-Blasius Hospital, Dendermonde, Belgium), principal investigator of the SEPARATE clinical trial. “Sensome’s tissue microsensor technology could become a novel tool to characterise the total occlusion in an objective and simple-to-use way that integrates perfectly with our current existing workflow.”
Franz Bozsak, chief executive officer and co-founder of Sensome, added: “After successfully applying our technology to the treatment of ischaemic stroke patients, we are excited about the opportunity to build on this work to potentially help millions of patients around the world whose lives have been impacted by PAD.”
The multi-society PAD Pulse Alliance is taking part in a peripheral arterial disease (PAD) public awareness campaign called “Get a Pulse on PAD”.
The group—formed of the Society for Vascular Surgery (SVS), the Association of Black Cardiologists (ABC), the Society for Cardiovascular Angiography & Interventions (SCAI) and Society of Interventional Radiology (SIR)—aims to educate people on PAD risk factors and potential symptoms, as well as to encourage patients to advocate for their own health with their doctors.
The awareness campaign, taglined “Kick Off the Conversation,” kicked off as the PAD Pulse Alliance released survey data showing that 70% of Americans are unaware of the disease, contributing to 400 amputations performed each day in the USA. The top risk factors for PAD are common chronic health conditions that disproportionately impact underserved communities. Yet among Black and Hispanic adults, nearly 80% report never having a doctor or healthcare provider discuss PAD with them.
“These new insights are particularly concerning among those most at risk and come at a time when a staggering one in 20 Americans over 50 years of age experience PAD,” said SCAI President George D Dangas (Mount Sinai Medical Center, New York City, USA). “The survey confirms what we feared: millions don’t have the tools they need to help start a conversation with their healthcare providers because patients are unaware of their risks and the common signs and symptoms. That’s why we’re encouraging anyone with leading risk factors, diabetes, high blood pressure and use of tobacco products, to know your ‘three for PAD’ and talk to your doctor.”
Data from the PAD Pulse Alliance survey highlights a disconnect among people between the risk factors and their personal perceived risk of PAD. Nearly 75% of Black and Hispanic adults surveyed report having or knowing someone who has diabetes, high blood pressure, or is a smoker, but only 30% believe they could be at risk. This is in stark contrast to real-world impact. Black people are twice as likely to suffer from PAD and up to four times more likely to undergo an amputation compared to white people. Hispanics present with more progressive PAD leading to worse outcomes including greater risk of amputation.
“The disturbing variations in PAD prevalence, treatments and outcomes underscore another perilous consequence of the health equity gap in managing chronic conditions,” said Foluso Fakorede (Cardiovascular Solutions of Central Mississippi, Cleveland, USA), co-chair of the Association of Black Cardiologists PAD Initiative. “It’s critical to increase awareness among racial and ethnically marginalised communities and the providers who serve them to close the gap. This campaign is one way we are doing just that, but it will take an ongoing conversation to ensure we’re meeting patients where they are with the tools and resources they need.”
“Screening for PAD is easy, quick, and non-invasive. Yet, this survey confirmed that critical patient-provider conversations addressing common symptoms aren’t happening,” said SIR President Alda L Tam (University of Texas MD Anderson Cancer Center, Houston, USA). “If we can educate more people on the risk factors and early warning signs associated with PAD, it’s our hope we can foster dialogue earlier between providers and patients to kick off screening and treatment—ultimately preventing amputations and saving lives.”
“The collaboration among these medical societies is a testament to the devastating impact PAD can have on people, families and whole communities if not diagnosed and treated early, and, importantly, early treatment usually consists of medication and lifestyle changes,” said SVS President Joseph L Mills (Baylor College of Medicine, Houston, USA). “We hope that care teams will continue to collaborate to ensure early and proper diagnosis with the ultimate goal of improving outcomes for patients.”
To help educate patients and give them the tools to start the conversation, the PAD Pulse Alliance published a website and patient toolkit at PADPulse.org.
Innova Vascular has announced successful early commercial use of the company’s Laguna thrombectomy system. Physicians at University of California (UCLA) Medical Center in Los Angeles, USA and Providence St. Joseph in Orange, USA, were the first to use this system in patients and have reported positively on their experience, a press release states.
Raj Khalsa (St. Joseph Hospital, Orange, USA) described the system as a “beautifully engineered device with easy prep, excellent trackability in challenging anatomies, and highly effective clot extraction. The design, with simplicity in mind, is a significant advantage in high-risk procedures.” Khalsa went on to state: “With increasing awareness of venous thromboembolism, the Innova system joins the ranks of a select few large-bore thrombectomy systems, with a remarkably efficient solution that offers substantial value to the healthcare system.”
John Moriarty (UCLA Medical Center, Los Angeles, USA) said: “The Laguna thrombectomy system is a valuable addition to the existing therapeutic options for venous thromboembolism. The system offers excellent navigability and ease of use enabling operators at all skill levels to remove clots efficiently. It addresses the need for large volume clot removal in a range of vessel sizes in various anatomical locations within the peripheral vasculature.”
The Laguna thrombectomy system encompasses two devices developed by Innova Vascular: the Malibu aspiration catheter system and the Laguna clot retriever system. Both devices received US Food and Drug Administration (FDA) 510(k) clearance in June 2023.
The Malibu aspiration catheter utilises a gradient structural design and a hydrophilic coating for excellent navigability through tortuous vessels. It is available in 24Fr, 20Fr, 16Fr, and 12Fr outer diameters to address a variety of clot morphologies and vessel sizes. The catheter can be used alone or in conjunction with the Laguna clot retriever, which utilises a self-expanding laser-cut Nitinol design and is available in two diameters. Radial strength and cell sizes of the retriever are optimised for maximising clot capture and enabling circumferential clot ingress.
“We are extremely pleased with the early clinical performance of the system and look forward to expanding our product launch in the period ahead,” said Sanjay Shrivastava CEO of Innova Vascular. “Successful use of the system marks an important milestone in our commitment to develop innovative technologies targeting large, underserved markets. We are grateful to our physician advisors, who play a key role in shaping these solutions.”
Following a review, the UK Medicines and Healthcare Products Regulatory Agency (MHRA) has updated guidance on the use of paclitaxel-coated devices stating that such devices can be considered for the treatment of peripheral arterial disease (PAD), including intermittent claudication and chronic limb-threatening ischaemia (CLTI).
The MHRA had previously issued a statement in April 2022 on the use of paclitaxel drug-coated-balloons or drug-eluting stents in patients with CLTI which stated that they should only be used in patients where ‘the benefits may outweigh the risks’. The parameters for use outlined that exposure should be kept to a minimum, which referred to using the lowest dose device available and avoiding/reducing repeated exposure to a device. Furthermore, the 2022 guidelines noted that paclitaxel devices should not be used in the routine treatment of patients with intermittent claudication due to the reported risk of longer-term increased mortality.
The updated guidance has been issued following an extensive review of the most recent published literature alongside the MHRA’s request for the advice of the Interim Devices Working Group (IDWG) and other invited experts. The IDWG advised that the new studies did not support a statistically significant increased risk of harm associated with the use of paclitaxel-coated devices in patients with PAD, irrespective of disease type or severity.
In this update, the MHRA make reference to the 2023 evaluation of numerous randomised controlled trials and real-world studies which compared paclitaxel-coated devices versus control devices in a patient-level pooled analysis. Led by Sahil A Parikh (Columbia University Irving Medical Center, New York, USA), the analysis included a total of 2666 participants with a median follow-up of 4.9 years. Their results showed that no significant increase in deaths were observed for patients treated with paclitaxel-coated devices, providing reassurance to patients, physicians and regulators on the safety of said devices.
Subsequently, the MHRA has removed its previous restrictions on indication, dose and repeated exposure for paclitaxel-coated devices for both intermitted claudication and CLTI.
The REDUCED-1 study, a US Food and Drug Administration (FDA) investigational device exemption (IDE)-approved pilot study of the treatment of hypertension with the proprietary Therapeutic Intra-Vascular Ultrasound (TIVUS) system (SoniVie), has completed enrolment.
“Initial results from the ongoing REDUCED-1 study are encouraging and we continue to diligently follow the enrolled patients,” said Christian Spaulding, chief medical officer of SoniVie, in a press release announcing the study milestone.
The trial had two enrolment cohorts that were conducted under an identical protocol in the USA and in Israel. Twenty-five patients were enrolled in the USA and 15 patients were enrolled in Israel. All patients (N=40) are now in the follow-up phase of the study where primary efficacy (change in daytime systolic ambulatory blood pressure) will be analysed at three months and safety will be analysed at one month and 12 months follow-up respectively.
Renal Denervation with TIVUS is a minimally invasive procedure that uses high-frequency non-focused ultrasound energy to ablate nerves in the renal arteries. This causes a reduction in the nerve activity, which may decrease blood pressure. This procedure is designed for patients who suffer from resistant hypertension.
“Our next commitment towards patients, physicians and regulators is now to clinically validate the TIVUS system in a global pivotal trial and expand its use under the pivotal study with radial access procedures,” said Tomaso Zambelli, chief executive officer, SoniVie.
Cook Medical has announced the first patient treated in the clinical study of the ZENITH FENESTRATED+ endovascular graft (ZFEN+) in the USA. The procedure was performed on January 29, 2024 at The University of Texas Health (UTHealth) in Houston, Texas, by Gustavo Oderich, global principal investigator.
“We are ecstatic at UTHealth Houston to have treated this first ZFEN+ patient. This is a huge step forward in getting the first patient-specific device for complex abdominal and extent IV thoracoabdominal aneurysms with fenestrations. Rather than a one-size-fits-all approach, the ZFEN+ device design aims to optimise patient needs,” said Oderich.
The ZFEN+ clinical study is being conducted under an investigational device exemption (IDE) from the US Food and Drug Administration (FDA). This clinical study will assess the safety and effectiveness of the ZFEN+ used in combination with the investigational Zenith Universal Distal Body 2.0 Graft (Unibody2), the investigational Bentley BeGraft Balloon-Expandable fenestrated endovascular aortic repair (FEVAR) bridging stent graft system and the commercially available Zenith Spiral-Z abdominal aortic aneurysm (AAA) Iliac leg graft (ZSLE).
The ZFEN+ clinical study will enrol patients in need of treatment of aortic aneurysms involving one or more of the major visceral arteries. Patients with juxtarenal, pararenal and extent IV thoracoabdominal aneurysms meeting specific anatomical requirements may be included in the study. The ZFEN+ device is designed with fenestrations aligned to a patient’s unique anatomy and to extend the proximal margin of aneurysmal disease that can be treated endovascularly.
“On behalf of Cook Medical, we are very excited to announce the first implant of ZFEN+. This is an exciting milestone in the advancement of fenestrated aortic technology. This next generation of patient-specific aortic endograft technology has received a breakthrough device designation from the FDA. This advancement will enable physicians to select up to five target vessels. Our team is committed to listening, collaborating and bringing these innovative technologies to a broader patient population,” said Johnny LeBlanc, director of aortic product management at Cook Medical.
“Our team is pleased to be the first commercial implanter of the new lower profile VBX stent graft,” said Darren Schneider, chief of vascular surgery and endovascular therapy, Penn Medicine, Philadelphia, Pennsylvania. “Combined with the flexibility, strength and deployment accuracy I’ve always trusted with the device, the new lower profile will enable me to treat most of my complex cases with a six or seven Fr device, reducing the risk of access complications while bringing trusted VBX stent graft outcomes to more of my patients.”
No changes to the stent design were made to achieve the lower profile. By focusing on improvements to the delivery system only, the valued characteristics and trusted performance of the stent graft itself remain unchanged and are joined by the enhanced versatility a lower profile provides. Depending on the practice, physicians may be able to use the VBX stent graft with a broader set of patients, experience a lower risk of complications at the access site.
“With the recently published five-year outcomes data, and the active pursuit of evaluating superiority versus bare metal stents in complex iliac occlusive disease through the Gore VBX FORWARD clinical study, this lower profile innovation gives me yet another reason to feel confident in the proven outcomes and broad versatility of this device in my practice,” said Ehrin Armstrong, interventional cardiologist and director of clinical research, Advanced Heart and Vein Center, Denver, Colorado.
Since its launch in the USA in 2017, more than 375,000 VBX stent grafts have been implanted worldwide. Here, the device is indicated for the treatment of de novo or restenotic lesions found in iliac arteries with reference vessel diameters ranging from five–13mm and lesion lengths up to 110mm, including lesions at the aortic bifurcation.
The lower profile device will be rolled out to the US market over the coming months and is also being studied in the Type IV Thoracoabdominal Aortic Aneurysms (TAMBE) trial.
“The approval and release of the lower profile VBX stent graft serves as a demonstration of the Gore Medical Products Division’s commitment to continual improvement and lifelong innovation in collaboration with physicians to solve tough challenges where there is a critical patient need,” said Jill Paine, peripheral business leader for Gore’s Medical Products Division. “We look forward to supporting our physicians and their patients through the delivery of this exciting innovation to their treatment toolbox.”
Surmodics hasannounced successful early clinical use of the company’s Pounce LP (low-profile) thrombectomy system. The Pounce LP system, which received US Food and Drug Administration (FDA) clearance in June 2023, is currently in limited market evaluation (LME), with full commercial launch planned following completion of the LME.
Surmodics’ Pounce thrombectomy devices are intended for the non-surgical removal of thrombi and emboli from the peripheral arterial vasculature. The new Pounce LP thrombectomy system is indicated for use in vessels ranging from 2–4mm in diameter, sizes typical of vessels found below the knee. A press release details that the Pounce LP system complements the original Pounce thrombectomy system, introduced in 2021, which is indicated for use in vessels 3.5–6mm in diameter.
Lucas Ferrer Cardona, a vascular surgeon with the Dell Seton Medical Center at the University of Texas Hospital in Austin, USA, was the first physician to use the Pounce LP system.
“In our first use of the device, the Pounce LP thrombectomy system performed exceptionally well in helping our team restore blood flow to the foot for a limb-threatened patient,” he said. “Using the device, we promptly removed acute and subacute thrombus from the mid-peroneal artery below the knee with no adjunctive use of thrombolytics and no embolisation. Thrombi or emboli in below-the-knee vessels have traditionally been very challenging to remove. I believe this device holds great promise in filling a major gap in our treatment algorithm.”
Elizabeth Genovese, a vascular surgeon at the Hospital of the University of Pennsylvania in Philadelphia, USA, who has experience using the original Pounce system, is among several other satisfied early users of the Pounce LP system. She recently deployed the Pounce LP device to revascularise a patient with arterial occlusions in both the anterior tibial and peroneal arteries.
“The Pounce LP system allowed me to treat chronic thrombus in these vessels with the effectiveness I’d expect from open surgical Fogarty embolectomy while maintaining the advantages of an endovascular approach for treating underlying and distal disease,” she said. “We were able to achieve an optimal outcome in a very complex lesion, and this type of result would not have been possible without this device.”
“We’re very pleased with the successful early clinical use of the Pounce LP thrombectomy system, which will extend the range of treatment for our Pounce platform to include removal of organised thrombotic or embolic clots from the iliac arteries in the pelvis down to tibial vessels below the knee,” said Gary Maharaj, president and chief executive officer of Surmodics. “Downstream embolisation of chronic material into below-the-knee arteries during an endovascular procedure can be an interventionist’s nightmare, sometimes requiring surgical rescue. The Pounce LP system’s ability to capture and remove these unexpected emboli adds yet more value to this device for BTK [below-the-knee] revascularisation.”
Baird Medical Devices, a microwave ablation medical device developer and provider in China and the USA, has recently announced that it has performed its first thyroid microwave ablation procedure in the USA since obtaining registration clearance from the US Food and Drug Administration (FDA) on November 22, 2023.
The minimally invasive procedure was performed on 12 January 2024 at Utah Endocrinology Associates by interventional endocrinologist Alireza Falahati, marking a significant advancement in thyroid nodule management, a press release states. The emergent microwave ablation procedure for thyroid nodules offers patients an alternative to traditional excision surgery, enabling swifter recovery, a reduction of scar tissue in the neck and chest area, and greater efficiency for physicians.
Falahati expressed his enthusiasm for the new treatment option: “The success of this procedure with Baird Medical’s ablation needle represents a leap forward in our ability to treat thyroid nodules effectively. I look forward to performing many more similar procedures in the near future.”
Thyroid nodules occur in 30–50% of the adult population, with a rise of incidence as people age, and are more common with women than men. Microwave ablation procedures utilise a small needle to safely deliver therapeutic microwave energy directly to the nodule being treated while sparing the surrounding healthy tissue and preserving the function of the thyroid, thereby eliminating hormone replacement therapy affiliated with surgical approaches.
“We congratulate Falahati and his first patient for breaking new ground with us in this important therapeutic area,” said Haimei Wu, founder and CEO of Baird Medical. “This procedure was conducted less than 60 days after the FDA’s clearance of our advanced technology for the market in the USA. We are excited about the opportunities this offers to millions of patients with unmet needs in the future.”
Due to recent technological advancements and increasing awareness, there has been a rapid increase in the number of minimally invasive, thermal ablation procedures performed. In September 2023, the American Thyroid Association (ATA) published their recommended guidelines for the safe implementation and adoption thermal ablation procedures to treatment of thyroid nodules, suggestive of the increased adoption of the procedure.
AngioDynamics today announced that the US Food and Drug Administration (FDA) has cleared the Auryon XL catheter, a 225cm radial access catheter, for use with the Auryon atherectomy system in the treatment of peripheral arterial disease (PAD).
According to an AngioDynamics press relaese, studies have shown that radial access is associated with a significantly lower risk of major bleeding and access site complications when compared to femoral access in the treatment of patients with PAD.
“Since its launch in September 2020, the Auryon atherectomy system, with its innovative solid-state laser technology, has fundamentally changed patient treatment for PAD and quickly become an essential tool for providers and patients,” said Kimberly Nelson, senior director of Auryon global marketing at AngioDynamics. “Our entry into the radial-to-peripheral (R2P) space with Auryon XL is an important part of our focus on advancing the quality of care delivery and it demonstrates our commitment to meeting the unmet needs of patients and atherectomy providers.”
AngioDynamics states that the Auryon XL catheter, available in 0.9mm and 1.5mm diameters, expands treatment access points in atherectomy procedures for PAD. It notes that use of a general radial access catheter may reduce incidents of major bleeding, when compared to femoral access, by more than 70%. Additionally, the Auryon XL catheter may eliminate the need for the use of femoral closure devices and allow for the treatment of bilateral disease in a single session, supporting improved patient mobility, earlier discharge and faster patient recovery times, the company adds.
“Radial access is more than an entry point; it’s a transformative expressway to enhanced patient outcomes,” said Ankur Lodha, interventional cardiologist at Cardiovascular Institute of the South located in Lafayette, USA. “With an innovative design and its ease-of-use, the Auryon XL catheter brings significant advancements to radial procedures as the first non-orbital atherectomy device—setting a new standard for laser atherectomy technology.”
Following US FDA 510(k) clearance, AngioDynamics initiated a limited market release of the Auryon XL catheter in the USA in January 2024 and expects to enter full market release in February 2024.
AngioDynamics details that the Auryon laser can be used to treat all infrainguinal lesion types, including above-the-knee (ATK), below-the-knee (BTK) and in-stent restenosis (ISR), and that, to date, it has been used to treat more than 50,000 patients in the USA.
The technology underlying the Auryon atherectomy system has been shown in clinical studies to be effective in treating lesions ranging from soft plaque to severely calcified, AngioDynamics reports. The company explains that the system uses a 355nm wavelength laser platform, enabling the use of short ultraviolet (UV) laser pulses with targeted biological reactions that are effective in treating PAD while minimising the risk of perforation and preserving the ability to vaporise lesions without thermal ablation.
Surmodics hasannounced successful early clinical use of the company’s Pounce LP (low-profile) thrombectomy system. The Pounce LP system, which received US Food and Drug Administration (FDA) clearance in June 2023, is currently in limited market evaluation (LME), with full commercial launch planned following completion of the LME.
Surmodics’ Pounce thrombectomy devices are intended for the non-surgical removal of thrombi and emboli from the peripheral arterial vasculature. The new Pounce LP thrombectomy system is indicated for use in vessels ranging from 2–4mm in diameter, sizes typical of vessels found below the knee. A press release details that the Pounce LP system complements the original Pounce thrombectomy system, introduced in 2021, which is indicated for use in vessels 3.5–6mm in diameter.
Lucas Ferrer Cardona, a vascular surgeon with the Dell Seton Medical Center at the University of Texas Hospital in Austin, USA, was the first physician to use the Pounce LP system.
“In our first use of the device, the Pounce LP thrombectomy system performed exceptionally well in helping our team restore blood flow to the foot for a limb-threatened patient,” he said. “Using the device, we promptly removed acute and subacute thrombus from the mid-peroneal artery below the knee with no adjunctive use of thrombolytics and no embolisation. Thrombi or emboli in below-the-knee vessels have traditionally been very challenging to remove. I believe this device holds great promise in filling a major gap in our treatment algorithm.”
Elizabeth Genovese, a vascular surgeon at the Hospital of the University of Pennsylvania in Philadelphia, USA, who has experience using the original Pounce system, is among several other satisfied early users of the Pounce LP system. She recently deployed the Pounce LP device to revascularise a patient with arterial occlusions in both the anterior tibial and peroneal arteries.
“The Pounce LP system allowed me to treat chronic thrombus in these vessels with the effectiveness I’d expect from open surgical Fogarty embolectomy while maintaining the advantages of an endovascular approach for treating underlying and distal disease,” she said. “We were able to achieve an optimal outcome in a very complex lesion, and this type of result would not have been possible without this device.”
“We’re very pleased with the successful early clinical use of the Pounce LP thrombectomy system, which will extend the range of treatment for our Pounce platform to include removal of organised thrombotic or embolic clots from the iliac arteries in the pelvis down to tibial vessels below the knee,” said Gary Maharaj, president and chief executive officer of Surmodics. “Downstream embolisation of chronic material into below-the-knee arteries during an endovascular procedure can be an interventionist’s nightmare, sometimes requiring surgical rescue. The Pounce LP system’s ability to capture and remove these unexpected emboli adds yet more value to this device for BTK [below-the-knee] revascularisation.”
An analysis of data from the SPYRAL HTN-ON MED trial of the Symplicity Spyral (Medtronic) radiofrequency denervation system for the treatment of uncontrolled hypertension has found that the technique can be expected to provide “good value for money” as a therapeutic approach.
The analysis, authored by Andrew Sharp (University Hospital of Wales and Cardiff University, Cardiff, UK) et al and published in the European Heart Journal – Quality of Care & Clinical Outcomes, examined the cost-effectiveness of radiofrequency renal denervation for the treatment of the broader uncontrolled hypertension patient group in the setting of the UK healthcare system.
Recent US Food and Drug Administration (FDA) approval for the therapy and updated recommendations from the European Society of Hypertension (ESH) in its 2023 Management of Arterial Hypertension guidelines will “substantially increase global access to this therapeutic option”, the study’s authors write. These developments, they add, contribute to a growing interest in understanding the health-economic implications of radiofrequency renal denervation adoption.
A decision-analytic model based on multivariate risk equations projected clinical events, quality-adjusted life years (QALYs) and costs. The model consists of seven health states, hypertension alone, myocardial infarction (MI), other symptomatic coronary artery disease, stroke, heart failure, end-stage renal disease and death.
Risk reduction associated with changes in office systolic blood pressure (oSBP) was estimated based on a published meta-regression of hypertension trials. The base case effect size of -4.9mmHg oSBP (observed versus sham control) was taken from the SPYRAL HTN-ON MED trial of 337 patients, with the costs based upon NHS England data.
Researchers evaluated the incremental cost-effectiveness ratio (ICER) against the National Institute for Health and Care Excellence (NICE) cost-effectiveness threshold of £20,000–30,000 per QALY gained. Findings from the study showed that radiofrequency renal denervation resulted in a relative risk reduction in clinical events over 10 years (0.80 for stroke, 0.88 for MI, and 0.72 for heart failure) with an increase in health benefit over a patient’s lifetime, adding 0.35 QALYs, at a cost of £4,763, giving an ICER of £13,482 per QALY gained. Findings were robust across tested scenarios, the researchers report.
“The analysis found that an effect size of 4.9mmHg, as observed in the SPYRAL HTN-ON MED study can be expected to lead to meaningful outcome improvement and related downstream cost savings in the long-term, which render the intervention good value for money,” Sharp et al write. “Specifically, a significant reduction of 20% for stroke and 12% for MI was found for a ten-year horizon in treated versus control subjects, indicating the potential for radiofrequency renal denervation to reduce or delay major hypertension sequelae.”
“The analysis took a conservative approach, using a base case blood pressure reduction that is lower than that achieved in the real world Global registry and yet still met the NICE standard for cost effectiveness,” Sharp told Cardiovascular News.
Calf angiogram obtained using the Summa Finesse catheter with 1 ml equivalent of 60% contrast.
Summa Therapeutics has announced that the first-in-man injectable angioplasty procedures for patients with below-knee peripheral arterial disease (PAD) were performed successfully using its Finesse Injectable balloon catheter platform.
The Summa Finesse injectable catheter is the industry’s first hybrid diagnostic and therapeutic angioplasty balloon catheter developed to facilitate treatment of patients at risk of limb loss due to below-the-knee PAD. It was designed to improve the efficiency of peripheral angioplasty procedures by reducing equipment and contrast needs.
The Summa Finesse injectable platform is designed to reduce the need for some cumbersome catheter exchanges through its ability to provide contrast injection on the fly, enabling users to move seamlessly from injection to balloon inflation throughout complex procedures. This distinct operator convenience streamlines the procedure and reduces the need for equipment. All users reported that the injection ability exceeded expectations.
Angioplasty procedures below the knee also require X-ray contrast, which can cause damage to kidney function. This is an especially critical issue because many patients undergoing angioplasty procedures below the knee have diabetes and kidney dysfunction. Operators reported that the Summa Finesse injectable catheter allowed for decreased use of X-ray contrast, with 100% of procedures requiring less contrast than typically used with conventional devices. In the calf, ultra-low contrast angiograms were obtained with as little as 1ml equivalent of contrast.
The first-in-man procedures were carried at Mount Sinai hospital in New York City, USA by Rahul Patel and Robert Lookstein, and at the advanced vascular and interventional services office-based laboratory in West Orange, New Jersey, USA by John Rundback and Kevin Herman.
“The Summa balloon platform is a game changer that provides several unique advantages,” said Rundback, interventional radiologist and vascular specialist. “In our busy limb-salvage practice, it will be an important tool.”
The Summa Finesse injectable is a multifunctional catheter that serves as a crossing catheter, diagnostic angiography catheter, and angioplasty catheter to reduce equipment and contrast needs. It was noted that in many cases with the Summa Finesse catheter functioning as a crossing catheter, microcatheters were not needed to cross arterial obstructions.
“Summa’s system makes below-the-knee angioplasty cases easier compared to a conventional setup,” said Herman, nationally acclaimed interventional radiologist. “I start with Finesse and use it to perform angiography, cross lesions, and do serial angioplasties of multiple arterial segments in the calf all with the same catheter. It’s a better designed system for below-knee angioplasty.”
“In the first cases, expectations were met or exceeded, including improved procedural efficiency and lower equipment needs,” said Timothy Murphy, CEO of Summa Therapeutics. “All users reported using less contrast and yet angiographic quality was described as excellent.”
FastWave Medical has announced the successful completion of enrolment for its first-in-human (FIH) study with the company’s peripheral intravascular lithotripsy (IVL) technology.
The prospective, single-arm study aims to assess the safety and performance of FastWave’s IVL system in patients with peripheral arterial disease of the superficial femoral or popliteal arteries with moderate to severe calcium. Principal investigators Miguel Montero-Baker from Houston Methodist Hospital and HOPE Vascular & Podiatry Clinic and Venkatesh Ramaiah from HonorHealth Vascular Group and Pulse Cardiovascular Institute, conducted the procedures successfully in collaboration with the hosting investigator, Antonio Muñoa.
Montero-Baker stated: “I am excited to be part of the initial cases to evaluate FastWave’s peripheral IVL platform. Their team has rapidly developed an easy-to-use system to address existing technological gaps, marking a significant milestone in achieving the company’s near-term goals.”
FastWave’s IVL platform is designed to treat calcific artery disease by fracturing calcium deposits using a balloon catheter that delivers shockwaves. The company’s peripheral IVL technology offers a user-friendly design with a highly deliverable, low-profile, rupture-resistant balloon that generates durable and predictable circumferential ultrasonic pressure, the company says in a press release.
“Calcium poses significant therapeutic challenges in treating peripheral artery disease, and many of the existing modalities are not optimal for addressing medial and deep plaque,” stated Ramaiah. “FastWave’s peripheral IVL technology is a promising advancement in calcium modification, and I am excited by the procedural success in these initial cases.”
“The successful enrolment of our FIH study is an important inflection point for FastWave, and we’re looking forward to advancing our peripheral IVL system toward a pivotal clinical trial this year,” said Scott Nelson, co-founder and chief executive officer of FastWave Medical. “I would like to congratulate Drs Montero-Baker, Ramaiah, and Muñoa for their outstanding support, and acknowledge the commitment of the entire FastWave team to achieve this milestone in such a short amount of time. It’s a true honour to work alongside such a talented group.”
Reflow Medical recently announced it has received CE mark certification in the European Union for the Bare Temporary Spur stent system. The device is intended to treat de novo or restenotic lesions in the infrapopliteal arteries with a commercially available drug-coated balloon (DCB) to enhance drug absorption.
“The device performance and clinical study data for patients suffering from chronic limb-threatening ischaemia (CLTI) has been quite impressive,” said Thomas Zeller, who is chief of the Department of Angiology at University Heart Center Freiburg in Bad Krozingen, Germany. Zeller was a principal investigator in the DEEPER OUS clinical trial.
A Reflow Medical press release details that the Bare Temporary Spur stent system, followed by DCB treatment, reduces clinically driven target lesion revascularisation (CD-TLR), improves wound healing, reduces recoil, and improves vessel patency through one year, compared to historical treatment outcomes with plain balloon angioplasty or a DCB alone.
Marianne Brodmann, a professor and vascular specialist with the Division of Angiology, Medical University Graz in Graz, Austria, and the principal investigator for the DEEPER LIMUS clinical trial to evaluate the Bare Temporary Spur stent system, said: “We have found that the Spur allows us to treat patients with BTK [below-the-knee] disease using stent therapy, without the long-term risk of a stent implant,” she said.
The Bare Temporary Spur stent system is a unique clinical solution intended to provide stent-like results while leaving no metal behind, Reflow Medical shares. Known as retrievable stent therapy, or RST, the self-expanding stent is designed with radial spikes for creating channels in the vessel wall to enhance drug absorption and reduce recoil. The stent is then recaptured, removed, and treated with a commercially available DCB.
“Earning the CE mark is a huge milestone for the company. It enables us to offer a clinically validated solution to an unmet need in a major disease area,” said Isa Rizk, Reflow Medical’s co-founder and CEO. “Our next goal is to expand our organisation to commercialise this breakthrough technology and serve the needs of physicians and their patients in countries accepting this certification.”
Reflow Medical states that the Bare Temporary Spur stent system was granted certification as a Class IIa medical device under the European Union Medical Device Regulation (2017/745).
Delcath Systems, an interventional oncology company focused on the treatment of primary and metastatic cancers of the liver, has announced the first commercial use of Hepzato Kit for the treatment of metastatic uveal melanoma.
The procedure took place at Moffitt Cancer Center in Tampa, Florida by Jonathan S Zager, chief academic officer at the facility. Zager was the global lead investigator for the FOCUS phase 3 trial.
“The fact that patients with difficult to treat metastatic uveal melanoma with limited treatment options now have another alternative is truly remarkable and exciting. There has been a large unmet need for liver directed therapy options to treat this patient population, and we intend to incorporate this as standard of care for appropriate patients,” said Zager. The investigators enrolled and treated the first and last patients on the FOCUS phase 3 trial and the team at Moffitt has performed the procedure over 200 times to date.
The company is working with numerous other leading cancer centres across the USA which have indicated interest in Hepzato Kit to ensure patients have nationwide access to the treatment. In conjunction with the first commercial treatment, Delcath also launched websites relating to the Hepzato Kit to support the commercial launch.
“The first commercial procedure utilising Hepzato Kit in the USA is a significant milestone for Delcath and patients suffering from metastatic uveal melanoma. We are proud to continue our relationship with Zager and the team at Moffitt Cancer Center to bring this unique treatment to appropriate patients in need. I want to thank all the collaborators and patients who participated in the long but necessary process to bring Hepzato Kit to market,” said Gerard Michel, Delcath’s chief executive officer.
Gore Viabahn VBX balloon expandable endoprosthesis
Gore has announced that the first patients have been enrolled in the Gore VBX FORWARD clinical study, a global prospective, multicentre, randomised controlled trial to compare the Gore Viabahn VBX balloon expandable endoprosthesis (VBX stent graft) to bare metal stenting for patients with complex iliac occlusive disease.
“Our team is pleased to be among the first to enrol patients in this important study,” said Fakhir Elmasri, interventional radiologist at Lakeland Vascular Institute (Lakeland, USA). “Our first patient presented with complex, bilateral iliac disease and was randomised to treatment with VBX stent grafts. I look forward to seeing the results of the study to inform device selection for durable outcomes in the future.”
“While stenting is common when treating complex iliac occlusive disease, the question around whether to use a covered or bare metal stent [BMS] remains a source of debate,” added Prakash Krishnan, interventional cardiologist at The Mount Sinai Hospital (New York, USA). “This trial is designed to answer the question as to whether covered stents are the superior modality among commonly used devices in contemporary practice.”
The VBX FORWARD study aims to enrol an estimated 244 patients across 40 sites in the USA, Australia, New Zealand and Europe, randomising them 1:1 to the VBX stent graft group or the control group (BMS) and conduct follow-up visits through five years from the initial procedure.
“Treating complex iliac occlusive disease often comes with significant challenges, including tortuous anatomy and calcified lesions with the potential for rupture,” remarked Melissa Kirkwood, professor and chief of vascular surgery at the University of Texas Southwestern Medical Center inDallas, USA, and VBX FORWARD study steering committee member. “The outcomes of this important trial will help determine whether the VBX stent graft, with its unique and versatile design, plays a meaningful role in addressing these challenges.”
A Gore press release details that the VBX stent graft offers precise delivery and supports positive outcomes in complex aortoiliac applications. It details that recently published long-term follow-up of patients treated with the VBX stent graft for aortoiliac occlusive disease (AIOD) demonstrates the robustness and durability of the device through five years.
“Today marks important progress in our continuing effort to raise the bar on endovascular treatment outcomes that demonstrate a positive impact on the lives of patients who suffer from this disease,” said Eric Zacharias, medical products division leader at Gore when the news was released on 16 January. “Not only can the results from this randomised controlled trial help determine which stent choice demonstrates better patency in patients with complex iliac occlusive disease, but it also aims to provide the quality of evidence necessary to inform practice guideline recommendations.”
Dr. Ari Kramer of Spartanburg Regional Hospital with Laminate's VasQ device after the successful inaugural U.S. implantation. Dr. Kramer expressed his enthusiasm for the transformative impact of VasQ on patient care, stating, "I am excited to revolutionize the standard of care for our fistula patients with VasQ. I firmly believe that this device offers my patients the optimal prospects for a sustained, well-functioning fistula with reduced complications and the need for additional procedures."
Ari Kramer with Laminate Medical’s VasQ device
Laminate Medical has announced the first implantation of their VasQ device in the USA, performed by Ari Kramer (Spartanburg Regional Hospital, Spartanburg, USA). The VasQ technology was granted US Food and Drug Administration (FDA) approval in September 2023, and is reported to be the only approved product on the market currently, designed to assist surgical fistula success from the point of creation.
A recent press release states that Kramer expressed his enthusiasm for the transformative impact of VasQ on patient care: “I am excited to revolutionise the standard of care for our fistula patients with VasQ. I firmly believe that this device offers my patients the optimal prospects for a sustained, well-functioning fistula with reduced complications and the need for additional procedures.”
VasQ is a nitinol-based external support device for the artery and vein anastomosis during the surgical creation of an arteriovenous fistula to promote maturation into a functional access for haemodialysis. The device was designed to provide structural reinforcement of the mobilised vessels and guides a more stable arterial flow profile as it transitions into the vein.
The importance of this innovation has been underscored by the surge in use of central venous catheters (CVC) during the COVID-19 pandemic, the press release details, leading to heightened risk of infection and mortality. Creating more functional fistulas, it is hoped that VasQ may help to reduce CVC use in this patient population.
In a statement, Laminate CEO, Tammy Gilon, hailed the successful completion of the inaugural VasQ case in the USA as a monumental achievement for Laminate Medical Technologies. Gilon remarked: “This accomplishment represents the culmination of 12 years of dedicated effort, and we are elated to introduce VasQ to the population of the USA.”
InkSpace Imaging, a company engaged with diagnostic medical device technology, has announced it received US Food and Drug Administration (FDA) clearance for its next-generation small body array for the Siemens Healthineers Magnetom Skyra and Vida series 3T magnetic resonance imaging (MRI) scanners.
This new medical device is part of their suite of MRI coils designed to revolutionise the patient experience while enhancing efficiency in MRI scans and clinical diagnosis.
As a recent press release states, the small body array is huggable, lightweight, and flexible. It wraps around patients like a blanket, ensuring unparalleled image quality. The body contouring design optimises the signal-to-noise ratio, which is crucial for detecting subtle abnormalities often missed by standard rigid, conventional coils. This leap in image quality means quicker and more accurate diagnoses, especially in complex cases.
InkSpace Imaging’s coils are up to 80% lighter and provide a 10–40% faster throughput. The design of the small body array is especially noteworthy for its flexibility which allows it to conform to a wide range of patient anatomies and sizes, significantly reducing scan times and minimising the duration patients need to remain still. This adaptability ensures all patients receive optimal imaging experiences, enhanced patient comfort, and significantly benefits technologists by streamlining the imaging process due to its high coil element density.
Peter Fischer, CEO of InkSpace Imaging, stated: “The FDA clearance of InkSpace Imaging’s small body array marks a pivotal moment in MRI technology advancement. Our suite of MR coils is a game-changer, offering total freedom in coil positioning and handling. What’s truly impressive is how our thin flexible coil contours to each patient’s body, offering comfort while enhancing image quality. It’s a win-win for patients and healthcare providers alike.”
Endovascular Engineering (E2) has announced US Food and Drug Administration (FDA) investigational device exemption (IDE) approval for its ENGULF US pivotal trial.
The study will evaluate the safety and effectiveness of the Hēlo thrombectomy system in treating pulmonary embolism (PE). The approval of the IDE follows the successful completion of the company’s 25-patient feasibility study.
“We are excited to be at the forefront of this innovative procedure with the completion of the ENGULF feasibility study. This significant achievement sets the stage for definitive results in the ENGULF pivotal trial. The Hēlo thrombectomy system represents a significant leap forward in pulmonary embolism treatment, and I am enthusiastic about investigating its full potential in the upcoming phase of the study,” said Jay Giri (University of Pennsylvania, Philadelphia, USA) the national principal investigator (PI) for the ENGULF feasibility study.
“We intend to build upon the robust foundation of clinical success we’ve seen thus far, solidifying the Hēlo thrombectomy system’s role as a transformative force in the treatment of pulmonary embolism,” said Andrew Klein (Piedmont Heart Institute, Atlanta, USA), the national PI for the ENGULF pivotal study.
Mike Rosenthal, CEO of E2, commented: “The positive results from our feasibility study give us confidence as we enter the pivotal phase. The Hēlo system introduces a differentiated technology with the potential to advance PE treatment options. Embarking on our ENGULF pivotal trial is a significant step, further validating the system’s safety and efficacy. It advances our efforts toward introducing this innovative technology to the market, ultimately helping patients with PE.”
Mentice recently announced that Ankyras, the company’s clinical decision support application, has received 510(k) clearance from the US Food and Drug Administration (FDA). The approval of this product by the FDA demonstrates the safety and effectiveness of Ankyras, and confirms Mentice’s commitment to providing innovative and high-quality healthcare solutions, as per a company press release.
The software is designed to assist interventional neuroradiologists in selecting the most suitable flow diverter prior to the interventional treatment of intracranial aneurysms. Ankyras offers an “intuitive and precise solution” for clinical treatment planning, leading to more accurate predictions than traditional methods, the release adds.
It is a platform that provides users with various functionalities to investigate device and treatment options in greater detail. Mentice states that the platform offers unique morphological assessment metrics that provide customers with a comprehensive and interactive analysis of all artery segments, ensuring they are better equipped to handle real-life challenges. The platform has technology supported by a “strong” intellectual property (IP) portfolio that enables users to evaluate final device length, local expansion and porosity, and precisely align the centreline to create accurate simulations for specific devices.
“Obtaining 510(k) clearance for Ankyras has been the number-one priority since the beginning of last year, and we are pleased that we have achieved this major regulatory milestone,” said Héctor Fernández, director of Ankyras Development. “The USA is the single largest market for flow diverters, and devices from all major manufacturers in the USA will now be available through Ankyras. This demonstrates our unwavering commitment to our expressed strategy of expanding into patient-specific decision support applications, which we believe will offer significant synergies with our existing training offering. By relying on a single provider for preprocedural clinical planning, 3D-printed physical simulation, and virtual simulation, we can offer significant benefits to both hospitals and industry.”
Moving forward, Mentice plans to continue improving the Ankyras solution by incorporating advanced functionalities and more treatment modalities, as well as integrating it with other Mentice solutions—especially the recently acquired Biomodex line of biorealistic haptic simulators.
A recent study published in Circulation concerning patients with chronic limb-threatening ischemia (CLTI) in the USA, has found that patients of low-income status and those who attended “safety-net” hospitals—facilities that treat patients regardless of insurance status or ability to pay—were more likely to receive low-intensity vascular care, which was associated with decreased long-term event-free survival.
As a precursor to their findings, lead investigator Eric A Secemsky (Beth Israel Deaconess Medical Centre, Boston, USA) et al detailed that inequities related to gender, race, ethnicity and socioeconomic factors, and subsequent risk of amputation in patients with CLTI, is “well documented”. However, the authors state that prior to their investigation little was known about how intensity of treatment drives clinical outcomes.
Using data from Medicare inpatient and outpatient hospital claims made between 2016–2019, beneficiaries over the age of 65 who were diagnosed with CLTI and underwent a major lower-limb amputation were identified. Patients were required to have at least one year of Medicare enrolment before major amputation to allow for the ascertainment of intensity of vascular care, and two years enrolment following the procedure to ensure adequate follow-up.
Secemsky and colleagues identified a total of 33,036 Medicare beneficiary major amputations, 7,885 (23.9%) of these which met inclusion criteria and were included in the study. Within this figure, they stated that 4,988 (68%) patients received low-intensity and 2,897 (36.7%) received high-intensity vascular care. The mean age of this cohort was 76.6 years of age, included 38.9% women, 24.5% Black patients, and 35.2% of reported low-income.
After multivariable adjustment, those of low income (odds ratio (OR)=0.65; 95% CI, 0.58–0.72]; P<0.001), male (OR=0.89, 95% CI, 0.81–0.98; P=0.019), and those who received care at a safety-net hospital (OR=0.87, 95% CI, 0.78–0.97; P=0.012) were most likely to receive low intensity of care before amputation. Conversely, the investigators highlight that high-intensity care was associated with a lower risk of all-cause mortality two years following amputation.
The authors emphasise that vascular care has “significantly improved” over the last 25 years and has gained a “better understanding of pathophysiology, greater pharmacological treatment options, and refinement of endovascular techniques”, which has caused the rate of major lower extremity amputations to “plateau”. However, Secemsky et al hazard caution at “[celebrating]” progress made before reflecting on the inequitable distribution of scientific advancements to all demographic communities.
“Disparities related to gender, race, ethnicity, and socioeconomic factors continue to affect chronically marginalised populations. Prior analyses have shown that low income and racial/ethnic minority adults are significantly more likely to undergo major lower extremity amputation. Our findings provide insights that may inform clinical, health system, and public health strategies to ensure more uniform and equitable delivery of vascular care in the USA.”
Regarding actions that are being taken to address these issues, the investigators highlight a recent update to the American Heart Association’s policy statement of guidelines to include a goal of reducing nontraumatic lower extremity amputations by 20% by 2030.
Secemsky and colleagues convey that this update advocates for “heightened awareness, improved clinician education, early detection, and systematic use of evidence-based therapies for peripheral arterial disease [PAD]”. The investigators concluded by stating that as efforts to raise public awareness of PAD and its risks continue, addressing “persistent” disparities in vascular care will be an “important extension” of this work.
HistoSonics, developer of a non-invasive platform and sonic beam therapy called histotripsy, has announced the treatment of the first patient in its pivotal #HOPE4KIDNEY trial.
The US Food and Drug Administration (FDA) approved the investigational device study earlier last year and it is designed to evaluate the safety and efficacy of the company’s Edison system to destroy targeted kidney tumours non-invasively and without the need for needles or incisions. The #HOPE4KIDNEY trial is a multicentre, open-label, single-arm trial, planned to enrol up to 68 patients.
Example of HistoSonics technology targeting kidney tissue to be destroyed in a non-invasive histotripsy procedure.
The procedure was performed by urologist Michael McDonald (AdventHealth Celebration in Kissimmee, USA), a leader in advanced urologic procedures, including robotics. “At the start of my surgical career in the 1990’s, open surgical techniques were the primary method of medical operations. However, this quickly changed with the introduction of laparoscopic surgery in the late 1990’s and robotic surgery in the early 2000’s,” said McDonald.
“I’m excited about the potential of emerging technologies such as histotripsy to improve patient safety and outcomes.” The procedure was conducted under the auspices of the AdventHealth Research Institute, where physicians and researchers are currently conducting more than 650 studies and clinical trials.
In 2020, there were an estimated 628,355 people living with kidney and renal pelvis tumours in the USA, and an additional 81,000 people to be diagnosed with kidney tumours in 2023. Current kidney therapies such as partial nephrectomy and thermal ablation are invasive and exhibit complications from bleeding and infection that non-invasive histotripsy may avoid. While surgical intervention is the “gold standard” in removing kidney tumours, a non-invasive approach with histotripsy provides the potential to destroy targeted tumours without damaging non-targeted kidney tissue. Additionally, histotripsy’s purely mechanical mechanism of cellular destruction could preserve function of the kidney’s urine collecting system.
“We are extremely excited to have McDonald and his team at AdventHealth Celebration treat the first patient at part of the #HOPE4KIDNEY trial,” said HistoSonics president and CEO, Mike Blue. “Our goal is to enable physicians to precisely target and destroy kidney tumours with our novel, non-invasive solution, avoiding the morbidity and complications seen with current invasive surgery or ablative techniques,” added Blue. The company expects to take advantage of key learnings from its initial Phase I kidney study, called the CAIN trial, and technical enhancements with its Edison platform during the #HOPE4KIDNEY study.
iVascular presented at Paris Vascular Insights (PVI) 2023 (8–10 November, Paris, France), delivering one year outcomes of the prospective, multicentre, consecutive, post-market study LUMIFOLLOW. This trial aimed to evaluate the performance of Luminor DCB in femoropopliteal lesions of 534 real-world patients, up to five years follow-up.
The trial included 77% patients with Rutherford stage higher than three from different centres from France. The average lesion length was 13cm and all type of TASC were included. In this cohort, 24% of the lesions were restenosis’, while the 76% were de novo. The bailout stenting rate was 43%, representing the percentage of TASC C and D lesions.
At one year follow-up an impressive 95.4% of freedom from target lesion revascularisation (fTLR) has been achieved, and a fTVR of 94.2%. At one year, patient symptomatology had decreased and 68% of the patients are asymptomatic (Rutherford stage 0). No safety concerns have been detected, the press release outlines.
Eric Ducasse (Centre Hospitalier Universitaire (CHU) de Bordeaux, Bordeaux, France), LUMIFOLLOW trial principal investigator, who was in charge of presenting the outcomes for the first time, stated: “LUMIFOLLOW confirms what we already knew about Luminor with a large population number: it’s an effective DCB for the treatment of femoropopliteal arteries. iVascular’s proprietary nanotechnology makes the difference vs other DCBs.”
iVascular reflect on the Luminor drug-coated balloon (DCB) in below-the-knee (BTK) outcomes obtained in the BIBLIOS trial one-year follow-up presented at the Paris Vascular Insights (PVI) 2023 (8–10 November, Paris, France).
BIBLIOS is a prospective, single-arm, multicentre study conducted in eight sites across Belgium, Italy and Spain.
A total of 150 subjects with critical limb-threatening ischemia (CLTI) Rutherford class 5 undergoing a significant degree of stenosis <70% or chronic total occlusion in P3 to the ankle-joint level lesions were enrolled with a follow-up of 12 months.
The efficacy primary endpoint of BIBLIOS is freedom from major adverse limb events (fMALE) at six months, defined as the absence of above-ankle target limb amputation or major reintervention to the target lesion(s). The primary safety endpoint is freedom from MALE at 30 days. Key secondary endpoints include target vessel functional flow assessment, freedom from clinical driven target lesion revascularisation (CD-TLR), amputation free survival, limb salvage, procedural success and wound healing status and time.
Koen Deloose (AZ Sint Blasius, Dendermonde, Belgium), the study’s principal investigator, highlighted that: “BIBLIOS’ objective is to confirm the safety and efficacy of Luminor in BTK in a well-defined study. Patient selection and wound care protocol are mandatory with this type of patients and illness. In BIBLIOS we tried to overcome some of the flaws in BTK trials/treatment: strategy, treatment, protocols and follow-up.”
12-month data of 150 subjects confirmed the excellent safety and efficacy of Luminor in BTK: at 1-year freedom from CD-TLR achieved was 86.6%. Freedom from MALE (95.6%) was maintained during the 12-month follow-up.
During his presentation at PVI, Deloose concluded: “These results showed that Luminor is a great option for the treatment of infrapopliteal lesions in patients with CLTI. It’s effective, it’s safe, and it’s available in all guidewire compatibilities and with small diameters”.
The roundtable focused on the current challenges in diagnosing and treating lower extremity revascularisation, knowledge and data gaps, and the potential role of IVUS in addressing these challenges. Experts shared their insights and experiences from the fields of interventional cardiology, interventional radiology, and vascular surgery. The expert consensus meeting was convened by SCAI and co-sponsored by: American Vein and Lymphatic Society (AVLS), American Venous Forum (AVF), Society of Interventional Radiology (SIR), Society for Vascular Medicine (SVM), and Society for Vascular Surgery (SVS).
“Improvements in outcomes following peripheral vascular intervention have lagged compared to other endovascular treatments, such as percutaneous coronary intervention. Both clinical experience and evidence support the greater use of peripheral IVUS to reduce adverse events and extend the patency of our lower extremity revascularisation procedures. By gathering experts from different specialties, we aimed to foster collaboration and exchange ideas to improve patient care for peripheral IVUS,” said Eric A Secemsky (Beth Israel Deaconess Medical Center, Boston, USA) lead author of the proceedings document. “The roundtable provided a unique opportunity to identify knowledge gaps and discuss how IVUS can enhance our understanding and treatment of peripheral arterial and deep venous pathology.”
Lower extremity revascularisation is a critical procedure used to restore blood flow to the legs and feet in patients suffering from peripheral arterial disease (PAD) and deep venous pathology. It is estimated that millions of people worldwide are affected by these conditions, which can lead to severe pain, non-healing wounds, and even limb loss if left untreated. Although angiography is the dominant imaging modality in revascularisation, it has inherent limitations. IVUS is a minimally invasive imaging technique that allows physicians to visualise the inside of blood vessels in real-time. It provides detailed information about the vessel wall, plaque composition, and blood flow characteristics, enabling more accurate diagnosis and treatment planning.
During the roundtable, participants highlighted the potential of IVUS in guiding revascularisation procedures, such as angioplasty and stenting, to optimise outcomes for patients. They also emphasised the need for further research and evidence to support the integration of IVUS into routine clinical practice.
“Vascular diseases are complex conditions requiring team-based care, research and information sharing to ensure that patients have access to appropriate, quality care for their condition,” said SIR President Alda L Tam (MD Anderson Cancer Center, Houston, USA). “Ongoing collaboration among these specialties is paramount to improving outcomes for patients worldwide.”
The roundtable concluded with a commitment to ongoing interdisciplinary collaboration and knowledge sharing among physicians. Participants agreed that treatment standards, formal training programs and global quality metrics remain needed to improve patient care.
GE HealthCare has entered into an agreement to acquire MIM Software, a provider of artificial intelligence (AI)-enabled image analysis and workflow tools across multiple care areas, including oncology, urology, neurology, and cardiology
GE HealthCare expects to leverage MIM Software’s imaging analytics and digital workflow capabilities across various care areas to accelerate innovation and differentiate its solutions for the benefit of patients and healthcare systems around the world, the company says in a press release.
MIM Software’s portfolio of innovative imaging solutions provides a variety of beneficial features, including: the integration of diagnostic images from multiple modalities into treatment plans; automation to help reduce repetitive tasks and manual interventions; quantitation and advanced processing in diagnostic imaging and nuclear medicine to help determine therapy response; and a platform to assist with Theranostics imaging and dosimetry.
GE HealthCare expects to integrate MIM Software solutions into its advanced visualisation offerings to facilitate AI-based segmentation and contouring as well as dosimetry analysis for patients across their treatment journeys and in the growing fields of radiology, molecular imaging, and radiation oncology.
“We are committed to providing comprehensive, connected devices and digital solutions that enable providers to improve patient care across multiple specialties,” says Peter Arduini, president & CEO of GE HealthCare. “We expect our efforts to bring these two complementary organisations and innovative product portfolios together to strengthen our capabilities as a leading provider of integrated imaging systems, analytics, and advanced digital workflows across several care areas and pathways – including Theranostics, radiation oncology, urology, neurology and cardiology. Now and in the future, we are working to transform patient care.”
“We are excited by the prospect of joining GE HealthCare and thrilled to share this exciting news,” adds Andrew Nelson, CEO of MIM Software. “Over the past two decades, we have worked to develop innovative vendor agnostic products and deliver quality services to earn the trust of our customers—this will not change. As a part of GE HealthCare, we anticipate developing new and increasingly integrated digital solutions to meet our customers’ most complex and pressing needs, today and into the future. Together, we will build upon our shared legacies of enhancing patient care.”
Founded in 2003, MIM Software is headquartered in Cleveland, Ohio, with additional offices in China and Belgium. The consummation of the transaction is subject to customary closing conditions, including regulatory approvals. Financial details of the transaction have not been disclosed publicly.
Percutaneous transmural arterial bypass using the Detour system
Endologix recently announced that the US Centers for Medicare & Medicaid Services (CMS) has granted a Transitional Pass-Through (TPT) payment for the Detour system, effective since 1 January 2024.
The TPT payment was created to facilitate patient access for qualifying new medical technologies that substantially improve the diagnosis or treatment of Medicare beneficiaries. TPT will provide hospitals with additional device reimbursement when the DETOUR system is used for eligible cases in the hospital outpatient setting. Details on the TPT, code C1604, can be found in the January 2024 Update of the Hospital Outpatient Prospective Payment System (OPPS), accessible on the CMS website and the Endologix website.
Percutaneous transmural arterial bypass (PTAB) with the Detour system, a US Food and Drug Administration (FDA) Breakthrough Device, received premarket approval in June 2023. Endologix states that PTAB offers a novel approach to treating complex peripheral arterial disease (PAD). The company details that Detour enables physicians to bypass lesions in the superficial femoral artery, by using conduits routed through the femoral vein via a transmural passage, to restore blood flow to the leg. According to Endologix, this approach is effective for patients with long lesions (20–46cm in length), those who have already undergone failed endovascular procedures, or those who may be suboptimal candidates for open surgical bypass.
“Being awarded the TPT designation marks an important milestone in our reimbursement strategy and the commercial launch of the Detour system for treating patients with complex PAD. At Endologix, our core mission is to deliver healthcare innovation to improve the lives of patients with vascular disease. With the support from CMS for qualified patients, we eagerly anticipate more patients to benefit from PTAB,” said Matt Thompson, president and CEO of Endologix.
The company advises that the Detour system is indicated for use for percutaneous revascularisation in patients with symptomatic femoropopliteal lesions from 200–460mm in length with chronic total occlusions (100–425mm) or diffuse stenosis >70% who may be considered suboptimal candidates for surgical or alternative endovascular treatments. The Detour system, or any of its components, is not for use in the coronary and cerebral vasculature.
Rescue stent placement following a failed thrombectomy procedure has demonstrated “good outcomes” and a low risk of clinically significant bleeding in a multiethnic cohort of acute ischaemic stroke patients from the Middle East, Africa and Asia. Writing in the Journal of Vascular and Interventional Radiology (JVIR), researchers conclude that their results are “similar” to those seen with post-thrombectomy rescue stenting in the published literature.
Yahia Imam (Hamad Medical Corporation, Doha, Qatar) and colleagues initially note that, while mechanical thrombectomy has “revolutionised” stroke therapy in recent years, rescue stent placement following an unsuccessful thrombectomy “remains controversial”—particularly for Asian patients, in whom intracranial atherosclerotic disease (ICAD) is more prevalent and is believed to contribute more significantly to occurrences of re-occlusion versus in Western populations.
As such, the authors of the JVIR study conducted a retrospective, observational review of a multiethnic stroke database to evaluate the safety and effectiveness of rescue stenting in acute stroke patients with a large vessel occlusion (LVO) refractory to a thrombectomy procedure.
Their primary outcomes included incidence of intracranial haemorrhage (ICH), recanalisation score, and favourable prognosis (modified Rankin scale [mRS] score ≤2), at 90 days. Imam and colleagues also detail that, after stent placement, an “aggressive” antiplatelet protocol was followed with glycoprotein IIb/IIIa infusion in all patients included in the analysis.
The review drew comparisons between patients from the Middle East and North Africa (MENA) region, and those from other regions. Fifty-five patients (87% men; mean age, 51.3 years) were ultimately included; 32 were from South Asia (58%), 12 from the MENA region (22%), nine from Southeast Asia (16%), and two from elsewhere (4%; West Africa and East Asia).
The authors report that successful recanalisation (modified thrombolysis in cerebral infarction [mTICI] score 2b/3) was achieved in 43 patients (78%), while symptomatic ICH occurred in two patients (4%). A favourable outcome at 90 days was also seen in 26 of the 55 patients (47%).
Imam and colleagues further detail that—apart from a significantly higher average age (mean, 62.8 years vs. 48.1 years) and greater coronary artery disease burden (four [33%] vs. one [2%], p<0.05)—MENA patients demonstrated risk factors, stroke severity, recanalisation rates, ICH rates, and 90-day outcomes, that were all similar to those seen in patients from South and Southeast Asia.
Their findings within a multiethnic cohort of MENA and South Asian patients are therefore “comparable” to prior reports from East Asia, the authors aver, and constitute level-three evidence that rescue stent placement may be deemed a “viable option” in cases of refractory LVO due to probable atherosclerosis in acute ischaemic stroke patients. Utilisation of aggressive post-stent placement platelet inhibition was comparably safe and effective as well, Imam and colleagues state.
AnX Robotica, a company involved in the development of gastrointestinal visualization technologies, announces US Food and Drug Administration (FDA) clearance of their NaviCam ProScan, an artificial intelligence (AI) assisted reading tool to “revolutionise” the field of gastroenterology.
Through de novo submission process, the FDA has granted clearance for ProScan, making it the first AI assisted reading tool designed to aid small bowel capsule endoscopy reviewers for adult patients in whom the capsule endoscopy images were obtained for suspected small bowel bleeding. AnX Robotics ProScan is a step forward in capsule endoscopy by enabling physicians with the latest technology to efficiently care for their patients, a press release states.
“As a clinician deeply immersed in the field of gastroenterology, I am thrilled to witness the FDA clearance of ProScan. This groundbreaking AI assisted reading tool represents a pivotal advancement in small bowel capsule endoscopy, particularly for patients suspected of gastrointestinal bleeding,” stated Cristiano Spada (Gemelli Hospital, Rome, Italy). “This clearance marks a significant leap forward in our pursuit of elevating patient care standards and signifies a new era in gastroenterological diagnostics.”
AnX Robotica’s ProScan software is said to complement clinician expertise. Importantly, it is not designed to replace clinical decision-making of the physician, but serves as a support system, enabling healthcare professionals to make well-informed and efficient decisions with the support of AI-assisted readings.
“We are delighted to announce the FDA clearance of NaviCam ProScan, a transformative AI assisted reading tool that addresses a critical need in the realm of small bowel capsule endoscopy,” said Stu Wildhorn, vice president of marketing and product management at AnX Robotica. “ProScan’s clearance underscores its potential to significantly enhance diagnostic workflows, allowing clinicians to make more informed decisions in a timely manner.”
Gore has announced the first patient implantation of the Gore ascending stent graft in the ARISE II trial, describing this as an exciting step in the development of treatments for pathologies involving the ascending aorta using endovascular repair rather than traditional open surgery.
On 1 December, national principal investigator Eric Roselli (Cleveland Clinic, Cleveland, USA) performed the case at Cleveland Clinic alongside study investigators Patrick Vargo and Frank Caputo. The patient was identified as a candidate for the study after presenting with a fusiform aneurysm of the ascending aorta and aortic arch.
The ARISE II study is the first multicentre pivotal study approved by the US Food and Drug Administration (FDA) investigating the use of a minimally invasive endovascular device to treat the ascending aorta. The study investigates the treatment of isolated lesions as well as chronic and residual type A dissections involving the ascending aorta. The Gore ascending stent graft is designed for investigational use in combination with the Gore Tag thoracic branch endoprosthesis.
“The treatment of the ascending aorta has long been a ‘final frontier’ in endovascular surgery. ARISE II is a significant step forward as we search for minimally invasive options that can be offered to higher risk patients,” said Roselli.
The ARISE II study will investigate how an endovascular stent graft, delivered via catheter, may be used to line the diseased portion of the ascending aorta as a potential alternative to open surgical repair. Endovascular technologies have been applied to other regions of the aorta to reduce the risk of complications and recovery times, but no endovascular device is currently approved for the ascending aorta.
“Our patient is recovering well. Having a minimally invasive alternative would be a significant advancement for patients not suitable for open surgery,” said Caputo.
Disclaimer: The suggestions and other information, which may include both Merit and third-party products, are for the practitioner’s convenience and for general information purposes only. This information does not constitute medical or legal advice, nor is it meant to endorse or guarantee the suitability of any of the referenced products or methods for any specific patient or procedure. Before using, refer to the instructions for use (IFU) for indications, contraindications, warnings, precautions, and directions for use. Before using any product, refer to the IFU for indications, contraindications, warnings, precautions, and directions for use.
Pavan Najran (The Christie Hospital NHS Foundation Trust, Manchester, UK), clinical lead for interventional radiology (IR) and consultant clinical and interventional radiologist, explores solutions for gaining access and management in the distal radial route specifically within interventional oncology setting.
The transition from femoral to radial access intervention has been supported by favourable evidence demonstrating improved mortality and morbidity outcomes1. In addition to this, radial access has been shown to be favourable to patients, a preference that has been supported by numerous studies2 which reference considerable patient data.
Traditional radial access has limitations, including ergonomics and patient positioning, which become apparent during longer procedures.
Distal radial access was first performed and reported in 20173 by Ferdinand Kiemeneij (Onze Lieve Vrouwe Gasthuis, Amsterdam, The Netherlands) et al and has since been adopted by both the cardiology and radiology groups. In the setting of interventional oncology, radial access offers significant benefits, particularly when performing prolonged procedures in patients with deranged clotting function, a group of patients commonly encountered in this setting.
How to anatomically navigate distal radial access
The anatomical snuff box houses the distal radial artery, a distal branch of the main radial artery, and as a result any occlusion of the vessel locally is less likely to compromise blood supply to the hand, adding to its advantage.
The anatomical snuff box is a depression at the base of the thumb. It is bordered by the extensor polices longus medially and the abductor polices longus, as well as the extensor pollicis brevis laterally. These structures can be identified easily when the thumb is fully extended.
The vessel is punctured distal to the superficial palmer branch and proximal from the pollicis brevis artery.
Distal radial access and ultrasound techniques
Advantage of a distal approach is that the access arm can be moved into various positions given the position of the hand at puncture, even allowing for left arm access from a right sided patient position.
The technique used for traditional radial access can be translated into distal techniques, however there are a number of points that require consideration.
The hand can be placed in a more natural position for the patient, with the thumb pointing towards the celling. Traditional radial access requires the palm surface of the hand to be facing the ceiling, which can become uncomfortable during prolonged procedures.
Ultrasound guided access is a must due to the marginal reduction in vessel diameter and close abutment of the adjacent tendons. A high-frequency probe with a small footprint is recommended due to the smaller surface contact; a musculoskeletal (MSK)-based hockey stick probe is recommended if available.
Managing distal radial access
Enable easier puncture, supporting a selection of sheath sizes and reduce risk of spasm.
A combination local anaesthetic and glyceryl trinitrate (GTN) (9ml of 1% lignocaine + 200mcg GTN) should then be infiltrated around the vessel carefully ensuring the vessel is bathed in the medication extending from the desired puncture site, proximally to the main radial artery. The local anaesthetic will provide the necessary analgesia, and the GTN will dilate the vessel; this will make the puncture easier and ensure that larger sheath sizes can be placed without difficulty. Further to this, proximal GTN and anaesthetic infiltration will ensure the main radial trunk is dilated and therefore reduces the risk of spasm as the sheath is inserted.
A 21-gauge needle is then used to puncture the vessel, which should be performed under ultrasound guidance in a transverse plane—this ensures the vessel is punctured in the 12 O’clock position reducing the risk of sub-intimal cannulation. An intraluminal puncture should produce prominent blood flow from the needle. Furthermore, a 0.018 guidewire should then be placed through the needle intraluminally. If there is any resistance to the wire insertion, a sub-intimal or side branch location is likely, so readjustment is required. A confirmatory ultrasound can then be performed ensuring an intraluminal location.
The sheath can then be inserted, a skin incision should not be performed as the traction from the skin will prevent the sheath from falling out. Again, a confirmatory ultrasound can be performed, ensuring an intraluminal location. Once in place, a cocktail of heparin (5000iu) and GTN (200mcg) should be instilled through the sidearm. Calcium channel blockers (verapamil 2.5mg) can also be used within the cocktail however, this should be used with caution, as if the patient is currently on antihypertensives, this can result in sudden hypotension.
Once the sheath is in place, access into the leading vessel is achieved via the catheter inserted into the sheath and a hydrophilic wire preloaded within it, allowing negotiation through to the aortic arch under fluoroscopic guidance.
Once the aortic arch is negotiated the catheter of choice is based on the target vessel. Pelvic vessels may favour a less aggressive angled tip catheter, whereas coeliac access intervention may require a more exaggerated angled catheter.
References
Chiarito M, Cao D, Nicolas J, Roumeliotis A, Power D, Chandiramani R, Sartori S, Camaj A, Goel R, Claessen BE, Stefanini GG, Mehran R, Dangas G. Radial versus femoral access for coronary interventions: An updated systematic review and meta-analysis of randomized trials. Catheter Cardiovasc Interv. 2021 Jun 1;97(7):1387–1396. doi: 10.1002/ccd.29486. Epub 2021 Jan 28. PMID: 33507598.
Satti SR, Vance AZ, Golwala SN, Eden T. Patient Preference for Transradial Access over Transfemoral Access for Cerebrovascular Procedures. J Vasc Interv Neurol. 2017 Jun;9(4):1–5. PMID: 28702112; PMCID: PMC5501120.
Left distal transradial access in the anatomical snuffbox for coronary angiography (ldTRA) and interventions (ldTRI) Kiemeneij F.EuroIntervention.2017;13:851–857.
Microbot Medical, developer of the Liberty endovascular robotic surgical system, has entered into a collaboration agreement with Corewell Health.
The objective of the collaboration, which will take place in multiple phases, is to enable telerobotics between remote centres by utilising the Liberty robotic system. The agreement with Corewell Health includes the right to mutually evaluate the Liberty system for remote procedures, which will be led by Ryan Madder (Spectrum Health, Grand Rapids, USA).
“Being able to connect between remote sites, especially at rural areas, has been a passion of mine for years, and as such I’m excited about the potential this collaboration can bring to benefit many patients in the USA and across the world,” said Madder.
“We are excited for the opportunity to collaborate with Corewell Health and Dr Ryan Madder, innovators in the field of robotics and healthcare. Working together with a health system such as Corewell, which provides care and services in 21 hospitals, 300+ outpatient locations and several post-acute facilities, to enhance the telerobotic feature of the Liberty system, fits well with our mission to enable accessibility to any user, anywhere across the world for any endovascular procedure,” said Harel Gadot, chairman, president and CEO of Microbot Medical. “We continue to demonstrate that the interest shown by leading medical centres in our Liberty system is a testament to its potential impact in the endovascular interventional space.”
Terumo Medical, announces the launch of its new AZUR HydroPack peripheral coil system in the USA. The AZUR HydroPack coil system is a soft, universal-shaped platinum and hydrogel coil designed to find and fill empty space within the vessel. It is also the only packing coil to use proprietary designed hydrogel technology to create a gel core for mechanical occlusion, a feature of AZUR peripheral coils. Terumo received US Food and Drug Administration (FDA) clearance for the AZUR HydroPack coil system earlier this year.
“The AZUR HydroPack peripheral coil system provides optimised stability and precise delivery. Its versatility and efficiency provide interventional radiologists and vascular surgeons with an ideal solution to ensure the best possible outcome for patients,” said Chris Pearson, executive vice president, Terumo Interventional Systems (TIS)—North America. “Its state-of-the-art design and uniform microcatheter compatibility set it apart from other packing coils. This is important as the market for peripheral coil embolization expands and diversifies.”
The AZUR HydroPack peripheral coil system has a true 0.018” primary wind and is available in long lengths—ranging from 5 to 60cm—making it the longest gel core coil on the market, the press release states. It allows for flexible sizing and can be deployed through 2.4Fr or 2.8Fr microcatheters in a single-coil platform. With no requirements for vessel-diameter sizing other than placement of an anchor coil, this may reduce the amount of inventory required to support a wide variety of peripheral embolization procedures. The soft coil design paired with an enhanced pusher allows for ease of delivery, optimised trackability and microcatheter stability.
“Our unique hydrogel technology is a key differentiator as it creates a gel core and promotes new tissue growth versus the basic thrombogenic response of a traditional platinum coil. It also will allow physicians to fill open vessel space confidently and efficiently while minimising reperfusion,” said Michael J Martinelli, chief medical officer for Terumo. “Additionally, the tight packing and durable occlusion associated with hydrogel technology put the AZUR HydroPack coil system in a category of its own in the peripheral coil market.”
The AZUR HydroPack peripheral coil system—the latest addition to the TIS embolotherapy portfolio—is designed to fill volume behind the Terumo AZUR CX peripheral coil system for vessel occlusion and to fill volume inside of the AZUR framing coil system for aneurysm occlusion.
This image shows a woman with pelvic mass and BRCA1 mutation. The arrows point to the right and left adnexa. Co-registered ultrasound shows a cyst with solid component in the right adnexa (B). Image C shows the relative total hemoglobin in the lesion, and image D shows the oxygen saturation, both of which are important predictors of malignancy. Pathology revealed a stage I high-grade serous carcinoma of the right ovary and fallopian tube.
This image shows a woman with pelvic mass and BRCA1 mutation. The arrows point to the right and left adnexa. Co-registered ultrasound shows a cyst with solid component in the right adnexa (B). Image C shows the relative total haemoglobin in the lesion, and image D shows the oxygen saturation, both of which are important predictors of malignancy. Pathology revealed a stage I high-grade serous carcinoma of the right ovary and fallopian tube.
Published in the December 2023 issue of Ultrasound in Obstetrics and Gynaecology, Quing Zhu (Washington University, St Louis, USA) et al state that they have developed a novel imaging method which combines photoacoustic imaging (PAI) with ultrasound to better diagnose lesions in the ovaries and adjacent adnexa.
Without a standard screening test that can assist with early detection of ovarian cancer, ultrasound imaging is most commonly used. Ultrasound in this setting is not always accurate, the researchers exposit, which has historically led some patients to have their ovaries unnecessarily removed.
In developing this technique, Zhu and colleagues incorporated functional biomarkers with PAI which illuminates tissue with a near-infrared light at specific wavelengths that are then absorbed differently by oxygenated and deoxygenated haemoglobin.
Enrolling 68 women with ovarian/adnexal lesion(s) suggestive of malignancy referred for oophorectomy—the surgical removal of the ovaries/adnexal lesions, participants underwent a clinical ultrasound examination followed by a co-registered ultrasound and PAI prior to oophorectomy. The researchers note that each ovarian/adnexal lesion was graded by two radiologists using the ovarian-adnexal reporting & data system (O-RADS) scale.
Among the included patients, 93 lesions were identified overall; 14 patients were found to have malignant lesions in their ovaries or adnexal regions, two patients had malignant fallopian tubes, and 52 patients had benign lesions. When comparing the malignant and benign lesions, Zhu et al found that the relative total haemoglobin in patients with malignant lesions in the ovaries and in the adnexal region was 1.8 times higher than in those with benign lesions. Blood oxygen saturation was 5% lower in those with malignant lesions, though this was not a statistically significant difference.
The team found that the most important predictors of malignancy were relative total haemoglobin, the O-RADS score, presence of the cancer antigen CA 125, and percentage of blood oxygen saturation (sO2). Their model, which incorporates all four features, achieved “superior performance” for sensitivity of 100% and specificity of 82%.
“Photoacoustic imaging combined with ultrasound provides complementary diagnostic imaging data involving structure and function,” Zhu said. “The ultrasound localises the lesion, and the photoacoustic images inform tumour haemoglobin content and percent of blood oxygen saturation.”
Co-principal investigator Matthew Powell (Washington University, St Louis, USA) expanded on the value of their findings: “Women frequently develop ovarian cysts, which cause a great deal of worry. This technology should quickly and easily be able to help assure both the doctor and the patient that most of these can be watched, and unnecessary surgery can be avoided. These surgeries can lead to loss of fertility and early menopause. This technology and other imaging advancements could be immensely helpful to improve the lives of our patients.”
Cary Siegel (Washington University, St Louis, USA)—a fellow co-principal investigator who worked alongside Powell and Zhu—adds that carrying out an assessment of an adnexal mass can be “challenging” for experienced radiologists, as “many different benign and malignant causes are often among possibilities for diagnosis”. However, by deploying their novel photoacoustic ultrasound technique “accuracy and confidence” can be given to radiologists to improve early diagnosis and treatment of ovarian cancer. “With early diagnosis, our ultimate goal is to improve ovarian cancer survival. Working with Powell, Zhu and her engineering team has been a highlight of my medical career,” Siegel concludes.
Micro Medical Solutions (MMS), an innovator in the field of microvascular intervention to improve clinical outcomes and quality of life in patients with chronic limb-threatening ischaemia (CLTI), announced that it has completed its USA pivotal clinical study enrolment evaluating the safety and effectiveness of the MicroStent system compared to the current standard of care, PTA (percutaneous transluminal angioplasty). The MicroStent system has already obtained CE mark approval for use in the European economic area (EEA).
STAND (A Clinical Evaluation of the MicroSTent PeripherAl Vascular SteNt in subjects with Arterial Disease Below the Knee) enrolled its final patient earlier this month marking the completion of the study. MicroStent is a vascular stent specifically designed to achieve and maintain tibioperoneal arterial patency improving blood flow and wound healing for below-the-knee amputation reduction in patients with CLTI resulting from progressive peripheral artery disease (PAD).
“I would like to thank the investigators and the research teams for their dedication, participation, collaboration and tremendous effort to help this complex and difficult patient population. I’m excited to continue to provide research expertise to the company and discuss the study results when available,” said lead investigator, Robert E Beasley (Palm Vascular Centers, Miami Beach, USA).
“CLTI is the most severe clinical manifestation of PAD. We are excited to see the data unfold to further understand the impact of angiosome directed endovascular intervention and its impact on wound healing, limb salvage and patient living independence. We are warmly appreciative to our patient population that participated in the study. The study’s goal has always been to demonstrate a lower amputation rate thereby, lowering the devastating mortality rate associated with limb loss,” commented Rita Jacob, vice president of clinical affairs.
“This is an encouraging step forward for MMS, millions of patients battling CLTI every day and clinicians treating and caring for these patients,” said CEO, Gregory Sullivan. “MMS developed the MicroStent platform in response to patients’ needs, and we are excited to move closer to putting MicroStent in the hands of interventionalists treating CLTI in the USA.”
Kaneka Corporation has acquired all shares of Japan Medical Device Technology Co and has made it a wholly owned subsidiary.
Kaneka manufactures and sells endovascular catheters, which are devices used in the treatment of cardiac, peripheral vascular, and cerebrovascular diseases. The company is aiming to expand its business in this treatment of coronary artery diseases such as atherosclerosis, the company said in a statement.
In the statement, Kaneka notes that Japan Medical Device Technology Co has “high technological capabilities in the research and development of coronary stents and is one of the leaders in the development of bioresorbable stents”.
In November, the most popular stories from Interventional News included stories from our latest issue concerning the global lack of interventional radiology (IR) devices for paediatric patients; an international heatmap of IR’s progression to primary specialty; a study which found moral injury to be prevalent among interventional radiologists in the USA; and Ian McCafferty’s (The Radiology Clinic, Birmingham, UK) delivery of the Graham Plant lecture at this year’s British Society of Interventional Radiology (BSIR; 8–10 November 2018, Newport, UK).
OncoSil Medical, a medical device company focused on localised treatments for patients with locally advanced pancreatic cancer (LAPC) announces the first patient has been treated in the PANCOSIL investigator initiated clinical trial on 28 November 2023.
“Are we truly upholding the notion that our children are the most valuable good of our society?”
Arguing that the lack of adequate medications and IR devices for children “tells a different story”, Premal Patel, Fernando Gómez Muñoz, and Alessandro Gasparetto survey the current state of paediatric IR and the global device deficit.
Inari Medical has announced the first patient enrolment in PEERLESS II. This prospective, global, multicentre randomised controlled trial (RCT) compares the outcomes of intermediate-risk acute pulmonary embolism (PE) patients treated with the FlowTriever system against those treated with traditional anticoagulation therapy alone.
A recent study concerning moral injury (MI) among interventional radiologists has found that the condition is “prevalent” throughout the field, and has been shown to negatively correlate with quality-of-life (QoL) indicators.
“If we do not take control and if we do not take charge of our own destiny, we will be jeopardising the future sustainability of IR. Maybe I am being a little nihilistic, but I believe that we must start changing things and it needs to happen sooner rather than later.”
Nick Brown, Raman Uberoi, Michael Lee, and Parag Patel discuss the current structure of IR and the value of obtaining specialty status, tracking the field’s burgeoning recognition, concurrent problems and future stability.
Patients diagnosed with benign bone tumours will be relieved to know that these are not malignant, and some tumours will involute spontaneously. However, this natural history can be unpredictable, and tumours can be associated with significant pain, pathologic fracture, or potential for growth and compression of critical structures such as nerves.
Fluidx Medical has released information about their new ULTRA embolic platform designed to make therapeutic embolization procedures safer, better, and faster, as the recent press release states.
Honoured as the BSIR travelling professor, Ian McCafferty gave the Graham Plant lecture at the annual meeting. Titled ‘Acute trauma intervention: Have we got it right?’
Baird Medical, leading microwave ablation (MWA) medical device developer and provider in China, has announced that its subsidiary, Betters Medical, has received clearance from the US Food and Drug Administration (FDA) under Section 510k, to begin marketing its portfolio of MWA systems and disposable MWA needles as regulatory class II devices in the USA.
Summa Therapeutics, a specialty angioplasty balloon medical device company, has announced that its innovative line of injectable angioplasty balloon catheters has been cleared for marketing by the US Food and Drug Administration (FDA) for the treatment of peripheral artery disease.
Summa’s new Finesse Injectable angioplasty balloon catheters are cleared by the FDA for percutaneous transluminal angioplasty (PTA) treatment of peripheral artery disease including iliac, femoral, popliteal, infra-popliteal, renal arteries and AV dialysis access.
The Finesse injectable angioplasty balloon catheter differs from conventional angioplasty balloon catheters because it provides a port for the injection of radiopaque contrast material or other fluids in addition to performance of balloon angioplasty.
“We are delighted to receive FDA clearance for our Finesse angioplasty balloon product line,” said Timothy Murphy, Summa’s chief executive officer. “This achievement underscores our commitment to delivering innovative, minimally invasive vascular solutions that address critical unmet needs in the field of interventional medicine. We believe that the Finesse product line has the potential to revolutionise angioplasty procedures, providing physicians with an advanced toolset to treat patients with critical limb-threatening ischaemia [CLTI].”
The new angioplasty balloon catheter was designed to facilitate increasingly complex below-the-knee angioplasty procedures for patients with CLTI, a risk factor for leg amputation. The Finesse Injectable angioplasty balloon catheter is the first injectable angioplasty balloon catheter designed to treat small arteries in the calf. The combination of a diagnostic catheter and angioplasty balloon catheter in one device is expected to reduce catheter exchanges, lower contrast doses, and shorten procedure times, and lead to better patient outcomes and lower costs. Summa plans to launch the product line in the fourth quarter of 2023 in the USA.
BD, a leading global medical technology company, have launched a new advanced ultrasound system designed to help improve clinician efficiency when placing peripherally inserted central catheters (PICCs), central venous catheters, IV lines and other vascular access devices.
The SiteRite 9 ultrasound system is an all-in-one system designed with a user-friendly experience on an updated 15.6 inch touch screen with enhanced image quality that provides industry-leading catheter placement tools and technologies to support clinicians during the vascular access device insertion process. The system includes integrated visualisation tools such as the Cue needle tracking system (BD) to provide nurses with continuous and real-time needle tracking, and the Sherlock 3CG+ Tip confirmation system (BD) to ensure proper catheter tip navigation and location.
“Our latest innovation in ultrasound technology is designed to make vascular access care delivery easier and more efficient for clinicians—whether they have been on the job for years or are new to the field,” said Eric Borin, worldwide president of medication delivery solutions at BD. “By combining our decades of leadership in vascular access with voice-of-the-customer enhancements, we have developed a best-in-class solution to aid in insertion success on the first attempt and reduce the need for repeated needlesticks to deliver a better care experience for everyone involved.”
SiteRite 9 also features smart, connected technology such as vessel assessment tools that automatically detect the vessel, then pair with vessel measurement tools to help clinicians select the appropriate catheter, so they can make an informed decision every time. Additional system capabilities include patient data look up with information capture, auto-filling capabilities and records transfer to help support clinician workflow.
Transit Scientific, a Utah-based medical device company specialising in innovative solutions for vascular procedures, has announced the US Food and Drug Administration (FDA) clearance of its microcatheter designed for the precise delivery of a broad range of embolic agents. This milestone marks a significant advancement in microcatheter technology, offering clinicians a differentiating new tool to enhance patient care.
Microcatheters are commonly used to deliver therapeutic embolic agents, and inject contrast media, during complex endovascular procedures.
Current microcatheters come with various limitations, sacrificing low profile for flow rates, and sacrificing trackability for torque response. Current wire-braided catheters limit torquability and control, making it challenging to reach distal vasculature and oftentimes requiring catheter escalation. The current hypotube catheter designs limit trackability performance. Many current microcatheters also come with limitations on embolic compatibility and flow rates.
The XO Cath microcatheter is designed to deliver new levels of trackability, torque response, and embolic compatibility for improved treatment delivery. The non-tapered, metal-alloy construction is designed to offer unparalleled precision translating to superior control over embolic material placement, ensuring optimal results in minimally-invasive procedures.
Richard Saxon (Tri-City Medical Center, Oceanside, USA), a renowned interventional radiologist, shared their thoughts about the newly cleared microcatheter, said: “This breakthrough technology could substantially improve the successful completion of embolic procedures. Its trackability, precision, and embolic compatibility features will likely make a significant difference in patient care.”
This 510k clearance includes the XO Cath 2F microcatheter with 0.021″ ID for use with standard 0.014″ and 0.018″ guidewires, and the XO Cath 2.6F microcatheter with 0.027″ ID for use with standard 0.014″, 0.018″, and 0.021” guidewires. Both microcatheters are offered with either or straight or bern-shaped tip and are available in 90cm, 110cm, 130cm, 150cm, 175cm, and the class-leading 220cm working lengths for radial access procedures.
“This FDA clearance underscores our commitment to developing cutting-edge medical solutions that cater to the evolving needs of interventional radiologists,” says Transit Scientific chief operations officer, Jennifer Arnold. “This innovative microcatheter technology represents a fusion of innovation, precision, and safety, addressing critical challenges in embolic delivery procedures.”
Fluidx Medical has released information about their new ULTRA embolic platform designed to make therapeutic embolization procedures safer, better, and faster, as the recent press release states.
Embolization is a minimally invasive catheter-based procedure that blocks blood flow to targeted blood vessels and organs. Over US$3.5 billion per year is spent on tiny embolic particles, metal coils, and liquid-to-solid devices to treat internal bleeding, aneurysms, fistula, uterine fibroids, tumours, prostates, malformations, and other conditions throughout the body.
“Embolic coils depend on the blood’s ability to clot and often require multiple coils to achieve complete occlusion,” said Ryan O’Hara, interventional radiologist and medical director at Comprehensive Integrated Care in Salt Lake City, Utah, USA. “Embolic particles are hard to visualise during delivery, increasing the risk of off-target embolization and leading to unintended harm of nearby tissues.”
The ULTRA platform is designed to address the needs of patients requiring moderately distal to proximal embolization. Unlike other embolic devices, ULTRA does not require refrigeration, use toxic dimethyl sulfoxide (DSMO), require special delivery catheters, need special mixers or preparation stations, or glue catheters into the body.
“We have seen a single delivery of ULTRA block a targeted vessel region quickly in an area that would usually require several coils,” noted Danny Smith, vice president of research and development at Fluidx Medical. “ULTRA is visible under X-ray giving clinicians greater control and visualisation of the embolic to ensure safe, accurate delivery.”
The success of the ULTRA embolic platform follows on the heels of another large milestone for Fluidx Medical, as their flagship product the GPX Embolic Device is currently under investigational device exemption (IDE) review with the US Food and Drug Administration (FDA). GPX, which completed a successful multicentre clinical trial as a multi-use embolic in 2023, focuses on embolization procedures where there is need for deep distal penetration.
Clinical professor of radiology Mishal Mendiratta-Lala (Michigan, USA), expands on the first data release from the #HOPE4LIVER trial, presented during the FIRST@CIRSE session at this years Cardiovascular and Interventional Radiological Society of Europe (CIRSE) meeting.
“We are very excited about histotripsy as a new form of liver directed treatment for liver cancer” states Mendiratta-Lala, noting that sights are set on future US Food and Drug Administration (FDA) approval to begin treating patient populations in both the USA and Europe with both primary and metastatic cancer, which she believes will “[add] another form of therapy to our arsenal”.
Video Attribuitons
Image: Jacob/stock.adobe.com
Music: Quirky-tension-investigation-(sleek-sneak)/performed by Apollo Audio/FineTune Music/stock.adobe.com
OncoSil Medical, a medical device company focused on localised treatments for patients with locally advanced pancreatic cancer (LAPC) announces the first patient has been treated in the PANCOSIL investigator initiated clinical trial on 28 November 2023.
The first patient has been treated in PANCOSIL investigator initiated clinical trial on 28 November 2023 in Amsterdam. This comes in the wake of ethics approval for the trial being granted in June 2023.
PANCOSIL aims to evaluate the safety and feasibility of computed-tomography (CT)‐guided percutaneous radionuclide therapy with the OncoSil device in patients with non‐progressive locally advanced pancreatic cancer. In all, 20 patients will be treated with the OncoSil device by percutaneous application over the course of the trial. This will, in turn, expand the available users who can deliver the OncoSil device.
Most of the funding contribution by OncoSil has already occurred in previous quarters, the press release states. Martijn Meijerink (Amsterdam University Medical Centers, Amsterdam, The Netherlands) said: “I am very excited that today we have been able to treat the first patient with OncoSil through a CT‐guided percutaneous implantation procedure. This novel means of implantation of the OncoSil device has a number of potential advantages, such as the ability to more precisely place the radioactive microparticles within the pancreatic tumour in a simpler procedure, which can be performed by interventional radiologists many of whom are used to working with radionuclide therapies in the treatment of various malignant diseases.”
Adding to their recent announcement, lead investigator Marc Besselink (Amsterdam University Medical Centers, Amsterdam, The Netherlands) said: “Today we set the first step in developing a more flexible approach to the OncoSil treatment by implanting the first patient using a percutaneous CT‐guided approach. Eventually, we aim to give caregivers more flexibility to treat their patients with LAPC with OncoSil as they will have the ability to select the route of administration of the device based on the tumour location, patient preference and the availability of different specialists within the multidisciplinary treatment team.”
OncoSil Medical CEO and managing director Nigel Lange contributed that: “We are excited by news that the first patient has been treated in the PANCOSIL study. The recruitment of patients to this study represents another significant milestone in our efforts to commercialise the OncoSil device. We expect the results of the study will help us to develop an alternative technique for OncoSil implantation and provide flexibility for users. This and other outcomes emerging from the PANCOSIL study will open the way for an increased number of medical professionals to deliver the device to patients with LAPC.”
Inari Medical has announced the first patient enrolment in PEERLESS II. This prospective, global, multicentre randomised controlled trial (RCT) compares the outcomes of intermediate-risk acute pulmonary embolism (PE) patients treated with the FlowTriever system against those treated with traditional anticoagulation therapy alone.
The first patient was enrolled by William H Matthai Jr (Penn Presbyterian Medical Center at the University of Pennsylvania, Philadelphia, USA), a press release details.
“PEERLESS II is challenging the most commonly administered first-line therapy for PE around the world,” said Matthai. “Despite advances in mechanical thrombectomy, anticoagulation alone remains the standard of care. This trial aims to generate definitive evidence to influence PE treatment guidelines worldwide.”
According to Inari Medical, PEERLESS II is the largest study of its kind and will include up to 1,200 randomised patients at up to 100 global centres. The study is running alongside the currently enrolling PEERLESS RCT, which is comparing FlowTriever to catheter-directed thrombolysis. Both trials aim to generate the high-quality clinical evidence needed to move the field forward and establish FlowTriever as the optimal therapy for intermediate-risk PE patients.
“PE is a leading cause of cardiovascular death and this first patient enrolment represents an important milestone in the evolution of care for this disease,” added global principal investigator Jay Giri (Hospital of the University of Pennsylvania, Philadelphia, USA). “The rigorous trial design, including meaningful patient-centric endpoints and independent adjudication of all safety events, lays the groundwork for this landmark study to impact future PE treatment decisions. Thank you to the PEERLESS II steering committee and clinical staff for helping us get the first patient enrolled.”
“Inari is actively enrolling three RCTs: PEERLESS, PEERLESS II and DEFIANCE, demonstrating our relentless commitment to guideline-changing research aimed at ultimately improving patient outcomes,” said Thomas Tu, Inari’s chief medical officer. “With the commitment of our dedicated investigators, we look forward to expedited enrollment to get us closer to changing the standard of care.”
Penumbra today announced that the first patient has been enrolled in STORM-PE, a prospective, multicentre, randomised controlled trial (RCT) evaluating anticoagulation alone versus anticoagulation plus Lightning Flash for the treatment of pulmonary embolism (PE).
In partnership with PERT Consortium, a multidisciplinary group dedicated to improving the care of patients with PE, the STORM-PE trial aims to advance the understanding of the role of computer-assisted vacuum thrombectomy (CAVT) in the management of acute PE, with a goal of improving the outcomes for patients with this condition.
“STORM-PE is the first head-to-head trial comparing anticoagulation, the mainstay and standard of care for treating acute PE, to CAVT,” said Rachel Rosovsky (Massachusetts General Hospital, Boston, USA), co-global principal investigator of STORM-PE. “We have already seen the significant impact Lightning Flash can have on patients. The results generated from this pivotal RCT study will provide level 1 evidence of how CAVT compares to current treatment paradigms and will inform us if treatment guidelines need to include this technology as a frontline therapeutic option in patients with intermediate high-risk PE.”
STORM-PE will enrol up to 100 participants at up to 20 sites. Penumbra’s Lightning Flash can be used to remove emboli and thrombi from vessels of the peripheral arterial and venous systems and can be used for the treatment of PE. A press release details that Lightning Flash combines hypotube-based Indigo Aspiration Catheters with LightningIntelligent Aspiration, a computer-assisted clot detection technology that can differentiate between clot and blood, designed to reduce blood loss and the need for clot-dissolving drugs, which may lower the risk of bleeding complications.
“Enrolling the first patient in STORM-PE RCT is an important milestone,” said Nicolas J Mouawad (McLaren Health Care, Bay City, USA). “This landmark RCT will be instrumental to advancing the standard of care for patients with [PE].”
“Endovascular therapy has been shown to be an increasingly safe and effective treatment for patients with a symptomatic acute [PE],” said Robert Lookstein (Icahn School of Medicine at Mount Sinai, New York, USA), co-global principal investigator. “We are proud to commence enrolment in the STORM-PE trial. This trial is designed to answer whether CAVT plus anticoagulation can restore normal function to the failing right ventricle faster and more reliably than anticoagulation alone. We are confident this trial will generate foundational data leading to the next generation of randomised studies in the field of venous thromboembolism for years to come.”
“Our commitment to clinical research and innovation enables us to lead with insight and continue to pioneer interventional therapies that have a significant impact on patients such as our CAVT technologies,” said James F Benenati, chief medical officer at Penumbra. “In partnership with PERT Consortium, we are committed to generating robust clinical evidence that will help transform care so patients, especially those with serious conditions such as PE, can return home quickly and live fully.”
A recent study concerning moral injury (MI) among interventional radiologists has found that the condition is “prevalent” throughout the field, and has been shown to negatively correlate with quality-of-life (QoL) indicators.
Principal investigator Andrew J Woerner (University of Washington, Seattle, USA) et al introduce MI within healthcare as the “lasting impact of repeated ethical dilemmas and moral conflicts” when physicians are unable to act in the best interest of their patients due to institutional or systemic constraints. Woerner and colleagues identify MI as a “risk factor” associated with burnout, which in previous studies has been correlated with medical errors, they note.
Using the MI Symptom Scale-Healthcare Professionals (MISS-HP) survey, Woerner et al report a total of 365 interventional radiologists returned MISS-HP and QoL responses. Of the respondents, 299 (81.9%) were male, 65 (17.8%) were female, and one preferred to not disclose gender. The ratio of female and underrepresented minorities in their study population was “similar” to ratios reported for the interventional radiology (IR) workforce in the USA, suggesting “demographically representative sampling”, the investigators state.
Among participants, 209 (57.3%) were familiar with the concept of burnout alone, 115 (42.5%) were aware of both burnout and MI, and one (0.3%) respondent was familiar with MI only. Woerner and colleagues outline that 146 (40%) of practice settings were academic, 121 (33.2%) were community based, 84 (23%) were hybrid, and 14 (3.8%) centres were reported as “other”.
Respondents included 299 (8.19%) practicing interventional radiologists and 66 (18.1%) interventional radiologists-in-training. The authors highlight that trainees were included in their survey population in an attempt to assess for the presence and impact of MI in early career interventional radiologists. Of trainees included in the study, 66 (18.1%) were interventional radiologists-in-training, 23 (6.3%) were <1 year post-graduate, 149 (40.8%) were 1–10 years post-graduate, 73 (20%) were 11–20 years post-graduate, and 54 (14.8%) were >21 years post-graduate.
Of their results, Woerner et al report that 233 (61.1%) of interventional radiologists who responded scored ≥36 on the MISS-HP and thus were categorised as having profession-related MI. They note that MISS-HP scores “varied across the practice experience durations”, noting the following subgroups listed in a decreasing order of the mean MI score: 10–20 years, 1–10 years, currently in training, >20 years, and <1 year (43.5, 40.5, 37.9, 36.8, and 36.5; p<0.05). Overall, they emphasise the “significant difference” in mean MI between the >20 years and 10–20 years of practice subgroups (36.8 ± 11.5 versus 43.5 ± 13.6; p<0.05).
Of their QoL data, the authors state that mean QoL for the entire cohort was 71.1 ± 17.0 (range: 0–100), suggestive of “good” QoL. However, they report that the mean QoL for the MI subgroup was “significantly different” from that of the rest of the group (67.6 ± 17.0 versus 76.6 ± 16.0; p<0.05). Continuing to expand on their data, Woerner et al note significant disparities between QoL between practice groups with >20 years versus 10–20 years of experience (73.9 ± 19.8 versus 66.4 ± 16.9; p<0.05).
Discussing their results, Woerner et al reflect that these data show an association and “potential causative link” between MI and QoL in interventional radiologists. However, they note that their results are suggestive of “lower burnout and increased wellness” in interventional radiologists who have practiced for a longer period of time.
In the open response section, the investigators also comment that respondents identified “ineffective leadership, barriers to patient care, corporatisation of medicine, non-physician administration, futile procedures, turf battles and reduced resources” as the main contributors to burnout and MI.
To initiate address of these issues by identifying MI, Woerner and colleagues hope that “moral repair” can be achieved to reduce the impact of MI on interventional radiologists. They aver that this could be achieved by: “Improving autonomy, reducing bureaucracy, enhancing administrative support, promoting physician-led leadership, ensuring sufficient staffing, reforming the medical system, unionising physicians, fostering transparency with insurance companies, increasing vacation time, and pursuing retirement or leaving medicine.” However, the authors note that unfortunately, “many” proposed solutions are “challenging” and “impractical”, as they are intrinsically linked to “external or systemic barriers” and institutional structures, which are “beyond the scope” of their study.
Concluding their discussion, the authors reiterate that MI is prevalent among interventional radiologists in the USA and negatively impacts QoL. They further that future research should explore how various radiology subspecialties compare via MI and QoL metrics, to “inform the department/hospital leadership on the various challenges across the radiology disciplines”.
A panel of leading experts has welcomed guidance published by the National Institute for Health and Care Excellence (NICE) recommending the use of hybrid closed loop systems for managing blood glucose levels in the management of type 1 diabetes in England & Wales.
The expert panel was chaired by Partha Kar, national specialty advisor, diabetes, NHS England and included: Alistair Lumb (Oxford University Hospitals NHS Foundation Trust, Oxford, UK), Geraldine Gallen (King’s College Hospital NHS Foundation Trust, London, UK) and Rachael Chrisp, Head of policy and public affairs at the charity JDRF.
The panel agreed that this multi-technology appraisal—to be implemented in a phased approach over five years—will expand access to the most advanced automated insulin delivery (AID) systems which will help simplify diabetes management and improve glycaemic outcomes for an additional 150,000 people regardless of their location or social background within these regions.
Priority will be given to children, pregnancy (including women trying for pregnancy), and adults with a haemoglobin A1c (HbA1c) test score of 7.5% or above, or who have disabling hypoglycaemia, despite optimal management with legacy technology.
“We have witnessed universal coverage of continuous glucose monitoring (CGM) in England & Wales shatter tech barriers for underserved communities, unleashing diabetes empowerment for all. With this decision, the benefits of hybrid closed loop therapy, the most advanced diabetes technology on the market, will be available as standard to the vast majority, regardless of background. This will make the UK one of the most progressive countries in terms of treating type 1 diabetes,” said Kar.
The panel called for investment in education for healthcare professionals so that they can be confident in discussing the technology-enabled support available to patients, as more people will be moving towards using closed loop to manage their condition. The experts also supported greater coordination with industry to increase awareness amongst healthcare professionals and patients so they are aware of the technology and can be confident in its use.
“This decision reinforces that CGM alone is not enough to manage diabetes and recognises that hybrid closed loop systems can, and should, be considered as standard of care for people with type 1 diabetes,” said Susan Monaghan, senior business director for Medtronic Diabetes in the UK, Ireland, Belgium, the Netherlands, and Luxembourg. “While there are clinical and legitimate reasons for a person to decide not to use a hybrid closed loop system, the healthcare provider who does not offer such technology for a qualifying person living with type 1 diabetes should justify the reason why they are not doing so given the elimination of cost. This will ensure equitable access across the country.”
As the leading healthcare technology company with a comprehensive ecosystem combining advanced hybrid closed loop technology, CGM and value-added services to people with diabetes and physicians, Medtronic is positioned to deliver on the promises to people living with diabetes in the UK and beyond and looks forward to partnering with NHS Trusts in England and Wales as they implement the new guidelines.
Final guidance is expected to publish in December 2023: https://www.nice.org.uk/news/article/nice-recommends-life-changing-technology-is-rolled-out-to-people-with-type-1-diabetes
NOTE: This video is ONLY available to watch in selected countries and geographies
Thierry de Baère (Paris, France), Laurent Milot (Lyon, France) and Govindarajan Narayanan (Miami, USA) sit down for an Interventional News Expert Panel discussion on robotics in Interventional Oncology.
The panel of experts discuss their early experiences and discovery moments in which they realised the value of Epione® (Quantum Surgical), what they feel are the clinical advantages of Epione®, as well as how to initiate a robotic programme within a practice or hospital.
One of the main discussion points is that this technology is not just beneficial for physicians that are at an earlier point in their career; even those who have “built [their] career on placing needles and doing CT-guided or image-guided ablations or biopsies” and are “skeptical about robotics because they can do better” will benefit from the use of Epione®, whether it is with robotic assistance for needle insertion or through the use of innovative planning software that allows for multi-needle placement.
The panel concludes that, with their experience in performing tumour ablation procedures, they found genuine value in the adoption of Epione® into their oncology programmes.
Biotronik has announced the presentation of two-year results from the investigator-initiated BIOPACT randomised controlled trial (RCT) by principal investigator Koen Deloose (AZ Sint-Blasius Hospital, Dendermonde, Belgium) at the Paris Vascular Insights (PVI) 2023 congress (8–10 November, Paris, France). The randomised controlled non-inferiority trial evaluated the safety and efficacy of the Passeo-18 Lux drug-coated balloon (DCB) catheter compared to the IN.PACT Admiral DCB (Medtronic), and showed excellent results for both balloons through 24 months.
The prospective, multicentre, core-lab adjudicated non-inferiority trial enrolled 302 patients in Austria, Belgium, France and Switzerland with Rutherford Class 2–4 disease. Patients were randomised 1:1 to either the Passeo-18 Lux DCB or IN.PACT Admiral DCB for the treatment of stenotic, non-stented restenotic or occlusive lesions in the femoropopliteal artery. Baseline patient and lesion characteristics were comparable across both arms.
As presented at PVI, the rate of clinically driven target lesion revascularisation (CD-TLR) for the Passeo-18 Lux DCB was noninferior to the IN.PACT Admiral DCB at 12 months, which was maintained at 24 months (93.3%, Passeo-18 Lux DCB vs. 94.6%, IN.PACT Admiral DCB at 24 months; p=0.0048).
Survival was also equivalent at 24 months, with a 95% rate of overall survival for both devices, and there were no major target limb amputations in either arm.
“The two-year results of the BIOPACT RCT have continued to demonstrate the noninferiority of the safety and efficacy of the Passeo-18 Lux DCB to the IN.PACT Admiral DCB, and they show persistent excellence of both devices,” said Deloose. “This study is critically needed to fill the gap of head-to-head data for peripheral DCBs to keep the most effective treatments accessible to our patients.”
The Passeo-18 Lux DCB has a paclitaxel dose of 3µg/mm2 and uses a Butyryl-tri-hexyl citrate excipient (IN.PACT Admiral DCB: 3.5µg/mm2 and urea excipient). The lower-profile Passeo-18 Lux DCB is on an 0.018″ platform and is 4-French compatible for diameters of 2–4mm and 5-French compatible for diameters of 5–7mm. In comparison, the IN.PACT Admiral DCB is 5-French compatible only for its 4mm diameter, and is 6-French or 7-French compatible for its diameters of 5–7mm.
“We are delighted to see confirmation of the continued performance and safety of our Passeo-18 Lux DCB in this important RCT, which will support our access in key new markets,” said Stuart Perks, vice president marketing vascular intervention at Biotronik.
A press release details that the BIOPACT RCT study will continue collecting follow-up data at 36, 48 and 60 months, which will be shared upon completion of each follow-up period.
The Irvine, California–based company earlier this month announced plans to acquire LimFlow for up to US$415 million. The deal came just weeks after Paris-based LimFlow won US Food and Drug Administration (FDA) premarket approval for its breakthrough CLTI treatment. Inari Medical intends to pay a total upfront consideration of US$250 million in cash at closing.
Contingent consideration of up to US$165 million in additional cash payments hinges on certain commercial and reimbursement milestones. Inari expects to pay those tranches out between 2025 and 2027. The company said it funded the acquisition at close from existing cash resources.
LimFlow designed its system for transcatheter arterialisation of deep veins. It diverts blood from a diseased tibial artery to a tibial vein to deliver oxygen to a patient’s ischemic foot.
In the initial announcement, Inari CEO Drew Hykes said the LimFlow acquisition aligns with the company’s mission to address significant unmet patient needs and adds another highly differentiated growth platform into Inari’s portfolio.
“The close of the LimFlow acquisition allows us to begin to integrate this exciting technology that is offering new hope to patients suffering from CLTI,” Hykes said in a recent news release. “LimFlow addresses one of the most significant unmet needs in all of vascular medicine, is closely aligned with our mission and adds another highly differentiated growth platform into our portfolio.”
Parosmia is the name given to the condition where the sense of smell does not work correctly and has long been identified as a symptom of COVID-19, with recent research showing that up to 60% of COVID-19 patients have reported this symptom.
Lead author Adam C Zoga (Jefferson Health in Philadelphia, Pennsylvania, USA) and colleagues state that the majority of patients recover their sense of smell after a period. However, some patients with long-COVID do not, these patients reporting symptoms that last weeks, months and even years, “negatively impacting their appetite for food and overall quality of life”, the researchers note.
“Post-COVID parosmia is common and increasingly recognised,” said Zoga, in a recent press release. “Patients can develop a distaste for foods and drinks they used to enjoy”. Concurrently, the investigators state that distorted sense of smell can affect smell perception, potentially causing phantosmia—a condition that causes individuals to detect smells that are not in their environment.
To investigate possible treatments for patients with long-COVID induced parosmia, Zoga et al considered the potential benefits of computed-tomography (CT)-guided stellate ganglion block. They expand that, as part of the autonomic nervous system, which regulates involuntary processes including heart rate, blood pressure, breathing and digestion, the stellate ganglia are nerves on each side of the neck. They deliver certain signals to the head, neck, arms and a portion of the upper chest.
Using a stellate ganglion block, the researchers injected anaesthetic directly into the stellate ganglion on one side of the patients’ neck, stimulating the regional autonomic nervous system. As Zoga and colleagues state, the procedure is minimally invasive and takes under 10 minutes, requiring no sedation or intravenous analgesia.
For their study, 54 patients were referred from an ear, nose and throat specialist after at least six months of post-COVID parosmia that was resistant to pharmaceutical and topical therapies. CT guidance was then used to position a spinal needle at the base of the neck for injection into the stellate ganglion. The researchers note that they added a small dose of corticosteroid to the anaesthetic in the pharmacologic preparation, suspecting that the COVID virus may be causing nerve inflammation.
Commenting on their initial results, Zoga observes a “tremendously positive outcome, almost immediately, with continued improvement to the point of symptom resolution at four weeks”.
Follow-up was obtained from 37 patients overall, and revealed 22 patients who reported “significant progressive improvement” by one month post-procedure. Furthermore, at three months, Zoga et al state there was a mean improvement in symptoms of 49% among the 22 patients.
The investigators offered patients a second injection on the other side of the neck at least six weeks after the first. They note that 26 patients returned for this procedure, but found that a second injection was not effective in patients who did not respond to the first. Of patients who did see improvement after the first, 86% reported additional improvements after the second injection.
“We have been surprised at some outcomes, including near 100% resolution of phantosmia in some patients throughout the trial,” Zoga comments, adding that “other treatments have failed to date” however “this injection is working”.
The researchers share these results ahead of their presentation at the RSNA 2023 meeting and state that data will continue to be updated right up until the session takes place.
Baird Medical, leading microwave ablation (MWA) medical device developer and provider in China, has announced that its subsidiary, Betters Medical, has received clearance from the US Food and Drug Administration (FDA) under Section 510k, to begin marketing its portfolio of MWA systems and disposable MWA needles as regulatory class II devices in the USA.
Thyroid nodules occur among 30% to 50% of the population of the USA. Like most thyroid conditions, nodules are more common among women than men, with an increased incidence observed with advancing age. By the age of 60, more than half of women will have developed a thyroid nodule.
Historically, treatment involving excision or therapy resulted in discomfort and inconvenience for patients. In contrast to these traditional approaches, Baird Medical has leveraged significant recent technological advances to develop a minimally invasive, thermal energy-based procedure to treat thyroid nodules, breast tumours, and other diseases for which the coagulation of soft tissues is indicated. Baird Medicals’ approach, they state, eliminates the need for surgery, thereby mitigating associated complications, risks, and scarring for the majority of patients.
The press release states that, during the procedure, therapeutic microwave energy is safely administered via a device approximately the diameter of a pen. This minimally invasive treatment precisely targets the nodule or tumour being treated, while preserving the surrounding healthy tissue. This precision is crucial, as it safeguards the function of the thyroid and reduces the likelihood that a patient will require expensive, lifelong thyroid hormone replacement therapy.
In light of the increasing scientific evidence demonstrating positive outcomes associated with the expanded availability of MWA, both the American Thyroid Association (ATA) and the European Thyroid Association (ETA) have published recommended guidelines for its implementation and adoption. Physician associations, such as the North America Society for Interventional Thyroidology (NASIT), have been established to raise awareness among physicians and patients that a minimally invasive solution exists for treating thyroid disease.
Haimei Wu, founder and CEO of Baird Medical, commented: “Attaining FDA clearance represents a significant milestone in our geographical expansion. This clearance grants us the ability to market our portfolio of MWA systems and disposable needles in the USA. Our team are ready to expand our market reach and deliver the much-needed benefits of our minimally invasive MWA procedure to patients across [the USA].”
This advertorial, sponsored by Penumbra, is intended only for readers outside the USA.
José Andres Guirola Ortiz
“The advances led by this technology have significantly revolutionised our procedures,” states José Andres Guirola Ortiz (Hospital Clinico Universitario Lozano Blesa, Zaragoza, Spain), discussing how the “invaluable” Lightning (Penumbra) CAVT system fits within his practice. Speaking to Interventional News, he shares how the unique mechanism of the device has benefits for both the operator and patient and he provides his thoughts on upcoming trial data for its safety and efficacy in the treatment of pulmonary embolism (PE).
In 2019, the European Society of Cardiology (ESC) guidelines1 updated recommendations to encompass percutaneous interventional technologies in patients with intermediate- or high-risk PE where haemodynamic deterioration has occurred as an alternative to rescue thrombolysis. For Guirola Ortiz, most patients he sees fall within this risk category, “irrespective of their suitability for fibrinolysis”.
“A decade ago, the majority were high- or massive-risk PE patients,” he reflects, but states that, retrospectively, this fact was influenced by a 2001 publication by Miguel Angel de Gregorio (University of Zaragoza, Zaragoza, Spain) on pulmonary fragmentation and fibrinolysis2.
“My mentor, [de Gregorio], collaborated with intensive care to be one of the first to formulate a protocol for addressing high-risk pulmonary embolism in unstable patients. At the time they required pulmonary angiography for diagnosis, primarily because computed tomography angiography was not available. Consequently, their thought process was: “If diagnosis is needed, why not treat simultaneously?”
With this simultaneous diagnosis and treatment de Gregorio later released scientific article which considered deviation from the eighth American College of Chest Physicians (ACCP) guideline in regard to PE catheter-directed therapies (CDT), a minimally invasive alternative to open surgery3 and was one of the first to make this suggestion.
Fast forward 20 years, and technological innovations are occurring quickly, Penumbra’s Lightning CAVT system an example of these advancements, which Guirola Ortiz stated has “revolutionised” his procedural workflow “notably reducing blood loss”. The Lightning system is designed with intermittent aspiration to facilitate quick thrombus removal in vessels of various sizes and minimize the potential for blood loss, speeding up procedures and reducing the need for thrombolytics. Powered by the Penumbra ENGINE, Lightning can detect pressure differentials within the catheter and provide audio-visual cues which are “invaluable” Guirola Ortiz highlights, “when determining whether the catheter has free-flow or is obstructed by a thrombus”.
With Lightning’s CAVT system, interventionalists have access to a robust safety profile that promotes an endovascular-first approach for treatment of PE patients. Guirola Ortiz expands on the clinical outcomes he looks for when treating these patients: “Primarily, we review the patient’s stability concerning arterial pressure and normalisation, and a reduction in cardiac frequency coupled with standard oxygen saturation levels”. Then, he continues, “we consistently measure the pulmonary artery pressure (PAP) before, during, and after thrombectomy—a decline of 10mmHg or more in systolic PAP significantly correlates with better patient outcomes” he opines.
Furthermore, Guirola Ortiz and his team then assess the patient’s cardiac conditions using echo tricuspid annular plane systolic excursion (TAPSE), and the right and left ventricular (RV/LV) ratio, pre- and post- 48 hours of treatment. Research such as that of Felix Götzinger (Universität des Saarlandes, Saarbrücken, Germany) et al4, has begun to suggest that interventional treatment options may lead to a rapid improvement in RV/LV function and pulmonary haemodynamics. For Guirola Ortiz, this data will “be instrumental in identifying patients who will benefit most” from CAVT for the treatment of PE, referencing the ongoing STRIKE-PE trial which aims to evaluate the long-term functional outcome, safety and performance of the Lightning system.
STRIKE-PE—a prospective, multicentre study of adult patients with clinical symptoms consistent with acute PE and a RV/LV ratio of 0.9 or greater—released interim data analysis at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark). Presented by John Moriarty (University of California, Los Angeles Medical Center, Los Angeles, USA) their interim analysis included 87 patients at 90 day follow-up with a mean age of 59.4 years, 59.8% of patients were male and 94.3% had intermediate-risk PE. All patients received frontline endovascular treatment with the Lightning 12 aspiration system.
Moriarty reported that the observed change in the RV/LV ratio was statistically significant, showing a 27.5% decrease. Investigators also saw a decrease in intraprocedural systolic pulmonary artery pressure (sPAP) of 9.4mmHg or 18%. Patients that required an intensive care unit (ICU) stay, the median length of stay was one day—36.8% of patients did not require an ICU stay. The researchers did note a 2.3% major bleeding event rate which occurred within 48-hours of treatment.
A unique aspect of STRIKE-PE was the emphasis on QoL (quality of life) outcomes. Moriarty noted the Borg dyspnea scale (range, 0 [none] to 10 [maximal]) at rest decreased from four to zero at 90-day follow-up. The distance covered during the six-minute walk test (6MWT) increased in this patient cohort from 179 metres at baseline, to 299 metres at 90-day follow-up. Additionally, the investigators reported a 17.7% Pulmonary Embolism Quality of Life (PEmb-QoL) survey average at 90-days (range, 0% [extent of daily life affected] to 100%) which was previously recorded as 36.7 on discharge.
“By assessing both short-term (RV/LV ratio) and long-term outcomes via quality-of-life surveys such as the PEmb-QoL survey and the functional outcome of the 6MWT, we will have a clearer picture of patient outcomes. Data from the STRIKE-PE trial will pave the way for guideline revisions in favour of minimally invasive endovascular thrombectomy,” Guirola Ortiz asserts.
So far, he continues, conclusions from the STRIKE-PE trial have shown “significant reductions” in RV/LV ratio and sPAP, as well as a quick thrombectomy time when deploying the Lightning 12 in the treatment of PE patients in a real-world population. A result which, makes him “optimistic for the future of minimally invasive pulmonary procedures”.
In light of ongoing research and the technological advancements embodied by the Lightning system for the treatment of PE, Guirola Ortiz considers whether there will be a paradigm shift in how these patients are considered for treatment in the future. For him, a “decline in the usage of fibrinolytics” is ahead, as well as a “[reduction] in the likelihood of significant bleeding complications with CDTs”.
This shift, he believes, will “largely depend on new randomised controlled trials (RCTs) presenting favourable outcomes”. Guirola Ortiz tells Interventional News how “most contemporary guidelines” are based on a 1988 RCT by Marc Verstraete (Katholieke Universiteit Leuven, Leuven, Belgium)5 which appraised intravenous and intrapulmonary recombinant tissue-type plasminogen activator in the treatment of acute high-risk PE, which he says “bears little resemblance to today’s treatment methods”. “Yet,” Guirola Ortiz continues, “since 1988, there have been no RCTs conducted comparing CDT with peripheral thrombolysis, leading to the present evidence deficit”.
However, while awaiting more robust contemporary data, Guirola Ortiz emphasises that safety and efficacy studies are important but “not every intervention requires an RCT for validation to be included in guidelines—as humorously illustrated by Gordon CS Smith’s paper6 on the use of parachutes”. Today, Guirola Ortiz underlines that, for his practice, the Lightning CAVT system “advances” the standard of care they can provide across a broad range of indications, such as deep vein thrombosis (DVT) and acute portal thrombosis for liver transplant patients, subsequently improving procedural efficacy, and overall patient care.
References:
Konstantinides et al 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). European Heart Journal, Volume 41, Issue 4, 21 January 2020, Pages 543–603.
de Gregorio MA et al. Mechanical fragmentation and intrapulmonary fibrinolysis in the treatment of massive pulmonary embolism haemodynamic repercussions. Arch Bronconeumol. 2001; 37; 58–4.
de Gregorio MA et al. Endovascular treatment of a haemodynamically unstable massive pulmonary embolism using fibrinalysis and fragmentation. Experience with 111 patients in a single centre. Why don’t we follow ACCP recommendations? Arch Bronconeumol. 2011 Jan; 4711; 17–24.
Götzinger F et al. lnterventional therapies for pulmonary embolism. Nature Reviews Cardiology, Volume 20, October 2023, 670–684.
Verstraete M et al. Intravenous and intrapulmonary recombinant tissue-type plasminogen activator in the treatment of acute massive pulmonary embolism. Circulation 77, No. 2, 353–360, 1988.
Gordon CS Smith, Jill P Pell. Parachute use to prevent death and major trauma related to gravitational challenge: Systematic review of randomised controlled trials. BMJ Volume 327 20-27 December 2003 bmj.com.
Disclaimer: The opinions and clinical experiences presented herein are for informational purposes only. The results may not be predictive of all patients. Individual results may vary depending on a variety of patient-specific attributes.
The International Accreditation System for Interventional Oncology Services (IASIOS) has reported experiencing exponential growth exceeding 150% in the past year. IASIOS has been at the forefront of standardising interventional oncology (IO) care worldwide, with a mission to make it safe and effective in facilities across the globe, as a recent press release states. The expansion efforts of IASIOS areia carried out in the hopes of redefining patient care in the field of IO.
IASIOS was established with a vision to drive the evolution and adoption of interventional oncology as a mainstream discipline in the treatment of cancer. Today, IO has emerged as the fourth pillar of cancer care, and IASIOS is precisely where it aspired to be.
Recently IASIOS reached a significant milestone by officially welcoming the Mallinckrodt Institute of Radiology at Washington University in the USA as an IASIOS-Accredited Centre, marking its successful entry into the market. This achievement represents a pivotal moment for both IASIOS and the global IO community, setting an industry benchmark for others to follow, the press release notes.
Andreas Adam (Kings College London, London, UK), a distinguished interventional oncologist and chairperson of the IASIOS steering board commented: “The primary purpose of IASIOS is to improve the care that interventional radiologists provide to patients with cancer. The global nature of this accreditation system is one of its greatest strengths, as it emphasises certain universal concepts, such as the need for interventional radiologists to look after their own patients. The enrolment of the Mallinckrodt Institute of Radiology into IASIOS is a major milestone, because the USA is the birthplace of interventional radiology (IR) and the largest provider of IR services. We are delighted to welcome the Mallinckrodt Institute of Radiology, as its enrolment is a perfect demonstration of the universality of the principles on which IASIOS is founded.”
This accomplishment represents a monumental step in IASIOS’s mission to set globally accepted standards for interventional oncology, ultimately making safe and effective minimally invasive IO procedures more accessible to patients worldwide. As IASIOS continues to grow and expand, it remains committed to its mission to advance IO care and enhance the lives of countless cancer patients.
Jack Jennings from the Mallinckrodt Institute of Radiology also shared his excitement, stating: “IASIOS raises the bar for our institution to bring the most up-to-date IO practices to our patients for the best outcomes. We benefit from this accreditation by being linked to other high-level IO institutions. We are the first institution in the USA to become associated with this esteemed accreditation and hope to lead the way for other IO practices in the USA!” Mallinckrodt Institute of Radiology’s pioneering accreditation sets the stage for all centres in the USA to follow suit.
IASIOS’s global expansion is evident, currently reporting accredited centres in Asia, Australia, Europe, the Middle East, North America and South America.
Cordis has announced the completion of patient enrolment in the RADIANCY premarket clinical study. The prospective, multicentre, single-arm study is designed to evaluate the safety and efficacy of the S.M.A.R.T. Radianz vascular stent system when used with the Brite Tip Radianz guiding sheath and Saberx Radianz percutaneous transluminal angioplasty (PTA) dilatation catheter for treatment of iliac and femoropopliteal artery lesions via radial artery access. Data from the RADIANCY study will be part of the clinical evidence towards pursuing the CE mark of the S.M.A.R.T. Radianz vascular stent system.
The RADIANCY study enrolled 151 patients at 12 sites across six European countries. The results of the first 100 patients were presented at Paris Vascular Insights (PVI; 8–10 November, Paris, France) by lead principal investigator Raphaël Coscas (Ambroise Paré Hospital, Boulogne-Billancourt, France). Coscas commented: “The results are very exciting and promising with excellent technical success (97.9%) and a great safety profile. These results attest to the technological innovation and patient advantages for peripheral arterial disease (PAD) treatment in terms of early mobility and safety. I applaud Cordis for a successful completion of this trial and strengthening the scientific evidence for radial to peripheral procedures.” The final results of the study are awaited.
“The transradial approach has been established as the standard access site in cardiology, with proven patient benefits such as less risk of complications at access site (bleeding, haematoma, groin infection), increased patient comfort, quicker time to ambulation/mobility of patients, and earlier discharge. With the Radianz radial peripheral system portfolio, we are proud to contribute to expanding these benefits to patients undergoing peripheral interventions,” added Dominique Boulet, president of Cordis EMEA.
The S.M.A.R.T. Radianz vascular stent system, specifically engineered for radial access, was approved for use by the US Food and Drug Administration (FDA) in February 2022, and by the Japanese Pharmaceuticals and Medical Devices Agency (PMDA) in March 2022.
Left to right: Premal Patel, Fernando Gómez Muñoz, Alessandro Gasparetto
Left to right: Premal Patel, Alessandro Gasparetto, Fernando Gómez Muñoz,
Lagging behind the rapid advancements within the speciality as a whole, a 2023 study titled ‘Is there really no kit for kids?’ has identified the continuing “unmet need” for paediatric interventional radiology (IR) devices. Although off-label device usage has been standard in paediatric cases, Premal Patel (Great Ormond Street Hospital, London, UK) told Interventional News of “changing regulations” in Europe— with repercussions worldwide—which has forced manufacturers to state a definitive ‘yes’ or ‘no’ in device instructions for use (IFU) in reference to children. In light of recent international device withdrawals and license regulation updates, Patel, Fernando Gómez Muñoz (Netherlands Cancer Institute, Amsterdam, The Netherlands) and Alessandro Gasparetto (The Hospital for Sick Children, Toronto, Canada) surveyed the current state of paediatric IR and the global device deficit.
In May 2021, the European Medical Devices Regulation (MDR) introduced an update stating their intention to “bring EU legislation into line with technical advances, changes in medical science and progress in law-making”, stating that all medical devices must meet “robust”, “internationally recognised” safety criteria and apply for new certification. The directive requires that manufacturers explicitly state whether devices can be used in paediatric patients, as well as additional costs to obtain certification for product lines.
In 2023, the European MDR extended the deadline for manufacturers to comply with the requirements to 2027–2028 depending on the device. “They are making it harder for companies to keep licenses,” Patel said, “the way companies typically got around this is by just not saying anything”.
Looking at this in greater depth, Patel et al’s cross-sectional analysis of device IFU assessed the inclusion of children in vascular access, biopsy, drainage and enteral feeding devices from 28 companies who sponsored the British Society of Interventional Radiology (BSIR), the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and the Society of Interventional Radiology (SIR) between 2019 to 2020. Their results show that 190 devices with IFUs from 18 medical device manufacturers were assessed—26% mentioned children, 3% explicitly stated that the device was not for use in children, and 29% implied they could be used in children with caution—the most common caution (14%) being the size of the device that could be accommodated in a child.
Patel and colleagues’ conclusion draws attention to the 29% of devices that may be suitable for paediatric use but lack explicit manufacturer support—“typically [IFUs] do not mention children, but manufacturers workaround this by stating ‘use an appropriate size for the patient’ which you can interpret how you want,” Patel explained. Now, however, manufacturers are “specifically saying no to children,” he updated, even stating that their data—collected in June 2023—are inaccurate due to recent Cook Medical withdrawals which have taken many of their device lines “off the shelf” for Patel and his team. “We have already seen the effect, the data in the paper are now out of date,” he said.
Device withdrawals and IFU criteria changes have left paediatric interventional radiologists with little option but to “look for avenues around these regulations” and treat patients effectively via off-label device use. In having to seek these avenues, Gómez Muñoz reflected that “children are being prevented from getting treatment,” in the event of no appropriate device being accessible, as well as “the impact of cost to both the interventional radiologist and the patient”. “You do not want to risk your license or your future doing something that, despite knowing it is completely safe and effective, is not plainly indicated for use in children,” he continued.
Sharing his experiences in treating paediatric patients, Gómez Muñoz stated that it is commonplace to use “homemade solutions” in IR due to the absence of any children-specific devices. “If you have to perform biliary drainage, the size of the drain can sometimes be the same size as the kid. You end up making your own holes or using drains that are not intended for internal use, risking the safety of the procedure,” he conveyed. Additionally, he expanded that placing a stent in a child is “completely different” to placing a stent in an adult— “an adult is not going to grow, but the kid may have an artery of 3.5mm, that, over the course of 18 years, may double in size”.
“This is something we suffer every day,” Gómez Muñoz said, and reading Patel et al’s 2023 research spurred him to write a ‘plea’ to the regulatory authorities and medical device companies, urging them to take action. His letter, titled ‘A plea to solve the unmet needs in paediatric IR devices’ begins by asking: “Are we truly upholding the notion that our children are the most valuable good of our society?” He argues that the lack of adequate medications and IR devices for children “tells a different story” and recalls a summit which took place a few years ago that heard a board member plainly confirm “we have no interest in funding research for children”. Although childhood cancer is thankfully “rare,” Gómez Muñoz’s exposits in his plea, the ”unfortunate” stance of medical device manufacturers that states children are not a “lucrative market” has driven a data deficit, risking interventional radiologists’ licenses in the event of complications when using off-label IR devices in low-complexity cases. For Gómez Muñoz, in some cases merely downsizing an existing adult device “will not suffice”, however he believes that “regulatory bodies should be aware of the situation at hand—if you have a catheter that has been approved for 30+ years in adults, [medical device developers] just need to reduce the size, and it should not need to go through the MDR approval process, as then it is not cost-effective and will take years—I do not see the necessity for that”.
In Canada, Gasparetto is in agreement with Gómez Muñoz that conducting clinical trials to collect data on paediatric IR device effectiveness would be “very difficult”. “It is very tough to run these studies to prove a certain piece of equipment is safe and effective because there are enough treatments that doctors and parents are comfortable with, and to try something new? Using a new device? This would require convincing families to take part, and this is very difficult,” he explained.
“Paediatric IR is an emerging specialty right now, there are not enough paediatric interventional radiologists in the world. We are nowhere near where surgery is or even where adult IR is.” Where “inventiveness” and “[adaptation]” reach their end, however, Gasparetto is hopeful that, as paediatric interventional radiologists grow in “manpower” they will be able to put pressure on manufacturing companies to mass produce smaller and shorter devices. He commented: “As we grow, more evidence will become available, and we will be able to push for paediatric-specific devices. But where we are standing right now, we do not yet have the numbers.”
Indicative of this growth, in 2023, the US Food and Drug Administration established the Paediatric Device Consortia which has funded development of medical devices for children, and brings together “experts from various fields, including clinicians, engineers and researchers, to promote the development and accessibility of paediatric devices”, Gómez Muñoz writes in his plea. Referencing Patel’s research, Gómez concludes that regulatory bodies must “collaborate with the increasing number of paediatric interventional radiologists worldwide” to further research and innovation.
Discussions on this topic are increasing, although “intimate” as Gasparetto put it, the Society of Paediatric Interventional Radiology (SPIR) meeting in recent years has facilitated “more conversations about this issue, gaining a voice”. Patel also relayed SPIR’s significance in the UK, and to the wider international specialty. “It was discussed at SPIR last year, although these are European regulations, once this change is implemented and affects a manufacturer’s ability to sell in Europe, they will withdraw non-viable products from the USA and UK markets too—and this is not just affecting IR worldwide, but interventional cardiology and others”, Patel underlined.
With sights set on the near future, Gasparetto believes that the development of medical devices indicated explicitly for children will occur “soon”, given the “rate of growth [paediatric IR] is experiencing” today. Although, proceeding with more trepidation, Gómez Muñoz stated that “more measures need to be considered”, such as the use of large registries for device clearance and the inclusion of children in IFUs, which will “improve treatment outcomes and patient satisfaction”. Pushing further, however, Gómez Muñoz concluded that the “final answer must come from a common effort from regulatory parties, private companies, public entities and healthcare providers” to support research and device innovation for paediatric IR.
Medtronic has announced approval from the USA Food and Drug Administration (FDA) for the Symplicity Spyral renal denervation (RDN) system for the treatment of hypertension. The company has said that it will immediately begin commercialisation following the approval.
“Medtronic has always believed in the potential of this therapy. We partnered closely with leading experts in our clinical community who could help us in our journey to get this technology to the people who need it most,” said Jason Weidman, senior vice president and president of the Coronary and Renal Denervation business within the Cardiovascular Portfolio at Medtronic. ‘It was the promise of this therapy that enabled Medtronic to keep going, even when others exited the renal denervation space. High blood pressure is a global health issue, and patients need more options to manage their blood pressure. The approval of the Symplicity blood pressure procedure represents a significant milestone for physicians and patients in the treatment of hypertension.”
The Medtronic Symplicity blood pressure procedure delivers radiofrequency energy to nerves near the kidneys that can become overactive and contribute to high blood pressure.
“The Symplicity blood pressure procedure is safe and effective, providing significant ‘always on’ blood pressure reductions for patients,” said David Kandzari (Piedmont Heart Institute, Atlanta, USA), co-principal investigator of the SPYRAL clinical programme. “This landmark approval is the culmination of rigorous scientific study and clinical trials, including long-term, sham-controlled studies in the presence and absence of medication, and the largest real-world study.”
Although currently limited for investigational use in Japan, China and Canada, the Symplicity Spyral renal denervation system is approved for commercial use in more than 70 countries around the world.
Ramon Varcoe presented the new data at VEITHsymposium 2023
Two-year data from the SWING trial, a first-in-human study of the safety and performance of the Sundance sirolimus drug-coated balloon (DCB; Surmodics), have been presented at this year’s VEITHsymposium (14–18 November, New York, USA).
The SWING trial is a 35-patient prospective, multicentre, single-arm feasibility study to evaluate the safety and performance of the Sundance sirolimus DCB when used to treat occlusive disease of the infrapopliteal arteries. The SWING trial enrolled patients with stenotic or occluded lesions of the infrapopliteal arteries, a reference vessel diameter of 2–4mm, and a total lesion length of ≤230mm for treatment with the Sundance sirolimus DCB at eight sites in Australia, New Zealand, and/or Europe. Study patients will be followed for 36 months post index procedure.
The primary safety endpoint is defined as the number of patients with a composite of freedom from major adverse limb event (MALE) and perioperative death at 30 days following the index procedure. The primary efficacy endpoint is the rate of late lumen loss at six months, as assessed by quantitative vascular angiography. Both primary endpoints of the SWING trial were achieved.
Primary safety endpoint data showed no perioperative deaths or major amputations at 30 days, and just one major reintervention was reported among the 35 trial patients. The per protocol (PP) population reported an 8.3% rate of major adverse events (two clinically driven target limb revascularisations) at six months, with no additional adverse events reported for PP subjects in the 12 or 24-month data. Primary efficacy data show late lumen loss of 1mm (±0.79mm) across 35 lesions at six months, indicating that the large luminal gain achieved immediately after the procedure was sustained post procedure.
Target lesion primary patency rate, defined as freedom from target vessel occlusion or target lesion revascularisation associated with deterioration of Rutherford clinical classification and/or increase in size of pre-existing wounds (or occurrence of new wounds), and lesion restenosis >50%, was 71.4% at 24 months in the PP population. The Rutherford clinical classification describes seven categories of peripheral arterial disease, including both the patient’s clinical symptoms as well as objective findings, and is used to assess disease progression.
Andrew Holden
“The two-year safety and performance results of the SWING trial continue to show promise for the Sundance sirolimus DCB in treating below-the-knee disease in a challenging CLTI [chronic limb-threatening ischaemia] patient population where options are currently limited,” said Andrew Holden (Auckland City Hospital, Auckland, New Zealand), co-lead investigator, in a Surmodics press release.
“We need to continue to strive for better treatments for treating infrapopliteal disease,” added co-lead investigator Ramon Varcoe (Prince of Wales Hospital, Sydney, Australia), who presented the new data at VEITHsymposium 2023. “These results are promising and will inform future trials, which we hope will continue to advance improved treatments for our patients.”
Vivasure Medical has enrolled the 100th patient in its PATCH clinical study, a multicentre, single-arm, pivotal study evaluating the safety and efficacy of the Vivasure PerQseal closure device system.
The US Food and Drug Administration (FDA) granted investigational device exemption (IDE) approval earlier this year to advance the PATCH study forward.
“We are grateful to the one hundred patients who have been enrolled in this study to date and the brilliant physician investigators working to gather data about our technology,” said Andrew Glass, chief executive officer of Vivasure Medical. “This marks an important milestone for Vivasure as it brings us closer to our goal of demonstrating PerQseal’s potential in supporting successful percutaneous cardiovascular therapies.”
Large hole arterial access is required for clinicians to perform numerous percutaneous cardiovascular procedures such as transcatheter aortic valve implantation (TAVI), thoracic and abdominal endovascular aneurysm repair (TEVAR and EVAR), and the use of a cardiac assist device (CAD).
The current approach to large-diameter arterial closure is a surgical repair or the use of suture- or collagen-based closure devices. Both can result in major vascular complications, such as vessel distortion at the closure site, which may lead to stenosis, thrombus formation or abrupt closure.
PerQseal is designed as a sutureless, fully absorbable synthetic implant for large-bore vessel punctures. Its low profile patch can be placed from inside the vessel and is intended to make deployment simpler and more controlled than conventional closure techniques. Clinical studies to date have shown a low complication rate and high technical success.
The PATCH pivotal study will enrol and follow up to 188 patients across the USA and Europe. The company intends to use the clinical study results to support an FDA premarket approval submission as well as multinational commercial launch of the PerQseal system for large hole vessel closure.
Clockwise: Nick Brown, Raman Uberoi, Parag Patel, Michael Lee
Clockwise: Nick Brown, Raman Uberoi, Michael Lee, Parag Patel
Over several decades, interventional radiology (IR) has scaled to significant heights, leading technological advancements and minimally-invasive techniques. As these milestones have been reached, however, historical pitfalls have deepened, prompting international discussion about the current structure of IR and the value of obtaining clinical specialty status. Building a figurative heatmap of IR’s progress to specialty today, Interventional News spoke to interventional radiologists around the globe to track the field’s burgeoning recognition, concurrent problems and future stability.
Introducing the ‘Applying for IR specialty status: lessons learned’ session at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark), Michael Lee (Beaumont Hospital and Royal College of Surgeons in Ireland, Dublin, Ireland) asked: “What is wrong with IR?” Among his responses, Lee noted “there is little recognition, little visibility and most importantly, little credibility”. Speaking to Interventional News, Lee expanded on his statement, averring that visibility remains a “big issue”, rendering IR “completely invisible” to the health authorities who provide vital funding, as well as medical students in training who may elect to subscribe to IR.
“We are fishing in the wrong pond,” Lee averred, “[medical students] do not know what IR is. There is little mentorship or teaching—I am generalising, as there are excellent medical student educational programmes in certain large academic centres, but in the real world, outside of these large centres, medical students do not know who we are.” He described how, often, their “pond” is synonymous with trainees who enter diagnostic radiology but “not to do a hands-on specialty” like IR, they then must be “[convinced]” otherwise by interventional radiologists like Lee advocating for the specialty.
In New Zealand and Australia, the line between diagnostic and IR is equally blurred—Nick Brown (The Wesley Hospital, Auchenflower, New Zealand) explained that interventional radiologists are recognised as ‘special diagnostic radiologists’, which is the only specialty title available to fellows of the Royal Australian and New Zealand College of Radiologists (RANZCR). Brown is advocating for the creation of a ‘Specialist interventional radiologist’ title which would provide “an identity” to “elevate [IR] status and promote the high-value care that interventional radiologists provide to patients”.
To gain formal recognition for IR at his centre however, practice must be accompanied by an accredited training programme, said Brown. “Thus, RANZCR is working with the Society for Interventional Radiology in Australia and NZ (IRSA) and the Australian and New Zealand Society of Neuroradiology (ANZSNR) to develop, for the first time, two specialist training programmes in IR and interventional neuroradiology (INR).” Having an “identified pathway” to IR specialism Brown said, will “unlock the full clinical capacity of IR”, including the creation of clinical units and consulting rights, and could “attract appropriate funding and reimbursement for their departments and hospitals”, he stated.
Issues with ill-defined IR training pathways are also reported in the UK, as Raman Uberoi (The John Radcliffe Hospital, Oxford, UK)—recipient of the British Society of Interventional Radiology (BSIR) 2023 Gold Medal for his ‘outstanding contribution to the work of both the society and interventional radiology’—explained, outlining a culture of “jumping through hoops” to access IR in the UK. He noted how entrance to the field can be “vague”. Often trainees enter into radiology and learn about imaging for the first three years before having the option to broach IR, “and of course that [traces] many challenges,” Uberoi asserted. With distinct IR specialty status, he stated, trainees could bypass these challenges and “learn about imaging, but relevant to IR techniques and procedures, with a clearer distinction of what we are about and what we are going to do—it makes it much more attractive”.
Implementing a training curriculum that includes clinical practice and IR procedural skills “from day one” is crucial, agreed Lee: “That is why IR specialty status is so important. We must have a dedicated training pathway from the get-go to attract trainees interested in a ‘hands-on specialty’ like IR or the field will continue to be impoverished of trainees. In addition to trainee impoverishment, the other main limitation of current training programmes is the difficulty of producing IR specialists with the clinical expertise required to deliver the necessary patient care associated with current IR practice.”
In a co-authored article published in CardioVascular and Interventional Radiology (CVIR) earlier this year, Lee and Uberoi collectively discuss the third and latest edition of the CIRSE European Board of Interventional Radiology (EBIR) curriculum, which forms a distinct syllabus and examination of IR competence throughout Europe. The latest iteration places focus on “greater clinical responsibility for patients”, defining “core competencies [..] to improve the future training and quality of interventional radiologists worldwide, improving patient outcomes and care”.
Parag Patel (Medical College of Wisconsin, Milwaukee, USA) who also presented at CIRSE, spoke to Interventional News to provide insight on behalf of IR in the USA, which gained primary specialty status in 2012. Patel explained that recognition for IR in the USA enabled the specialty to “not just highly encourage or strongly suggest, but require, base-line competencies in training for interventional radiologists.
“Primary specialty recognition allowed us to fundamentally change those requirements, expanded the training to two full years of IR training, not just procedural but clinical intensive care unit management admission discharge,” Patel highlighted.
Certification of this programme by the Accreditation Council for Graduate Medical Education (ACGME) and IR specialty recognition from the American Board of Medical Specialties (ABS) has also improved recruitment, with Patel noting an uptick in senior medical students applying to join the clinical specialty. “These are future leaders—these are bright, young individuals who would have been leaders in vascular surgery, cardiology, oncology, and are now going to be leaders in IR,” he said, emphasising their “elevated workforce of talent”.
Yet, Patel remarked, “there are always growing pains”, explaining how IR is still “[appropriately]” housed within the department of radiology. Although their chairman, who oversees their division, understands imaging, they “do not always understand how to support [IR] clinical practice” he stated.
For Lee, clinical practice and longitudinal care represents a clear distinction that can be made between the needs of IR and diagnostic radiology, but without primary specialty or a chairman who is an interventional radiologist, asking for dedicated time for clinical practice “is met with friction and confrontation” he said. Uberoi added that longitudinal care is a “critical” feature of IR, and for patients, knowing that the doctor who initially assesses you will be the one to treat you and to whom questions can be directed is essential. Without the “trust and communication” that is built through regular touchpoints with a dedicated specialist who takes “ownership” of their patients, interventional radiologists are left with “unrealistic” and ineffectual practices today, said Lee.
Equally, this remains an issue in the USA, Patel conveying that “if IR is not given the same [recognition] in its ability to see patients and manage them in a multidisciplinary format, then we are not supported and frankly our treatments will not be advocated for”. He explained it is a “rare instance” that a specialty will advocate for another’s procedures, and that only your own specialty will be willing to do so, proving that ultimately “if you are not at the table, you are on the menu, as they say”, Patel punctuated.
As the frequency of these conversations increase, the “deficiencies” in IR are thrown into light, Lee conveyed, but the “chance to talk to the right people about what IR is all about and its problems” has been instrumental in sparking progress. “We now have a national programme for IR in Ireland to look at the current situation. Over the next 10–15 years, IR should be a robust part of Irish healthcare and hopefully a primary specialty. This may have never happened if we had not embarked on this—I always remember that song and Mick Jagger singing: You can’t always get what you want, but you may get what you need.”
Despite positive conversations, the speakers concurred that unanimous action to strengthen the field of IR “not because you feel it is better, but based on what is best for patients” as Patel stated, is still crucial. For Brown, a strategy of “good planning and perseverance” has promised a formal training programme by 2026, with specialty status to shortly follow, which he believes will be the “single greatest boost to IR practice in recent times”.
Finally, the speakers agree that these changes must happen to secure IR practice for the future, in Lee’s words: “If we do not take control and if we do not take charge of our own destiny, we will be jeopardising the future sustainability of IR. Maybe I am being a little nihilistic, but I believe that we must start changing things and it needs to happen sooner rather than later.”
CMS outlined in the decision memo, dated 11 October, that it had found “coverage of percutaneous transluminal angioplasty (PTA) of the carotid artery concurrent with stenting is reasonable and necessary with the placement of a US Food and Drug Administration [FDA]-approved carotid stent with an FDA-approved or cleared embolic protection device” for Medicare patients who have symptomatic carotid stenosis ≥50% and asymptomatic carotid stenosis ≥70%.
In the July proposed decision, the federal agency detailed an expansion that would significantly broaden coverage for carotid stenting, expanding Medicare coverage to individuals previously only eligible for coverage in clinical trials, removing the limitation of coverage to only high-surgical-risk individuals, and removing facility standards and approval requirements.
What is next?
Looking ahead, new evidence is on the horizon for carotid artery stenosis patients, with data from the carotid revascularisation and medical management for asymptomatic carotid stenosis (CREST-2) trial due to be released next year. CREST-2 consists of two independent multicentre, randomised controlled trials of carotid revascularisation and intensive medical management versus medical management alone in patients with asymptomatic high-grade carotid stenosis.
Speaking on behalf of the Society for Interventional Radiology (SIR), immediate past president Parag Patel (Medical College of Wisconsin, Milwaukee, USA) provided the following comments:
SIR applauds the decision to expand coverage for PTA with CAS to include individuals of standard surgical risk, patients with symptomatic carotid artery stenosis ≥50%, and patients with asymptomatic carotid artery stenosis ≥70%.
SIR supports the decision to allow operators trained in performing these procedures to also complete the requisite neurologic assessments prior to and following treatmentThis underscores the expectation and requirement for ownership of the clinical management of the patients that we treat. We support the requirement for shared decision-making processes among physicians and the patient in determining an appropriate treatment.
This expansion will allow comparable therapies to be offered in a balanced discussion with patients as they determine with their doctors the best course of action. By expanding coverage to patients at standard surgical risk, Medicare is allowing all to benefit from the advantages of a minimally invasive procedure.
It is clear that we are improving in our knowledge and use of medical management—CREST-2 is comparing differences between intensive medical management (IMM) alone compared to CAS plus intensive medical management for patients with severe asymptomatic carotid stenosis. Prior studies have demonstrated positive results but were not followed long enough to sufficiently determine long-term benefits.
We should be in the business of disease prevention, and I suspect that we will see significant advantages with intensive medical management for many patients and likely prevention of many requiring any intervention at all.”
Liz Kenny of the Royal Brisbane and Women’s Hospital (Brisbane, Australia) gave her radiation oncologist’s take on the “120-odd-year” history of radiation therapy, how to plan it, and its delivery at the 2023 European Conference on Interventional Oncology (ECIO; 16–19 April, Stockholm, Sweden). “We—and you—stand on the shoulders of giants,” was one of her key take-home messages for delegates, specifying that these giants span many scientific disciplines and nations and have enabled the development of radiation oncology into the area of medicine it is today.
“Every single advancement in radiation therapy has been made hand-in-hand with physicists, industry, physicians, and radiation therapists across nations,” Kenny began. “The aim has always been to work out how we can maximally treat cancer tissue, while maximally protecting normal tissue.” In order to advance this area of clinical practice, Kenny elaborated on the “unwavering commitment to quality assurance” has also been necessary, alongside “our understanding of cancer biology and radiobiology” and “minimising short-and long-term complications, while knowing what they are”.
Kenny paid homage to Rod Withers (University of California, Los Angeles, USA), who she described as “a father of radiobiology who led us to understanding the relationship between the overall treatment time, total dose and the number of treatments. Lester Peters (University of Queensland Medical School, Queensland, Australia) was next in Kenny’s roll call of significant contributors to radiation oncology, as someone who spearheaded the need to embed quality assurance, in both trials and daily clinical practice, demonstrating the increased cure that this brings. Vincent Gregoire (Léon Béard Cancer Center, Lyon, France) was then attributed with the sage advice that intensity-modulated radiotherapy needs daily image guidance.
Computed tomography (CT) scanning was one of the advancements that Kenny credited with “revolutionising everything” in the field of cancer care. “The basic design of linear acceleration cannot really change,” she pointed out, “but how we manage it, how we rotate the treatment beams around patients, shaping the beams and modifying the dose coming through are all factors that can be altered as we treat. And, of course, computers, they have changed the world,” Kenny emphasised, before highlighting that planning systems, likewise, “have evolved apace” with “our ability to manage motion and reproducibility”. Machine learning also featured on Kenny’s list, which she explained “allows us to be 85% ready before we even start”. Then addressing the audience, she opined that “that has direct applicability in the [interventional radiology] world.
“We started off with chinagraphs, drawing on orthogonal films, and with two-dimensional planning, so we had a massive risk of geographic miss,” Kenny recalled. She commented that, even with the evolution to 3D planning, collateral damage was by no means a thing of the past. “So, with medical physicists we waged the war on normal tissue damage.” She charted the move from static to rotational beams, to changing the dose delivered in those beams, and changing the shape. “That is what allows me to treat someone’s very complex nasopharynx cancer, or ablate a patient’s lung cancer,” Kenny celebrated, all the while knowing “what outcome and side effects I expect, and what the cure rate has the potential to be”.
“Once we have made a decision to treat, the first step is planning, and planning is designating the right dose to the right place and determining what dose we will allow normal tissue to receive,” Kenny proceeded, referring to the capabilities nowadays for calculating the dose to different parts of the surrounding tissue ahead of delivery. However, she conceded that there may well still be plenty of scope for evolving diagnostic and functional imaging further.
Kenny called planning a “multistep process that involves a cast of thousands” to enable quality assurance at every step, from simulation, image fusion, to mapping out dose on every CT scan slice, to peer review, final acceptance of the treatment plan and then testing on a phantom “which is not so easy for [interventional radiologists]”. Planning and delivery can also be tailored according to whether the patient will be free breathing or assuming a deep breath hold or tracking the tumour during the delivery of treatment. Kenny supplemented, going on to detail that for stereotactic brain treatment, the immobilisation system with thermoplastic shells is “very exacting”.
Concluding, Kenny walked the audience through her radiation oncologist’s approach to delivering dose to patients, using image guidance: “There is no consolation for missing the target volume, no matter how sophisticated the technique of planning and delivery”. This, she summed up, by saying that “you have to be in the right place”. This is all the more critical when performing stereotactic ablative treatment in the brain, where there is a “0.02 to 0.05mm” tolerance.
“We have evolved in the last 40 or 50 years from 2D planning and treatment to 3D conformal planning to Intensity Modulated Radiation Therapy, all image driven. We can now sculpt and manipulate dose,” were among Kenny’s closing remarks. “It has been a wonderful journey, with our equipment following suit all the way through to helical devices and protons, with treatment rooms now looking like something out of Star Trek”. Kenny believes that machine learning through cloud-based sharing will enable continuous improvement in the field of planning and delivery of radiation therapies. “As imaging advances, we will become more accurate again and even now we are starting to be able to adapt during treatment.”
Liz Kenny is a professor at the University of Queensland and senior radiation oncologist at the Royal Brisbane and Women’s Hospital (Queensland, Australia).
Shape Memory Medical, developer of custom shape memory polymers for endovascular markets, announced that one-year data from the AAA-SHAPE safety trial will be presented during the 50th annual VEITHsymposium (14–18 November, New York City, USA) on Tuesday, November 14, 2023.
AAA-SHAPE is the company’s prospective, multicentre, early feasibility study of the IMPEDE-FX RapidFill device when used for abdominal aortic aneurysm (AAA) sac management during elective endovascular aneurysm repair (EVAR). The trial, which enrolled a combined 35 patients in New Zealand and The Netherlands, is evaluating the application of shape memory polymer in AAA patients and its potential to remodel the AAA sac and improve aneurysm sac regression following EVAR. Patients will be followed for five years.
Michel Reijnen (Rijnstate Hospital, Arnhem, The Netherlands) and principal investigator for AAA-SHAPE Netherlands will present the data. “We are encouraged by the one-year results and how shape memory polymer technology may ultimately influence sac behaviour,” stated Reijnen.
IMPEDE-FX RapidFill, the study device, incorporates the company’s novel shape memory polymer, a proprietary, high volume, porous embolic material that is crimped for catheter delivery and self-expands upon contact with blood for rapid conversion to organised thrombus. Pre-clinical studies have shown that shape memory polymer is regenerative, activating the formation of new cellular growth as the thrombus remodels and the material is absorbed.
Andrew Holden, (Auckland City Hospital, Auckland, New Zealand) principal investigator of AAA-SHAPE New Zealand, remarked: “We are increasingly becoming more aware of the importance of AAA sac regression after EVAR. Active sac management with shape memory polymer may become an important addition to EVAR.”
“The availability of one-year data from the early feasibility study presented at VEITH marks an important milestone in the clinical development of shape memory polymer for aneurysm sac management,” said Ted Ruppel, president and CEO, Shape Memory Medical. “We look forward to the next phase of the AAA-SHAPE program in a head-to-head study.” The company recently announced US Food and Drug Administration (FDA) investigational device exemption (IDE) approval to initiate the AAA-SHAPE pivotal trial, a randomised controlled study comparing EVAR plus sac management with IMPEDE-FX RapidFill to standalone EVAR.
Interventional radiology (IR) is a main player in modern clinical oncology practice. Almost every tumour board has a seat for IR. Clinical oncology is a rapidly evolving field as well; new therapies are being introduced frequently allowing for treatment of a wide spectrum of cancers. Among these treatment options, radiotheranostics represent a unique platform where diagnostic and therapeutic purposes are combined into a single paradigm. This allows diagnosis and treatment of advanced stages of cancer with high precision, fitting very well into the modern concept of personalised medicine.
Peptide receptor radionuclide therapy (PRRT) is the most common radiotheranostic form in clinical practice. The two most widely available radiopharmaceuticals currently are Lutathera for treatment of gastroenteropancreatic neuroendocrine tumours (GEP- NETs) and Pluvicto for treatment of castration resistant metastatic prostate cancer. Different clinical specialties, including nuclear medicine, IR, medical and radiation oncology have high interest in radiotheranostics. With many specialties digging into this field, it is extremely important for the interventional radiologists to be updated about the advances in radiotheranostics. The aim of this article is to update IRs about the key concepts of radiotheranostics and to explore ways by which IR remains a key player in modern oncology practice.
To start with, most interventional radiologists are familiar with the use of yttrium-90 (Y90), loaded on resin or glass microspheres, for transarterial treatment of liver tumours. However, there are significant differences between Y90 therapy and PRRT. Resin or glass loaded Y90 microspheres are essentially flow directed therapists; blood flow dynamics are the main factors controlling microspheres distribution. PRRT have the additional advantage of being linked to receptor specific ligands. This allows these radiopharmaceuticals to attach to active, disease specific, receptors which can be easily screened for and quantified using advanced PET/CT imaging tracers. Additionally, there are key differences between Lutetium-177 (177Lu) (a common radionuclide for clinical PRRT radiopharmaceuticals) and Y90. While both are beta particle emitters, Y90 is known to have a longer penetration range (maximum=11mm, mean=3.9mm) and higher energy (mean of 0.94MeV) compared to 177Lu which has a mean energy of 0.15MeV and shorter penetration range in human tissues (maximum=1.7mm, mean=0.23mm). These differences may have implications on patients selection for either therapies, as detailed later herein.
Interventional radiologists need to be aware of the fact that, as more clinical theranostic therapies become available, the decision-making process regarding the best treatment option in specific clinical scenarios will become more sophisticated. For example, many metastatic NETs present with liver metastatic disease. These patients have historically been treated by liver directed therapies (LDTs) and thermal ablation. With Lutathera now on board, questions may arise about whether metastatic liver disease would respond better to LDTs versus PRRT. The answer to this question is onerous and requires expertise in the field, sometimes even extended discussions in multidisciplinary tumour boards. A higher somatostatin receptor expression, reflected by a higher Krenning score of 3 or 4, is a good predictor of favourable response to PRRT. On the other hand, lower Krenning score metastatic deposits reflect lower receptor expression and may respond better to LDTs. Another factor to consider is the extent of metastatic disease. In our experience, patients with extrahepatic widespread metastatic disease are good candidates for intravenous PRRT therapy, while liver only/dominant metastatic disease may be better candidates for early LDTs, preserving PRRT for later advanced stages. The higher penetration range and beta particle energy of Y-90 spheres may favor the use of Y-90 intra-arterial therapy for large infiltrative tumours and may explain that tumours >2–3cm in size may not respond well to PRRT.
An exciting potential opportunity for interventional radiologists is the possible intra-arterial administration of PRRT, combining the high selective advantage of catheter-directed therapy with precise receptor-targeting potential of PRRT. Several studies have demonstrated a higher tumour to background uptake using the intra-arterial approach. However, more studies are needed to investigate how this may reflect on progression-free and overall survival. If proved to add survival benefit, intra-arterial PRRT can be a unique niche for those interested in this field.
To conclude, theranostics therapy is a rapidly evolving field with lots of potential in modern oncology practice. Interventional radiologists, who are already key players in interventional oncology practice, need to realise the added value of this innovative paradigm and make necessary changes to their practice in response to the advances in the field. Radiotheranostics should not be visualised as a source of threat for IR practice, but rather a gateway to one of the most revolutionary treatments of cancer in the coming years.
Islam Elhelf is a clinical assistant professor and programme director at Augusta University (Augusta, USA).
Presenting on machine learning (ML) to predict responders following prostatic artery embolization (PAE) at the British Society of Interventional Radiology (BSIR; 8–10 November 2023, Newport, UK) annual meeting, Ganesh Vigneswaran (University of Southampton, Southampton, UK) sets out his case for the use of ML to “personalise care in PAE, to empower our patients to make better informed decisions and avoid complications”.
Looking first at PAE itself, Vigneswaran averred that therapeutic success is “not the same for everyone”, however bolstered by ML, there is potential to predict who may benefit most from this treatment. “ML is a branch of artificial intelligence,” he explained, “it can find complex patterns in data and works by creating a series of dependant variables or predictors linked with an outcome to build an algorithm that enable it to learn the rules of the game to predict future outcomes with new data”.
To set about proving this hypothesis, Vigneswaran told BSIR delegates, him and his team reviewed data from the UK-ROPE multicentre study which pulled data from 17 UK centres between 2014–2016 including around 216 PAE patients. Inputting urodynamic, radiological and clinical predictor variables, Vigneswaran stated they had over 40 different predictors however there were “significant missing data” which led the investigators to restrict the subanalysis to 6–7 variables to predict international prostate symptom score (IPSS) at one year which showed some “significance”.
“But should we just stop there?” Vigneswaran asked the audience, musing if we can learn more through “analysing our errors”, or if, through “domain expertise” physicians can “move beyond just aiming for an accurate model and actually analyse why”.
Reviewing their data on IPSS reported and predicted outcomes from baseline to one year, Vigneswaran reported some “discordance” between the two, which he believes shows an “underlying role of psychology in PAE outcomes”. He iterates however that “the more data the better”—in order to “increase the power of prediction”, more predictive variables are needed.
Using the example of prostate volume and maximum flow rate (Qmax) at one year in this dataset, the speaker outlined that additional predictors including baseline volume, Qmax, residual volume, Abrams Griffiths number, and IPSS, which resulted in an increase in regression values, notably an increase of 0.05 to 0.27 in Qmax.
Summarising his discussion, he stated that there is predictive value within the clinical radiological and urological variables and avers that more data should be collected. “Machine learning has shown promise in the ability to predict PAE outcomes and our research has shown a clear signal from preprocedural variables”. The speaker went on to note that more data are needed, adding that this will “improve our performance and be used to counsel and guide individual patient decisions in urology and interventional radiology clinic”.
Honoured as the British Society of Interventional Radiology (BSIR) travelling professor, Ian McCafferty (The Radiology Clinic, Birmingham, UK) gave the Graham Plant lecture at the BSIR annual meeting (8–10 November 2018, Newport, UK). Titled ‘Acute trauma intervention: Have we got it right?’ McCafferty’s discussion focused on paediatric interventions, posing the central question: “Can we really ignore paediatric trauma? What does it say about us if we ignore the younger generation?”
Setting out the numbers, McCafferty first highlighted a workforce consensus which was carried out by The Royal College of Radiologists in 2021, showing that there are approximately 230 interventional radiologists in the UK, with an upward trend in recent years. “But this increase is not as much as we need,” McCafferty stated, noting that this census was the first to consider paediatric interventional radiology (IR).
“By the current definition, if you do predominantly 50% of you direct clinical care as an interventional radiologist in paediatrics, [the census found] that there are currently 12 in the UK,” he told BSIR delegates. Comparing this statistic to the population of the UK, he highlight that the UK is operating via a “one in a million” paediatric IR service, showing the stark contemporary deficit in active operators. “There is a disparity between the accessibility for paediatric services,” McCafferty too making notice of the “problems” within adult IR services in the UK, as only 50% are currently able to provide 24/7 care.
Having carried out a WhatsApp survey among colleagues at several centres, McCafferty said he looked to find out what interventional radiologists are performing at their sites. “Unsurprisingly,” he found all of the adult and children, and children’s institutions had paediatric services available on site, however found that, in children’s national treatment centres (NTC), there were “very few” paediatric interventional radiologists, reducing service accessibility overall.
“I think there is an unconscious or conscious unwillingness to help,” McCafferty told delegates, reminding them of the familiar mantra which states that children should not be treated as “little adults”. “The problem with this is it induces fear and anxiety in adults potentially having to treat children who do not routinely do so. That causes a lot of anxiety, but also potentially causes trust anxiety—there are always concerns of medical and legal risks.”
Speaking on the long-term effects of the deficit in paediatric trauma management in the UK, McCafferty noted the “astronomical” economic and social burden that could occur as a result of “having trauma badly managed”, emphasising the detrimental effects that could be attributable to lack of IR access on the “developmental potential” of this “adversely affected” group.
From centre to centre, McCafferty makes clear that there is a “void” in knowledge of paediatric IR. In his understanding of the environment navigated by Alex Barnacle (Great Ormond Street Hospital, London, UK)—the 2018 BSIR Graham Plant lecturer—he stated that, when acting as travelling professor, Barnacle oftentimes was asked to speak about paediatric intervention, proving that “they are not seeing it locally”, said McCafferty.
Concluding his BSIR lecture, McCafferty bolstered his central theme, stating that paediatric IR must be recognised so that young people are not overlooked: “We have to look at ourselves and say: Can we really ignore paediatric trauma? It is not very common, which means it will present randomly at all of your centres and we must think about what this does say about us if we are ignoring the younger generation.”
A new study published in BJS Openhas found that revascularisation treatment to restore blood flow to the legs of patients with severely blocked arteries is no more expensive than carrying out an amputation.
The peer-reviewed paper is the first to compare the total costs of follow-up care after revascularisation and major lower limb amputation across primary, secondary and community settings in the UK.
Many previous studies have focussed only on the immediate costs of the procedures to a hospital.
The observational research, carried out by the Department of Cardiovascular Sciences at the University of Leicester and commissioned by global healthcare company Abbott, analysed routinely collected data for 4,252 patients who were diagnosed with critical limb-threatening ischaemia (CLTI) between January 2016 and January 2019.
296 patients (6.9%) underwent an angioplasty, 75 (1.7%) had bypass surgery, and 141 (3.3%) a major lower-limb amputation as their first procedure.
Patients undergoing amputation had the highest number of community care appointments in the 12 months after their operation, and far longer inpatient stays if they needed to be readmitted to hospital during that time. They also had the highest number of cardiovascular events and deaths at one-year.
This meant the combined costs of postoperative care at one year following major lower- limb amputation (£7,140.90) were comparable to those of the most common procedures to restore blood flow such as angioplasty (£7,040.00) and bypass surgery (£7,481.90).
CLTI is a severe form of peripheral artery disease (PAD), a common condition which affects a fifth of the population over the age of 55, where a build up of fatty deposits in the arteries restricts blood supply to the legs. It is the most common cause of limb amputation.
Athanasios Saratzis (University of Leicester, Leicester, UK), lead author of the paper, said: “There had been a misconception that revascularisation is more expensive than amputation, but by looking at the true combined costs of follow-up care across the whole health system, we have for the first time been able to reveal the significant postoperative costs of amputation. With better patient outcomes, we are calling for revascularisation to become the default treatment option for eligible patients.”
Hany Zayed, consultant vascular and endovascular surgeon, Guy’s and St Thomas’ NHS Foundation Trust, said: “It is important to consider the overall cost of patients with CLTI to the wider healthcare system. In order to achieve this, we needed to examine the cost implications of the patients’ contacts with health services throughout their whole journey. This approach will provide real reflection of the financial burden on the NHS of various management approaches to CLTI. This study highlights the real cost of limb amputation, which contrary to some beliefs, seems to be more expensive overall than most limb salvage approaches. This work provides valuable knowledge to inform those who look after patients with CLTI and those who fund their care.”
Jonathan Wood, regional director of Abbott Vascular North Europe added: “Our goal is to continue to support physicians with the technology and research they need to deliver improved patient health outcomes. This new study provides a valuable resource for physicians who may be considering appropriate treatment for patients with CLTI.”
Interventional radiologist and medical director for The Royal College of Radiologists, Raman Uberoi (The John Radcliffe Hospital, Oxford, UK), gave this year’s Andreas Gruentzig Lecture at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark). Central to his lecture was the designation of speciality status in interventional radiology (IR), and the liberty this may provide clinicians to affect innovation in the field, as well as furthering its “vital” evolution for the next generation of interventional radiologists.
In a presentation titled ‘Interventional radiology: The next generation’, Uberoi began by making no uncertain parallel between the “futuristic and technologically-driven” evolution of Star Trek’s computer-generated imagery (CGI)—a passion of his—and the evolution of IR, which is “reshaping and changing, with new horizons, challenges and frontiers”, he told the CIRSE 2023 delegates. Before looking ahead however Uberoi explained that “it is important to look back”, giving a brief overview of the evolution or, “the roots”, of IR to date, spanning from the first angiography conducted in 1923, to the development of stents and contemporary tools used today.
“We are involved with just about every aspect of clinical practice, we have roles in patient safety, service improvement and patient outcomes—we would be forgiven for thinking ‘we are really in a nice position, we are doing exceptionally well’, but there is a problem.” Uberoi then introduced the challenges presented by the technician versus clinician dichotomy that faces interventional radiologists today, and has ultimately influenced “who is clinically responsible for the patient”, he posited. “The best outcomes for patients come when we are clinical interventional radiologists”, said Uberoi, which, he stated, begs the question: “Are we preparing the next generation for the needs of modern IR?”
What is needed to produce the next generation of modern interventional radiologists, Uberoi then flagged, is multifactorial. This includes increased touchpoints with patients throughout the treatment process, access to the latest technologies, and a revision of “unrealistic expectations” which assert that interventional radiologists must be “experts in imaging”, creating an environment in which burnout can thrive, he stated.
“We must gain control of our working lives, our practices, and our future” said Uberoi. Signalling a central theme of his lecture, he introduced the potential ways in which IR becoming a speciality could provide “solutions” to many of the field’s prevalent challenges. Among these challenges are the few UK trusts which have resource to provide 24/7 IR services—48%, Uberoi revealed, alongside the growing prevalence of burnout which has reduced the retirement age of interventional radiologists today to 44.
This “shocking” statistic reaffirms the importance of giving the new generation of interventional radiologists “control of their working future and working lives” which, he stated, means “rationalising the workload” and placing more focus on “core IR activities”. In order to make these changes, the speaker conveyed that evidence is needed to prove that IR is “improving and saving lives”, displaying several research titles that have been published in the space in recent years which have bolstered efforts of interventional radiologists worldwide, helping to distinguish IR as a speciality.
Leaving no stone unturned, Uberoi conveyed that the “strongest message” he can impart is that, with speciality status, interventional radiologists will be able to “control [their] destiny and future”, and this will enable clinicians to “gain control” over training and patient safety. He believes that speciality status could also help create a more defined career path for interventional radiologists, while “widening the pool” of potential takers who are considering the speciality.
“[Speciality status] will strengthen the voice of interventional radiologists—being a speciality gives you a strong voice at the table”, Uberoi asserted to delegates. With a touch of realism, he bookended this statement by noting that, if speciality status is universally granted, “nothing will change overnight”, but he underlined that “we cannot stand around waiting for somebody to deliver speciality status to us, we must start developing it ourselves”.
Imparting his final thoughts to the CIRSE 2023 audience, Uberoi highlighted that there are “hugely powerful drivers for change”, reiterating that evolution and speciality status are “vital” to the future survival of IR. “It is about improving training, the visibility of IR, improving workforce planning, and ultimately, high-quality patient-focused care”, Uberoi said, concluding that these crucial developments will only be achieved by fundamentally “improving the lives of interventional radiologists”.
Cordis has announced that its board of directors has appointed Scott Drake as chief executive officer (CEO) effective immediately. Drake most recently held the position of executive chairman of the Cordis board of directors. He will succeed Shar Matin, who has stepped down as CEO.
“Scott Drake has been on the Cordis board of directors since we acquired Cordis in 2021,” said Hunter Philbrick, H&F partner and Cordis board member. “He has a long history building world-class medical device organisations, bringing to market groundbreaking patient saving innovations and driving commercial excellence—along with the reputation of attracting, retaining, and developing world-class talent. Scott believes in Cordis’ ability to transform the medical industry, and with him as CEO, Cordis will achieve its vision of pioneering breakthrough cardiovascular technologies.”
Drake has over 30 years of medical device experience including as the president and CEO of the Spectranetics Corporation, where he increased shareholder value from approximately US$170 million to US$2.2 billion during his six-year tenure.
“I want to thank Shar for all he has done to stand Cordis up as an independent company. I have been on the Cordis board of directors for over two years, and I am thrilled to be taking on a more active role as CEO,” states Drake. “We are entering the next phase of the business, where Cordis is launching new products and driving a revolutionary business model with Cordis-X that will benefit our team, customers, patients, and shareholders.”
Obesity has been steadily increasing worldwide for at least 50 years. It directly contributes to the rising incidence of cardiovascular, musculoskeletal, and oncological diseases. Becoming one of the most concerning public health issues, obesity accounts for a majority of healthcare expenditures in Western countries, causing approximately three million deaths per year globally. While lifestyle interventions such as diet and exercise remain the foundation of weight management, only around 2% of individuals can sustain weight loss over a 12-month period.
For individuals with morbid obesity (BMI [body mass index]> 40kg/m²) or obese patients with significant comorbidities (BMI between 30–39.9kg/m²), bariatric surgery is considered the gold standard. This surgical procedure has demonstrated long-term weight loss and substantial improvements in metabolic syndrome, and overall survival. However, it is associated with a direct mortality rate of up to 2%, a high incidence of early complications including gastrointestinal fistulas, abdominal abscesses, thromboembolic events, as well as long-term nutritional deficiencies that can lead to chronic anaemia and bone fractures, among others. It is also a very expensive procedure, costing an average of US$38,000 without complications and US$64,000 with complications, which makes it almost impossible to be offered in public health systems of developed countries.
Over the past decade, we have witnessed the emergence of new drugs such as GLP-1 agonists, initially designed to treat diabetes, but now predominantly used for weight loss purposes. While they have been associated with weight loss of up to 15% within one to two years, they also come with a high incidence of adverse effects, including nausea, vomiting, diarrhoea, abdominal pain, and headache. Additionally, these drugs are costly, leading to treatment discontinuation and subsequent weight regain.
Hence, there is a need for minimally invasive, cost-effective, and long-lasting procedures for obesity treatment, and this is where bariatric artery embolization (BAE) comes into play. BAE aims to induce ischaemic changes in the gastric fundus, reducing the number of viable orexigenic cells and consequently lowering the concentration of acylated ghrelin in the bloodstream.
Ghrelin is the sole peripheral orexigenic hormone responsible for increasing appetite in the human body and is directly associated with fat accumulation and metabolic syndrome. From the first prospective clinical trial conducted in 2015 to the present, we have been able to demonstrate that BAE is a very safe procedure, with only 3% of serious adverse events and no reported deaths thus far. It consistently leads to a sustained decrease in plasma ghrelin levels of up to 32%, and a total body weight loss of approximately nine to 10% within 12 months.
Most trials conducted so far have utilized microspheres ranging between 300–500μm in size. While shallow ulcers are often observed during upper gastrointestinal endoscopy within one week post-procedure, they are mostly asymptomatic and disappear entirely within one month. In our trial titled ‘Bariatric embolization in the treatment of patients with a body mass index between 30 and 39.9kg/m2 (Obesity class I and II) and metabolic syndrome: A pilot study’, although we target multiple feeders of the gastric fundus (left gastric, short gastric, and gastroepiploic arteries) in 90% of the participants, the majority of ulcers were found in the lesser curvature, possibly due to unnoticed reflux of the embolic agent, while none were detected in the gastric fundus itself, making it a safe target for embolization.
This trial also demonstrated the direct impact of the procedure on insulin resistance, with normalisation of mean fasting blood glucose and a significant reduction in homeostatic model assessment for insulin resistance (HOMA-IR) from 7.3 to 3.7 within six months.
More robust data from randomised, prospective trials are forthcoming, which will probably establish BAE as an essential tool in the clinical management of obesity in the near future.
Rapael Braz is an interventional radiologist at the Real Medical Center (RIVOA) in Rio de Janeiro, Brazil.
Recor Medical's Paradise ultrasound renal denervation system
Recor Medical’s Paradise ultrasound renal denervation system
Recor Medical has become the first company in the USA to have a device-based therapy approved for the treatment of hypertension, after it was announced that the US Food and Drug Administration (FDA) has approved the company’s Paradise ultrasound renal denervation (RDN) system this week.
The Paradise system is intended as an adjunctive treatment option when lifestyle changes and medications have not adequately controlled a patient’s blood pressure. The Paradise catheter features the HydroCooling system, which circulates sterile water through the balloon catheter during the procedure to help protect the renal artery wall.
Approval of the Paradise system follows Recor’s positive FDA Advisory Committee Panel in August 2023. Earlier this year, results from Recor’s US pivotal study, the RADIANCE II randomised clinical trial, were published in the Journal of the American Medical Association (JAMA). In the study, the Paradise system met both the primary safety and effectiveness endpoints without any major adverse events.
“Despite the longstanding availability of dozens of affordable anti-hypertensive medications, blood pressure control rates in the USA are alarmingly low and falling. Given the significant blood pressure reductions seen in the ultrasound renal denervation trials, the Paradise ultrasound renal denervation system offers a much-needed advancement in our currently available options to control hypertension,” said site principal investigator Naomi Fisher (Brigham and Women’s Hospital, Boston, USA). “Ultrasound renal denervation has proven efficacy in patients with truly resistant hypertension, a population for whom medication therapy often fails. It is also effective in patients with mild to moderate hypertension who cannot tolerate enough medication to control their blood pressure.”
The Paradise system previously received CE mark and has been successfully introduced in Europe and is an investigational device in Japan.
“Recor is leading the way in bringing an innovative solution to clinicians and their patients struggling to control blood pressure. This FDA approval is the culmination of years of technical research and rigorous clinical studies,” said Lara Barghout, President and CEO of Recor Medical. “We are grateful to the patients who participated in the studies and to the clinical trial investigator teams whose diligence and dedication made FDA approval possible. We look forward to making this technology available to physicians and their patients nationwide.”
“Approval of the Paradise ultrasound renal denervation system marks an important milestone for the company and provides a new adjunctive treatment option for hypertension which remains inadequately controlled despite conventional therapies,” said Noriko Tojo, president and representative director of Otsuka Medical Devices and executive director of Otsuka Holdings Co, Ltd, the parent company of Recor Medical. “We are excited for patients and their healthcare professionals to have access to this technology to assist in managing hypertension and improving outcomes.”
Interventional News’ most read stories in October included significant data releases from TCT 2023 (23–26 October, San Francisco, USA); results from a study investigating sex disparities in outcomes post-TCAR; among several device updates.
Published in the Journal of Vascular and Interventional Radiology, a recent retrospective study which evaluated pain relief after percutaneous image-guided cryoablation in patients with symptomatic extraperitoneal endometriosis (EE), has found the treatment to be “safe and effective”.
ABK Biomedical, a medical device company dedicated to the research, development, and commercialisation of advanced imageable embolic medical devices, has announced the first patient treated in its Route90 US investigation device exemption (IDE) pivotal study.
While sex disparities regarding the outcomes of carotid revascularisation have “long been a concern”, new prospective data published in the Journal of Vascular Surgery (JVS) indicate that no such disparity exists between male and female patients treated with transcarotid artery revascularisation (TCAR; Silk Road Medical)—one of the most prominent approaches used to treat carotid artery stenosis.
Results of the LIFE-BTK randomised controlled trial have just been presented at TCT 2023. The data show that, in patients with chronic limb-threatening ischaemia (CLTI) due to infrapopliteal artery disease, an everolimus-eluting resorbable scaffold was superior to angioplasty at one year with respect to the primary efficacy endpoint.
Data from a patient-level meta-analysis—a factor in the US Food and Drug Administration’s (FDA) recent change of position on the use of paclitaxel-coated devices to treat peripheral arterial disease (PAD)—have been made public for the first time at TCT 2023 (23–26 October, San Francisco, USA).
Data from the REAL-PE study were presented at TCT 2023 (23–26 October, San Francisco, USA) demonstrating that patients treated for pulmonary embolism (PE) with the Ekos endovascular system (Boston Scientific) had lower rates of adverse events, including statistically significant lower rates of major bleeding, within seven days following their procedure compared to the FlowTriever system (Inari Medical).
Robocath has announced the results of its CARE clinical trial focusing on robotic carotid stenting—the first phase of a research programme launched in July 2021 by Robocath and Rennes University Hospital (Rennes, France), which, in the long term, is aiming to enhance current and future generations of robots used in the treatment of neurovascular diseases.
Cardio Flow announced it has received US Food and Drug Administration (FDA) 510(k) clearance for the company’s FreedomFlow orbital atherectomy peripheral platform. The company details in a press release that the FreedomFlow platform is designed with a modern mechanism of action to clear plaque blockages in the arteries of the legs.
Merit Medical Systems, a leading global manufacturer and marketer of healthcare technology, has announced the expansion of its Maestro microcatheter product line to now include a new longer length for radial embolization procedures.
Delcath Systems, an interventional oncology company focused on the treatment of primary and metastatic cancers of the liver, have announced the publication of an article entitled ‘Selective internal radiotherapy (SIRT) and chemosaturation percutaneous hepatic perfusion (CS-PHP) for metastasized uveal melanoma: A retrospective comparative study” in the peer-reviewed oncology journal Cancers.
Interventional News is delighted to welcome professor of interventional radiology Robert Morgan (St George’s Hospital NHS Foundation Trust, London, UK) as editor-in-chief. Morgan is currently a clinical director for diagnostics at St George’s, clinical lead for the South West London Integrated Care System (ICS), and chair of the Royal College of Radiologists Academic Committee.
Morgan has held several prestigious roles, which include but are not limited to his appointment as president of the Cardiovascular and Interventional Radiology Society of Europe (CIRSE) in 2018, and is now chair of the Endovascular Subcommittee of CIRSE. Of his active positions, Morgan is the current vice president of the British Society of Interventional Radiology (BSIR) and will become BSIR president in November 2023.
Of his contributions to academia, Morgan has previously acted as deputy editor-in-chief for the scientific journal CardioVascular and Interventional Radiology: Endovascular, and was instrumental in the creation of the European Board of Interventional Radiology (EBIR) examination which is now sat by interventional radiologists around the globe. Furthermore, Morgan has written 197 peer-reviewed articles, edited four books, authored 47 book chapters and delivered over 300 invited lectures.
His research and clinical interests focus on imaging and the endovascular treatment of aortic and peripheral vascular disease; and non-oncologic embolization including haemorrhage, visceral artery aneurysms and endoleaks.
Robert Morgan accepting his 2023 CIRSE Gold Medal
His distinguished service to his specialty has been recognised by several bodies—Morgan was awarded the Gold Medal of the BSIR in 2020 and, recently, the Gold Medal of CIRSE in 2023.
On joining as editor-in-chief of Interventional News alongside Professor Andy Adam (King’s College London, London, UK), and Professor Brian Stainken (Stamford, USA), Morgan writes:
“It is a great privilege and honour to join the senior editorial team in Interventional News. I have read this publication since its inception and look forward to its arrival in my inbox or through my letterbox every month.
Interventional News and its sister publications, including Vascular News, fulfil important roles for the interventional radiology landscape. They are able to present in a readable informal manner current hot topics in interventional radiology, and to summarise for readers key points and highlights from recent major interventional radiology congress programmes and speaker presentations at meetings. There are few better ways for interventional radiologists to learn about newsworthy items, from the literature and congresses, without actually reading the scientific papers or attending the meetings.
In my new role as co-editor-in-chief for Interventional News, I would like to continue the excellent work by Professors Andy Adam and Brian Stainken. I would like to assist in further improving the quality of the editorial content and in time to introduce new editorial concepts to ensure that Interventional News continues to be the ‘great read’ that it already is.”
Patients diagnosed with benign bone tumours will be relieved to know that these are not malignant, and some tumours will involute spontaneously. However, this natural history can be unpredictable, and tumours can be associated with significant pain, pathologic fracture, or potential for growth and compression of critical structures such as nerves.
Interventional approaches are increasingly being applied to this domain after multidisciplinary discussions. Two common indications that interventionists may encounter are:
Osteoid osteoma and osteoblastoma
Most often these lesions are treated due to pain. Single-session biopsy and thermal ablation has become a standard of care at many institutions. The majority of cases will be treated with general anaesthesia as instrumentation of the nidus can create significant involuntary patient movement due to pain. Utilisation patterns of radiofrequency (RF), microwave, and cryoablation, and other options such as laser ablation and high-intensity focused ultrasound will be dictated by operator preference and device availability, and local insurance coverage.
RF ablation has the benefit of a long track record in the literature and colloquial familiarity in the orthopaedic surgery and neurosurgery domains. Use of cooled RF systems may be helpful to prevent carbonisation in heavily sclerotic lesions. Cryoablation has emerged as a convenient alternative as it can provide a larger zone of ablation per probe chance to visualise the extraosseous extent of the ice ball and extrapolate the intraosseous treatment zone.
Aneurysmal bone cyst
Most often these lesions are treated due to impending pathologic fracture. Depending on the size and location of the lesion, multiple sessions and modalities may be applied to achieve osseous consolidation of the lesion. Intralesional sclerotherapy is a valuable option and can serve as a monomodal therapy, sometimes requiring multiple sessions. In cases where there is halted progression but slow osseous consolidation, augmentation with osteoconductive cements may be considered; compared to polymethylmethacrylate these biologic agents will allow natural bone ingrowth. Thermal ablation can be considered if loculations limit spread of sclerotherapy agent, with cryoablation serving a unique role as the ice-ball can be completely visualised and some of these lesions are in proximity to important nerves or open physes.
Embolization has a role in lesions that are particularly high risk for thermal ablation due to adjacent structures, have insufficient cortex to contain sclerotherapy agents, and are in surgically unfavourable locations (such as the pelvis). Embolization can be a monotherapy or enable other aforementioned therapies by allowing interval consolidation and remodelling of the cortex to contain injectable agents.
In summary, benign bone tumours serve as an opportunity to apply a broad range of interventional techniques to achieve pain relief and prevent skeletal events such as pathologic fracture.
Sirtex Medical, a leading manufacturer of interventional treatment solutions, has announced the commercial availability of the LAVA liquid embolic system, the first and only liquid embolic approved for the treatment of peripheral vascular haemorrhage.
LAVA provides volume and viscosity options that optimise the flexibility needed to treat patients with controlled target vessel occlusion. The product’s 2ml and 6ml options are optimised for the peripheral vasculature, and its viscosity options allow for the distal embolization of small vessels that may be inaccessible via other embolics.
“This product’s ability to maximize the packing density within the target vessel is incredibly important, as it allows us to minimise the likelihood of a future recurrence or restoration of vessel patency,” said Gary Siskin (Albany Medical Center, Albany, USA).
In a study of the LAVA liquid embolic system for the embolic treatment of arterial haemorrhage in peripheral vasculature, the product met both the primary safety and effectiveness endpoints, with 100% of patients experiencing no major adverse events in 30 days and 94% of lesions meeting clinical success in 30 days.
“The trial was an incredible success. Our goal was to achieve 70% efficacy for the existing data and outcomes, but we were able to achieve 94% efficacy,” said Bulent Arslan (Rush Medical College, Chicago, USA) . “I am overjoyed that it is now available for all of our patients.”
“The approval and availability of LAVA is especially meaningful to our team because it is addressing previously unmet needs in vascular medicine, with the potential to create significant impact on patients’ lives,” said Matt Schmidt, chief commercial officer of Sirtex. “We are delighted to expand our Sirtex product portfolio with this treatment milestone that directly furthers our mission to improve the quality and longevity of patient lives through innovative medical solutions, and we thank everyone who played a role to achieve it.”
The Duo venous stent system (Vesper Medical/Philips) showed a 98.7% freedom from major adverse events (MAEs) at 30 days and 90.2% primary patency at 12 months, results from the VIVID trial revealed.
The data—which covered 162 subjects with nonthrombotic, acute thrombotic or chronic post-thrombotic clinically significant venous outflow obstruction—were revealed during The VEINS 2023 (28–30 October, Las Vegas, USA) by Mahmood Razavi (St Joseph Heart & Vascular Center, Orange, USA), who highlighted how the trial provided “more clinical evidence in terms of durability and clinical improvement in these patients with venous outflow obstruction and venous stenting.”
The prospective, multicentre, single-arm, non-blinded clinical trial is designed to investigate the safety and efficacy of the Duo system as compared to pre-defined performance goals related to stenting of iliofemoral venous outflow obstructions.
The 98.7% freedom from MAE safety endpoint exceeded the peer-reviewed literature-driven performance goal of 89% with a highly significant p value, Razavi told The VEINS. The 12-month primary patency rate of 90.2% similarly exceeded its performance goal of 77%, he added.
“As expected, the best outcomes were in the non-thrombotic patients, followed by the acute thrombotic patients followed by the post-thrombotic patients,” Razavi explained.
He outlined significant sustained clinical improvement in term of CEAP (clinical, etiology, anatomy, pathophysiology) classification, Villalta score and venous clinical severity score (VCSS).
“The safety and efficacy of the stent system were established, and the endpoints were met,” Razavi concluded.
Endologix has announced results from a pooled analysis of the DETOUR1 and DETOUR2 studies evaluating percutaneous transmural arterial bypass (PTAB) with the Detour system.
A press release details that PTAB with the Detour system offers a novel approach to treating complex peripheral arterial disease (PAD), enabling physicians to bypass lesions in the superficial femoral artery (SFA), by using conduits routed through the femoral vein via a transmural passage, to restore blood flow to the leg. This approach is effective for patients with long lesions (20–46cm in length).
Data were aggregated from DETOUR1 and DETOUR2, both of which were prospective, single-arm, multicentre, international studies designed to evaluate the Detour system. Inclusion criteria and prespecified endpoints were similar. Both studies utilised imaging core lab and independent adverse event adjudication. Endpoints included freedom from major adverse events (MAEs) through 30 days, symptomatic deep vein thrombosis (DVT), and length of stay. For the pooled analysis, primary patency was defined as freedom from target vessel revascularisation (TVR).
The results from the 275 pooled patients were presented at VIVA 2023 (30 October–2 November, Las Vegas, USA) by one of the study’s principal investigators, Sean Lyden (Cleveland Clinic, Cleveland, USA).
The presented results included the following:
Primary patency, defined as freedom from TVR, was 79.1% at one year and 68.1% through two years
Freedom from MAEs through 30 days was 97.8%
Clinical success rate was 92.9%, 96%, and 95.3% at 30 days, one year and two years, respectively
Symptomatic DVT was 3.3% and pulmonary embolism (PE) rate was 0%, respectively through the two-year time point
Average length of hospital stay was 1.3 days.
Ninety-four percent of the patients had chronic total occlusions of the SFA, with a mean lesion length of 31.6cm
“These results not only demonstrate the clinical utility of this therapeutic strategy in managing long complex femoropopliteal lesions but also highlight that PTAB with the Detour system achieves similar results to open surgical prosthetic femoropopliteal bypass without the need for general anaesthesia, long length of stay, and high rate of complications. We eagerly await more comprehensive data from broader real-world settings to further corroborate these findings,” stated Lyden.
“We are pleased to present the combined results of the DETOUR1 and DETOUR2 studies. The data are congruent between the studies and strengthen our confidence in the transformative potential of the Detour system,” said Matt Thompson, president and CEO of Endologix. “The DETOUR system offers a compelling alternative for addressing long, complex femoropopliteal lesions. As we look ahead, we are eager to bring PTAB using the Detour system to patients with complex PAD.”
InspireMD recently presented 30-day results from the C-GUARDIANS US investigational device exemption (IDE) clinical trial evaluating its CGuard embolic prevention stent (EPS) system for stroke prevention at the annual Vascular Interventional Advances (VIVA) meeting (30 October–2 November 2023, Las Vegas, USA). The presentation, which was accepted as a late-breaking abstract, was delivered by Chris Metzger (OhioHealth, Columbus, USA), principal investigator of the C-GUARDIANS trial.
C-GUARDIANS is a pivotal trial designed to evaluate the safety and efficacy of the CGuard carotid stent system when used to treat symptomatic and asymptomatic carotid artery stenosis in patients undergoing carotid artery stenting (CAS) and at a high risk for carotid endarterectomy (CEA).
From July 2021 to June 2023, 316 patients were prospectively enrolled in this single-arm carotid artery stenting study, performed at 24 sites in the USA and Europe. The primary endpoint was a composite of either: incidence of major adverse events including death (all-cause mortality), any stroke or myocardial infarction (DSMI) through 30 days post-index procedure; or ipsilateral stroke from day 31 to day 365 post-procedure.
Stenting with the CGuard carotid stent system in patients with carotid artery stenosis and at high risk for CEA had a DSMI rate of 0.95%, from procedure through 30 days of follow-up, as per an InspireMD press release.
“The follow-up data from C-GUARDIANS once again support the safety of the CGuard EPS stent, with its novel MicroNet technology, as reflected in the low rate of major adverse events observed through 30 days,” said Marvin Slosman, chief executive officer of InspireMD. “We believe the neuroprotective qualities of CGuard set it apart from competing stents on the market and should help accelerate the ongoing shift in carotid revascularisations from ‘surgery-first’ to an endovascular ‘stent-first’ approach. We look forward to reporting 12-month results as we continue to advance CGuard EPS toward potential FDA [Food and Drug Administration] approval in the first half of 2025.”
InspireMD also anticipates reporting primary endpoint results from C-GUARDIANS—which may support a premarket approval (PMA) application—in the second half of 2024.
Contego Medical has announced the presentation of late-breaking clinical results from the PERFORMANCE II carotid stent trial at the annual Vascular Interventional Advances (VIVA) meeting (30 October–2 November 2023, Las Vegas, USA). PERFORMANCE II is a prospective, multicentre study evaluating the safety and effectiveness of the Neuroguard integrated embolic protection (IEP) system in 305 patients at 40 clinical sites.
“The one-year event rates in the PERFORMANCE II study are the lowest ever reported in any adequately powered, prospective, multicentre study of any type of carotid artery revascularisation, regardless of patient risk,” said William Gray (Main Line Health, Philadelphia, USA), co-national principal investigator of the PERFORMANCE II trial. “These results can elevate the standard of care for patients with severe carotid artery disease who are deemed appropriate for intervention by delivering demonstrated best-in-class stroke protection.”
In the PERFORMANCE II study, the reported 30-day stroke rate was 1.31% in the intention-to-treat analysis and 0.98% in a per-protocol analysis, with no major strokes or contralateral strokes, and all patients returning to baseline neurologically within 30 days, according to a Contego press release. At one-year follow-up (all stroke within 30 days, and ipsilateral stroke between day 31 and 12 months), the reported stroke rate was 1.68% in the intention-to-treat analysis and 1.35% in a per-protocol analysis. No major strokes or neurological deaths occurred in the study.
The release details that the Neuroguard IEP system leverages Contego’s clinically proven IEP technology—a unique platform with a micro-filter integrated on the delivery catheter, which is designed to deliver added safety during stent placement and balloon dilation. The micro-filter with 40µm pores captures the micro-emboli that other protection mechanisms do not, the release adds, giving physicians the procedural confidence that comes with advanced stroke protection in the treatment of their patients. The Neuroguard closed-cell stent also utilises FlexRing technology, providing optimised radial strength and flexibility while leveraging nitinol’s proven long-term material performance, Contego further claims.
“The recent change in coverage by the Centers for Medicare & Medicaid Services (CMS) increases patient access to carotid artery treatment,” said Contego chief executive officer Ravish Sachar. “We are committed to providing the most advanced and clinically proven technology to all patients and their physicians in the vascular community.”
In addition to the PERFORMANCE II study—in which Neuroguard was placed via transfemoral or transradial access—the PERFORMANCE III study is currently enrolling patients to evaluate the same stent placed via direct transcarotid access.
“Our mission is to provide a new class of products which improve patient outcomes and procedural efficiency,” said Stacy Enxing Seng, operating partner at Lightstone Ventures and chairman of the board at Contego. “The IEP platform, as demonstrated in the PALADIN, PERFORMANCE I and PERFORMANCE II studies, meaningfully advances stroke protection for patients. For physicians, it offers reduced catheter exchanges and improved efficiency with a three-in-one design, combining the Neuroguard stent, balloon and filter all in one device.”
Penumbra, a global healthcare company focused on innovative therapies, announced the latest STRIKE-PE data evaluating Penumbra’s Indigo aspiration system with Lightning. The results show Penumbra’s computer assisted vacuum thrombectomy (CAVT) is safe and effective at reducing right heart strain.
It also improved clinical outcomes, including heart rate and respiratory rate, and functional outcomes, including dyspnoea, walking distance and New York Heart Association (NYHA) classification, when used to treat acute high and intermediate risk pulmonary embolism (PE). The data were presented at this week’s Vascular Interventional Advances (VIVA; 30 Oct–1 Nov, Las Vegas, USA) conference.
“The latest STRIKE-PE data looking at the first 150 patients show that not only is Penumbra’s Indigo system safe and effective for removing thrombus, but also confirm that the removal of the clot can have a significant, positive physiologic impact on patients,” said James F Benenati, chief medical officer at Penumbra. “The latest STRIKE-PE data add to the growing body of evidence that demonstrates the significant benefits of CAVT, which is redefining the way physicians treat significant symptomatic pulmonary emboli.”
Penumbra’s CAVT is designed to allow physicians to remove large blood clots in the body safely, simply and with speed. The interim results of the prospective, multicentre study, which evaluated Penumbra’s Lightning technology in 150 of 600 anticipated patients to be enrolled, include:
Safety & Performance:
Low 48 hour major adverse event rate of 2.7%
Low 48 hour major bleeding rate of 2.7%
Significant reduction of right ventricle/left ventricle ratio by 25.7%
Functional Measures:
Significantly improved patient reported shortness of breath (dyspnoea) by discharge with increasing improvement by 90-days
Functional ability, measured by six-minute walk distance, significantly increased by 120 meters from discharge to 90-days
Patients returned to pre-PE state with no significant difference in NYHA classification from before the event to 90-days
“The complexity of treating pulmonary embolisms appropriately cannot be overstated. They are often complicated to diagnose and, in many cases, if not treated quickly, can be life-threatening,” said Ido Weinberg (Massachusetts General Hospital, Boston, USA) who presented the data. “While surviving a pulmonary embolism is a victory, patients regaining their quality of life and ability to function without ongoing limitation is critical. The STRIKE-PE data set is very encouraging as it confirms the promise of CAVT to restore blood flow quickly, safely and effectively while also showing promising, prompt and lasting improvement in patient outcomes.”
Additional STRIKE-PE data were previously presented at the recent TCT annual scientific meeting, showing improved quality-of-life outcomes, including improved mobility and ability to provide self-care and a decrease in pain/discomfort from discharge to 90-day follow-up.
“The real-world data from STRIKE-PE allow us, for the first time, to continuously evaluate the impact of intermediate and high-risk PE treated with CAVT,” said John Moriarty (University of California Los Angeles, Los Angeles, USA) principal investigator of the STRIKE-PE study and interventional radiologist. “The latest results continue to show improved functional outcomes and quality of life, suggesting that CAVT should be considered as a valuable frontline treatment option.”
In the USA, an estimated 900,000 cases of symptomatic PE occur annually. Incomplete physical recovery after PE has been documented as a common outcome as patients often report decreased quality of life and persistent shortness of breath. Pulmonary embolism can be life-threatening with 10–30 percent of individuals dying within one month of diagnosis.
“We believe that our CAVT technology will help transform care so PE patients can return home quickly with minimal impairments and minimal impact on their quality of life,” said Adam Elsesser, president and chief executive officer of Penumbra. “The latest STRIKE-PE data confirm that the safety, speed and simplicity of our devices can have a lasting impact on patients and our focus on clinical evidence will continue to advance the patient care paradigm.”
Penumbra is also conducting STORM-PE, a first-of-its kind randomised controlled trial comparing CAVT using Penumbra’s Lightning Flash with anticoagulation versus anticoagulation alone, with the goal of showing the clinical benefits to patients who receive CAVT.
LimFlow announced today that it has entered into a definitive agreement to be acquired by Inari Medical.
A press release details that, under the terms of the agreement, LimFlow will receive US$250 million in cash at closing and be eligible to receive up to US$165 million in additional payments based on certain commercial and reimbursement milestones, for a total potential transaction value of up to US$415 million. The transaction is expected to close in the fourth quarter of 2023.
LimFlow’s acquisition by Inari Medical is expected to increase patient access to its LimFlow system for transcatheter arterialisation of the deep veins (TADV), which is designed to re-establish blood flow in deep veins for “no-option” chronic limb-threatening ischaemia (CLTI) patients who have no other suitable endovascular or surgical treatment options and are facing major amputation.
US Food and Drug Administration (FDA) approval for the LimFlow system was received in September 2023 based on successful outcomes seen in the PROMISE II pivotal trial, recently published in the New England Journal of Medicine, and from positive clinical results seen in earlier studies. In the PROMISE II study, 76% of no-option CLTI patients were able to keep their leg and experienced progressive wound healing, with many having significant pain relief during the time following LimFlow treatment. LimFlow details that its system is the first and only FDA-approved device for TADV and previously received Breakthrough Device designation from the FDA.
“We are thrilled to join forces with Inari Medical, expanding the reach of our remarkable technology to bring renewed hope to patients who are currently suffering,” said LimFlow CEO Dan Rose. “Our heartfelt gratitude goes out to the exceptional LimFlow team, our dedicated clinical partners, and our investors who believed in our mission. Together, we eagerly anticipate advancing our shared vision of addressing crucial unmet needs in the realm of vascular disease.”
LimFlow investors include Sofinnova Partners (through its Crossover Strategy), Bpifrance, Balestier (an affiliate of M&L Healthcare Investments), Longitude Capital, Soleus Capital and Inari Medical. LimFlow was incubated by MD Start and co-founded by Martin Rothman and Tim Lenihan.
“The acquisition of LimFlow is closely aligned with our mission to address significant unmet patient needs and adds another highly differentiated growth platform into our portfolio,” said Drew Hykes, CEO of Inari. “We see the CLTI market as poised for durable growth, driven by compelling technology, outstanding clinical results, and multiple opportunities for expansion As a minority investor and board observer in LimFlow since early 2022, we have seen firsthand the life-changing impact this technology has on patients, as well as how complementary our two businesses are.”
Surmodics has announced the commercial launch of its most advanced hydrophilic medical device coating technology, the Preside hydrophilic coatings.
As per a company press release, Preside hydrophilic coatings complement Surmodics’ existing Serene hydrophilic coatings by providing customers with a unique, low-friction and low-particulate generation coating to further enhance distal access for neurovascular applications, as well as improve crossing for challenging coronary lesions or chronic total occlusions.
Preside hydrophilic coatings are “specifically formulated to meet the challenge of achieving the right balance of enhanced lubricity (reduction in friction) and excellent coating durability (resulting in low particulates) for the next generation of neurovascular, coronary and peripheral vascular devices”, the release adds.
Surmodics’ Preside hydrophilic coatings allow customers to leverage their existing coating processes, resulting in easy implementation in a manufacturing environment, according to the company.
“Hydrophilic coatings are an essential feature to help medical devices access and navigate tortuous vascular pathways, allowing physicians to reach distal treatment sites for improved therapeutic outcomes,” said Charlie Olson, Surmodics senior vice president and president of the company’s Medical Device Coatings business. “We are pleased to secure the first 510(k) device clearance that leverages this new technology. Our Preside hydrophilic coatings strengthen our existing portfolio and set a new performance standard for the industry, and the medical device manufacturers we serve.”
Endovascular Engineering (E2) has announced positive initial results from its ENGULF study, demonstrating successful outcomes among the first 15 patients evaluated in the trial using the Hēlo thrombectomy system for the treatment of acute sub-massive pulmonary embolism.
The ENGULF Study is a single-arm, multicentre, feasibility study evaluating the safety and performance of the Hēlo thrombectomy system, conducted under a US Food and Drug Administration (FDA) investigational device exemption (IDE).
An interim analysis of core lab adjudicated outcomes among the first 15 patients treated at seven sites demonstrated a significant reduction in right ventricular to left ventricular ratio (RV:LV), the FDA-recognised metric associated with increased morbidity and mortality. There were no major adverse events (MAE) reported for any of the patients through 30-day follow up.
The Hēlo Thrombectomy System is a next-generation technology that addresses clot removal in a single pass. Its dual-action technology simultaneously combines the power of aspiration with advanced mechanical clot disruption. The dual-action mechanism occurs within an atraumatic funnel tip, as the high-speed agitator actively engages and removes clot under controlled suction. Its low-profile design paired with this innovative approach facilitates the extraction of a wide range of clot morphology.
“The Hēlo Thrombectomy System has the potential to change how we perform thrombectomy by combining the power of aspiration with mechanical maceration to retrieve both fresh and organized thrombus,” said Eric Secemsky (Beth Israel Deaconess Medical Center, Boston, USA). “The low-profile catheter along with the funnel tip allows for the ability to navigate both simple and complex anatomies without sacrificing lumen size. As the first next-generation thrombectomy system to receive this level of clinical evaluation, I look forward to completion of the clinical study and presentation of the results.”
“The device has thus far been very safe with no instances of pulmonary artery injury or cardiac injury noted,” said the national principal investigator, Jay Giri (Hospital of the University of Pennsylvania, Philadelphia, USA). “It has been easy to deliver in a single pass to the pulmonary arteries given its low profile and has the ability to remove clot in a differentiated way.”
“We are very pleased with the initial clinical experience observed during the ENGULF feasibility study and the tangible progress in our mission to provide a differentiated clinical solution to patients and physicians,” said Mike Rosenthal, CEO of E2. “The Hēlo Thrombectomy System is performing as expected in this clinical study. We look forward to additional enrolment in the ENGULF study and the continuation into the pivotal trial phase.”
New research from the FLASH registry shines a light on the effectiveness of large-bore mechanical thrombectomy in managing high-risk pulmonary embolism. The study, titled “Mechanical thrombectomy for high-risk pulmonary embolism: Insights from the US cohort of the FLASH registry,” provides valuable insights into this life-saving procedure. The findings were released today in the Journal of the Society for Cardiovascular Angiography & Interventions (JSCAI).
Pulmonary embolism (PE) is a potentially life-threatening condition caused by the blockage of blood vessels in the lungs. High-risk PE, in particular, requires immediate medical intervention. The study shows that mechanical thrombectomy can significantly improve outcomes for patients with high-risk PE.
Mechanical thrombectomy is a minimally invasive procedure that uses specialised instruments to remove blood clots in the pulmonary arteries. Unlike traditional anticoagulant therapy alone, mechanical thrombectomy directly addresses the source of the blockage, improving outcomes for patients with PE.
The research analysed data from the prospective, multicentre FLASH registry, a comprehensive database that tracks the outcomes of real-world patients with PE undergoing mechanical thrombectomy using the FlowTriever system (Inari Medical). Here, acute outcomes through 30 days were evaluated for the subset of patients with high-risk PE as determined by the investigational sites. An independent medical monitor adjudicated adverse events (AEs), including major AEs (MAEs): device-related mortality, major bleeding, or intraprocedural device- or procedure-related AEs.
Of 799 patients in the U.S. cohort, 63 (7.9%) were diagnosed with high-risk PE. Among these 63 high-risk patients, 30 (47.6%) had systolic blood pressure <90 mmHg, 29 (46.0%) required vasopressors, and 4 (6.3%) experienced cardiac arrest. The mean age of patients with high-risk PE was 59.4±15.6 years, and 34 (54.0%) were women.
At baseline, 45 (72.6%) patients were tachycardic, 18 (54.5%) had elevated lactate ≥2.5 mM, and 21 (42.9%) patients had depressed cardiac index <2 L/min/m2. Immediately following mechanical thrombectomy, heart rate improved to 93.5±17.9 bpm and mean pulmonary artery pressure improved to 24.3±9.6 mmHg. Twenty-five (42.4%) patients did not require an overnight stay in the intensive care unit, and no mortalities or MAEs occurred through 48 hours. Moreover, no mortalities occurred in 61 (96.8%) patients followed through the 30-day visit.
The results demonstrate that the procedure is not only safe but also associated with a significant reduction in acute mortality among patients with high-risk PE, when viewed in context with the historically high mortality rates for this patient population.
James M Horowitz (New York University Grossman School of Medicine, New York, New York), lead author of the study, stated: “Our findings highlight the effectiveness of mechanical thrombectomy as a first-line treatment for high-risk pulmonary embolism. By removing blood clots from the lungs, this procedure can rapidly restore blood flow and prevent fatal complications.”
Researchers state that the study further contributes to the growing body of evidence supporting the use of mechanical thrombectomy in managing high-risk PE. The insights gained from the FLASH registry pave the way for further advancements in the field of interventional cardiology and treating patients who can be stabilised for catheterisation.
A recent publication in the journal Obstetrics & Gynaecology has reported an increase in the risk of hysterectomy after endometrial ablation from one to five years post-procedure.
The risk assessment was conducted by Tamara J Oderkerk (Maxima Medical Center, Eindhoven, The Netherlands) et al, who used the EMBASE, MEDLINE, ClincalTrials.gov and Cochrane databases to search for eligible articles from inception, to June 13, 2022 to present. To do so the investigators note that search terms included endometrial ablation and hysterectomy, and described the incidence of hysterectomy within a specific time after ablation with a minimum follow-up duration of 12 months.
Yielded from their search, the authors identified 3,022 articles, with a total of 53 studies that met their inclusion criteria. These articles consisted of six retrospective studies, 24 randomised controlled trials and 23 retrospective studies.
A total of 48,071 patients underwent endometrial ablation between 1992 and 2017, with a follow-up duration that varied between 12 and 120 months. Oderkerk et al’s analysis by follow-up found a 4.3% hysterectomy rate at 12 months (n=29 studies), 11.1% at 18 months (n=1 study), 8% at 24 months (n=11 studies), 10.2% at 36 months (n=12 studies), 7.6% at 48 months (n=2 studies), and 12.4% at 60 months (n=6 studies).
The authors state that two studies reported a mean hysterectomy rate at 10 years after ablation of 21.3%.
Concluding their review, Oderkerk and colleagues state that clinicians “can use the results of this review to counsel patients on the 12% risk of hysterectomy five years after endometrial ablation”. A statement which garnered response from Vance McCausland (George Washington University School of Medicine, Washington, USA) et al—author of the 2007 paper ‘Long-term complications of endometrial ablation’— who addressed the issue of postablation intrauterine scarring and contracture which can “obstruct persistent or regenerating endometrial tissue trapped behind the scar”.
McCausland and colleagues relay however that entering the uterus for diagnostic purposes after endometrial ablation in order to exclude carcinoma for example, “appears to be a useful diagnostic tool” within practice today. Furthermore, in their response, the authors supplement that further investigation will be required to “better understand long-term postablation problems”.
David Dexter (Sentara Vascular Specialists, Norfolk, USA) shared one-year data from the CLOUT registry this week at The VEINS 2023 (28–30 October, Las Vegas, USA).
Long-term, prospective outcome data after mechanical thrombectomy for deep vein thrombosis (DVT) are lacking. The CLOUT (ClotTriever Outcomes) registry is a prospective, multicentre study evaluating patient outcomes for proximal lower extremity DVT treated with the ClotTriever system (Inari Medical).
CLOUT is the largest mechanical thrombectomy study in the field of DVT, said Dexter, and although positive results have been previously published, this is the first report of one-year outcomes for all available patients. Patients in CLOUT were aged ≥18 years and enrolled regardless of bilateral disease, duration of symptoms, prior treatment failure for the current DVT event, or contraindications to thrombolytic therapy. A total of 310 patients completed the one-year follow-up visit.
One year after mechanical thrombectomy, moderate-to-severe post-thrombotic syndrome (PTS; Villalta score ≥10) was observed in 8.8% of treated limbs. The overall PTS rate (Villalta score ≥5) was 19.3%. Venous patency, as measured by the presence of flow with normal or partial compressibility on duplex ultrasound, was observed in 94.2% of cases. Additionally, significant improvements from baseline in revised Venous Clinical Severity Score, Numeric Pain Rating Scale score, and EQ-5D questionnaire score were demonstrated.
In the real-world, all-comer CLOUT registry, one-year outcomes demonstrate a low rate of PTS following treatment with the ClotTriever system, which was complemented by patient-centric improvements in symptom relief and quality of life. Study follow-up through two years is ongoing.
Dexter stated that these favourable clinical outcomes highlight the need for randomised controlled trial data comparing mechanical thrombectomy with standard of care anticoagulation treatment. The recently initiated randomised controlled DEFIANCE trial will compare the ClotTriever system to anticoagulation for the treatment of symptomatic iliofemoral DVT.
Muneeb Ahmed is an interventional radiologist specialising in interventional oncology (IO) at Beth Israel Deaconess Medical Centre (Boston, USA) and current president of the Society of Interventional Oncology (SIO). Speaking to Interventional News, Ahmed describes the nature of his appointment to date, his past clinical experiences which valuably inform his role, and what he hopes to achieve throughout his presidency.
IN: Please introduce yourself—what does your clinical practice look like?
I am currently the chief of interventional radiology (IR) at Beth Israel Deaconess Medical Center (BIDMC), professor of radiology at Harvard Medical School, and current president of SIO. Originally from Pakistan, I completed training in diagnostic radiology here at BIDMC, IR training at the Johns Hopkins Hospital, and have been a practicing attending IR physician at BIDMC since then. I lead a busy clinical IR practice, with 12 IR faculty and multiple residents every year at a large academic medical centre. My own clinical focus is on IO, including all forms of image-guided tumour ablation and transarterial therapies, and in the treatment of complex portal hypertension. In addition, I oversee a translational research laboratory where we study the effects of thermal ablation on tumour biology.
IN: Why did you want to become involved in the board of SIO? How did this come about?
The Society of Interventional Oncology annual scientific meeting (SIO; 25-29 January, 2024, Long Beach, USA)—formally known as the World Conference of Interventional Oncology (WCIO)—was developed more than 25 years ago out of a desire for the IO community to come together to discuss clinical practice, research and education. I originally became involved as a resident, presenting my research at WCIO and seeing leaders in the field who had similar interests in IO. As an attending interventional radiologist, I continued to volunteer—joining the annual meeting program committee, and ultimately, serving as program chair for the 2017 WCIO meeting.
As the WCIO progressed into the more formal SIO, I have continued to volunteer for larger roles, which has led to holding positions on the SIO board, such as treasurer, and now president. Throughout my 20+ years of involvement with the WCIO/SIO, the core values of the society—its commitment to advancing IO and how effective it has been in fostering research and education—have continued to impress me. My own positive experiences highlight the opportunity for all of us in the field to contribute and help advance IO, and the SIO has been a great place to do just that.
IN: You became president in January of this year—how has it been so far? What have you been working on?
Assuming the role of president of SIO is both very exciting and daunting at the same time. I have the privilege of continuing the work of many prior successful and well-known previous presidents, most recently Matt Callstrom (Mayo Clinic College of Medicine, Rochester, USA), our immediate past-president. It has been a very busy year already, as the SIO is working on many fronts to meet the needs of IO.
First up, we launched the SIO’s first clinical trial—the ‘Ablation with confimation of colorectal liver metastases’ (ACCLAIM) trial, which is a prospective international multicentre trial designed to demonstrate the importance of intraprocedural ablation margin confirmation. We just announced a new call for grant proposals in Y90 radioembolization and immunotherapy, sponsored by AstraZeneca. At the same time, we continue to build on our exciting IO master class educational programs, having successfully held our Y90 radioembolization master class in June, and another in-person musculoskeletal IO master class in the fall. On top of this, we are working on engaging with more members of the IO community by partnering with IR societies in Asia and Latin America. The SIO team and our group of volunteer physicians has been very active and I have been busy keeping track and making sure we are progressing on all of these fronts.
IN: Do you feel like there are aspects of your clinical practice that complement your position as president? How has your career as an IR thus far set you up for taking on this responsibility?
Definitely. Clinically, I have always had a strong focus on IO, including the introduction of new treatments at my institution, building a robust practice through tumour board participation, and developing novel multidisciplinary clinics at a large academic institution. In fact, our multidisciplinary liver tumour clinic is one of the most well-rounded and busiest growing practices within our own cancer centre. At the same time, we have an active IR training program, teaching residents how to practice evidence-based, comprehensive clinical IR.
Finally, I have always had a strong interest in translational research, leading a basic science and transitional animal lab with a focus on studying interventional oncology related tumour biology, and now strategies to augment IO induced immunotherapy. All of these experiences have provided me with a comprehensive perspective on the opportunities within the IO specialty, and what the day-to-day challenges are that practicing interventional oncologists face. This has really influenced my thoughts on where the society can help serve its membership and its broader patient and physician constituencies. My own experiences in working in every day with medical, radiation, and surgical oncologists to accommodate different perspectives and offer the best clinical care for each patient has also taught me the value of successful collaboration, which I bring to my work as SIO president in continuing to build out our own partnerships and relationships with many different collaborating organisations and individuals.
IN: What are your goals for the rest of your presidency?
It is an exciting time to be in IO and leading the SIO in particular. My overall goal is to leave the SIO better off at the end of my presidency than when I started. To this end, I want to continue to grow SIO as the strongest voice for the IO community, meeting the needs of physicians and our patients by advancing innovative research, providing the best possible educational programs and training, and advocating for IO inclusion in clinical practice guidelines. Ultimately, I would like to see the SIO build an even bigger tent, so that anyone doing IO will see the SIO as their home and community, just as I have all these years.
Data from the REAL-PE study were presented this week atTCT 2023 (23–26 October, San Francisco, USA)demonstrating that patients treated for pulmonary embolism (PE) with the Ekos endovascular system (Boston Scientific) had lower rates of adverse events, including statistically significant lower rates of major bleeding, within seven days following their procedure compared to the FlowTriever system (Inari Medical).
According to Boston Scientific, the analysis is the largest comparative study to use near real-time health system-based electronic health record (EHR) data to understand clinical practices and outcomes related to PE.
A press release details that, while treatment for PE has historically included anticoagulant medication, the use of new interventional therapies—such as the EKOS system—is increasing. The EKOS system uses a combination of ultrasound energy and a low thrombolytic drug dose to restore blood flow in patients with PE and other occlusions in the peripheral vasculature.
The REAL-PE study reviewed data from Truveta, a data and analytics company that provides EHR data from more than 30 US health systems and 100 million patients, including lab values, comorbidities, images, demographics and clinical outcomes, as well information about the performance of specific medical devices. In the REAL-PE analysis, 2,259 patients who experienced PE and received interventional treatment with either the EKOS system or the FlowTriever system between 2009 and 2023 were identified, and safety events associated with both devices were compared.
“In the past decade, there have been a number of advances in interventional therapies for the treatment of PE, but gaps in clinical evidence still exist when it comes to determining the optimal modality for each patient’s unique needs,” said Peter Monteleone, an interventional cardiologist with Ascension (Austin, USA) and principal investigator of the REAL-PE study. “The REAL-PE study provides comprehensive data and unprecedented insight into the real-world performance of specific interventional devices, which can help physicians make more informed clinical decisions.”
Major bleeding events in the REAL-PE study were based on definitions derived from established clinical criteria and guidelines, with statistically significant lower rates within seven days of the procedure consistently found in the cohort of patients treated with the EKOS system:
A rate of 12.4% for patients treated with the EKOS system vs. 17.3% for those treated with the FlowTriever system (p=0.0018), using the International Society on Thrombosis and Haemostasis (ISTH) definition, and;
A rate of 11.8% for patients treated with the EKOS system vs. 15.4% for those treated with the FlowTriever system (p=0.0190), using the Bleeding Academic Research Consortium type 3b (BARC3b) definition.
Medical coding data in the analysis also demonstrated that intracerebral haemorrhage within seven days following the procedure occurred statistically significant less frequently among patients treated with the EKOS system (0.3% vs. 1.3%, p=0.005). All other studied safety events also trended in favour of the EKOS system, including in-hospital mortality (2.6% vs. 3.7%) and all-cause 30-day readmission rates (5.1% vs. 5.4%). Median lengths of hospital stay were comparable at 3.6 days for both groups.
“Electronic health record data of this scale provides in-depth information about larger, more diverse patient populations, while also accounting for multiple variables including complex medical histories or comorbidities that often exclude patients from clinical trials,” said Michael R Jaff, chief medical officer and vice president, clinical affairs, technology and innovation, peripheral interventions, Boston Scientific. “While data from clinical trials and registries will always play an important role in healthcare, access to the breadth of data such as that used in the REAL-PE study has the potential to better inform and accelerate clinical decision-making and, ultimately, improve patient care.”
To date, Boston Scientific shares, the EKOS system has been used to treat more than 100,000 patients with PE globally, and the next-generation Ekos+ endovascular system received US Food and Drug Administration 510(k) clearance in 2022.
Philippe Pereira (SLK-Clinics GmbH, Heilbronn, Germany) pairing OPTIQ with personalised, multidisciplinary oncological medicine, “we have a big and bright future”.
Bernhard Gebauer (Charité University Hospital, Berlin, Germany) expands on the “excellent effect” of the new ARTIS icono technology when performing prostate artery embolization (PAE) and uterine artery embolization (UAE).
Maximilian de Bucourt (Charité University Hospital, Berlin, Germany), dives into
why OPTIQ radiation exposure control provides “huge step forward” in CO2 angiography.
Bernhard Meyer (Hanover Medical School, Hannover, Germany) shares
his team’s “amazing” experience after transitioning to Structure Scout and expands on its “essential benefits” during material-specific imaging.
Thomas Werncke (Hanover Medical School, Hanover, Germany) speaks to about his research into imaging quality, radiation dose reduction and material-specific imaging variables when using Siemens Heathineers’ OPTIQ and Structure Scout technology.
This advertorial, sponsored by BD, is intended only for readers outside the USA.
Left to right: Houman Jalaie (Aachen, Germany), Michael Lichtenberg (Arnsberg, Germany), Suat Doganci (Ankara, Turkey), Alejandro Rodriguez-Morata (Malaga, Spain), Almamoon Justaniah (Riyadh, Saudi Arabia) and Domenico Baccellieri (Milan, Italy)
“A dedicated, holistic venous approach is mandatory—including deep, superficial and pelvic venous systems,” says Houman Jalaie (University Hospital RWTH Aachen, Aachen, Germany), outlining what he believes was the key message emanating from a thoroughly successful BD Venous Summit (19–21 June 2023, Riga, Latvia).
The summit—for which Jalaie was co-director alongside Lowell Kabnick (Morristown Medical Center, Morristown, USA)—saw venous experts gather from far and wide to discuss a range of topics; perhaps most notably, the criticality of adopting multidisciplinary approaches, and engaging all relevant centres and specialties, to ultimately improve patient outcomes.
“There is a need for a couple of high-volume venous centres in each bigger country,” Jalaie continues, digging deeper into how these multidisciplinary, collaborative strategies can be implemented in a ‘real-world’ sense. “In order to offer the best possible diagnosis, indication and treatment, there is a clear need for running a multidisciplinary approach well.
“This does not mean that all departments should perform the interventions. For example, if one discipline has decided to go for dedicated venous care—taking the lead of the venous centre—there should be a cooperation with other medical departments for the best possible diagnostics, the best possible labour and also the best possible postoperative support. This also means the best anticoagulation approach.
“In order to achieve this aim, other specialities should be included regularly in decision making; of course, under the [guidance] of the main leading discipline. They should also be invited to venous congresses even if they are not directly treating these patients. A cooperation in research and science would be very helpful in order to create a team feeling as well.”
Providing her take-home messages from the summit, Wassila Taha (Alfa Scan Imaging Center, Cairo, Egypt)—another of the venous experts in attendance—states that, “depending on the specific venous condition, various treatment options should be offered to our patients”.
“These may include medications, minimally invasive procedures like sclerotherapy or endovenous ablation, or surgical interventions in more severe cases,” she adds. “The appropriate treatment will depend on the individual patient and the severity of the condition—and a well-detailed diagnostic workup with ultrasound and cross imaging.”
Making venous care holistic
Many of these messages were reflected throughout the Venous Summit—for example, in a presentation from Domenico Baccellieri (Vita-Salute San Raffaele University, Milan, Italy), who discussed his experiences of building a successful, dedicated venous centre. In addition to echoing Jalaie’s sentiment that a multidisciplinary approach is “mandatory” in this process, Baccellieri highlighted in-hospital and extra-hospital promotional activities, as well as research programmes, as “key” tools.
He went on to note the importance of establishing physician referral networks and ‘human contact’ with general practitioners (GPs), informing the Venous Summit audience that these—along with patient engagement and education—these considerations pose a challenge to the formation of specialised venous care in Italy. Jalaie agreed with Baccellieri on this point, commenting that “the same problem” is present in Germany as well.
Houman Jalaie
Discussions in Riga also saw Taha outline the successes of an initiative at her own hospital in which less specialised practices like wound dressing and compression therapy for venous leg ulcers were performed by ‘non-experts’, ultimately resulting in positive patient outcomes. Based on this, Taha asserted the importance of involving medical staff of all levels in venous care strategies.
Manjit Gohel (Addenbrooke’s Hospital, Cambridge, UK) later supported these key points raised by Taha, not only emphasising the vital role of compression therapy, stating that “we must not forget the basics”, but also of effective communication between primary and secondary centres so that patients can be transferred from everyday hospitals to specialised institutions. He concluded that “we have to form partnerships”.
Elsewhere on the programme, Suat Doganci (Health Sciences University, Ankara, Turkey) corroborated many of his colleagues’ views, highlighting public awareness programmes as useful mechanisms for improving venous care—giving social media as an example of a place where these programmes and campaigns can be hosted, and shared more widely.
This led Jalaie and Efthymios Avgerinos (Athens Medical Group, Athens, Greece) to agree on the utility of social media for spreading awareness and transmitting patient education, although Avgerinos also noted this is likely best done “in moderation” while Jalaie advised caution, owing to the fact that “misinformation can spread quickly”.
Future directions
Reflecting on the three-day summit, Taha highlights the need to calculate a ‘good’ inflow; prior iliac venous reconstruction; and assuming a good inflow threshold flow volume to maintain long-term venous stent patency, as important considerations in venous care. And, speculating on the future needs of the specialty, she notes that a trial involving genetic therapy as a means for mitigating the progression of venous disease is also to offer promise.
“Increasing patient compliance of wearing compression garments, and improving the manufacturing of these garments to adapt to countries with hot weather,” Taha avers, returning to the topic of compression therapy, and the unmet needs that must be tackled in this space.
Once again homing in on the concept of multidisciplinary venous care—and providing a brief glimpse of the direction the specialty should take moving forward—Jalaie states that, following an “extensive basic vascular education” as a vascular and endovascular surgeon, interventional radiologist or angiologist, “one should make a deep dive into the venous field and go for a holistic, dedicated approach to care”.
“This includes diagnostics, indication-making, treatment, postoperative evaluation and support,” he adds. “And, all this should be supported by an interdisciplinary team—haematology, gynaecology, internal medicine and radiology. These big venous centres should also focus on clinical and basic research in order to achieve more evidence.; with more evidence, better governmental support with [improved] reimbursement will be achieved, which will further boost the rising field of vascular medicine.”
Thrombolex has announced never-before-reported major reductions in obstruction in all of the segmental pulmonary arteries (PA), based on independent core lab data analysis of 107 patients from 18 sites in the USA, with acute intermediate-risk pulmonary embolism (PE), using the Bashir endovascular catheter and small doses of tissue plasminogen activator (tPA).
The National Institutes of Health (NIH)-sponsored RESCUE trial also showed unsurpassed efficacy and safety in this patient population compared to recently published studies with other US Food and Drug Administration (FDA)-cleared devices, Thrombolex reports in a press release. These new data have just been published in the Journal of the American College of Cardiology (JACC): Advances online.
The RESCUE trial demonstrated that pharmacomechanical catheter-directed thrombolysis (PM-CDT) therapy using the Bashir endovascular catheter to administer recombinant tPA (r-tPA) in small doses (7mg for unilateral and 14mg for bilateral PE over five hours) resulted in a 71.1% (40.5% to 11.7%; p<0.0001) reduction in the number of segmental PA branches with total or subtotal occlusions at 48 hours, using contrast-enhanced chest computed tomography angiography. Proximal PA branch total or subtotal occlusions decreased by 61.3% (28.7% to 11.0%; p<0.0001). The reduction in segmental artery occlusions correlated significantly with the reduction in right ventricular/left ventricular (RV/LV) ratio (P=0.0026) whereas that in the proximal PA did not (p=0.173).
Gregory Piazza, associate professor of medicine, Harvard Medical School (Boston, USA) and chairman of the RESCUE Data Safety Monitoring Board noted: “A growing body of literature supports the hypothesis that reperfusion of the distal pulmonary vasculature is a critical therapeutic target, influencing right ventricular recovery, symptom relief, and gas exchange.”
“The critical finding in the present study is that by using the Bashir endovascular catheter and small doses of tPA we are able to markedly reduce segmental and main pulmonary arterial occlusions. Assessment of segmental artery patency after catheter-based therapies of acute PE may be critical to understanding the long-term benefits of these therapies and should be part of all future clinical trials in acute PE,” said Brian G Firth, chief scientific officer, Thrombolex.
L-r: Ramon L Varcoe, Brian G DeRubertis and Sahil A Parikh
Results of the LIFE-BTK randomised controlled trial have just been presented at TCT 2023 (23–26 October, San Francisco, USA). The data show that, in patients with chronic limb-threatening ischaemia (CLTI) due to infrapopliteal artery disease, an everolimus-eluting resorbable scaffold was superior to angioplasty at one year with respect to the primary efficacy endpoint.
Ramon L Varcoe (Prince of Wales Hospital and University of New South Wales, Randwick, Australia) shared this and other key findings at TCT on behalf of co-principal investigators Brian G DeRubertis (New York Presbyterian–Weill Cornell Medical Center, New York, USA) and Sahil A Parikh (Columbia University Irving Medical Center, New York, USA). The trial results were simultaneously published in the New England Journal of Medicine (NEJM).
Parikh shares his thoughts on the significance of these results with this newspaper: “This trial is the first of its kind to demonstrate superiority of a technology for below-the-knee [BTK] intervention along a relatively long time point for this patient population.” He describes the effects of the technology as durable and notes they are “continuing to diverge” at the 12-month time point. “It is a highly clinically significant result”.
Peter Schneider (University of California San Francisco, San Francisco, USA) provides some context, noting that LIFE-BTK follows multiple failed trials in the BTK segment. “The key thing I think is that we do not have the tools we need to treat BTK disease. Yes, catheter-based treatments for limb salvage are quite good, they performed well in both the BEST-CLI and BASIL-2 trials, but it is still somewhat limited in terms of the number of options we have,” he says. “We have had a number of failed trials below the knee—three failed [drug-coated balloon] trials and one failed drug-eluting stent trial—and the fact that we now have a successful trial is really I would say wind in the sails of this whole effort to try to improve the tools and the approaches that we have for BTK disease.”
In this multicentre, randomised controlled trial, 261 patients with CLTI and infrapopliteal artery disease were randomly assigned in a 2:1 ratio to receive an everolimus-eluting resorbable scaffold (Esprit BTK; Abbott Vascular) or angioplasty.
The primary efficacy endpoint was freedom from amputation above the ankle of the target limb, occlusion of the target vessel, clinically driven revascularisation of the target lesion, and binary restenosis of the target lesion at one year. The primary safety endpoint was freedom from major adverse limb events at six months and perioperative death.
The authors report in NEJM that the primary efficacy endpoint was observed—by which they mean no events occurred—in 135 of 173 patients in the scaffold group and 48 of 88 patients in the angioplasty group (Kaplan–Meier estimate, 74% vs. 44%; absolute difference, 30 percentage points; 95% confidence interval [CI], 15 to 46; p<0.001 for superiority). This is “a highly statistically significant result,” Parikh remarks in conversation with this newspaper.
Parikhadds that the primary safety endpoint was “statistically indistinguishable between the two groups”. Writing in NEJM, the investigators elaborate that this endpoint was observed in 165 of 170 patients in the scaffold group and 90 of 90 patients in the angioplasty group (absolute difference, -3 percentage points; 95% CI, -6 to 0).
Finally, the investigators relay in their NEJM report that serious adverse events related to the index procedure occurred in 2% of the patients in the scaffold group and 3% of those in the angioplasty group.
Lessons learned
Parikh, an interventional cardiologist, notes that resorbable scaffold technology has “significantly improved” since the early iterations used in the coronary arteries. He expresses his hope for use of this technology in the peripheral vessels: “I would like to make clear that this is a new iteration of this technology,” he says. “The scaffold thickness is substantially less, it is in fact comparable to the contemporary drug-eluting coronary stents that we now use, with a thickness of less than 100 microns.”
Parikh adds that the lesion lengths that can be treated now are much longer. “In fact, in this trial, the lesions that were treated were up to 17cm, with overlapping scaffolds,” he shares.
According to Parikh, the success of current resorbable scaffold technology is a testament to lessons learned from past versions. “It is a similar technology to predecessors, but has benefitted from the experience that we have learned from other trials, and what we have learned is that fastidious implantation technique, adequate sizing, and appropriate pharmacotherapy are really the mainstays of treatment, and they are probably critically important to all vascular interventions, but specifically using a drug-eluting resorbable scaffold.”
He urges caution when comparing use of resorbable scaffolds in different vessels, although notes that “in this specific instance, the technology has proven itself to be superior in a randomised controlled clinical trial”.
Based on the positive findings from LIFE-KTK, Parikh is hopeful for the future of treatment in patients with CLTI due to infrainguinal disease: “We are extremely excited about the prospect of this technology being part of our armamentarium.”
On whether the results will change practice, Schneider opines that “this is a tool that all of us are going to want to have on our shelf”. However, he advises that interventionalists “keep in mind that a randomised controlled trial […] is not the same as an everyday algorithm of when to use and in which patients and in which situation”. The next step, according to Schneider, should be to develop that algorithm.
Questions remain, he says, including ‘is this something we are going to be using every day, or something we are going to be using once in a while in specific situations?’ and “that is the part that I think we need to go forward and figure out”.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark) saw presenters explore where thyroid thermal ablation treatments sit within practice today and how guideline recommendations worldwide have shifted to encompass the treatment option for patients today.
Consistent “near-zero” complication rates with thermal ablation techniques
Teresa Dionisio (Centro Hospitalar Vila Nova de Gaia/Espinho, Vila Nova de Gaia, Portugal) began her presentation by setting out contemporary techniques for thyroid thermal ablation, expositing radiofrequency, microwave and laser ablation as the three “most applied” methods used today. After brief description of each technique, Dionisio poses her central question: “What do we know about these different techniques?”
In past guidelines such as the American Association of Clinical Endochronologists’ (AACE) Dionisio explains, microwave ablation has often been placed as a secondary treatment option due to the “higher risks of minor and major complications”. “At that time we only had access to 40–60 gauge needles, so it was like killing a fly with a canon—it worked but caused a lot of collateral damage”.
Recent guidelines however have stated that laser, radiofrequency and microwave are “similarly safe and effective”, Dionisio said, broadening treatment options for patients dependant on “individual competencies and the research of the hospital”. Adding to this, she shares that overall complication rates for these ablation techniques are less than 4%, major complications less than 1% and there have been no life threatening complications reported to date.
Concluding Dionisio stated: “Thyroid ablation is a very safe procedure, if you plan for these events and understand the neck anatomy well, you can keep the complication rate near to zero”.
“Optimum” characteristics presented for successful thermal ablation of benign lesions
“Patient selection is of central importance,” Bulent Cekic (Antalya Education and Research Hospital, Antalya, Turkey) underlined, placing this among his key messages when describing the current indications and contraindications for thermal ablation of benign thyroid lesions during his presentation at CIRSE 2023.
“We do not ablate every nodule” when considering the best candidates for thermal ablation Cekic explained, nodule features such as spongiform echostructure, nodules with a liquid component, and soft nodules, are all elements that crucially increase volume reduction rate (VRR).
Continuing, Cekic conveyed his approach to treating toxic adenomas below 10ml in volume, noting the primary factor which affects the success of thermal ablation in these cases is the volume of the adenoma before treatment. Supporting this, Cekic references a study conducted by Roberto Cesareo (Santa Maria Goretti Hospital, Latina, Italy) et al, who divided their toxic adenoma group into two—those with a volume of more than 12ml and less than 12ml. Their results showed that, in the smaller volume group, euthyroidism via thermal ablation was achieved in 86% of patients, compared to 45% in the large volume group.
Supported by this research, Cekic’s clinic have found a “solution” that informs “ongoing clinical training” which stipulates, for adenomas below 10ml, thermal ablation is performed initially, followed by an injection of 4–5 cubic centimetres (cc) of 90% ethanol. By using this technique Cekic tells the audience, they “always have a 95% VRR” with a recurrence rate of adenomas of 1–2%.
Cekic adds that “careful anatomical assessment should always be performed before the procedure”, reiterating that clinicians must understand and apply their “[knowledge of] managing potential complications following the procedure” to have the best results.
Thermal ablation for malignant thyroid lesions has “come of age” worldwide
Closing out the session, Myrsini Gkeli (Agios Savvas General Anticancer Oncological Hospital, Athens, Greece) describes how “thermal ablation for malignant thyroid lesions as come of age around the world”, however “optimal” ablation techniques and “proper indications” remain as “challenges” for the future.
First, Gkeli cast an eye over global radiofrequency ablation (RFA) guidelines for the treatment of recurrent thyroid cancers in years past. Reaching 2022, he outlined an international multidisciplinary consensus statement which recommended RFA for the treatment of both benign and malignant thyroid disease.
Displaying a range of meta-analyses and long-term studies which have investigated the safety and effectiveness of RFA for these patients, the speaker relayed how these data demonstrate “significant tumour volume reduction” at six months, seven and nine years follow-up, respectively.
“The use of thermal ablation may be considered as an alternative option to active surveillance in incidentally discovered low-risk papillary thyroid microcarcinoma patients who are not eligible for surgery,” Gkeli told CIRSE delegates.
The analysis led investigators to conclude that there is no association between mortality risk and paclitaxel-coated device exposure or dose, and should provide reassurance to patients, physicians and regulators on the safety of paclitaxel-coated devices, they say.
The release of the data, which has also been published today in The Lancet, draws a line in the sand over the question of the safety of paclitaxel, which is used in peripheral interventions to prevent restenosis, after data from a summary-level meta-analysis put forward in 2018 pointed to an increased risk of death at two and five years following the use of paclitaxel-coated devices in the femoropopliteal artery.
William A Gray (Lankenau Heart Institute, Wynnewood, USA) told TCT attendees that the analysis provides the most complete and current follow-up data of pivotal studies associated with FDA-approved paclitaxel-coated devices and represents the most complete patient-level analysis to date, or likely to be available in the future.
Gray presented the findings on behalf of an independent physician steering committee, comprising Sahil Parikh (Columbia University Irving Medical Center, New York, USA), Peter Schneider (University of California San Francisco, San Francisco, USA), Christopher Mullin and Tyson Rogers (both North American Science Associates [NAMSA], Minneapolis, USA), who were enlisted by the regulator and industry to dig into the final and updated patient-level datasets and address limitations of prior paclitaxel meta-analyses. Funding for the study came from BD, Boston Scientific, Cook, Medtronic, Philips, Surmodics and TriReme Medical, though the funders of the study had no role in its design, data analysis, data interpretation, or writing of the report, but did provide patient-level data for the analysis, which was independently conducted.
The use of paclitaxel-coated devices for the treatment of PAD dropped by as much as 50% due to changes in practice patterns worldwide, Gray said, which was in response to the FDA’s 2019 statement that use of paclitaxel-coated balloons and paclitaxel-eluting stents was “potentially associated with increased mortality”. This change in position came after a meta-analysis from Konstantinos Katsanos (University of Patras, Patras, Greece) et al had first raised the spectre of a mortality risk. FDA removed the red flag in July this year, stating that “additional data from the pivotal randomised controlled trials (RCTs) ha[ve] become available” in a letter to healthcare providers in which it set out the decision.
Gray presents the findings at TCT 2023
To inform this decision, Gray and his co-investigators analysed randomised trials that evaluated FDA-approved paclitaxel-coated devices versus uncoated devices for the treatment of femoropopliteal artery disease, looking primarily at the mortality risk on an intention-to-treat basis, with key secondary analyses including dose/mortality and covariate interactions.
Data from 10 trials were included, encompassing 2,666 participants over a median follow-up of 4.9 years. One-year follow-up was available in 98.7% of evaluable participants and five-year follow-up in 95%, which Gray noted represents an additional 3,355.5 patient years since a 2020 analysis by VIVA Physicians, in which investigators identified an absolute 4.6% increased mortality risk associated with paclitaxel-coated devices, albeit demonstrating a weaker mortality signal than was initially reported in December 2018 by Katsanos et al.
Results of the latest analysis presented by Gray and published in The Lancet demonstrated an overall hazard ratio (HR) for the intention to treat populationof 1.14 (95% confidence interval [CI] 0.93–1.40). In post-hoc analyses assessing the proportional hazards assumption, there was no evidence the assumption was violated. HRs for individual studies ranged from 0.32 to 1.52, and there were no studies in which the CI did not include the null value of 1. The HR for the as-treated analysis was 1.13 (0.92–1.39). Furthermore, the as-treated crossover analyses also did not show a significant difference in deaths between the paclitaxel-coated and control groups, with an HR of 1.07 (0.87–1.31) when late crossovers were censored, and 1.04 (0.84–1.28) in the time-varying analysis of late crossovers. Examination of late crossover using iterative parameter estimations also failed to detect a significant effect on deaths.
In their report of the findings in The Lancet, investigators describe their dataset as “very likely to be the most complete and thoroughly vetted dataset to emerge regarding paclitaxel-coated devices and death, given the likelihood that randomised trials against control devices will no longer have clinical equipoise for effectiveness, and the substantial coordination efforts for data collection, analysis and multilateral consensus will be difficult to recapitulate”.
They also praise the collaborative and thorough efforts of many clinicians, industry sponsors, and regulators over several years that enabled this research.
“The most important takeaways are that: number one, we [have] learned a tremendous amount about how future studies should be planned, so that we do not go down a blind alley again to be fooled by a summary level meta-analysis,” Schneider tells this newspaper, reflecting on the takeaways from the research.
“The second thing is that this was a tremendous effort to resolve this problem, and that included collaboration like we have never had before between physicians of different specialties in different parts of the world, with industry and with regulatory bodies all over the geography, but especially with FDA, [which] has been extremely collaborative and has been all about problem solving since the beginning of this issue.”
“Here we have probably the most complete dataset that will be feasible from the randomised controlled trials,” comments Parikh. “We looked at the overall percentage of patients identified with vital status at five years, and it was 95% of the total cohort of almost 2,700 patients. I think it will be hard to find a more complete dataset at this level of detail.”
More importantly, adds Parikh, was the opportunity to conduct crossovers analyses.
“We are identifying exposure to paclitaxel in any way, to the maximum extent possible, and, with each subsequent iteration of the analysis, our findings showed a closer and closer point estimate to no hazard at all, to unity,” he says. “That really emphasises that going the extra mile to identify every exposure to paclitaxel, in this case most often with a contralateral limb intervention or reintervention, was the appropriate approach to adjudicate paclitaxel exposure and its risk.”
ABK Biomedical, a medical device company dedicated to the research, development, and commercialisation of advanced imageable embolic medical devices, has announced the first patient treated in its Route90 US investigation device exemption (IDE) pivotal study. The Eye90 microspheres radioembolization procedure was performed by Eric A Wang (Charlotte Radiology, Charlotte, USA).
“This is an exciting time for multidisciplinary, liver cancer treatment teams.” said Wang. “Hepatocellular cancer (HCC) is a severe form of cancer. Over the past 40 years, liver cancer incidence rates have more than tripled, and death rates have more than doubled during that time period. Eye90 radioembolization represents an advancement in liver-directed HCC therapy. Eye90 microspheres with multimodality imaging, controlled visible administration, and personalised dosimetry is advancing the field of radioembolization. We are excited to be a part of this pivotal study and look forward to establishing the effectiveness and safety of this new Y90 radioembolization technology.”
The Route90 pivotal clinical study is designed to evaluate the safety and efficacy of Eye90 microspheres in patients living with unresectable HCC. The study will evaluate HCC tumours’ response rates and duration of response from Eye90 microspheres treatment as co-primary endpoints. Eye90 microspheres is the first and only in-procedure imageable Y90 microspheres device. The study also includes endpoints to evaluate safety, the potential benefits of intra-procedural visualisation, and the ability to perform post-treatment computed tomography dosimetry with imageable microspheres, the press release outlines.
“While Y90 radioembolization is established as a safe and effective therapy for the treatment of HCC, rigorous prospective clinical studies are needed to establish credible data to support US Food and Drug Administration (FDA) premarket approval,” said David Dobrowski, vice president of clinical and regulatory affairs, ABK Biomedical. “The Route90 study will collect the high-quality data long needed with Y90 radioembolization therapy establishing a new standard of treatment. We are enthusiastic to treat our first patient and continue to work diligently with the top Y90 treatment centres in the USA and all of our highly motivated investigators on enrolling patients to complete the study”.
Andrew Kennedy (Sarah Cannon Cancer Institute, London, UK) is principal investigator for the Route90 study and one of the early pioneers of Y90 radioembolization research and treatment. “The Route90 pivotal study will not only confirm the effectiveness of Eye90 treatment but will also establish the importance of three-dimensional (3D) radiation dosimetry in advancing therapy and patient outcomes.
This is a significant milestone for all those involved at ABK, the clinical research team at Charlotte Radiology, and the multiple other sites that are about to begin patient enrolment. We look forward to rigorously and efficiently completing this important trial to offer the HCC community a long-overdue, advanced Y90 radioembolization therapy”, said Kennedy.
Robocath has today announced the results of its CARE clinical trial focusing on robotic carotid stenting—the first phase of a research programme launched in July 2021 by Robocath and Rennes University Hospital (Rennes, France), which, in the long term, is aiming to enhance current and future generations of robots used in the treatment of neurovascular diseases.
The prospective, single-arm, non-randomised CARE trial, launched in November 2021, saw François Eugène and Quentin Alias (both Rennes University Hospital, Rennes, France) perform a total of seven robotic procedures using R‑One, an innovative robotic platform developed and marketed by Robocath. This first-generation robot is designed to improve treatments by enhancing physicians’ hand gestures through increased precision, as well as drastically reducing medical staff’s exposure to X-rays.
According to Robocath, all procedures in the CARE trial were performed without any medical complications, giving R-One a 100% clinical success rate. From a technical standpoint, only one of the procedures required a complete manual conversion.
“I am honoured to have been part of this clinical trial, which marks an important first step on the road to making robotic procedures routine practice for the treatment of strokes,” said Eugène. “The success of these procedures is down to two key factors: accuracy and speed of patient care. Just like human hands, Robocath’s robot can move with millimetre precision and ensure the instruments remain in a fixed position for the entire duration of the procedure. Moreover, the technology opens up the possibility of long-distance treatment for stroke patients.
“Given these advantages, I believe that, in the years to come, robotic technology will be a driver of change in our patient care. Thanks to this technology, we can make treatment more effective and offset the unequal distribution of resources which currently leaves many stroke patients without access to a local treatment centre. Robotics has the power to bring equal access to treatments to all patients across France and in other countries facing similar public health challenges.”
“In our line of work, precision is key to the success of each intervention,” Alias added. “I am impressed by the pinpoint accuracy of the robot’s movements. The use of robotics could become, in time, the go-to treatment option for vascular diseases.”
“Conducting this first study in interventional neuroradiology was an essential step in the development of our robotic platform,” said Lucien Goffart, CEO of Robocath. “Since then, we have worked hard to integrate the expectations of users in order, ultimately, to offer them an intelligent robotic solution they can use in their daily practice to the patient’s benefit.”
Cardio Flow recently announced it has received US Food and Drug Administration (FDA) 510(k) clearance for the company’s FreedomFlow orbital atherectomy peripheral platform.
The company details in a press release that the FreedomFlow platform is designed with a modern mechanism of action to clear plaque blockages in the arteries of the legs. This proprietary, catheter-based design leverages the physics of angular momentum, creating a spiral geometry that puts five diamond-coated spheres in simultaneous contact with the vessel wall, whether advancing or retracting. A diamond-coated tip also helps ease the driveshaft through tight blockages.
According to Cardio Flow, this unique approach gives physicians a highly efficient, effective, and flexible way to treat complex peripheral arterial disease (PAD) in a wide range of vessel diameters—from 2mm in the ankle to 8mm in the hip—and greater versatility in treating multiple arteries and multiple blockages in the same vessel, all with a single device.
The company adds that the simplicity of the FreedomFlow platform likewise offers time savings and cost efficiencies, with quick and simple device setup, no capital equipment, no lubricant, and reduced inventory needs. It also provides faster run times, consistent treatment outcomes, and a nearly flat learning curve for physicians, making it an ideal choice for today’s hospitals, ambulatory surgical centres, and office-based labs.
Thomas Davis, director of cardiovascular research at Ascension St John’s Hospital in Detroit, USA, commented: “The incidence of patients presenting with multilevel PAD has increased dramatically in my practice, so having a flexible, efficient, and easy-to-use device that can treat PAD in a broad range of vessel sizes is a key advantage for physicians and patients as we seek to reduce the number of PAD-related amputations.”
Michael J Kallok, CEO of Cardio Flow, stated: “Cardio Flow is committed to providing meaningful solutions that directly address the needs of physicians and their PAD patients through innovative product development. Many of the existing atherectomy devices on the market have various design constraints and capital equipment costs. With FreedomFlow, we strove to provide physicians with the freedom to treat complex PAD hip to heel with a simple yet sophisticated device that would answer the call for flexible treatment options and cost savings for healthcare systems. We are excited that FreedomFlow will now be available to physicians.”
Interventional Systems have announced that Micromate has been granted a new 510(k) clearance, allowing the commercial sale of the robotic system in the USA for percutaneous procedures using computed tomography (CT) optical navigation, such as biopsies and ablations, to diagnose and treat conditions in the chest, abdomen, and musculoskeletal structures.
This latest US Food and Drug Administration (FDA) clearance further expands the scope of Micromate, which has been available in the USA since 2021 for any percutaneous needle intervention performed under live imaging using cone-beam CT, CT fluoroscopy, or a fluoroscope. The miniature robot was also cleared for integration into third-party navigation stations.
As Pedro Costa, CEO of Interventional Systems, remarks: “This clearance is a long-awaited milestone for us, and it allows us to meet the growing demand for our system in the USA. We are already in the process of executing the first installations overseas, bringing the benefits of our robotic platform to patients in the USA. We designed Micromate for versatile use within the scope of work of any interventional radiologist or oncologist, and we expect it to help hospitals gain efficiency in an era where both demand for precision and staff shortages are pressing concerns.”
Srdjan Milosavljevic, chief technology officer of Interventional Systems, also highlights: “The clinical data reviewed by the FDA as part of our submission demonstrates that we provide high accuracy in all major anatomical regions, making procedures faster and safer. We believe that both large institutions and ambulatory centres can benefit from Micromate’s unique features, and we will make sure we will always keep cost-effectiveness in mind when building on our innovative robotic technology.”
Delcath Systems, an interventional oncology company focused on the treatment of primary and metastatic cancers of the liver, have announced the publication of an article entitled ‘Selective internal radiotherapy (SIRT) and chemosaturation percutaneous hepatic perfusion (CS-PHP) for metastasized uveal melanoma: A retrospective comparative study” in the peer-reviewed oncology journal Cancers.
CS-PHP utilises CHEMOSAT, Delcath’s proprietary European CE Marked hepatic delivery system (HDS), to administer high-dose chemotherapy (melphalan) to the liver, while controlling systemic exposure and associated side effects during a PHP procedure. Initial findings were previously presented on September 9, 2023 at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark).
Descriptive Survival by Treatment.Adjusted Conditional Survival by Treatment.
Uveal melanoma usually shows a liver-dominant metastasis spread and is often treated with liver directed therapies. This retrospective study compared two cohorts of patients with liver dominant uveal melanoma treated at the University Hospitals Tubingen, Germany with multiple cycles of either CS-PHP (N=28) or SIRT (N=34).
Patients included in the study were treated between December 2013 and February 2020. Allocation to treatment was determined by a multidisciplinary team.
Presence of extrahepatic disease at baseline favoured the SIRT group (68% and 41%, CS-PHP and SIRT, respectively), as did the hepatic tumour load (0–25%: 57% and 76%; 26%–50%: 29% and 24%; >50%: 14% and 0%, for CS-PHP and SIRT, respectively). Tumour responses were evaluated by consensus reading by two experienced radiologists.
Disease control rates (DCR) were 30% and 18%, for CS-PHP and SIRT, respectively. Median overall survival (mOS) was 516 days for CS-PHP and 300.5 days for SIRT. In a Cox regression model, there was a significant difference between SIRT and CS-PHP treatment, HR = 0.46, CI 95% (0.23; 0.93), p = 0.030.
An adjusted Cox regression analysis, including the variables age, sex, presence of extrahepatic metastasis and hepatic load at baseline, also showed a significant effect of choice of treatment, HR=0.32, CI 95% (0.14; 0.73), p=0.006.
Median progression-free survival (mPFS) was 408.5 days for CS-PHP and 127.5 days for SIRT; the adjusted Cox regression analysis showed a trend favouring CS-PHP (p=0.090).
When initially presented at CIRSE, Gerd Groezinger (University of Tübingen, Tübingen, Germany) stated “liver directed treatment, including transarterial radioembolization and CS-PHP, is a critical treatment modality for patients with metastatic uveal melanoma, given the longer overall survival seen in the CS-PHP cohort, we conclude that for metastatic uveal melanoma patients, CS-PHP might be the superior liver directed treatment option”.
“There is a scarcity of comparative studies between liver directed therapies. This peer reviewed publication authored by experienced investigators, supports that the PHP procedure, whether utilising melphalan delivered by Delcath’s CE Marked Chemosat or the US Food and Drug Administration (FDA) approved HEPZATO KIT, may be the preferred liver directed treatment option for patients with liver-dominant metastatic uveal melanoma,” said Vojo Vukovic, Delcath’s chief medical officer. “We remain committed to making this treatment option available to patients in the USA by the end of this year.”
Published in the Journal of Vascular and Interventional Radiology, a recent retrospective study which evaluated pain relief after percutaneous image-guided cryoablation in patients with symptomatic extraperitoneal endometriosis (EE), has found the treatment to be “safe and effective”. Lead author Francois H Cornelis (Memorial Sloan Kettering Cancer Center, New York City, USA) and colleagues detail that the minimally invasive procedure “significantly reduced pain” and succeeded in obtaining local control of EE in their patient population.
Affecting around 190 million women of reproductive age worldwide, EE is a chronic disease that many women have “limited awareness” of, the study authors state. For this reason, they believe that lengthy delays can occur between symptom onset and diagnosis. Therapeutic options most commonly offered to these patients are hormonal agents or surgical excision. However, among the minimally invasive procedures developed during the last decade, Cornelis et al explain, cryoablation has become a “promising option” for the treatment of abdominal wall EE, with “satisfactory outcomes and low morbidity”.
“Cryoablation of soft-tissue lesions may be performed safely because the ice produced remains visible using the imaging techniques used in interventional radiology [IR] to guide the procedure,” Cornelis and colleagues explain, noting the improved precision cryoablation can provide when assessing the margins of ablation, thus reducing risks.
Conducted between 2017 and 2022, theirs was an observational and retrospective study, which employed the database of a single institution identifying patients who were referred to the IR department for cryoablation of symptomatic EE. The authors delineate that diagnosis of EE was based on the results of a pathologic analysis or via the identification of clinical/radiological features of EE, such as a mass accompanied by pain that is often cyclical in its recurrence.
Cornelis and colleagues identified a total of 42 women from the database with whom had a median age of 37 years. Among this cohort, 47 lesions were treated. Patients were made aware that cryoablation is offered as a minimally invasive alternative to surgery, but that a secondary surgical resection could be performed if necessary.
The median follow-up duration was 13.5 months after cryoablation, the authors convey that the median pain-free survival rate post-procedure was 93.8% (95% confidence interval [CI], 77.3–98.4) at six months and 82.7% (95% CI, 58.8–93.5) after 12 months. Pain decreased from a median of eight out of 10 on the visual analogue scale, to zero out of 10 at last follow-up. Additionally, their results show the efficacy rate of cryoablation to avoid secondary surgery was recorded as 92.8%. Characterised by a recurrence of pain, Cornelis et al reported a 2% rate of adverse events in this cohort, noting four patients who reported pain in the days following the procedure, and one patient that reported a recurrence of symptoms a year following.
Restating the “excellent safety profile” of cryoablation seen in their results, the authors emphasise that due to the freezing procedural temperatures, the ice is visible under real-time imaging guidance, reducing the “risks of injuring the skin or bowel”. Although previously demonstrated, Cornelis and colleagues note that their findings confirm cryoablation “can be performed safely” in patients under local anaesthesia and on an outpatient basis, “reducing the length of hospitalisation and postoperative recovery”.
Moreover, Cornelis et al convey the effectiveness of cryoablation for EE in their results, but conclude that the procedure “must be evaluated in multidisciplinary committees to ensure adequate selection and follow-up of women”. They state that prospective trials must be carried out to confirm the technique so that it can be incorporated into future guidelines for the therapeutic treatment of EE.
New research examining the safety and efficacy of using radial access for peripheral artery interventions has found that radial access allows early ambulation and same-day discharge with no serious adverse events.
These are the conclusions of a study published in the Journal of the Society for Cardiovascular Angiography & Interventions (JSCAI), conducted by a team of researchers from eight prominent US medical centres, aimed at examining the safety and feasibility of radial artery access for complex endovascular lower extremity interventions.
Peripheral artery interventions are commonly performed to treat vascular conditions that obstruct blood flow to the lower extremities, though traditionally these procedures have used a femoral artery access approach. In recent years, there has been increasing interest in using radial access, which involves accessing the arteries of the wrist or forearm, as an alternative approach.
From June 2020 to June 2021, 120 patients at eight centres were enrolled. The mean age of the patient population was 68.7 years and 31.7% were women. The 224 lesions treated were in iliac (12.9%), femoropopliteal (55.3%), isolated popliteal (11.9%) and tibial (19.5%) vessels.
The primary efficacy endpoint, procedural success, defined as the successful completion of the procedure without conversion to femoral access and without radial access complications peri-procedure, was achieved in 112 (93.3%) patients. One patient (<1%) required femoral access conversion to complete the procedure. Thirty (25%) patients required one or more additional access to facilitate crossing and/or to complete the planned treatment (5 femoral, 10 tibial, and 17 pedal). No serious adverse events were adjudicated to the procedure. Mean procedure time and time to ambulation was 74 minutes and 3 hours 30 minutes; respectively, with 93.3% same day discharge. At 30 days, 97.2% of patients had ultrasound-confirmed radial access patency.
The findings of the study also demonstrate that radial access for peripheral artery interventions was associated with favourable safety profiles. Notably, the incidence of access site complications and major adverse cardiovascular events was significantly lower compared to the traditional femoral access approach. The results also showed comparable procedural success rates and long-term clinical outcomes between the two approaches.
Additionally, radial access was found to have the potential to be a safe and effective alternative for performing peripheral artery interventions. The researchers believe that the wrist and forearm offer several advantages over the traditional femoral access site, including improved patient comfort, reduced bleeding complications, and faster ambulation. Further research and clinical trials are warranted to validate these findings and establish radial access as a mainstream approach in this field, the study’s authors note.
“This study contributes to the growing body of evidence supporting the use of radial access for peripheral artery interventions,” stated Mehdi Shishehbor (University Hospitals Harrington Heart & Vascular Institute, Cleveland, USA), lead author of the study. “As medical professionals continue to explore different approaches, advances in technology and techniques are expected to further enhance the safety and efficacy of these procedures. With its potential to improve patient outcomes and satisfaction, radial access may revolutionise the field of peripheral artery interventions.”
Writing in the conclusion to their paper, the study’s authors note that their research shows the safety and efficacy of the radial access approach for treating complex, multilevel peripheral arterial disease. “Radial approach allowed same day discharge for most patients with no serious adverse events,” Shishehbor et al write. “Future randomised trials should examine the clinical and cost effectiveness of this approach compared with femoral access for patients with peripheral arterial disease.”
While sex disparities regarding the outcomes of carotid revascularisation have “long been a concern”, new prospective data published in the Journal of Vascular Surgery (JVS) indicate that no such disparity exists between male and female patients treated with transcarotid artery revascularisation (TCAR; Silk Road Medical)—one of the most prominent approaches used to treat carotid artery stenosis.
Writing in JVS on behalf of the ROADSTER trial investigators, Vikram Kashyap (Frederik Meijer Heart and Vascular Institute at Corewell Health, Grand Rapids, USA) and colleagues report “exceptionally low” rates of stroke, death and myocardial infarction (MI) derived from prospective TCAR trial data. They further note that these low rates “do not differ by patient sex”.
Previously, several studies of carotid revascularisation have demonstrated increased frequencies of postoperative death and stroke for female patients after either carotid endarterectomy (CEA), or transfemoral carotid artery stenting (CAS). In addition, adverse events after transfemoral stenting are higher in female patients, particularly in symptomatic cases, the authors relay.
In prospectively analysing results from the ROADSTER 1, ROADSTER 2 and ROADSTER Extended Access TCAR trials, Kashyap and colleagues’ objective was to investigate post-TCAR outcomes stratified by patient sex. They hypothesised that the results would be similar between males and females.
All included patients had verified carotid stenoses meeting the criteria for carotid intervention (≥80% in asymptomatic and ≥50% in symptomatic patients), and were included based on anatomical or clinical high-risk criteria for carotid stenting. The researchers’ primary outcomes were a combination of stroke/death (S/D) and stroke/death/MI (S/D/M) at 30 days, while secondary outcomes were the individual components of stroke, death, and MI.
Kashyap and colleagues included a total of 910 patients for analysis, roughly two thirds of whom were male (n=604; 66.4%). They note that female patients were more often <65 years old (20.6% vs 15%) or ≥80 years old (22.6% vs 20.2%), and were more often of Black/African American ethnicity (7.5% vs 4.3%), as compared with their male counterparts.
“There were no differences by sex in term of comorbidities, current or prior smoking status, prior stroke, symptomatic status, or prevalence of anatomical and/or clinical high-risk criteria,” the authors disseminate. “General anaesthetic use, stent brands used and procedure times did not differ by sex—although flow reversal times were longer in female patients, [and] more contrast [was] used in procedures for female patients.”
In addition, both the 30-day rates of S/D (2.7% male vs 1.6% female) and S/D/M (3.6% male vs 2.6% female) were similar between the two groups of sex-stratified patients. The researchers also found that these key outcome measures did not differ when patients were stratified by symptom status either. Comparable findings were identified in terms of secondary outcomes—including stroke rates at 30 days—too.
“Univariate analysis demonstrated that history of a prior ipsilateral stroke was associated with increased odds of S/D (odds ratio [OR] 4.19) and S/D/M (OR 2.78), as was symptomatic presentation with increased odds for S/D (OR 2.78),” Kashyap and colleagues aver in conclusion.
HistoSonics, the manufacturer of the Edison System and novel histotripsy therapy platforms, has announced the marketing authorisation of its “breakthrough” platform via the US Food and Drug Administration’s (FDA) de novo classification request process, a rigorous pre-market review pathway for medical devices with no existing predicate. Marketing authorisation makes Edison the first and only histotripsy platform available in the USA.
“This is HistoSonics’ most meaningful milestone to date and represents over two-decades of tireless efforts, from its inception in 2001, overcoming what was once thought to be impossible”, commented Mike Blue, President, and CEO of HistoSonics.
FDA authorisation was based, in part, on data from the #HOPE4LIVER trials in 13 trial sites across the USA and Europe. Data pooled from both the USA and European/UK trials were used to assess the clinical safety and efficacy of histotripsy in destroying targeted primary and secondary liver tumours. Histotripsy was noted to have achieved both primary safety and efficacy endpoints in the pooled data where 44 subjects were evaluated for safety and 44 tumours treated were evaluated for efficacy.
Important to note was the heterogeneity of the treated subjects, 18 of which had hepatocellular carcinoma (HCC) tumours and 26 had metastatic tumours to the liver from the colon, rectum, breast, and other primary origins. As recently presented at the annual Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 meeting (9–13 September, Copenhagen, Denmark), a technical success rate of 95.5% was achieved indicating that physicians can precisely target and destroy liver tissue and unresectable liver tumours. Also, only three procedure related Common Terminology Criteria for Adverse Event (CTCAE) Grade 3 or higher adverse events through 30 days post-histotripsy were observed across all 44 subjects treated, representing a complication rate of 6.8% with each event being common to focal liver therapies and not specific to histotripsy.
“This is HistoSonics’ most meaningful milestone to date and represents over two-decades of tireless efforts, from its inception at the University of Michigan in 2001, overcoming what was once thought to be impossible—integrating the many complexities of histotripsy into a completely non-invasive clinical platform,” commented Mike Blue, president, and CEO of HistoSonics. The company noted it has expanded its commercial and operational capacity over the previous year in preparation for commercial activities. Blue added, “We have been thoughtfully adding professionals with deep domain experience in operations, market development and education and are prepared to begin scheduling physician training immediately. This is a fantastic day for patients who will benefit from the novel advantages of histotripsy, and I commend the FDA for working so expeditiously with us throughout the review process.”
The science of histotripsy uses focused sound energy to produce controlled acoustic cavitation that mechanically destroys and liquifies targeted liver tissue, including tumours, at sub-cellular levels. HistoSonics’ Edison System uses proprietary technology and advanced imaging to deliver personalised, non-invasive histotripsy treatments with precision and control. The company believes that the novel mechanism of action of their proprietary technology may provide significant advantages to patients, including the ability of the treatment site to recover and resorb quickly. Uniquely, the HistoSonics’ platform also provides physicians the ability to monitor the destruction of tissue under continuous real-time visualisation and control, unlike any modality that exists today.
“As a surgeon, it’s rewarding to be able to offer a procedure where we can precisely destroy liver tumours without using a scalpel or needles, hopefully enabling the patient’s quick recovery while avoiding certain complications like surgical site infections or radiation illness common with other modalities,” commented Joe Amaral MD, vice president of medical affairs for HistoSonics. “Based on the data and patient experiences in our studies we are confident histotripsy will have a meaningful impact for patients suffering from unresectable liver disease, including liver tumours, and we look forward to the role histotripsy will play in treatment strategies going forward,” added Amaral.
The Edison System is indicated for the non-invasive destruction of liver tumours, including unresectable liver tumours, using a non-thermal, mechanical process of focused ultrasound.
“We wanted to find a common language between interventional radiologists and nephrologists and we wanted to be sure that the angioplasty we have done has a functional improvement”, associate professor of interventional radiology, Stavros Spiliopoulos (Athens, Greece) speaks to Interventional Newsabout the VOLA II trial, of which he was principal investigator.
VOLA II, a prospective, multicentre study of 100 arteriovenous fistula (AVF), which revealed post-procedural volume flow (VF) is an independent predictor of patency, and has been submitted for publication. Expanding on the significance of their findings, Spiliopoulos imparts: “I advise everyone to use this tool because it will change their practice and improve their outcomes”.
Video Attributions
Images and footage attribution: Kateryna/stock.adobe.com
Music: QUIRKY-TENSION-INVESTIGATION-(SLEEK-SNEAK). Performed by FineTune Music. stock.adobe.com
Merit Medical Systems, a leading global manufacturer and marketer of healthcare technology, today announced the expansion of its Maestro microcatheter product line to now include a new longer length for radial embolization procedures.
The Maestro is part of a comprehensive offering of embolotherapy solutions, which includes embosphere microspheres, the most widely studied and clinically utilised round embolic on the market. Embolization is a minimally invasive procedure that blocks one or more blood vessels or abnormal vascular channels to treat a number of clinical conditions. The new 165cm Maestro length will be available in 2.1French (F), 2.4F, 2.8F, and 2.9F catheter diameters to support a broad range of embolization procedures.
“Merit Maestro’s longer length is ideal for radial access,” said Mary Costantino (Advanced Vascular Centers, Oregon, USA) and a paid consultant of Merit. “Radial access can streamline patient care by enabling some patients to be treated in outpatient and office-based lab settings where they can return home on the day of their procedure, improving patient satisfaction and saving healthcare resources.”
“The Maestro expansion continues our strong legacy of advancing solutions for our healthcare partners,” said Fred P Lampropoulos, Merit Medical’s chairman and CEO. “We are especially pleased to bring new technology to our embolotherapy portfolio. Through ongoing innovation, as well as the reinvention of existing products, we enhance the alignment of our portfolios with our mission of improving lives around the globe.”
The Maestro microcatheter is compatible with coils up to 0.018″ and embolics up to and including 900µm. Three tip designs are available, including a swan neck designed to seat the catheter in the vessel, reducing the recoiling effect of the microcatheter as embolic is delivered. A hydrophilic coating aids in smooth tracking through tortuous anatomy.
Merit is a market leader in radial access with a portfolio that includes the recently launched PreludeSYNC EZ radial compression device, PreludeSYNC distal radial compression device, and Prelude IDeal hydrophilic sheath introducer.
Radial artery access is a minimally invasive approach to diagnosing and treating a wide range of medical conditions. Through a small hole in the wrist, a catheter is inserted into the radial artery. Under imaging guidance, the catheter is then threaded through the body’s network of blood vessels to the location needing treatment. Compared to femoral access procedures, or those performed through the femoral artery in the groin, benefits of radial access include fewer bleeding complications, improved patient comfort, and decreased procedure costs, the press release states.
Roger Malcolm Greenhalgh, the surgeon internationally renowned for his unparalleled contribution to vascular education, training and research, died peacefully on 6th October, aged 82. At the time of his death, he was emeritus Professor of Surgery at Imperial College in London and head of its Vascular Surgery Research Group.
Roger Greenhalgh, born in Derbyshire, was not from a medical background. His parents were very entrepreneurial in their different ways and his grandfather, Fred Poynton, broke the world record in road walking over 20 miles in 1924. He went to Ilkeston Grammar School, a state school with entry by scholarship only. There he followed the advice of his headmaster, John Hewitson, that he should consider medicine as a career. He was the first in his family to attend university. Within a term of arriving at Clare College, Cambridge, his medical tutor, Dr Gordon Wright, predicted that Roger Greenhalgh would be a surgeon. At St Thomas’s Hospital in London, he qualified as a doctor and was allowed to move up the surgical ladder with a rotation to learn research methods at the Hammersmith Hospital after his surgical training at St Thomas’s. During this time, he discovered a love of vascular surgery. The pioneer vascular surgeon, Peter Martin, inspired him by saying that he would go on to solve problems that he could not. Whilst in training, in 1974, he won the prestigious Moynihan Fellowship of the Association of Surgeons of Great Britain & Ireland. The £1,000 stipend enabled him to visit many worldwide vascular centres of excellence using the connections of his mentors Peter Martin, Frank Cockett and Professor Gerry Taylor.
Roger Greenhalgh joined the surgical consultant staff as senior lecturer at Charing Cross Hospital in 1976, less than 10 years after being a medical student. His career did not follow a conventional path by moving from the St Thomas’s system to St Barts and finally, to Charing Cross. He went on to become professor of surgery, head of the university department and dean of the Charing Cross & Westminster Medical School for four years, between 1993 and 1997, during which time he oversaw a merger with Imperial College London. His junior at St Bart’s and then Secretary of the Vascular Society of Great Britain and Ireland (VSGBI), Professor Bruce Campbell, said to Professor Greenhalgh, who was the millennium president of the Vascular Society from 1999 to 2000: “You always do your own thing, you know you do.”
Michael DeBakey (far left), Karin Greenhalgh and Roger Greenhalgh in 1989
Professor Greenhalgh’s long and distinguished research career started with an interest in hyperlipidaemia when he was a resident, during which he attempted to elucidate the role played by serum lipids and lipoproteins in arterial disease as lead author of a 1971 paper published in The Lancet. His research, with more than 300 original published papers, spanned all areas of vascular surgery: venous, carotid, peripheral and aortic. His most significant contributions came from his early adoption of the rigour of prospective randomised trials to address the grey areas in vascular disease management. He led more than a dozen trials in the field of aneurysm management to promote level-one evidence in clinical practice, including the UK Small Aneurysms Trial (UKSAT) and the UK endovascular aneurysm repair (EVAR 1 and 2) trials. UKSAT was the first trial to show that there was no long-term survival benefit of early elective open repair of small abdominal aortic aneurysms. The 15-year follow up of the EVAR 1 and 2 trials were published in The Lancet in 2016 showing EVAR has an early survival benefit but an inferior late survival compared with open repair, which needs to be addressed by lifelong surveillance of EVAR and reintervention if necessary. Professor Greenhalgh was also the principal investigator of the mild to moderate intermittent claudication (MIMIC) trials which finally proved the adjuvant benefit of angioplasty over supervised exercise and best medical therapy in patients with stable mild and moderate intermittent claudication.
Inspired by the impact of these many landmark trials, Andrew W Bradbury, Sampson Gamgee Professor of Vascular Surgery, University of Birmingham, UK, and principal investigator of the randomised controlled BASIL trials, wrote to Professor Greenhalgh: “Your achievements are greater than anyone alive or dead.” Professor Bradbury recently presented first-time results from the BASIL-2 trial at CX 2023 during a session chaired by Professor Greenhalgh.
Princess Anne attends the CX Symposium in 1982
Professor Greenhalgh founded the Charing Cross series of international symposia and annual books in 1978 when he was 37 years of age. This started as a small, focused symposium, with topics such as smoking and arterial disease, held at the Charing Cross Hospital. The earliest symposia had just 100–200 delegates but were always accompanied by a book covering the main presentations and discussions. The Charing Cross (CX) Symposium has grown exponentially and has been forced to move to much bigger venues to cope with the increasing popularity of the meeting which peaked at over 4,000 in-person attendees in the years immediately before the Covid pandemic. Pioneers such as Michael DeBakey, Denton Cooley, Jesse Thompson, John Mannick, John Bergan, Jimmy Yao, Ted Diethrich, Juan Parodi and Frank Veith have all graced the podium. Tom Fogarty spoke of his catheter and Andreas Grüntzig spoke of his angioplasty in the 1980s. Julio Palmaz gave news of endovascular aneurysm repair (EVAR) at CX 1990. CX continues to provide top class vascular education and critical discussion of cutting-edge developments in the management of vascular disease. Professor Greenhalgh presided over the 45th symposium earlier this year. Many speakers feared his acerbic wit and the tolling of the bell if they strayed overtime.
Professor Greenhalgh, who was quick to embrace digital methods of transmission, recently spoke from the state-of-the-art CX Vascular studio in London to detail the global interest in the Charing Cross brand of education. In 2023, the symposium saw registrations from 2,500 in-person attendees and an additional 7,000 people participated digitally, tuning in mainly from China. He was always in his element at the CX podium, his secret passion for the theatre on full display, enjoying the cut and thrust of discussing the current, hot-button issues in the vascular field with global experts. Age did not wither nor custom stale his delight in unpicking an argument to get to the core of the matter, always endeavouring to outline the research and education required to drive the topic forward. In the days before his passing, Professor Greenhalgh’s passion for the quality of the CX Symposium programme burned brightly right to the very end as he worked on the CX 2024 version in the Hammersmith Hospital’s De Wardener ward intensive care unit.
Professor Greenhalgh played a pivotal role in the creation of the European Society for Vascular Surgery (ESVS) and the establishment of its journal. The ESVS was launched at CX in 1987 and Professor Greenhalgh wrote the constitution. He was founder and chairman of the editorial board for the European Journal of Vascular and Endovascular Surgery (EJVES) from 1987 to 2003. He became the first ESVS European honorary member because of his role in the ESVS foundation. He also played a major role in the development of surgical training and standards across Europe through his role as President of the European Board of Surgery for the European Union of Medical Specialists (Union Européenne des Médecins Spécialistes – UEMS) from 1998 to 2002 and the European Board of Vascular Surgery (2002-2006). The European Board of Vascular Surgery honoured Professor Greenhalgh as Honorary Life President in recognition of his founding role.
His brilliant surgical skills were recognised by innumerable international surgical societies as well as the White House Medical Unit for the support he provided during the visit of President George H Bush to London in 1991. More recently, Professor Greenhalgh became a company director, founding BIBA Medical with his son, Stephen, in 1994. Professor Greenhalgh was editor-in-chief of the company’s foremost medical publication, Vascular News, from its inception in 1999 to 2023, overseeing a total of 100 editions of the newspaper in this time. He captured his experiences in the roles of surgeon, professor and company director in his 2011 autobiography, Born to be a Surgeon.
Professor Greenhalgh received recognition for his lifelong contributions to vascular surgery from multiple prestigious groups, including most recently, an honorary Fellowship of the American College of Surgeons in October 2018 and the first Living Legend or International Lifetime Achievement Award from the Society for Vascular Surgery (SVS) in June 2018 after being nominated by the ESVS. Enrico Ascher (New York University, New York, USA), who presented the award and is a past president of the SVS, said of Professor Greenhalgh at the time: “He leads by example. Not only by his contributions, or his political influence, or his knowledge, or trials, but actually as a person. As a person who is totally committed to his profession, to his family, to his friends, to his peers. He thinks first about them, and not about himself. That is what makes him a moral leader, and what sets him apart.”
Writing in EJVES following Professor Greenhalgh’s receipt of this award, his long-time research partner, Professor Janet Powell (Imperial College, London, UK) described him as a “brilliant” clinician with a “long and distinguished” research career, as well as highlighting his prowess as an educator and mentor, noting that “medical students and junior doctors have queued for the opportunity to work in his team”. She also hailed him as a “legendary figure” whose wit, humour and charm “have made him many friends across the world”.
Roger Greenhalgh receiving the first Living Legend or International Lifetime Achievement Award from the Society for Vascular Surgery (SVS) in 2018 from Enrico Ascher
Professor Greenhalgh had many sporting skills and interests. He rowed in international regattas with future Olympian, Peter Thomas, at stroke whilst he was captain of boats as a medical student at St Thomas’s Medical School. He remained a strong supporter of the Imperial College Boat Club and even had a boat named after him. His love of skiing saw him create the Association of International Vascular Surgeons (AIVS) which was used to forge international professional friendships and the AIVS continues to this day under the chairmanship of Mark A. Adelman. He was supported throughout by his Austrian wife, Karin, whose ability to speak multiple European languages and communicate with people from all cultures, proved invaluable.
Professor Roger Greenhalgh, MA MD MChir FRCS, was married to Karin Maria (née Gross)—who died in April 2020 from COVID-19. They were happily married for over 55 years and her constant support was integral to his success. He was at his most relaxed amongst his family. He is survived by his two children, Stephen (Lord Greenhalgh) and Christina, and three grandchildren Sebastian, Francesca and Marcus of whom he was immensely proud.
Artivion has announced presentation of interim results from the Ascyrus medical dissection stent (AMDS) PERSEVERE clinical trial in a late-breaking science session at the 37th European Association for Cardio-Thoracic Surgery (EACTS) annual meeting (4–7 October, Vienna, Austria).
Fernando Fleischman (Keck Hospital of the University of Southern California, Los Angeles, USA) delivered data from the PERSEVERE US investigational device exemption (IDE) trial in a late-breaking presentation titled, “Interim results of AMDS hybrid prosthesis in acute DeBakey Type I [ADTI] dissection with malperfusion”, including interim data on 52 study participants at 30 days post-implantation and an additional eight participants in total follow-up.
As Artivion details in a recent press release, these interim data demonstrate a clinically meaningful reduction of all-cause mortality and primary major adverse events (MAEs), with 79% of participants experiencing no target MAEs at 30 days (41 of 52 patients).
In PERSEVERE, rates of all-cause mortality (13.5%), new disabling stroke (9.6%), new onset renal failure requiring dialysis (7.7%) and myocardial infarction (0%) all compared favourably to ‘historical reference’ rates, according to Artivion.
The interim data also demonstrate “excellent” results for additional PERSEVERE endpoints, including a technical success rate of 98.3%; an unanticipated aortic reoperations rate of 1.7%; and no instances of distal anastomotic new entry (DANE) tears, distal stent-induced new entry (d-SINE), occlusion of supra-aortic vessels, or new postoperative paraplegia or paraparesis.
“The current standard of care to manage acute Type I aortic dissections is technically meticulous and often leads to distal anastomotic new entry tears, or DANE tears, which are associated with increased risk for re-intervention and mortality,” said Fleischman. “I am encouraged by the interim results of the PERSEVERE study, which indicate that the use of AMDS offers substantial clinical benefit—notably the absence of DANE tears and an improved all-cause mortality rate—for patients presenting with malperfusion and ADTI dissection at 30 days, while adding minimal time and complexity to the procedure.”
Interventional News’ most read stories in September included first data releases from the this year’s Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark) such as STRIKE-PE results; Laminate Medical announce FDA approval of flagship VasQ External Vascular Support device and a multi-society update on guidelines for varicose vein management.
Presenting data from the MOTIV bioresorbable scaffold (Reva Medical) below-the-knee (BTK) trial during Saturday’s FIRST@CIRSE session at CIRSE 2023 annual meeting (9–13 September, Copenhagen, Denmark), Thomas Rand (Klinikum Floridsdorf, Vienna, Austria) underlined the “promising future applications” of the device for the treatment of BTK arteries.
Find out how, by taking away the difficulties associated with freehand alignment and targeting, Micromate helps physicians focus on improving reproducibility, speeding up the procedure, reducing radiation dose, and deploying the system even for complex indications.
Presenting real-world population data in patients with pulmonary embolism (PE), John Moriarty (University of California, Los Angeles Medical Center, Los Angeles, USA) demonstrated results from the STRIKE-PE study at this year’s CIRSE 2023 annual meeting.
Mishal Mendiratta-Lala (University of Michigan, West Bloomfield, USA) presented “much awaited” data from the #HOPE4LIVER trial at CIRSE 2023, which demonstrated the “successful, non-invasive destruction” of liver tissue using hepatic histotripsy.
Laminate Medical Technologies has announced their flagship device, the VasQ External Vascular Support, has been cleared by the US Food and Drug Administration (FDA) for use to create arteriovenous fistulas (AVFs) for dialysis access.
Tze Tec Chong (Singapore General Hospital, Singapore) presented results from the PRISTINE registry at CIRSE 2023, which aimed to investigate the performance and safety of the Selution SLR (MedAlliance) sirolimus-eluting balloon (SEB) for the treatment of complex occlusive lesions in chronic limb threatening ischaemia (CLTI) patients in Singapore.
LimFlow, a developer of minimally-invasive technologies for the treatment of chronic limb-threatening ischemia (CLTI), a severe form of peripheral artery disease (PAD), has announced that the US Food and Drug Administration (FDA) has approved the LimFlow system to help people with CLTI who have no other suitable endovascular or surgical treatment options and are facing major amputation.
In sessions dedicated to radiation protection at CIRSE 2023, contemporary risk management strategies for staff and patients, and challenges faced by interventional radiologists in the developing world were among key takeaways across Sunday and Monday.
Biotronik has announced the two-year results from the BIOLUX P-III BENELUX all-comers registry, presented by principal investigator Frank Vermassen (Ghent University, Gent, Belgium) at CIRSE 2023.
The Society for Vascular Surgery (SVS), American Venous Forum (AVF), and American Vein and Lymphatic Society (AVLS) have released the second and final part of new guidelines for the management of varicose veins of the lower extremities. The recommendations, which update the 2011 SVS and AVF guidance on the topic, were published online ahead of print in the Journal of Vascular Surgery: Venous and Lymphatic Disorders (JVS-VL).
Yuji Okuno (Tokyo, Japan), winner of the Award of Excellence and Innovation in Interventional Radiology during the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 meeting, discusses his pioneering work on the treatment of chronic musculoskeletal inflammation and pain with Ziv Haskal (Charlottesville, USA), emeritus editor-in-chief (2011-2020) of Journal of Vascular and Interventional Radiology (JVIR).
Okuno previously published research in CardioVascular and Interventional Radiology (CVIR) in 2014 examining the short-term clinical outcomes of transarterial embolization (TAE) for knee osteoarthritis using imipenem/cilastatin microspheres, which reported significant improvements in pain scores up to 12-month follow-up.
Focusing now on sports injuries in a “highly active, high-demand” cohort that is prone to overuse, Okuno states that they intended, “due to safety concerns” over the use of embolization for knee osteoarthritis including frozen shoulder syndrome and chronic lower back pain, to “develop the use of temporary embolic material” to combat inflammation and pain.
Video attributions
Music: Quirky-tension-investigation-(sleek-sneak)/performed by Apollo Audio/FineTune Music/stock.adobe.com
MedAlliance has been acquired by Cordis for a 2022 investment of US$35 million and a 2023 upfront closing payment of US$200 million, together with regulatory achievement milestones of up to US$125 million and commercial milestones of up to US$775 million through 2029, for a total consideration of up to US$1.135 billion.
Cordis is a developer and manufacturer of interventional cardiovascular and endovascular technologies. MedAlliance’s sustained sirolimus drug-eluting balloon (DEB) program, SELUTION SLR (Sustained Limus Release), has provided a flagship product family which complements Cordis’ existing product portfolio, together with their sales, marketing and distribution expertise, the companies said in a press release. Cordis customers will benefit from the extensive clinical study programme and publication plan that have been executed by MedAlliance to further Cordis’ heritage of bringing innovative products to patients, the press release states.
“The Cordis acquisition will accelerate access to this breakthrough technology for patients around the globe suffering from coronary and peripheral disease,” said Jeffrey B Jump, founder, chairman and CEO of MedAlliance. “I want to thank our entire MedAlliance team—including physicians, distributors and clinical patients—who have succeeded in disrupting the coronary and peripheral markets to provide a safe and effective new technology. The arsenal of SELUTION SLR DEB clinical data is designed to change medical practice and improve patient outcomes.”
“Nearly 20 years ago, Cordis introduced Cypher, the first drug-eluting stent, transforming cardiovascular treatment for patients around the world,” said Shar Matin, Cordis CEO. “As a newly independent company, we are beyond proud to further our legacy of innovation and market disruption with MedAlliance and the first MicroReservoir sirolimus drug-eluting balloon, Selution SLR.”
“We are excited to report on the positive Selution SLR data to date, with first-hand experience of the impressive clinical outcomes from patients treated with Selution SLR in Japan, India, Europe, and South America. We are now leading the effort to emulate these results in the USA. This technology has the distinct opportunity to change the treatment paradigm for patients suffering from cardiovascular and peripheral vascular disease,” commented George Adams (Cardiovascular and Peripheral Vascular Research, Rex Hospital, Raleigh, USA) Steering Committee member of both the US SELUTION4SFA and SELUTION4BTK IDE studies.
SELUTION SLR was awarded CE mark approval for the treatment of peripheral artery disease in February 2020 and for the treatment of coronary artery disease in May 2020. MedAlliance was the first drug-eluting balloon company to receive US Food Drug Administration (FDA) breakthrough designation status.
In addition to the below-the-knee (BTK) and superficial femoral artery (SFA) indications for which the company received FDA investigational device exemption (IDE) approval in May and August 2022 respectively, MedAlliance received coronary in-stent restenosis (ISR) IDE approval in October 2022 and de novo coronary artery lesions approval in January 2023.
Subsequent to achieving IDE Status, three FDA studies involving SELUTION SLR are currently enrolling with a fourth, involving patients with coronary de novo artery disease, planned to start in the next few weeks. The latter will complement the experience gained with the ground-breaking SELUTION DeNovo trial in Europe, which has now enrolled over 1,700 patients, halfway towards a planned 3,326 patients. SELUTION DeNovo compares the treatment strategy using SELUTION SLR versus any limus drug-eluting stent (DES).
MedAlliance’s DEB technology involves MicroReservoirs which contain a mixture of biodegradable polymer intermixed with the antirestenotic drug sirolimus applied as a coating on the surface of an angioplasty balloon. These MicroReservoirs provide controlled and sustained release of the drug for up to 90 days. MedAlliance’s proprietary Cell Adherent Technology (CAT) enables the MicroReservoirs to be coated onto balloons and efficiently transferred to adhere to the vessel lumen when delivered via expansion of the balloon.
SELUTION SLR is commercially available in Europe, Asia, the Middle East, and the Americas (outside USA) and most other countries where the CE mark is recognised. Over 40,000 units have been used for patient treatments in routine clinical practice or as part of coronary clinical trials.
Laminate Medical Technologies has announced their flagship device, the VasQ External Vascular Support, has been cleared by the US Food and Drug Administration (FDA) for use to create arteriovenous fistulas (AVFs) for dialysis access. The device, designated by the FDA as a Breakthrough Technology, was cleared based on a de novo review of the 144 patient VasQ US pivotal study as well as a track record of safety and effectiveness of use in multiple studies from outside the USA.
As recently published in the Journal of Vascular Access, VasQ patients in the VasQ study met the primary endpoint of improved primary patency (freedom from intervention plus adequate flow for haemodialysis) at 6-months. No serious adverse event associated with the device was reported over the two year study. Additional analysis comparing VasQ patients against claims data for traditional AVFs created by the same surgeons in the study, reported statistically superior rates of functional success (confirmed use of the AVF for dialysis), and reduced need for additional procedures. The result was central venous catheters (CVC), the primary source of hospitalisation due to infection in dialysis patients, were able to be removed in 80% of the patients within the first year as compared to 62% of unsupported fistulas as reported by the National Institute of Health’s United States Renal Data System.
Ellen Dillavou, division chief of vascular surgery at WakeMed Hospital Systems, stated, “I, along with other study investigators who have used the device, are excited that we can now offer VasQ to our fistula patients. We believe this will give our patients a better chance to receive a functioning fistula with fewer additional procedures and will allow earlier removal of central venous catheters before they lead to serious infections.”
VasQ is a nitinol-based device implanted around the artery and vein during the surgical creation of an arteriovenous fistula. The device was designed to provide structural reinforcement of the mobilised vessels now freed from its native supporting tissue as well as guides a more stable arterial flow profile as it transitions into the vein. Magnetic resonance imaging as well as computational fluid dynamic models have supported the proposed mechanistic benefits of the VasQ design that have led to consistent beneficial clinical outcomes in multiple studies.
“We are excited to finally bring VasQ to the dialysis patient population in the USA,” said Laminate CEO Tammy Gilon. “We could not be more appreciative of our principal investigators as well as the global community of dialysis access physicians that saw the potential in VasQ and produced the wealth of data supporting the devices safety and effectiveness.”
Shockwave Medical has announced that Nick West has joined the company in the role of associate chief medical officer (CMO). He will report to current CMO Keith Dawkins, and will be based in Santa Clara (USA) with plans to succeed Dawkins as CMO in mid-2024.
“Dr West brings to Shockwave a wealth of expertise in the interventional cardiology space,” said Dawkins. “Having known Nick for many years, I am confident that his expertise will be highly influential in further developing intravascular lithotripsy (IVL) as the standard of care for calcium modification, and will also be a valued asset in the evaluation and development of novel transformational technologies to augment our portfolio in the years to come.”
West joins Shockwave from Abbott Vascular, where he served as CMO and divisional vice president of global medical affairs for the past four years. Prior to his time with Abbott, West served as an attending cardiologist at the Royal Papworth Hospital NHS Foundation Trust (Cambridge, UK).
“There is no denying the exceptional job Shockwave has done to generate significant momentum behind IVL in a relatively short period of time. I am extremely excited to utilise everything I have learned from my time both in industry and previously as an interventional cardiologist to help continue to propel Shockwave forward as one of the most innovative players in the cardiovascular space,” said West. “I look forward to contributing to the company’s mission of developing exceptional solutions to revolutionize treatments for underserved patient populations.”
West graduated in medicine from Trinity Hall, University of Cambridge (Cambridge, UK) and St Thomas’ Hospital Medical School (London, UK) and trained in interventional cardiology at the John Radcliffe Hospital (Oxford, UK) and Green Lane Hospital (Auckland, New Zealand). He has published over 170 peer-reviewed papers and book chapters on topics including vascular biology, coronary physiology/microvascular function, intracoronary imaging/vulnerable plaque detection, and bioresorbable scaffold technology. He is a founding member and CMO of the Cambridge-based vulnerable plaque startup, PlaqueTec, and sits on the Innovation Council of the UCLA School of Biodesign.
West was also a co-author of the ILUMIEN IV late-breaking clinical trial presented at the European Society of Cardiology (ESC) congress (25–28 August, Amsterdam, The Netherlands) last month. “His expertise in intravascular imaging will be especially beneficial to many Shockwave IVL customers as the use of imaging continues to increase, and, as a result, there arises a greater appreciation for the presence and diverse morphology of cardiovascular calcium,” Dawkins concluded.
TechsoMed, a medical software innovator dedicated to enhancing clinical impact in ablation therapy, announced today that it has received 510(k) clearance from the US Food and Drug Administration (FDA) for its VisAble.IO software intended to assist physicians in planning liver ablation procedures, and confirming ablation zones, with the goal of increasing treatment precision.
Ablation therapy is a preferred minimally invasive treatment that uses extremely high or low temperatures to destroy abnormal tissue. However, insufficient image guidance precision and treatment control, lead to high risk of recurrence and complications, creating significant barriers to widespread adoption and limiting patients’ eligibility.
VisAble.IO is the first product to be released as part of TechsoMed’s full BioTrace solution, an end-to-end software solution for full visualisation and control for image-guided ablation therapy. By utilising AI-based technology, BioTrace leverages standard imaging—such as ultrasound along with computed tomography (CT) or magnetic resonance imaging (MRI) to provide visualisation of the full extent of the ablation zone in real-time, together with smart, personalised treatment planning and assessment tools, allowing physicians to provide their patients with optimised care.
VisAble.IO employs advanced computation and image registration to assist physicians in crucial steps of planning and assessing the ablation coverage of a liver tumour. Its key features include three-dimensional (3D) visualisation of the ablation target within a patient-specific anatomical view, overlay and position of virtual instruments and estimated ablation regions onto medical images and finally, a unique interactive 3D view of ablation margins and missed volumes to help users assess ablation target coverage immediately post procedure.
“There is a real need for a good and efficient assessment tool, and it can serve any physician performing thermal ablations” said Ryosuke Tateishi (University of Tokyo, Tokyo, Japan).
“We are excited to receive 510(k) clearance for our VisAble.IO solution and appreciate the relentless efforts of our entire team in achieving this milestone. This is a pivotal step forward in our journey of elevating ablation therapy into image guided ablation therapy and making it available for every patient everywhere,” said Yossi Abu, CEO and founder of TechsoMed. “The FDA’s validation of VisAble.IO’s safety and effectiveness not only reflects the exceptional quality of our product but also paves the way for significant commercial opportunities”.
The full BioTrace platform also includes the BioTrace.IO Lite software system, which is currently under review by the FDA through the de novo pathway, following the successful completion of a multicentre pivotal trial conducted in the USA. With its algorithm-powered technology, BioTrace.IO Lite will be the first software device to provide visualisation of the ablated area based on standard real-time ultrasound imaging.
Presenting real-world population data in patients with pulmonary embolism (PE), John Moriarty (University of California, Los Angeles Medical Center, Los Angeles, USA) demonstrated results from the STRIKE-PE study at this year’s Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark), which, he stated, provides “valuable insight into functional patient outcomes and quality of life measures”, and displays “significant improvements” in generic and disease-specific patient symptoms.
Foregrounding the study for delegates in attendance, Moriarty made clear note that venous thromboembolism (VTE) is “both incredibly common and rising in prevalence” today, exhibiting a graph which depicts its “substantial financial impact” in Europe—nearly €8.5 billion annually—and presents “a morbidity and mortality that ranks as the third highest among all of the cardiovascular disorders”, he explained.
“These trials have been designed to investigate the real-world applicability of computer-aided mechanical aspiration thrombectomy,” Moriarty relayed to delegates, describing their study design which, to date, includes 55 sites and 600 patients. Their interim, 90-day analysis included 87 patients with a mean age of 59.4 years, 59.8% of patients were male and 94.3% have submassive PE. Moriarty added that inclusion criteria specified that patients have a right/left ventricle (RV/LV) ratio of less than 0.9.
Expanding on their primary and secondary endpoints, Moriarty began by making “important” mention of their finding of zero all-cause mortality at 30-days, which he concluded, is “impressive given the background mortality risk in these patients”. Additionally, he noted two major adverse bleeding events within their interim cohort, however reiterated that there were no mortalities.
Of their interim results, Moriarty highlighted that the observed change in the RV/LV ratio was “statistically significant”, and showed a 0.43 or 27.5% decrease. Investigators also saw a decrease in intraprocedural systolic pulmonary artery pressure (sPAP) of 9.4mmHg or 18%. He stated that these results are “similar or better than most of the investigation device trials done on this patient population previously,” concluding that STRIKE-PE to date has provided “valuable insight” into patient functional outcomes and EQ visual analogue scale (EQ VAS), showing “improvements” in quality-of-life measures.
Rendering of HistoSonics treatment head demonstrating histotripsy delivery and targeted destruction of liver tissue
HistoSonics
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark) played host to another FIRST@CIRSE session, which saw first data releases from various interventional radiology trials. Mishal Mendiratta-Lala (University of Michigan, West Bloomfield, USA) presented “much awaited” data from the #HOPE4LIVER trial which demonstrated the “successful, non-invasive destruction” of liver tissue using hepatic histotripsy.
Mendiratta-Lala, providing key background for the study, began by highlighting limitations of locoregional therapies for primary and metastatic hepatic malignancies, including the “degree of invasiveness, inability to treat near clinical structures, lack of real-time visualisation during treatment, collateral damage, and variability in local tumour control”.
“If we had technology which could address these concerns, this could be a major clinical advancement in the treatment of liver tumours,” the presenter averred, then introduced histotripsy—a non-thermal, mechanical process of focused ultrasound through precisely controlled acoustic cavitation.
In order to evaluate the efficacy of histotripsy, Mendiratta-Lala proceeded to describe their prospective, multicentre, single-arm investigational device exemption (IDE) trial, using the HistoSonics System (HistoSonics) for the treatment of liver tumours. Two iterations of the study were carried out, in Europe and the USA respectively, comprised of six European and eight US sites.
Hepatic histotripsy was performed on 44 tumours in the first 40 evaluable subjects enrolled between the two trials, with a primary endpoint of technical success at ≤36 hours post-index procedure, or of 70%, and a primary safety endpoint of no major complications up to 30-days post procedure. The speaker underlined that positive results were required for both primary endpoints for the trial to be considered “successful”.
Of their technical success endpoint, the speaker told CIRSE delegates that “based on the 44 treated tumours, 42 were successfully treated giving us a primary efficacy of 95.5%.” Mendiratta-Lala pointed out that the two tumours that were not successfully treated were due to “user error, not device error”. Concerning their safety endpoint, Mendiratta-Lala explained that the investigators encountered three complications (6.8%), due to the “known risks of focal liver therapies and not unique to histotripsy,” a result which still “[met] the pre-specified performance goal of less than 25%”.
Noting the limitations of their study, Mendiratta-Lala emphasised their “small, heterogeneous patient cohort”, and made clear that the majority of this patient population were recorded to be at an advanced stage of disease, and although their findings “show the effect of histotripsy tissue destruction,” its direct effect on the disease process “was not evaluated”. The presenter concluded however, that both safety and effectiveness endpoints were met in the #HOPE4LIVER trials, “demonstrating successful, non-invasive destruction of liver tissue via histotripsy”.
Presenting data from the MOTIV bioresorbable scaffold (Reva Medical) below-the-knee (BTK) trial during Saturday’s FIRST@CIRSE session at this year’s Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark), Thomas Rand (Klinikum Floridsdorf, Vienna, Austria) underlined the “promising future applications” of the device for the treatment of BTK arteries in patients with rest pain or minor tissue loss due to chronic limb-threatening ischaemia (CLTI), which allowed for “full recovery of vasomotor and endothelial function” at 24-month follow-up, the investigators assert.
Theirs was a prospective, multicentre study, with a total of 58 patients, 60 study limbs and 76 Motiv scaffolds. The study involved patients with lesions in BTK arteries of a maximum of 100mm length, with Rutherford classification scores ranging from four to five. Referencing Chong and fellow presenters in this session, Rand stated that their patient demographics are “more or less the same”, consisting of “many” diabetic patients.
Presenting their updated results, Rand conveyed their “excellent” outcomes, underlining data which show a 2% clinically-driven TLR rate and 95% limb-salvage rate among their patient cohort. Continuing, he reported “high primary patency rates”—81.7% at 24-months—and presented a 98.3% CD-TLR outcome, including a case study to visually bolster these data and display the positive healing results of an individual in their patient population.
“We are very optimistic for the future,” Rand told the CIRSE 2023 audience, concluding that the “excellent tracking and visibility” which has provided them “problem free delivery” and offers demonstrable “[improvements] in Rutherford classification and wound healing”. Finally, Rand made mention of a “new concept” which promotes a “leave nothing behind” best approach, which he stated the Motiv scaffold can facilitate, allowing for “full recovery of vasomotor and endothelial function”.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark) hosted sessions dedicated to radiation protection, contemporary risk management strategies for staff and patients, and challenges faced by interventional radiologists in the developing world. Among key takeaways across Sunday and Monday of the meeting was the assertion that optimisations for radiation mitigation must be implemented universally, although “steps should be taken by national and international institutions” to ensure these needs are met so that radiation exposure no longer represents a deterrent to entering the field of interventional radiology (IR).
Radiation protection for interventional radiologists in developing countries with resource-limited facilities
Presenting in Sunday’s ‘Radiation protection: a worldwide challenge’ session, Gabriel Bartal (Tel Aviv University, Tel Aviv, Israel) began by situating his focus in Africa, where he asserted problems in radiation protection are “most prominent” today. Providing an overview of the current measures in place in these countries, Bartal stated first that “IR has changed clinical medicine worldwide”, however “incorporation of IR methodologies in these countries is much behind where is desired, if at all”.
Aiming to improve conditions, Bartal referenced the International Atomic Energy Agency’s (IAEA) multinational prospective study which surveyed 55 hospitals in 20 low-resource nations, reporting that workloads have doubled in 30% of countries within the last three years. Kerma-area product (KAP) measures were only available in half of the institutions included, and “none” of the surveyed clinicians stated prior experience with its use. To Bartal, these data display the “requirement of more certified interventional radiologists, radiation protection and training”, to meet the “rising” demand for image-guided interventions in African countries.
Addressing strategies to improve radiation protection conditions in Africa, Bartal described a survey conducted by Wilbroad Muhogora (Tanzania Atomic Energy Commission, Arusha, Tanzania) et al, which reported that lead aprons are used in all participating African hospitals. However, only 44% reported the additional use of lead goggles. In concurrence with Muhogora et al’s findings, Bartal reiterated that, although optimisation steps have been taken, challenges faced by interventional radiologists in low-resource settings are “incomparable” to high-income countries, concluding that efforts to implement further safety measures and collect crucial maintenance data must be bolstered by international IR societies.
Meanwhile, he stated that several leading interventional radiologists from North America and Europe are training radiologists from several African countries on site, to safely perform complex interventional procedures. Of his final thoughts, Bartal stated that voluntarily assisting IR training worldwide is “the way to make sure that the patients will undergo minimally invasive procedures without complications and without needing lengthy hospitalization—interventional radiologists are encouraged to join these valuable efforts via www.Road2IR.org”, Bartal concluded.
Does low dose always mean low radiation?
Eliseo Vano (San Carlos University Hospital, Madrid, Spain) gave his presentation in Monday’s session titled ‘Protecting yourself, protecting your staff!’, describing the links between occupational and patient radiation doses in IR, and in what circumstances low dose procedures may involve high exposure for clinicians.
Central to his discussion was the relationship between procedural radiation dose and exposure to the clinician. Vano stated that understandably high patient doses involve a high level of scatter radiation, which inevitably increases occupational exposure. However, in low patient dose procedures—which he noted are “usually the most frequent”—occupational doses may remain high if “protection tools are not used properly”.
To this end, Vano emphasised the importance of communication around radiation protection to the CIRSE audience, which, if compromised, should be “alerted, corrected and discuss[ed] in training sessions”. Furthering his proposal for dose mitigation, the speaker asserted that an audit of occupational doses should be made monthly, referring to a study he led that described the added importance of dose management systems (DMS) when auditing dose more closely over time.
In their study, Vano et al collected data from C-arm dosimeters in five international IR facilities, surveying patient dose indicators, occupation dose values, the ratio between occupational doses, and the doses measured by the reference dosemeter at the C-arm, and the ratio between occupational and patient dose values.
Among the 4,500 procedures and 8,000 records of occupational exposures included within their review, Vano and colleagues note that patient and staff dose data was available for 3,043 procedures, which the investigators positively conclude provides an “advantage”, integrating both staff and patient dose for a clearer outlook on procedural exposure. Finalising his presentation, Vano added that implementation of sensitised alerts should be central to future education programmes for interventional radiologists.
The IR gender gap: Mitigating radiation hazard perception
Opening her presentation, Maureen Kohi (University of North Carolina, Chapel Hill, USA) described a prospective online survey carried out by CIRSE evaluating the gender gap in IR and the barriers facing women trainees specifically. “There is a paucity of women in IR in CIRSE and around the world,” Kohi noted, foregrounding a key and perhaps influential finding from the survey which pointed to women’s concern about radiation, particularly during pregnancy.
However, Kohi made clear that concern over radiation exposure is not singularly attributed to women—referencing a survey carried out by Yarelis Vazquez Perez (University of Maryland, Baltimore, USA) et al, she drew attention to the equal percentage of male and female respondents who rated radiation exposure as a the main deterrent to pursuing a career in IR. “Men are also worried about radiation exposure—it is not unique to the female sex,” Kohi continued, but “as females are the only sex that can be pregnant, it is a big concern during this time”.
“But what do we know about occupational radiation exposure?” Kohi asked the CIRSE 2023 audience, briefly describing the variations that exist in regulations concerning occupational radiation exposure during pregnancy. Currently, in the USA, maximum foetal dose is set at five millisieverts (mSv), although in Europe this limit is 1mSv. “But when you look at more data,” Kohi expands—referencing a study conducted by Stephane Manzo-Silberman (Pitié-Salpêtrière Hospital, Paris, France) and colleagues—“and you look at the dose that would be required to cause [prenatal] effects, we are so beneath that threshold”. To this Kohi emphasised Manzo-Silberman et al’s finding which marked 100mGy of radiation as the occupational dose threshold after which foetal effects were reported.
“The theory exists, but it is virtually not possible,” Kohi averred, to which she reiterated that “radiation exposure should not be a barrier for female or male trainees in becoming interventional radiologists”. Concluding, Kohi underlined that education is needed for female trainees on the safety of prenatal radiation exposure. She stated: “We need to mentor our pregnant female trainees so that they are not afraid—we want these women to continue their career while pregnant.”
Tze Tec Chong (Singapore General Hospital, Singapore) presented results from the PRISTINE registry at this year’s Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark), which aimed to investigate the performance and safety of the Selution SLR (MedAlliance) sirolimus-eluting balloon (SEB) for the treatment of complex occlusive lesions in chronic limb threatening ischaemia (CLTI) patients in Singapore. He highlighted their “[achievement] of technical success” and freedom from device- or procedure-related mortality, which Chong reported were 100% respectively at 12-month follow-up.
First expositing the intentions of the trial to the audience, Chong described the prospective, single-arm, single-centre study, which includes patients with a Ruthford classification between four and six, and TASC II C or D lesions. He defined their primary endpoints as freedom from mortality, major amputation and clinically-driven target lesion revascularisation (CD-TLR), and procedure-related mortality through to 30 days, and to six months.
Detailing patient demographics, Chong then conveyed their collected Wound, Ischemia, and foot Infection (WIfI) classification data which revealed an average score of 4.07 in their population, which, he stated, is indicative of “severe” disease. Additionally, he continued to note that, based on this average, these patients are “at significant risk of amputation” and fall within moderate- to high-risk risk categories.
Of their outcomes, Chong stated that 100% technical success was achieved in all patients, as well as device or procedure-related mortality, although two patients were lost to follow-up. Looking at the data with more granularity, Chong highlighted that amputation-free survival at 12-months was 72.6%, which he asserted is “in line with the type of patients we treat, and quite reasonable in a population that is more than 90% diabetic and 30% with renal failure”. Furthermore, he underlined that complete wound healing was achieved in 79.2% of their population at 12-months.
Concluding his presentation with a case study from the PRISTINE patient cohort, Chong reiterated the key continued patency of the Selution SEB from six to 12 months, noting finally that, “in these difficult to treat vessels, this target lesion primary patency rate is quite acceptable.”
Christoph Binkert (Winterthur, Switzerland) and current president of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) tells Interventional News about the three-fold focus and goals for interventional radiology (IR) in Europe, as defined by the society: clinical care; training and quality standards.
Clinical care requires infrastructure, time, dedicated staff and beds. But the first step, he says, “is to simply talk to your patient before and after the procedure. Everybody can do that.”
Video Attributions
Music: Quirky-tension-investigation-(sleek-sneak)/performed by Apollo Audio/FineTune Music/stock.adobe.com
Raman Uberoi (Oxford, UK), who delivered this year’s Andreas Gruentzig Lecture at the CIRSE annual meeting told Interventional News: “We need to radically think about how we train future generations, [and] how we support interventional radiologists to give them control over their working lives […] to be able to deliver the 24/7 interventional practice that we want to give patients.”
“Now, I believe the way we can do that is to create a specialty of interventional radiology, not just in the UK, but every country throughout the world,” Uberoi exhorts, noting this is “ultimately about improving patient care right around the world,” while noting that globally, two countries (the USA and Japan) have succeeded in obtaining specialty status for interventional radiology (IR).
Video attributions
Music:
Quirky-tension-investigation-(sleek-sneak)/performed by Apollo Audio/FineTune Music/stock.adobe.com
LimFlow, a developer of minimally-invasive technologies for the treatment of chronic limb-threatening ischemia (CLTI), a severe form of peripheral artery disease (PAD), has announced that the US Food and Drug Administration (FDA) has approved the LimFlow system to help people with CLTI who have no other suitable endovascular or surgical treatment options and are facing major amputation.
The LimFlow system for transcatheter arterialization of deep veins (TADV) is designed to re-establish blood flow in deep veins for “no-option” CLTI patients. The therapy is designed to save patients’ legs from major amputation, as limb loss is associated with significant complications, mortality, and deterioration of quality of life. CLTI affects up to four million Americans and disproportionately impacts minority and underserved patients, resulting in more than 150,000 major amputations per year in the US FDA approval of the LimFlow system will enable these patients to have access to a minimally invasive treatment giving them a chance to save their limbs and improve their quality of life.
“With LimFlow, we now have an option for the sickest patients who were previously consigned to limb loss and the downward spiral that accompanies it,” said Daniel Clair (Vanderbilt University Medical Center, Nashville, USA), PROMISE II/III co-principal investigator. “Using this new treatment, we have seen many patients whose limbs have been saved, whose pain has been reduced or resolved, whose chronic wounds are healed or healing, and who can now look forward to happier and more active lives.”
The LimFlow system
FDA approval was based on successful outcomes seen in the PROMISE II pivotal trial, recently published in the New England Journal of Medicine, and from positive clinical results seen in earlier studies. In the PROMISE II study, 76% of no-option CLTI patients were able to keep their leg and experienced progressive wound healing, with many having significant pain relief during the time following LimFlow treatment.
The LimFlow system is the first and only FDA-approved device for TADV and previously received breakthrough device designation from the FDA.
“At LimFlow, our vision is to achieve great outcomes for patients suffering from CLTI. We developed a novel way to make a vein function as an artery with the goal of saving limbs, and by doing that, saving patients’ lives,” said LimFlow CEO Dan Rose. “We thank the FDA for their collaborative review process and we look forward to introducing and expanding use of the LimFlow system in the USA.”
Biotronik has announced the two-year results from the BIOLUX P-III BENELUX all-comers registry, presented by principal investigator Frank Vermassen (Ghent University, Gent, Belgium) at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023 annual meeting (9–13 September, Copenhagen, Denmark).
The prospective, international, multicentre post-market registry evaluated the safety and efficacy of the Passeo-18 Lux drug-coated balloon (DCB) catheter in isolated popliteal artery lesions. This indication is considered a difficult vessel bed to treat due to its biomechanical constraints that usually preclude the placement of stents.
BIOLUX P-III BENELUX registry enrolled 99 patients in Belgium, The Netherlands, and Luxembourg with Rutherford 2–5 disease and at least two centimetres of healthy vessel segment between lesions in the popliteal artery and lesions in the distal superficial femoral artery. All patients were treated with the Passeo-18 Lux DCB. The bail-out stenting rate was 14%.
At 24 months:
Freedom from clinically driven target lesion revascularisation (CD-TLR)2 was 81.6%
Freedom from major target limb amputation was 98.0%
Freedom from all-cause of death was 89.4%
Significant improvement of Rutherford classification was observed for 88.1% of the patients.
“We face a scarcity of data evaluating endovascular therapy for isolated popliteal artery lesions, known as a difficult vessel bed to treat as we don’t want to leave anything behind,” said Vermassen. “It is encouraging to see that we can safely and effectively treat these lesions with a DCB-only approach.”
“Biotronik is proud to be a leader in research of paclitaxel-coated balloons, striving to study device performance in the most challenging anatomy and patient characteristics,” said Stuart Perks, vice president of marketing, vascular intervention at Biotronik. “We repeatedly see the safety and effectiveness of Passeo-18 Lux DCB demonstrated in a diverse range of clinical presentations.”
Sirtex Medical, a leading manufacturer of interventional treatment solutions, has announced the establishment of a collaboration and exclusive worldwide distribution agreement with Magle Group, a Sweden-based contract development and manufacturing organization as well as degradable starch microspheres (DSM) sales and marketing company.
Under the terms of the agreement, Sirtex will exclusively distribute Magle Group’s chemoembolization product, EmboCept S DSM 50μm, in the existing and new geographic areas to support expanded patient access to the product. Together, Sirtex and Magle also intend to establish a joint development plan to increase product range in the field of embolization by utilising Magle Group’s DSM platform.
Indicated for chemoembolization of liver and lung tumours, EmboCept S DSM 50μm is an adjuvant in the intra-arterial treatment of inoperable liver and lung tumours in combination with cytostatic agents. Due to its degradability, EmboCept S can be applied for super-selective treatments of single-liver segments and used for a selective targeting of one liver lobe to treat multifocal, diffuse tumours and non-visible micro tumours.
“We are delighted to team up with Sirtex to unleash the full commercial potential of EmboCept S, our proprietary product for chemoembolization of inoperable liver and lung tumours. Sirtex has a well-established sales force and is also well-equipped to support our continuous efforts to expand Magle Group’s DSM-based product range in the field of embolization,” says Justin Pierce, chief executive officer of Magle Group.
According to the National Institute of Health, liver cancer is the fourth most common cause of death globally, accounting for over 800,000 deaths annually. As of 2020, the World Health Organization found that 2.2 million people are diagnosed and 1.8 million people die from lung cancer yearly. This makes lung cancer responsible for the highest number of cancer-related deaths and the second most common cancer.
“We are thrilled to expand our product portfolio to address unmet needs in liver and lung oncology.” said Kevin R Smith,chief executive officer of Sirtex. “Our partnership with Magle will allow us to continue in our unrelenting pursuit to deliver quality treatments to improve patients’ lives globally.”
EmboCept S DSM 50µm is currently approved for sale in Europe, Argentina, Singapore, and Malaysia.
Achieving consistency, accuracy, and ease of use in interventional radiology (IR) and interventional oncology (IO) procedures, including biopsy and ablation, while limiting procedure time, can present challenges for interventional radiologists. These range from planning interventions across multiple planes without angular limitations and aligning needles to sub-millimetre accuracy, to inserting instruments securely, and all this while aiming to limit the patient and physician’s exposure to radiation.
By taking away the difficulties associated with freehand alignment and targeting, Micromate helps physicians focus on improving reproducibility, speeding up the procedure, reducing radiation dose, and deploying the system even for complex indications.
Micromate tabletop setup
Setup
The system is table-mounted and compact, allowing close-up, full-body patient access from all angles (even inside the gantry). The robot can be mounted to any standard table, with configurable positioning arms, table adapters, and baseplates Setting up, loading DICOM data, and performing automatic registration takes less than five minutes, and when the physician walks into the room after the registration scan, the system is ready for targeting without requiring any additional steps.
Workflow integration
The clinical team need not deviate from their usual workflow, as setup is quick, the learning curve with Micromate is short—around one hour of focused, hands-on training and support on the first couple of days of cases—and there is no need for clinical support specialists to always be present in the room to use the system. Micromate also supports key imaging modalities—cone beam computed tomography (CBCT), fluoroscopy, computed tomography (CT) and CT fluoroscopy. Full ultrasound integration is under development, too.
Micromate
Intraoperative planning
The system allows the physician to rely on updated intraoperative scans for planning purposes. Interventional Systems’ proprietary, intuitive software for accurately planning single or multi-needle interventions without angular limitations.
Alignment
Perform an automatic or joystick-controlled alignment with sub-millimetre accuracy to your planned trajectories within seconds with the help of navigation and live-imaging.
Instrument insertion
Micromate is compatible with all needles from 8 to 21G. The operator can securely advance their instrument of choice under live imaging while keeping haptic feedback. Lateral system deviations to the trajectory during and after instrument insertion are signaled by the system, allowing for correction.
In summary, Micromate decreases user and patient radiation thanks to its live imaging capabilities, navigated alignment, and misalignment detection, and it reduces the need for control scans.
Subscription model supplements Micromate’s procedural advantages
In addition to the advantages Micromate affords the operator in terms of consistency, accuracy, and ease of use, the system also has the benefit of being more affordable than similar robotic planning and navigation devices. This is the case thanks to a subscription option the company offers centres who wish to use Micromate for their percutaneous procedures.
Subscriptions are flexible depending on how many patients the hospital may require the system for, and there is no upfront capital investment or mandatory service agreement. The user instead pays a monthly fee that includes access to free software updates, as well as the robotic platform itself. The monthly service also includes disposable covers and needle guides and specialised onboarding assistance for the initial cases.
In conversation with Pedro Costa
Pedro Costa
Pedro Costa is the CEO of Interventional Systems and he took time to sit down and speak to Interventional News about the company’s origins, vision, product offering, and what he is most looking forward to achieving in the near future in the medical robotics and navigation space with Interventional Systems.
The conversation begins at the beginning of the company, which Costa explains was founded in 2010 by Michael Vogele. It originated from a product Vogele had developed for “patient positioning using moveable tables to get an optimised radiation therapy treatment”, which then became an exploration of whether the patient could “stay still, and you move the therapeutic instruments”—relevant for interventional and surgical procedures, Costa highlights. “And then Interventional Systems was founded.” The company today, he continues, “develops solutions for different applications, and interventional oncology [IO] is one of these”. Endo-urology, cranial neurosurgery and spinal surgery are the other areas that Interventional Systems works or has worked in, Costa informs. “Now we have grown our team and [we are continuing] to look for other surgical areas where we can make a difference—that is it in a nutshell,” he summarises.
One system offering multiple solutions
Costa then seeks to clarify a key aspect of the company’s offering—a miniature robot as opposed to larger systems that solve “the clinical accuracy problem” only. These tend to be repurposed from their original industrial applications and so only provide “incremental” advantages, whereas Interventional Systems’ focus is creating robotic devices “from scratch”, Costa qualifies. The robot—Micromate—can be used “with any image device”, and is “simple, affordable” and allows for “fast training”.
Homing in on affordability, Costa next addresses what it is about the Interventional Systems offering that ensures this for customers. Hospitals rarely get reimbursed for the use of robotic systems, he explains. Therefore the focus is on proving that the cost of investment will be offset by the advantages the robot will bring, such as procedural accuracy and reduced radiation exposure. “So, for us, it is all about the quadruple aim of providing less expensive care […] by controlling the whole supply chain so that we are still able to keep viable margins, while [offering a good price].” Costa relays how surgical robots can cost up to €1 million, but Interventional Systems’ is around €200,000 and “our price per procedure is less than €200”. He goes on to underline a key feature of the company’s offering: the subscription model. “Those hospitals that cannot buy a system upfront, they are able to subscribe and pay a monthly fee […] Patients can then be treated using the technology without the need for a huge investment by hospitals.”
Practicality is another factor that Interventional Systems has considered, Costa proceeds, in terms of greater usability for staff, but also a better patient experience. “We have been able to prove […] that with two days’ training (that include already initial cases on patients) you should be ready to fly solo.” He adds that starting with using the robot for simple cases lends itself to gradually moving on to using it for more complex cases, to the point where all cases become “routine”. Moreover, from a patient point of view, Costa adds, the patient spends less time under anaesthesia when anaesthesia is used, and less time—almost half of what it would be without the system—in the operating theatre overall. Radiation exposure can be reduced as a result by “close to half”, he celebrates. All this offsets the cost of the robot, according to Costa, “and it is better for everybody”.
Cultivating ‘centres of excellence’
Interventional Systems has a scheme whereby they partner with the hospitals that use Micromate, “rather than just [being] a supplier”. The relationship with the hospital is ongoing, Costa details, and there is a cloud-based ‘academy’ environment though which staff can access “everything from case reports to training, to narrated cases and videos from other physicians”. Users can also store information on the platform, Costa elaborates, and share tips or presentations with the rest of the user community. “Everyone can crosspollinate and learn from each other” while going through “sequential steps to learn and train with the technology”. There is also the capability of contacting the Interventional Systems team with queries, Costa supplements further. “It is a way for us to provide continuous training and value without being there and it is available 24/7.”
Beyond this, Costa goes on, is the idea of having a “symbiotic partnership” with around a dozen interventional radiology/ endo-urology departments, which will gain the title of ‘centre of excellence’ in return. “We understand that for IR and interventional oncology [IO], there is no silver bullet, you cannot say ‘this robot will solve all problems’,” Costa avers, but he emphasises the value robotics can bring, and especially in cooperation with interventional radiologists. This is because the technology is designed to solve the most pressing of the “thousands” of problems within IR, “with different organs, needles, and in different procedures”. For the ‘centres of excellence’, Costa conveys how the company absorbs a proportion of the installation costs for Micromate in return for the interventional radiologists in those centres “giving back to the community by sharing their experiences”, including study results. This will help other physicians, and also the company, in terms of shedding light on “which areas to focus on [developing] and which not” going forward.
What the future holds
Costa turns to reflect on the “year-on-year growth in terms of users” that Interventional Systems has seen, including outside Europe and the USA, which indicates “interest in the technology” and, as Costa sees it, “that robotics is here to stay”. He refers to the expansion of the navigation technology market outside robotics too, pointing out that this market competition will “enable” the continued growth of the company, to the benefit of interventional radiologists.
Micromate offers “[definite] added benefit” according to user of 13 years
Marco van Strijen
Marco van Strijen is an early adopter of Micromate (Interventional Systems), having used the robotic assistance system for over a decade at St Antonius Ziekenhuis (Nieuwegein, The Netherlands). At the 2023 European Conference on Interventional Oncology (ECIO; 16–19 April, Stockholm, Sweden), Van Strijen delivered a symposium to discuss why he uses Micromate in his specialist non-vascular intervention and interventional oncology practice. Among the features that set the technology apart when it comes to planning and executing needle placement for his procedures, Van Strijen highlighted its multimodality compatibility, how it compares to freehand needle introduction, and its proven clinical performance for ablation and biopsy.
Van Strijen began his presentation by outlining the “challenges [we have] as interventional oncologists,” which include patients moving if they are not under general anaesthesia, moving anatomy as the patient breathes and their heart beats. Another challenge is when one has to resort to “steep approaches to avoid critical structures in the thoracic cavity,” Van Strijen noted, and “the difficulty of trying to enter oblique planes during bone interventions, where the needle can easily slip off the intended path”.
The advantages Micromate affords
With these obstacles to overcome, Van Strijen described the benefits robotic assistance can afford those in his line of work as it “improves the accuracy and reproducibility of every single needle intervention we perform”. He added that robotic systems such as Micromate are “also very helpful in reducing human error and the learning curve time [and…] robotics can help speed up procedures, thus potentially limiting complications”. Speeding up the procedures also involves reducing the radiation dose for the operator, according to the speaker. “We are now capable of expanding our interventions [to lesions and indications] considered too complex or too distant.”
Next, Van Strijen homed in on how Micromate lends itself well to specific types of cases. “I do a lot of lung biopsies,” he informed delegates, going on to describe how this requires him to navigate the “challenge of moving anatomy on breathing”. However, Micromate helps him overcome this issue, offering a “proper fix of the needle [independent of the patient for] a very stable and safe approach”. As a clinical example of complexity and stability, the case of using Micromate in biopsying a periorbital mass was demonstrated as “very easy to perform without damaging any of the critical structures close by”, and likewise, kidney cryoablation with “up to five needles” is “never really a problem,” Van Strijen shared. Thanks to Micromate, it is possible “to manoeuvre in between complex anatomy, and in my hospital, we have had a decrease in mortality over the past three years,” the speaker celebrated.
Micromate’s proven clinical performance
The presenter followed this up by addressing his centre’s clinical results with Micromate for biopsy in the initial computed tomography (CT)-guided environment. The study included seven biopsies (of the lung, spleen, and pelvic bone), and had a 100% diagnostic yield, meaning all biopsies were correctly sampled and histological diagnosis achieved, and there was one small bleeding complication unrelated to the robot. “On average we only used two to three scans per patient”, and Van Strijen also pointed out that the average radiation exposure per procedure was “very low”. More extensive study results were presented with the analysis of the prospective last 149 procedures performed with cone beam computed tomography (CBCT) needle guidance. These were compared to the results dating back 10 years from the same hospital and showed a significant decrease in procedure time (12:15m vs. 28:30m), reduction of radiation dose (6.73 mSv vs. 12.7 mSv) and an increase in diagnostic yield (96% vs. 91.4%). These results were consistent even in more complex procedures. Van Strijen also noted that comparable results were found in ablation procedures with Micromate, pointing to the fact that “as complexity increases, Micromate’s performance stays high”. Micromate allows for a lower radiation exposure, faster procedures, and equivalent or better diagnostic yields. Procedure time is 50% less than freehand and radiation exposure is not linked to how complex a case is but instead, individual patient anatomy or requirements of the case.
Regarding the complication analysis for biopsy, “the complication rate was in line with the literature despite an increase in average case complexity”. Of the 144 cases analysed, there were 13 pneumothoraces, Van Strijen highlighted, only three of which required chest tube drainage. Most of the complications occurred in lung cases—there were two soft tissue bleeds which could be treated locally, the speaker continued. The bone cases saw no complications, he added, and none of the total complications were linked to the use of the robot.
One system for multiple modalities
Van Strijen has used Micromate for CT and CBCT, and informed his audience that the main differences between CT and CBCT lie in the fact that after acquisition and planning, the C-arm angulation with CBCT is automated, whereas the gross positioning is manual for CT. Moreover, in the CBCT environment, needle placement uses fluoroscopy, whereas it is fully automatic for CT, involving no further radiation.
In conclusion, Van Strijen stated that they “definitely see added benefit [using Micromate including] in challenging cases, such as endoleak, trigeminal ablation, complex drainages, and bone interventions”. Additional benefits of using Micromate, Van Strijen reiterated, are its short learning curve, the device’s stability and accuracy, the shorter procedure time, and the reduction in radiation exposure that it affords. Finally, it is a multimodality solution, compatible with CT, CBCT, and fluoroscopy.
“This robot has helped us expand our limits”
Dimitrios Filippiadis
Dimitrios Filippiadis is associate professor of diagnostic and interventional radiology (IR) at the National and Kapodistrian University of Athens (Athens, Greece), whose practice centres around musculoskeletal (MSK) interventions and diagnostics, and interventional oncology (IO) and cancer pain management. He has been using the Micromate robotic navigation system (Interventional Systems) in the computed tomography (CT) suite since November 2022, and predominantly for biopsies, neurolyses, and ablation procedures.
What benefits come with utilising navigation and robotics in IR procedures? How do you envision the future of these technologies?
Navigation and robotics can be utilised to increase excellence and “repeatability” in performing percutaneous or vascular procedures. For example, in ablation, technologies can significantly impact ablation standardisation for the better, providing invaluable services to simulation, performance, and verification of success. The greatest advantage of utilising such systems is the potential to reduce duration and ionising radiation exposure during the procedure and, at the same time, increase the accuracy of a specific therapeutic approach. However, navigation systems and robotics for IR procedures are not a panacea, are not a solution or remedy for all difficulties and they should not substitute clinical judgement. They should be used as tools for providing a patient with a better and more reliable clinical care. I hope and feel that soon, these systems will be invaluable tools assisting all operators in implementing his or her clinical thought and judgement in practice. For this to happen, a complete system giving answers to all practical steps of a procedure is necessary.
What will the role of robotics be in medical students’ education and in training new doctors?
A cryoablation case with Micromate
While the utilisation of robotics is rapidly growing in everyday clinical practice, it is a fact that medical students and residents still have limited experience and familiarity with them. As robotic procedures are becoming more widespread, early exposure to their applications for medical students and residents could be an integral part of training, helping them to have more meaningful observation experience and allowing them to recognise the significance of utilising such technologies in everyday clinical practice. However, before anything else, to enhance engagement of medical students and residents with robotics, inclusion of their application in the current curricula is a prerequisite. Once this is achieved, educators will be able to consider hands-on and other simulation programmes for medical students and residents aiming to shift training in robotics to earlier during IR and other specialty/subspecialty training.
Can you discuss the current limitations or challenges associated with gaining funding for robotic/navigation technologies? How does their cost impact accessibility and widespread adoption?
It goes without saying that the current limitation of these systems is the challenge of acquiring one of them due to funding limitations, thus hindering widespread adoption and utilisation. Vendors could start reaching out to users with more flexible and less rigid financial proposals before the discussion for reimbursing navigation systems and robotics in IR procedures has properly begins. Finally, there is a need for developing a system which will contribute ease of use, reliability and repeatability in all the steps of a procedure starting from simulation to performance (through navigation) and verification of success.
What procedures have you performed with Micromate? Any interesting cases you would like to share?
The greatest advantage of Micromate is that it can be used for all kinds of percutaneous procedures. After the initial learning curve, which I have to say is quite short, mainly because the robot is extremely user-friendly and easy to master, we started using it for all the cases during which multiple apparatuses or inclined approaches are necessary. I would not want to focus on a specific interesting case. I would rather say that the utilisation of this robot has helped us expand our limits and treat lesions in extremely challenging locations during a technically easier, shorter, and more cost-efficient session.
“This crucial [planning] step of the ablation is simplified”
Alexander Kupferthaler
Alexander Kupferthaler is an interventional radiologist at the Ordensklinikum Linz (Linz, Austria) whose work is predominantly interventional oncology (IO)-based. He carried out the first computed tomography (CT)-guided liver ablation with Micromate (Interventional Systems), and beyond this, has used the system for a range of biopsies and kidney cryoablation. Kupferthaler has also used Micromate with cone beam (CB) CT and talks through his experience.
I understand you have experience using Micromate for microwave ablation of the liver. How long have you been doing this procedure? Do you use Micromate for any other procedures?
As I work in an cancer centre hospital, IO has played a major role since I started interventional radiology (IR). So, for as long as I can remember, I have done microwave ablation procedures.
I started using ultrasound guidance when placing the probes, then for the more complicated ablations, I used the previous model of the Micromate robot with CBCT guidance and image-fusion when needed. When Interventional Systems showcased their new Micromate CT-guided workflow I was quite fascinated.
I have used the Micromate system for complicated lung biopsies, bone and soft-tissue biopsies, coeliac trunk blockades, osteoid-osteoma radiofrequency ablations, and kidney cryoablations.
How does doing microwave liver ablation differ with CT vs. CBCT guidance? How does Micromate help with the challenges that each of these means of carrying out ablations present?
The major difference between the two modalities is the image quality. CT scanners typically offer higher spatial resolution, larger coverage of the imaged volume, while reducing noise and image artifacts. This offers better visualisation of the tumour, nearby blood vessels, and critical structures, while reducing the risk of complications and providing a faster workflow. And while I do prefer the Micromate CT-based navigation workflow, time for interventional procedures in the CT suite is restricted. So, whenever safe and feasible for the patient, I also use the Micromate robot in the interventional suite.
For the Micromate CT-guided workflow, Interventional Systems has developed a complete solution that assists especially in angled trajectories and complicated-to-reach lesions. Doing out-of-plane trajectories in CT is challenging. With the easy-to-use user interface of the Micromate system, this crucial step of the ablation procedure is simplified. When the planning is done, positioning the robot and placing the needles or probes is quick and straightforward.
1. In liver segments V&VI there is a hypervascular lesion 2.7cm in size. Note the fiducials of the robot on the right side of the patient. 2. Out-of-plane trajectory of the microwave antenna. Contour of the robot on the top right side. 3. Final ablation zone in contrast-enhanced CT after the intervention. 4. Micromate setup for the liver ablation case.
What is the significance of the Interventional Systems armrest when doing liver ablations?
Patient positioning is the key to success in liver ablations. Most of the time, the patient is lying in a supine position on the CT table. If the arm is then positioned next to the body in an adducted position, the treatment area is limited. Thus, placing the arm on the armrest will increase the treatment area. Additionally, the armrest provides stability, prevents unwanted movement and reduces strain on the patient’s arm and shoulder muscles.
Would you be able to share some images from a liver ablation case you found particularly memorable?
I can, actually. See the images here and their descriptions, as well as a photo of the Micromate setup.
The Society for Vascular Surgery (SVS), American Venous Forum (AVF), and American Vein and Lymphatic Society (AVLS) have released the second and final part of new guidelines for the management of varicose veins of the lower extremities. The recommendations, which update the 2011 SVS and AVF guidance on the topic, were published online ahead of print in the Journal of Vascular Surgery: Venous and Lymphatic Disorders (JVS-VL).
The new document focusses on the following topics:
Evidence supporting the prevention and management of varicose vein patients with compression
Treatment with drugs and nutritional supplements
Evaluation and treatment of varicose tributaries
Superficial venous aneurysms
The management of complications of varicose veins and their treatment
The publication—authored by Peter Gloviczki (Mayo Clinic, Rochester, USA) and 19 other members of a multispecialty guideline writing committee—follows last year’s release of part one of the guidelines, which addressed duplex scanning and treatment of superficial truncal reflux.
Gloviczki and colleagues outline in their introduction the reason behind the two-part publication of the updated guidelines. They note that all recommendations in part one were based on a new, independent systematic review and meta-analysis that “provided the latest scientific evidence to support updated or completely new guidelines on evaluation with duplex scanning and on the management of superficial truncal reflux in patients with varicose veins”. However, the authors recognised “several additional important clinical issues” needed to be addressed, despite many having varying levels of scientific evidence associated with them. For this reason, when a systematic review was not available, the writing committee based ungraded statements on a comprehensive review of the literature, combined with unanimous consensus of the expert panel.
Alongside a series of recommendations, the writing committee highlight “several” knowledge gaps on the natural history, evaluation, prevention and treatment of patients with varicose veins, highlighting their top 20 recommendations for future research. The most important three they identify are comparative studies of polidocanol endovenous micro-foam versus physician-compounded foam for treatment of varicose tributaries, comparative studies of polidocanol endovenous micro-foam versus other techniques of thermal and non-thermal ablation of incompetent superficial truncal veins, and best metric of axial reflux to determine ablation of superficial truncal veins.
Delcath Systems, an interventional oncology company focused on the treatment of primary and metastatic cancers of the liver, has announced that it raised approximately US$35 million through the exercise of all the Tranche A warrants issued as part the previously announced March 29, 2023 private investment in public equity (PIPE) financing.
The warrants were exercisable until the earlier of March 3, 2026 or 21 days after the US Food and Drug Administration (FDA) approval of the Hepzato Kit (melphalan) for injection/hepatic delivery system, which occurred on August 14, 2023. Tranche B warrants, also issued as part of the PIPE financing, could generate approximately US$25 million in additional proceeds and are also exercisable until the earlier of March 3, 2026 or 21 days following the Company’s public announcement of recording at least US$10 million in quarterly US revenue from the commercialisation of Hepzato.
The FDA approval and additional financing triggers an extension of the interest-only period from September 30, 2023, to December 31, 2023, for an existing loan agreement with Avenue Venture Opportunities Fund.
“With the exercise of these warrants we have, as planned, accessed adequate capital to fund the commercial launch of Hepzato Kit without adding to our fully diluted share count,” said Gerard Michel, Delcath’s chief executive officer. Michel continued: “We can now focus on providing access to Hepzato Kit to uveal melanoma patients as well as expanding our development efforts to treat other liver dominant cancers.”
The company plans to have commercial product available for uveal melanoma patients by the end of 2023. Until that time patients will continue to be enrolled and treated at expanded access program (EAP) sites.
Interventional News’ most popular stories from August include a commentary on intra-arterial approaches to advanced pancreatic cancer; perspectives on 25 years of day-case IR in the UK; study results concerning high-dose dexamethasone for post-embolization syndrome in PAE; and a window into IR training in the USA offering insights into contemporary experiences within the speciality.
When utilised as a first-line technique for medium vessel occlusion (MeVO) stroke, aspiration and stent-retriever thrombectomy have demonstrated “no significant difference” in imaging-related or clinical outcomes. That is according to a multicentre, propensity score-matched analysis including more than 400 patients, the results of which have been published in the journal Stroke: Vascular and Interventional Neurology.
Alucent Biomedical has announced that the US Food and Drug Administration (FDA) granted an investigational device exemption (IDE) for a US clinical study of AlucentNVS, a unique light-activated, drug-coated balloon catheter technology.
Ripal Gandhi provides commentary on approaches to treating hypovascular tumours and contemporary investigations in trans-arterial micro-perfusion (TAMP). Early studies of TAMP using gemcitabine chemotherapy in patients with locally advanced pancreatic cancer (LAPC), has shown the approach to be safe with no obvious local toxicity.
AngioDynamics announces the completion of enrolment and final treatment in its pivotal study of the NanoKnife system for ablation of prostate tissue in an intermediate-risk patient population (PRESERVE).
Authors from King’s College Hospital (London, UK) publish a letter in Clinical Radiology detailing their centre’s experience after 25 years of day-case interventional radiology (IR) services, advocating that the model “[enables] rapid recovery, [expediting] ambulation and [promoting] same-day discharge”.
In 2010, the UK Royal College of Radiologists (RCR) with the Royal College of Paediatrics and Child Health (RCPCH) published a report focused on how to improve paediatric interventional radiology (PIR) services. In June 2023, an updated report was published to “identify how PIR services can be expanded and improved” and “suggest solutions” that can be enacted by commissioners, healthcare leaders and hospitals.
Petra Svarc (Rigshospitalet, Copenhagen, Denmark) presented her group’s findings during the scientific paper session at the European Conference on Embolotherapy (ET; 21–24 June, Valencia, Spain). They found that high-dose dexamethasone is ineffective in reducing the symptoms of post-embolization syndrome in patients who have undergone prostate artery embolization (PAE).
Ayman Al Sibaie, a consultant interventional radiologist at Rashid Hospital (Dubai, UAE) speaks to Interventional News to delve into his practice in Dubai, to get his take on how interventional radiology (IR) practice varies between the Middle East-North African (MENA) region and the Western world, and his perspective on PAIRS’ work, having been president for the past four years.
Oluwatoyin (Toyin) Dada is a current fifth-year postgraduate trainee (resident) in interventional radiology (IR) and diagnostic radiology (DR), and Ariana Mills, a first-year resident at the Icahn School of Medicine at Mount Sinai (New York City, USA) answer questions about their journeys into IR from their US perspective.
“The median thrombus age of DVT patients treated in our centre is 14 days – says Dr Andrew Wigham from Oxford University Hospitals. – We know that traditional treatment options such as thrombolytics and other thrombectomy devices are less effective once thrombus is more organised. When using the ClotTriever System, we are able to treat those patients effectively”.
Along with the benefits of being able to treat the full chronicity of DVT, dr Wigham highlights a single-session treatment, lytic-free approach and minimising the hospital length of stay for patients, as the additional advantages of the ClotTriever system.
“We treat more and more young patients with DVT and the fact that we can offer a lytic-free treatment and eliminate bleeding risks related to thrombolytics, makes a huge difference – says dr Wigham.
Access to the interventional treatment for eligible DVT patients, remains still a challenge due to the lack of awareness, both among referring and treating physicians, of the effective clot removal from the iliac veins. “There are still many patients receiving thrombolysis and although their symptoms are not improving, they don’t get any interventions – says dr Wigham. – Building dedicated DVT pathways is a crucial task to make sure that the patients receive the right treatment.
To learn more about the ClotTriever system, join the INARI Symposium at CIRSE 2023 where Dr Andrew Wigham and other experts will be discussing a lytic-free thrombectomy as the first choice for both DVT and acute PE (FlowTriever) treatment on Sunday 10th September at 1pm (Auditotium 15).
This video was filmed by Inari Medical and is being sponsored for distribution in association with Vascular News, Interventional News, Venous News and CX Vascular. Biba Medical bears no responsibility for the assets used in the production of this video.
The incidence of lung cancer has increased considerably in the last few decades with the lung as the most common site of metastatic involvement. Despite the improvements in the diagnosis and treatment for malignant lung tumours, the prognosis of the patients is still unsatisfactory.1 Currently, locoregional chemotherapeutic techniques such as transpulmonary chemoembolization (TPCE) for the treatment of lung malignancies have gained increasing importance. The purpose of this retrospective study was to evaluate local tumour response and patient survival after the treatment of pulmonary metastases using TPCE as a palliative treatment method.
Thomas Vogl
In TPCE, a 5 French (Fr) endovascular sheath and 5Fr headhunter catheter are routinely placed transfemorally under fluoroscopy until the pulmonary artery and subsequently the tumour-feeding segmental pulmonary branch are reached. A balloon catheter (up to 7mm in diameter) is optionally placed for better results.2 This selective pulmonary artery catheterisation results in a blockage of the arterial supply to the tumour tissue, resulting in regional ischaemic necrosis in the target tumour tissues while reducing damage to the surrounding normal lung parenchyma. Thereafter, mitomycin and gemcitabine as chemotherapeutic agents are administered in combination with an embolization of lipiodol and microspheres. This extends the storage time of the injected cytostatics in the tumours and reduces the outflow into the circulatory system.3 Consequently, the frequency and severity of systemic effects are limited. Other occlusion materials used are coils, polyvinyl alcohol, degradable starch microspheres, and gelatin sponges.
In our study, 223 patients (138 women, 85 men; mean age: 59.3±11.9 years) with unresectable lung metastases and/or not responding to systemic chemotherapy received repetitive TPCE (mean number of sessions 4.7±3.7) between January 1990 and May 2021. Patients had predominant lung metastases and in most cases with bilateral lung involvement. Origin of the metastases were either colorectal carcinoma (n=139) or breast cancer (n=84). Tumour-supplying vessels were catheterised selectively in order to apply chemotherapeutic agents locally, combined with lipiodol and microspheres. The response was assessed according to the revised RECIST criteria.
Of the evaluated 183 cases, partial response was achieved in 4.9% (n=9), stable disease in 62.3% (n=114), and progressive disease in 32.8% (n=60) of the patients. Mean and median overall survival time were 23.5 and 14 months, respectively.
TPCE can be used as a palliative treatment in unresectable lung malignancies to reduce the tumour burden or to achieve local tumour control,4 or as a neoadjuvant or curative treatment option combined with thermal ablation such as radiofrequency ablation (RFA) and microwave ablation (MWA) (Figure 1).5,6
1a: Axial CT diagnosis with documentation of two colorectal carcinoma lung metastases (T3N0M1) in the right middle and upper lung field with 13mm and 18mm in diameter (arrows). Post-inflammatory subpleural lesion on the left.1b: Transpulmonary chemoembolization (TPCE) via a transpulmonary-arterial catheter into the right pulmonary artery supplying the middle lobe. Injection of perfusion using mitomycin, cisplatin, irinotecan. Embolization was performed using Embocept (PharmaCept).1c: Partial response with massive volume reduction of the intrapulmonary lesions. Here the size of lesions remained constant over a total of six months (arrows).
A multicentre study may include a larger population of patients and combine expertise from different institutes. Although TPCE has the potential to improve local tumour control and to prolong survival, randomised controlled trials are still needed.
Thomas Vogl is director of the Institute for Diagnostic and Interventional Radiology at University Hospital Frankfurt (Frankfurt, Germany).
Disclosures: The author shared no relevant disclosures
References:
Lemjabbar-Alaoui H, Hassan OU, Yang Y-W et al. Lung cancer: Biology and treatment options. Biochim Biophys Acta 2015; 1856: 189-210.
Vogl, TJ, Herzog C, Zangos S, Lindemayr S. Transpulmonale Chemoembolisation (TPCE) als palliatives Behandlungskonzept bei primären Lungentumoren. Fortschr Rçntgenstr 2007; 179: 300-307
Vogl TJ, Mekkawy AIA, Thabet DB, et al. Transvenous pulmonary chemoembolization (TPCE) for palliative or neoadjuvant treatment of lung metastases. Eur Radiol 2019, 29: 1939-1949
Vogl TJ, Shafinaderi M, Zangos S et al. Regional chemotherapy of the lung: transpulmonary chemoembolization in malignant lung tumors. Semin Interven Radiol 2013; 30: 176-184
Smith SL, Jennings PE. Lung radiofrequency and microwave ablation: A review of indications, techniques and post-procedural imaging appearances. Br J Radiol 2015; 88, 20140598
Vogl TJ, Hammann L, Adwan H. Transvenous Pulmonary Chemoembolization and Optional Microwave Ablation for Colorectal Lung Metastases. J Clin Med 2023; 12(10):3394
In February 2023, the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), in conjunction with the European Union of Medical Specialists (UEMS) Interventional Radiology (IR) division, published a new curriculum and syllabus, an update to the previous version released five years prior. According to the CIRSE website, the society provides interventional radiologists with the curriculum and syllabus so they have access to “a standardised IR training guideline that covers the breadth of clinical and technical skills that are needed to perform safe and effective treatments”.
Left to right: Maria Weren, Mick Lee, Raman Uberoi,
Different countries have different requirements when it comes to declaring interventional radiologists ‘qualified’, and therefore, there can be variation in knowledge and skill bases from one country to another. However, CIRSE’s European Board of Interventional Radiology (EBIR) qualification is one example of a “voluntary and supplemental” certification that has widespread recognition, and is designed to demonstrate holders’ commitment to, and competency in IR. The updated European Curriculum and Syllabus for Interventional Radiology “serves as the framework for the EBIR examination” and is the basis for the ‘blueprint’ used to create examination questions.
In December 2021, CIRSE created a task force for updating the curriculum, which the website states is “the most comprehensive” of all available IR curricula. Between then and February this year, chairperson Raman Uberoi (Oxford University Hospitals, Oxford, UK) and 17 international task force members have adapted the latest version. Mick Lee (University of Medicine and Health Sciences, Royal College of Surgeons, Dublin, Ireland), who led the European Training Requirements (ETR) group, also succeeded in getting the new version included among the European Training Requirements (ETR) at the UEMS. They did this by rewriting large sections of the document to reflect the advancements in IR that have occurred in the last five years, as well as the new quality standards necessary for modern IR training.
Curriculum task force chairperson on the updates
Speaking to Interventional News, Uberoi provided insight into the importance of the syllabus—“in 2006, the CIRSE board recognised the need to standardise IR training and assessment across Europe so that patients get the best treatments possible regardless of geography by well trained IR clinicians. In other words, this means that no matter where future young IR trainees practice, they would achieve the same fundamental competencies.” He went on to explain that this led to the first European curriculum being published in 2013, with this latest edition the third iteration. In Uberoi’s words, “it sets out the objectives, learning methods, outcomes, supervision and assessment of IR training, forming the basis of the syllabus used to blueprint the EBIR (European Board of Interventional Radiology) examination, a high-level professional global examination of IR competence”. There are now almost 1,500 EBIR holders across the world, he added.
What has changed in this version?
When asked about the major changes from the last version of the curriculum, Uberoi clarified that the amendments and additions as a whole “[ensures] that IR education continues to adapt to the changing environment, work practices and needs of current and future interventional radiologists”. Specifically, the changes include a “greater emphasis on clinical responsibility and training requirements for new procedures,” a more “streamlined format”, and creation of four chapters dedicated to interventional oncology (IO). Uberoi also mentioned that the curriculum specifies the level trainees must have reached in core competencies by different points in their training. Regarding regulatory bodies, the chairperson noted that the curriculum reflects what national IR accreditation boards expect of their interventional radiologists, in addition to the UEMS.
The curriculum goes beyond requirements for trainees, it also sets out the requirements for trainers and training centres too, Uberoi continued, “to ensure that trainers are appropriately qualified to train and that training centres have the right infrastructure to support training”. An example of these requirements is that, depending on the centre, trainees may need to rotate between hospitals to gain sufficient exposure to, and practice in, different procedures.
Finally, Uberoi touched on how the curriculum pertains to EBIR examinations, “the traffic light system has also been updated to make it easier for candidates to focus on the most commonly assessed areas of IR practice” when preparing for assessment. “The objective is always to improve the training and quality of interventional radiologists in Europe and globally, and ultimately patient outcomes and care,” Uberoi concluded.
The importance of inclusion in the ETR
As referred to above, being included in the ETR is a significant achievement. The stringent requirements are set out by the body responsible for standardising medical training across European countries: the UEMS. Recognition by the UEMS represents a “strong recommendation for national medical authorities all over Europe” to adopt these requirements and the corresponding assessment for national IR training pathways. This will increase the likelihood that interventional radiologists in different countries, at least in Europe, will have harmonised training and achieve common standards and competencies, leading to greater uniformity in IR care provisions across the continent.
Lee, the aforementioned leader of the group dedicated to achieving this milestone, and president of the UEMS’s IR division, weighed in on why UEMS endorsement matters: “For the first time, the Division of IR of the UEMS Radiology section and CIRSE collaborated to produce this third edition of the curriculum and syllabus. The IR curriculum underwent a rigorous appraisal by all of the other UEMS medical specialties and was eventually approved by the UEMS Council in October 2022 with universal support. This is a landmark achievement for European IR and potentially a potent mechanism for achieving the necessary resources to structure and run competent IR training programmes across Europe.”
The longer-term impact?
Asked to elaborate on the mid- to long-term impact of the UEMS approval, Lee opined that with “this IR training curriculum, and with competency assessment through the EBIR, patients will be treated safely and effectively throughout Europe, and perhaps, in the fullness of time, the putative goal of harmonisation of training across Europe, and the free movement of IR professionals across borders, will become a reality”.
Like Uberoi, Lee emphasised the significance of the curriculum including the resources and requirements for trainers and training institutions, as this has not been done in previous versions. This will enable “robust training”, he added, the product of which will be “doctors who are fit for purpose”. Moreover, Lee underlined how important it is that the curriculum and UEMS endorsement break new ground—“it is another step on the road for interventional radiologists in forging their own destiny”.
Benefits of multilingual curriculum and syllabus “manifold”
Maria Weren, head of certification and accreditation at CIRSE, added her voice to the discussion on the latest curriculum update. She began by outlining how this comprehensive training programme consisting of a curriculum, an examination, an article and structured learning resources can be “easily, fully or partially, adopted by, or integrated into, national training and certification pathways, which will push clinical services in IR and support the further development of IR as an established and growing medical field”. The ultimate goal off the back of this is that, with more trained practitioners, more patients can access IR services, she expanded. Regarding access to the curriculum itself, Weren averred that there are plans to publish it in additional languages, “not least because the [EBIR] examination is offered in German and Spanish through collaboration with national IR societies”.
Probed as to the potential global reach of a multilingual curriculum and EBIR, Weren set out benefits to interventional radiologists in and outside of Europe using them. “All areas of the broad medical field are covered, [meaning] an interventional radiologist [can] expand their general IR knowledge and have this excellent knowledge base attested to through EBIR certification. Widespread recognition also allows greater job mobility and can be a real career boost for young doctors. In countries like Switzerland or Germany, the qualification has found its way into hospital accreditation, which means it is a prerequisite for centres to employ certified interventional radiologists.”
Supplementing this, Weren mentioned that EBIR diploma holders “can also gain advanced certification in the field of endovascular therapy, as CIRSE also offers the European Certification for Endovascular Specialists”. She explained that this is a documented-experience certification that aims to further recognition of interventional radiologists as experts in minimally invasive and image-guided endovascular treatment.
Weren’s final note summarises the importance of the new curriculum and syllabus and its endorsement by over 40 national IR societies, within and outside Europe, “whose common goal is to strengthen IR and help many patients with its minimally invasive therapy options”.
Ayman Al Sibaie is a consultant interventional radiologist currently working at Rashid Hospital (Dubai, UAE), and has been the president of the Pan Arab Interventional Radiology Society (PAIRS) since 2019. Interventional News interviewed him to delve into his practice in Dubai, to get his take on how interventional radiology (IR) practice varies between the Middle East-North African (MENA) region and the Western world, and his perspective on PAIRS’ work, having been president for the past four years.
IN: Would you be able to provide some insight into your background and IR training?
I am originally Syrian and have German nationality. I studied medicine in Germany and graduated from Friedrich Schiller University Medical School (Jena, Germany) in 1992. Then I did my radiology residency in the same university hospital and finished my postgraduate studies in 1997. I have been in love with IR since the very beginning and I worked as an interventional radiologist in many German cities like Jena and Gera before becoming a consultant of IR in 1998. In 2005, I decided to go to Dubai to start a new career there.
IN: How was it starting a new IR career in Dubai?
It was far from an easy ride. When I first came to Dubai there was nothing—IR was rather a new specialty so I had to start from scratch. The infrastructure was good and the hospital authorities were willing to do anything to help the patients, however I had to talk to companies from my connections in Germany to get the tools. I then started recruiting residents who could help me with cases, and talking to doctors from other specialties to send patients. Fortunately, after 18 years, I can definitely say we have a practice in Dubai that is not at all inferior to those in Europe and the USA.
IN: What is your special interest within IR?
Practising IR in the MENA region requires you to cover a wide spectrum of procedures. For example, the hospital I work in is a trauma centre—one of the biggest emergency and trauma centres in the Middle East—that has different specialties like neuro and vascular, and I am the only IR consultant. This means I have to cover almost all IR procedures, including for aneurysms, arteriovenous malformations, stroke, the aorta, critical limb ischaemia, pulmonary embolism and deep vein thrombosis. Also emergency embolization for bronchial, gastrointestinal bleeds, and renal, as well as elective embolization for uterine fibroids, prostate, and varicose vein management.
IN: What are the key differences in IR practice between the MENA region and Europe?
There are substantial differences on many levels. For example, the regulations are much more flexible in our region, allowing us to use a wide range of supplies from all over the world. There is a lot of variation in diseases in my region due to the difference in weather and our younger population, not to mention the difference in health insurance coverage and a bigger private sector with self-payors in the MENA region compared to in the Western hemisphere.
I would also like to add that there is huge heterogeneity in my region when it comes to IR, from countries with a remarkably advanced IR practice like UAE, Egypt and Saudi Arabia, to countries with no access to IR services at all. Even if there is IR provision in a country, it will tend to be centralised in the major cities, depriving the rural areas. So, in a country like Egypt, of 120 million people, with a high-volume IR practice, almost 90% of trained interventional radiologists are in Cairo.
IN: Talking now about PAIRS, how much progress have you seen in the past few years with the society? What are the challenges, and for the specialty overall? What is your vision for the future?
In 2018, PAIRS had 30 active members. In 2023, we now have more than 1,000. In 2014, the annual meeting was attended by 150 people, whereas in 2023 it was attended by 4,300 people. Now, we are collaborating with all the big IR societies and meetings worldwide like the Cardiovascular and Interventional Radiological Society of Europe, Leipzig Interventional Course, Global Embolization Symposium Technologies, as well as being the regional hub for the different national societies in the MENA region.
As for my vision (although this vision belongs to the whole of the current board), I remember having an eight-hour board meeting in Dubai in the holy month of Ramadan in 2019, when we planned for the years ahead. Our main goal was to transform PAIRS from a successful annual meeting to a fully functioning multicommittee society, working to face challenges, and help doctors and patients in the region to access IR. If you look now, we have a decent website with a big academy, housing hundreds of lectures accessible to all members. We have the Arab Journal of Interventional Radiology growing every day led by Mohammad Arabi as editor-in-chief; we also have the educational committee led by Refaat Salman doing dozens of webinars, which has also started our hands-on courses.
The board has a vision of investing in the younger generation, so we formed the very active residents, fellows and students (RFS) committee led by Rana Khafagy, who initiated the Global IR Juniors Summit organised in collaboration with the Society of Interventional Radiology RFS, the European Trainees Forum, and the British Society of Interventional Radiology. It will be its fourth year in PAIRS next year, and the RFS committee has been also working on the PAIRS IR curriculum, which will be published by the 2024 annual meeting.
Regarding PAIRS’s vision to further promote IR training in the region and to recruit more and more young minds to join IR, PAIRS initiated the #I_AM_ PAIRS IR awareness campaign led by our secretary Karim Abd El Tawab, and it took place in six medical schools in Egypt, Morocco, Saudi Arabia, Tunisia, UAE, and Syria, with almost 1,000 total attendees. Finally, we have the Women in IR committee headed by Noha Guzaiz (King Abdullah Medical City, Makkah, Saudi Arabia), which is dedicated to boosting numbers of female interventional radiologists in the region. Five or six years ago, none of these committees even existed.
IN: What advice do you have for interventional radiologists just starting out?
My advice would be this: you are an interventional radiologist, so you are a hero, as every day you will save lives and can treat disease all over the body. The important thing you have to learn is when not to do cases, where to stop and say “I should not do this case” or “there is a better option for this patient”. As long as you are developing your clinical skills, you should concentrate on making the best decisions for your patients.
NICE’s Scientific Advice programme will work with companies looking to attain both FDA approval and payer coverage
The UK’s Medicines and Healthcare products Regulatory Agency (MHRA) has designated three new approved bodies to increase the country’s capacity to certify medical devices.
TÜV SÜD, Intertek, and TÜV Rheinland UK join the four current UK Approved Bodies, almost doubling current capacity for the certification of medical devices in the UK, MHRA says in a press release.
TÜV SÜD and Intertek have been designated as UK Approved Bodies to assess and certify general medical devices in accordance with Part II of the UK Medical Devices Regulations 2002. TÜV Rheinland UK has also been designated to assess and certify general medical devices as well as in-vitro diagnostics in accordance with Part IV.
With the exception of the very lowest risk devices, manufacturers must apply to a UK approved body for UKCA certification. Products can only be placed on the market in England, Wales and Scotland after they have achieved certification.
Laura Squire, MHRA chief healthcare quality and access officer said: “By almost doubling capacity for medical device assessment in the UK, we’re supporting patients to access the safe and effective products they need to protect their health.
“Approved Bodies play a critical role in the supply of medical devices and expanding capacity has been a key priority for us to support manufacturers to bring their products to the UK.”
Before appointing an Approved Body, the MHRA conducts a detailed assessment process to ensure that organisations are stable and able to undertake impartial and objective conformity assessment activities, that they have an appropriate quality management system, the capacity and competence to undertake assessments and the processes they use meet the relevant regulatory requirements.
After successful designation, the MHRA monitors UK approved bodies’ activities including by regular audits and by witnessing some of their audits of manufacturers.
A recent Inari Medical roundtable webinar examined how to build a venous practice effectively—three experts from different specialties discussed the importance of forming and maintaining internal and external networks; what to consider when building a deep vein thrombosis (DVT) pathway; and how to choose the right treatment for each DVT patient. The webinar is part of the first edition of the ClotWarrior Academy DVT Webinar Programme set up by Inari Medical to initiate further education and conversation around the effective management and treatment of the full range of DVT chronicity.
Stephen BlackGerd GrözingerMichael Piorkowski
Stephen Black, vascular surgeon at Guy’s and St Thomas’ NHS Foundation Trust (London, UK) began proceedings, focusing on “the power of the multidisciplinary team”. Black also pinpointed how crucial it is to know the data and the literature relating to venous work, as well as to spend time with “people who have done it” before and “utilise their skill”—namely, those with established practices. In terms of data, there are more to come, Black added. “We have launched DEFIANCE, a randomised controlled trial (RCT) evaluating its clinical outcome in DVT treatment. Its goal is to demonstrate that mechanical thrombectomy is superior to anticoagulation alone. Other RCTs in the DVT space have all focused on catheter-delivered lytics and we know that the downside of lytics is bleeding, which was a significant outcome of the ATTRACT study. Trying to find something that avoids lytics is going to be really useful for this therapy.”
In terms of building the team, Black made the point that venous patients can be “more needy than their arterial [counterparts]”, and so lots of staff from different departments need to be involved in their care, including in theatre, interventional radiology (IR), haematology, ultrasonic angiology, and research. Black emphasised that even the intervention itself can be multidisciplinary depending on circumstances, with “another member of the team finishing it off”. He then touched on the protective, supportive aspect of working as a team—“if something goes wrong, […] and it will, you are very vulnerable if you are by yourself […]”, whereas as part of a team, this is guarded against.
Next, Black addressed how introducing pathways into the hospital is key “because you cannot be there all the time” to oversee every patient’s referral and care. These pathways enable smooth follow-up and decision-making around “who to treat and who not to treat”. Having an eye for detail is also important, he continued, stating that “it is not good enough to [just] hope for the best”.
After the procedure, Black advocates for duplex follow-up, then reflecting on the outcome, and repeating this after every procedure, having considered the success of factors such as “stent choice and placement, errors, and IVUS”. Moreover, he suggested that “most errors of a technical nature are the fault of the user, not the product”. Returning each time to consider outcomes will ensure that they keep getting “better and better”, Black averred.
Michael Piorkowski, interventional angiologist and cardiologist at CCB Frankfurt (Frankfurt, Germany) was next to speak, first outlining how the interventional DVT programme at his centre started. He described his hospital’s large cardiovascular outpatient service and how “every day, there are up to ten patients referred from general practice with suspected DVT”. The programme has office hours of 8am to 6pm Monday to Friday, with various lab testing capabilities as well as those for other types of imaging, including several vascular ultrasound machines and computed tomography (CT) and magnetic resonance imaging (MRI) with cardiovascular-specialised radiologists.
“When I started here in 2014, the majority of patients, even those with iliofemoral DVT, were treated with compression stockings and oral anticoagulation,” Piorkowski relayed, going on to say that when he first treated acute DVT in 2012, he used a rotational thrombectomy device. He then switched to a pharmacomechanical aspiration device but “most patients still also had some form of lysis”. This limited the indication, Piorkowski went on, adding that the research at the time was also not really venturing beyond chronic venous disease.
Nowadays, he noted that they still see patients who underwent DVT treatment 10 or 15 years ago—“there is a high patient loyalty”. They have started to treat chronic venous occlusions, especially in middle-aged women who experienced an iliofemoral DVT in their twenties or following childbirth. “There is a growing recognition of the need for a treatment with high thrombus removal and without lytics,” Piorkowski then affirmed. “We were one of the first centres outside of the US to introduce the ClotTriever system and in my opinion this is the most efficient way to remove acute and chronic clots. I faced the problems of patients developing PTS over the long term, including problems with varicose veins, leg ulceration, constant heaviness and swelling of the legs. By removing all of the clot, in the acute phase, we can prevent all of this.
Gerd Grözinger, interventional radiologist at the University of Tübingen (Tübingen, Germany) followed Piorkowski, sharing his experience of how he takes on DVT referrals. Firstly, he outlined an example of a case he has seen—a 30-year-old woman with five-day-old leg pain, who had never had thrombosis before nor had a family history of it. She took the contraceptive pill and was a smoker, Grözinger shared. She received an ultrasound, which confirmed the DVT, and she was then referred to Tübingen. This led Grözinger to make the point that networks of hospitals including specialist centres are crucial in providing adequate care for DVT, so that hospitals in rural areas that may not have the required expertise can work with bigger, more specialised hospitals to refer their patients over if necessary.
“The team is very important,” he continued, expanding on this to describe his hospital’s vascular centre, which has all the specialties combined, including vascular surgery, cardiology, angiology, IR and dermatology. There are two vascular board team meetings each week, at which DVT patients are discussed, and a 24/7 service for vascular emergencies, Grözinger detailed. Different external specialists refer DVT patients to the vascular centre, including internal medicine and emergency departments, and primary care physicians.
Grözinger then highlighted a “holistic approach” as key, which, at his centre, means they have a linked pulmonary embolism (PE) team, and often see patients who are being seen, for example, by oncology for metastatic lymph nodes in the pelvis, which has gone on to cause compression disease and subsequently DVT. Standardised treatment pathways for DVT and PE are necessary, he stipulated. Grözinger shared that, at his hospital, their DVT pathway is mostly based on the European Society of Cardiology guidelines. “All patients with a proximal DVT have cross-sectional imaging with MRI, as it is the only modality that can assess the real age of the thrombus”.
“I think we all have to consider that DVT is not a life-threatening condition,” Grözinger then mused, reflecting on how the bleeding risk with treatments including catheter-directed thrombolysis (CDT) may not be worth it. Therefore, there is “a need for a mechanical thrombectomy system without CDT”—ClotTriever (Inari Medical) is an answer to this need, he put forward. “The system is a mechanical thrombectomy system designed to remove large thrombi from large vessels in a single session, without the need for thrombolytic drugs or consequent intensive care stay. The patient I mentioned earlier, who was referred to us, was also treated with ClotTriever system. She had a complete occlusion and the clot which we removed during the intervention was organised thrombus. This is what we experience in a number of patients—they develop chronic DVT and thrombolysis would not work in those cases.”
Grözinger’s last word was on increasing the visibility of this “undertreated disease”, which he believes can be achieved with “satisfied patients with quick improvement of symptoms”. He would also advise good communication about cases with the referring centre beforehand, and offering lectures and educational material to these referring physicians to “raise awareness”.
To learn more about the lytic-free mechanical thrombectomy ClotTriever and FlowTriever systems, join Inari’s symposium at CIRSE 2023 on Sunday 10 September at 1pm (Auditorium 15).
Koen Deloose (Sint Blasius Hospital, Dendermonde, Belgium) talks to Interventional News about the importance of treating femoropopliteal disease patients and why some of the new generation bare metal stents are more advantageous for those complex lesions. He also discusses the PRIZER study, currently under enrolment, which aims to confirm the safety and efficacy of the Renzan peripheral stent system (Terumo Interventional Systems).
How prevalent is femoropopliteal disease and what is the impact of non-treatment for both patients and wider healthcare systems?
I think we are all aware of the fact that today the prevalence of peripheral arterial disease (PAD) in people over the age of 70 is around 15% and one out of every three of these definitely needs treatment. Interventional treatment can include supervised walking exercises as well as medicament therapy. My experience, and indeed my preference, is a combination of treatments. It is important for the patient that they are on the right drugs, that they are doing sufficient exercises but also that they are revascularised, whether with a bypass or, our preference, with a minimally invasive endovascular approach.
There are two categories of PAD patients—on one side you have the claudicants, and on the other the chronic limb-threatening ischaemia (CLTI) patients. We know that 5% of the severe claudicants are also evolving towards becoming CLTI patients. However, in a lot of countries they do not treat the claudicants with anything other than a conservative approach. In Belgium and in many other European countries we have noticed that there is definitely a space for the treatment of claudicants, especially as severe claudication has a very profound impact on the quality of life of the patient, and on their independent wellbeing.
These patients (Rutherford 4+) have rest pain or they have a lot of tissue loss and so if you stick to just a conservative approach these people are definitely going to end up with major amputation or death. Lack of treatment thus can have a huge impact on the social life of patients and ultimately a financial impact on healthcare systems as well. So we need to avoid this and we need to intervene, on time, in this category of patients.
How can the use of different stents to treat calcified lesions help resolve the unmet needs of these patients?
I noticed in my own practice in Dendermonde that the idea of ‘leaving nothing behind’ just did not work. It only worked for the straightforward, easy, non-calcified, stenotic, relatively short lesions, where it was feasible to treat these patients with angioplasty alone or a drug-coated balloon (DCB). But the vast majority of lesions that, as a vascular surgeon, I come across are chronic total occlusions. They tend to be more than 15cm TASC C and D severely calcified lesions. And so I noticed that the dream of leaving nothing behind remained a dream.
Because of this, in more than 50% of these patients, we need a scaffold. So I think there should be a greater focus on the need for bare metal stents, because a lot of interventionalists have almost forgotten the existence of bare metal stents. But in this category of patients, DCB alone or angioplasty alone is insufficient and we need bail-out scaffolding.
There are currently a wide range of stents available. For example, we have stents with very low chronic outward force that we use to scaffold a flow limiting dissection in the less calcified lesions. But then we also have the severely calcified lesions where we need bare metal stents with a very high radial resistive force and crush resistance such as the Renzan stent which is the new kid on the block. It is definitely important to select the right bare metal stent for the right indication and that is the challenge we need to overcome today.
How have stents evolved over time and why is it important to have next-generation stents like self-expandable micro-mesh stents available on the market?
In my mind and in my hands there are some essential requirements when it comes to the ideal bare metal stent. For me, as a pragmatic vascular surgeon, it first of all needs to be easy to use. If it is too complex, takes too many steps to implant, forget it. And of course accuracy of deployment. For example, if you really want to end up at the ostium of your superficial femoral artery for instance you need 100% accuracy. The nice thing about the Renzan stent is the fact that it is repositionable. So if you make a mistake, if you did not take into account tortuosity in the access towards the vessel and you made an error, you can reposition and try again.
When we are talking about the femoropopliteal area, visibility, flexibility, and conformability to the vessel anatomy are also extremely important. You need the right chronic outward or radial forces. I notice that especially in the USA, a lot of physicians are using distal embolic protection devices to avoid distal embolization. These definitely have some disadvantages, including additional steps to the procedure that come with their own potential difficulties and complications. However, we now have a bare metal stent available with dual layer micro mesh technology, which aims to prevent plague prolapse and distal embolization based on experience in other therapeutic areas.
Renzan peripheral stent system
What is the PRIZER study and what do you expect or hope to see?
The PRIZER study is a prospective multicentre post-market single-arm study which is looking to assess the performance of the Renzan stent in femoropopliteal disease treatment. There are two endpoints, a safety endpoint—defined as freedom from deaths, TLR and any amputation of the index limb at 30 days—and then we have an efficacy endpoint which is defined as primary patency at one year. We plan to enrol 135 patients in this study with follow-up of 36 months. There are 13 centres enrolling patients across five European countries: Germany, The Netherlands, Belgium, France and Spain.
I am actually excited about the spotlight again being on bare metal stents. I have mentioned that the dream of leaving nothing behind with a DCB has remained, in 2023, a dream, especially for the more complex lesions. On the other side of the spectrum if we are talking about drug-eluting stents, which have a lot of advantages but also some disadvantages such as the short lengths of some devices, so when treating a 30cm lesion I might need three stents which, in the Belgian healthcare system, is unpayable. There is also data showing signs that in the long run there can be some toxicity of paclitaxel.
On the other hand, we have access today to a completely new generation dual-layer micro-mesh stent that is repositionable with the right chronic outer force, radial resistive force and crush resistance. To ensure a proper stent deployment, it is important to respect some key aspects of the instructions for use and do an extensive vessel preparation before implanting the stent. There is also a learning curve that you need to overcome in order to be an expert at Renzan implantation.
I am happy about this device, and I hope that the PRIZER study with the Renzan stent will confirm my enthusiasm.
Disclaimer: The Renzan Peripheral Vascular Stent System is indicated for use in patients with Peripheral Vascular Disease. Refer to instructions for use, contraindications and warnings for additional information. Renzan is manufactured by MicroVention Europe and distributed by Terumo Europe N.V. All brand names are a Trademark or registered trademarks of TERUMO CORPORATION, its affiliates, or unrelated third parties. Renzan is CE marked only, and not approved for use in the USA.
There has been major progress in the treatment of peripheral arterial disease (PAD) globally in the last few years, “but there are still issues that need to be addressed”, Marianne Brodmann (Medical University of Graz, Graz, Austria) told Interventional News, reviewing her experience as co-director of the recent BD PAD Summit (20–21 June, Riga, Latvia). She said the event highlighted the “consensus and strong will” among physicians to “improve” the picture when it comes to fighting the disease.
The summit was led by course chair Bruno Migliara (Pederzoli Hospital, Pescheria del Garda, Italy), alongside co-directors Brodmann, Koen Deloose (AZ Sint-Blasius Hospital, Dendermonde, Belgium), and Marco Manzi (Policlinico Abano Terme, Abano Terme, Italy).
Aimed at “shaping the future of PAD patient care”, its programme was divided into five sections. Sessions on diagnostic tools and algorithms were complemented by presentations on access and crossing lesions, treating lesions and optimising patency, and finally, on the future of PAD treatment. Across a day and a half, over 170 attendees were offered 24 hours of hands-on sessions, as well as the opportunity to hear 31 presentations by 20 key opinion leaders in the field. Rapid-fire debates followed most presentations, while a research and development session offered education on further new advances.
Brodmann opened the conference by addressing what she called the historical underappreciation of the problem of PAD—236 million adults worldwide have the condition—when compared with other conditions such as coronary artery disease and stroke.
More recently, she said, there has been “increasing recognition that PAD is an important cause of cardiovascular morbidity and mortality”, with particular attention given to its status as a “leading cause of physical disability”, especially when it progresses to critical limb ischaemia (CLI).
The problem is growing, she suggested, noting a study which found that the prevalence of the disease jumped by 45% globally between 2000 and 2015. “It can only be changed by awareness campaigns […] from healthcare providers as well as the general population,” she told Interventional News.
Part of the issue, Brodmann suggested, lies with difficulties in diagnosing PAD. This set the stage for the beginning of the first session on diagnostic tools, where Christos Rammos (University of Duisburg- Essen, Essen, Germany) highlighted a selection of new options in angiography, among them carbon dioxide angiography. Following him came Daniel van den Heuvel (St Antonius Hospital, Nieuwegein, The Netherlands), who assessed duplex ultrasound as a method for developing an “objective endpoint” in the definition of optimal results from revascularisation procedures.
Algorithms came to the forefront next, with Brodmann stepping in to deliver the absent Maria Ruffino’s (Institute of Imaging of Southern Switzerland, Lugano, Switzerland) presentation on the need for clarity on the best aortoiliac lesion treatment. A compelling discussion followed, where it was suggested by one audience member that lack of evidence-based treatment in this area could be due to physicians’ preference. In conversation with Interventional News, Brodmann said: “This is indeed the case. Therefore, there is a need for creating strong treatment algorithms in different areas.” This, she suggested, was a need that could be met by physicians.
Deloose, meanwhile, also contributed to the session by telling the audience to base their treatment algorithms on their prepping algorithms—which should in turn be based on how you pass the lesion. PAD below the knee (BTK) was addressed during this session by Marc Sirvent (General University Hospital of Granollers, Granollers, Spain), who, in an assessment of different strategies, highlighted the “essential” nature of good angioplasty technique.
Next up came a set of talks on access and crossing lesions. Ralf Langhoff (Sankt Gertrauden Hospital, Berlin, Germany) set the tone by alerting listeners to the fact that up to 11% of peripheral vascular interventions result in access complications, underscoring the importance of addressing them. Also speaking in this session was Giacomo Isernia (Azienda Ospedaliera di Perugia, Perugia, Italy), who outlined why the guidewire is “essential” in complex occlusion cases. Yann Gouëffic (University Hospital of Nantes, Nantes, France) addressed the audience too, stating on the subject of vessel preparation devices that “no studies have shown” that they offer a decisive advantage in cutting intimal hyperplasia.
Following one packed day of presentations came another, with the session on lesion treatment opening with further discussion from Rammos, who presented on a rotational atherothrombectomy device. In the subsequent talks on lesions, Mercedes Guerra (University Guadalajara Hospital, Guadalajara, Spain) gave a strong presentation on the need for better classification of extremely calcified lesions, which she said require their own treatment approach.
Migliara spoke to Interventional News following the summit to praise Guerra’s talk, which he said “analysed very well and deeply one of the most challenging and discussed questions: how to treat calcium”. The presentation and discussion which followed illuminated the need to “better define the best treatment choice for every different type of lesion”, he added.
Migliara himself presented during this session, returning to the rotational atherothrombectomy device explored by Rammos, which he said held particular promise for the treatment of in-stent restenosis. Its advantage, he averred to Interventional News, was that it “allow[s] retreatments without increasing their complexity”. In the debate following his talk, he suggested its repeated use for debulking poses fewer risks than bypass.
One highlight of the conference was what Migliara described as its “best debate”, between Deloose and Sherif El Kerdawy (Wadi El Neel Hospital, Cairo, Egypt) on the benefits of covered and uncovered stents in iliac artery treatment. Through this “scientific but also friendly debate”, Migliara said, “we understood better where the best choice is uncovered and where [it is] covered.” The audience swayed to the side of El Kerdawy: a post-debate poll found 42.9% on the side of the covered stent and 57.1% on the side of the uncovered.
“I learned many new ideas not only about techniques, but also about new materials and devices,” Migliara said of the concluding session on the future of PAD. Drawing special attention to vessel preparation and resorbable stents for BTK, he also praised a talk by Marta Lobato (Hospital de Cruces, Barakaldo, Spain) on new arterialisation techniques.
Migliara thanked those who spoke at the summit. Their “interesting presentations” and “active discussions” provided opportunities for learning, he said in review, and allowed him and his co-directors “to achieve the aim of this meeting”.
Researchers behind a new study published in the Annals of Vascular Surgery, among them lead author Laura Anderson and corresponding author Benjamin Brooke (both University of Utah Health, Salt Lake City, USA), have found that severe obesity risks a greater likelihood of maturation failure in the arteriovenous fistulas (AVFs) of patients looking to start dialysis.
Their work cites a 2008 Kidney International-published meta-analysis by Y Wang (Johns Hopkins University, Baltimore, USA) et al, which suggested that 33% of all US cases of end-stage kidney disease (ESKD) are associated with obesity and metabolic syndrome. Anderson and colleagues further aver that there has been a 42% increase in ESKD cases in the USA, which significantly includes a sevenfold increased risk of developing the condition for those with a body mass index (BMI) ≥35.
In reviewing the existing literature, the authors of this study note that, while some research has found higher AVF patency rates for obese patients, other research has found higher rates of failure and stenosis. Anderson and colleagues sought to clarify the effect of a BMI ≥35, “the most severe classes of obesity”, with a view to facilitating better clinical decision-making.
They conducted a retrospective cohort study, analysing the data from patients who received either a radiocephalic, brachiocephalic, or brachiobasilic AVF at a single centre during the period 2016–2019. The primary outcome was functional maturation following AVF creation, defined as use of the AVF with two needles for 75% of dialysis sessions in a continuous four-week period. Secondary outcomes included AVF depth and diameter, as well as flow volume, which was measured using a postoperative ultrasound examination.
A total of 426 AVF procedures were performed during the study period, with 202 available for analysis following the exclusion criteria. Among these were 49 (24%) with radiocephalic, 87 (43%) with brachiocephalic, and 66 (33%) with brachiobasilic AVFs. Stratification by BMI yielded 53 patients (26%) in the severely obese group and 149 (74%) in the remaining categories. There were “no significant differences” between the groups on other factors, apart from a higher percentage of female patients in the former group.
The authors found a “significantly lower rate of functional maturation” in the severely obese group (58% severe obesity vs. 80% non-severe obesity; p=0.002). A subanalysis by fistula type found that differences in primary and assisted maturation between obesity groups on brachiocephalic AVFs were significant, but were not so for those with radiocephalic and brachiobasilic AVFs.
On the secondary outcomes, outflow average vein depth was “significantly increased” in severely obese patients compared to the other groups, with the difference marked across all three types of AVF (p<0.05 for all comparisons). There was also a statistically significant larger average vein diameter for those severely obese patients with brachiocephalic AVFs (6.8mm severe obesity vs. 5.9mm non-severe obesity; p=0.007). The authors did not find significant differences in flow volume for any AVF type between any of the groups.
Multivariable logistic regression analyses, which controlled for a variety of other factors including sex, age, smoking status, and AVF type, found that severely obese patients were 62% less likely to achieve functional maturation than AVFs in patients with BMI ≤34.9 (odds ratio [OR] 0.38; 95% confidence interval [CI] 0.18-0.78, p=0.009).
The data suggest that obesity is of greatest concern in fistula maturation for severely obese patients with a brachiocephalic fistula, the authors say in their discussion, adding that it can also impact brachiobasilic AVFs “even after transposition”. Drawing attention to the “obesity paradox”, the finding of some studies that patients with higher BMIs have better survival rates with ESKD, sometimes attributed to “nutritional preserve and protection against wasting in the setting of acute illness”, they argue that their results indicate that this does not extend to fistula maturation. For treatment of severely obese patients with an AVF who cannot be cannulated, Anderson et al note that transposition and superficialisation of the fistula are established options.
Outlining some limitations, including the retrospective cohort design of their study and its focus on functional maturation outcomes rather than primary or secondary patency, the authors nevertheless conclude that their results support the claim that BMI ≥35 reduces functional maturation rates. “These data,” they state finally, “can help guide decision making when planning AVF placement in severely obese patients, which should include scheduling adjuvant superficialisation procedures on appropriate patients.”
When utilised as a first-line technique for medium vessel occlusion (MeVO) stroke, aspiration and stent-retriever thrombectomy have demonstrated “no significant difference” in imaging-related or clinical outcomes. That is according to a multicentre, propensity score-matched analysis including more than 400 patients, the results of which have been published in the journal Stroke: Vascular and Interventional Neurology.
“Altogether, these findings do not suggest one technique […] to be associated with any greater probability of technical success, safety, or better long‐term functional outcomes,” write authors Adam A Dmytriw (Massachusetts General Hospital, Boston, USA) et al. “The technical success rates with either technique were high (80–90%) and are consistent with those reported from secondary analyses of clinical trials.”
Led by first author James Siegler (Cooper Neurological Institute, Camden, USA), the researchers initially note that, due to the lack of data regarding MeVO thrombectomy, they set about evaluating outcomes according to first‐line techniques in a large, multicentre registry referred to as ‘MAD-MT’. This consortium was founded by Dmytriw and Adrien Guenego (Erasme University Hospital, Brussels, Belgium). Imaging, procedural and clinical outcomes were assessed, with acute proximal or distal MeVO patients being treated at 37 sites across 10 countries and analysed according to the first‐line thrombectomy technique they received—aspiration or stent retriever.
Multivariable logistic regression and propensity‐score matching were used to estimate the odds of the primary outcome—expanded thrombolysis in cerebral infarction (eTICI) scores of 2b–3, defined as ‘successful recanalisation’—between the two treatment groups. Secondary outcomes included the ‘first‐pass effect’, eTICI scores of 2c–3, intracerebral haemorrhage, 90‐day modified Rankin scale (mRS) scores, and 90‐day mortality.
Of 440 included patients, 55.5% were treated with aspiration thrombectomy versus 44.5% with a stent retriever. Dmytriw et al report those treated via stent-retriever thrombectomy as having lower baseline Alberta stroke programme early computed tomography scale (ASPECTS) scores (median=8 vs 9); higher National Institutes of Health stroke scale (NIHSS) scores (median=13 vs 11); and non-significantly fewer medium‐distal occlusions (M3, A2, P2 or other; 17.4% vs 23.8%).
Use of a stent retriever was associated with a 15% reduction in the likelihood of successful recanalisation (odds ratio [OR]=0.85)—but this difference was not found to be significant after multivariable adjustments across the total cohort (adjusted OR=0.88), or in the propensity score-matched cohort, in which both groups included a total of 105 patients (adjusted OR=0.94). Furthermore, there was no significant association between thrombectomy technique and secondary outcomes in the propensity score-matched, adjusted models, the authors relay.
As such, they conclude that—in this large, heterogenous, multinational cohort of MeVO patients—no significant differences in imaging-related or clinical outcomes were observed between aspiration and stent-retriever thrombectomy. Dmytriw et al go on to assert that there appears to be “no significant technical or functional advantage” to using either specific technique.
However, despite this cohort being “one of the largest to date” to report outcomes associated with first-line aspiration versus stent-retriever thrombectomy in MeVO/distal vessel occlusions, they acknowledge the non-randomised allocation of the techniques; the influence of unmeasured confounding factors; and some missing reperfusion data as well as between-site variations, as limitations of the analysis.
“Other clinical and imaging predictors, such as clot composition or hyperdense vessel sign, warrant further exploration to better understand the selective vulnerability of certain occlusions to one device or another,” they add, also noting that multiple ongoing randomised trials are “anticipated to shed light on these treatment considerations”.
The use of catheter-based localised delivery of drugs for treatment of cancer patients has proven to be effective and provides the benefit of reduced systemic toxicity. A critical prerequisite for these modalities is the angiographic identification and engagement of feeder vessels of appropriate size into the tumours in order to deliver the designated therapy. Therefore, hypovascular tumours are not optimally treated with these catheter-based techniques. For instance, pancreatic tumours, unlike their liver counterpart, are generally hypovascular, and are without any obvious arterial feeder vessels. Novel approaches to overcome this obstacle for drug delivery in these tumours has the potential to significantly improve outcome and potentially survival in these patients.
One such approach currently being investigated is trans-arterial micro-perfusion (TAMP). TAMP first isolates an artery of interest using a double balloon catheter to occlude the proximal and distal part of the vessel, followed by exclusion of major side branches. Upon infusion of drugs between the balloons in this isolated section, the increased intravascular pressure permits active diffusion of infusate directly across the vessel wall into the surrounding tissue.
Early studies of TAMP using gemcitabine chemotherapy in patients with locally advanced pancreatic cancer (LAPC), has shown the approach to be safe with no obvious local toxicity.
Currently, a phase III clinical trial, TIGeR-PaC, is comparing the efficacy of this approach using intra-arterial gemcitabine (IAG) versus standard of care IV gemcitabine/nab-paclitaxel (GN) for patients with LAPC. The trial is designed with an induction phase for all patients of upfront systemic chemotherapy and radiation prior to randomisation to IAG or continuation of GN. LAPC patients receive three cycles of GN and one cycle of radiation (stereotactic body radiation therapy; 33Gy in five fractions). Following induction, patients with non-progressive disease are randomised to receive IAG (eight treatments biweekly for 16 weeks) or continuation of GN for four cycles over 16 weeks. After the 16 weeks of randomised therapy, patients with non-progressive disease receive continuation systemic therapy of GN or low-dose oral capecitabine, per investigator’s preference until disease progression and are followed for survival only.
Recently, the first interim analysis of the trial was presented at the World Congress on Gastrointestinal Cancer (28 June–1 July, Barcelona, Spain). At the time, 45 patients had been randomised in the trial; the survival, progression-free survival (PFS) and the adverse events data (AE) comparing the two arms were presented. Of the 45 patients randomised, 23 were randomised to IAG and 22 to GN. There were equal number of primary events (13) in each arm. Patients enrolled in the study were randomised after the induction phase that lasted, on average, 5.5 months.
After randomisation, the median survival in the control arm is 10 months, vs. 16 months in the IAG arm. The p values based on Wilcoxson non-proportional hazard ratio (HR) is 0.08 between the two arms. The PFS in control arm was seven months vs. 15 months in IAG (HR 0.55; confidence interval [CI]: 0.21–1.47). There was a threefold increase in AE in the control arm versus IAG (245 vs. 85); most of difference in AE were haematological (neutropaenia and thrombocytopaenia), followed by transaminitis. Lastly, in term of tolerability of completing all four cycles of active treatment without treatment modification, 61% of patients in IAG completed all intended treatment vs. 18 % of the patients in GN. The first interim look at the trial results is very encouraging in favour of IAG. Currently, the trial continues to enrol in 17 centres in the USA, with a second interim look at the data expected at end of 2024.
Ripal Gandhi is a vascular and interventional radiologist at Miami Cardiac and Vascular Institute and Miami Cancer Institute (Miami, USA).
The Society for Cardiovascular Angiography & Interventions (SCAI) has welcomed the review of scientific data related to the premarket approval applications for two renal denervation systems, describing this as a “step forward to advancing access to additional therapies for people with uncontrolled hypertension”.
The US Food and Drug Administration (FDA) Circulatory Systems Devices Panel met this week to review scientific evidence on interventions aimed at reducing blood pressure in patients with hypertension, scrutinising data for two renal denervation systems—the Paradise system from Recor Medical and Medtronic’s Symplicity Spyral device—as tools to reduce blood pressure in adults with uncontrolled hypertension, who may be inadequately responsive to, or are intolerant to, anti-hypertensive medications.
While the FDA panel voted in favour that available data supporting the efficacy and safety of both of the devices, votes differed on whether the benefits outweighed the risks. The committee voted unanimously in support of safety, eight to three in support of its effectiveness, with one member abstaining, and 10 voted the benefits outweigh risks while two disagreed for the Paradise system. For the Medtronic Symplicity Spyral device, the committee voted unanimously in support of safety, seven in support and six against on effectiveness, and six voted yes, seven against (with tiebreaker by chair) and one abstained on the benefits outweigh risks.
In a statement issued on Thursday, SCAI said that it is encouraged by the panel’s vote as a step toward advancing access to additional therapies for people with uncontrolled high blood pressure. “Advancements like renal denervation are imperative to enhancing shared decision-making that can lead to better treatment and outcomes for patients,” the statement reads. “The FDA, renal denervation industry and healthcare personnel community spent many hours working and collaborating closely on these trials and deliberations for the betterment of patients and the care they receive.”
Ahead of the votes this week, SCAI released a position statement on renal denervation for hypertension regarding patient selection, best practices for optimal techniques, competence, training and organisational recommendations.
In conclusion, SCAI agrees that device therapies targeting the renal sympathetic nervous system hold promise as adjuncts to abate or interventions to abolish hypertension, depending upon the underlying severity of blood pressure elevation. Appropriate patient selection, pre-procedure evaluation, careful procedural planning and technique, implementation of strict operator training standards and facility requirements are paramount to programmatic success.
“It is important we continue to seek out new treatment options for patients, including the use of renal denervation, given the growing global prevalence of uncontrolled hypertension increase year over year,” George Dangas (Icahn School of Medicine at Mount Sinai, New York, USA), SCAI president, was quoted as saying in the statement. “The panels’ vote will allow physicians and patients access to a renal denervation procedure for the first time with the potential to improve the treatment and quality of life for those suffering from hypertension.”
Boston Scientific has received 510(k) clearance for expanded indication of the Visual Ice cryoablation system. The clearance grants this device an indication expansion to now be used in the treatment of pain associated with tumours that have metastasised to bone in patients who cannot receive standard radiation therapy or if standard radiation therapy has not provided relief.
Boston Scientific is the first company in the USA to receive on-label indication for cryoablation of bone metastases. This, the press release states, is important becausecryoablation can offer rapid and durable pain relief for patients who have been taking opioids and non-opioid analgesics or have undergone radiation therapy but still experience severe pain.
“Thanks to advancements in cancer treatments, people with cancer are living longer, but that can also mean that many patients living with late-stage cancer may also experience painful bone metastasis” said Peter Pattison, president of interventional oncology & embolization at Boston Scientific. “As the only company to hold this on-label indication for cryoablation, I am proud that we can help improve quality of life for these patients.”
This indication adds to the wide range of uses for Boston Scientific’s Visual Ice cryoablation system and cryoablation needles, including kidney, liver and lung tissue, prostate cancer, liver metastases, cryoanalgesia, and breast fibroadenomas.
Oluwatoyin (Toyin) Dada is a current fifth-year postgraduate trainee (resident) in interventional radiology (IR) and diagnostic radiology (DR), and Ariana Mills, a first-year resident. Both are based at the Icahn School of Medicine at Mount Sinai (New York City, USA) and have answered some questions for Interventional News about their journeys into IR from their US perspective.
IN: What led you into medicine? What has since led you to pursue IR?
OD: Some of my greatest influences growing up were my mom, who was a health aide for a short time, and my older sister, who pursued medicine. Naturally, I wanted to be like them, so medicine was always something I had at the back of my mind. I also had the opportunity to work with a child who had autism and volunteered at our community hospital during high school. Being in those environments gave me a deep appreciation for medicine. In medical school, I knew I wanted to go into a field that had a lot of variety and allowed me to do procedures, as I already loved hands-on activities. I went to a Latino Medical Student Association conference as a second-year student and met an IR attending who chatted with me about the variety of cases in IR, their complexity, and what they were able to offer patients. After that interaction, I made it my mission to learn more about the field of IR, and the rest is history!
AM: I wanted to become a doctor after taking a human biology class in sixth grade. I loved science and admired the tremendous commitment to helping patients inherent in medicine. After seriously exploring that childhood dream through shadowing, I was certain I wanted to begin the path to applying to medical school by the time I started college. I learned about IR from an attending physician on a panel during my first semester of medical school. After shadowing that physician, I was drawn to the specialty. I liked the field’s procedural nature, the ability to treat various pathologies, the countless opportunities for research, the supportive professional community, and the novelty of devices and interventions. After leading a research project on fertility after transcatheter arterial embolization for obstetric haemorrhage, I was certain I wanted to train in IR because the field constantly identifies safe and innovative alternatives for patients.
IN: What did you do to prepare for your application to IR? What was the greatest challenge?
OD: I did a two-week IR rotation at the beginning of my clinical years and did a quality improvement project with the IR faculty at my institution. I also tried to attend conferences and symposia geared toward medical students, which provided a window into other IR departments across the country. I would say the biggest challenge when applying was the number of people telling me not to pursue IR/ DR for fear of poor work-life balance, artificial intelligence taking over, turf wars, radiation exposure, etc. I decided to apply anyway and have been extremely happy with my choice thus far.
AM: I prepared for my application by exploring my interest in IR. Specifically, I shadowed during preclinical years, participated in multiple clinical rotations, completed two visiting student electives, attended and presented at academic conferences and symposia, and volunteered with the Society of Interventional Radiology (SIR) Medical Student Council. Not only was this process helpful for building my application, but it gave me a multifaceted view of IR that informed my decision to apply to the specialty. I wanted to remain open-minded about other specialties during medical school too, so my greatest challenge was maintaining a strong involvement with IR while also exploring other fields.
IN: Toyin, what has been the highlight of your residency so far? The biggest challenges? Ariana, what are you most looking forward to, and what do you think the greatest challenge will be?
OD: The biggest highlight of residency was finding that I was staying at my current institution for IR training! It felt like all the hard work finally paid off. Because IR/DR is a rapidly evolving field and there is not much exposure as medical students, I found that the learning curve was incredibly steep. Thankfully, with repetition and experience, I am finding it much easier now to grasp concepts. Additionally, there are multiple amazing resources (SIR Learning Center, the Backtable podcast, etc.) that are available to trainees to make learning IR concepts much easier.
AM: I am most looking forward to being even more involved in patient care as a resident physician. I am also excited to spend more of my time learning experientially, working towards a collective goal as a part of a team, and contributing to a rapidly growing specialty. Given that residents are learning at such a fast pace and being pushed to their full potential, I think the greatest challenge for me will be to keep in mind how much progress I have made without harping on how much I still cannot do and how much I still do not know.
IN: I can see from Twitter etc. that you are involved in IR outreach)—what made you want to be involved in this?
OD: Many people invested time in me as a medical student and resident, and it has paid off greatly. I feel that it is my duty to pay it forward to those coming up behind me. Additionally, while I have had (and still have!) amazing mentors, I find that not many people in IR look like myself—a black woman. I feel it is important to be visible and show others like me that we are here, and that there is plenty of room for them at the table too.
AM: Dr Daryl Goldman started an elective called ‘Introduction to IR and Minimally Invasive Procedures’ that was offered to students at our institution. During the pandemic, she recognised that the widespread adoption of virtual education could enable the department to expand the elective to any student worldwide interested in IR. She kindly reached out to me to see if I would like to help her facilitate this iteration of the course, and I was subsequently co-course director for two years. It was very impactful to witness that the course fostered excitement in students, and I look forward to working on similar initiatives in residency.
IN: What words of advice would you give to current medical students trying to decide what specialty to go into?
OD: The best advice I received as a medical student is to stay open to all possibilities and treat each rotation as if that is the specialty you are going into. I took that advice very seriously and I am in a completely different field than the one I first thought I would pursue. I am very happy with my choice and would gladly choose IR all over again.
AM: Deciding on a specialty involves a lot of reflection. It is helpful to be extremely honest with yourself about who you are, including your proclivities, strengths, areas for growth, limitations, and professional and personal aspirations. As you learn about different fields, consider what is required in the training and especially what is required as an attending. Through this process, you can evaluate whether you see yourself being successful professionally in this field, whether you are excited about what the field can add to your life, and what you believe you can offer to the field.
IN: How well is IR introduced to med students in the USA? What, if anything, do you think med schools in the USA could do to better inform students of opportunities in IR, or what a career in IR entails?
OD: Depending on the institution, IR is not readily offered as an elective or is often limited to a small number of students. A strategy that I have seen work really well, especially at Mount Sinai, is that it is offered as a subspecialty elective within the required surgery rotation. Speaking from my own experience, I learned about IR at a non-IR conference, and that was pivotal in my career path. Symposia and conferences geared towards medical students are fantastic ways to reach potential recruits early on.
AM: It is well established that students do not have much exposure to IR in medical school, and in my experience it is not for lack of enthusiasm from the IR community. I hope the general medical education teams can do more to reduce barriers to exposing students to IR. For example, schools could invite interventional radiologists to be involved in preclinical education, such as around IR procedures like uterine fibroid or prostate artery embolization during relevant lectures, and schools could allow rotations in IR to meet acting internship requirements.
Pellerin started his presentation by outlining what is necessary for “optimal” renal tumour treatment. He listed among these requirements treatment planning and assessment, the visibility of the tumour, access to the patient intervention site and tumour, the radiation dose to patient and operator, and the procedure morbidity.
Moving on to focus on radial access, Pellerin questioned rhetorically whether the “big push” towards the approach in the last five to 10 years is solely down to industry, or whether it is because it actually offers a “real advantage” when it comes to achieving optimal renal tumour treatment. He made the point that this approach is “widely used and accepted” by cardiologists. The evidence from the last decade comparing femoral with radial access, Pellerin detailed, spans transarterial chemoembolization (TACE), yttrium-90, angioplasty of the superior mesenteric or renal arteries, and renal embolization. This evidence shows that the technical success between the two access approaches is “similar, but it is probably one point to renal access”.
Continuing, Pellerin stated that a radial approach can lower access site complications, based on the existing literature, however, this is “cardiology literature”, he conceded. He then stated that where patient comfort is the concern, radial access is “preferred”, as it only requires “a small puncture under local anaesthesia”. Possible limitations with radial access, Pellerin stipulated, include for procedures where the objective of the intervention is to control a symptom which itself “does not involve the vital prognosis of the patient”, as is the case for uterine artery embolization for symptomatic fibroids, or prostate artery embolization for dysuria management. The choice of vascular access, the speaker set out, “must be guided by a detailed study of risks versus benefit in relation to complications linked to vascular access”. In other words, Pellerin invited the audience to question whether “a haematoma at the puncture site is preferable to a stroke” and similarly, these types of questions “must also be addressed with regard to cancer management”. Whether there is increased morbidity linked to longer procedures has “not yet been studied”, Pellerin added.
Moving on to address navigation, the presenter defined it as “performing the ideal placement of probes based on a predefined trajectory”. Compared to in the past, navigation is “different”, as it has become “more and more stereotactic”, Pellerin noted. Artificial intelligence also assists with needle planning, simulating the ablation zone, and predicting success. It is also possible now to optimise targeting, which means “finding the best option for insertion into the lesion, avoiding critical structures,” Pellerin explained. Robotic arms can also aid in delivery, and there is also confirmation software to help ascertain whether the target has been reached.
Lastly, Pellerin touched on angio-CT which he likened to a Swiss army knife as it “expands your possibilities a lot—you have a very high level of imaging quality”. He then referenced the emerging CT technologies, including spectral CT, which can “totally change the vision of the work we do [by] making possible the comparison of multiple functional parameters”. For example, it can “improve visualisation of lesions to facilitate procedure planning and enable accurate assessment of ablation margins”, while also “characterising tissue to better guide procedures and facilitate clinical decision-making, and analysing quantities such as iodine concentration to help determine procedural success”.
Focusing on the disease through the patient’s lens, establishing well-functioning multidisciplinary teams, to potentially enhance both the patient’s journey and clinical outcomes got top billing at BD’s second EMEA End-Stage Kidney Disease (ESKD) Summit (9–10 May 2023, Milan, Italy). With a multispecialty faculty comprising 22 leading voices including nephrologists, vascular and transplant surgeons, and interventional radiologists (with a combined knowledge of over 400 years), selected from 12 countries, BD’s second edition of “The Changing Face of a Dialysis Patient” showed commitment to a new format of scientific peer-to-peer communication, characterised by open interaction and vibrant discussion. More than 30 presentations including challenging cases, 14 hands-on workshops and the participation of 200 attendees marked the event.
Scientific directors of the summit, interventional radiologist Fabrizio Fanelli (Florence, Italy) and vascular access and transplant surgeon Nicholas Inston (Birmingham, UK), welcomed delegates to a programme that encouraged placing patients at the heart of care in dialysis access creation, restoration and maintenance.
Disease overview and patient journey
Charting the various difficult terrains of end-stage kidney disease (ESKD) in the renal patient pathway, Inston said each person’s course depends on age, comorbidities, “events” and interventions that were influenced by decisions made by clinicians, and importantly, by patients. Even simple clinical decisions can have a disproportionate, and sometimes uncaptured, impact on a patient’s life, he underscored. “When a fistula does not work, clinicians may simply plan to create another one, but this might have major disruption on a patient’s life and can potentially create a very negative loop for patients as they have likely gone through six to 12 months of other procedures to get to this point,” he said.
Based on his clinical experience, Inston referenced the concept of “much more tailored” minimally disruptive medicine (MDM). In this context, “the appropriate focus of treatment is the situation and the individual tackled as a whole”. MDM aims to reduce workload and individualise treatment, taking into account the effects of, for instance, “12 hours of dialysis per week, transport, maintenance interventions, clinical appointments and possible surveillance on a person’s life and calendar”.
Is there a case for rebooting questionnaires?
Inston kickstarted a discussion of wide-ranging quality of life issues with questions such as: “Is measuring patients’ quality of life via questionnaires of any use? Are they representative or do they misguide us? Do we add to the patients’ workload with more surveys/ questions/studies? Are we considering what we can do to tailor care to the patient and reduce workload? And can minimally disruptive medicine be applied to dialysis care?”
Daniel Gallego, a patient advocate and president of the European Kidney Patient’s Federation, has been a kidney patient since 1993, undergoing haemodialysis since 1995. To Inston’s points, he responded: “Twenty years of in-centre haemodialysis is different from home haemodialysis or peritoneal dialysis. Health questionnaires have been decided by clinical professionals and they do not include components on self-esteem, physical appearance, or things that really matter to us. […] Many aspects that might improve the life or quality of life of patients are not really captured in the outcomes. […] And sometimes these are misguiding us.” He called for a redesign of the questions asked and the management of information gathered so that the right decisions for patients can be made. Gallego also placed the spotlight on including the perspective of care-partners and families who influence the quality of life experiences for patients.
Responding to a question from the audience on whether a patient can influence the final decision on treatment modality, Gallego pressed on to say that with enough information and involvement at every stage, yes, patients can be responsible for both the choice and consequences of that choice for their access.
Külli Kuningas, lead renal research nurse, Queen Elizabeth Hospitals, Birmingham, UK, then outlined the “Our Arteriovenous Fistula (AVF) Lives” project, a patient-led ethnographic research undertaking run by the hospital to capture more in-depth patient perspectives on living with vascular access for dialysis. Relying on primary source material in the form of video diaries and the filming of patients in their own environments without the use of questionnaires, researchers aim to analyse how patients describe their conditions and what is important to them, to capture a repository of “true patient perspective”.
Gallego stressed that patient-reported outcomes were received usually from articulate, perhaps educated respondents who have the luxury of time. A critical component will be to validate these responses so that they become applicable to patients who might have poor language skills, come from populations with different cultures and languages and to those who might never answer questionnaires. He also addressed the discussion point of disparities in guidelines by stating that a consensus was needed, without bias, on the right treatment. This sparked the question: should care be “guideline-driven” or “tailored to the individual patient”? “We need to adapt, because every single patient is unique,” said Gallego.
The ensuing panel discussion on harnessing multidisciplinary expertise into the care of patients with kidney disease painted the picture of a changing paradigm. In “the old days”, and according to the panel’s experience, the “thinkers” were the nephrologists and the “doers” interventionalists and surgeons. With nephrologists also embracing interventional skills, there is a merging of the “thinkers” and “doers” responsible for a patient’s access, but this varies considerably based on local expertise, the panel said. According to their experience, there was acceptance that the nephrologists and nurses were ‘closer’ to the kidney patient’s journey and pivotal in coordinating care within multidisciplinary teams. Longstanding relationships with the patient, underpinned by trust and time were also identified as central to the patient’s experience of care. The panel agreed that a close connection in the discussion between patients, nephrologists and vascular access teams was core to good patient care. “More than the specialties of clinicians, communication is the key, and having one person in charge, potentially a nurse or dialysis access coordinator, who communicates in simple language along the whole journey with patients, is vital,” offered Gallego.
Ounali Jaffer (interventional radiologist, London, UK), Fien Gryffoy (vascular surgeon, Antwerp, Belgium), Gürkan Sengölge (interventional nephrologist, Vienna, Austria) and Ioannis Griveas (nephrologist, Athens, Greece) contributed to the discussion.
Looks as well as books
Panos Kitrou (interventional radiologist, Patras, Greece) detailed the importance of the Haemodialysis Arteriovenous Access Cosmesis Scale (AVACS), which is a new measure for vascular access. While clinical decision-making is often based on the twin-pillars of safety and effectiveness, the impact that vascular access has on the patient is also very important, he said.
Research has shown that lumps, bulging and related tortuosity, “mega access”, access-related scarring and number of scars, and the noticeability of the vascular access have been identified as some issues that play on patients’ minds.
Kitrou noted that there is a paucity of reports about the effect of AV access cosmesis on patients’ quality of life, dialysis experience, and decision-making about choice of vascular access type and creation.
“The cosmetic effect has an influence on patients’ psychology and therefore on the type of vascular access selected,” Kitrou posited.
“Cosmesis in the context of access is defined as the preservation of, or change in, limb physical appearance after AV access creation. It is one of many important factors to be considered in choosing vascular access within the context of the patient’s ESKD Life-Plan. By creating a scoring instrument that allows stratification of cosmesis of AV accesses, factors that affect cosmesis can be assessed,” he informed delegates. “In doing so, both clinicians and patients will be better informed to make access decisions in line with a patient’s priorities,” he concluded.
Interventional radiologist Shagran Binkhamis (Riyadh, Saudi Arabia) leads a hands-on session
New guidelines signal change
Narayan Karunanithy (interventional radiologist, London, UK) and José Ibeas (interventional nephrologist, Barcelona, Spain) then delved into the updates on the most recent guidelines.
The former unpicked the latest UK Kidney Association (UKKA) guidelines to point out that these guidelines, from the oldest continuously active nephrology society in the world, are not funded by any external organisation, commercial company or charity.
The recent haemodialysis access guideline update marks a considerable shift in how the organisation recommends that clinicians approach choices in vascular access for patients and does away with the idea of targets to place patient choice at the heart of vascular access creation and care. The team behind the guidelines have said it is a pragmatic guideline that had active representation from a variety of specialties but also three active patient representatives. “The guideline emphasises different patient characteristics rather than just saying: ‘This is the best access for you,” Interventional News was informed.
Karunanithy noted the endovascular-first approach to access dysfunction and that the additional value of covered stents and drug-coated balloons was discussed. Despite high-quality data in many areas, evidence gaps still exist, he pointed out.
Ibeas then turned to the most recent guidelines from the European Renal Association (ERA), European Society for Vascular Surgery (ESVS), Kidney Disease Outcomes Quality Initiative (KDOQI) and El Grupo Español Multidisciplinar del Acceso Vascular (GEMAV) to distil the areas of commonality and dissonance in their recommendations.
“According to my experience, evidence-based medicine is subject to the influence of several factors, that is, the methodology, perspective of the specialty, geographical area or health management system; and the values and circumstances of the patient […] and to their interpretation,” he said.
“[…] the most important point is the effort for consensus on the one hand and generating evidence in the areas of conflict on the other. When reading the guidelines, it is convenient to understand how each recommendation in each guide is justified. In this way, the clinician can generate his own critical judgment and contribute to the implementation of the guidelines in his environment in the most rational way. That can benefit the ultimate recipient of the guidelines, the patient,” Ibeas said.
Lean, clean and controlled: New tools for healthcare
Fanelli then brought to the fore an award-nominated project at the Careggi University Hospital, Florence, Italy, that applied lean management concepts to the patient’s journey. This approach seeks to define the process and the problem; measure performance; analyse the process for issues and root causes; improve by determining and implementing actions; and exercise control to maintain the improvement. When applied to endovascular procedures, lean management resulted in improved capacity and productivity; reduced procedure time; lowered operator stress; improved quality and reduced hospital stay.
“Lean healthcare is used in a growing number of hospitals to increase efficiency and quality of care. In healthcare organisations, it attempts to empower staff to generate continuous improvement through incremental but regular improvements in work processes. Periodic, detailed and specific feedback is extremely important to decrease complication rates and increase the service quality,” he shared.
Vascular surgeon Robert Shahverdyan (Hamburg, Germany) leads a hands-on session
Innovative highlights
Within the endoAVF creation session, Matteo Tozzi (vascular surgeon, Varese, Italy) presented a novel case report of Wavelinq endoAVF creation using carbon dioxide (CO2) contrast.
Detailing the clinical benefit of preserving residual renal function (RRF) in dialysis patients, Tozzi commented that those with residual renal function had better control of serum potassium and sodium, acid-base status and volemia.
Outlining his goals for the case, Tozzi explained that he planned distal injection through a drug-coated balloon or plain balloon to use CO2-viscosity wisely and enable a faster procedure with reduced risk and complexity.
His take-home message from this innovative approach to imaging: There was no damage on kidney residual function in chronic kidney disease patients and no damage on kidney residual function in kidney replacement therapy patients. “Non-iodinated contrast can be used in the implementation of [an] endovascular approach for vascular access creation,“ he submitted.
Tobias Steinke (vascular surgeon, Düsseldorf, Germany) then doubled down on the reasons for pursuing an endovascular creation strategy. He stated: “EndoAVF systems are designed to be less invasive and maybe to last longer; reduce the rate of primary failure and enable more medical specialties to participate in the creation of AVF, which can be relevant in areas underserved by vascular surgery.”
“Based on my experience, attempts to optimise perioperative haemodynamic conditions, regional blocks and endovascular technique modifications are worthwhile to improve fistula outcome and have the potential to increase the number of functional endoAVFs,” he underlined.
Yousof Al Zahrani (interventional radiologist, Riyadh, Saudi Arabia) then detailed the simplicity of his experience from learning to mastering WavelinQ in a hospital setting that caters for 2,100 beds with the expertise of 12 interventional radiologists, four neuroradiologists, two paediatric interventional radiologists and six fellows.
In pursuing an endoAVF creation programme, the team has performed 32 percutaneous procedures, with the majority of patients undergoing a WavelinQ procedure under regional anaesthesia.
“Procedural success was 85%, with successful cannulation achieved in 88% with a time to cannulation of four to eight weeks. There were no device-related complications and reinterventions were needed in five patients (18%),” he detailed.
In a session examining restoration of dysfunctional AVF, Jose M Abadal, president of the Spanish Interventional Radiology society (SERVEI; Madrid, Spain) shared his approach to percutaneous angioplasty (PTA) balloon selection based on the type of stenosis. He exhorted that the degree of stenosis was not enough of a measure, but that the type of stenosis is vital in determining the choice of device. In his centre, choice rests on a combination of medical evidence, cost containment and a clinical practice that is heavily reliant on Doppler ultrasound use. He reminded delegates that the technique of PTA is still variable, quipping “standardisation is clearly reserved for cardiologists”. Abadal stated that plain balloon angioplasty is the first choice followed by a double whammy of angioplasty then drug-eluting balloon. Ultra-high pressure balloons are the first choice and in case of recoil either these or scoring balloons are applied, with stent grafts only selected if there is a clear indication. “Ultrasound is mandatory for sizing and new Doppler ultrasound criteria will be used to determine technical success,” he noted.
Joseph Touma (vascular surgeon, Paris, France) spoke on his centre’s experience of drug-coated balloon in fistula maintenance and Luka Novosel (interventional radiologist, Zagreb, Croatia) updated on the AVF cohort of the Lutonix AV Global registry, drawing out the patient and procedural variables of the study.
In the maintenance session for dysfunctional AVF, Griveas described the access life circuit that begins with vascular access stenosis. “Drug-releasing balloons can be a useful therapeutic option for patients with AVF stenosis due to accelerated endothelial hyperplasia. The use of paclitaxel-coated balloons helps reduce the risk of restenosis of arteriovenous anastomoses and is a safe, minimally invasive and immediate solution to AVF management,” he quoted from a paper published by his group in Nephrology Dialysis Transplantation in 2020.
Jaffer opened the second day’s plenary with a general introduction around the pathology of lesions making the point that “veins are not arteries”. It is important to drill-down into why stenoses occur, he said. “Lesion characteristics can be complex. A UK expert consensus approach for managing symptomatic arteriovenous fistula (AVF) stenosis in haemodialysis patients, published in CardioVascular and Interventional Radiology in 2021, recommends that if a patient requires four or more interventions for the same stenosis in a 12-month period (or three or more in a six-month period), a multidisciplinary meeting and patient discussion on access options should be triggered. For de novo stenosis, plain balloon or high-pressure balloon angioplasty are acceptable first interventions. Bare metal stents have a place only for central region stenosis and if there is recurrence between three and 12 months, consider a drug-coated balloon,” he reported.
This was followed by Kitrou presenting on endovascular treatment of dysfunctional AVF including an algorithm option and Jamal Al Koteesh (interventional radiologist, Al Ain, United Arab Emirates) presenting cases of complex AVF lesions.
Karunanithy then described to delegates why covered stents are key to haemodialysis access salvage.
Katarzyna Kolasa (health economist, Warsaw, Poland) presented findings from a literature review to examine whether covered stents are a cost-effective choice to treat AVF stenosis in haemodialysis patients.
Setting out that only 35% of haemodialysis patients remain alive after five years of treatment, Kolasa pointed out that these survival rates remain worse than those for many common cancers.
AVF is the preferred access choice, and vascular access-related complications and interventions account for almost one-third of hospital admissions among patients receiving dialysis, she said.
To mitigate against the high economic burden associated with AVF stenosis, early consideration of additional procedures along with angioplasty in the course of treatment and postponing additional procedures until it is absolutely necessary have the greatest potential to produce long-term savings, she commented.
Identifying the clinical evidence required for budget holders to ensure funding of covered stents for AVF stenosis, Kolasa said real-world data confirming that the covered stents lower the risk of reintervention, economic modelling data showing the same findings and more such data verifying long-term outcomes for patients would be valuable tools.
“As the outcomes of haemodialysis patients are variably monitored, there is a need for country-specific data collection efforts to inform reimbursement decisions in order to improve access to treatment,” she said.
Inston and Fanelli summed up the discussions when they told Interventional News: “The ESKD summit brings together the multidisciplinary team to consider more than just procedures and devices. It approaches treatments as more than just isolated procedures, and consciously reframes these in the context of a patient’s journey. This journey may have one clinician at the centre or have multiple inputs into treatments, but it is one that has a profound impact on each individual patient and their families. We feel that the summit achieved this vision by using a patient-centred approach.”
Editor-in-chief Brian Stainken, author of this letter
Interventional News began more than 20 years ago as an effort to better cover the global interventional space, selecting news stories and other content that is not the province of peer-reported journals, but still important to the practising interventionalist. We focus on content that is relevant and on conversations that you might not hear on other channels.
I am a newly retired, USA-based interventional radiologist. I finished fellowship training in 1992 and enjoyed a practice in both clinical and academic environments. It has been a privilege and an education to watch our profession evolve over the past half-century (yes, the Society of Interventional Radiology [SIR] turns 50 this year!) As a past leader in SIR, with a leadership focus on international interventional radiology (IR), I have had a front row seat for at least half of that time, so I thought I would offer one man’s perspective on what’s better, what’s not, and what’s next. When you read this, understand my focus is our global IR community and that my opinions are not necessarily Prof Adam’s (my co-editor-in-chief), Interventional News’, or those of our representative societies. Let us start with the good news:
What’s better:
Our tools. Frankly, IR is a lot easier now because the random stent migrations, wire fractures, ‘stuck’ devices and oversized introducers are mostly a thing of the past. We even have devices for haemostasis! As a fellow, after a long lytic case, I still remember holding groins for days…This evolution in equipment has allowed our field to advance into progressively more novel and technically demanding approaches, solving more problems with less risk compared with the alternatives. But we should never fall for the fallacy that there is any relationship between introducer size and risk. As many of us know based on first-hand experience, one disadvantage of IR access approaches when compared with predicate open procedures is potential for loss of control. A poorly trained provider can do a lot of harm through a small hole. As IR becomes ever more complicated, we need to accept that our training and certification systems must evolve in parallel, on a global scale.
Our culture. Dotter’s vision has arrived. IR is for patients, not procedures. This culture becomes a progressively important bedrock as our techniques mature and tools improve. It is all too easy to apply low- or no-risk solutions. It is not just risk/benefit that matters, it is also about alternatives. Like any surgeon, when we can avoid a procedure, we must. A great example is supervised exercise for claudication. Many patients do not want it over a simple percutaneous transluminal angioplasty [PTA], but unless and until there is a proven benefit for superficial femoral artery interventions over no intervention for claudicants, we must stand down. Yes, the data may say others do it more and we will lose market share, yes the patient may go to the ‘competition’, but our culture must be about standards of practice, clinical integrity, rigorous training and professional certification. Our superpower is a cautious culture that maximises the public benefit of our tools because we put our patients first.
Imaging. Am I the only one who remembers Dr McCoy solving problems on Star Trek with his ‘wand’ thing? Look like an ultrasound probe to anyone else? I bet that McCoy had at least four years of training and demonstrated clinical imaging competency before they let him apply it to the crew of the Enterprise. In the USA, IR is the primary specialty that delivers image-guided care. As the imaging tools used to guide our solutions evolve, the fundamental need for demonstrable core imaging competency among IR providers will grow. Advances in imaging have made IR better, for sure, but that is only evident and possible if you understand what you are looking at. Excellence in IR requires excellence in imaging.
What’s not:
We can’t do it all. It was amazing to learn IR in a time when the specialty had no boundaries other than solving a problem in a better way. I am not sure what I will do with the skill sets like building endografts, cannulating pedal lymphatics, freezing prostates with five 24Fr probes, or mounting stents on balloons—by hand. At the time, it was what we had to work with. For the future, we must accept that core IR requires advanced training and certification. Subspecialised IR requires even more to establish clinical equipoise and meet our specialty’s culture of excellence. You cannot do it all. When it is outside your wheelhouse, refer. Embrace subspecialised practice. Be the best.
We are no longer alone. We should do a better job looking at the macroeconomics of disease state management. What are the least expensive, most efficacious solutions? In the USA, our payment structures and departmental hospital structures can interfere with closer collaboration among professional peers. Globally, regulators and payors or hospitals often restrict less invasive advances in care because of bias, or overly simplistic/outdated thinking. The result is that far too many open procedures are done around the world simply because the local system favours sutures over devices! We need to work together to educate stakeholders about the economics of the solutions we bring. IR is more flexible, and it is cheaper and safer when delivered by well-trained providers. We need to make our case and champion a right of access to IR care around the world.
What’s next:
Grow global training. Our existing national societies are busy working on the needs of their members as they should. But we need to accept that the ultimate success of IR as a specialty, to some degree, rests in the development of skilled providers worldwide. There are not enough interventional radiologists, and far too few training options for most young doctors interested in the field. This is not insurmountable, but our strategy must change. Rather than funnelling trainees through a few excellent centres located far from home, we must build our in-country ‘national’ training centres. Training concepts and best practice strategies should be shared among centres. Other national groups should mentor, endorse, and provide needed faculty. To do this we need money! This is where our major societies need to join with industry to create a fund/ foundation focused on improving access to quality IR worldwide through the development of in-country training centres.
Demand recognition/access/payment. Show me a country that does not recognise our peers in cardiology or vascular surgery. IR is a primary specialty with a unique competency that must be recognised. We need to focus and drive this message home, worldwide. It is time to collaborate to achieve the global goal of professional recognition.
The programme seeks to further establish interventional oncology (IO) as a “fundamental pillar within comprehensive cancer care”. IASIOS has been developed to recognize facilities that adhere to the CIRSE Standards of Quality Assurance in Interventional Oncology.
What sets IASIOS apart, the press release states, is its multi-tiered accreditation system. Facilities can earn the ‘Enrolled Seal’ by actively implementing necessary changes to meet the core criteria required for accreditation. Upon successfully demonstrating compliance with the core criteria through the IASIOS application process, facilities are awarded the ‘Accredited Seal’. For those that go above and beyond to meet both core and extended criteria, the ultimate recognition comes in the form of the Centre of Excellence Seal.
A dedicated steering board and committee has been appointed to the IASIOS programme, with further support from a network of representatives from leading IO hospitals across the globe. Moreover, with support from over 40 interventional radiology societies worldwide, the IASIOS community seeks to drive advancements in IO and patient care.
Since its public launch in 2021, IASIOS has reported positive growth. Starting with just 12 participating facilities, IASIOS has increased to 40. IASIOS Accredited Seals have been awarded to 15 centres from countries spanning Australia, France, Germany, Greece, Italy, Netherlands, Singapore, Switzerland, Turkey, and the UK. Now, in 2023, IASIOS intends to make its mark in new territories, as the press release conveys, welcoming facilities from South America, the USA, the UAE, Belgium and Ireland to its network.
Through the implementation of the membership annual benefits program, IASIOS offers a number of initiatives for career and professional development, networking, mentorship, workshops, promotion, recognition, and valuable survey opportunities, aiming to elevate the standard of care for a greater number of cancer patients worldwide.
Data on hundreds of thousands of patients who have received lower limb endovascular treatment provide confidence in paclitaxel safety. This central message from a Boston Scientific symposium at the recent Leipzig Interventional Course (LINC 2023; 6–9 June, Leipzig, Germany) was delivered a month before the US Food and Drug Administration (FDA) removed restrictions on use of paclitaxel in peripheral arterial disease (PAD) treatment.
The LINC 2023 symposium—moderated by Marianne Brodmann (University of Graz, Graz, Austria) and Koen Deloose (AZ Sint-Blasius, Dendermonde, Belgium)—saw various speakers outline existing and new data concerning the use of the Eluvia drug-eluting stent (DES) and the Ranger drug-coated balloon (DCB) in the superficial femoral artery (SFA), including four-year data from the Ranger II SFA randomised controlled trial (RCT) and several registries.
The role of RCTs in shaping clinical practice
Brodmann opened the session with a presentation on RCT data, which she described as “the pinnacle of proof”, stressing their importance in proving device performance against standard of care, and in shaping clinical guidelines.
The first RCT discussed was the Ranger II SFA RCT that assessed the Ranger DCB versus standard percutaneous transluminal angioplasty (PTA). In this single-blind, superiority trial, 376 patients were randomised 3:1.
Brodmann shared long-term follow-up results, revealing specifically three-year patency and four-year clinical safety results. The investigators “demonstrated outstanding three-year primary patency of 77% for the [Ranger] DCB and four-year freedom from clinically driven target lesion revascularisation [CD-TLR] which is greater than [that] reported in other DCB studies previously published,” she summarised.
Aside from the Ranger II results, Brodmann also informed the LINC 2023 audience about three other RCTs—COMPARE, IMPERIAL and EMINENT— and relayed their positive outcomes.
COMPARE showed similar primary patency between the low-dose Ranger and the high-dose IN.PACT DCB (Medtronic), the presenter outlined, while IMPERIAL demonstrated superior primary patency for Eluvia over Zilver PTX (Cook Medical) at 12 months, a “significant” TLR advantage at 24 months and similar safety outcomes out to five years. Brodmann continued that, in the EMINENT RCT, the Eluvia DES showed superiority in terms of efficacy compared to bare metal stents (BMS) and is the first and only DES to do so in SFA intervention.
Real-world evidence: Registries complement, and do not replace RCTs
Giovanni Torsello (St Franziskus Hospital, Münster, Germany) then shared real-world evidence on the Eluvia DES. “The real-world data are consistent with RCT results for Eluvia DES despite markedly increased lesion complexity and patient comorbidities,” he remarked.
Torsello spoke on several registries studying the Eluvia DES, including Auckland, DESAFINADO, Regal, and Münster. The studies all demonstrated around 90% primary patency for the Eluvia DES at 12 months despite often involving long lesions and high patient comorbidity. According to Torsello, the available registry data “provide more evidence and more confidence that the Eluvia RCT results are generalisable and repeatable”.
Osamu Iida (Osaka Police Hospital, Cardiovascular Division, Osaka, Japan) then shared real-world data on drug-eluting therapies from Japan, concluding that they “provide more evidence of Eluvia DES and Ranger DCB successful outcomes”.
The presenter outlined that in the CAPSICUM registry (1,097 patients), three-year follow-up showed acceptable restenosis rates for the Eluvia DES, and decreasing annual event rates for restenosis, re-occlusion and stent thrombosis.
Iida also addressed the CAPRICORN propensity-matched cohort (1,456 patients), which demonstrated significantly lower one-year restenosis rates for the Eluvia DES versus the IN.PACT DCB. He noted that this was the first study to demonstrate superiority of DES over DCB in real-world practice.
Finally, Iida shared that the PROSPECT MONSTER study (581 patients) showed that the low-dose Ranger DCB performed similarly to the high-dose IN.PACT DCB. This result was also observed in the COMPARE RCT, as Brodmann had previously noted.
Big data from big databases—PTX safety
Yann Gouëffic (Groupe Hospitalier Paris Saint Joseph, Paris, France) addressed the topic of paclitaxel safety with an overview of studies that included more than 180,000 patients, such as SWEDEPAD, VOYAGER PAD, and SAFE-PAD. He detailed that these studies all refute the findings of the 2018 Katsanos meta-analysis, by showing no difference in mortality between patients treated with either a drug-coated device or a non-drug-coated device. He closed by introducing the DETECT study, based on French national healthcare data. This study includes ~260,000 patients and, as reported by Gouëffic, it confirmed the conclusion on paclitaxel safety. The final analysis is expected later this year.
On 11 July, soon after LINC 2023, the US Food and Drug Administration (FDA) updated its guidance on the use of paclitaxel-coated devices to treat PAD, determining that additional long-term clinical data from the pivotal RCTs do not support an excess mortality risk for paclitaxel-coated devices.1
In a Boston Scientific statement released following the FDA announcement, chief medical officer Michael Jaff commented that the update recognises the safety and efficacy of devices such as Eluvia and Ranger, “both of which have demonstrated excellent safety profiles and very low revascularisation rates in the hundreds and thousands of patients treated worldwide with these devices”.2
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) added to the subject in an online editorial dated 12 July, underscoring that re-analysis of old data and new outcomes data do not support a link between paclitaxel-coated balloons and paclitaxel-eluting stents and mortality. On this basis, CIRSE encourages the use of these devices for treating PAD in femoropopliteal disease, relying on their published efficacy.3
References:
UPDATE: Paclitaxel-Coated Devices to Treat Peripheral Arterial Disease Unlikely to Increase Risk of Mortality – Letter to Health Care Providers | FDA
News Releases – Boston Scientific: Boston Scientific Position on FDA Update About Use of Paclitaxel-Coated Devices to Treat Peripheral Arterial Disease
Müller-Hülsbeck S, Fanelli F, Haage P, et al. Re-analysis of old data and new outcomes data do not support a link between paclitaxel-coated balloons and paclitaxel-eluting stents and mortality: these devices should be used in PAD (peripheral arterial disease) treatment in femoropopliteal disease on the basis of their published efficacy. Cardiovasc Intervent Radiol. 2023;46:977–980. https://doi.org/10.1007/s00270-023-03507-w
For information purposes only. The content of this article/publication is under the sole responsibility of its author/publisher and does not represent the opinion of BSC. PI-1656303-AA
In 2010, the UK Royal College of Radiologists (RCR) with the Royal College of Paediatrics and Child Health (RCPCH) published a report focused on how to improve paediatric interventional radiology (PIR) services. In June 2023, an updated report was published, this time by the RCR on its own. The purpose of the report is to “identify how PIR services can be expanded and improved” and “suggest solutions” that can be enacted by commissioners, healthcare leaders and hospitals. The conclusion of the 2023 report states that “the 2010 report recognised the value and importance of PIR to the National Health Service (NHS) and made recommendations to grow and support PIR but has not driven change”. In light of this, what do the updated recommendations suggest is needed to drive change successfully this time round?
The introduction to the report seeks to clarify that “PIR is more than just IR in children, and requires specific skills, staff and infrastructure to be done right”. In spite of this, according to the latest RCR workforce census, the UK has 743 consultant interventional radiologists, but less than 20 of those are formal PIR posts. The report goes on to state how the majority of these posts are in London, meaning children and families across most of the UK do not have easy access to PIR services. The RCR’s goal in providing an update to the joint report is to finally “bring PIR service provision into the 21st century”.
PIR in the UK in 2023 The main body of the report begins by listing the advantages to making PIR services fit for purpose, which will bring about faster recovery times through less invasive procedures, and therefore the use of fewer inpatient beds and other resources, as well as a more manageable experience for the patient and their family. The report further informs readers that there is, roughly, only one paediatric interventional radiologist per million children in the UK, to the USA’s one per 342,000 children. Moreover, it states, there is roughly one adult interventional radiologist per 74,000 adults in the UK, yet even this is jeopardised by the “[worrying]” shortage of radiologists generally.
The report also outlines how PIR services are currently delivered, and that a variety of models are used. In a small number of hospitals, the entire PIR service is delivered by paediatric interventional radiologists. In others, some procedures are carried out by adult interventional radiologists, some by paediatric diagnostic radiologists, and others by paediatric interventional radiologists. There are further centres where PIR services are either carried outby adult interventional radiologists, or commissioned to a paediatric specialist at another centre. Beyond this, there are centres where there is no provision in the wider region beyond an adult IR, which can take care of some procedures, but not all.
Acknowledging that some progress has been made Although the report laments that the 2010 RCR/RCPCH document “has not driven change”, it acknowledges that the latter may have had a hand in bringing about certain recent advances that the RCR “welcome[s]”. These include a new IR training post at Birmingham Children’s Hospital (Birmingham, UK),the second national PIR training post in the UK, and the recent integration of PIR into the adult IR training programme at Guy’s and St Thomas’ and the Evelina London Children’s Hospitals (London, UK). Recently, additional PIR posts have been created at Leeds Children’s Hospital(Leeds, UK), Alder Hey Children’s Hospital (Liverpool, UK), and The Royal Hospital for Children (Glasgow, UK).Beyond this, the RCR has collaborated with the British Society of Interventional Radiology (BSIR)’s PIR special interest group on “the development of a rolling PIR cross-skilling programme, aimed at adult IRs, paediatric diagnostic radiologists, surgeons and anaesthetists”. Nevertheless, the report proceeds to question whether PIR can become centrally funded “so organisations do not view it as an unfeasible financial burden”, which is a current barrier to these positive steps being more widespread.
Solutions set out in the report In terms of recommended action from various colleges and governmental bodies, the 2023 report echoes much of that which was stipulated 13years prior. Firstly, to address the shortfall in numbers of PIR consultants, the report advocates for doubling the PIR consultant posts available every five years, so that there are 96 in the UK by 2038. Linked to this, cross-skilling, such as has been discussed in collaboration with BSIR, is also key, the RCR believes, as there are insufficient numbers of doctors across radiology and IR, among other specialties, which can impact existing PIR care offered under the various models enumerated above. Adult IR, paediatric surgeons, anaesthetists, radiographers, and nurses could be trained in certain areas of PIR care provision to help compensate for inadequate numbers of PIR service-providing consultants.
The report further recommends that national training bodies such as Health Education England could provide funding for PIR trainee posts, open to final-year(ST6) trainees in IR or paediatric radiology. There is also a need “to consider how to better integrate PIR into existing training curricula” to address the problem of the “relative invisibility” of PIR to medical students and junior doctors. Regarding how to deliver a PIR service, the report emphasises the need for a “clear PIR service delivery policy in all hospitals that offer care to children”. It adds that “unambiguous arrangements must be in place for the early referral of children requiring PIR care that cannot be provided locally in a timely manner”. In order to achieve this, PIR must be included in treatment algorithms, local service models and referral pathways, in cooperation with other specialties such as anaesthesia and paediatric surgery.
Speaking to Interventional News, report author and PIR consultant at Great Ormond Street Hospital (London, UK), Alex Barnacle, gave her take on which recommendations will be the easiest to achieve. She believes that PIR in the UK is most likely to see an increase soon in the number of PIR practitioners through cross-skilling of healthcare professionals, and training capacity in PIR, as well as some refinements in how data is collected. On the flip side, substantially increasing PIR consultant post numbers poses the greatest challenge.
Asked to comment on the issues outlined in the report, president of the RCR, Katharine Halliday said: “For some of our sickest children, PIR can be a lifeline, providing minimally invasive treatment and reducing lengthy hospital visits. But too few children, whose lives could be improved through these life-changing procedures, do not have access. We are urging the [UK]Government and trusts to take note: this is highly effective, cost-saving care that desperately needs to be resourced.”
Yuji Okuno (Okuno Clinic, Tokyo, Japan) shared with delegate sat the European Conference on Embolotherapy (ET; 21–24 June, Valencia, Spain) an analysis of the best embolization approaches to certain sports injuries associated with overuse.
Okuno began his presentation by defining overuse sports injury as “an injury occurring in the absence of a single, identifiable traumatic cause”. The priorities when it comes to treating these injuries are achieving reliable results and the patient being able to return to their activity quickly, as often, it is high-level athletes who are affected. However, these injuries are usually quite difficult to manage with usual conservative treatment, such as steroid or stem cell injections, and therefore “good indications” for musculoskeletal (MSK) embolization. This is because of the treatment’s minimally invasive nature, which limits patients’ recovery time, Okuno clarified.
Among the overuse sports injuries that can be best treated with embolization, according to Okuno, are tennis elbow, jumper’s knee, Achilles tendonitis, hip pain as a result of hamstring injury, and pain in the lumbar region from spondylolysis. To begin treating these patients, Okuno set out that first, he will evaluate using magnetic resonance imaging (MRI) or ultrasound to “confirm the presence of the hypervascular region”. For the first three types of injury, Okuno shared with delegates that soluble gelatin microspheres (100–300 micrometres)are a good, “safe”, embolic choice. For the hip, lumbar region, and stress fractures, the speaker conveyed how he “always” uses imipenem/cilastatin. A permanent microsphere is an option for tennis elbow or jumper’s knee. During the procedures, Okuno continued, there are two endpoints—the imaging endpoint and the physical endpoint, or the disappearance or decrease in localised “painful tenderness” at the injury site.
A key takeaway Okuno wished to give his audience was that the evidence shows that, when doing lumbar embolization, some particles can cause the nerve root or spinal cord to necrose. This is the case even for some temporary materials. Therefore, imipenem is the only embolic he would recommend.
Erik Cressman (MD Anderson Cancer Center, Houston, USA) took to the podium, also at 2023 Global Embolization Oncology Symposium (GEST, 18–21 May, New York City, USA), to dive into why tumour ‘temperature’ matters—explaining what the terminology refers to, and its significance for patient treatment.
He first addressed how cancer is “eventual failure of the immune system”—depending on the source, Cressman explained that a single cell’s DNA can take “10,000 hits per day”. Of our roughly 100 trillion cells, five billion are replaced everyday, leading the presenter to posit that “on the one hand, it is amazing that we are not all sitting here with cancer, while on the other hand, it is amazing that the immune system works as well as it does”. Not all the cell damage that occurs leads to a tumour, but unfortunately, natural selection is at work in damaged or unregulated cells, and Cressman added how the selection process favours scenarios that evade or suppress immune surveillance.
Next, the speaker alluded to the “mixed bag” that is immunotherapy, which, while yielding “some inspiring success stories”, it also fails, which can be for a number of reasons. “It isa complicated thing,” he summarised, elaborating that some of the failures are “spectacular” in how they “unleash the immune system”. The older immunosuppressant drugs such as steroids are often not specific enough in responding to unregulated cell proliferation. Now, Cressman expanded, “we have these very highly specific antibodies that have a long-circulating half-life, [which you might only need]once every month or once every three months”. The downside of this type of immunotherapy is that “you are going to be hit with a high bill.
“The concept of an immunoscore to assess the tumours when we are talking about hot and cold” is well over a decade old, Cressman continued, coming to the pivotal focus of his presentation. The speaker referred to Galon and Bruni’s 2019 review to unpack this concept and “look at what is going on at the centre of the tumour and at the margin”. A low immunoscore correlates with a low response to T-cell checkpoint inhibition, Cressman stated, proceeding to celebrate that the prognostic value of immunoscore is “better than much of what we were taught”.
The presenter then showed delegates microscope images of hot versus cold tumours, where hot means a lot of immune cells throughout and cold, not being able to see any. He also showed the audience how “excluded” tumours are those that have a lot of immune cells, but which are yet to penetrate the tumour itself. “Suppressed” means there are some immune cells, “not particularly excluded”, but which do not function as typical immune cells.
“To summarise, the hot tumours have a high degree of T-cell and cytotoxic T-cell infiltration, and checkpoint activation is clearly going on”. Checkpoint inhibitors have a “greater likelihood of success” in these tumours, Cressman set out. Immunosuppressed tumour cells with an intermediate immunoscore have “poor, albeit not absent” T-cells and cytotoxic T-cell infiltration, and the presence of soluble inhibitory mediators, as well as T-cell checkpoints. There is a “modest response to immunotherapies” in these tumours. Immune-excluded tumours have “no T-cell infiltration inside the tumour bed and accumulation of T-cells at the tumour border”, as well as abnormal vasculature and hypoxia, and they yield a poor response when immunotherapies are used. “Cold” tumours have no T-cells either within or at the tumour edges, and there is failed T-cell priming, leading to poor response from immunotherapies.
“So, what can you do to improve outcomes? You can use image-guided injection of some of these antibodies to ramp up the immune system locally”, Cressman suggested, listing normalising the vascularity by triggering angiogenesis, addressing metabolism, restoring a normal pH as acidity is immunosuppressive, depleting immune-suppressive cell populations, and implementing a “combination of all of the above”, as additional strategies.
“Even [in Singapore], healthcare costs are spiralling, so we are also learning how to be prudent.” Farah Gillan Irani is an Indian-born and educated interventional radiologist who has practised in Singapore since 2009. She has been a principal investigator in a drug-eluting balloon (DEB) angioplasty trial, a reviewer for CardioVascular Interventional Radiology and the Journal of Interventional Radiology for the last 10 years, and is vice chair of the cardiovascular interventional radiology (IR) subsection of the Singapore Radiological Society (SRS). She charts the progress in IR that she has observed in South East Asia and the Indian subcontinent to Interventional News, explains the value of fellowships abroad, and imparts her passion for extreme climbing and cycling pursuits.
What attracted you to a career in IR? During my training, IR in India was a very nascent field and we did not have much exposure to its enormous potential. Having completed my finals, I happened to attend an IR conference where I heard Dr Sundeep Punamiya speak. The science he presented, his clarity of thought and depth of knowledge about this radiology subspecialty completely drew me in. Having wanted to be a surgeon, I wanted to work with my hands and have direct patient contact. In IR, I found the happy medium of being in one of the most rapidly innovating fields of medicine with the ability to alleviate patient suffering through minimally invasive procedures.
Who were your mentors? Prof Andreas Adam and Dr Tarun Sabharwal from Guy’s and St Thomas’ Hospital (London, UK), Prof Afshin Gangi from the University of Strasbourg (Strasbourg, France), and Prof Bien Soo Tan from Singapore General Hospital (Singapore).
Could you describe a particularly memorable case of yours? Sometimes it is not the most technically challenging case or the thrill of using a new device that stays with you, but the impact of the simplest procedure on a patient’s outcome. I was on call and the team got called in for a massive gastrointestinal bleed in a62-year-old patient with a duodenal ulcer which, in spite of clipping, continued to bleed. The patient was in haemorrhagic shock with three inotropes and on his third round of the massive blood transfusion protocol. In the chaos of treating a very unwell patient, the IR nurse and radiographers maintained their calm and prepped the patient. A simple gastroduodenal artery embolization using glue and coils stopped the bleed 20minutes after accessing the femoral artery to closure. Following a short hospital stay he was discharged home, and then came to see us in clinic ever so grateful. This case remains with me as it shows that our simple minimally invasive IR procedures are highly effective and that teamwork saves patients’ lives.
How does practising in India compare to practising in Singapore? I have not worked as a consultant IR in India and hence, I cannot compare the practice in these two very different countries. India is a huge country with great disparities in wealth and access to healthcare. In rural India, the health infrastructure mainly caters to family medicine with just basic services available. While, in large urban cities, state-of-the-art IR services are available, however affordability of IR kit can put many procedures out of reach. This is in contrast to Singapore, which has a small population and one of the best healthcare systems in the world. The latest imaging equipment is readily available, able to use these expensive devices in our patients. Yet, even here, healthcare costs are spiralling, so we are also learning how to be prudent. Luckily, IR is also now starting to be recognised as a speciality in its own right in India and there are several IR fellowships available to train the next generation.
Credits: NB Illustration/Andy Watt
What are the priorities for the IR subsection of the Singapore Radiological Society (SRS), of which you are currently vice chair? What challenges does IR face in Singapore and your wider region? Minimally invasive IR procedures are front and centre and critical to the running of any major acute hospital, but many of the public do not know who we are and what IR is about. As part of the IR subsection, public education has been part of our goal. This year, we want to extend that outreach to medical students early in their career so that our field is recognised, and we can attract the brightest and most talented young people into our fold.
IR is also now recognised as a Chapter in the Singaporean College of Radiologists (CRS) under the Academy of Medicine Singapore. We are working with the College to get subspecialty recognition by the Singapore Medical Council and Ministry of Health. On a related note, it is gratifying to see that IR is now practised at a high level in Thailand, Malaysia, Vietnam and has a presence in Bangladesh, Myanmar, Mongolia, and even Cambodia. The latter is thanks to the outreach programmes organised by the Asia Pacific Society of Cardiovascular and Interventional Radiology.
“It is gratifying to see that IR is now practised at a high level in Thailand, Malaysia,Vietnam.”
You have been a reviewer for CVIR for the last 10 years? What have you learned through doing this? It has been an amazing journey. As a reviewer, you geta ring-side seat observing the amazing innovation in your field and delve into the depths of various aspects of anatomy, physiology, imaging and new devices. Being a reviewer carries responsibility. As a gate keeper for the wider IR community, you need to make sure that the science is sound, safe, truthful, verifiable and beneficial to patients, doctors and healthcare systems. As a reviewer, I have gained immense knowledge and it has inspired me to undertake research of my own.
You were principal investigator for a randomised trial comparing drug-eluting balloon angioplasty with conventional angioplasty for haemodialysis arteriovenous fistula or arteriovenous graft stenoses. What led you to become involved and what did you take away from the trial? In Singapore, we have a very high incidence of renal failure for which many patients depend on long-term haemodialysis, as our renal transplantation numbers are low due to a lack of organs. Repeated and frequent interventions to maintain access circuit patency is costly. Hence, when drug-eluting balloons were introduced, our team decided to evaluate whether these devices truly increased duration of lesion and circuit patency and reduced healthcare costs. Along with our renal medicine physicians and vascular surgery colleagues, we designed and undertook this trial. Running trials is hard work and requires input from many people. Research co-ordinators, statisticians and allied health staff are just as important as the clinicians. As principal investigator, I was but a representative of the amazing and dedicated team. The adage “it takes a village to raise a child” is very applicable.
You undertook fellowships in London, Strasbourg and Toronto. What advice would you give to (interventional) radiologists-in-training who are considering spending time in hospitals abroad? I would highly recommend that everyone does a fellowship abroad. The wealth of experience gained is immeasurable. You are exposed to a different system of medicine and are able to take ideas back to your own practice. It also helps you appreciate the attributes of your own system. You learn different ways of doing the same procedure and these experiences help you formulate your own best way of doing it. On a personal level, you are exposed to a different culture which you need to respect, and you are out of your comfort zone, so the experience teaches you about your own strengths and weaknesses. It is an important lesson in life and just not medicine.
What are your hobbies and interests outside of medicine? I enjoy sports, and these days, I am into cycling, the gym and golf (which I have recently taken up). Singapore General Hospital celebrated its bicentenary in 2021, and as part of the celebrations, we cycled200km around Singapore to raise funding for our patients. I also enjoy hiking and trekking and have been lucky to have undertaken trips in the Americas, Africa, Europe and Asia. I was recently introduced to via ferratas, which I find thrilling; I have done the one in Kinabalu and one in the Dolomites. Being a Parsee, food is an integral part of our culture. Living in Singapore—a food lover’s paradise—I enjoy discovering, and eating at, amazing Hawker Centre stalls as well as the gourmet Michelin Star restaurants. I enjoy cooking and one of my goals is to do a gourmet cookery course.
Instylla, a company developing next-generation liquid embolics for peripheral vascular embolotherapy, today announced the closing of a US$30 million financing round.
This financing round was led by new investor, Delos Capital, with continued participation from the investor syndicate of Excelestar Ventures, Ascension Ventures, Catalyst Health Ventures, Amed Ventures, Sparta Group, and Incept. The funds from this financing are anticipated to see Instylla through the ongoing prospective clinical trials and early commercialisation.
“At Instylla, we are executing two large pivotal clinical trials in North America in pursuit of our two initial indications for the embolization of hypervascular tumours and peripheral arterial bleeds. The funds will allow us to complete the clinical trials and prepare for the commercialisation of Embrace Hydrogel Embolic System (HES) from Instylla. “We are excited to have Delos Capital join our strong group of healthcare investors who share our values,” said Amar Sawhney, CEO of Instylla and managing director of Incept.
The Instylla HES hypervascular tumour pivotal study is currently enrolling patients in the US and Canada to evaluate the safety and effectiveness of the Instylla HES compared with standard of care transcatheter arterial embolization or transcatheter arterial chemoembolization for the vascular occlusion of hypervascular tumours. The HALT Study was recently launched in the US and is continuing to enrol patients to study the safety and effectiveness of Embrace HES for the embolization of arterial bleeding in solid organs and peripheral arteries.
As part of this round of financing, Henry Chen, Managing Partner, Delos Capital has joined the Instylla board of directors. “Instylla has demonstrated impressive progress, having already advanced its next-generation liquid embolic technology to human clinical studies. We are honoured and thrilled to support Instylla as it continues developing breakthrough solutions that will meaningfully improve patient outcomes,” said Henry Chen.
MedAlliance has announced completion of patient enrolment in the SAVE clinical trial with the Selution Sustained Limus Release (SLR) 018 drug-eluting balloon (DEB) for the treatment of failed arteriovenous fistulas (AVFs) in renal dialysis patients. Selution SLR is a “novel sirolimus-eluting balloon that provides a controlled sustained release of drug, similar to a drug-eluting stent (DES)”, states a press release.
SAVE is a prospective multi-centre, single-blinded, randomised controlled trial. A total of 84 patients have been randomised to either standard high-pressure balloon angioplasty followed by local application of Selution SLR or high-pressure balloon angioplasty with no further lesion treatment. Subjects have been recruited at three sites in Europe and Singapore and are being followed up to 24 months. Endpoints of the study are primary patency at six months with angiographic follow up and freedom from serious adverse events at 30 days. Major secondary endpoints at six months are clinical success, freedom from serious adverse events, late lumen loss and binary vessel restenosis.
“We very much look forward to the analysis of the primary endpoint of this important trial at six months, as this is the first prospective randomised trial of a sirolimus-coated balloon in AVF patients with angiographic follow up. Furthermore, we have also measured fistula volume flow rates, which is another key index of failing or maintained fistula function. I thank MedAlliance for initiating a trial in this difficult patient population,” commented principal investigator (PI) Konstantinos Katsanos (Patras University Hospital, Patras, Greece).
“MedAlliance continues to invest in meaningful clinical trials to evaluate the safety and efficacy of Selution SLR in different patient populations”, added Jeffrey B Jump, chairman and CEO of MedAlliance. “Patients on dialysis rely on access to receive their treatment: they call this their ‘lifeline’. An AVF is considered the gold standard for haemodialysis access; however, it sometimes requires ongoing angioplasty. This is the first randomised study evaluating Selution SLR in stenotic lesions in AVF.”
MedAlliance was the first drug-eluting balloon company to receive FDA reakthrough Designation status, the press release continues. Currently three investigational device exemption (IDE) clinical studies are evaluating Selution SLR in the USA: in chronic limb-threatening ischaemia (CLTI) patients with below-the-knee (BTK) disease; superficial femoral artery (SFA) / proximal popliteal artery (PPA); and coronary in-stent restenosis (ISR). In addition, MedAlliance received IDE approval for de novo coronary artery lesions in January 2023. Selution SLR was awarded CE Mark Approval for the treatment of coronary artery disease in May 2020. This complements the substantial experience that the company has gained with the SELUTION DeNovo and SUCCESS trials in Europe and SELUTION SFA in Japan.
MedAlliance’s “unique DEB technology” involves “microreservoirs” which contain a combination of biodegradable polymer intermixed with the anti-restenotic drug sirolimus, applied as a coating on the surface of an angioplasty balloon. These provide controlled and sustained release of the drug for up to 90 days. MedAlliance’s proprietary cell adherent technology (CAT) enables the microreservoirs to be coated onto balloons and efficiently transferred to adhere to the vessel lumen when delivered via expansion of the balloon, the press release notes finally.
Microbot Medical, the developer of the LIBERTY Robotic Surgical System, the first single-use endovascular robotic system, today announces the expansion of its global team of experts supporting the company as scientific advisory board (SAB) members, with Francois H Cornelis joining Microbot’s SAB.
Cornelis is an interventional radiologist who specialises in neuro interventions and image-guided minimally invasive therapies that allow for pain palliation and tumour control in the bones and spine. Professor Cornelis uses a variety of technologies to treat tumours and cancer-related pain, such as radiofrequency and microwave energy, cryotherapy, focused ultrasound, and electroporation, as well as image-guided modalities, including navigation software, magnetic resonance imaging (MRI), robotics, and positron emission tomography and computed tomography (PET-CT)-guided procedures. He is pursuing research, mainly into intra-arterial therapies for brain tumours and in the fields of mentoplasty, osteoplasty, and fixation, which help reinforce bones to reduce pain.
Cornelis received his MD in 2003 and completed his radiology training and his fellowship in 2008 and 2010, respectively, at the University of Bordeaux in France. He stayed on the faculty, with appointments in Radiology at the Bergonié Institute (2010) and the University of Bordeaux (2012). He was appointed as a tenured professor of radiology in France in 2017 and served as chief of the department of interventional radiology and oncology at the Sorbonne University in Paris before heading to New York.
“The support and endorsement of a global leader such as Cornelis is a vote of confidence and a great honour for the company. Cornelis joins a team of global leaders in their fields that are already serving as members of our SAB,” said Eyal Morag, chief medical officer of Microbot Medical. “The significant contributions of our SAB members to the company, including their participation in our pre-clinical studies, is expected to greatly support our forthcoming plans, including clinical trials and collaborations with leading medical centres worldwide.”
Xeltis has announced the closing of an additional €12.5 million in funding from the European Innovation Council (EIC) Fund, set up by the European Commission. Today’s extension from EIC and the closure of the Series D2 financing round announced in February 2023, brings the total amount raised to €44.5 million.
The additional funding will support the continued clinical development of Xeltis’ “transformative implants”, says a press release. In April 2023, Xeltis shared “highly-encouraging” six-month data from its first-in-human (FIH) aXess vascular graft trial. An ongoing pivotal trial for aXess is enrolling patients across Europe. Moreover, the EIC Accelerator funding will be used to advance Xeltis’ coronary artery bypass graft (CABG) program.
Svetoslava Georgivea, chair of the EIC Fund Board said: “It is the ambition of the European Innovation Council (EIC) Fund to invest in European companies that develop cutting-edge technologies with high impact. Xeltis, with their restorative medical device technology is an excellent example of such a company, which the EIC Fund invests in to support their potential to scale and grow their business.”
Eliane Schutte, CEO of Xeltis, commented: “Securing this additional investment from the EIC is an important validator of Xeltis’ work to enable a better standard of care for patients with major life-threatening diseases through our transformative vascular implants. We look forward to providing updates from our pivotal aXess trial in due course, with enrollment progressing well.”
In December 2021, Xeltis secured €15 million from the EIC Accelerator, part of the European Commission’s Horizon Europe program, following a rigorous selection process. The €15 million consists of a €2.5 million grant and a €12.5 million equity investment through the EIC Fund. The company is one of a select group of European start-up companies funded under the program to help bring promising technologies to market, the release concludes.
“We need to eliminate symptoms as fast as possible—it is not OK just to make things a little better,” says Rick de Graaf (Clinical Centre of Friedrichshafen, Friedrichshafen, Germany), setting out why intervention in acute deep vein thrombosis (DVT) is important. De Graaf cites quality of life and economic burden as key factors. “That does not allow us to be too risky,” he continues, commenting that avoiding complications, such as bleeding or recurrent DVT are fundamental to any intervention.
According to De Graaf it does not make sense to use a device that takes out, 50, 60 or 70% of thrombus. He argues that full removal should be the ultimate strategy to optimise clinical outcome.
De Graaf cites ClotTriever (Inari Medical) as one such device that makes fast, safe and efficient thrombectomy possible. Outcomes of the device in a real-world DVT population have been demonstrated through the ongoing CLOUT registry, a 500-patient, prospective, multicentre, all-comer study, taking place at 43 centres across the USA, making it the largest mechanical thrombectomy study in the field of DVT. Results have so far been shown out to 30 days, with follow-up planned out to two years. The trial’s primary endpoint is technical success, defined as complete or near-complete (>75%) removal of thrombus by core lab-assessed Marder score.
“That is spectacularly high when you compare that to other devices and benchmarks,” says David Dexter (Sentara Vascular Specialists, Norfolk, USA) an investigator in the study, of the primary endpoint goal. However, he offers the view that investigators saw ClotTriever as likely to hit this target, “because of its purely mechanical nature in the acute phase and maybe in the subacute arm”.
Results out to 30 days, presented at The VEINS 2022 (30–31 October, Las Vegas, USA), demonstrate that the primary endpoint (>75% thrombus removal), was achieved in 91.2% of patients, while nearly two thirds of patients had 100% of clot removed. The intermediate number of 90% clot removal was seen in around 70% of patients.
Safety was also assessed, and the study has shown a serious adverse event (SAE) rate of 0.2%. Added to this, most patients were treated in a single session (99.4%), with minimal blood loss (40ml) and minimal use of thrombolytic therapy (0.4%). From an improvement standpoint, Dexter says, the first goal is restoration of flow. At baseline only 27.6% of patients in CLOUT had flow, but 30 days post-treatment, 85% of patients had some or all flow restored.
For Steven Abramowitz (Medstar Health, Washington DC, USA), putting these data in context with previously published studies is an important next step to guide future treatment decisions, in line with the universal goal to “function in an evidence-based world”. To achieve this aim, data from CLOUT have been compared to those from the ATTRACT trial, which assessed the use of pharmacomechanical catheter-directed thrombolysis, in a propensity-matched study. “ATTRACT is one of the fundamental reference trials in the USA, and I think globally, for guiding intervention for DVT,” says Abramowitz. The analysis looked at 153 pairs of similarly matched patients within the two trials based on 11 baseline covariates.
Results show better thrombus extraction with the ClotTriever system, with nearly 88% of the CLOUT patients achieving thrombus clearance ≥75%, compared to 66% who received an intervention in ATTRACT. There was also a significant difference in the number of patients with 100% thrombus clearance, totalling 58% in CLOUT, compared to 30% in ATTRACT. The analysis also compared reduction in Villalta Score—an indicator of the severity of post-thrombotic syndrome in lower-extremity DVT—recorded in the two trials, showing a significant decrease at 30 days in CLOUT with 27% of patients with a Villalta Score ≥5 vs. 40% in ATTRACT.
“Propensity matched analysis shows us that contemporary interventional strategies with ClotTriever do stand their ground and have comparable, if not potentially better results than those patients treated with interventional options available at the time of ATTRACT enrolment,” says Abramowitz.
Merit Medical has announced that is has completed enrolment in its WRAPSODY Arteriovenous Access Efficacy (WAVE) pivotal study. Merit’s WAVE study is a prospective, randomised, controlled, multicentre study comparing the Merit WRAPSODY cell-impermeable endoprosthesis (CIE) to percutaneous transluminal angioplasty (PTA) for treatment of stenosis/occlusion in the venous outflow circuit in patients undergoing haemodialysis.
Creation and maintenance of an arteriovenous fistula or graft (AVF/AVG) to achieve long-term vascular access is required for patients undergoing haemodialysis. However, progressive stenosis and/or occlusion of blood vessels where the AVF and AVG are located can prevent delivery of haemodialysis, which can have life-threatening consequences. WRAPSODY was developed to help physicians treat patients with stenosis/occlusion in the vessels used for haemodialysis.
The WAVE study enrolled 244 patients with AVFs and 113 patients with AVGs across sites in Brazil, Canada, the UK, and the USA. Merit intends to collect safety and efficacy outcomes throughout the study follow-up period. Merit anticipates filing primary outcomes with the US. Food and Drug Administration (FDA) for premarket approval (PMA) after six months post-enrolment completion. Merit intends to follow patients enrolled in the WAVE study for 24 months following completion of enrolment.
“Given the inadequacy of therapeutic options to maintain vascular access in haemodialysis patients, understanding WRAPSODY’s overall performance—due to its unique cell-impermeable stent covering in helping to maintain AV fistulas and grafts—is of high value to physicians and the scientific community,” says Mahmood K Razavi, medical director of clinical research at St Joseph Heart and Vascular Center (Orange, USA), co-principal investigator of the WAVE study, and paid consultant of Merit.
“The WAVE study has now completed the anticipated recruitment thanks to the patients that participated and to the hard work of all the global investigators and their respective teams,” says Rob Jones, consultant interventional radiologist at Queen Elizabeth Hospital Birmingham (Birmingham, England), co-principal investigator of the WAVE study, and paid consultant of Merit. “I am looking forward to the data analysis and the next step in this device’s journey in providing definitive management to AV access patients.”
“Enrolment of the last patients in the WAVE study represents an important milestone,” says Fred P Lampropoulos, Merit’s chairman and CEO. “We believe it will enable us to provide critical insight to our physician partners and support our submission of a PMA application to the Food and Drug Administration.”
AngioDynamics has announced the completion of enrolment and final treatment in its pivotal study of the NanoKnife system for ablation of prostate tissue in an intermediate-risk patient population (PRESERVE). The PRESERVE study was initiated by AngioDynamics. in partnership with the Society of Urologic Oncology Clinical Trials Consortium (SUO-CTC).
“The PRESERVE study demonstrates AngioDynamics’ commitment to innovating care delivery,” said Juan Carlos Serna, AngioDynamics senior vice president of clinical and scientific affairs. “As we mark the completion of enrolment and final treatment in the study, we take another important step towards demonstrating the NanoKnife system’s ability to expand treatment options for patients with intermediate-risk prostate cancer and advance our mission to improve patient quality of life. We appreciate the support provided by our PRESERVE study sites and the partnership with the SUO-CTC team in this important effort.”
The co-principal investigators leading the study are Jonathan Coleman, urologic surgeon at Memorial Sloan Kettering Cancer Center (New York, USA), and Arvin George, urologic surgeon at University of Michigan (Ann Arbor, USA). The PRESERVE study will have its primary endpoint analysis at 12 months following treatment.
“As diagnostic tools develop to allow earlier identification and localisation of clinically significant forms of prostate cancer, there is a matching need to establish effective forms of treatment that target the disease and preserve patients’ quality of life. Evidence is growing to support the use of partial gland ablation for prostate cancer as a reasonable alternative treatment strategy in carefully selected patients. The PRESERVE study, studying the efficacy of irreversible electroporation (IRE) with the NanoKnife system from AngioDynamics in men with intermediate-risk tumours (Gleason Grade 3+4 and 4+3), will help to address further the validity of this therapeutic approach using a treatment, which is well tolerated and easy to apply in prostate tissue,” said Coleman.
The NanoKnife system utilises irreversible electroporation (IRE) technology to destroy targeted tissue effectively, delivering precise treatment margins while preserving vital structures by retaining the structural integrity of the targeted tissue. The delivery of non-thermal energy allows for the preservation of the extracellular matrix, facilitating post-ablation histological and functional tissue regeneration. To learn more and view risk information, visit NanoKnife.com.
The PRESERVE study’s primary objectives are determining the NanoKnife system’s ablation effectiveness by measuring the negative in-field biopsy rate at 12 months and determining the NanoKnife system’s procedural and post-procedural safety profile by evaluating adverse event incidence, type and severity through 12 months. The study enrolled and treated 121 patients in 17 facilities across the USA. Learn more about PRESERVE at angiodynamics.com/studies/preserve.
Alucent Biomedical has announced that the US Food and Drug Administration (FDA) granted an investigational device exemption (IDE) for a US clinical study of AlucentNVS, a unique light-activated, drug-coated balloon catheter technology.
AlucentNVS combines an intravascular device with a photochemical process to link structural proteins in the wall of a blood vessel to control vascular remodelling. The intervention is designed to promote patency of the vessel’s lumen and establish sustained improvement of blood flow. AlucentNVS is also designed to retain the natural functionality and flexibility of the vascular wall, while avoiding traditional complications of inserting permanent implants.
“IDE approval by the FDA’s Division of Coronary and Peripheral Interventional Devices is another validation of our novel approach to treating vascular disease,” said Myles Greenberg, CEO of Alucent Biomedical. “AlucentNVS technology is poised to change the standard of care in treating patients undergoing life- and limb-saving vascular procedures.”
AlucentNVS is currently being evaluated in two feasibility trials in Australia and Poland, also examining its use in treating peripheral artery disease (PAD) and promoting the maturation of arteriovenous fistulas (AVF) for patients requiring haemodialysis. Enrolment in those trials is expected to conclude by the end of 2023.
Authors from King’s College Hospital (London, UK) have recently published a letter in Clinical Radiology detailing their centre’s experience after 25 years of day-case interventional radiology (IR) services. The King’s experience, according to the title of the response letter, has been “worth the effort”, which corresponding author Nuran Seneviratne et al explain is because day-case IR at King’s has proven to be “efficient, [to reduce] patient anxiety, [optimise] the role of the interventional radiologists in elective and emergency preassessment, [maintain] patient safety” and to pave the way for treating a “broader selection of patients” through a wider variety of procedures.
Seneviratne and colleagues responded to a paper published earlier in 2023, also in Clinical Radiology, by Lakshminarayan et al, which makes the case for providing IR care in a day-case setup. Their reasoning for advocating for this model is, as outlined in the paper’s introduction, that IR has, over time, become less invasive, which “[enables] rapid recovery, [expediting] ambulation and [promoting] same-day discharge”. This model, Lakshminarayan et al detail, can improve patient experience and cost-effectiveness.
The authors of the King’s letter outline that they wish to “offer encouragement” to other hospitals motivated to establish or improve their day-case unit to profit from the advantages it can offer, as set out in Lakshminarayan’s paper. At King’s College Hospital, theirs is a “dedicated 10-bedded, nurse-led day-case interventional unit”, the letter conveys. It “initially focused on peripheral angiography, vascular access, liver biopsy, and percutaneous drainage work, [but] the service has now expanded to encompass a broad range of arterial and venous interventions, a large hepatobiliary service, and interventional oncology procedures”. The authors add that since its foundation in 1997, the unit has carried out over 2,500 percutaneous liver biopsies.
The letter goes on to include details of the vascular procedure data the unit gathered to assess the value of the unit. “The number of procedures increased steadily over time, andthe proportion of interventional to purely diagnostic angiography also increased. There were also significant cost benefits compared to admission (£131.15 versus £318.65 in 2007). The complication rate was well within the accepted Royal College of Radiologists’ standards at the time, with only 5.2% of cases requiring admission due to complications.”
Seneviratne and colleagues proceed to acknowledge that IR procedures are increasingly complex, and that, therefore, the day cases “now [require] more extensive input from interventional radiologists to ensure optimal patient selection, clinical optimisation, and effective co-ordination
with other specialties”. As was the setup back in 1997, the authors state that “the nurse-led model for the organisation of the day-case unit, with pre-assessment conducted within the unit” today enables consultant interventional radiologists to work as efficiently as possible.
The authors conclude their letter by sharing how their hospital is “poised to move into the next phase of day-case radiological intervention”, celebrating Lakshminarayan et al’s paper once again as “a timely reminder of the potential of IR”. Speaking to Interventional News, the King’s authors set out the next steps for their IR service. “We are further developing the clinical nurse specialist role to provide enhanced specialised care and support from our nursing staff, advocating for the patients’ needs, and coordinating care across the domains involved in the patient pathway. We are endeavouring to make the whole procedure experience for the patient ‘holistic’ with ‘fluid’ movement between the physicians and surgeons caring for the patient, with the radiologists pivotal to the care management strategy.
“We are also developing an anaesthetic pre-assessment system, guided by anaesthetists, focusing on comprehensive evaluations, prioritising patient safety during and after day case procedures. In addition, we will expand the modalities for pre-assessment system as our institution covers a large catchment area, with patients often having to travel far for our services. This includes ensuring in-person reviews are necessary and considering alternatives such as video calls and mobile assessment units. Better access to clinical information, including blood tests, from services closer to the patient will help reduce unnecessary patient journeys and improve their experience. With regards to technique, improved usage of variation in the vascular access route e.g. radial artery access in certain procedures, is being expanded to improve patient ambulation post-procedure and shorten recovery times.
“Through these initiatives, we aim to advance patient care, optimise outcomes, and strengthen our institution’s commitment to excellence.”
Petra Svarc (Rigshospitalet, Copenhagen, Denmark) presented during the scientific paper session at the European Conference on Embolotherapy (ET; 21–24 June, Valencia, Spain). She imparted on the audience the results of hers and colleagues’ double-blinded randomised controlled trial (RCT) of high-dose dexamethasone to reduce the symptoms of post-embolization syndrome (PES) in patients who had undergone prostate artery embolization (PAE; the DEXAPAE trial). The group’s findings were that 24mg of dexamethasone is “safe”, as the participants reported no side-effects, but that “it does not reduce PES following PAE” any more than “our standard treatment, which is paracetamol”.
PES is “an umbrella term for the systemic response to tissue necrosis,” Svarc began, detailing that it can include fever, influenza-like symptoms, local pain, and a worsening of lower urinary tract symptoms (LUTS). In a small number of PAE patients, PES can be severe and “mimic” urinary tract sepsis.
Theirs is the “first trial that examined [steroids’] efficacy” in reducing the inflammatory response of PES in PAE patients, Svarc went on. It was a single-centre, double-blinded RCT, where 31 participants were allocated 1:1 to receive either 24mg of dexamethasone or a placebo. Inclusion criteria included having LUTS secondary to benign prostate hyperplasia (BPH), a prostate volume >80ml, an International Prostate Symptom Score (IPSS) of eight or more, being eligible for catheter-based intervention, and having no contraindication to dexamethasone.
The primary outcomes assessed in the trial, Svarc noted, were morning rectal temperature at two days following PAE and pain severity and interference scores on the Brief Pain Inventory used for the first five days post-PAE. Secondary outcomes included hospital admission, levels of c-reactive protein (CRP) and acute urinary retention. “Most patients in both groups were subfebrile for all of the five days,” Svarc shared. Regarding pain, the scores were “generally low, and low means higher quality of life,” she added. The only significant difference regarding secondary outcomes, was the level of CRP—a mean of 108mg/l [range=54–161mg/l] in the control group vs. 10mg/l [5–33mg/l], p value<0.01 in the dexamethasone group.
Svarc then clarified for delegates why the trial ended after only 31 patients were randomised, when 60 had been recruited initially. The reasons were, she explained, that they saw no significant difference in primary outcomes and the control group had only mild PES symptoms.
In terms of conclusions, Svarc’s group found that 24mg of dexamethasone is safe, but does not help reduce PES symptoms following PAE. They also suggest based on their findings that mean temperature and pain may not warrant active treatment, “especially when we look at the control group”.
Interventional News’ most popular stories from July included point of view pieces from interventional radiologists on fallopian tube recanalisation and interventions for postpartum haemorrhage, respectively; news of an editorial from The Cardiovascular Interventional Radiological Society of Europe (CIRSE) which takes a stance on paclitaxel-coated devices; and a report of a Society of Interventional Radiology (SIR) position statement offering recommendations on the management of chronic iliofemoral venous obstruction with endovascular placement of metallic stents.
A French group of interventional radiologists and urologists has recently published the results of its randomised, multicentre, open-label, phase 3 superiority trial of prostate artery embolization (PAE) versus medical therapy (PARTEM) in The Lancet. The group, of whom Marc Sapoval (Hôpital Européen Georges Pompidou, Paris, France) is the corresponding author, states in its publication that the PARTEM trial met its primary endpoint
Alberto Alonso Burgos and Luis Chiva de Agustín (Universidad de Navarra, Pamplona, Spain) explain how where fertility is concerned, each woman is unique, and a one-size-fits-all approach is not appropriate for addressing what can be extremely complex reproductive health issues.
Biotronik has announced one-year subgroup results from the investigator-initiated BIOPACT randomised controlled trial (RCT), which were presented by principal investigator Koen Deloose (AZ Sint-Blasius, Dendermonde, Belgium) at this year’s Leipzig Interventional Course (LINC 2023, 6–9 June, Leipzig, Germany).
The SIR has published a position statement offering recommendations on the management of chronic iliofemoral venous obstruction with endovascular placement of metallic stents. The statement, published online in the Journal of Vascular and Interventional Radiology, is a companion to the 2022 statement on the treatment of acute iliofemoral deep vein thrombosis.
Terumo Aortic has announced that the Japanese Pharmaceuticals and Medical Devices Agency (PMDA) has granted approval of the Thoraflex Hybrid Frozen Elephant Trunk (FET) device for commercial sale in Japan for the treatment of patients with complex aortic arch disease.
Following the news that the US Food and Drug Administration (FDA) has changed its stance on the use of paclitaxel-coated devices to treat peripheral arterial disease (PAD), Boston Scientific has announced its position on the update.
Endologix has shared in a press release that the first patients underwent percutaneous transmural arterial bypass (PTAB) using the Detour system since US FDA approval of the system was granted. This marks the official start of its US targeted market release.
In June 2023, CIRSE published an editorial in Cardiovascular Interventional Radiology (CVIR). Written on behalf of CIRSE’s Endovascular Subcommittee, the authors “advocate that the benefits of paclitaxel-coated device used in the femoropopliteal segment in terms of increased primary patency and reduced target lesion revascularisation warrant their use in the routine treatment of patients with femoropopliteal disease”.
Francis Medical has announced that the first patient has been treated in the company’s VAPOR 2 pivotal clinical study evaluating the safety and efficacy of its Vanquish minimally invasive water vapour ablation therapy for managing prostate cancer.
Lakshmi Ratnam (St George’s University Hospitals NHS Foundation Trust, London, UK) speaks about how the CIRSE 2020 Standards of Practice document for gynaecological and obstetric haemorrhage are among the most comprehensive guidelines in interventional radiology (IR) for obstetric interventions.
IceCure Medical has announced in a press release that Health Canada, the Canadian government’s regulatory agency, has approved IceCure’s ProSense system, disposable cryoprobes, and introducers as cryosurgical tools for indications including:
Tumours—ablation of benign and malignant tumours of the lung, liver, kidneys, and musculoskeletal system, and benign tumours of the breast;
General surgery;
Palliative intervention; and
Other surgeries.
“As we continue to gain traction in the USA, this approval in Canada will create synergies for us in the broader North American market. We have been directly engaging with healthcare providers through education, hands-on training seminars, marketing, and sales in the USA and we will expand these activities into Canada. We have already been contacted by multiple Canadian healthcare providers with requests to purchase and implement ProSense,” stated IceCure Chief Executive Officer Eyal Shamir.
Canada’s healthcare system is ranked as one of the top in the world, with total health spending estimated at $331 billion in 2022.
IceCure’s cryoablation system currently has regulatory approval for various indications in 15 countries, including in the USA, Europe, and China.
Humacyte today announced completion of enrolment in its Phase II/III vascular trauma trial (V005) that is expected to support a Biologics License Application (BLA) filing for the company’s Human Acellular Vessel (HAV) in vascular trauma repair.
A press release details that the HAV is designed to provide surgeons with an off-the-shelf bioengineered human artery that has been observed to repopulate with the patient’s own cells to provide a durable, infection-resistant replacement for damaged and diseased arteries. The HAV has the potential to assist healthcare professionals in saving life and limb in some of the most difficult circumstances. The results from the Phase II/III vascular trauma trial are intended to support a BLA filing with the US Food and Drug Administration (FDA), planned for the fourth quarter 2023.
The V005 trial is a single-arm, open-label, pivotal study of patients suffering from vascular trauma injuries, conducted at Level I trauma centres in the USA and Israel. The primary efficacy assessment will be based on a 30-day HAV patency (presence of blood flow) in patients who have vascular trauma of the extremity, as compared to historic benchmarks reported in literature. Humacyte, the clinical trial sites, and contracted service providers are preparing for locking of the trial database in order to report the V005 results. The company currently expects to complete these activities and report top-line results from the trial before the end of the third quarter 2023.
“We believe that the HAV could revolutionise the ability of surgeons to save the lives and limbs of patients suffering vascular injuries, not only in civilian settings, but also in more challenging environments like the battlefield,” said Laura Niklason, CEO of Humacyte. “The completion of the target enrolment in Humacyte’s Phase II/III vascular trauma trial is expected to enable BLA submission, and is another important landmark moment for our groundbreaking science. Our regenerative medicine technologies create dramatic new therapies—with the potential to provide treatment options for patients facing loss of life or limb for whom current therapies are either inadequate or not available.”
Humacyte’s HAV is a universally implantable, bioengineered human artery that is designed to overcome the challenges associated with traumatic injuries, the company states. It is available to the surgeon immediately, and eliminates the need to harvest and repurpose a vein. Because it is available off the shelf, the HAV can ultimately save valuable time and potentially reduce complications like amputations and tissue loss. Because the HAV is comprised of the same tissue that makes up natural human vessels, it has the potential to repopulate with the patient’s own cells. Clinical results suggest that the HAV is highly infection resistant and therefore is well suited for treating the contaminated wounds created by major traumatic injuries. Importantly, the HAV can be produced at commercial scale in Humacyte’s existing manufacturing facilities, providing thousands of vessels for treating injured patients.
The V005 study is intended to support Humacyte’s BLA filing with the FDA for treatment of extremity vascular trauma when a synthetic graft is not indicated and when an autologous vein is not feasible. The completion of V005 enrolment comes on the heels of Humacyte receiving the FDA’s Regenerative Medicine Advanced Therapy (RMAT) designation for the HAV in vascular trauma in May 2023. The RMAT designation allows for close collaboration between Humacyte and the FDA, and increases the chance for a priority review of a BLA after it is filed. At the time of V005 target enrolment, a total of 68 patients had received the HAV in the V005 trial, of which 51 had vascular trauma of the extremity and comprise the primary efficacy analysis.
In addition to the V005 trial, Humacyte notes that the HAV is also being used in Ukraine under a humanitarian aid programme that has treated 19 vascular trauma patients in the ongoing war, demonstrating a high rate of favourable outcomes in treating some of the most difficult and infection-prone vascular injuries. The data from the Ukraine humanitarian program will be included in the BLA filing with the FDA. The HAV has accumulated more than 1,000 patient-years of experience worldwide in a series of clinical trials in multiple indications, including vascular trauma, arteriovenous access for haemodialysis, and peripheral arterial disease.
Humacyte advises that the HAV is an investigational product and has not been approved for sale by the FDA or any other regulatory agency.
Bracco Imaging has announced the publication of the PROMISE trial in Radiology. The PROMISE study was a prospective, multinational, crossover (within-patient), double-blind comparison of the safety and efficacy of 0.05 mmol/kg gadopiclenol (Vueway) with 0.1 mmol/kg gadobutrol (Gadavist) in adult patients referred for contrast-enhanced magnetic resonance imaging (MRI) of head and neck, thorax (including breast), abdomen (including liver, pancreas, and kidneys), pelvis (including ovaries, uterus, and prostate), and musculoskeletal (including extremities).
Despite being administered at half the dose of gadobutrol, gadopiclenol provided a comparable degree of contrast enhancement and quality of morphologic assessment of lesions. The type and severity of adverse events (AEs) were similar with the two gadolinium-based contrast agents, with Vueway (4.2%) having a slightly lower rate to that of Gadavist (5.5%).
The publication of the results of the PROMISE study comes on the heels of those of the PICTURE clinical trial, which were published in Investigative Radiology and showed non-inferior quality of morphologic assessment of lesions of the brain and spine with 0.05 mmol/kg Vueway compared with 0.1 mmol/kg gadobutrol (Gadavist). The combined results of the PROMISE and PICTURE trials, and additional clinical evidence, supported the regulatory application for gadopiclenol submitted to the US Food and Drug Administration (FDA), resulting in priority review and subsequent approval in 2022.
The PROMISE trial included 273 adult patients suspected of having an enhancing abnormality in one of three different body regions (head/neck, breast/thorax/abdomen/pelvis, or musculoskeletal). Off-site blinded readers with expertise in the respective body regions rated border delineation, internal morphology, and visual contrast enhancement. All primary and secondary endpoints of the study were achieved. For all blinded readers, 0.05 mmol/kg gadopiclenol was non-inferior to 0.1 mmol/kg gadobutrol for all visualisation parameters and all readers (P<.001), and superior to unenhanced images (P<.001). Two of three readers yielded higher percentage enhancement for gadopiclenol (P<.001). Lesion-to-background ratio did not differ. For most participants (75%–83%), readers reported no preference between 0.05 mmol/kg gadopiclenol and 0.1 mmol/kg gadobutrol images.
“The results of the PROMISE Study led to the approval of the use of gadopiclenol with MRI of the head and neck, thorax, abdomen, pelvis, and the musculoskeletal system,” said Alberto Spinazzi, chief medical and regulatory officer at Bracco. “Of note, gadopiclenol was approved for both MRI of the central nervous system and of the body at the dose of 0.05 mmol/kg, which showed to provide similar contrast enhancement efficacy compared with a dose of 0.1 mmol/kg of Gadavist. This is thanks to the high relaxivity of gadopiclenol.”
Vueway injection is a Group II agent within the American College of Radiology’s classification of gadolinium-based agents relative to the risk of nephrogenic systemic fibrosis (NSF), indicating association with few if any, unconfounded cases. It is approved for use in adult and paediatric patients aged two years and older with MRI of the brain, spine, and surrounding tissues, and the body (head and neck, thorax, abdomen, pelvis, and musculoskeletal system).
MediView announced it has received 510(k) clearance from the US Food and Drug Administration (FDA) for its XR90 augmented reality-based surgical visualisation and navigation platform. XR90 is intended to be used adjunctively for minimally invasive ultrasound and computed tomography (CT)-guided needle-based procedures for soft tissue and bone. “This is not only the first 510(k) clearance for MediView, but it is the first 510(k) clearance for an augmented reality device utilising live imaging combined with 3D XR visualisation for pre- and intra-operative indications for use, which sets the stage for further advancements in augmented reality in the healthcare space.” said Adam Cargill, director of Quality, Regulatory and Clinical Affairs at MediView.
“MediView is excited to receive 510(k) clearance for our XR90 platform and appreciate the team’s efforts and FDA’s partnership in achieving this milestone. We are in a new era of visualisation, collaboration, and data insights in healthcare that can create patient, clinician and financial benefits,” said Mina Fahim, president and CEO of MediView. “XR90 expands the MediView portfolio of solutions available to practitioners as they look to simplify, democratise, and inform care delivery with the ultimate goal of improving and expanding access to the best care. Thank you to our employees, investors, and partners for making this possible. We are just at the beginning of a journey seeing the clinical adoption of game-changing data and digital healthcare solutions.”
MediView is utilising augmented reality to address the long-standing limitations of current medical imaging technologies. Flat panel monitors limit practitioners to 2D imaging and require them to look away from the patient’s procedural site, disrupting hand-eye-coordination, resulting in reduced clinician confidence and potentially impacting outcomes.
Through Microsoft’s HoloLens 2 AR headset, clinicians are able to visualise the patient’s ultrasound, as well as displays of other procedural information to facilitate their workflow. XR90 overcomes the limitations of two-dimensional imaging by providing physicians with 3D “X-Ray vision” during procedures – the ability to visualise a patient’s comprehensive internal anatomy in 3D underneath their skin, including bone, tissue, organs and vasculature.
The device projects 3D virtual models of the patient’s own anatomy based on their CT imaging and combines that CT with live ultrasound to perform minimally invasive procedures, such as biopsies and tumour ablations. XR90’s augmented reality capabilities include a holographic light ray that tracks and displays the path of the physician’s instrument, CT-based 3D holographic anatomy display, and live ultrasound that is projected and displayed anatomically into the patient as the clinician scans, similar to a flashlight beam. The system is designed to provide visual information and reference to clinicians for analysis of procedural options during preoperative planning, to help facilitate workflow, and to provide enhanced ergonomics to the user for heads-up, intraoperative display of medical images during ultrasound-guided needle procedures. XR90 is indicated to be used adjunctively to standard-of-care imaging.
XR90 is a diverse imaging tool providing a new way to view patient anatomy and visualise instrumentation pathway while maintaining natural alignment of senses. Clinicians at remote locations can also collaborate real-time with shared visualisation, communication, and the ability to provide guidance during procedures for collaborative patient care. These features can provide increased support for understaffed facilities, rural or underserved populations and a distinct ability to limit caregiver and patient exposure to COVID-19 while maintaining care levels.
Francis Medical announced the first patient has been treated in the company’s VAPOR 2 pivotal clinical study evaluating the safety and efficacy of its Vanquish minimally invasive water vapor ablation therapy for managing prostate cancer. The first patient procedure was successfully completed by Dr. Naveen Kella (center) of The Urology Place in San Antonio, Texas. Francis Medical founder and CTO Michael Hoey (left) and CMO Dr. Christopher Dixon (right) attended the major milestone.
L to R: Francis Medical founder and CTO Michael Hoey, Naveen Kella and CMO Christopher Dixon
Francis Medical, Inc, a privately held medical device company developing an innovative and proprietary water vapour ablation therapy for the treatment of prostate, kidney, and bladder cancer, has announced the first patient has been treated in the company’s VAPOR 2 pivotal clinical study evaluating the safety and efficacy of its Vanquish minimally invasive water vapour ablation therapy for managing prostate cancer.
VAPOR 2 is a prospective, multicentre, single-arm study that will treat 235 patients with intermediate-risk, localised prostate cancer at up to 30 US clinical sites. Arvin George from Johns Hopkins (Baltimore, USA) and Samir Taneja from NYU Langone (New York, USA) are co-principal investigators on the study, and the first patient procedure was successfully completed by Naveen Kella of The Urology Place in San Antonio, USA.
“I am excited to be participating in the VAPOR 2 study and it is a great privilege to treat the first patient,” said Kella. “Currently, prostate cancer patients find themselves in the difficult position of balancing the oncological risks of the disease with the life-altering side effects that can often accompany traditional treatments. Water vapour therapy shows great promise to provide patients with another option to proactively manage their cancer risk while preserving quality of life.”
Francis Medical’s Vanquish water vapour technology applies the thermal energy stored in a few drops of sterile water to deliver targeted treatments to the cancerous tissue through a simple transurethral procedure. The therapy is designed to ablate cancer cells while protecting surrounding structures, lessening the likelihood of life-altering side effects common with other prostate cancer treatments.
“The first patient treated in the VAPOR 2 study is an important milestone for the company,” said Michael Kujak, Francis Medical president and chief executive officer. “We would like to thank our employees, investors, patients, and physician partners for bringing us to this stage. We are more confident than ever that this ground-breaking technology will ultimately become the first-line treatment of choice for men and their doctors.”
The company anticipates using the one-year follow-up data from the VAPOR 2 study in support of a US Food and Drug Administration submission for US market clearance. VAPOR 2 patients will be followed for a period of five years to gather longer-term cancer outcomes. Further information on the VAPOR 2 study can be found at clinicaltrials.gov (NCT05683691).
“The vision that started this company and continues to drive us is to create a better experience for the patient,” said Michael Hoey, Francis Medical founder and chief technology officer. “Water vapour is an ideal tool for accomplishing this goal. It is simple, natural, and gentle, but powerful. The first VAPOR 2 study treatment is an important milestone bringing us one step closer to getting this ground-breaking technology into the hands of urologists and their patients.”
The Society of Interventional Radiology (SIR) has published a position statement offering recommendations on the management of chronic iliofemoral venous obstruction with endovascular placement of metallic stents. The statement, published online in the Journal of Vascular and Interventional Radiology, is a companion to the 2022 statement on the treatment of acute iliofemoral deep vein thrombosis.
In the new statement, a multidisciplinary group of experts from interventional radiology (IR), vascular medicine, and vascular surgery indicated that among patients with chronic venous disease and iliofemoral venous obstruction, those who are experiencing life-disrupting symptoms or disability and who have anatomic features that favour long-term patency, may be more likely to benefit from stenting as an adjunct to conservative management. Most other patients with chronic iliofemoral venous occlusions would be better served with conservative management alone, such as use of medical therapy and compression garments, and re-evaluated over time.
“There is strong consensus on the panel that excellent clinical decision-making around venous stent placement will be most likely when the treating physician has strong familiarity with key clinical considerations around optimal diagnosis and evaluation of iliac vein obstruction, as well as assessment of its clinical severity and life impact,” said Suresh Vedantham, interventional radiologist and professor at Washington University School of Medicine (St Louis, USA), who is the lead author of the statement. “The statement provides a framework against which IR physicians can review their practices, address knowledge gaps, deliver treatment effectively, and ensure that patients selected for stent placement are likely to benefit from it.”
The statement authors note that additional research is needed to better guide the use of stents in this patient population. If completed, two ongoing multicentre randomised controlled trials—C-TRACT and BEST—can enable a strong and unbiased understanding of the treatment effects associated with the addition of venous stent placement to standard care, Vedantham said.
“For both studies, success will depend on whether providers make it a priority to refer patients to study sites,” he said. “It is hoped that physicians will promote the welfare of future venous disease patients by actively choosing now to enrol eligible patients in ongoing clinical trials that are designed to generate high-quality evidence on the benefits, risks, and best practices around venous stent placement.”
While this research proceeds, SIR believes that adherence to the statement’s recommendations will enable judicious use of endovascular therapy in a manner that optimises benefit and minimises harm.
“The new statement provides the best assessment of the current evidence we have to date, and SIR is grateful to the authors for their time and energy in ensuring that we have evidence-based guidance for the treatment of chronic venous occlusions,” said SIR President Alda L Tam, interventional radiologist and professor at the University of Texas MD Anderson Cancer Center (Houston, USA). “SIR remains committed to supporting ongoing and future research in this area to ensure that physicians have the information they need to optimize patient care now and in the future.”
Endologix has shared in a press release that the first patients underwent percutaneous transmural arterial bypass (PTAB) using the Detour system since US Food and Drug Administration (FDA) approval of the system was granted. This marks the official start of its US targeted market release.
PTAB with the Detour system offers a disruptive, novel approach to treating complex peripheral arterial disease (PAD), enabling physicians to bypass lesions in the superficial femoral artery, by using stents routed through the femoral vein to restore blood flow to the leg. This approach is effective for patients with long lesions (20–46cm in length), those that have already undergone failed endovascular procedures, or those that may be suboptimal candidates for open surgical bypass.
For the rollout, Endologix collaborated with two healthcare systems known for clinical excellence. PTAB using the Detour system was first performed at Cleveland Clinic’s Sydell and Arnold Miller Family Heart, Vascular & Thoracic Institute (Cleveland, USA) and at Salinas Valley Health Medical Center (Salinas, USA).
“We are delighted to be able to introduce PTAB using the Detour system into clinical use,” said Matt Thompson, president, and CEO of Endologix. “The Detour system is a pivotal addition to our product portfolio, which now offers differentiated therapies for both abdominal aortic aneurysms and PAD. The successful introduction at these leading institutions underscores our commitment to continuing to innovate on behalf of patients. Broadening our therapeutic profile is a key achievement as we transform Endologix into a leading interventional vascular company.”
The European Institute for Biomedical Imaging Research (EIBIR) has today announced the appointment of Regina Beets-Tan as its new scientific director. Beets-Tan, EIBIR states, will contribute to further enhancing the organisation support of European biomedical imaging research and networking activities between institutes and disciplines.
Beets-Tan chairs the department of Radiology at the Netherlands Cancer Institute and is professor of Radiology at the University of Maastricht, The Netherlands and adjunct professor of Abdominal and Oncological Radiology at the University of Southern Denmark.
Beets-Tan also is the former Chair of the Board of Directors of the European Society of Radiology (ESR), which has today announced the commencement of the new ESR board of directors and executive council.
Adrian Brady from Ireland assumes the prestigious position of chairperson of the ESR Board of Directors, the highest governing role within the society. Carlo Catalano from Italy takes on the esteemed position of ESR president and will also chair the ECR 2024 Programme Planning Committee. The ESR extends a warm welcome to Minerva Becker, who joins the ESR board of directors following her successful election in June.
The ESR has extended its sincere appreciation to Beets-Tan for her outstanding leadership as chairperson of the society during the past year and eagerly anticipates her valuable support as ESR past-president in the coming year.
On her new appointment, Beets-Tan pointed out that “multidisciplinary research in biomedical imaging is not merely a pursuit of knowledge but a catalyst for change. It is through collaboration and bridging the gaps between disciplines that we can unlock the potential of biomedical research to move forward the field of precision medicine.” She further stated that “it is with great honour that I assume the responsibility of leading this esteemed organisation. I am grateful for the opportunity to build further upon the outstanding work of my predecessor Gabriel Krestin and guide EIBIR towards new horizons”.
At the same time, the EIBIR community and the team at EIBIR acknowledge and celebrate outgoing scientific director Gabriel Krestin, who, the organisation states, has made remarkable advancements, positioning it as a leading entity in supporting scientists and securing funding for their projects, and substantially contributing to the advancement of biomedical imaging in Europe.
Under Professor Krestin’s guidance, EIBIR has helped researchers secure more than €171 million for research as part of 34 projects, and EIBIR-supported projects have resulted in more than 725 peer-reviewed publications so far.
In June 2023, the Cardiovascular Interventional Radiological Society of Europe (CIRSE) published an editorial in Cardiovascular Interventional Radiology (CVIR). Written on behalf of CIRSE’s Endovascular Subcommittee, the authors “advocate that the benefits of paclitaxel-coated device used in the femoropopliteal segment in terms of increased primary patency and reduced TLR [target lesion revascularisation] warrant their use in the routine treatment of patients with femoropopliteal disease”. The editorial was published this week in the wake of the US Food and Drug Administration (FDA) letter stating that the data do not show that paclitaxel-coated devices come with an excess mortality risk.
The authors, including corresponding author Robert Morgan (St George’s University Hospitals NHS Foundation Trust, London, UK) begin their editorial by outlining the background to the controversy around use of paclitaxel-coated balloons and paclitaxel-eluting stents. They reference initial “encouraging data” that led to “increasingly widespread” recourse to drug-based therapies to treat peripheral arterial disease (PAD) in femoropopliteal disease up until Katsanos et al published their meta-analysis in 2018. The findings of this meta-analysis—that all-cause mortality following treatment with paclitaxel-coated balloons and paclitaxel-eluting stents in the femoropopliteal segment in claudicants was 14.7% at five years, with the rate post-percutaneous transluminal angioplasty (PTA) calculated as 8.1%—“resulted in a metaphorical tsunami destroying confidence worldwide in paclitaxel” as safe for preventing restenosis.
Morgan et al outline that after the Katsanos meta-analysis was published, the US FDA created an expert panel to provide updates to healthcare providers. Other national medical regulators also made recommendations in light of the findings to be “[cautious]” in using paclitaxel, with the UK Medicines and Healthcare Products Regulatory Agency (MHRA) among those advocating for limiting its use to patients with chronic limb-threatening ischaemia (CLTI) only. This reduction in use of paclitaxel in these settings led to the “loss of the proven benefits of drug-based device therapies to patients in terms of reduced patency of femoropopliteal angioplasty and stenting using non-paclitaxel-coated devices, and probably an associated increase in the need for hospital readmission rates for repeat revascularisation procedures”.
The editorial proceeds to highlight the findings of a subsequent meta-analysis based on the same randomised trials included by Katsanos et al: “that there is a minimal or no increase in mortality associated with paclitaxel-coated devices. Moreover, when the patient-level data of the trials used for the Katsanos meta-analysis were assessed, the absolute increased mortality risk associated with paclitaxel use at five years decreased from 14.7 to 4.6%”. Morgan et al suggest that the difference in these reported outcomes could be attributed to different study designs and data sources, among other factors.
“One major flaw” in the conclusions reached by Katsanos, the CIRSE editorial opines, is that “none of [the trials included in the meta-analysis] were designed to assess for a difference in mortality between the patient groups”. Morgan et al also list various studies post-Katsanos that suggest paclitaxel to be “associated with improved efficacy but was not associated with increased mortality” (the full list can be found in the footnotes of the CVIR publication here).
Rounding off their editorial, the CIRSE authors point out that “a robust body of evidence now exists to refute the existence of a long-term mortality signal associated with paclitaxel-coated devices i.e. any mortality risk is negligible or absent”. They go further to conclude that “all efforts to find a link and a causal explanation for the perceived mortality risk between paclitaxel dose and mortality have failed”. Looking to the future, Morgan et al urge that “endovascular trial designs must incorporate strategies and methods to maximise patient retention and facilitate long-term assessment and reporting of vital statistics, including mortality”. In addition, they express their interest in seeing data on the efficacy of sirolimus-eluting devices and on the comparative efficacy of paclitaxel-coated versus sirolimus-eluting devices.
For the time being, as stated above, the authors support using paclitaxel-coated devices in the femoropopliteal segment to increase primary patency and reduce TLR in patients with femoropopliteal disease.
This advertorial is sponsored by Terumo Interventional Systems
Philippe Pereira
LifePearl™ microspheres (Terumo) are polyethylene glycol (PEG) embolization microspheres that can be loaded with chemotherapeutic drugs including doxorubicin, irinotecan, idarubicin and epirubicin¹. Philippe Pereira (SLK-Kliniken GmbH, Heilbronn, Germany) speaks to Interventional News about his experience using LifePearl microspheres in his interventional oncology practice. He shares his knowledge on how to achieve the optimal transarterial chemoembolization (TACE) procedure, and how the latest pooled analysis data from hepatocellular carcinoma (HCC) patients reinforce the evidence on efficacy and safety of drug-eluting microspheres (DEM) TACE with LifePearl microspheres in patients with HCC.
Pereira begins by outlining some of the current challenges of TACE. “Having a personalised approach to chemoembolization is very important and one of the main advantages of local therapies,” he stipulates, “and every chemoembolization is different—regarding the dose, the vessel anatomy, etc. He also stipulates the need to preserve the patient’s liver function following TACE. Altogether, you need a very high level of experience, and for the large majority of tumours, a superselectivity of your catheterisation is absolutely required”.
How do you perform your TACE procedures for HCC?
Next, Pereira details the advantages of using LifePearl microspheres as a means of overcoming the challenges often associated with TACE, drawing on his own experience, having used it for eight years. “In Germany, the preparation [for TACE] with cytotoxic drugs is no longer done in the radiology department, but in the pharmacies. As our pharmacists have said to me, it is really easy to load them with only few preparation steps required”. Another advantage, according to Pereira, is that the LifePearl microspheres are available in a variety of sizes, including “a very small size (100µm) for the treatment of primary and secondary liver tumours”. This is coupled with a narrow size distribution for targeted treatment. The third benefit, he continues, is the “long time stability” of LifePearl microspheres mixed with contrast medium allowing a smooth delivery²⁻³.
Furthermore, Pereira explains that he uses “a 2.4Fr Progreat microcatheter for TACE procedures and in some more difficult situations where you have a complex intrahepatic arterial anatomy, you should be very selective and we sometimes go to a 2.0Fr microcatheter”. OcclusafeTM micro balloon microcatheter can also allow for blood flow redistribution during TACE, which is not possible with a standard microcatheter and can be beneficial for some types of tumours.
What are the highlights of the latest clinical evidence with LifePearl microspheres from your perspective?
Pereira then outlines some of the key findings from the pooled analysis of 580 patients with unresectable HCC treated with LifePearl microspheres, first highlighting the “median overall survival of 50.8 months, which appears to be much more than 25–37 months usually obtained with [conventional] TACE”, although this figure can vary depending on the patient’s Barcelona Clinic Liver Cancer (BCLC) stage.
Also, of interest to Pereira is the “stratification following the ALBI [albumin-bilirubin] scores, allowing maybe a better selection of patients or a more personalised approach with DEM-TACE”. In addition, he notes “the importance of a low level of liver damage” observed in the patients treated with LifePearl microspheres, and that “a low level of hepatic damage is extremely important for continued targeted therapy with TACE or for allowing a stage migration with systemic treatment.”
In a similar vein, Pereira suggests some of the reasons why LifePearl microspheres achieved a greater median overall survival rate as compared to previous reports—“maybe because they have a higher elution rates as demonstrated in in vitro comparative testing, maybe in relation to the tighter size calibration of microspheres allowing a more targeted embolization, maybe both, since there is better standardisation for TACE with microspheres versus conventional TACE.” The improvement of the TACE technique over the years (with superselectivity, improved images etc) can also explain these latest outcomes.
What would be your recommendations for performing an optimal TACE procedure?
Pereira proceeds to speak about recommendations for carrying out an optimal TACE procedure in HCC patients, where superselectivity is key. In the German guidelines, Pereira states, it says that for HCC, “if you cannot be superselective, it is not recommended to perform TACE in HCC”. Moreover, in his opinion, Pereira says that this is true “independent of the size of the tumour”—even if there are “satellite” tumours surrounding it, “you should address each tumour-feeding artery in a selective way”. Another reason why selectivity matters so much for HCC, he elaborates, is to reduce the toxicity of the TACE, especially for patients with the beginnings of liver insufficiency. “It is very important because the TACE will be repeated and you keep, also, the possibility to move to another treatment.” In summary, Pereira states that, with selectivity, “you increase efficacy, and you reduce the adverse effects”.
Pereira returns next to his personal experience, and what is, for him, crucial for an optimal TACE procedure. “Imaging is important—good quality will reduce radiation,” he says. Going into more detail on imaging, Pereira specifies that real-time monitoring can help to analyse the perfusion of HCC tumours in some more tricky cases. “As HCC is mostly a highly perfused tumour, this online monitoring may work very well. It is not necessary for all patients, but in some cases, we use it if we are not sure whether there might be another tumour-feeding artery that we would need to perform TACE on.”
What do you think can be done to further improve clinical outcomes for TACE?
First of all, Pereira suggests that “to improve clinical outcomes, we need to improve training of interventional oncologists on performing TACE procedures—it is a prerequisite”.
Looking ahead to the potential for further innovation, Pereira suggests that “perhaps we need, in the future, resorption of the microspheres to be able to repeat the treatment”. BioPearlTM microspheres (Terumo) is an example of this technology to which Pereira refers to reinforce this point—access to the tumour over time can become problematic due to “changes in morphology in the already-treated tumour-feeding artery, such as if you need to treat the same tumour multiple times”. Resorbable microspheres can guard against this, Pereira underlines, but that how quickly different embolic agents are resorbed remains a question to be answered through future research.
Staying on the subject of future developments, Pereira suggests that we should also improve the possibility of loading DEM-TACE microspheres with different cytotoxic drugs or even immunotherapies, such as immune checkpoint inhibitors.” Pereira points out that there is some preliminary experience of loading embolic microspheres with immunotherapies and treating locally, but that this should be also studied further.
Summarising, Pereira believes that the first way to improve TACE procedures is for the interventional oncologist to develop and standardise the technical aspects, including use of imaging and microcatheters, but that another possible means of achieving better procedural outcomes is to better select the patients and “work together with hepato-oncologists to improve the treatment strategy by combining local and systemic therapies”.
1. LifePearl microspheres IFU PD111943-02 rev A 2018-01
2. De Baere T et al. J Vasc Interv Radiol 2016;27:1425–31
3. Pereira P et al. Anticancer Drugs 2016;27:873–878
Biotronik has announced one-year subgroup results from the investigator-initiated BIOPACT randomised controlled trial (RCT), which were presented by principal investigator Koen Deloose (AZ Sint-Blasius, Dendermonde, Belgium)at this year’s Leipzig Interventional Course (LINC 2023, 6–9 June, Leipzig, Germany).
The randomised controlled non-inferiority trial evaluated the safety and efficacy of the Passeo-18 Lux drug-coated balloon (DCB) catheter compared to the In.Pact Admiral DCB (Medtronic) and showed excellent results for both balloons through 12 months across a variety of sub-cohorts, Biotronik reports.
The prospective, multicentre, core lab-adjudicated non-inferiority study enrolled 302 patients in Austria, Belgium, France and Switzerland with Rutherford 2-4 disease. Patients were randomised 1:1 to either the Passeo-18 Lux DCB or In.Pact Admiral DCB for the treatment of stenotic, non-stented restenotic or occlusive lesions in the femoropopliteal artery.
The primary safety endpoint was a composite of freedom from device- and procedure-related death through 30 days post-index procedure, freedom from major target limb amputation and clinically driven target vessel revascularisation through 12 months post-index procedure. It showed no statistically significant difference between balloons for the full data set and across subgroups:
Diabetes: 94.7% vs. 95.2% (Passeo-18 Lux DCB vs. In.Pact Admiral DCB in diabetics); 97.1% vs. 95.6% (Passeo-18 Lux DCB vs. In.Pact Admiral DCB for non- diabetics)
Lesion length: 95.9% vs. 90% (Passeo-18 Lux DCB vs. In.Pact Admiral DCB, respectively, for patients with target lesions ≥100 mm); 96.7% vs. 97.9% (Passeo-18 Lux DCB vs. In.Pact Admiral DCB for patients with target lesions <100 mm)
Calcium: 98.1% vs. 96.8% (Passeo-18 Lux DCB vs. In.Pact Admiral DCB, respectively, in severely calcified lesions); 92.9% vs. 89.7% vs (Passeo-18 Lux DCB vs. In.Pact Admiral DCB in none/moderately calcified lesions)2.
Bailout stenting: 100% vs. 100% (Passeo-18 Lux DCB vs. In.Pact Admiral DCB, respectively, with bailout stenting); 96.1% vs. 95% (Passeo-18 Lux DCB vs. In.Pact Admiral DCB without bailout stenting)2.
Occlusions: 100% vs. 100% (Passeo-18 Lux DCB vs. In.Pact Admiral DCB, respectively, in occlusions); 95.8% vs. 94.7% (Passeo-18 Lux DCB vs. In.Pact Admiral DCB in stenoses)
“Interestingly, we found that across all variations and cohorts, there was no statistically significant difference in safety, primary patency, or clinically driven target lesion revascularisation,” said Deloose. “There is a scarcity of randomised head-to-head data, especially in the drug-coated balloon space, so the more data we have available, the more answers we have.”
One-year results from the full cohort, presented last year at Paris Vascular Insights 2022, showed comparable results between treatment arms, with a freedom from clinically driven target lesion revascularisation rate of 97.2% for Passeo-18 Lux DCB and 97.0% for In.Pact Admiral DCB (p=0.0002).
A press release details that the Passeo-18 Lux DCB has a paclitaxel dose of 3.0 µg/mm2 and uses a Butyryl-tri-hexyl citrate excipient (In.Pact Admiral DCB: 3.5 µg/mm2 and urea excipient). The lower-profile Passeo-18 Lux DCB is on an 0.018″ platform and is 4Fr compatible for diameters of 2–mm and 5Fr compatible for diameters of 5–7mm. In comparison, the release continues, the In.Pact Admiral DCB is 5F compatible only for its 4mm diameter, and is 6Fr or 7Fr compatible for its diameters of 5–7mm.
The BIOPACT study will continue collecting follow-up data at 24, 36, 48 and 60 months, which will be shared upon completion of each follow-up period. Biotronik advises that the 24-month full-cohort results will be announced later this year.
Data published in the Journal of the American Heart Association(JAHA), in a meta-analysis by Konstantinos Katsanos (Patras, Greece) and colleagues, suggest that there is an “increased risk of death at two and five years” following the use of paclitaxel-coated balloons and stents in the femoropoliteal artery. Some physicians questioned the finding as lacking individual patient-level data from randomised trials.
“Inclusion in SWEDEPAD studies stop!” reads a statement on the website of the SWEDEPAD (Swedish drug-elution trial in peripheral arterial disease) project, shortly after the publication of Katsanos’ meta-analysis. The decision was taken in consultation with the trial’s Data Safety Monitoring Committee.
Executives from Medtronic and Boston Scientific stated that they were not backing away from drug-eluting devices used in blood vessels in the legs, despite the findings of the meta-analysis linking them to a significantly increased risk of death at two and five years following use in the femoropoliteal artery.
The story hit the headlines in the January 2019 edition of Vascular News
The US Food and Drug Administration (FDA) begins the process of evaluating its recommendations for the use of paclitaxel-coated devices in the legs. While the review of data is ongoing, “continued surveillance” is recommended for patients treated with paclitaxel, though the Agency states that the “benefits continue to outweigh the risks” for approved devices used within their indications.
Data presented at the Leipzig Interventional Course (LINC, 22–25 January 2019, Leipzig, Germany) finds no association between paclitaxel dose and mortality. Experts expressed confidence in the continued use of paclitaxel-coated devices as a result of the release of the data.
Following a review of the Katsanos meta-analysis, experts from the Society for Cardiovascular Angiography and Interventions (SCAI) issues a statement in which it claims that the “benefits of paclitaxel devices continue to outweigh any potential risks”, but says that it is keeping the situation under examination.
Polling at the 31st International Symposium on Endovascular Therapy (ISET; 27–30 January 2019, Hollywood, USA), taking place soon after the publication of the Katsanos meta-analysis, indicated that 79% of audience members did not see the findings as significant enough to change their practice. Despite this result, 31% of respondents said they would use paclitaxel-coated devices less.
The Society for Vascular Surgery (SVS) pulls together a Task Force on Paclitaxel Safety to evaluate all data related to paclitaxel use in patients with peripheral arterial disease, after expressing concerns at the finding of the Katsanos meta-analysis.
Following preliminary analysis, the FDA recommend that “alternative treatment options to paclitaxel-coated balloons and paclitaxel-eluting stents should generally be used until additional analysis of the safety signal has been performed.” Elsewhere, the UK’s Medicines and Healthcare products Regulatory Agency (MHRA) convened an independent Expert Advisory Group to review the available data.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) releases a statement on the use of paclitaxel-coated balloons and stents in the treatment of PAD, in which it states that, in the majority of patients undergoing lower limb recanalisation therapies, alternatives to drug-eluting devices should be used.
Delegates at the 2019 Charing Cross (CX) Symposium (15–18 April 2019, London, UK) voted overwhelmingly against the notion that there was a demonstrable danger in any organ of the body attributed to circulating paclitaxel.
The UK’s MHRA acted to limit the future use of paclitaxel-eluting stents and paclitaxel-coated balloons in routine clinical care following recommendations from the independent Expert Advisory Group on the use of these devices, after concluding that the statistical analysis used by the investigators in the Katsanos paper was robust.
The cover of the June 2019 edition of Vascular News, which featured an in-depth look at the discussion at CX 2019
Writing in a paper published in the Journal of Endovascular Therapy (JEVT) Andrew Holden (Auckland, New Zealand) and colleagues find that the methodology underpinning the conclusion by Katsanos et al that there is a positive dose-response relationship between paclitaxel and mortality is flawed.
Following a two-day discussion, an FDA Circulatory System Devices Panel Advisory Committee concluded that there is a “mortality signal” as first described in the Katsanos JAHA paper, but that better data collection was necessary going forward, as some data were missing.
The US FDA issues a letter to healthcare providers, in which it states that clinical studies of paclitaxel-coated balloons and paclitaxel-eluting stents “may continue and should collect long-term safety (including mortality) and effectiveness data”. This is due to “the demonstrated short-term benefits of the devices, the limitations of the available data, and uncertainty regarding the long-term benefit-risk profile of paclitaxel-coated devices”.
A real-world safety analysis of paclitaxel-based devices in peripheral arteries, conducted by Eva Freisinger (Münster, Germany) and colleagues and published in the European Heart Journal, showed no evidence for increased mortality over a period of 11 years.
A further meta-analysis by Katsanos, published in the Journal of Vascular and Interventional Radiology (JVIR), suggests significantly worse amputation-free survival at one year with the use of paclitaxel-coated balloons in arteries below the knee in the treatment of chronic limb-threatening ischaemia (CLTI). However, some experts advised cautious interpretation of the results and questioned whether the data would impact practice.
The first virtual CX Symposium, in the era of COVID-19, saw further data and discussion on the issue of paclitaxel devices in PAD. Polling during the session asked the audience: “Do you consider paclitaxel dose level to be crucial?” with 53% of respondents voting “yes”. The US FDA’s Misti Malone also offered an update onto the ongoing investigation into the issue.
In a field safety notice the UK MHRA stated that a warning and clinical summary section would be added to the instructions for use (IFU) of 12 paclitaxel-coated balloons and paclitaxel-eluting stents used in the treatment of PAD of the lower limbs.
Andrew Farb, Misti Malone, and William H Maisel, representatives of the Center for Devices and Radiological Health, US FDA, authored a perspective piece in the New England Journal of Medicine (NEJM), titled, “Drug-coated devices for peripheral arterial disease [PAD]”. In the paper, they stated that clinical studies of these devices should continue and should collect long-term mortality data.
In the presence of representatives from the US FDA and UK MHRA, an audience vote at CX 2021 saw 74% of participants support that view that “it is time to change the agency recommendations regarding paclitaxel use in peripheral interventions”.
The UK MHRA issued an updated position statement on the use of paclitaxel-coated devices, in which it stated that such devices may continue to be used in critical limb ischaemia patients “where the benefits may outweigh the risks”. For intermittent claudication, however, the statement recommended against the use of paclitaxel-coated devices, “as the mortality risk generally outweighs the benefit”.
The US regulator issues a letter to healthcare providers on 11 July, in which it states that, based upon its review of the totality of the available data and analyses, “we have determined that the data does not support an excess mortality risk for paclitaxel-coated devices”.
Following yesterday’s news that the US Food and Drug Administration (FDA) has changed its stance on the use of paclitaxel-coated devices to treat peripheral arterial disease (PAD), Boston Scientific has announced its position on the update. The company’s full statement reads as follows:
On 11 July 2023, the FDA published a letter to healthcare providers stating that, based on its review of the totality of the available data and analyses, the excess risk of mortality associated with paclitaxel-coated devices to treat PAD is no longer supported. The letter recognises the safety of paclitaxel-coated devices and provides updated guidance that eliminates the requirement for device manufacturers to include specific warning language within device labelling.
“We are pleased that, after continued analysis of data and collaboration among a broad set of stakeholders, the FDA has determined the large body of long-term clinical data do not support an excess mortality risk for paclitaxel-coated devices used to treat patients with PAD,” said Michael R Jaff, chief medical officer and vice president, Peripheral Interventions, Boston Scientific. “We remain dedicated to helping physicians provide the best care possible for their patients through access to life-changing technologies, including the Eluvia drug-eluting vascular stent system (DES) and the Ranger drug-coated balloon (DCB), both of which have demonstrated excellent safety profiles and very low revascularisation rates in the hundreds of thousands of patients treated worldwide with these devices.”
Approximately 200 million people around the world are affected by PAD, a common circulatory problem in which plaque builds up and narrows arteries, consequently reducing blood flow to limbs.
The Ranger DCB has a low therapeutic drug dose and proprietary coating, which efficiently transfers the drug into the tissue, resulting in the highest primary patency rates from prior studies examining other peripheral DCBs. The low-profile platform of the balloon also assists clinicians in performing streamlined procedures and navigating through challenging anatomy in order to deliver consistent therapy.
The Eluvia DES, which features sustained release of the lowest dose of paclitaxel for peripheral drug-eluting devices, re-opens blocked arteries and restores blood flow while utilising a drug-polymer combination to prevent excessive tissue regrowth. Eluvia has the highest primary patency and lowest revascularisation rates among stents used to treat PAD in the superior femoral artery (SFA) and has shown superiority in two randomised controlled comparative effectiveness trials.
Verve Medical has received approval from the US Food and Drug Administration (FDA) to initiate its Natural Orifice via renal pelvis denervation (NOVEL-Denervation) pivotal investigational device exemption (IDE) trial for the treatment of uncontrolled hypertension to lower blood pressure.
The Verve RPD, NOVEL pivotal trial will enrol up to 300 patients, and will be a 2:1 randomised, sham-controlled, double-blinded study to determine the safety and efficacy of the Verve RPD minimally invasive, non-vascular renal pelvic denervation system to treat hypertension.
In contrast to other renal denervation approaches in the renal artery, Verve’s method accesses the renal nerves through the natural orifice of the urethra, like a common urology procedure. The Verve RPD system ablates afferent and efferent nerves in the renal pelvis and is likely more effective due to the increased density of innervation in the renal pelvis, where easier access can be obtained versus the traditional arterial renal denervation approach, Verve Medical says in a press release.
“The Verve RPD, NOVEL–Denervation, pivotal trial will be another critical milestone toward making this differentiated therapy available to helping the over one billion uncontrolled hypertension patients worldwide, including 80 million in the USA, who struggle with managing this serious condition,” said Verve president and CEO, David Springer. “This Pivotal trial is designed to provide the basis for approval of the procedure in the US.”
Renal denervation is a minimally invasive procedure designed to treat hypertension. The procedure targets overactive nerves in the kidneys that cause high blood pressure. By delivering energy to these nerves, it decreases their activity and helps to regulate blood pressure.
Cagent Vascular has announced the results of its below-the-knee (BTK) RECOIL study. This core lab-adjudicated Recoil analysis— the first of its kind, according to the company— evaluated vessel recoil in lesions treated with Serranator verses plain balloon angioplasty.
The study results demonstrated that lesions treated using serration angioplasty exhibited 49% less average recoil than plain balloon angioplasty. Stefan Stahlhoff (Arnsberg Clinic, Arnsberg, Germany) and Venita Chandra (Stanford University, Stanford, USA) led the RECOIL study as co-principal investigators.
The Serranator percutaneous transluminal angioplasty (PTA) serration balloon catheter is the first and only angioplasty balloon that is US Food and Drug Administration (FDA) cleared and CE marked that embeds serration technology into a semi-compliant balloon for treating peripheral arterial disease (PAD), a press release reads. The device is designed to create multiple longitudinal lines of interrupted micro-serrations to aid arterial expansion.
Thirty-six patients with 39 lesions in up to 22cm in length were matched 1:1 using either the Serranator or plain balloon angioplasty. The study objectives were to assess the ability to define and measure post treatment recoil in infrapopliteal arteries and to show preliminary evidence as to the differences between serration angioplasty and standard balloon angioplasty as defined by post-treatment recoil, lumen gain, and dissection. In each procedure the lumen diameter was measured immediately post angioplasty and then again at 15 minutes post inflation. The degree of vessel recoil was assessed angiographically and then core lab adjudicated. These data showed a mean percent recoil of 6% in the Serranator group vs. 55% in the plain balloon angioplasty group representing a 49% reduction in recoil using serration angioplasty. Notably, there were no flow limiting dissections in either lesion treatment group, suggesting that optimal inflation technique impacts dissection rates, but not recoil rates.
“The recoil phenomenon is well understood as one of the greatest headwinds to successful BTK treatment and ultimately wound healing,” stated Michael Lichtenberg (Klinikum Hochsauerland, Arnsberg, Germany) who participated in the study. “The 49% difference demonstrated in the RECOIL study between Serranator and [plain balloon angioplasty] is statistically significant and in my view also clinically relevant. Wound healing requires a durable lumen to support brisk blood flow, and 55% recoil for [plain balloon angioplasty] treated lesions is a signal that our current 40-year [plain balloon angioplasty] standard therapy is inadequate. I believe this study is a further step in demonstrating serration angioplasty as a definitive treatment for BTK lesions.”
Chandra added: “We know that BTK interventions are highly susceptible to vessel recoil, however the impact of recoil on residual stenosis at 15 minutes post procedure makes the true severity of this challenge clear. Our [chronic limb-threatening ischaemia] patient population is particularly vulnerable and at greater risk of limb loss and the associated increase in mortality that accompanies amputation. While this initial RECOIL study did not follow patient outcomes, in the future we intend to evaluate how impactful serration angioplasty’s recoil improvement is to healing BTK wounds and savingslimbs. The results from this comparative RECOIL study are indicative that serration angioplasty may be the tool that finally addresses this longstanding challenge with [plain balloon angioplasty].”
FDA has issued new guidance for the use of paclitaxel coated devices in peripheral arterial disease
FDA has issued new guidance for the use of paclitaxel coated devices in peripheral arterial disease
In a letter to healthcare providers dated 11 July 2023, the US Food and Drug Administration (FDA) communicates that the risk of mortality associated with paclitaxel-coated devices to treat peripheral arterial disease (PAD) is no longer supported based on the totality of the available data and analyses.
This update signals a lowering of the red flag raised in a 2019 letter from the Administration—published in response to a meta-analysis that indicated a late mortality signal—warning that treatment of PAD with paclitaxel-coated balloons and paclitaxel-eluting stents was “potentially associated with increased mortality”.
Alongside the letter, the US FDA has updated its recommendations for healthcare providers regarding the use of paclitaxel-coated balloons and stents for PAD. As well as removing reference to the possibility of increased mortality with these devices, the amended guidance softens the language around the monitoring of patients who have been treated with paclitaxel-coated stents and balloons, stating that healthcare providers should continue ‘routine’ rather than ‘close’ monitoring of these patients, as had previously been stated.
The safety of paclitaxel—used in peripheral interventions to prevent restenosis—was called into question by data put forward in 2018 by Konstantinos Katsanos (University of Patras, Patras, Greece) et al that pointed to an increased risk of death at two and five years following the use of paclitaxel-coated balloons and paclitaxel-eluting stents in the femoropopliteal artery.
The FDA responded, notifying healthcare providers in early 2019 about a late mortality signal in patients treated for PAD in the femoropopliteal artery with paclitaxel-coated balloons and paclitaxel-eluting stents. Their most recent update on the topic, prior to that shared on 11 July 2023, was posted in August 2019.
In its new update, the FDA notes that “additional data from the pivotal randomised controlled trials (RCTs) has become available,” and that the Administration has worked with device manufacturers and external stakeholders to develop the protocol and analysis plan for new data generation.
The FDA references the fact that device manufacturers collaborated in an updated meta-analysis, which included “additional studies, more complete vital status information, and longer-term follow-up compared to prior studies”. Patient follow-up in these studies ranged from two to five years, the Administration notes, and led it to conclude that the updated RCT meta-analysis “does not indicate that the use of paclitaxel-coated devices is associated with a late mortality signal”.
Furthermore, the FDA states that it also reviewed additional analysed of the risk for late mortality, including the SWEDEPAD trial interim analysis, the VOYAGER PAD study, the German BARMER Health Insurance study, the US Veterans Health Administration study and the Medicare SAFE-PAD study. “None of these studies, with mean or median follow-up ranging from 1.7 to 3.5 years, found a risk for late mortality associated with paclitaxel-coated devices,” the FDA communicates, adding that longer-term follow-up in several of these studies is ongoing.
Boston Scientific has received US Food and Drug Administration (FDA) 510(k) clearance for its Embold soft and packing coils, the company has announced in a press release. The coils are designed for use in a variety of embolization procedures.
These coils further strengthen Boston Scientific’s embolic portfolio by creating a single platform consisting of just three coils, which is designed to make it simpler for physicians to address a variety of different patient needs and anatomies, while also streamlining hospital inventory. The soft and packing coils complete the trio by building on the success of the Embold fibred coil, which launched last year and is currently available in the USA, Canada and Japan.
“The addition of the soft and packing coils now completes the Embold platform, and is expected to build upon the success we have already seen with the launch of our fibred coil last year,” said Peter Pattison, president, Interventional Oncology and Embolization, Boston Scientific. “With the full platform of Embold coils, along with our conformable embolic, Obsidio, we will be able to offer our customers a complementary and highly differentiated portfolio of embolics, enabling them to provide highly personalised care to address the unique needs of their patients.”
Alberto Alonso-Burgos (L) and Luis Chiva de Agustín (R)
Each woman is unique, and a one-size-fits-all approach is not appropriate for addressing what can be extremely complex reproductive health issues.
Natural Procreative (NaPro) technology, is a groundbreaking medical approach that focuses on understanding and treating the underlying causes of women’s health issues rather than merely addressing symptoms. Developed by Dr Thomas Hilgers in the 1990s, NaPro combines the best aspects of reproductive medicine and natural fertility awareness methods to provide personalised and effective care for women. This involves identifying and treating the root causes of infertility, irregular cycles, and other male and female conditions. NaPro’s effectiveness is supported by extensive research and a growing body of evidence. Studies have shown that NaPro can significantly improve fertility rates, with success rates rivalling or surpassing those of conventional treatments.
Up to 67% of all infertility cases can be attributed to fallopian tube disease. In cases where infertility is caused by blockage of the fallopian tubes, a simple and obvious alternative might seem to be to try unblocking the tubes in question. Fallopian tube recanalisation (FTR) is a procedure that aims to reopen blocked or damaged fallopian tubes, allowing the possibility of restoring natural conception. By reopening the blocked tube, sperm can reach the egg, potentially leading to successful fertilisation and pregnancy. This can be particularly meaningful for couples who desire to conceive without the assistance of assisted reproductive technologies. Moreover, FTR is a less invasive procedure compared to major surgeries like tubal ligation reversal or in vitro fertilisation. This makes it an appealing option for those who would prefer a natural approach to conception. Additionally, FTR is often considered a cost-effective alternative, as other approaches can be costly.
The American Society for Reproductive Medicine recommends that patients who have proximal tubal obstruction undergo selective salpingography and tubal recanalisation before considering more invasive and costly treatments. Since hysterosalpingography followed by FTR could potentially be considered for any woman undergoing infertility investigation, it is unfortunate that numerous infertility clinics remain unaware of this procedure, or they may have knowledge of it but lack access to an interventional radiologist capable of performing it. Consequently, several interventional radiologists may also lack awareness regarding the procedure and the number of potential patients who could benefit from it.
In this context, several controversial questions may arise. Within this straightforward procedure, over 85% of patients are discharged with a satisfactory outcome (successful tubal recanalisation), and more than 30% achieve pregnancy within the first year following the procedure. However, if tubal recanalisation (FTR) is indeed a simple, safe, and cost-effective method, why is it seldom utilised? Why are other more invasive techniques, which are not free of side-effects and considerably more expensive, routinely employed? Why do insurance companies include the tubal recanalisation as any other artificial fertility treatments and fail to provide coverage for this treatment of a straightforward condition such as tubal obstruction? Even when development of new materials and kits for this purpose should be considered, yet the industry appears to be blind to this.
When talking about fertility, a tailored treatment plan to meet the specific needs of each patient should be performed in the fertility unit and an interventional radiologist should play an active part in this.
Alberto Alonso-Burgos is head of the Interventional Radiology Unit and Luis Chiva de Agustín, director of the Department of Obstetrics and Gynaecology at the University of Navarra, Pamplona, Spain.
Disclosures: The authors declared no relevant disclosures.
Canon Medical has announced the commercial availability of its two latest ultrasound systems, Aplio flex and Aplio go, in Europe. With the growing challenges faced by medical staff, including high workload and work-related musculoskeletal disorders, Canon Medical recognises the importance of supporting healthcare professionals in their daily tasks, the company has said in a press release. The introduction of Aplio flex and Aplio go aims to revolutionise the healthcare market by providing compact, manoeuverable, and technologically advanced ultrasound systems that meet the evolving needs of medical practitioners.
Meeting healthcare challenges
Canon Medical has established a strong presence in the ultrasound market by incorporating user feedback into its systems. With over 50 years of Japanese development technology and a successful 20-year Aplio history, Canon Medical has consistently provided superior ultrasound solutions, renowned for their reliability.
As technology advances, the need for smarter, smaller, more portable systems becomes increasingly significant. Canon Medical has proactively responded to this trend, aligning its designs with the integration of artificial intelligence (AI) and prioritising energy efficiency. These ultrasound systems are developed with a focus on energy consumption, aligning with Canon Medical’s corporate social responsibility goals.
Advancements in AI technology
Quite often, the time required for an ultrasound examination will increase with the amount of measurements needed. In an era where AI is seamlessly integrated into various aspects of the care pathway, Canon Medical understands that to enable the necessary measures to be performed in a minimum of time, it is needed to implement applications on its systems that use AI technologies such as deep learning and machine learning.
For example, Auto IMT can automatically trace the intima-media thickness (IMT) of the common carotid artery in any area in a shorter time than in the past. Similarly, Auto EF with global longitudinal strain was developed using AI algorithm technology. Thanks to these new AI technologies, powered by Altivity, the company’s bold new approach to AI innovation, Canon Medical provides smart technologies to achieve a whole new level of quality, insight, and value across the entire care pathway.
Enhanced user experience and workflow efficiency
Canon Medical understands the importance of fast and safe operation, reducing training time for medical professionals. The redesigned control panel of Aplio flex and Aplio go ensures efficient and intuitive operation from the moment the systems are installed. With this new control panel, direct operation is simplified, promoting ease of use and productivity. Everything needed is conveniently accessible at the users’ fingertips.
Finally, both Aplio flex and Aplio go are equipped with ApliGate, an innovative technology that enhances collaboration. Whether you work at a large university or local hospital, in a private practice or imaging centre, or even outside the hospital, this tool for remotely sharing images enables you to directly connect with fellow professionals or Canon experts. You can seek advice, share discoveries, and engage in online collaboration with subject
Interventional News’ most popular stories from June included a letter from the joint editor-in-chief on the current state of interventional radiology (IR) practice and where it needs to be; an interview with a New Zealand interventional radiologist on Australasian interventional oncology (IO); and news of the launch of several devices, including for mechanical thrombectomy, and to treat peripheral arterial disease (PAD).
Teleflex has announced that the Arrow EZ-IO Needle is the first and only intraosseous (IO) needle to receive 510(k) clearance from the US Food and Drug Administration (FDA) for magnetic resonance (MR) conditional labelling. The EZ-IO Needle has a patented diamond tip designed for fast, precise and steady insertion.
According to a company press release, RevCore is the first mechanical thrombectomy device designed to address venous in-stent thrombosis. The Triever16 Curve catheter is purpose-built to be versatile for both pulmonary embolism and peripheral thrombectomy.
Biotronik shared the limited release of its Oscar (One Solution: Cross. Adjust. Restore) multifunctional peripheral catheter and start of promotional activities at this year’s Leipzig Interventional Course (LINC 2023; 6–9 June, Leipzig, Germany).
Nick Brown (The Wesley Hospital, Auchenflower, New Zealand) sat down with Interventional News at the European Conference on Interventional Oncology (ECIO; 16–19 April, Stockholm, Sweden) to discuss the current picture of IR and IO in Australasia.
According to a company press release, Merit Medical Systems has completed the acquisition of a portfolio of dialysis catheter products and the BioSentry biopsy tract sealant system.
Endologix has announced in a press release that the US Food and Drug Administration (FDA) has granted approval for the Detour System to treat patients with complex PAD.
Interventional News’ joint editor-in-chief Andreas Adam traces the evolution of interventional radiology and shares what he believes the modern interventional radiologist needs to have in their armoury and have access to, in order to provide the best care to patients.
A company press release notes that the SurVeil DCB may now be marketed and sold in the USA to physicians for percutaneous transluminal angioplasty, after appropriate vessel preparation, of de novo or restenotic lesions (≤180mm in length) in femoral and popliteal arteries having reference vessel diameters of 4mm to 7mm.
Argon Medical has announced the launch of the SuperCore Advantage semi-automatic biopsy instrument as the newest addition to its soft tissue biopsy product portfolio in the USA.
The ‘Connect the world: Japan’ session at this year’s Leipzig Interventional Course (LINC 2023, 6–9 June, Leipzig, Germany)—in collaboration with the Japanese Endovascular Treatment Conference (JET)—sparked discussion surrounding the latest data in femoropopliteal interventions.
Why is clot removal crucial for patients suffering from DVT? What are the major benefits of a lytic-free thrombectomy? Watch Michael Lichtenberg (Arnsberg, Germany) present the outcomes of the Arnsberg ClotTriever Study which confirms the safety and efficacy of the Inari ClotTriever system. He also highlights the cost effectiveness of the device.
“I am confident to call a system efficient if I can remove more than 90% of the clot in acute deep vein thrombosis (DVT). Our data confirmed over 95% clot removal using the ClotTriever system”, explains Lichtenberg. “The fact that this treatment option gives us the possibility to completely avoid thrombolytics is a huge advantage.”
This confirms that the outcome of the Arnsberg ClotTriever Study is fully aligned with CLOUT results—the only registry capturing data on mechanical thrombectomy in DVT. Both studies conclude that there is 0% vessel damage with minimal blood loss using a single-session treatment.
Lichtenberg believes these results are very promising with the potential for long-term benefits when treating patients with DVT. “More data are needed, and more data are coming”, says Lichtenberg. “our centre is part of the DEFIANCE randomised controlled trial (RCT). Its goal is to prove that mechanical thrombectomy is superior to anticoagulation alone. We look forward to seeing the results of this latest trial.”
This video was filmed by Inari Medical and is being sponsored for distribution in association with Vascular News, Interventional News, Venous News and CX Vascular. Biba Medical bears no responsibility for the assets used in the production of this video.
A French group of interventional radiologists and urologists has recently published the results of its randomised, multicentre, open-label, phase 3 superiority trial of prostate artery embolization (PAE) versus medical therapy (PARTEM) in The Lancet. The group, of whom Marc Sapoval (Hôpital Européen Georges Pompidou, Paris, France) is the corresponding author, states in its publication that the PARTEM trial met its primary endpoint of clinically significant superior reduction of International Prostate Symptom Score (IPSS) after PAE at nine months compared to following combined medical therapy (CT), “in patients who failed to improve after single alpha-blockers therapy”.
The authors detail that “the aim of the trial was to compare effect on lower urinary tract symptoms (LUTS) of PAE versus medical treatment in patients with symptomatic benign prostate hyperplasia (BPH) who still complained of bothersome LUTS despite >1 month of treatment with alpha blockers”.
Also noted in the introduction to the paper was the fact that, to the authors’ knowledge, “this is the first randomised trial showing that PAE provides a clinically significant benefit over [CT]”. Additionally, they found that embolization provided the PAE cohort with better sexual function compared to the CT arm.
The authors set out the background to their study as being that PAE is an “increasingly recognised treatment option” owing to its “good risk/efficacy profile”.
Sapoval et al carried out their study in 90 randomised patients (aged 50 to 85 years) between September 2016 and February 2020, of whom 44 and 23 patients were assessed for the primary endpoint in the PAE and CT groups, respectively. The study took place across 10 French hospitals and the population was selected based on having bothersome LUTS defined by an IPSS >11, quality of life >3 (according to the last question of the IPSS questionnaire), and BPH ≥50 ml resistant to alpha-blocker monotherapy.
The CT group received oral dutasteride 0.5mg/tamsulosin hydrochloride 0.4mg per day.
The authors also outline that four patients in the PAE group underwent unilateral embolization, of whom two underwent a second attempt at bilateral PAE. “Unilateral embolization was done when it was impossible to catheterise the prostatic artery selectively,” they elaborate, explaining that this was related to excessive angulation, calcification or stenosis.
The PAE cohort’s nine-month change in IPSS was −10.0 (95% confidence interval [CI]: −11.8 to −8.3), versus −5.7 (95% CI: −7.5 to −3.8) in the CT group. The authors go on to note no treatment-related adverse events or hospitalisation for either group, and the respective number of invasive prostate retreatments in the PAE versus CT groups at nine months was five versus 18.
From their study, Sapoval et al have been able to conclude that “in patients with BPH ≥50 ml and bothersome LUTS resistant to alpha-blocker monotherapy, PAE provides more urinary and sexual symptom benefits than CT up to 24 months”.
Moreover, as part of the study, the authors carried out an economic evaluation, as they recognise that “the choice of an optimal treatment strategy for BPH is also informed by economic data due to the high prevalence of the condition and the costs of surgery”. Sapoval et al add that “the selection outcome for the economic evaluation was driven by the clinical relevance of treatment success at nine months and the limited sensitivity of generic quality of life measures EQ-5D over a short period”.
Sapoval gave the following statement to Interventional News regarding the importance of his and colleagues’ findings: “This study helps to advise patients suffering from bothersome LUTS related to BPH >50 ml that PAE may be a valid option able to provide significant symptom relief.”
The Cardiovascular Interventional Radiological Society of Europe (CIRSE) 2020 Standards of Practice document for gynaecological and obstetric haemorrhage are among the most comprehensive guidelines in interventional radiology (IR) for obstetric interventions. The guidelines cover the use of IR for both elective and emergency procedures. The indications for IR are for postpartum haemorrhage and post-surgical bleeding in the emergency setting, and electively for the embolization of tumours either as a primary treatment or as an adjunct to surgery; embolization for arteriovenous fistulae and malformations; and the elective use of prophylactic occlusion balloons in abnormal placentation.
The guidelines cover the basics of anatomical knowledge required to perform an effective embolization. The operator must be aware of potential causes of failure of embolization including failure to search for and treat collateral supply to the uterus. Recommendations are made for appropriate imaging equipment which should ideally consist of an IR or hybrid theatre setting with digital subtraction angiography. However, it is recognised that lifesaving embolization may be required and can be performed successfully in an obstetric theatre using portable image intensifiers. In such non-optimal settings, the operator must be aware of the higher potential for non-target embolization secondary to poor visualisation. The guidelines also suggest having available an ‘emergency haemorrhage control box’ which would have all the essential equipment needed to provide this procedure in a setting remote to the IR suite.
Active extravasation is only seen in 21–52% of cases and is mostly seen with uterine atony. In most cases of postpartum haemorrhage, a focal bleeding point is not identified. It is important in this situation to perform bilateral empirical embolization of the uterine arteries. The embolic agent of choice in this situation is absorbable gelatine sponge. This allows for later recanalization of the artery when it has healed. In an emergency, patients usually require rapid catheter angiography and embolization. However in a more elective situation, for example where there is a slow bleed, but the patient is not unstable, a triple phase computed tomography (CT) scan may be useful in identifying a source of bleeding, thus enabling targeted embolization. If focal bleeding points are identified, for example, a pseudoaneurysm, permanent embolic agents can be used, such as coils. The choice of embolic agent is dependent on operator expertise and availability.
Approximately 5–10% of patients undergoing embolization may re-bleed. Causes of failure of embolization include development of arterial spasm, collateralisation after primary embolization of the uterine arteries, bleeding from non-uterine artery sources, previous surgical ligation or dilatation and curettage, unilateral embolization, and abnormal placentation. Potential complications from embolization include non-target embolization resulting in limb and buttock claudication, and necrosis of structures with pelvic arterial supply. These risks can be mitigated by using high-quality imaging, avoiding the use of very small particles, and being aware of collateral and cross-uterine blood supply.
The placement of prophylactic occlusion balloons in the management of patients with abnormally adherent placenta is also becoming more commonplace with the increase in incidence of abnormally adherent placenta and this is also discussed briefly in the guidelines.
Postpartum haemorrhage remains the leading cause of maternal morbidity and mortality worldwide. In 2015, postpartum haemorrhage was reported to be responsible for more than 80,000 maternal deaths worldwide. The use of embolization in the treatment of obstetric haemorrhage was first reported in the 1970s. Since then, the use of IR in the treatment of both elective and emergency haemorrhage has increased and the success rates of embolization for postpartum haemorrhage are reported as being between 79% and 100%. Despite this, the rates of hysterectomy remain high and the use of IR for the treatment of postpartum haemorrhage is still significantly underutilised. Much more needs to be done to promote the availability and access to IR for patients. CIRSE’s 2020 guidelines and the 2022 International Federation of Gynaecology and Obstetrics guidelines both recommend the use of IR after failure of conservative measures to control haemorrhage, and before contemplating surgery. We need to move beyond these guidelines to make this a reality in practice for patients.
Lakshmi Ratnam is a consultant diagnostic and interventional radiologist at St George’s University Hospitals NHS Foundation Trust in London, UK.
Disclosures: The author declared no relevant disclosures.
Terumo Aortic have today announced that the Japanese Pharmaceuticals and Medical Devices Agency (PMDA) has granted approval of the Thoraflex Hybrid Frozen Elephant Trunk (FET) device for commercial sale in Japan for the treatment of patients with complex aortic arch disease.
Thoraflex Hybrid
Thoraflex Hybrid is a single use medical device combining a Gelweave polyester graft with a Nitinol self-expanding stent graft and is indicated for the open surgical repair or replacement of damaged or diseased vessels of the aortic arch and descending aorta with or without involvement of the ascending aorta in cases of aneurysm and/or dissection.
Kotaro Yoshida, senior vice president of Asia Pacific added: “The PMDA approval of Thoraflex Hybrid is a fantastic opportunity for Terumo Aortic in Japan. This innovative hybrid device complements our open surgical graft and endovascular portfolio currently available in Japan; the approval of this device will contribute significantly in the delivery of our commitment to providing solutions for every aorta.”
Thoraflex Hybrid received CE Mark approval in 2012 and US Food and Drug Administration (FDA) approval in 2022 with more than 13,000 devices sold around the world.
Osteoarthritis is the most common form of arthritis, and for patients who are not yet ready for surgery, RFA pain management products provide minimally invasive relief without the use of opioids by denervating the nerves in the area causing the patient pain.
From the NICE announcement: “Radiofrequency energy is used to denervate the target nerves. The radiofrequency energy can be delivered as conventional radiofrequency, cooled radiofrequency or pulsed radiofrequency. The aim is to reduce pain and delay the need for knee arthroplasty. There is good evidence to show that this procedure relieves pain in the short term. There are no major safety concerns, and the complications, including numbness, are well recognised.”
“The new interventional procedure recommendations published by NICE is a great step forward to help adopt radiofrequency ablation therapy for the treatment of osteoarthritic knee pain,” said Robin Correa, consultant in Pain Management and Anaesthetics, University Hospitals Coventry and Warwickshire NHS Trust (Coventry, UK). “Having observed the transformation in the quality of life of patients under my care using this treatment, I am delighted to see the publication of the NICE recommendations. I hope this will now help to increase awareness of this innovative therapy leading to improved outcomes for many more patients.”
Microvention, a wholly owned subsidiary of Terumo, has announced that the Eric retrieval device is now commercially available in the USA for ischaemic stroke treatment, having received 510(k) clearance from the US Food and Drug Administration (FDA) on 31 March 2022.
“The Eric retrieval device’s ability to rapidly interact and trap the embolus, coupled with its low-profile design, facilitates synergistic use with SOFIA catheters [Microvention] and reduces time to recanalisation,” said Adel Malek (Tufts Medical Center, Boston, USA). “We are excited to have been the first centre in Massachusetts to have clinical experience using the Eric device and since then have integrated Eric into our stroke practice.”
Eric delivers thrombus control inside and outside of the device; offers no clot integration wait-time to drive procedure efficiency; and offers versatile treatment options for mechanical thrombectomy, as per a press release from Microvention.
The device is a self-expanding, laser-cut clot retriever with multiple retrieval cages, located on a pusher wire delivery system. Unlike tubular stents, in which the ends are open, Eric is designed to control the thrombus through its cage-like design. It has an atraumatic design that conforms to the natural vessel, offering soft, outward radial force, minimal vessel wall contact, and an exceptionally flexible design, the release also states.
Eric is offered in three sizes that treat a wide vessel size range of 5.5mm down to 1.5mm, and is compatible with Microvention’s Headway 17 and Headway 21 microcatheters. As part of an initial limited release, the first Eric cases in the USA were performed by the neurovascular team at Riverside Methodist in Columbus, USA—consisting of Peter Pema, Abdulnasser Alhajeri and Ronald Budzik—in February 2023.
Microvention states in the release that ERIC delivers safe and effective outcomes, showing similar results in terms of successful revascularisation, and clinical and safety outcomes, when compared to other retrieval devices.
With the introduction of the Eric retrieval device, the company now claims to offer a “comprehensive and streamlined” portfolio of stroke solutions, delivering compatibility, versatility and speed “unlike any other”. In addition to Eric, Microvention’s integrated stroke solution portfolio includes the Sofia catheters, Bobby balloon guide catheter, Wedge microcatheter, Headway microcatheters, and Traxcess guidewire.
“Today’s introduction of the Eric retrieval device is guided by our continued commitment to meaningful advancement in stroke innovation,” said Carsten Schroeder, president and CEO of Microvention. “Eric underscores this commitment to offering physicians and patients vital versatility when every second counts. We are thrilled to now offer a comprehensive, fully integrated stroke portfolio that delivers compatibility, versatility, and speed—a true standout in the neurovascular space. This is the result and honour of working side-by-side with leading physicians around the world to identify the evolving needs in patient care, and then transform those insights into innovative technologies that help to save patient lives.”
As announced at the Society for Vascular Surgery (SVS) Vascular Annual Meeting (VAM 2023; 14–17 June, National Harbor, USA), the Advance Serenity hydrophilic percutaneous transluminal angioplasty (PTA) balloon catheter product line is now available with even more options. Interventionists who perform peripheral intervention procedures in the USA and Canada now have access to the Advance Serenity product for below-the-knee and above-the-knee procedures to treat patients with peripheral artery disease (PAD).
Now, Advance Serenity is available to help physicians treat complex lesions with more balloon sizes. Advance Serenity is still made with its laser-formed, low-profile entry tip. The hydrophilic coating provides lubricity to navigate through diseased vessels with reduced friction. The Advance Serenity 18 is now larger, with balloon diameters from 5mm to 10mm, and is compatible with 4, 4.5, 5 and 5.5Fr sheaths to help physicians treat complex lesions with options to include larger-vessel PAD. The Advance Serenity 14 and Serenity 18 balloons are still available in 4Fr sheath compatibility and 2mm to 4mm balloon diameters. All Advance Serenity products are available in both the USA and Canada and will be available in Europe in the coming months.
“After looking at the needs of patients with this condition, we built on our previous innovation and are excited to expand the sizes, uses and availability of this product. The Serenity balloon complements our balloon portfolio for interventionists who are treating patients with complex lesions,” said Alec Cerchiari, director of product management for Cook’s PAD and Venous Specialty.
The US Food and Drug Administration (FDA) has granted approval for Cook Medical to initiate an investigational device exemption (IDE) study on the Zenith fenestrated+ endovascular graft (ZFEN+).
The clinical study will assess the safety and effectiveness of the ZFEN+ in combination with the Bentley InnoMed BeGraft balloon-expandable fenestrated endovascular aortic repair (FEVAR) bridging stent graft system (BeGraft) for the endovascular treatment of patients with aortic aneurysms involving one or more of the major visceral arteries.
The ZFEN+ is predicated on the commercially available Zenith fenestrated abdominal aortic aneurysm (AAA) endovascular graft, but extends the proximal margin of aneurysmal disease that can be treated endovascularly to include patients with more complex aortic disease. For patients with complex aortic disease, the only currently established treatment option is open surgical repair.
“The clinical community has been asking for a durable, low-profile commercial device that allows them to easily treat more patients,” Johnny LeBlanc, director of Aortic Product Management, Cook Medical, was quoted as saying in a press release. ” We pioneered this technology with key thought leaders and continue to listen and innovate to the market needs. The ZFEN+ has received breakthrough device designation from the FDA, so we are excited to see this innovation progress into a clinical study. The ZFEN+ is the next generation and future of fenestrated technologies.”
“Outside the USA, Bentley has supplied 300,000 BeGraft stents to patients in 80 countries around the world. We are pleased that this study approval of the FDA brings us one step closer to making our leading technology also available to American patients suffering from vascular diseases,” said Sebastian Büchert, CEO, Bentley.
The ZFEN+ clinical study is a prospective, multicentre, single-arm study that will include sites in the USA and Europe. At this time, the FDA has approved enrolment of the first 30 patients. Ultimately, Cook intends to enrol 102 patients in the pivotal study. The primary safety endpoint is a composite measure of device technical success and procedural safety within 30 days. Likewise, the primary effectiveness endpoint is a composite measure of freedom from aneurysm-related mortality and freedom from clinically significant reintervention through 12 months post procedure. A composite measure is a group of variables collected during the clinical study and analysed.
“The ZFEN+ endovascular graft will meet a significant need for our patients,” said Gustavo Oderich (University of Texas Health Science Center at Houston, Houston, USA), who is the global principal investigator of the study. “There are not many options to treat complex aortic aneurysms other than open repair or off-label use of devices. Even long after off-the-shelf devices become available, the ZFEN+ will offer a tailored approach specific to the patient anatomy. The ZFEN+ clinical study will provide a benchmark for safety and effectiveness of a less invasive option to treat complex abdominal aortic aneurysms.”
Following the publication of an animal study examining the performance of embolization coils in arteries in the Journal of Vascular and Interventional Radiology (JVIR) in 2019, a second, similar study, published in the May 2023 issue of JVIR, examined fibered and non-fibred embolization coil performance, this time in the venous system.
In this newly published venous ovine study, fibred Nester (Cook Medical) coils and non-fibred coils were deployed in 24 veins in six sheep. The study’s data confirmed that fibered coils demonstrate several advantages over non-fibred coils. These advantages include the following:
Fibres significantly boosted the immediate occlusive capacity of coils. In the study, fibred coils achieved stasis in 5.3 minutes, while non-fibred coils took nine minutes.
A significantly lower average radiation dose was required when fibred coils were used: 25.3mGy for fibred coils compared with 34.9mGy for non-fibred coils.
The venous fibre study also substantiated the findings of the earlier arterial fibre study: The two studies found that fewer fibred coils are needed to achieve acute occlusion compared to bare metal coils. Both studies confirmed that significantly less coil length is needed if the coil is fibred.
In the venous fibre study, on average five fibred coils, or 70cm of fibred coil length, were needed to achieve occlusion compared with 8.75 non-fibred coils, or 122.5cm of bare metal coil length.
In the arterial fibre study, on average 1.3 fibred coils, or 9.1cm of coil length, were required to achieve occlusion, compared to 3.2 non-fibred coils, or 22.4 cm of non-fibred coil length, that was needed to obtain occlusion.
Should the study results translate to the human experience, patients treated with fibred coils could potentially experience shorter procedure times, require fewer implants and have less radiation exposure to achieve the same outcomes.
In this venous fibre study, a new approach was also applied to generating histologic images. A unique method of cutting 5µm thin sections of tissue with metallic implants was developed by Cook Research Incorporated (CRI) and Alizée Pathology. Thin sectioning results in clearer and more detailed histologic images, allowing a pathologist to read and interpret tissue changes. An image showing a 5µm thick microscope slide of Cook embolization coils in an ovine vein can be seen on the front cover of the May 2023 issue of JVIR.
“When we see in vivo results like this in studies, we hope the same benefits will be applicable to human patients,” said Remco van der Meel, director of product management for Cook’s interventional specialty. “We are constantly evaluating our embolization portfolio, exploring cutting-edge technology and gathering data to create new technology. Additionally we want to understand how we could best support our customers in achieving the best possible outcomes for patients. This study helps us make data-based decisions on how to best meet the needs for effective embolisation in a cost-efficient manner, while reducing exposure to ionising radiation for both doctor and patient. These are key elements in today’s healthcare environment.”
Surmodics has announced the receipt of US Food and Drug Administration (FDA) approval for the SurVeil drug-coated balloon (DCB).
A company press release notes that the SurVeil DCB may now be marketed and sold in the USA to physicians for percutaneous transluminal angioplasty, after appropriate vessel preparation, of de novo or restenotic lesions (≤180mm in length) in femoral and popliteal arteries having reference vessel diameters of 4mm to 7mm. The SurVeil DCB received CE mark Certification in the European Union in June 2020.
“Obtaining FDA approval for our SurVeil DCB is one of the most important achievements in Surmodics’ history,” said Gary Maharaj, president and CEO of Surmodics. “It represents a major milestone in our efforts to develop next-generation products to help millions of people affected by peripheral arterial disease and the physicians that treat them. I would like to thank our internal SurVeil DCB team and our external advisors, investigators and partners for their multi-year efforts to make this achievement possible.”
Abbott has exclusive worldwide commercialisation rights for the SurVeil DCB. Surmodics will manufacture and supply the product and realise revenue from product sales to Abbott and a share of profits from Abbott’s third-party sales. Surmodics will also receive a US$27 million milestone payment from Abbott. The company expects to recognise approximately US$24 to US$24.5 million of revenue related to the milestone payment in the third quarter of its fiscal year 2023.
Maharaj continued: “Building on our recent progress, Surmodics remains focused on supporting Abbott and its exclusive worldwide commercialisation rights for the SurVeil DCB. We will discuss details on the developments and update our fiscal year 2023 financial guidance during our third quarter earnings call.”
“I am excited that the Surveil DCB will be available to treat patients in the USA,” said Kenneth Rosenfield (Massachusetts General Hospital, Boston, USA), co-principal investigator of the TRANSCEND clinical trial. “The Surveil DCB is the next generation DCB as established by results from the TRANSCEND trial which is the only head-to-head pivotal study that has been conducted versus the market-leading DCB. The Surveil DCB successfully demonstrated non-inferior safety and effectiveness at two years post-treatment with a substantially lower drug dose.”
On 5 June, the Society of Interventional Radiology (SIR) held a briefing in Washington DC, USA, of which the focus was benign prostate hyperplasia (BPH). The briefing took place in conjunction with the US Congressional Men’s Health Caucus. Shivank Bhatia (University of Miami, Miami, USA) took to the podium to introduce prostate care as an “issue of great importance to men’s health”—all the more relevant the week before National Men’s Health Week (12–18 June) in the USA. His talk during the session centred around prostate artery embolization (PAE).
It was Bruce Kava, professor of urology at the University of Miami, who presented first during the session, outlining what BPH is—“bigger is not always better, and at some point [around the age of 30 for most men], the prostate begins to grow”. The more severe consequences of an enlarged prostate, the audience heard, can include “urinary retention, recurrent infection, bladder stones, or [even] kidney failure”. The symptoms as a whole are classified as lower urinary tract symptoms, or “LUTS”, Kava explained—“the burden of LUTS for people with BPH is immense”. The symptoms are not usually life-threatening, Kava went on, but they create bother, “which translates to lower quality of life, [including] anxiety, depression, and loss of productivity”. Kava then informed his audience that around 25% of men over the age of 50 have LUTS of “at least moderate severity”.
Access to care for BPH—namely medication or surgical procedures—differs based on race, Kava lamented, stating that it is “less for African American and Hispanic males”. Members of these groups, therefore, “present to the emergency room much more frequently than Caucasians do”.
BPH treatment options
Treatment, when it is accessible, centres on reducing symptom severity, namely improving urinary flow, reducing urinary tract infections, and improving renal insufficiency. Kava also noted that BPH treatment is designed to slow the growth of the prostate. However, he pointed out that medications show only “modest effects” in terms of International Prostate Symptom Score [IPSS] reduction. The minimally invasive surgical treatment transurethral resection of the prostate (TURP) can be an outstanding option, Kava suggested, but side-effects, which include an overnight hospital stay, occasional bleeding (in particular for larger prostate glands), and ejaculatory dysfunction may mean it is not always the perfect option for some men.
Nowadays, Kava explained that in urology, they have been offering treatment via other modalities, including a number of laser procedures, prostatic urethral lift, water vapour thermotherapy, and aquablation. Size of the prostate is often the key determinant of success with these modalities. For instance, prostatic urethral lift and water vapour thermotherapy are more efficacious with smaller prostate glands. There is demand for a minimally invasive modality that is highly effective in patients with larger prostates, that offers a rapid recovery, and that reduces the risks of transfusion and other adverse effects.
The advent and advantages of PAE
Bhatia, who is chair of the Department of Interventional Radiology and professor of urology, then took to the podium to speak about prostatic artery embolization (PAE) as the answer to other treatments’ size-related limitations. Bhatia first set out how image-guided interventions—such as PAE—are largely unknown to the public. He then explained that PAE involves using small microsphere to embolize and therefore cut off blood flow to large prostates, causing them to shrink.
“Ninety-nine per cent of men eligible for treatment for BPH do not receive invasive therapy,” Bhatia shared, adding that for some, their reason for avoiding treatment will be that they do not like the options available—such as resection. This is where minimally invasive options such as PAE come in. Bhatia noted that “PAE has been [US Food and Drug Administration]-approved since 2016.”
Bhatia relayed that advantages of PAE over surgical treatment are that it does not require general anaesthesia, is a same-day, outpatient procedure, with no size limit of the prostate. He explained that one can avoid the risk of bleeding and adverse impact on sexual function associated with surgical procedures. From the patient’s perspective, PAE offers a “90% success rate”, the benchmark for which Bhatia described as around a “50% improvement in symptoms [according to the IPSS]”. After PAE, he went on, the prostate will keep shrinking and will not start growing again “for three to five years”.
PAE at the University of Miami
Bhatia then shared his centre’s experience treating over 1,000 patients over six years, as presented at the SIR 2023 annual scientific meeting (4–9 March, Phoenix, USA), before thanking his patients for having put “their trust in [him]” to have the PAE procedure. Among the study’s notable findings was a persistent, years-long reduction in prostate size among the patients, he underlined, as well as dramatic decreases in patients’ IPSS and self-reported quality of life. Bhatia mentioned that one of the most crucial limitations of PAE was the lack of awareness about this procedure.
Following this, one of the first 25 patients treated by Bhatia, Roland Klein, spoke from his point of view on the merits of PAE.
“I started having symptoms long before PAE existed,” Klein provided as background to his experience, conveying how he began researching the various treatments available to him, with his symptoms worsening at this time. “I decided I was going to fly to Brazil to try PAE,” he explained, “because it was the least invasive treatment you could possibly get”. As he was continuing to read up on PAE, Klein reported that he saw that the University of Miami was starting a trial programme, “so [he] contacted Dr Bhatia […] was told [he] would be a candidate, and [he] went down and had the procedure”. Klein then emphasised how, in his eyes, “the procedure is a ‘nothing’ procedure”, involving only a “pinhole” incision and a few hours in the hospital pre-, during and post-procedure, in total. He reported how he experienced “a little pain” when urinating for “about three to five days” before returning to work. “It has [now] been nine years, and I still do not have any issues with urination,” he concluded.
In summary, Bhatia and Kava delivered a briefing to the Congressional Men’s Health Caucus, explaining different options available to treat symptoms related to enlarged prostate, with an emphasis on PAE, a minimally invasive option with no risks of sexual side-effects or leakage, no need for a urinary catheter, and efficacy similar to more invasive options.
Shang Loh is chief of vascular surgery and endovascular therapy at Penn Presbyterian Medical Center and professor of clinical surgery at the University of Pennsylvania (both Philadelphia, USA). Ahead of the Embolization for Vascular Surgeons: Techniques, Tips and Tricks lunch session at the Society for Vascular Surgery (SVS) Vascular Annual Meeting (VAM; 14–17 June, National Harbor, USA), he spoke to Interventional News about the embolization-related challenges vascular surgeons can come up against in their practice, and how cross-specialty partnership is key for maximising the quality of this type of therapy.
IN: Would you be able to outline the embolization procedures that fall into the vascular surgery wheelhouse?
SL: I don’t think that any embolization procedure is necessarily out of the wheelhouse for a vascular surgeon if they have the desire to learn the skills. However, traditionally, the majority of embolization work falls into the following categories: primary treatment of aneurysms such as splenic, mesenteric, and pseudoaneurysms; adjuncts to aortic aneurysm treatment including embolization of branch vessels and accessory vessels; endoleak treatment; chronic dissection management; venous disease; arteriovenous (AV) or venous malformations; trauma and bleeding.
IN: What does your vascular surgery practice focus around, particularly from an embolization perspective?
SL: My practice involves all areas of vascular surgery but primarily on the arterial side. My practice is mostly focused on aortic diseases but I also do aneurysm work in other areas, as well as peripheral and cerebrovascular work. I perform all my own embolizations except for venous disease and AV/venous malformations. Trauma is handled mostly by interventional radiology (IR) at our hospital but I will perform my own trauma embolizations if I am already involved in their care. The majority of my embolization work revolves around adjunct treatments for aortic aneurysms (such as branch or accessory vessel occlusion), embolization for type II endoleaks, embolizations for aortic dissections, and embolization as primary treatment for other peripheral aneurysms. I also teach courses, along with Dr Darren Schneider, on various techniques for embolizations of type II endoleaks and speak about embolization techniques.
IN: What are some of the challenges that vascular surgeons may face when doing these procedures?
SL: One of the main challenges is acquiring the proper skill set. This is heavily dependant on prior training with older surgeons not necessarily having been trained in this. As a corollary, surgeons starting out in the embolization realm may find challenges in getting the proper inventory in place—and having the right imaging equipment. However, the focus of sessions such as this one is to help bridge that gap and allow them to incorporate these elements into their practice if they desire. The other main challenge is that other specialties, such as interventional radiology, perform similar procedures. It is critically important to discuss this from a multidisciplinary perspective in order to determine everyone’s role in treating the different types of patients. I strongly believe in cross-specialty participation in embolization and believe a partnership provides the best care for patients.
IN: In your experience, what does this cross-disciplinary approach to caring for patients who require an embolization entail?
SL: As I previously mentioned, I strongly believe in a partnership with a cross-specialty approach to embolization. This skill set is present in a few different specialties. The most important step is to have representation from all the specialties at the table and to formally outline areas that are treated by one specialty versus areas treated by more than one. This can also include how patients will be referred. It is also important to decide how the emergency cases will be handled and whether there should be a shared call schedule for these. This is most important in the trauma setting. This removes any confusion when referring patients and when patients need emergent treatment.
The 50th patient has been treated using the Epione robot from Quantum Surgical by the team of Laurent Milot, deputy chief vascular and interventional radiology at the Hospices Civils de Lyon (HCL; Lyon, France), highlighting a successful collaboration only eight months post-acquisition.
Installed in November 2022, the HCL team are convinced of the value of this platform from Quantum Surgical and celebrating that 50 patients have benefited from Epione. Epione can be used to treat early-stage abdominal tumours that are inoperable or particularly difficult to reach, due to their size or location.
HCL is the second hospital in the world offering this platform to their patients. The first Epione robot was acquired by the Institut Gustave Roussy (Villejuif, France) in January 2022 where the team has already treated more than 100 patients. The very first patient in the USA was also successfully treated using the Epione robot at Baptist Hospital in Miami (Miami, USA) last month.
Beyond the new procedural advantages it provides, Epione makes it possible to offer patients a minimally invasive treatment. It improves their comfort and facilitates their recovery, due to the absence of surgery.
For practitioners and hospitals, Epione combines advanced robotic assistance with image-guided navigation and ablation confirmation tools to promote the standardisation of minimally invasive tumour ablation procedures.
“I am very pleased with this milestone, which above all underlines the perfect match between the HCL teams and the Epione robot, which delivers all its promises. We are very excited to continue to explore the many benefits of Epione and to support the next steps in the development of robotics in interventional radiology. This will undoubtedly lead to significant progress and extend hope for patients we do not have treatment solutions for so far” explains Milot.
“The implementation of the Epione robot within the Hospices Civils de Lyon is a success: in eight months, 50 patients have already benefited from our technology, as part of their cancer treatment. Prof. Laurent Milot’s teams are particularly enthusiastic. We are delighted with this collaboration, which improves access to care and patient comfort” said Bertin Nahum, president and co-founder of Quantum Surgical.
Merit Medical Systems has announced that it has completed the acquisition of a portfolio of dialysis catheter products and the BioSentry biopsy tract sealant system.
“We are selectively investing to expand our product portfolio in key strategic markets that leverage our existing commercial footprint,” said Fred P Lampropoulos, Merit’s chairman and CEO. “These acquisitions strengthen our position in the dialysis and biopsy markets, and expand the foundation of our growing specialty dialysis device offering, which includes Wrapsody cell-impermeable endoprosthesis, Haemodialysis Reliable Outflow (HeRO) graft, and the Surfacer system devices. Many dialysis patients rely on these solutions to receive vital therapies. Combining this broad portfolio of interventional solutions within Merit will allow us to leverage our physician relationships and commercial infrastructure to serve more patients in the multi-billion dialysis market.”
The acquired dialysis catheter portfolio includes the BioFlo DuraMax dialysis catheter with Endexo technology, a proprietary material that a press release states is more resistant to thrombus, in vitro, compared to conventional non-coated dialysis catheters. In addition to the dialysis portfolio, Merit also acquired the BioSentry biopsy tract sealant system from AngioDynamics, which complements Merit’s “comprehensive” biopsy portfolio, according to the press release. The BioSentry system is designed specifically to reduce the incidence of biopsy-related pneumothorax. Pneumothorax, the press release states, is a potentially life-threatening complication that can extend hospitalisation and occurs in approximately one-quarter of patients undergoing lung biopsy.
Merit’s purchase of the AngioDynamics dialysis catheter portfolio follows Merit’s recent acquisition of the Surfacer inside-Out access catheter system from Bluegrass Vascular Technologies. The Surfacer is a “unique device designed to obtain right-sided central venous access in patients with venous obstructions”, and the press release states that this provides this population “with access to life saving therapies including haemodialysis and chemotherapy”.
Editor-in-chief Andreas Adam, author of this letter
Interventional radiology (IR) is unique amongst procedural disciplines because its ‘parent specialty’ is a diagnostic discipline that has no infrastructure for clinical practice. Charles Dotter, who performed the first angioplasty on 16th January 1964, recognised the risks inherent in this unique situation, stating: “If my fellow angiographers prove unwilling or unable to accept clinical responsibilities, they face forfeiture of territorial rights based solely on imaging equipment others can obtain and skills that others can learn.”
IR requires four sets of skills: first, its practitioners need to be able to interpret the radiological images that they need for their procedures. Second, they must have sufficient manual dexterity to master the necessary techniques. Third, they need to understand the pathology, physiology, and clinical aspects of the diseases that they encounter. Finally, they need to be able to assess a clinical situation and decide how best to treat the patient, sometimes quickly and based on incomplete information. The first two requirements pose no significant challenges. Image interpretation is the essence of radiology. And although not all radiologists are particularly dextrous, many have the practical skills for the performance of common interventional radiological procedures. Knowledge of pathology, physiology and clinical medicine is more problematic. In some countries, including the UK, substantial clinical experience used to be expected before beginning radiological training.
In the 20th century, many British radiologists had a formal qualification in internal medicine before radiology training, but this is now unusual. As imaging became more complex, many training organisations sacrificed clinical experience in favour of more lengthy training in radiology. The ability to make swift decisions about treatment is a substantial challenge. Most diagnostic radiologists are thinkers and problem-solvers. Radiology attracts people who enjoy detecting abnormalities and using the related clues to suggest a possible diagnosis. This is a complex and immensely valuable skill and has placed imaging at the heart of modern medicine. Most radiologists have the mindset of a physician rather than a surgeon. A “surgical mindset”, however, is much more useful in IR, and not only because timely action is necessary in emergency situations. Diagnostic radiologists are not usually required to make decisions on clinical management: their role is to provide accurate information which informs decisions taken by others. Interventional radiologists must consider the risks and potential benefits of intervention, which often depend on the likelihood of success of the intended procedure.
For a few decades after the discovery of X-rays in 1895, radiotherapy and diagnostic radiology were practised within the same specialty. Radiation oncology separated from diagnostic radiology in the middle decades of the twentieth century. One important reason for the separation was that both disciplines had increased in complexity, making the volume of the required knowledge too great for one specialty. But there was also an obvious need for different patterns of practice. Radiation oncologists must work as clinicians. Although this is just as true of IR in most countries, it remains an integral part of radiology. Even in the USA, where it is recognised as a primary specialty, and in the UK, where it is a formally accredited subspecialty of radiology, those training to be interventional radiologists spend much of their time learning imaging rather than clinical and procedural skills. And most interventional radiologists spend a lot of their time reading diagnostic imaging studies unrelated to the patients they are treating.
A true clinical specialty of IR would make a huge contribution to contemporary patient care. Its practitioners would spend more of their training years learning clinical and procedural skills, rather than irrelevant facts about aspects of imaging they are unlikely to encounter in their daily practice. They would have the appropriate supporting staff and infrastructure to hold outpatient clinics. They would attend tumour boards as treating physicians and not as imagers, which would allow the procedures that they can offer to be explained fully and to be considered alongside other mainstream treatments rather than as ‘optional extras.’
The current pattern of practice is a barrier to interventional oncology’s expansion. It is not unusual for patients to be deemed suitable for ablation, to then undergo surgery.. This happens because enthusiastic young surgeons see the patients afterwards and persuade them to have surgery, genuinely believing that this is best treatment for them. The solution would be to hold joint clinics. But this could happen only if interventional radiologists spent more of their time seeing patients and less interpreting diagnostic studies.
The arguments in favour of IR being a primary clinical specialty are compelling. After all, radiation oncologists are just as dependent on imaging as interventional radiologists but would find it impossible to serve their patients well without being able to practise as
true clinicians.
Many interventional radiologists do not receive systematic training in all the procedures that they undertake in routine practice, especially the more complex ones. The disproportionate emphasis on diagnostic radiology training precludes the acquisition of sufficient clinical experience. The examination of the European Board of Interventional Radiology (EBIR) under the auspices of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) is a commendable effort but is a ‘voluntary supplemental examination’ which cannot be compared with equivalent tests undertaken by surgeons in their own disciplines. Interventional radiologists could point out that vascular surgeons undertaking IR procedures could be trained better, but that does not excuse the
lack of a more robust system of training in IR.
The greatest responsibility for the failure of IR to establish itself as a real clinical specialty lies with institutions responsible for establishing curricula for training and holding examinations. The best decisions in medicine, whether large or small, are taken when considered from the patient’s perspective. Presidents and deans of radiological colleges should imagine that they are lying on a computed tomography (CT) table and are about to have percutaneous ablation of a small renal tumour. They have been asked to choose between two newly appointed staff interventional radiologists available to perform this procedure. One of them had two years of clinical experience, followed by three years of training in diagnostic radiology, which included studying subjects such as the appearance of unusual bone tumours, minutiae of mammography and details of interstitial lung disease. Then, as he was fortunate enough to train in a country where IR is recognised as a subspecialty, he studied this discipline for two years. This was far too short a period to master percutaneous ablation. This would be his first unsupervised procedure. The patient met this person only once, just before entering the CT unit, when informed consent was given. All previous clinical contact was through the patient’s oncologist, who is also going to be responsible for the patient’s care in hospital and the post-procedure follow up–an arrangement that can cause delays and confusion in dealing with recurrent or residual tumour.
The second interventional radiologist has followed a curriculum established by a fictional college. After two years’ clinical training, she entered a dedicated course in IR, learning the aspects of imaging relevant to her chosen specialty. She studied, in detail, the procedures and equipment used in IR, and learned clinical skills, assisting her trainers with ward rounds and outpatient clinics. By the time she was appointed as permanent staff, she had carried out 20 percutaneous ablations.
A primary clinical specialty of IR should have appropriate supporting staff and facilities, including dedicated CT equipment and other machines specially designed to guide procedures rather than provide images for diagnosis. Sharing CT units between diagnostic and interventional radiologists is as inefficient as running an outpatient clinic in an operating room. A more intense focus on the procedural and clinical skills required in IR would serve patients very well.
The recent haemodialysis access guideline update from the UK Kidney Association (UKKA), which was published in the run-up to the 2023 UK Kidney Week conference (UKKW; 5–7 June, Newport, UK), marks a considerable shift in how the organisation recommends that clinicians approach choices in vascular access for patients. Two of the UKKA update’s authors, Damien Ashby (Hammersmith Hospital, London, UK) and Catherine Fielding (University Hospitals of Derby and Burton NHS Foundation Trust, Derby, UK) spoke to Interventional News to detail how that shift was built on a desire to better consider the patient voice in all aspects of access care.
Asked what distinguishes this version of the UKKA guideline, Fielding began by highlighting the multidisciplinary involvement in the writing of the update. The text of the guideline states that nephrologists, surgeons and radiologists were all involved—as well as nurses like herself. Explaining the reasoning behind this, Fielding said: “It sometimes feels like it is not those who perform procedures like cannulation who are writing the guidelines on them. I am not saying that they should not have their own perspectives, but it leads you to wonder how some guideline proposals can be put into clinical practice. I think that practical, pragmatic element comes strongly through in this guideline—so that it is not just doctors but other professions that can implement it.”
Not only were a variety of specialties included, but there were also “three very active patient representatives” at the heart of the process. Developing this point, Ashby added: “The big thing that moves the needle with this guideline is how we constantly tried to involve the patient voice. The guideline emphasises different patient characteristics rather than just saying: ‘This is the best access for you.’”
Asked what might surprise some readers about the update, Ashby said that, though it would not surprise patients or nurses, it may be unexpected for some clinicians that the update does away with the concept of targets. Other guidelines, he suggested, prescribe fistulas as theoptimum form of access and provide a percentage of patients that should receive one. “It is not consistent with making the patient voice and patient choices the centre of care that hospitals should need to reach targets for types of access,” he argued. “We are moving away from that by recognising patient characteristics and what is sometimes the uncertainty of the evidence base.”
The patient voice is the fundamental difference in this guideline compared to both those issued by the UKKA in the past and those seen elsewhere, Ashby and Fielding agreed. Fielding also noted that the writing team contended with a “mushrooming” breadth of research in vascular access, which meant they were required to judge carefully what now warranted recommendation, and what still called for more research. In particular, however, they looked at qualitative data, something which they suggest may not have been included to the same degree in previous guidelines. “Once you start looking at studies of patient perspectives, it changes your own,” Ashby said.
The consideration of the patient perspective meant making the guideline more readable, too. Comparing the UKKA guideline with the Kidney Disease Outcomes Quality Initiative (KDOQI) guideline on vascular access, Ashby made the case that the references “running into the thousands” in the latter make it a comprehensive and impressive document, but one that is more of a challenge for readers. Part of the UKKA guideline team’s motivation was to provide information in a clear manner even to patients and carers, facilitating more informed decision-making.
On the content of the update itself, Ashby and Fielding concurred on a range of issues it addresses. “Timely treatment” of thrombosis, it suggests, is most effective—and it makes fistulas in particular more likely to work. Ashby highlighted that this is “an example of something where a better access outcome is also better for a patient’s experience […] which might even be a better reason to do it”.
The guideline has added a dedicated section on central venous stenosis (CVS) because, Ashby averred, “it is an important but maybe hidden problem that we wanted to highlight in the correct way”. Ashby advised, however, that the CVS recommendations are “not easy to summarise due to a complex and diverse literature”, and that the section demands more detailed reading. Ashby and Fielding concurred elsewhere also that an endovascular approach to many types of access dysfunction is “at least as good” as a surgical one. On new technologies such as drug-coated balloons, there was not sufficient existing evidence to make definitive recommendations, they said.
Queried on the potential consequences of giving patients an increased role in clinical decisions, Fielding stated that “actually putting all of the responsibility on the patient to make those decisions is very difficult”. However, she explained that the move towards shared decision-making is connected to a drive towards better informing patients, too. It is also about asking not only what is the best access from a clinician’s point of view, but taking a broader look at a patient’s life—and what kind of life they want to have after they receive their access.
“The other thing we have really highlighted through the guideline—and this is something both Damien and I are passionate about—is how important it is that the information we give patients is accurate and that we have interpreted the research accurately,” Fielding said. She further emphasised that it is vital that patients are informed of gaps in research, stating that “we should not be afraid” to tell patients when the literature is “ambiguous”. She also said that it is important to remember the “actual consequences to having a vascular access”, particularly on patients’ “day-to-day life”, referencing not only infection risk but also the “adverse effects of using it for haemodialysis”, such as cannulation pain.
Ashby concurred, saying: “It is not like giving someone a menu in a different language then asking what they want for dinner. You have got to help people to work out what those choices are and what they mean.” He drew a comparison with oncology, where he argued that cancer patients are often presented with a range of treatments, and he suggested that kidney disease patients should be offered similar “genuine choices” that reflect their needs and preferences. He referred to William Osler, who stated: “The good physician treats the disease; the great physician treats the patient who has the disease.”
Their concluding assessment of the guideline was that it “honestly summarises” the research in the field, “acknowledging uncertainties”. Most of all, they stressed its focus on the patient, while Fielding said that the full text of the guideline provides “very detailed rationales” for its suggestions. Both paid tribute to one of the patient representatives on the writing team who passed away during the writing process, which Ashby said served as a “big reminder” of the reality behind the recommendations. “For these people, it is their lives and their lifestyle. There is no way you can be doing this without remembering that this is all about a patient and their experience.”
A multicentre study presented at the recent European Stroke Organisation Conference (ESOC; 24–26 May, Munich, Germany) has found that vision recovery and an increased likelihood of early neurological improvement are among the potential benefits endovascular therapy (EVT) can offer in posterior cerebral artery (PCA) occlusion stroke. However, the same study indicated that EVT was not linked to improved odds for reduced disability, and was also associated with higher mortality and symptomatic intracranial haemorrhage (sICH) rates, as compared to medical management (MM).
Findings from PLATO—a case-control study conducted at 27 sites, and including consecutive patients with isolated PCA occlusions presenting 0–24 hours from symptom onset—were delivered for the first time by Simon Nagel (Heidelberg University Hospital, Heidelberg, Germany). Nagel and his colleagues included 1,023 patients (median age=74 years, 57.6% male) in the study, 379 (37%) of whom received EVT. The majority of PCA occlusions were either located in the P1 (41.2%) or P2 (49.2%) segments.
Regarding the trial’s co-primary endpoint, which contrasted 90-day ordinal modified Rankin scale (mRS) scores between the two groups, there was no statistically significant difference with EVT versus MM. However, Nagel did report EVT being associated with greater odds of achieving a decrease >2 points on the National Institutes of Health stroke scale (NIHSS) at 24 hours or upon discharge, as well as “complete vision recovery”, compared to MM. This was the case following adjustments for numerous comorbidities and variables, including age, sex, NIHSS score, baseline mRS, occlusion location, and whether or not intravenous thrombolysis (IVT) was administered.
The presenter further detailed a higher likelihood of an excellent functional outcome (mRS 0–1) with EVT—despite increased mortality (10.1% vs 5%) and sICH (6.2% vs 1.7%) rates versus the MM group. As such, Nagel concluded that “these results support continued enrolment into ongoing trials comparing EVT versus MM in patients with distal vessel occlusion”, referring primarily to the DISTAL, ESCAPE-MeVO and DISCOUNT studies.
A brief discussion between Nagel and session moderator Marc Ribó (Hospital Vall d’Hebron, Barcelona, Spain) culminated in an ESOC audience member suggesting that mRS is primarily focused on mobility, and may not take vision-related outcomes into account as much as it should. Nagel agreed with this view, citing it as a key motivation for vision recovery being included as a separate outcome measure in PLATO.
Findings from the PLATO study have since been published in full in the journal Stroke.
A new frontier in stroke intervention?
ESOC 2023 also saw Fouzi Bala (University of Calgary, Calgary, Canada) present late-breaking data from a sub-analysis of the AcT randomised controlled trial, which was published last year and demonstrated non-inferiority of tenecteplase versus alteplase in acute ischaemic stroke patients.
Fouzi Bala
The analysis in question focused solely on patients with medium vessel occlusion (MeVO) stroke—a population not dissimilar to the one included in the PLATO study, as well as those in the aforementioned trials assessing EVT in strokes caused by more distal occlusions. At the outset of his presentation, Bala noted that the safety and efficacy of tenecteplase in MeVO stroke is “still not well studied”. Patients with baseline M2/M3, P2/P3 and A2/A3 occlusions were included in Bala and colleagues’ AcT sub-analysis. The primary endpoint was the proportion of 90-day mRS 0–1, while secondary endpoints included 90-day mRS 0–2, mortality and sICH, as well as successful reperfusion (expanded thrombolysis in cerebral infarction [eTICI] 2b–3) on first and final angiographic acquisitions.
Bala reported that, across a total of 1,577 AcT patients, 455 (28.8%) had a MeVO stroke. The primary outcome was achieved in 37.9% in the tenecteplase group compared to 34.7% in the alteplase group. In addition, rates of 90-day mRS 0–2, sICH and mortality were all similar between the two drug types. Across 87 patients (19.1%) who underwent EVT, they found a significantly higher rate of final successful reperfusion in patients who received tenecteplase (71.7%) versus alteplase (60%). However, treatment effect modification by occlusion location was also assessed, and the researchers found no heterogeneity between groups here.
As such, Bala et al concluded that intravenous tenecteplase was observed to have shown a comparable safety profile and impact on functional outcomes versus alteplase among MeVO patients included in the AcT trial.
Surmodics announced in a press release that it has received US Food and Drug Administration (FDA) 510(k) clearance for its Pounce LP (low profile) thrombectomy system.
Introduced in 2021, the Pounce thrombectomy system is intended for the non-surgical removal of thrombi and emboli from the peripheral arterial vasculature in vessels 3.5mm to 6mm in diameter. The Pounce LP thrombectomy system, a new addition to the Pounce platform, is indicated for use in vessels ranging from 2mm to 4mm in diameter, sizes typical of vessels found below the knee.
“We are excited to secure [US] FDA clearance for the Pounce LP thrombectomy system, which will extend the range of treatment for our Pounce platform to include removal of organised thrombotic or embolic occlusions in smaller vessels below the knee,” said Gary Maharaj, president and chief executive officer of Surmodics. “Catheter-directed thrombolysis in these vessels is limited against organised clot and requires intensive care admission, while small-diameter aspiration thrombectomy devices may struggle to remove organised material in the distal lower extremity. By expanding the treatment range of the Pounce platform we are addressing tibial clots, an important component of treatment in this vulnerable patient population which fills a gap in care.”
Maharaj added, “[US] FDA clearance of the Pounce LP thrombectomy system brings us one step closer to providing the complete mechanical thrombectomy solution for all peripheral arteries and demonstrates our commitment to leadership in this critical-needs space.”
Terumo Aortic announced in a press release the launch of the company’s global post-approval study (PAS) known as EXTEND for Thoraflex Hybrid, the only frozen elephant trunk (FET) device approved by the US Food and Drug Administration (FDA) for the treatment of patients with complex aortic arch disease.
This study is a prospective, multicentre, non-randomised, single arm, all-comer, postmarket study of Thoraflex Hybrid and RelayPro non-bare stent (NBS).
The aim of the EXTEND study is twofold, the company states: to evaluate the Thoraflex Hybrid device on its own in a “real-world” environment, and in combination with the RelayPro NBS graft for the treatment of aortic disease affecting the aortic arch and descending aorta with or without involvement of the ascending aorta.
This global study will include up to 55 centres at leading healthcare institutions in Europe and North America. A minimum of 200 patients will be enrolled with a follow-up period of 10 years; a minimum of 65 patients will have a RelayPro NBS distal extension implanted in addition to Thoraflex Hybrid.
Christian Shults, cardiac surgeon at MedStar Washington Hospital Center (Washington DC, USA) enrolled the first subject.
European principal investigator Martin Czerny, consultant cardiovascular surgeon, University Hospital Freiburg, (Freiburg, Germany), commented: “The EXTEND study is an exciting opportunity to gather long-term follow-up data on grafts used to treat a wide range of aortic pathologies while demonstrating the continued safety and performance of the Thoraflex Hybrid device alone and in combination with the RelayPro NBS device.”
North American principal investigator Joseph Bavaria, vice chief, Division of Cardiovascular Surgery, University of Pennsylvania (Philadelphia, USA), added: “We look forward to contributing to this unique global study and collecting long-term data on Thoraflex Hybrid and RelayPro in highly complex aortic interventions. To date, the majority of studies on hybrid grafts are limited to short-term follow-up and this study will be a significant step towards understanding long-term outcomes and the benefits for patients.”
Jeffrey Mifek, global vice president, Clinical and Medical Affairs at Terumo Aortic said: “We are in the fortunate position to study this combination as Thoraflex Hybrid is the only [US] FDA-approved hybrid graft in the USA for frozen elephant trunk procedures and RelayPro NBS is the only endovascular graft [US] FDA-approved to extend Thoraflex Hybrid. It is anticipated that the data collated in the coming years will provide the global surgical community with insights on extension devices helping to revolutionise future treatment options for patients. Terumo Aortic is committed to building clinical evidence that supports the entire aortic solutions portfolio.”
Interventional radiologist Nick Brown is clinical director of the radiology service at The Wesley Hospital (Auchenflower, New Zealand) and associate professor at the University of Queensland (Brisbane, Australia). He sat down with Interventional News at the European Conference on Interventional Oncology (ECIO; 16–19 April, Stockholm, Sweden)to discuss the current picture of interventional radiology (IR) and interventional oncology (IO) in Australasia—the progress that has been made recently, and how far they still need to go to achieve specialty status, alongside a programme of IR training, education and ultimately, a qualification unique to the region.
“We are certainly very proud to be the first site in Australia and New Zealand to be accredited,” Brown begins, referring to the International Accreditation System for Interventional Oncology Services (IASIOS) certification that I-MED at The Wesley Hospital gained back in September 2021. “There are two other enrolled sites, and possibly some more about to be,” he continues, highlighting how the programme is gaining traction among hospitals in his region as centres seek to be able to demonstrate to referring clinicians that their IO service is high performing. Showing this to patients as well is key, as understanding of IR and IO among the public is often minimal, he explains. “It is always better to have a team working together to promote [IO].”
IASIOS certification improves IO recognition
In Australia and New Zealand, as elsewhere in the world, Brown clarifies, “there are challenges—getting recognition for IO and getting a seat at the MDT [multidisciplinary team] table, having the value of what we do recognised by the hospitals in which we work, by the referring physicians, and by the patients themselves”. Therefore, Brown defines “true success” with IO standards as having a “network of IASIOS sites across Australia and New Zealand and throughout Asia”. This is advantageous, he elaborates, because the centres will be able to “support each other and learn from each other”, rather than having the nearest reference points and collaborators in Europe “on the other side of the world” and in different time zones. Brown adds that the Royal Australian and New Zealand College of Radiologists (RANZCR) does already have a relationship with Singapore “and hospitals in Singapore have been accredited”. The next step towards “a great foundation on which to build”, he stipulates, would be for a hospital in New Zealand to become accredited—“Auckland Hospital may be on the cards”.
Next, Brown turns to address the impact accreditation has had on the service his centre provides, nearly two years on. “We have the IASIOS symbol at the bottom of all our reports, letters, and emails,” he relays, notwithstanding having it prominently displayed in clinic. This prompts some patients to ask about the value of the certification, which Brown sees as a positive thing. However, he says the “real value” lies in how it has informed referrers. “We can say that we are a clinic that has most of our interventional radiologists EBIR [European Board of Interventional Radiology]-certified and we are now accredited with IASIOS—we can explain what this means and why it matters,” Brown details. This has led to an increase in referrals for several key IR procedures, he says.
Striving for better as both a hospital and discipline
“It was a lot of work to get to this standard—we needed dedicated staff and time set aside,” Brown wishes to underline, but nonetheless, he believes his centre has ‘IASIOS Centre of Excellence’ status “within [its] reach”. He then emphasises how important it is that they, at his hospital, “do what we do knowing that it is the best we can do and meets the highest expectations”. Quality assurance in IR and IO has been, and can be, more difficult to achieve than for other specialties like radiation oncology, with quality control “inbuilt”. Wanting to “do better” is what Brown thinks IR, as a whole, should keep at the heart of its practice, in order to bring about better outcomes.
Accreditation, such as IASIOS, is one aspect of the solution to the lack of public recognition of IR, Brown says, moving on to examine the bigger picture—there is a problem everywhere in that people are not familiar with IR. He laments the fact that there are “limitations to what individual interventional radiologists can do” to resolve this issue, so there needs to be a set of strategies at a college, society and government level in all countries for realising better IR recognition through avenues such as policy.
A region-specific training programme is key
Training is another aspect Brown mentions, citing RANZCR’s new training programme currently in development for interventional radiologists and interventional neuroradiologists, as well as a new qualification which will be recognised in Australia and New Zealand. This is superior to relying on certification such as from EBIR and IASIOS, as it is purpose-built, with the locoregional health system and accreditation processes in mind. In addition, Brown stipulates the need to train more interventional radiologists in order to achieve a workforce of adequate size and quality, as part of the solution to under-recognition of IR is “a numbers game”.
Brown then makes a point about the onus that rests on the shoulders of individual clinicians, who can sometimes “take the easy road”. He urges doctors to “not be limited in their thinking by the constraints of the status quo”, and to not simply “do things the way they have always been done”. An example of active change for the better, he adds, would be for consultants to make an effort to do ward rounds themselves, even if this strays from the status quo. “We all need to be the change that we want to see in the world”—this will help enormously in the effort to increase IR awareness through delivering services of the highest possible standard.
Why specialty status matters
Another “really important part” of resolving the lack of recognition, Brown then notes, is achieving specialty status for IR—and this is true of many countries where this is not already the case. Not having IR recognised as a full specialty accompanies the further problem of not having an official IR training programme and qualification. “EBIR is very good in that respect […] as a platform to launch from,” Brown admits, but “long-term structural change” spearheaded by colleges and societies working together is the only way to ensure uniformity of recognition and a high standard of IR training, he avers. It has taken time for RANZCR, the Interventional Radiology Society of Australasia, and the Australian and New Zealand Society of Neuroradiology to collaborate on advancing the cause of IR and INR and to “support a plan specific to [the region]”, learning from some of the European and North American experiences where specialty status has either already been obtained, or is in progress.
Concluding, Brown first sums up the impact of achieving IR specialty status on him—he is looking forward to “no longer being just a diagnostic radiologist, but a dual-trained specialist interventional radiologist as well, with hospital managers and colleagues knowing exactly what that means”. At a national and regional level, Brown then summarises that “we have to stand on our own two feet in our jurisdiction […] as the international standards are not sufficient to create that change for us” in Australia and New Zealand, as regards specialty status, training programmes and qualifications.
Presenting first-time data from large multicentre European studies at this year’s Leipzig Interventional Course (LINC 2023; 6–9 June, Leipzig, Germany), Arne Schwindt (St Franziskus Hospital Münster, Münster, Germany) and Ralf Langhoff (Sankt Gertrauden Hospital, Berlin, Germany) delivered results that “confirm” the safety and efficacy of the Roadsaver (Terumo) dual-layer micromesh carotid stent (DLMS).
First to the podium, Schwindt identified 30-day outcomes in male versus female patients treated using the Roadsaver device. He defined that the majority of patients were treated using a femoral approach, adding that radial access was more common in the female group. The researchers found no difference in the use of embolic protection in their cohort, however Schwindt noted that in the cases where protection was employed, female patients more frequently received distal protection.
Their primary endpoint concerned any major adverse event (MAE) between the female and male groups. Additionally, Schwindt explained that of their 2,000-patient cohort, participants were evenly split between symptomatic and asymptomatic.
Schwindt and his team found that the MAE rate in their patient population was 2.2%— recorded as 2.0% for males and 2.6% for females—which he reported to the LINC 2023 audience—was not statistically significant. Schwindt did pinpoint a trend toward higher stroke risk in their study’s female group, however this was also not statistically significant. Among the entire cohort, stroke risk was seen in 1.9%—which expanded to 1.6% in male and 2.6% in female patients.
“We saw that the majority of these events still take place within 48 hours to three days after the procedure,” Schwindt noted, “but we see these curves flatten out and nothing much happens towards the end of the 30-day period.” Concluding his presentation, Schwindt emphasised the “very low” MAE rate in both male and female patients and “[similarly]” low 30-day rates of minor or major stroke, despite a “small trend” toward lower incidence in males. Schwindt stated: “Given that both groups undercut the stroke rates defined by the S2 guidelines from Germany, the currently most strict guidelines concerning clinical outcome, CAS with dual layer micromesh stent can be concerned as a valid treatment option for males and females alike.”
Ralf Langhoff speaks at LINC 2023
Following Schwindt, Langhoff subsequently presented first-time data on the 30-day safety results in patients treated using the Roadsaver device—their investigation assessed the influence of predilatation on outcomes. “A major difference,” Langhoff posited, became apparent when observing transient ischaemic attack (TIA), which in patients who had received predilatation, was seen to be “significantly” more prevalent. His team identified a 1.6% to 2.0% split, which emphasised the effect of predilatation that Langhoff himself “did not expect”.
Summarising their findings, Langhoff stated that there was low overall need for predilatation in real-world elective carotid artery stenting (CAS) patients treated with the Roadsaver DLMS. Equally, he noted that there were low and comparable 30-day MAE rates between the groups with and without predilatation, “[confirming]” the safety of the Roadsaver device when performing CAS.
Delivering first-release data, Scott O Trerotola (University of Pennsylvania, Philadelphia, USA) conveyed the “consistent results” in a real-world environment for the Lutonix arteriovenous (AV) post-approval study (PAS) for drug-coated balloon (DCB)-AV on the afternoon of the second day at this year’s Leipzig Interventional Course (LINC 2023; 6–9 June, Leipzig, Germany).
The study objective was to demonstrate safety and assess the clinical use of the Lutonix DCB for treatment of dysfunctional AV fistulae located in the arm as part of a post approval study mandated by the US Food and Drug Administration (FDA). In order to be enrolled, Trerotola defined that there needed to be successful predilation—meaning no significant dissection or extravasation, residual stenosis less than 30%, and complete effacement of the waist on the initial pretreatment angioplasty high-pressure balloon, after which point the DCB is used.
Trerotola highlighted that they intend on enrolling 213 patients but are, at present, halfway enrolled, noting his presentation currently regards the 81 patients for which the interim analysis was performed. Expanding on the demographics of their patient population, the speaker additionally noted that 64.2% of patients are male and enrolled participants currently have a mean age 64.6.
Presenting their data to the LINC 2023 audience, Trerotola emphasised that “importantly—not to anyone’s surprise at this point—the safety and lack of events is 100%, so the device is safe and this is something that has come out of all of the trials.” He noted specifically to the six month target lesion primary patency (TTLP) for the Lutonix device was 77.6%, this endpoint defined as the time to clinically driven reintervention or thrombosis.
Comparing their results to the Lutonix global registry trial and the IN.PACT investigational device exemption (IDE) trial, which received 73.9% and 82.2% six month primary patency for the Lutonix DCB and IN.PACT DCB respectively, Trerotola highlighted the “extremely reassuring and heartening” outcome they have achieved, delivering “as good or better” results in their post-approval study.
Comparing these data to those from other studies, Trerotola stated that there are prevalent “demographic differences” between the Lutonix IDE and PAS studies when compared to the IN.PACT IDE trial and Lutonix Global registry, as the Lutonix studies enrolled only North American patients resulting in far fewer forearm fistulae. Furthermore, dosage differs between the devices which Trerotola noted to the audience.
Finally concerning the execution of DCB research, Trerotola made clear mention of the requirement to “do everything right to get the best results”. “We learned the lesson the hard way in our post-approval study when we initially told investigators they needed to inflate for 30 seconds. We later had to increase this to two minutes due to emerging data, and in the IN.PACT study they were all over three minutes—those variables are important.”
In summary of their first-release study data, Trerotola stated that the Lutonix is the first US Food and Drug Administration (FDA) post-approval study in the AV setting, and that it “very reassuringly shows us very good results at six months and a good safety record.
“We will now eventually add an additional 213 subjects to an emerging level of evidence of over 800 subjects studied prospectively to date with the Lutonix device, and I think it is very important when moving forward to pay attention to the heterogeneity in the DCB studies and to try and figure out how to personalise DCB used in the future.” Trerotola concluded his presentation by reiterating that, most importantly, “if we are going to use these devices, we have to use them correctly and we have to get the vessel ready correctly before we do so”.
Marianne Brodmann presents first-release data at LINC 2023
The ‘Connect the world: Japan’ session at this year’s Leipzig Interventional Course (LINC 2023, 6–9 June, Leipzig, Germany)—in collaboration with the Japanese Endovascular Treatment Conference (JET)—sparked discussion surrounding the latest data in femoropopliteal interventions. Giving platform to multiple first-time data releases, the LINC 2023 audience were presented with awaited updates from global trials.
Stepping up to the podium first, Marianne Brodmann (Medizinische Universität Graz, Graz, Austria) presented the initial Ranger superficial femoral artery (SFA) II randomised controlled trial (RCT) three-year patency and four-year clinical safety results. This study compared the Ranger drug-coated balloon (DCB; Boston Scientific) plain balloon angioplasty.
The study aimed to evaluate the safety and effectiveness of the Ranger DCB (paclitaxel dose density 2μg/mm2) for treating SFA or proximal popliteal artery lesions—Brodmann explaining briefly that paclitaxel-coated balloon treatment prevents reinterventions however dosage and coating characteristics can differ, affecting efficacy determination.
Regarding their cohort demographics and clinical history, Brodmann noted there was no major differences between study arms, however around 40% of patients were identified as having diabetes. Lesion characteristics were also similar between groups—mean lesion length Brodmann addressed as being not statistically significant, although a higher degree of calcium was found in the plain balloon arm. Additionally, she added that there was a higher percentage of total occlusion in the plain balloon arm.
Summarising their long-term outcomes for the LINC 2023 audience, Brodmann highlighted the three-year primary patency of DCBs at 177.4% over plain balloon angioplasty at 73.5%—“in comparison to other DCB trials out there, our three-year primary patency is much higher” she concluded. Turning to outcomes concerning major amputation and four-year mortality rates, they found no significant difference in all-cause mortality and amputation in both arms. However, when regarding four-year efficacy data, Brodmann stated that the DCB provided higher freedom from clinically driven target lesion revascularisation (CD-TLR) at 78.7% compared with 74.5% for the plain balloon arm.
Concluding her presentation, Brodmann observed that their study “demonstrated outstanding three-year primary patency of 77% for the low-dose paclitaxel DCB and four-year freedom from CD-TLR which is greater than those reported in other DCB studies previously published”.
Brodmann later returned to the podium to deliver another first-data release from the ELEGANCE registry, the purpose of which was to collect real-world data from underrepresented minorities (URMs) and women who have “previously not been represented” in peripheral arterial disease (PAD) trials. The aim of this registry, Brodmann summarised, is—as the trial is ongoing—to examine variation in treatment among sociodemographic groups for those treated with DCBs.
The registry has recruited 566 subjects across 31 sites, in three countries/regions to date which have been treated with the Ranger DCB. Expanding on patient demographics, Brodmann stated that theirs is a complex subject cohort due to the “higher prevalence” of chronic limb threatening ischaemia (CLTI) in Black and Hispanic patients, longer lesion length in Black subjects, while 61.1% of patients were identified with moderate/severe calcification.
Of their conclusions to date, Brodmann conveyed the higher burden of atherosclerotic risk factors faced by women and URMs, and that baseline clinical characteristic differences between sex and race/ethnicity groups suggest variability in time to diagnosis, treatment planning and access to care.
Koen Deloose
Next, reporting on the four-year results from the TINTIN trial investigating the combination of the Luminor DCB with the iVolution bare metal stent (both iVascular). Koen Deloose (AZ Sint-Blasius, Dendermonde, Belgium) gave a brief description of the study, which was performed in nine centres and enrolled patients who had TASC C or D lesions that were more than 150mm in length. Similar to Brodmann et al’s research, Deloose and his team defined their primary endpoint to be freedom from CD-TLR at one year, with a follow-up period of up to five years.
Presenting the 48-month results of the TINTIN trial, Deloose outlined that in the 100 patients in their cohort 72% were claudication patients and 28% chronic limb-threatening ischaemia (CLTI) patients. The mean lesion length in this group was 24cm. Additionally, they identified occlusions in 60% of patients and 70% had severe calcification. At 48 months, Deloose noted that they have had 36 deaths and some withdrawals/missed visits, so their current data is drawn from the 52 remaining patients.
“In terms of survival, you notice how diseased this vascular population is with lesions up to 24cm—in the CLTI patient group we saw a survival rate of 61% at four years, which I think is completely in line with findings in the literature,” Deloose opined. The reasoning for this outcome, he continued, is due to a “heterogeneous group of causes, which are not related to procedure, nor device”.
Freedom from major adverse events (MAEs), CD-TLR or major amputation was found to be 44.6% at four years, while they have identified 19 CD-TLRs and a single case of major limb amputation in the CLTI group. Deloose stated that they reached their 30-day primary safety endpoint without any occurrence of an event.
Moving on to consider freedom from CD-TLR more closely when using this combination therapy, Deloose posited that, at four years, they saw “quite good results” showing freedom from CD-TLR to be at 75% in the remaining population—”this means three out of four did not have reintervention if they were still alive at four years”.
Comparing their results with similar studies, Deloose confirmed that theirs data are in the “same area”, and that the TINTIN trial shows the “durability of a combination of an efficient DCB and scaffolding in the most complex lesions”.
Wouter Lansink
Subsequently presenting another first-time data release, (Ziekenhuis Oost-Limburg, Genk, Belgium) delivered results from the REGAL registry—a real-world, all-comer study comparing the Eluvia DCB (Boston Scientific) and bare metal stents. The study concerned patients aged 80 or older, with Lansink emphasising that this means they have received “all kinds of treatments”. Furthermore, he made a clear note that “these are very ill patients”, with lesion lengths of up to 10cm and a 50% chronic total occlusion rate.
“The Kaplan Meier primary patency projection through to 12 months was 92%” Lansink observed, “which is of course very good looking ahead to 24 months.” He also emphasised the durability of primary sustained clinical improvement at 24 months, which is a “good sign for these kind of stents”. Additionally, major amputation rates remained low in the patient population and was recorded as 2.2% at 24 months.
Summarising their findings for the LINC 2023 audience, Lansink restated that this is real-world data pulled from patients with complex lesions, high rates of chronic total occlusion and high rates of diabetes. Despite the high-risk nature of their population, at 12 and 24 months the Kaplan Meier primary patency rates were 92% and 83%, respectively, Lansink confirmed. Freedom from CD-TLR was recorded as 93% and 88%, while sustainable clinical improvement was seen in 83% and 81% of patients at 12 and 24 months.
“Collectively, the data demonstrates the safety and efficacy of the Eluvia stent in SFA, proximal popliteal lesions and even in a population with advanced peripheral arterial disease and a higher occurrence of comorbidities,” Lansink conveyed.
Percutaneous transmural arterial bypass using the Detour System (Graphic: Business Wire)
Endologix has announced in a press release that the US Food and Drug Administration (FDA) has granted approval for the Detour System to treat patients with complex peripheral arterial disease (PAD).
Patients with long blockages of the superficial femoral artery (SFA) have had limited treatment options. The recommended therapy is open surgical bypass, which is invasive, has a high early complication rate, and requires prolonged recovery. Endovascular treatments are feasible in selected patients but have limited patency.
Percutaneous transmural arterial bypass (PTAB) with the Detour System offers a novel approach to treating complex PAD, enabling physicians to bypass lesions in the SFA by using stents routed through the femoral vein to restore blood flow to the leg. This approach is particularly effective for patients with long lesions (20–46cm in length), those that have already undergone failed endovascular procedures, or those that may be suboptimal candidates for open surgical bypass.
“We are delighted to receive [US] FDA approval of the DETOUR System,” said Matt Thompson, president, and CEO of Endologix. “PTAB therapy represents a significant step forward for patients with complex PAD. They have long needed a more effective and less invasive treatment option for long lesions of the SFA. We are proud to be pioneering this novel approach and continuing to innovate on behalf of patients. We look forward to launching this new therapy in the US through a targeted market release in the coming weeks.”
In a second compassionate use case, interventional vascular surgeon Stefan Stalhoff of Klinikum Hochsauerland (Arnsberg, Germany) used VeinWay‘s Traversa for venous recanalisation to save a patient’s arm, with supervision by VeinWay scientific advisory board member Michael Lichtenberg. The patient had been in so much pain, that she could not hold her young children.
This news follows the first-in-human compassionate use case announced in March, where interventional radiologists David M Williams and Minhaj S Khaja (both University of Michigan Health used VeinWay’s Traversa for venous recanalisation to save a patient’s leg that was close to being amputated.
Details of both compassionate use cases were presented today at the Leipzig Interventional Course (LINC; 6–9 June, Leipzig Germany) by Michael Lichtenberg (Klinikum Hochsauerland, Arnsberg, Germany).
VeinWay CEO Jordan Pollack said, “VeinWay’s Traversa helped the doctors in Germany to successfully cross a previously uncrossable blockage in the patient’s vein and restore blood flow. The patient experienced immediate relief of symptoms. I only wish we could have captured the joy on her face, as she can hold her children again pain-free.”
Stalhoff said, “By using the Traversa we saved hours of procedure time and were able to achieve a goal previously unreachable, with comparable ease. This makes two successful clinical outcomes using the Traversa thus far.”
Another milestone achieved – Bentley sold its 300,000th BeGraft
Another milestone achieved – Bentley sold its 300,000th BeGraft
Bentley announced at the annual Leipzig Interventional Course (LINC; 6–9 June, Leipzig Germany) that it has reached an important milestone: having sold the 300,000th BeGraft. This milestone was celebrated at the Bentley booth at LINC.
After launching the first BeGraft in 2012, the product found its way quickly to the clinics carrying out the most advanced and challenging endovascular procedures. The BeGraft is available in over 80 countries and has become the market leader in most of them.
Martijn Nugteren, director sales and marketing at Bentley, is delighted with this six-figure number and mentioned in a statement: “It is amazing what we have achieved with the BeGraft in such a short time. We have been able to treat so many patients globally, giving them the best stent for the treatment of their vascular disease.” He also highlighted that “thanks to the acquisition of Qmedics in mid-April, Bentley is ready for the future growth of the BeGraft covered stent portfolio, which is much needed with the expected new indication and state-of-the art pipeline that we have.”
The 300,000th BeGraft was sold to the company NovaHealth in Thailand, which has been a partner of Bentley since 2015.
Inari Medical today announced the launch of two new purpose-built products, the RevCore thrombectomy catheter, and the Triever16 Curve catheter.
According to a company press release, RevCore is the first mechanical thrombectomy device designed to address venous in-stent thrombosis, an increasingly common occurrence impacting more patients every year. The device includes a diameter-controlled coring element designed to engage thrombus within stents.
With RevCore, Inari has developed a solution for an entirely new patient population not currently addressed by the ClotTriever or FlowTriever platforms, the press release reports. Inari will be co-hosting a webinar with the Venous Symposium today, Wednesday 7 June at 7pm ET (4pm PT) to introduce RevCore and review the initial case experience. Register here.
“Until now, physicians have had limited options to treat patients suffering from symptoms of venous stent failure and some patients are relegated to repeated suboptimal interventions,” said Steven Abramowitz (MedStar Health, Washington, DC, USA). “RevCore is a game changer as it physically removes in-stent thrombus, restores flow, and could potentially reduce the need for additional reintervention. There are a lot of patients out there that may benefit from the RevCore procedure.”
The Triever16 Curve catheter, the latest addition to the FlowTriever platform, is purpose-built to be versatile for both pulmonary embolism and peripheral thrombectomy. The trackable catheter features a pre-shaped curve for targeted aspiration. Inari claims that Triever16 Curve offers unique advantages over 16Fr continuous aspiration catheters, including compatibility with the FlowSaver blood return system and simple access to larger, more powerful 20Fr or 24Fr catheters within the company’s price-per-procedure model.
“Triever16 Curve is an important addition to the already comprehensive Inari venous thromboembolism [VTE] toolkit,” said Angelo Marino (Yale School of Medicine, New Haven, USA). “Every VTE patient is different. With both aspiration and mechanical bloodless thrombectomy options available, including multiple sizes and shapes of large-bore aspiration catheters, we are equipped to treat nearly every VTE patient that comes in the door.”
New draft guidance for clinical trials has been issued by the FDA
The US Food and Drug Administration (FDA) has released draft guidance with updated recommendations for good clinical practices (GCPs) aimed at modernising the design and conduct of clinical trials.
In a statement, the regulator said that the updates are intended to help pave the way for more efficient clinical trials to facilitate the development of medical products, with an aim to be “more agile without compromising data integrity or participant protections”.
The draft guidance is adopted from the International Council for Harmonisation’s (ICH) recently updated E6(R3) draft guideline that was developed to enable the incorporation of rapidly developing technological and methodological innovations into the clinical trial enterprise.
“A more robust clinical trial ecosystem that is capable of producing reliable evidence more efficiently may support more informed decision-making in developing medical products to help patients,” said FDA commissioner Robert M Califf. “These draft recommendations propose a major step forward in this work. Building quality into the design and conduct of trials and encouraging the use of innovative trial designs and health technologies are essential to truly advance clinical trials and generate meaningful results.”
GCPs ensure the safety of trial participants, as well as the integrity of the data generated from trials. Over the years, the clinical trial enterprise has been viewed as costly, inefficient and constrained by inadequate collaboration and insufficient utilization of technology, data sources and innovations in design and conduct. The COVID-19 pandemic highlighted many of these challenges, while also spurring the development of new approaches, FDA’s statement adds.
“These draft recommendations were developed with the aim to streamline trials, making them more efficient and flexible as the trial enterprise continues to evolve,” said M Khair ElZarrad, director of the FDA’s Center for Drug Evaluation and Research’s Office of Medical Policy. “We hope these recommendations, once finalised, will encourage thoughtful approaches to conducting clinical trials with a focus on participant safety and data integrity.”
ElZarrad led the ICH Expert Working Group in developing the ICH E6(R3) draft guideline. Academic clinical trial experts from various ICH member countries also played an important role in informing the work of the expert group.
This draft guidance, once finalised, would update the existing guidance titled, E6(R2) Good Clinical Practice: Integrated Addendum to ICH E6(R1). The revised draft recommendations are designed to be applicable to a broad range of clinical trials including those with innovative design elements.
The draft guidance will be open for public comment for 60 days. The ICH Expert Working Group will review and consider comments on this draft guidance, as well as feedback from other ICH member countries before finalising the ICH guideline.
Teleflex has announced in a press release that the Arrow EZ-IO Needle is the first and only intraosseous (IO) needle to receive 510(k) clearance from the US Food and Drug Administration (FDA) for magnetic resonance (MR) conditional labelling. The EZ-IO Needle, a critical component of the Arrow EZ-IO intraosseous vascular access system, has a patented diamond tip designed for fast, precise and steady insertion.
The EZ-IO System can be used when intravenous access is difficult or impossible to obtain in emergent, urgent, or medically necessary cases. The new labelling allows the clinician to care continuously for patients who require magnetic resonance imaging (MRI) scans without interruption to the established site for vascular access.
“Clinical and Medical Affairs is committed to supporting the expanded use of Teleflex medical devices in a continuous effort to improve patient care,” said Michelle Fox, corporate vice president and chief medical officer, Teleflex. “Patients who require emergent or urgent MRI now have an additional vascular access option.”
“Teleflex continues to innovate on behalf of clinicians who are seeking to provide continuous care during critical situations,” said Kevin Robinson, president and general manager, Anaesthesia and Emergency Medicine, Teleflex. “We are excited to have the Arrow EZ-IO Needle cleared as MR conditional and look forward to finding new ways to deliver outstanding care solutions for patients and providers.”
Argon Medical Devices, Inc. Logo. (PRNewsFoto/Argon Medical Devices, Inc.)
Argon Medical has announced the launch of the SuperCore Advantage semi-automatic biopsy instrument as the newest addition to its soft tissue biopsy product portfolio in the USA.
The SuperCore Advantage is a disposable soft tissue biopsy instrument that provides a superior volume of tissue samples. Collecting more tissue volume may increase the likelihood of an accurate diagnosis, allowing healthcare professionals to feel confident sending tissue samples to pathology for analysis. The new design is available in a full range of lengths and gauge sizes so that physicians can select the best fit device for the clinical application.
“Precise and reliable biopsies are critical in the quest for better patient outcomes,” said Paul Guzzetta, interventional radiologist, Advocate Christ Medical Center (Oak Lawn, USA). “By delivering greater tissue volume, the new SuperCore Advantage provides the pathologist with the tissue needed to perform necessary diagnostic tests and determine potentially life-altering diagnoses or treatment options for patients.”
“Argon is proud of the innovation we are bringing to soft tissue biopsies. The SuperCore Advantage was designed with input from healthcare professionals to help address the clinical needs and wants of those who perform biopsies on patients at a critical crossroad in their lives,” said George Leondis, president and CEO, Argon Medical. “We are very pleased to bring this long-awaited product to market.”
“We take pride in offering a full portfolio of best-in-class soft tissue biopsy solutions for our clinician customers. Adding the SuperCore Advantage to this portfolio among other segment leaders like the BioPince Ultra full core biopsy instrument, will fortify our reputation as a leading provider of soft tissue biopsy devices,” said Tom Younker, senior vice president of global marketing, Argon Medical.
Profound Medical has announced in a press release that, with sponsorship and support from multiple physician specialty societies, the American Medical Association (AMA) has established three new Current Procedural Terminology (CPT) category 1 codes for magnetic resonance imaging (MRI)-monitored transurethral ultrasound ablation (TULSA) of prostate tissue, performed using Profound’s TULSA-PRO system.
The first CPT Code describes the complete TULSA procedure when furnished by a single physician, such as a urologist. The other two CPT codes each describe a part of the TULSA procedure when TULSA is furnished by two physicians, such as a urologist in collaboration with a radiologist.
“We are honoured that the TULSA application was approved by the AMA’s CPT editorial panel for Category 1 code status,” said Profound’s CEO and chairman, Arun Menawat. “The establishment of these permanent codes specific to TULSA is a critical milestone for the broader adoption of the technology to treat prostate diseases in the USA. The application was independently sponsored and submitted without the direct involvement of Profound, which is a testament to the level of physician support for this new procedure. We would like to take this opportunity to thank the societies for their support, as well as the independent TULSA-PRO users who provided their invaluable feedback. Looking forward, as we continue to work toward realising TULSA’s full potential for a broad spectrum of patients with prostate disease, we believe having multiple distinct CPT Category 1 codes for TULSA will give our physician users the flexibility to either do the entire procedure on their own, or collaborate and be reimbursed for their part of the service.”
The three new CPT Category 1 codes and their descriptors covering the TULSA procedure will be included in a future edition of the CPT Codebook and will be effective on January 1, 2025.
Shape Memory Medical has announced the publication of results from the company’s prospective, open-label, single-arm, safety study of the IMPEDE embolization plug in peripheral vascular embolization. The study was published this month in the peer-reviewed journal, Vascular, ahead of print.
Ted Ruppel, CEO of Shape Memory Medical said, “We would like to congratulate the investigators and clinical research team at Auckland City Hospital [Auckland, New Zealand] for completing the study and retrospective review of follow-up imaging. The publication is a significant milestone for the company as we continue to evaluate the potential of shape memory polymer and specifically the IMPEDE embolization plug family in a variety of arterial and venous applications.”
Both the IMPEDE and IMPEDE-FX embolization plugs incorporate shape memory polymer (‘smart’ polymer), a porous, radiolucent, embolic scaffold that is crimped for catheter delivery and self-expands upon contact with blood for acute thrombosis and occlusion. The material is highly conformable and able to accommodate irregular surfaces with low chronic outward force. Shape memory polymer has also been shown in preclinical studies to be fully bioresorbable, over time, with collagen formation and fibrosis and without chronic inflammation.
The safety study was registered with the Australian New Zealand Clinical Trials Registry (ANZCTR): 12617000906358. Procedures were performed from August 2017 to December 2019. Embolized peripheral vascular vessels include inferior mesenteric arteries, testicular veins to treat varicoceles, internal iliac, renal accessory, and left subclavian arteries to treat or prevent endoleaks, and a profunda branch prior to tumour resection and hemiarthroplasty. Acute technical success of target vessel embolization was achieved in all implantation cases, and no serious adverse events related to the study device occurred. No recurrent clinical symptoms attributable to treated vessel embolization or recanalisation were documented through 30-day follow-up.
A retrospective review of follow-up imaging through a mean of 22.2 months (range, <1–44 months) was performed post-procedure. “We have been impressed with the performance and durability of the IMPEDE devices which did not show any evidence of recanalisation through long-term imaging follow-up,” said Andrew Holden, principal investigator and director of interventional radiology at Auckland City Hospital. “The tissue ingrowth into the device is intriguing, and the clinical advantages of this property may emerge in further studies,” stated Holden. “We look forward to seeing how shape memory polymer in clinical practice continues to evolve.”
‘Shape memory polymer technology in peripheral vascular embolization’ was first published online in Vascular on May 22, 2023 and is available via open access.
Biotronik today announced the limited release of its Oscar (One Solution: Cross. Adjust. Restore) multifunctional peripheral catheter and start of promotional activities at this year’s Leipzig Interventional Course (LINC 2023; 6–9 June, Leipzig, Germany).
As indicated per Instructions for Use, the Oscar catheter is intended for dilation of stenotic segments in peripheral vessels. The device is comprised of three fully user-adjustable components (support catheter with integrated Lock Grip, extendable dilator and length-adjustable percutaneous transluminal angioplasty [PTA] balloon). It was developed to provide support during access into and to dilate stenoses in femoral, popliteal and infrapopliteal arteries.
The multifunctional system will be featured in the first symposium focused on the Oscar catheter at LINC 2023, with presentations from Koen Deloose (AZ Sint-Blasius, Dendermonde, Belgium), Peter A Schneider (University of California San Francisco, San Francisco, USA), Ralf Langhoff (Sankt Gertrauden-Krankenhaus, Berlin, Germany) and Mariano Palena (Maria Cecilia Hospital, Cotignola, Italy) on Wednesday 7 June at 12:30pm in Main Arena 1 during the session “Versatility without compromise: The peripheral arterial disease [PAD] workflow of the future with a new all-in-one solution”.
The first commercial procedure with an Oscar catheter in the USA was performed by Schneider. “With the Oscar catheter, I have a platform, support, pushability and crossability that I don’t have by cobbling together multiple other catheters and wires,” he commented.
Christoph A Binkert (Kantonsspital Winterthur, Winterthur, Switzerland) performed the first commercial procedure using an Oscar device in Europe. He remarked: “The Oscar catheter undoubtedly reduced several procedural steps and device exchanges. The ability to dilate the full lesion length followed by focal areas of residual stenosis with the same balloon was a great benefit to my procedural flow.”
The device began its initial commercial roll out in both the USA and Europe in late April.
“We are eager to get the Oscar catheter into the hands of peripheral interventionalists around the world and help to potentially change the way they approach difficult cases both above and below the knee,” said Joerg Pochert, President Vascular Intervention at Biotronik.
The Oscar multifunctional peripheral catheter will continue commercial expansion in the USA and CE mark-accepting regions over the coming months, a company press release advises.
Interventional News’ most popular stories from May included a forecast of where embolization is headed from a Global Embolization Oncology Symposium (GEST, 18–21 May, New York City, USA) presenter, the announcement of Bentley’s first US product launch and Quantum Surgical’s first US patient treated with the Epione robot, and new data on a range of procedures, from (endo)grafts for abdominal aortic aneurysm (AAA) and haemodialysis, to prostatic urethral lift (PUL) for benign prostatic hyperplasia (BPH).
Varian, a Siemens Healthineers company, is introducing the Isolis cryoprobe, a single-use, disposable device designed for use with CryoCare systems that seeks to improve procedural efficiency and precision for cryoablation. The new Isolis cryoprobe offers the interventional radiologist greater operational control.
Speaking at GEST 2023, Lindsay Machan (University of British Columbia, Vancouver, Canada) gave a comprehensive outlook on the next five years in embolization, outlining procedures that will be characteristic, and the advancements that are needed to propel practice into the future.
Bentley has announced the US launch of its BeBack crossing catheter, which is designed for the treatment of heavily calcified lesions. This is the company’s first product to be launched in the USA.
The first US patient has been enrolled in the SELUTION4SFA sirolimus drug-eluting balloon (DEB) study by Arthur Lee (Cardiac & Vascular Institute, Gainesville, USA). This study evaluates SELUTION SLR in the treatment of occlusive disease of the superficial femoral artery (SFA) and proximal popliteal artery (PPA).
Endologix has announced the online publication of the final five-year results of the LEOPARD trial in the Journal of Vascular Surgery (JVS). The study’s findings showed that there was no significant difference in aneurysm-related outcomes between patients randomised to the AFX endograft system, with anatomical fixation, and commercially available endografts with proximal fixation.
Vivasure Medical has announced it has enrolled the first patients in the company’s PerQseal PATCH clinical study, a multicentre, single-arm, pivotal study evaluating the safety and efficacy of the Vivasure PerQseal closure device system. The first patients were enrolled at Kaleida Health’s Buffalo General Medical Center-Gates Vascular Institute (Buffalo, USA).
Xeltis has presented “highly-encouraging” six-month data from its first-in-human (FIH) aXess vascular graft trial at the 13th Congress of the Vascular Access Society (VAS; 27–29 April, Porto, Portugal). A press release outlines that six-month data from the FIH trial found that the aXess vascular access graft for haemodialysis demonstrated high patency rates.
Govindarajan Narayanan, chief of interventional oncology at Miami Cancer Institute and a vascular interventional radiologist with Miami Cardiac & Vascular Institute (both Miami, USA), successfully treated the first patient in the USA with a liver tumour using Quantum Surgical’s Epione robot. The procedure took place at Baptist Health South Florida (Miami, USA).
Akura Medical announced today it has initiated its first-in-human clinical study of the Akura mechanical thrombectomy platform—a low-profile solution designed to easily access and efficiently remove large-volume, mixed-morphology clots, and eliminate the guesswork around the procedure. The initial five cases were performed in Bradenton, USA and marked the first use of mechanical thrombectomy for pulmonary embolism (PE) in the country.
Teleflex has announced new research findings reinforcing the long-term durability of PUL with the UroLift system and lower complication rates compared to other minimally invasive procedures for men with enlarged prostate, also called BPH.
Medtronic has announced that Ken Washington has been appointed chief technology and innovation officer.
Washington joins Medtronic from Amazon where he served as vice president and general manager of consumer robotics, and will lead technology development across industries including robotics, consumer products, automotive and space in a newly created role, Medtronic said in a press release.
“This new leadership role will help Medtronic to harness the innovative spirit of our founders and ensure we are capitalising on our scientific and technological knowledge to invent, innovate and disrupt the healthcare technology market of the future,” said Geoff Martha, chairman and CEO, Medtronic. “Dr Washington will help Medtronic expand use of our technology platforms across our portfolio—including robotics, sensors, implantables and AI—improving our returns on investments in innovation and expanding our technological competitive advantage to drive durable growth.”
Prior to his role at Amazon, he was chief technology officer at Ford Motor Company, overseeing development of the company’s technology strategy including next-generation vehicle architectures, controls, and automated systems; and he spent seven years at Lockheed Martin in various leadership roles including chief technology officer, chief privacy officer and vice president, Advanced Technology Center, Lockheed Martin Space Systems Company.
Dr Washington earned a Bachelor of Science, a Master of Science, and a doctorate in nuclear engineering from Texas A&M University (College Station, USA).
IceCure’s ProSense® System was installed at Kovai Medical Center and Hospital KMCH) in Coimbatore, India. The event was attended by Tammy Ben Haim, Consulate General of Israel, and several executives and doctors from KMCH.
The ProSense System was installed at Kovai Medical Center and Hospital in Coimbatore, India. The event was attended by Tammy Ben Haim, Consulate General of Israel, and several executives and doctors from the hospital.
IceCure Medical has announced that ProSense was recently installed and inaugurated at Kovai Medical Center and Hospital (KMCH) in Coimbatore, India. This development, to the company’s knowledge, constitutes the first instance of cryoablation for breast cancer treatment being offered in the country. KMCH, a leading hospital in southern India, is an innovator that has had numerous technology firsts in the region.
The installation of ProSense was unveiled by Tammy Ben Haim, Consulate General of Israel, along with executives and doctors from KMCH including Nalla G Palaniswami (chairman), Arun N Palaniswami (executive director), Mathew Cherian (chief of radiology services), and Rupa Renganathan (lead consultant in breast cancer at KMCH).
In her public statement at the inauguration, Ben Haim said: “With this innovative Israeli technology, IceCure’s ProSense mission is to make cancer treatment safer and more effective by providing minimally invasive solutions for patients around the world. Although ProSense’s capability spans the treatment of different types of tumours, here in India its first application will be in the fight against breast cancer.
“We are pleased that women in India now can choose a minimally invasive procedure that has shown high efficacy in interim study results. This installation is the latest in our global commercial rollout,” stated Tlalit Bussi Tel Tzure, IceCure’s vice president of marketing. “We have a productive relationship with our in-country distributor in India, which is a significant market for us, and we look forward to participating in the 10th Annual Conference of the Breast Imaging Society of India later this year.”
Penumbra has announced the US Food and Drug Administration (FDA) clearance and launch of Lightning Bolt 7, which the company claims is the most advanced and powerful arterial thrombectomy system on the market.
Lightning Bolt 7 introduces a new method for removing blood clots—modulated aspiration, which pairs Penumbra’s Lightning intelligent aspiration technology with an advanced microprocessor algorithm. When used alongside this innovation, Lightning Bolt 7 is designed to enhance the ability to rapidly remove large, fibrous blood clots in the arteries with minimal blood loss, addressing conditions like acute limb ischaemia (ALI), hibernating thrombus and visceral occlusions.
“The unique mechanism of Lightning Bolt 7 provides modulated aspiration at the tip of the catheter, enabling the quick removal of these rigid and stiff blood clots, which oftentimes require open surgery and frequently result in amputation,” said Kalyan Veerina (Cardiovascular Institute of the South [CIS], Opelousas, USA). “Advancements like Lightning Bolt 7 provide a critical frontline option for physicians to treat patients and improve patient outcomes.”
Powered by the Penumbra Engine, Lightning Bolt 7 is engineered to detect the difference between blood clotting and blood flow. Additionally, it is designed to identify friction within the catheter, and orchestrate the rapid opening and closing of the valves to disrupt any resistance between the clot and the catheter tip. This facilitates maximum vacuum force at the catheter tip for optimal, rapid ingestion of blood clots. Lightning Bolt 7 is compatible with Penumbra’s arterial catheters, which are made with MaxID hypotube technology, allowing a larger inner diameter while maintaining a lower profile and a soft, atraumatic tip design to maximise the circumferential sweep in the artery.
“This era of computer-aided technology offers the promise of unheralded procedural efficiency that was not previously available to endovascular specialists,” said Sahil Parikh (Columbia University Irving Medical Center, New York City, USA). “Our ability to rapidly revascularise vessels with minimal blood loss is exceptional with these intelligent devices.”
“Technologically, Lightning Bolt 7 is a big leap forward,” said Raghu Motaganahalli (Indiana University Health Physicians, Indianapolis, USA). “The computer-aided components offer a safety profile that, when combined with the clot-removal speed and efficiency, will promote an endovascular-first approach for a broader range of cases before considering open surgery.”
Lightning Bolt 7 received US FDA clearance and became available in March 2023. It is part of Penumbra’s Indigo system with Lightning portfolio, which are the only computer-aided mechanical thrombectomy systems currently available in the USA, according to a press release from the company.
“With our latest advancements in computer-aided technologies, Penumbra offers one of the most comprehensive mechanical thrombectomy product lines for arterial, venous, pulmonary and mesenteric thrombus,” said James Benenati, chief medical officer at Penumbra. “Lightning Flash and Lightning Bolt 7 will continue to advance the standard of care for these difficult conditions, removing clot from the body quickly, safely, in a single session, and without the need for lytics or open surgery, potentially improving quality of life for our patients.”
Adept Medical has announced the launch of the Head Immobiliser—a radiolucent support for a range of interventional radiology (IR) and neuroradiology procedures. Now commercially available, the positioning device can help mitigate the costs of retakes, from reducing the amount of mid-procedure interventions caused by head movement in awake patients, to enabling interventionalists to consider conscious sedation as an option, as well as minimising patient exposure to radiation.
Stephen Florance, lead product design engineer from Adept Medical, said the following of the Head Immobiliser: “Many interventional neurologists and radiologists have conveyed to us their frustration with holding the head still during conscious sedation neurointerventional imaging procedures. The solutions currently in place for head fixation during these procedures are inadequate, resulting in poor image quality, higher patient radiation exposure, and longer procedure times.
“We knew we had to create a product that can immobilise the head quickly, and more consistently than the current makeshift solutions. Radiolucency was also a must.
“A key hurdle we had to overcome was the ability to manufacture the hoods. Unable to rely on a supplier, we had to be creative and so we developed our own unique thermoforming process in-house. We are very happy with the final product.”
The Head Immobiliser uses vacuum suction to lock the hood shape, and with it, the patient’s skull, reducing unwanted movement comfortably. This helps to align the 3D roadmap and angiography, ensuring interventions are performed under optimal conditions, providing benefits to patient management and procedural workflow.
With an aluminium equivalence of 2.23mm through the hood, the Head Immobiliser has been designed to have minimal interference with X-Ray imaging.
Compatible with most imaging tables, the Head Immobiliser is easy to set up, and takes up minimal space in the operating theatre.
ABK Biomedical has received approval for its investigational device exemption (IDE) application from the US Food and Drug Administration (FDA) to commence a multicentre pivotal clinical study in the USA for its Eye90 microspheres yttrium-90 (Y90) radioembolization therapy.
The pivotal clinical study, Route90, is designed to evaluate the safety and efficacy of Eye90 microspheres in patients living with unresectable hepatocellular carcinoma (HCC). The Route90 study will evaluate HCC tumour response rates and duration of response from Eye90 microspheres treatment as co-primary endpoints. Eye90 microspheres is the first and only imageable Y90 microspheres device. The study also includes endpoints to evaluate safety, the potential benefits of intraprocedural visualisation, and the ability to perform post-treatment computed tomography (CT) dosimetry with imageable microspheres.
Andrew Kennedy is physician-in-chief of radiation oncology at Sarah Cannon Cancer Institute (Nashville, USA) and will serve as principal investigator for the Route90 study. Kennedy is one of the early pioneers of Y90 radioembolization research and treatment. “I am excited to participate and lead the Route90 study. Eye90 microspheres is a significant and meaningful technology advancement to Y90 radioembolization therapy not seen in over almost two decades since the current therapies became clinically available,” said Kennedy.
“We are motivated to begin this pivotal study and assess the Eye90 microspheres technology in a large well-controlled, well-designed study. We continue to build upon the results of our first-in-man Eye90 microspheres study conducted recently in New Zealand. The initial results from this study are highly encouraging with an excellent safety profile and robust tumour response rates”, said Aravind Arepally, ABK Biomedical’s chief medical officer.
Mike Mangano, president, and CEO, ABK Biomedical, said: “[US] FDA approval of this pivotal study is a significant milestone for ABK. The ABK team has worked tirelessly to develop this unique technology. We have created extensive manufacturing and supply-chain efficiencies, established robust quality assurance in all our processes, and collaboratively engaged regulatory bodies for proper guidance. We believe this will become a seminal study for treating patients with unresectable HCC. We designed our Y90 radioembolization technology to align with the most recent, advanced Y90 treatment methods, techniques, and appropriate patient populations. This has the promise to significantly improve outcomes for targeted patients living with unresectable HCC”.
Twelve-month results from the SELUTION SFA trial have been presented for the first time at the Japan Endovascular Treatment (JET) Conference (26–28 May, Tokyo, Japan). The objective of this study was to assess the safety and efficacy of the Selution SLR sirolimus-eluting balloon (MedAlliance) for the endovascular therapy of de novo and non-stented restenotic lesions in the superficial femoral artery (SFA) and popliteal artery (PA).
The prospective, multicentre, single-arm trial has involved 134 patients treated across 13 sites in Japan. A press release reports that the primary endpoint of 12-month primary patency of the target lesion was achieved in 87.9% of patients; there was 97% freedom from target lesion revascularisation (TLR); no major amputations or deaths; and a 0.7% rate of thrombosis. These results were achieved despite the presence of challenging patients enrolled in the study.
“These data demonstrate that limus can be as effective as paclitaxel without the associated safety concerns and welcomes a new era for [drug-coated balloons]”, said Osamu Iida (Osaka Police Hospital Cardiovascular Center, Osaka, Japan).
“We are pleased to see that the Japanese 12-month data [are] completely aligned with the [first-in-man] done by Professor Zeller five years ago,” commented Jeffrey B Jump, chairman and CEO of MedAlliance. The US [investigational device exemption] SFA study is now enrolling, which will hopefully confirm the same benefit in US patients as we have seen in Europe and Japan.”
The company advises that Selution SLR is commercially available in Europe, Asia, the Middle East, and the Americas (outside USA) and most other countries where the CE mark is recognised.
Cora Therapeutics has announced the presentation of the results of a clinical trial at the Canadian Association of Interventional Radiologists (CAIR) annual meeting (25–27 May, Quebec City, Canada), assessing the efficacy of its proprietary antioxidant complex in safeguarding DNA from radiation exposure during aortic aneurysm stenting procedures guided by X-ray technology.
Kieran Murphy, founder, inventor, and chief medical officer of Cora Therapeutics, presented the results at the CAIR meeting.
During these high-intensity image-guided procedures, physicians were administered the antioxidant complex as two capsules, one hour prior to exposure. The results clearly showed the treated group experiencing a significant 78% reduction in DNA breaks detected by P53 tests in their cell nucleus, surpassing expectations compared to the placebo group.
Murphy’s team has demonstrated the protection of mitochondrial DNA from radiation in these subjects, marking a significant milestone in medical literature. The group given the antioxidant formulation exhibited a 54% decrease in mitochondrial DNA damage based on STAT 3 testing when compared to the placebo group. Considering that mitochondrial DNA is inherited maternally and is 13 times more vulnerable to radiation than nuclear DNA, this achievement holds tremendous promise.
The was conducted by two independent teams of scientists, one at Princess Margaret Hospital, University Health Network, Toronto, and the other at McMaster University, Hamilton, Ontario, Canada.
The research findings will now undergo the peer-reviewed publication process. This antioxidant formulation has the potential to mitigate DNA breaks in patients undergoing computed tomography (CT) scans, X-rays, mammography, angiography, dental X-rays, and could become an integral part of the daily routine for the 2 million healthcare workers worldwide who perform cardiac and angiographic interventions under X-ray guidance or work in radiology and cardiology departments.
Murphy’s previous prospective, randomised human study showcased an impressive over 90% reduction in DNA breaks among patients undergoing Nuclear Medicine bone scans. This research was published in the Journal of Vascular Interventional Radiology in 2016.
Radiation, classified as an oxidative stressor, leads to the accumulation of harmful free radicals in the body, much like air pollution, ultraviolet (UV) light, smoking, processed diets, and frequent flying. Unprotected, these deleterious free radicals infiltrate DNA, elevating the risk of DNA damage and gene mutation. However, the Halo antioxidant complex, which can be taken daily or one hour before radiation exposure, has demonstrated significant efficacy in reducing DNA breaks, as indicated by the collected data.
Halo is an antioxidant formulation that consists of carefully selected natural ingredients that comply with NHPD guidelines, ensuring maximum safety and optimal efficacy while upholding the highest standards for nutraceutical products. The patented blend of ingredients effectively neutralises free radicals, preventing them from damaging the body’s cells. Cora Therapeutics has employed pharmaceutical-level scientific rigor to develop this innovative nutraceutical.
Halo has received clearance from Health Canada and the US Food and Drug Administration (FDA). It is protected by four issued patents globally and has been the subject of nine peer-reviewed publications, solidifying its scientific validity and potential.
On 24 May, the US Food and Drug Administration (FDA) granted an investigational device exemption (IDE) approval for Concept Medical’s MagicTouch percutaneous transluminal angioplasty (PTA) sirolimus-coated balloon (SCB) for treatment of the superficial femoral artery (SFA).
This marks the fourth IDE approval for the company’s SCB, a press release reports. Concept Medical has already received three other pivotal IDE approvals for its SCB MagicTouch family of products for coronary in-stent restenosis (ISR), coronary small vessel and below-the-knee indications.
The IDE approval will allow Concept Medical to initiate a pivotal clinical study to demonstrate safety and effectiveness of the MagicTouch PTA SCB in femoral and popliteal segments. The data generated from this IDE clinical study will support a future premarket approval (PMA) application in the USA.
According to the company, MagicTouch PTA is the world’s first SCB with extensive commercial usage in Europe, major markets of Asia and the Mid-Eastern markets. Concept Medical further claims that the device is the most clinically studied sirolimus drug-coated balloon (DCB) for peripheral arterial disease (PAD) treatment, referencing the largest head-to-head randomised controlled trial (RCT) against a paclitaxel DCB, and the largest RCT against an uncoated balloon.
“We are extremely proud to have received the fourth IDE approval from the US FDA for the MagicTouch PTA in the SFA indication,” said Manish Doshi, founder and managing director, Concept Medical Group. “This milestone underscores our unwavering commitment to advancing medical technology and providing innovative solutions that have the potential to transform patient care.”
Govindarajan Narayanan, chief of interventional oncology at Miami Cancer Institute and a vascular interventional radiologist with Miami Cardiac & Vascular Institute (both Miami, USA), successfully treated the first patient in the USA with a liver tumour using Quantum Surgical’s Epione robot. The procedure took place at Baptist Health South Florida (Miami, USA) a few days after the US Food and Drug Administration (FDA) cleared Epione robot for treatment of all abdominal cancers.
Quantum Surgical’s flagship product, the Epione robotic platform, is dedicated to the curative treatment of cancers. Epione allows physicians to treat inoperable tumours that are particularly difficult to reach, due to their size or their location, at an early stage, in a simple and effective way. More than 150 patients have already been treated with the Epione robot in Europe, and Narayanan successfully treated the first patient in the USA.
“I am honoured to be the first physician to utilise Epione in the USA as this robotic-assisted equipment is going to change the way we deliver effective treatments to our patients for cancerous tumours,” said Narayanan. “Baptist Health has always been at the forefront when it comes to providing the very best care to the South Florida community and beyond. I am proud to be a part of such an incredible team.”
Bertin Nahum, president and co-founder of Quantum Surgical stated in a press release: “We are very proud of this first intervention with our Epione robot in the USA. We are delighted to have been able to work with Narayanan and Baptist Health South Florida. This first intervention coincides with the US FDA extension clearance to deploy our robotic solution in the USA. Dr Narayanan is paving the way for physicians who will be able to offer more patients to benefit from innovative and less invasive treatments, and improve their lives.”
Epione is a robot-assisted technology designed to plan, target, perform and confirm tumour ablation. Epione enables physicians to perform percutaneous tumour ablations, a minimally invasive treatment in which one or more needles are inserted through the skin into the tumour to destroy it.
A new study using data from millions of patients hospitalised across the USA has determined whether population density and associated urban versus suburban versus rural environments predispose patients with peripheral vascular disease for chronic poor blood flow in their lower extremities. The findings were presentedat the Society for Cardiovascular Angiography & Interventions (SCAI) 2023 Scientific Sessions (18–20 May, Phoenix, USA).
Advanced and chronic peripheral arterial disease can significantly increase a patient’s risk for all-cause mortality including myocardial infarction (MI), stroke, and heart failure. The study aimed to identify the role that sociodemographics, including population density in a patient’s hometown affect outcomes including mortality from chronic limb-threatening ischaemia (CLTI).
In the study, deidentified patient data from the National Inpatient Sample (NIS) from 2001–2013 were queried. Inclusion criteria included a diagnosis of CLTI. Data were analysed using SPSS software in a binary logistic regression model, a p value <0.001 was considered statistically significant, and samples were standardised for comparison using predicted probabilities.
Of the 100m+ patients in the NIS, there were 1,907,089 patients identified with CLTI. Patients living in an urban setting with a population greater than one million people were found to be at a statistically significant decreased risk of mortality from CLTI (odds ratio [OR]=0.647, p<0.001). Females were also at a statistically significant decreased risk of mortality (OR=0.846, p<0.001). There was no statistically significant increase in mortality among different age groups, races, insurance carriers, median household income, or elective admission status (p<0.001).
“We now know that we need to ambulate our patients and encourage aggressive physical activity earlier and more frequently, especially for men,” said Harsh Jain (Montefiore Health System, New York, USA), lead author of the study. “This is a very low cost, low barrier to adoption that has significant ramifications including improved mortality for millions of people, decreased burden on healthcare resources, and millions of dollars in healthcare spending. Furthermore, men should be more vigilantly monitored when diagnosed with peripheral vascular disease, as they seem to fare worse regardless of where they are across the nation.”
Based on the findings, researchers suggest that patients with CLTI should be encouraged to maintain an active lifestyle and engage in vigorous exercise regimens earlier in their disease course to prevent progression and decrease their risk of mortality.
Using data from Medicare, the CLIPPER cohort was created to develop and test process measures for CLTI, which could ultimately be used to measure and improve quality of care.
Using inpatient and outpatient claims data from patients with fee-for-service Medicare from 2010 to 2019, a coding algorithm was used to identify patients with CLTI. To qualify for a CLTI diagnosis, patients had either 1) one diagnostic code for peripheral arterial disease and one diagnostic code for ulceration, infection, or gangrene on the same inpatient or outpatient claim, or 2) one CLTI-specific diagnostic code, as well as a procedure code indicating arterial vascular testing within six months before or after the qualifying CLTI diagnostic code(s).
The cohort comprised 1,130,065 patients diagnosed with CLTI between 2010 and 2019. Mean age of the cohort was 75±5.8 years; 48.4% were women and 14.6% were Black. Within 30 days of CLTI diagnosis, 20.4% of patients underwent percutaneous or surgical revascularisation. Within six months, 3.3% of patients underwent major amputation; 16.7% of patients died at one-year follow-up and 50.3% at five-year follow-up.
“CLTI is an incredibly deadly disease if not treated quickly after diagnosis, but we know very little about how hospitals perform with respect to treatment,” said lead author Alexander Fanaroff (University of Pennsylvania, Philadelphia, USA). “Comprehensive process measures are needed for patients in order to advance care and improve the chance of survival. Our hope is that this study is a first step toward developing better process measures.”
The authors note they plan for the CLIPPER data to be used for future studies on CLTI, including developing process measures that can be captured from administrative claims data, and measuring their association with limb outcomes and corresponding racial, ethnic, socioeconomic, gender-based, and geographic variability.
Steven Abramowitz (Washington DC, USA) explains the significance of the CLOUT registry—the only registry capturing data on mechanical thrombectomy in deep venous thrombosis (DVT). CLOUT confirms excellent safety results and effectiveness of the ClotTriever system in real-world DVT patients. In a propensity-score matched analysis, comparing this modern mechanical thrombectomy and historical ATTRACT treatment outcomes, ClotTriever shows better thrombus extraction and improvement in 30-day Villalta score, suggesting potentially long-term implications for patient outcomes. Apart from the CLOUT Registry, the ClotTriever system is part of the DEFIANCE Trial, a randomised controlled trial (RCT) evaluating its clinical outcome in DVT treatment. “The goal of DEFIANCE is to demonstrate that mechanical thrombectomy is superior to anticoagulation alone. The previous RCTs have all focused on catheter-delivered lytics and we know that the downside of lytics is bleeding, which was a significant outcome of the ATTRACT study—says Stephen Black (London, UK). “Trying to find something that avoids lytics is going to be really useful for this therapy”.
To learn more about clinical outcomes in the CLOUT Registry, the design of the DEFIANCE trial and benefits of the ClotTriever system, join the INARI Symposium at LINC 2023 (June 6–9, Leipzig, Germany) on June 7th (Wednesday) at 12:35–13:20 (Technical Forum).
This video was filmed by Inari Medical and is being sponsored for distribution in association with Vascular News, Interventional News, Venous News and CX Vascular. Biba Medical bears no responsibility for the assets used in the production of this video.
Six-month outcomes from FLASH registry have shown that patients with pulmonary embolism who were treated with mechanical thrombectomy showed significant improvement in symptoms, quality of life and cardiac functions.
The findings were presented as late-breaking clinical research at the Society for Cardiovascular Angiography & Interventions (SCAI) 2023 scientific sessions (18–20 May, Phoenix, USA).
FLASH is a prospective, single-arm, multicentre registry of acute pulmonary embolism patients treated with the FlowTriever system (Inari Medical). Six-month clinical outcomes were assessed, including Modified Medical Research Council (Mmrc) dyspnoea score, right ventricular (RV) function, six-minute walk test (6MWT) distances, and PEmb Quality of Life (QoL) scores.
Initial data show the safety and effectiveness of long-bore thrombectomy, removal of blood clots using a mechanical catheter, for the treatment of pulmonary embolism rather than the current standard-of-care, anticoagulation along with the use of catheter-based interventions, but limited data exist on longer-term outcomes.
The trial enrolled 800 patients across 50 US sites, 54.1% were male and the mean age was 61.2 years. Thrombolytic contraindications were reported in 32.1% of patients, and 77.1% were classified as intermediate-high-risk and 8% as high-risk. Most patients (74.8%) completed all study visits through a six-month follow-up.
In 599 patients who completed a six-month follow-up, multiple statistically significant functional and clinical improvements were reported during the study period.
Findings show that the proportion of patients with normal echocardiographic RV function increased from 15.1% pre-thrombectomy to 95.1% and 94% had normal pulmonary artery pressures. Furthermore, all-cause mortality was 0.3% at the 48-hour visit, 0.8% at the 30-day visit, and 4.6% at study exit (median=199 days post-treatment).
Patient exercise tolerance and symptoms also improved significantly after treatment, with the distance a patient were able walk in six minutes increasing from 180 meters at 48 hours post treatment to 398 meters.
Median mMRC dyspnea score improved from 3 at baseline to 0 (p<0.0001), and the percentage of patients with normal RV function on echocardiography increased from 15.1% at baseline to 95.1% (p<0.0001), and RV systolic pressure ≤40mmHg improved from 28.4% at baseline to 93.9%.
Six-month prevalence of site-reported chronic thromboembolic pulmonary hypertension was 1% and chronic thromboembolic disease was 1.9%.
“It is encouraging to see the dramatic and rapid improvement in both clinical outcomes and daily activities of our patients, like taking a walk without running out of breath,” said Sameer Khandhar (University of Pennsylvania Penn Presbyterian Medical Center, Philadelphia, USA), a study co-author. “We are hopeful these FLASH data serve as a next step in understanding the importance of thrombectomy as a treatment option for patients that shows in their recovery and improvements in day-to-day quality of life.”
In addition to significant improvement in patient symptoms, cardiac function and quality of life, long-term low mortality was also reported following treatment with the FlowTriever System. These data suggest that rapid extraction of thrombus may prevent long-term impact in pulmonary embolism patients, though comparative data relative to conservative management are needed.
Following the initial results of the BEST-CLI (Best endovascular versus best surgical therapy in patients with critical limb ischaemia) trial in 2022, which found surgical intervention superior to endovascular revascularisation, questions remained regarding how inclusive the enrolled patient population was, how reflective the specialty of the physicians who performed the procedures are compared to the broader breakdown of US specialists performing peripheral procedures, and whether outcome rates are similarly observed in clinical practice among Medicare beneficiaries.
The BEST-CLI trial compared two CLTI treatment options, endovascular revascularisation and surgical bypass to understand which approach leads to better outcomes. While the study found surgical revascularisation to be superior, the generalisability of this study to the clinical population with CLTI has not been evaluated.
The new study sought to analyse a broader clinical population by identifying all Medicare beneficiaries between 2016–2019 and aged 65–85 years with a diagnosis of CLTI who underwent endovascular or surgical revascularisation. Revascularisation was stratified by endovascular, autologous graft, and non-autologous graft. The endpoint was a composite of major adverse limb events (MALE) and death.
A total of 66,153 patients were included in this study (10,125 autologous graft; 7,867 non-autologous graft; 48,161 endovascular). Compared to BEST-CLI Cohort 1, patients were older, more often female and had a greater burden of comorbidities. Endovascular operators for the study population versus BEST-CLI were less likely to be surgeons (55.9% vs. 73.0%) and more likely to be interventional cardiologists (25.5% vs. 13.0%). The risk of death or MALE in this cohort was higher with surgery (56.6% autologous grafts vs. 42.6% BEST-CLI Cohort 1; 51.6% non-autologous grafts vs. 42.8% BEST-CLI Cohort 2) but similar with endovascular (58.7% real-world vs. 57.4% Cohort 1; 47.0% real-world vs. 47.7%). Of those receiving endovascular treatment, major interventions occurred less frequently compared to the trial (10.0% real-world vs. 23.5% Cohort 1; 8.6% real-world vs. 25.6% Cohort 2).
“For critical limb ischaemia, the key is ensuring timely access to vascular care. Although the BEST-CLI trial is important, it does not fully capture the full range of CLI patients, including older patients with greater comorbidities,” said Eric A Secemsky (Beth Israel Deaconess Medical Center, Boston, USA), the study lead, in a SCAI press release. “The findings from our study point to the need to individually tailor revascularisation strategies based on patient risks, benefits and preferences.”
The authors note that older CLTI patients may not experience the same benefit with bypass surgery as observed in BEST-CLI where at the time, fewer Medicare patients were enrolled in the trial.
Discussing the role of artificial intelligence (AI) in improving outcomes within research and practice development, Hamid Mojibian (Yale School of Medicine, New Haven, USA) explicated the ways in which AI is changing interventional radiology (IR) at the 2023 Global Embolization Oncology Symposium (GEST, 18–21 May, New York City, USA).
“AI is here” was Mojibian’s introductory statement, pointing to the definite AI integrations that are already occurring in radiology. Expanding on this, he described an AI-based workflow that can identify critical findings through image acquisition, automatic AI application and prioritisation of key findings. These findings can then trigger an alert which connects patients with the most appropriate care teams, and subsequently automate patient follow-up.
Using pulmonary embolism (PE) as an example, Mojibian draws parallel comparison between the workflow with and without AI—with more steps and a less direct pathway to treatment in the non-AI roadmap, Mojibian highlighted how AI can enable a “more effective” care system.
Following this, he discussed disease discovery modules that utilise natural language processing (NLP) to analyse radiology reports. Potential uses for this technology span from uterine fibroids, spine compression fractures and detecting inferior vena cava (IVC) filters that are eligible for removal—Mojibian stated in a single month they identified 91 filters that were eligible. Furthermore, he added that in deep venous thrombosis cases, NLP systems have the potential to increase patient recruitment for randomised trials.
Continuing to outline the effectiveness of AI’s employment within healthcare, Mojibian explained a prospective research workflow enabled by the technology. Initiated by a notification, he described how AI can then enable patient stratification and inclusion through integration with electronic medical records. He opined that this system improves efficiency and maximises collaboration throughout the research process, while also incorporating advanced image processing which can benefit classification, segmentation and quality control.
Of his concluding thoughts Mojibian noted that AI will not replace clinicians, but clinicians who do not take up AI technology will be replaced by those who do. Now is the time to plan and act, he stated, emphasising that greater awareness is needed to spot opportunities to lead and co-innovate with fellow healthcare professionals.
Speaking in the Vanguard session on the first day ofthe 2023 Global Embolization Oncology Symposium (GEST, 18–21 May, New York City, USA) yesterday, Lindsay Machan (University of British Columbia, Vancouver, Canada) gave a comprehensive outlook on the next five years in embolization, outlining procedures that will be characteristic, and the advancements that are needed to propel practice into the future.
Machan began by describing the first therapeutic embolization in 1972, defining the achievement via the radiologists’ “conviction”, the equipment of the time, the research that was carried out and the comparisons drawn with existing treatment options which enacted its success.
Skipping ahead to present day, Machan introduced the current and future expansion of therapeutic embolization, briefly listing the areas he predicts to be of note including musculoskeletal (MSK) embolization, granulomatous amoebic encephalitis (GAE), shoulder/elbow enthesopathy/tendinopathy, osteoarthritis (OA) hand, lumbar facet disease and acute sporting injuries.
Observing the applications of MSK embolization, Machan stated that complex knee pain, PCS and neural mechanisms are key areas which would benefit most from the advancement of MSK embolization. Interrogating what is needed to advance the field, Machan emphasised that improved data sought through large, prospective, multicentre trials, as well as smaller and resorbable embolics are the pathways to take to do so.
Next, addressing lymphatic interventions such as peripheral lymphatic embolization, retrograde transvenous and transcervical accesses and mesenteric lymphangiography, Machan moved on to explore future opportunities within embolization. Referencing a study published in Radiology titled ‘Imaging and interventions for lymphatic and lymphatic-related disorders’, Machan explained that the lymphatic system is involved in all disorders that present with fluid accumulation. For this reason, he opined that more evolved imaging, better access tools and new embolic agents are essential to continued progression in the specialty.
Acknowledging two pivotal changes, the speaker then recognised the seismic shifts artificial intelligence (AI) and consumerism have made in healthcare delivery. Discussing the role of AI in embolization, Machan noted a preliminary study—published in the Annals of Vascular Surgery—that concerned AI-assisted microcatheter shaping for intracranial aneurysm coiling by Changya Liu (Huazhong University of Science and Technology, Wuhan, China). Using this example, the speaker then used the increasing prevalence of AI’s deployment within treatment to draw attention to the growing imbalance between healthcare—which makes up a sixth of US gross domestic product (GDP)—and the economy, which is expanding at a much slower rate. Additionally, he stated that medical errors are the eighth leading cause of death in the USA, while too making note of the “easily tracked” cost versus outcome dichotomy in contemporary treatment.
Concluding his presentation, Machan painted a clear picture of the future of embolization, making particular mention of more frequent MSK embolization and lymphatic procedures to come, alongside reduced usage of onxy and glue. He averred that healthcare professionals in this space will “continue to be referred patients that no one else wants to treat”, however he affirmed that it is essential that time is used advantageously to create data and exploit the pervading “digitisation of everything”.
Setting the audiences sights on the horizon at the 2023 Global Embolization Oncology Symposium (GEST, 18–21 May, New York City, USA) yesterday, Daniel Sze (Stanford University, Stanford, USA), editor in chief of the Journal of Vascular and Interventional Radiology, gave his predictions on what the interventional oncology (IO) space will look like in five years. His forecast identified the important research changing the landscape of IO, the developments that have brought us to present day, and the current areas with unmet medical needs that are receiving the most investment.
Opening his presentation with the words of Søren Kierkegaard: “Life can only be understood by looking backward; but it must be lived looking forward”, Sze began by describing recently published research articles with important implications for future practice which have been selected for editor’s awards by the Journal of Vascular and Interventional Radiology.
Delving into the content of these research papers, Sze discovered dialysis access to be the most prevalent topic to appear among award-winning papers, because of large, prospective, randomized, industry-sponsored trials. Of the most frequently awarded research within IO, Sze identified papers that explored the interactions between locoregional therapies and the immune system or immunotherapy, a topic more frequently awarded than trans-arterial radio-embolization (TARE), trans arterial chemoembolization (TACE), and ablation research publications.
Reflecting on changes that have occurred in the last five years, Sze outlined the treatments carried out now that were not performed, or as much, five years ago. Compiling a list of six treatments, Sze included musculoskeletal ablation and stabilisation, ablative dose TARE, pressure-augmented TACE, thyroid ablation, genomics biopsy and venous deprivation. Applying a set of probing questions for each, Sze interrogated the procedures respectively, asking—“why not use the concept of FLR?” for ablative dose TARE, “what is the pressure endpoint?” when performing pressure-augmented TACE, and “how can we block accelerated tumour growth without blocking hepatocyte growth?” in venous deprivation.
Pivoting to the next segment of his presentation, Sze addressed the unmet medical needs which are receiving the most investment today. First, he described new ablative technologies such as sonication, being explored by HistoSonics with their Edison histotripsy system. Additionally, Sze included the Galvanize Aliya pulsed-electric-field technology and Erik Cressman’s (MD Anderson Cancer Center, Houston, USA) development of thermochemical ablation.
Continuing, Sze outlined new anatomical targets that are receiving greater investment, such as bronchial and pulmonary TACE and renal, prostate and intracranial TARE. Alongside, these he noted new radionuclides that have received contemporary attention, for example radio-opaque TARE from ABK Biomedical and holmium-166 TARE developed by Quirem Medical, among others. Finally, Sze highlighted new immunotherapies and combination treatments that have received investment to help meet unmet medical needs, citing the large variety of non-PDL and non-CTLA4 immunotherapies in development. He foresees increased involvement of IR with in-situ vaccination, since practitioners in the field are uniquely qualified in drug delivery and local tumour environment modulation.
Casting an eye to the future, Sze concluded his presentation by stating that “five years is not a long time”, emphasising that physicians should be looking ahead not just 5 but also 15 and 50 years to identify ways that IR can lead the fight against cancer, and possibly for patients in earlier stages rather than salvage settings. Wrapping up his most salient premonitions for future practice, Sze predicted that in five years, interventional radiologists should expect to be performing incrementally improved ablation, TACE and TARE, combining locoregional therapies “more rationally” with immunotherapy, increasingly informed by tumour genetics, and most importantly, continuing the pursuit of the elusive abscopal response, the holy grail of IO.
Bentley has announced the US launch of its BeBack crossing catheter, which is designed for the treatment of heavily calcified lesions. This is the company’s first product to be launched in the USA.
A press release notes that, after the acquisition of the GoBack catheter in September 2022, Bentley worked behind the scenes on the rebranding of the device from GoBack to BeBack, making sure the device would benefit from the Bentley corporate branding.
The BeBack catheter—available in 80cm and 120cm lengths and in sizes of 2.9Fr and 4Fr—is designed for steering through chronic total occlusions (CTOs). The device makes use of a steerable and adjustable (in length) Nitinol needle, which is used for crossing and targeted re-entry purposes. A radiopaque marker indicates the direction in which the curved needle, located near the tip of the catheter, protrudes. Multiple treatment options from antegrade, retrograde and crossover are possible with the BeBack crossing catheter for intraluminal and subintimal approaches of stenotic or occluded lesions, the company details.
Robert Beasley (Palm Vascular Centers Miami Beach, Miami Beach, USA) was the first to use the BeBack in the USA. “Now that the BeBack is available I use it more frequently compared to other re-entry devices that are available on the market. The unique features of the BeBack make the most complex lesions easy to cross, and therefore the device helps to reduce the procedure time,” he said. “Reducing the procedure time is of huge benefit for both the clinical centre, the physician and of course for the patients, who will benefits the most. This and the unique features makes the BeBack such a game changer for CTO procedures.”
Bentley advises that the BeBack crossing catheter is now commercially available nationwide and that the device will be showcased and presented at several upcoming conferences both nationally and internationally.
The BeBack is CE marked and US Food and Drug Administration (FDA) cleared for commercial purposes, the company adds.
Dynamic Coronary Roadmap in use for a PCI procedure
The use of an image-guidance system that overlays angiographic images on live fluoroscopic images has been shown to reduce the amount of contrast used during percutaneous coronary intervention (PCI), trial data shared at EuroPCR 2023 (16–19 May, Paris, France) indicate.
Dynamic Coronary Roadmap (DCR) is an imaging technology developed by Philips and is designed to reduce total iodinated contrast media volumes administered during PCI procedures. The software is intended to provide a real-time and dynamic angiographic roadmap of coronary arteries, which is automatically generated from previously acquired coronary angiograms during the same procedure.
Javier Escaned (Hospital Clinico San Carlos, Madrid, Spain) delivered results of the Dynamic Coronary Roadmap for Contrast Reduction—DCR4Constrast—trial during a late-breaking trial session at EuroPCR, where he revealed that the system reduced the use of contrast media on average by 28.8% compared to PCI using angiography alone (95% Confidence Interval: 18.9%, 38.2%).
Additionally, the trial found that the DCR system was able to reduce the number of angiograms per PCI procedure on average by three runs based on a PCI procedure with an average of 11 runs or 26.3% reduction (95% Confidence Interval: 16.8%, 35.1%).
Javier Escaned
Running in centres across the USA, Europe and Israel, DCR4Contrast randomised 371 patients undergoing both ad hoc and planned PCI procedures. Patients were stratified according to the number of vessels to be treated.
Patients within the DCR group underwent PCI procedures where DCR was used to guide the advancement of coronary wires, balloons, stents and other PCI diagnostic or therapeutic devices. Patients assigned to the control group underwent PCI without DCR support following standard care.
Speaking to Interventional News, Escaned said that the DCR technology potentially has a particular benefit among patients undergoing complex PCI, as well as those with renal impairment.
“There is a great interest nowadays in so-called ultra-low contrast PCI, which is basically the skillset needed to reduce dependence of contrast administration particularly in complex patients during PCI,” said Escaned, highlighting that the issue features in a chapter in this year’s PCR-EAPCI textbook, published to coincide with the EuroPCR meeting.
“This feels like a very promising tool for this purpose, because it reduces radiation, the amount of contrast, and also it helps in transitioning from a culture of requiring the use of repeated vessel pacification with contrast, to something that relies more on a different technology.”
Escaned said that the system is relatively simple to use, given its use of existing techniques that most interventional cardiologists will be familiar with.
Speaking during a press conference at the EuroPCR meeting, William Wijns (Lambe Institute for Translational Medicine, Galway, Ireland) described the findings of the study as “really important” due to the potentially life-threatening impact of contrast induced necropathy and other side effects related to contrast usage.
A recent proposal has called for “whole-person, multidisciplinary interventions” after an interrogation of the interplay between lower extremity peripheral arterial disease (PAD) and mental health impacts. Published in the Journal of The American College of Cardiology, researchers have put forward a “biopsychosocial” PAD management roadmap, offering solutions to current care “obstacles” to better attend to both behavioural and social health needs throughout vascular treatment.
Posing significant public health concerns, Kim G Smolderen, clinical psychologist, and Carlos Mena-Hurtado, interventional cardiologist (Yale University, New Haven, USA) et al note that PAD affects roughly 8.5 million individuals in the USA and 220 million globally. Individuals of workforce age have become a growing area of concern, however, due to an increase in PAD-related hospital admissions presenting with critical limb ischaemia, the “most severe” form of the disease.
With PAD, multimorbidity is “common,” which includes both mental and physical health conditions that the authors assert disproportionately affect underrepresented groups and younger people. “Younger patients are most likely to present with mental health conditions and modifiable cardiovascular risk factors with a behavioural component” Smolderen and Mena, founders of the Vascular medicine outcomes (VAMOS) lab at Yale, et al state. They note that these can include obesity, smoking and poor dietary habits.
Rooted in “maladaptive” health behaviours, the authors believe these conditions are directly undermining cardiovascular health and disease management. This link can be seen between depression and anxiety in the context of endovascular and surgical revascularisation, which are associated with increased mortality, major amputation and higher costs.
The “PAD experience,” including the clinical and financial burden of the comorbid conditions linked with PAD, have received “little consideration,” Smolderen, Mena and colleagues opine. This lack, they believe, is driving the need to “expand the PAD care paradigm” to a biopsychosocial one, which acknowledges the contribution of both behaviour and psychosocial factors on disease management and outcomes. “The substantial societal cost of healthcare for patients with PAD, including the need to close the gaps for observed disparities and health inequities in PAD, requires a broader perspective of PAD care,” the researchers convey.
Their roadmap identifies four domains that, once addressed, can redesign vascular specialty care services to attend to the behavioural and social health needs of all patients.
Identifying first a “fundamental problem” in the way physical and mental health are divided when providing care, the authors pinpoint the “major advocacy efforts” that are needed across professional organisations serving populations of PAD. Their recommendations begin at trainee level across disciplines and specialties, defining “core competencies” which reduce stigma and “unawareness” around mental illness and its effects on PAD.
Second, they outline the evolution of highly technological and procedural care which has been “valued disproportionately” over preventative and psychosocial care in the context of reimbursement and code availability—which the authors note are both presently absent from cardiovascular speciality care. To rectify this, they believe payment reform is needed, allowing for “codes and compensation for integrated care models” which should be piloted to integrate quality metrics of care delivery, including mental health screening and treatment tracking in such a manner to affect payment of services.
Thirdly, Smolderen, Mena and colleagues emphasise that despite several evidence-based interventions stemming from high-level randomised controlled trial evidence across cardiovascular populations, there is a prevalent “lack of awareness” among health administrators regarding the “scope of practice” of allied mental and behavioural health physicians in the context of chronic disease. They believe adopting a formal approach to assessing behavioural health could be a solution for this, assigning “routine components of care” and “expanding system capacity to address health disparities and behavioural health conditions”.
As an extension of their solution, they assert that “interprofessional team-based training” that promotes “a climate of mutual respect and shared values, moving away from a hierarchical system of care delivery and delineating roles” be established. Furthermore, Smolderen, Mena, et al state that investments in programme building and coordination for vascular patients must be made, as well as the promotion of integrated care for diverse and uninsured populations, to “broaden access” and remove barriers to PAD care.
Their fourth and final area of proposed reform concerns integrated behavioural care practice guidelines for PAD management, and the formation of better evidence-based workflows derived from comparative effectiveness and implementation research—which they currently believe to be “lacking”.
“Funding budgets for research,” the authors state, “is needed to generate evidence for implementation models of integrated care delivery, tailored to the PAD context”. Smolderen, Mena et al conclude that research is needed to address “clinical, operational and financial” outcomes—which includes decreased cost of care for comorbid patients—relevant to multiple stakeholders. To this end, they believe quality efforts at a national level will help to “benchmark data” for PAD care, “integrating social determinants of health, and tracking the use of integrated care services for vascular populations”.
Varian, a Siemens Healthineers company, is introducing the Isolis cryoprobe, a single-use, disposable device designed for use with CryoCare systems that seeks to improve procedural efficiency and precision for cryoablation.
The new Isolis cryoprobe offers the interventional radiologist greater operational control, with features designed to enhance predictability, precision, and efficiency. It features a small 2.1mm/14G shaft and a sharp probe tip to facilitate smooth and accurate placement.
Isolis is also the first cryoprobe to offer optional integration with the Siemens Healthineers myNeedle laser guidance system, which was developed for image-guided interventional procedures. The clinician can use the myNeedle laser to guide the insertion and trajectory of the cryoprobe while using imaging to monitor placement progress.
“The Isolis cryoprobe reflects the significant opportunity Varian has as a Siemens Healthineers company to seek to raise the standards of procedural efficiency and precision,” said Francis (Frank) Facchini, president, Interventional Solutions at Varian. “This exciting development represents the first new interventional radiology product since combining with Siemens Healthineers, and a first step towards our goal of making these impactful, minimally invasive treatment options easier to execute and more widely accessible to the patients who can benefit. We look forward to further collaboration and innovation on behalf of patients worldwide, as we continue to advance our mission to help create a world without fear of cancer.”
Akura Medical announced today it has initiated its first-in-human clinical study of the Akura mechanical thrombectomy platform. A press release notes that the Akura platform is a low-profile solution designed to easily access and efficiently remove large-volume, mixed-morphology clots, and eliminate the guesswork around the procedure. The initial five cases were performed in Georgia and marked the first use of mechanical thrombectomy for pulmonary embolism (PE) in the country.
Ehrin Armstrong (Advanced Heart & Vein Center, St Helena, USA) and S Jay Mathews (Bradenton Cardiology Center, Bradenton, USA) proctored the first procedures in Georgia. A prospective, single-arm, multicentre study will evaluate the safety and performance of the Akura mechanical thrombectomy platform for venous thromboembolism (VTE), the company reveals.
“The Akura platform is differentiated with a state-of-the-art design that aims to address the major challenges of today’s options, specifically catheter clogging and having to confirm contact with the clot prior to initiating removal,” said Mathews. “The system’s integrated aspiration and maceration technology is equally efficient against mixed morphology thrombus without clogging the catheter. Additionally, physicians can inject contrast at any time to identify catheter position relative to the clot and capture the clot without crossing it.”
“Akura’s platform incorporates continuous monitoring of hemodynamic data which will change how we approach thrombus removal. This information can enable physicians to know when a substantial clot has been removed and provides actionable metrics around the procedure,” added Mahmood Razavi (Vascular & Interventional Specialists, Orange, USA).
The Akura platform will be showcased during Innovator’s Day at EuroPCR 2023 (16–19 May, Paris, France). Razavi will present on behalf of the company during the pulmonary embolism session beginning at 3:25pm CET on Monday 15 May. Akura Medical will be at booth M23 where PCR attendees can learn more about the platform.
“The first-in-human cases mark an important milestone for Akura in addressing the challenges physicians face with VTE today,” stated Murali Srivathsa, president and chief executive officer, Akura Medical. “I would like to thank the entire team for their seamless execution and our physician advisors for their expertise and guidance in designing and supporting this initial clinical experience. We look forward to sharing additional details about the high-performance Akura platform at PCR next week.”
Guerbet has announced in a press release that based on the most recent scientific and clinical evidence, the American College of Radiology (ACR) Committee on Drugs and Contrast Media has classified Elucirem (gadopiclenol) as a group II agent. This highly stable macrocyclic gadolinium-based contrast agent (GBCA), has the highest relaxivity in its class for magnetic resonance imaging (MRI) and is indicated for use in adults and children aged two years and older. Elucirem requires only half the gadolinium dose of conventional non-specific GBCAs, addressing practitioners’ concerns about gadolinium exposure.
“This new classification from the ACR is a real game changer for the future of Elucirem,” said Jared Houk, commercial vice president at Guerbet. “This is an important moment for our team as it really shows the benefit of this product and its potential in the market.”
The classification states that gadopiclenol “demonstrates kinetic stability and a long dissociation half-life that are comparable to other group II macrocyclic agents. Based on the most recent scientific and clinical evidence, the ACR Committee on Drugs and Contrast Media considers the risk of [nephrogenic systemic fibrosis] among patients exposed to standard or lower-than-standard doses of gadopiclenol is sufficiently low or possibly non-existent such that it has been classified as a group II agent.”
Elucirem (gadopiclenol) injection is used to detect and visualise lesions with abnormal vascularity in the central nervous system (brain, spine, and associated tissues) and the body (head and neck, thorax, abdomen, pelvis, and musculoskeletal system).
GBCAs improve the contrast between lesions and surrounding tissues by accelerating the relaxation of protons thanks to interaction with gadolinium atoms. Gadopiclenol, the active drug substance of Elucirem, has been designed to enable twice as much interaction.
Stereotactic body radiotherapy (SBRT) is being used increasingly in early-stage lung cancer. Between 2012 and 2018, the proportion of otherwise healthy patients treated with SBRT increased from 15 to 26%.
A study at the Yale University School of Medicine (New Haven, USA) looked at data from the National Cancer Database for this six-year period and compared the five-year survival rates for patients who had surgical resection and patients who elected to have SBRT. Overall, 30,658 patients were identified, including 24,729 (80.7%) who underwent surgery and 5,929 (19.3%) treated with SBRT.
In propensity-matched patients, survival favoured SBRT for the first several months, but reversed after one year and long-term significantly favoured surgical management (five-year survival 71.0% for surgery vs. 41.8% for SBRT). When the propensity-matched analysis was repeated to only include SBRT patients who had documented refusal of a recommended surgery, surgical management again had a superior five-year survival with (71.4% vs. 55.9%).
The increasing usage of SBRT in otherwise healthy individuals represents a potential loss in life years for patients with early-stage non-small-cell lung cancer. Among patients who are eligible for either treatment, long-term survival favours surgical management, particularly for patients with a health-related life expectancy exceeding two years.
Microbot Medical, the developer of the Liberty robotic system, the first single-use endovascular robotic system, has received the histopathology report from the research laboratory that performed the animal study for the Liberty robotic system in October 2022. The company also reports that it has initiated preparations for potential first-in-human cases using the robotic system in Brazil.
During the animal study, the physicians conducted 63 navigations to the targeted sites using the investigational Liberty robotic system and performed an equal number of procedures manually. The Liberty robotic system received overwhelmingly positive feedback from participating physicians, and there were no observable immediate intraoperative adverse events, or harm, to the test subjects.
The new data from the report, which included histopathology data, exhibited equivocal results which were identified as related to unusual physiological animal responses in both manual and robotic test groups.
The company believes the results of the study allow it to move forward and focus on the next phases to ultimately include a USA-based pivotal preclinical study.
The company, together with its regulatory experts and consultants, believe a larger sample size and robust data generated by this study will advance the company’s efforts towards the submission of investigational device exemption (IDE) with US Food and Drug Administration (FDA).
Microbot Medical has also shared in a press release that it has initiated preparations for potential first-in-human cases in Brazil, by engaging with interventional radiologist Francisco Cesar Carnevale (University of São Paulo, São Paulo, Brazil). This collaboration is expected to support the company’s intention to conduct a FIH clinical trial in Brazil as part of its ongoing clinical and regulatory efforts.
“Following the successful usage of the LIBERTY system in over 100 preclinical catheterisation procedures, and the value the key opinion leaders that have performed those cases see in the Liberty system, the engagement with Prof Carnevale to perform the first clinical cases represents a major step as we aim to continue our efforts toward regulatory approvals and commercialisation,” commented Harel Gadot, chairman, CEO and president of Microbot Medical. “Parallel to working in our main target markets for our innovative robotic system, like the USA and Europe, we are constantly seeking additional collaboration and key opinion leaders, who wish to benefit their patients and the healthcare provider in their respective markets.”
The potential clinical cases are expected to commence upon completion of the verification and validation process of the Liberty robotic system, as well as obtaining the necessary regulatory approvals to perform those cases.
Judges of the CX 2023 Dragon’s Den-style contest—the finale of the Charing Cross (CX) Symposium (25–27 April, London, UK) Innovation Showcase programme—described the field of entrants to this year’s edition of the competition as the strongest line-up in its history.
The judging panel of physician-innovators selected HeartEye, a Netherlands-based developer of handheld electrocardiogram (ECG) devices, as the overall winner of the innovation prize, which comes with a £1,000 award. Honourable mention was given to four other entrants from the field of 12.
Peter Doevendans (UMC Utrecht, Utrecht, The Netherlands) gave an overview of the HeartEye technology in a short presentation entitled ‘ECG anytime, anywhere in 60 seconds’, describing it as a “digital transformation” for ECG acquisition. HeartEye is a pocket-sized device that can take clinical-standard ECG readings wirelessly, negating the need for a large, stationary ECG unit.
The technology, which has been developed with the support of an Innovative Medical Devices Initiative (IMDI) grant from the Netherlands Organisation for Health Research and Development (ZonMw) is patented, and could be marketed to healthcare providers or direct to consumers within two years, Doevendans explained.
“We have been doing this for a number of years, and this was the toughest by far,” said judging panellist Robert Mitchell (Park City, USA), before the announcement of HeartEye as the winner of the prize.
Euphrates Vascular, the developer a nano-scale endovascular system to address microvascular occlusion and no reflow, was among those singled out by the judges as being of particular interest. Presenter David Deaton (Medstar Georgetown University Hospital, Washington, DC, USA) told the judges that the Pulse NanoMed device extends the reach of current therapies, and has been given approval to begin a US Food and Drug Administration (FDA) investigational device exemption (IDE) trial in patients with acute ischaemic stroke.
Tilo Kölbel (right) details the Mokita Medical technology
Tilo Kölbel (University of Hamburg, Hamburg, Germany) introduced Mokita Medical, which has developed a technology to address air embolisation during procedures such as thoracic endovascular aneurysm repair (TEVAR) and transcatheter aortic valve implantation (TAVI), a cause of stroke and cognitive decline. The Mokita technology uses a gas soluble fluid to eliminate air from devices, and is being developed into a disposable device that can be connected to the delivery system for a transcatheter procedure. The company is planning a first-in-man study for 2024, and anticipates commercialisation from 2026 onwards.
Mitchell praised Kölbel’s work in this area as being “really important and impactful”, and said that the entry had been one of the strongly considered options for the prize.
Another technology featured in the session included a non-invasive, wearable monitoring system for arteriovenous fistulas (AVFs), intended to aid early identification of failing AVFs. The innovation, presented by Ali Kordzadeh (Anglia Ruskin University, Braintree, United Kingdom) is worn like a wristwatch by patients to monitor venous outflow. Novel device coating materials were also exhibited, with Tony Simula (Mawson Lakes, Australia) detailing Bioinvisible, a drug-free polymer coating that could replace existing drug coatings in devices such as stents, vascular grafts and heart valves.
Several of Interventional News’ most read stories from April covered the topic of interventional oncology (IO)—its interrelation with immuno-oncology, a robot-assisted lung metastases treatment, and articles featuring analysis of current guidelines for cancers in the liver and kidneys. The profile of Theresa Caridi from the latest print issue also grabbed readers’ attention this month, as did three stories focused on peripheral arterial treatments.
AVS, an early-stage medical device company focused on safely and effectively treating severely calcified arterial disease with its pulsatile intravascular lithotripsy (PIVL) therapy, has announced that it closed an additional US$8.8 million in new financing, bringing its Series B round to US$28.8 million total.
A session at the Society of Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA) put the focus on the landscape of interventional radiology (IR) in Latin America and the initiatives that SIR has implemented to strengthen IR worldwide, including in South and Central America.
Antonia Digklia, a specialist in medical and interventional oncology at the Centre hospitalier universitaire de Lausanne (Lausanne, Switzerland) tells Interventional News how recent advances in immuno-oncology are transforming the practice of medical oncology.
A new investigation into the association between end-stage renal disease (ESRD) and major adverse limb events has found that not only is it strong, but ESRD is particularly associated with below-knee amputation.
Surmodics has announced that Ankur Lodha (Cardiovascular Institute of the South, Lafayette, USA) and Pradeep Nair (Cardiovascular Institute of the South, Houma, USA) were the first physicians to use the company’s Sublime radial access microcatheter.
Theresa Caridi is an interventional radiologist based at the University of Alabama at Birmingham (UAB; Birmingham, USA), where she is Interventional Radiology (IR) Division director. She recounts some of the key points on her IR career journey to date for Interventional News.
Surmodics has announced enrolment of the first patient in PROWL, the Pouncethrombectomy system retrospective registry. The Pounce system is indicated for the non-surgical removal of emboli and thrombi in the peripheral arterial vasculature.
Christos Georgiades (Johns Hopkins University, Baltimore, USA), delves into the various national society guidelines for treating renal cell carcinoma (RCC) for Interventional News readers, recommending what he believes is the route to ensuring the best outcomes for patients.
Alessandro Vitale (University of Padua, Padua, Italy) presented current advice and practice concerning bridging colorectal liver metastases (CRLM) to liver transplantation at the European Conference on Interventional Oncology (ECIO; 16–19 April, Stockholm, Sweden).
Xeltis has presented “highly-encouraging” six-month data from its first-in-human (FIH) aXess vascular graft trial at the 13th Congress of the Vascular Access Society (VAS; 27–29 April, Porto, Portugal).
A press release outlines that six-month data from the FIH trial found that the aXess vascular access graft for haemodialysis demonstrated high patency rates (80% primary patency, 95% primary assisted patency, 100% secondary patency). At six months, a 0% infection rate and low re-intervention rates were reported, resulting in a highly favourable safety profile. Haemodialysis was successfully performed through the graft, and compared to current standard of care measures, which typically show lower rates of patency combined with a greater risk of infection or rejection, aXess demonstrated “extremely promising” results.
The full data will be presented by Matteo Tozzi (University of Insubria, Varese, Italy) in a presentation entitled “aXess Vascular Graft—FIH trial 6-month outcomes” at the VAS conference.
Tozzi, who is principal investigator in Xeltis’ FIH clinical trial, said: “These six-month data are very promising in terms of patency and infection rates and suggest that aXess has great potential to be a game-changing alternative to existing vascular access options, which have a number of significant shortcomings. Xeltis’ vascular access implants, which harness the power of the body’s natural healing processes, could play a vital part in significantly improving the lives of patients requiring haemodialysis.”
The aXess FIH trial is a single-arm, non-randomized FIH feasibility study in Europe evaluating the preliminary safety and performance of the aXess graft in subjects who are older than 18 years with end-stage renal disease, and who are deemed unsuitable for fistula creation. Follow-up visits were conducted at regular intervals after initial procedure, with full study follow-up visits to be conducted at five years. The aXess pivotal trial is currently enrolling up to 110 patients across up to 25 sites in nine EU countries.
This study evaluates SELUTION SLR in the treatment of occlusive disease of the superficial femoral artery (SFA) and proximal popliteal artery (PPA) and has been designed to support US Food and Drug Administration (FDA) approval. It follows investigational device exemption (IDE) approval in the US in August 2022. SELUTION SLR is the first and only limus release DEB to receive FDA IDE approval for SFA and PPA indications.
SELUTION4SFA is being conducted in over 30 centres in the US plus an additional 10 centres worldwide. The study will enrol 300 patients, with the aim of demonstrating the superiority of SELUTION SLR over balloon angioplasty (POBA). The primary efficacy endpoint is primary patency of the target lesion at 12 months and the primary safety endpoint is freedom from death at 30 days. Enrolment into the study will be complete by the end of 2023.
“We are excited to introduce the first Sirolimus DEB to US patients, and look forward to a rapid enrolment of this important study”, commented Jay Mathews (Manatee Memorial Hospital, Bradenton, USA), co-principal investigator. “We hope to learn how this technology can potentially benefit patients with complex peripheral arterial disease.”
“We are pleased to be enrolling our third IDE study in US patients, and look forward to the results of these three studies as well as future IDE studies to come”, added Jeffrey B Jump, chairman and CEO of MedAlliance.
SELUTION SLR was awarded CE mark approval for the treatment of coronary artery disease in May 2020. MedAlliance was the first drug-eluting balloon company to receive FDA Breakthrough Designation status. Currently three IDE clinical studies are evaluating SELUTION SLR in the US: in CLTI patients with BTK disease; SFA/PPA; and coronary ISR. In addition, MedAlliance received IDE approval for de novo coronary artery lesions in January 2023. This complements the substantial experience that the company has gained with the SELUTION DeNovo and SUCCESS trials in Europe.
MedAlliance’s unique DEB technology involves MicroReservoirs which contain a combination of biodegradable polymer intermixed with the anti-restenotic drug sirolimus, applied as a coating on the surface of an angioplasty balloon. These MicroReservoirs provide controlled and sustained release of the drug for up to 90 days. MedAlliance’s proprietary CAT (Cell Adherent Technology) enables the MicroReservoirs to be coated onto balloons and efficiently transferred to adhere to the vessel lumen when delivered via expansion of the balloon.
SELUTION SLR is commercially available in Europe, Asia, the Middle East, and the Americas (outside USA) and most other countries where the CE mark is recognised. Over 10,000 units have been used for patient treatments in routine clinical practice or as part of coronary clinical trials.
Teleflex has announced new research findings reinforcing the long-term durability of prostatic urethral lift (PUL) with the UroLift system and lower complication rates compared to other minimally invasive procedures for men with enlarged prostate, also called benign prostatic hyperplasia (BPH). Results were presented at the Annual Meeting of the American Urological Association (AUA; April 28–May 1, Chicago, USA).
“Arriving at the intersection of effective BPH treatment, patient priorities and available technology can be a daunting task,” said Olly Kayes, honorary senior lecturer at the University of Leeds (Leeds, UK) and primary investigator of the PULSAR study. “These new analyses show that the UroLift system offers unique benefits for many men searching for long-term relief of burdensome symptoms affecting their quality of life. The UroLift system can be an excellent option for patients seeking quick and durable symptom improvement with preservation of sexual function and low risk of serious complications.”
Key findings from the studies presented are:
Early treatment prior to severe symptoms positively impacts long-term durability
Pooled outcomes in more than 330 UroLift system subjects treated in a controlled setting were analysed and reported by Claus Roehrborn et al.
PUL with the UroLift system was durable in most subjects at one and five years. 13.7% of subjects needed surgical retreatment at five years, which is consistent with the five-year surgical retreatment rates reported in the LIFT study (13.6%).
Treatment earlier in the disease continuum, indicated by factors such as better overall International Prostate Symptom Score (IPSS) and quality of life (QoL) scores at baseline, facilitates long-term durability.
Earlier intervention in patients with urinary retention increases the likelihood of becoming catheter-independent after treatment
The PULSAR study (n=51), reported by Olly Kayes et al, prospectively examined 12-month outcomes of the UroLift system treatment in subjects with urinary retention. Results were compared to 388 retention patients in the real-world retrospective study.
After treatment with the UroLift system, 73% of controlled study subjects and 80% of real-world study subjects were catheter- and surgery-free at 12 months; success was associated with higher voiding efficiency during the perioperative period.
Variables that influenced success included age under 70 years at procedure, lower baseline prostate-specific antigen (PSA) and post-void residual (PVR) levels, and shorter pre-procedural catheter duration.
These data may help providers to better understand results after the UroLift system procedure and enable more men with urinary retention to obtain safe and effective BPH treatment.
“We are in the midst of a paradigm shift in the BPH landscape,” said Kevin Hardage, president and general manager of Teleflex Interventional Urology. “As clinicians listen to their patients’ goals, technological advances are allowing them to deliver treatments that reflect those priorities better than ever before. The data presented at AUA reinforce the importance of earlier intervention in BPH and the UroLift system as an effective and durable BPH solution that improves patients’ quality of life and supports a superior patient experience.”
Vivasure Medical has announced it has enrolled the first patients in the company’s PerQseal PATCH clinical study, a multicentre, single-arm, pivotal study evaluating the safety and efficacy of the Vivasure PerQseal closure device system. The first patients were enrolled at Kaleida Health’s Buffalo General Medical Center-Gates Vascular Institute by Vijay Iyer, chief of Cardiology at the University of Buffalo and Director, Structural Heart Interventions at Buffalo General Hospital (all Buffalo, USA).
“With the recent proliferation of large bore arterial access, there is a moment at the completion of each procedure when vessel management is critical and clinicians must quickly and effectively close it to reduce unnecessary, potentially life-threatening bleeding,” said William Gray, system chief in the Division of Cardiovascular Disease at Main Line Health and co-director at the Lankenau Heart Institute (both Philadelphia, USA) and the principal investigator for the PerQseal PATCH study. “I look forward to evaluating the PerQseal technology and its simplified, controlled technique—with the ultimate goal of reducing vascular complications for these patients.”
Large hole arterial access is required for clinicians to perform percutaneous cardiovascular procedures, including transcatheter aortic valve replacement (TAVR), thoracic and abdominal endovascular aneurysm repair (TEVAR and EVAR), and the use of a cardiac assist device (CAD). The current approach to large-diameter arterial closure is a surgical repair or the use of suture- or collagen-based closure devices. Both can result in major vascular complications, such as vessel distortion at the closure site, which may lead to stenosis, thrombus formation or abrupt closure.
PerQseal is the first sutureless, fully absorbable synthetic implant for large-bore vessel punctures. It is placed from inside the vessel, making deployment simpler and more controlled than conventional closure techniques, the company claims.
“Large bore closure can be challenging, and PerQseal is a promising technology for interventional cardiologists as a growing number of treatment options for patients utilise fully percutaneous approaches,” said Iyer. “I am honoured to participate in this study and look forward to gathering additional clinical evidence supporting this innovation’s potential benefits.”
Vivasure’s pivotal study will enrol up to 171 patients across the USA and up to 90 patients in up to eight European investigational sites. The data will support a premarket approval submission to the US Food and Drug Administration (FDA).
Endologix has announced the online publication of the final five-year results of the LEOPARD trial in the Journal of Vascular Surgery (JVS). The study’s findings showed that there was no significant difference in aneurysm-related outcomes between patients randomised to the AFX endograft system, with anatomical fixation, and commercially available endografts with proximal fixation.
“The publication of these final five-year results in JVS reinforces the performance of our AFX2 endovascular AAA [abdominal aortic aneurysm] system in the treatment of patients with [AAAs],” said Matt Thompson, president and CEO of Endologix. “We are proud to have conducted the first randomised controlled trial comparing commercially available endografts, and we remain committed to providing the highest quality clinical evidence that underpins our life-changing vascular therapies. Importantly, the comparable performance results from the LEOPARD study between AFX/AFX2 and other endografts align with a recent publication that was authored on behalf of the Society for Vascular Surgery’s Patient Safety Organization and used linked registry claims data.”
LEOPARD was a prospective, randomised, multicentre trial that enrolled 455 patients across 56 US centres. Two hundred and thirty five patients were included in the AFX/AFX2 arm and 220 patients in the comparator arm.
The primary endpoint was freedom from aneurysm-related complications (ARC), a composite endpoint consisting of perioperative death, aneurysm rupture, conversion to open surgical repair, postoperative endoleaks, endograft migration, aneurysm enlargement, endograft limb occlusion, and device- or aneurysm-related reintervention.
The results presented included:
Freedom from ARC at five years was:
63.8% in AFX/ AFX2 device cohort
55.5% in comparator endografts
There was no clinically significant difference in aneurysm-related mortality, all-cause mortality, rupture, secondary interventions, and type 1 and type 3 endoleaks between the two cohorts
The type 3 endoleak rate for the AFX/AFX2 device cohort was 1.5% at five years and was not statistically different from the comparator devices
The type 2 endoleak rate reached a statistically significant lower rate at 21.2% at five years for the AFX2 cohort than the rate of 31.6% seen with the comparator devices
The US Food and Drug Administration (FDA) has granted the third investigational device exemption (IDE) approval for Concept Medical’s MagicTouch sirolimus-coated balloon (SCB). Along with this latest IDE approval for the treatment of small vessels, Concept Medical received two other IDE approvals for the MagicTouch SCB family of products for the treatment of coronary in-stent restenosis and for below-the-knee treatments.
The current IDE approval will allow Concept Medical to initiate a pivotal clinical study to support safety and effectiveness of the MagicTouch SCB in small vessel coronary disease. The data generated from this IDE clinical study will support a future premarket approval (PMA) application in the USA.
MagicTouch SCB is the world’s first SCB with extensive commercial usage in Europe, major markets of Asia, and the Middle East. More than 100,000 patients have been treated with MagicTouch SCB in these markets.
Currently, there are no US FDA-approved drug-coated balloons (DCBS) for the treatment of coronary artery disease in the USA—physicians use drug-eluting stents or uncoated balloons.
MagicTouch SCB has already been widely studied globally in multiple clinical trials, including the EASTBOURNE Registry (2123 patients), NANOLUTE, and ongoing trials like the TRANSFORM 1, TRANSFORM 2, GINGER, TITAN, and Hybrid Bifurcation drug-eluting balloon. Sirolimus has already proven to be safer in coronary artery disease treatment.
Martin Leon, founder and chairman Emeritus, Cardiovascular Research Foundation (New York, USA), who will lead the coming IDE trials, stresses the importance of this achievement. “The US FDA approval to initiate the MAGICAL-SV Clinical trial using the MagicTouch SCB with novel coating technology represents a landmark event in our decades-long quest to find an optimal therapy to manage patients with small vessel coronary obstructive disease. Our US clinical investigators are thrilled and anxious to begin enrolment in close collaboration with the Cardiovascular Research Foundation and Concept Medical.”
Philips has announced the launch of Zenition 10, a new addition to the company’s Zenition mobile C-arm series. Based on Philips’ flat panel detector technology, Zenition 10 helps to expand patient access to routine surgical care and minimally invasive procedures. Now commercially available, the high-image-quality mobile C-arm enables surgeons to treat more patients at a lower cost while helping improve patient outcomes, the company has said in a press release
“Philips Zenition mobile C-arms have long been recognised for their high-quality imaging and efficiency-enhancing performance. With the introduction of Zenition 10, we are making those benefits available on a C-arm that meets the wide-ranging needs of routine open and minimally invasive surgery, allowing more patients in more parts of the world to receive the high-quality care,” said Mark Stoffels, general manager, Image Guided Therapy Systems at Philips.
To help alleviate operating room staff shortages and rising healthcare costs, Philips Zenition 10 provides a cost-effective imaging solution for routine surgery, delivers the speed and efficiency needed to deal with high patient throughput, while being flexible enough to meet the needs of orthopaedics, trauma, and other areas of surgery to maximise utilisation. It comes with exceptional C-arm manoeuverability, application-specific protocols, and personalised user profiles.
Consistent image quality is facilitated by application-specific protocols, customisable presets, and unique user profiles that automatically adjust Zenition 10 settings to suit an individual user’s preferences whenever they log in. An uninterruptible power supply allows the unit to be moved from one operating room to another without the need to reboot the entire system, and its C-arm geometry provides the manoeuverability needed for operating room staff to access target anatomies. Philips BodySmart facilitates dose efficiency by automatically adapting the measuring field to the area of interest.
For images of patients with metal implants, Philips MetalSmart software automatically enhances image quality and dose efficiency, and a dedicated paediatric mode automatically reduces dose rates for young patients. The system’s digital subtraction angiography capability further enhances the range of surgical procedures facilitated by the Zenition 10, allowing clear imaging of vasculatures.
The American Urological Association (AUA), in partnership with the Society of Urologic Oncology (SUO), released the 2023 clinical practice guidelines for the diagnosis and management of non-metastatic upper tract urothelial carcinoma (UTUC). Of key importance is the fact that the recommendation for kidney-sparing treatment in these guidelines is tumour ablation.
UTUC is a rare disease, posing unique challenges to clinical management and significant risks to patients—both from the disease and treatment forms. UTUC is a cancer in either the inner lining of the ureter, calyces, or renal pelvis. While it is not very common, the diagnosis of UTUC of the renal pelvis is associated with a five-year mortality rate of more than 50%, comparatively worse than the less than 25% rate for bladder cancer.
“UTUC requires a specialised approach, and there is a need for updated strategies to help this vulnerable patient population,” said Jonathan Coleman, chair of the guideline panel and surgeon at Memorial Sloan Kettering Cancer Center (New York, USA). “New information and guidelines like these can help improve cancer control and survival. Clinicians will not only learn how to evaluate patients, but they will get the most up-to-date information on treatment, surveillance, survivorship and more.”
This guideline has 38 recommendations and serves as a useful reference on the effective evidence-based diagnosis and management of non-metastatic UTUC.
The contents of the guidelines cover:
Diagnosis and evaluation
Risk stratification
Kidney-sparing management
Surgical management
Lymph node dissection (LND)
Neoadjuvant/adjuvant chemotherapy and immunotherapy
Post-treatment surveillance
Survivorship
Within the section on kidney-sparing management, the guidelines stipulate that “tumour ablation should be the initial management option for patients with low-risk favourable UTUC.
“Tumour ablation may be the initial management option offered to patients with low-risk unfavourable UTUC and select patients with high-risk favourable disease who have low-volume tumours or cannot undergo radical nephrouretectomy,” is a further recommendation included for managing kidney-sparing.
Furthermore, it states that “tumour ablation may be accomplished via a retrograde or antegrade percutaneous approach and repeat endoscopic evaluation should be performed within three months.”
“SUO has been honoured to work alongside the AUA to help develop numerous guidelines in urology,” said Jeffrey Holzbeierlein, president of SUO and vice president and physician-in-chief at the University of Kansas Cancer Center (Kansas City, USA). “We believe it is important to take difficult diagnosis like non-metastatic UTUC and disseminate the most up-to-date information possible.”
During a recent satellite symposium, which took place at the 2022 Cardiovascular Interventional Radiological Society of Europe (CIRSE) annual meeting (10–14 September, Barcelona, Spain), experts emphasised the clinical value of drug-eluting technologies (DET) in peripheral arterial disease (PAD). The speakers, including Marianne Brodmann (Medical University of Graz, Graz, Austria) and Steven Kum (Mount Elizabeth Novena Hospital/Changi General Hospital, Singapore), gave an overview of trial results from Boston Scientific’s DET clinical programme and from independent investigators. Enrolment in these studies will exceed 10,000 patients in over 15 countries.
Brodmann quoted the principal investigators of the EMINENT randomised controlled trial (RCT) who concluded that based on the EMINENT and IMPERIAL RCTs the Eluvia drug-eluting stent (DES) should be considered as the stent of choice for treating the superficial femoral artery (SFA) and/or proximal popliteal arteries of intermediate length. Kum also concluded that despite having more complex patients and longer lesions, the outcomes achieved in real-world registries are consistent with the data found in RCTs.
The power of RCTs
Opening the session, Brodmann delivered a presentation on RCTs for drug-eluting technology in PAD. The speaker first considered the power of randomised data, remarking that—after performance sensing through bench and pilot tests—“properly powered RCTs are essential to prove device performance against current standard of care with clinically meaningful primary endpoints”. After this, she noted, registry data should be used to confirm findings in real-world populations to “complement, not replace” RCTs.
The weight given to RCTs in clinical guidelines highlights their importance, Brodmann told the CIRSE audience, explaining that Level I evidence must be obtained from at least one RCT or from a meta-analysis of RCTs.
The first trial Brodmann mentioned was the COMPARE RCT, which included 414 patients. “This is the first head-to-head trial of drug-coated devices,” the presenter stated, detailing that the trial looked at the Ranger low-dose paclitaxel-coated device (Boston Scientific) versus the IN.PACT high-dose paclitaxel-coated device (Medtronic).
At 12 months, Brodmann reported, the primary endpoint for non-inferiority for a low-dose paclitaxel-coated DCB compared to a high-dose paclitaxel-coated DCB was met, as was the primary endpoint for non-inferiority regarding safety. The presenter added that, in the longer term (out to 790 days), the low-dose device performed as well as the high-dose device.
Brodmann then moved on to the RANGER II SFA Global study—an RCT of 396 patients that compared the Ranger DCB to plain balloon angioplasty. “We once again have good evidence at 12 months with regard to the primary patency*,” the presenter revealed, noting that this was superior to plain balloon angioplasty at a rate of 89.8% compared to 74.0% and was statistically significant.
The primary safety endpoint was also met, Brodmann continued, stating that clinically driven target lesion revascularisation (TLR) in the Ranger DCB arm was only 5.5% compared to 16.5% in the plain balloon arm. At two years, Brodmann communicated that primary patency was also statistically significant in favour of the Ranger DCB, as was freedom from TLR. “Longer-term data are very much needed for DCBs,” she stressed.
Moving on to the next study, Brodmann informed delegates that the head-to-head IMPERIAL study of 465 RCT patients directly compared the Eluvia (Boston Scientific) and the Zilver PTX (Cook Medical) devices. At this point, Brodmann explained that the drug release from the Eluvia system is sustained much longer than the Zilver PTX. At one year, the presenter reported that primary patency for the Eluvia was 86.8% compared to 77.5% for the Zilver PTX—a “statistically significant difference”. There were also statistically fewer TLRs in the Eluvia arm compared to the Zilver PTX arm, Brodmann added.
Finally, Brodmann spoke on the randomised EMINENT trial, which compared the Eluvia stent to a bare nitinol stent in 775patients. “This is the largest randomised trial of DESs for SFA and proximal popliteal arteries reporting patency to date,” she remarked, going on to describe it as a “landmark trial” in this field. Statistically significantly greater primary patency was achieved in patients treated with the Eluvia compared to the bare metal stent, Brodmann noted, adding that there was also sustained primary clinical improvement.
Brodmann quoted the EMINENT RCT principal investigators’ conclusion that, “Based on the EMINENT and IMPERIAL RCTs, the Eluvia DES should be considered as the stent of choice for treating the SFA and/or proximal popliteal arteries of intermediate length.”
Real-world data
Following Brodmann’s presentation, Kum reiterated that the results of these randomised studies “cannot be fully extrapolated to daily practice” and must be complemented by real-world registries.
Kum made this comment during a presentation on real-world patients and drug-eluting technologies, citing the single-centre Münster registry (62 patients), single-centre Auckland registry (51 patients), single-centre DESAFINADO registry (67 patients) and the multicentre Japanese CAPSICUM registry (1,097 patients) as key examples of real-world data on the Eluvia DES.
The 12-month primary patency results in the four registries were 87%, 94%, 84% and 87% and 12-month freedom from TLR rates were 87%, 94%, 92% and 93.8%, respectively, Kum reported. He also concluded that despite having more complex patients and longer lesions, the outcomes achieved in real-world registries are consistent with the data found in randomised clinical trials.
In the final presentation of the symposium, Brodmann gave a progress update on the ELEGANCE registry, underlining first the key issue at the centre of this study: “Despite the high prevalence of PAD in women and under-represented minorities, clinical trials rarely include significant sized cohorts.”
“Given the heterogeneity of PAD patient representation, there is a need to better understand how PAD treatments affect such cohorts,” she added.
The ELEGANCE registry aims to include up to 5,000 patients at up to 100 global study centres, with enrolment targets of 40% women and 40% under-represented minorities. The patients will be treated with drug-eluting devices from Boston Scientific.
Brodmann reported that 634 patients had been enrolled as of September 2022, and that the trial is ahead of its inclusion targets at 42% women and 42% under-represented minorities.
“To make a difference, we need to be different,” Brodmann commented. “ELEGANCE is an excellent example of partnership between industry and physicians as we aim to be a diverse, multi-dimensional source of real-world data in PAD treatment outcomes. By emphasising diversity and inclusion in clinical trial leadership and patient enrolment, we can expand patient representation in PAD trials and improve clinical decision-making and outcomes.”
Closing the session, moderator Gunnar Tepe (Klinikum Rosenheim, Rosenheim, Germany) considered what is next for the space, acknowledging that there are some open questions that need addressing. He referred, for example, to the use of drug-eluting devices in long lesions or in the case of restenosis after DCB. Overall, however, he summarised that, based on the data presented during the symposia, “paclitaxel-coated devices are safe in the SFA”.
A question from Manj Gohel (Cambridge University Hospitals NHS Foundation Trust, Cambridge, UK) on what the Charing Cross (CX) audience should take back to their multidisciplinary team meetings from the first-time presentation of BASIL-2 led chief investigator Andrew Bradbury (University of Birmingham, Birmingham, UK) to deliver the stark message: a patient who needs a below-the-knee revascularisation with or without a femoropopliteal revascularisation is likely to do better if they are treated with a best endovascular-first strategy rather than a vein bypass-first approach.
Click here to read our full coverage of the BASIL-2 results.
Penumbra recently announced the launch of the latest addition to its RED family of catheter devices for mechanical thrombectomy, the RED 43 reperfusion catheter.
According to the company, this device is intended to take distal aspiration “to the next level” with optimised lumen occupation as well as a soft distal design that allows for enhanced and compliant delivery in tortuosity.
With a 0.043-inch lumen, RED 43 provides powerful distal aspiration alongside the Penumbra ENGINE and features REDglide technology for advanced hydrophilic coating for smooth trackability.
As per the company’s website, additional features of this newly launched device include:
A 1.52mm (0.060-inch) outer dimension: low profile and atraumatic design for distal deliverability
Precision tip: articulating marker band with short polymer tip design for optimal visualisation and placement
Full-length polytetrafluoroethylene (PTFE) liner: designed for durability and lumen integrity under powerful aspiration
Proximal hybrid stainless steel and nitinol coil wind: engineered to provide optimal support and softer profile atraumatic navigation
A question from Manj Gohel (Cambridge University Hospitals NHS Foundation Trust, Cambridge, UK) on what the Charing Cross (CX) audience should take back to their multidisciplinary team meetings from the first-time presentation of BASIL-2 led chief investigator Andrew Bradbury (University of Birmingham, Birmingham, UK) to deliver the stark message: a patient who needs a below-the-knee revascularisation with or without a femoropopliteal revascularisation is likely to do better if they are treated with a best endovascular-first strategy rather than a vein bypass-first approach.
In the BASIL-2 (Bypass versus angioplasty for severe ischaemia of the leg) trial of 345 patients with chronic limb-threatening ischaemia (CLTI), a best endovascular treatment-first revascularisation strategy was associated with better amputation-free survival than a vein bypass-first strategy in those who required an infrapopliteal repair—with or without a more proximal infrainguinal procedure. This result was largely driven by fewer deaths in the best endovascular treatment group. Bradbury presented this key finding at the 2023 CX International Symposium (25–27 April, London, UK). The results were simultaneously published in The Lancet.
“It all seems to be pointing towards attempting an endovascular procedure first and then if that does not work, doing something else—which could be more endovascular,” Bradbury said in response to Gohel. Alternatively, he added, this could be the point at which the vascular specialist switches over to a bypass approach. BASIL-2, however, “lends quite a lot of weight” to an endovascular-first revascularisation strategy, “with all the caveats that we have to consider”.
Bradbury, delivering the data for the first time during day one of CX 2023, revealed that 63% of patients randomised to a vein bypass-first strategy of treatment underwent a major amputation or died during follow-up, compared to just 53% of those allotted to a best endovascular-first approach—BASIL-2’s primary outcome measure (adjusted hazard ratio 1.35, 95% confidence interval [CI] 1.02–1.08, p=0.037).
“Essentially this means that, in this cohort, a vein bypass revascularisation strategy resulted in a 35% increased risk of amputation or death during the follow-up compared with a best endovascular-first revascularisation strategy,” Bradbury told the CX audience.
Median survival for the whole cohort was 3.8 years—3.3 years for the vein bypass group and 4.4 for the endovascular arm, he said. “The significant difference we have observed in favour of best endovascular therapy with amputation-free survival is very largely driven by the fact that there were more deaths in the vein bypass group—53% of vein bypass patients and 45% of best endovascular therapy patients,” Bradbury continued. “There is no significant difference of 30-day mortality but you can see that the median survival of the two groups is quite different.”
CLTI is the “severest manifestation” of peripheral arterial disease (PAD) and presents as ischaemic pain at rest or tissue loss, or both, the authors detail in The Lancet. Against this backdrop, Bradbury and colleagues were comparing effectiveness of a vein bypass-first with a best endovascular treatment-first revascularisation strategy in terms of preventing major amputation and death in patients with CLTI.
Roger Greenhalgh
“It is important to emphasise that the best way of analysing this trial, which is the way our statistical colleagues have done it, is on the intention-to-treat population; however, for completeness they have done some sensitivity analyses, and this includes a per protocol analysis, which includes only patients who were adherent—that is, they received the allocated intervention they were randomised to,” Bradbury explained at CX. “They also performed an as-treated analysis, which is based upon the first revascularisation that the patient actually received following randomisation, and as you can see here they both trend towards reduced amputation-free survival in the vein bypass-first group.”
The BASIL-2 co-investigators, namely Catherine Moakes, Gareth Bate and Matthew Popplewell (all University of Birmingham, Birmingham, UK) and Lewis Meecham (University Hospital Cardiff, Cardiff, UK) also presented during the session on the journey from BASIL-1 to BASIL-2, a hypothesis-generating prospective cohort study, methodology, study limitations and future work, among other topics.
BASIL-2 was an open-label, pragmatic, multicentre, phase 3, randomised trial performed at 41 vascular surgery units in three countries: the United Kingdom (n=39), Sweden (n=1) and Denmark (n=1). The central site was the University of Birmingham. “Eligible patients were those who presented to hospital-based vascular surgery units with [CLTI] due to atherosclerotic disease and who required an infrapopliteal, with or without an additional more proximal infrainguinal, revascularisation procedure to restore limb perfusion,” they state in The Lancet.
Bradbury and colleagues randomly assigned participants 1:1 to receive either vein bypass or best endovascular treatment as their first revascularisation procedure through a secure online randomisation system. The Lancet paper details that participants were excluded if they had ischaemic pain or tissue loss considered not to be primarily due to atherosclerotic PAD. Most vein bypasses used the great saphenous vein and originated from the common or superficial femoral arteries, the authors communicate, while most endovascular interventions comprised plain balloon angioplasty with selective use of plain or drug-eluting stents.
Patients were followed up for a minimum of two years, Bradbury et al write, with data collected locally at participating centres. In England, Wales and Sweden, the authors note, centralised databases were used to collect information on amputations and deaths. They add that data were analysed centrally at the Birmingham Clinical Trials Unit.
The primary outcome of amputation-free survival was defined as time to first major (above the ankle) amputation or death from any cause measured in the intention-to-treat population. Safety was assessed by monitoring serious adverse events up to 30 days after first revascularisation.
Between 22 July 2014 and 30 November 2020, the triallists enrolled and randomised 345 patients with CLTI—65 (19%) women and 280 (81%) men with a median age of 72.5 years (62.7–79.3). The patients were randomly assigned to either the vein bypass group (172 [50%]) or the best endovascular treatment group (173 [50%]).
Bradbury detailed at CX that major amputation or death occurred in 108 (63%) of 172 patients in the vein bypass group and 92 (53%) of 173 patients in the best endovascular treatment group. The relevant mortality numbers were 91 (63%) among the vein bypass group and 77 (53%) in the endovascular arm.
In both groups, the authors write, the most common causes of morbidity and death— including that occurring within 30 days of their first revascularisation—were cardiovascular (61 deaths in the vein bypass group and 49 in the best endovascular treatment group) and respiratory events (25 deaths in the vein bypass group and 23 in the best endovascular treatment group). They add that the number of cardiovascular and respiratory deaths were not mutually exclusive.
In the discussion section of their paper, Bradbury et al consider how their findings compare to those from the BEST-CLI trial, which were presented for the first time last November. “At first glance,” they remark, “our results appear to conflict with the BEST-CLI trial”. However, they note that there were “many differences” between the two trials, including the primary endpoint. “Our clinical experience suggests that few patients with [CLTI] are deemed suitable and have an optimal vein for infrapopliteal bypass,” Bradbury and colleagues comment, adding that future work is required to determine whether the patients enrolled in BASIL-2 are more like the patients with a non-optimal vein in the BEST-CLI trial.
During the panel discussion following the BASIL-2 presentations at CX, Andres Schanzer (UMass Memorial Health, Worcester, USA) asked Bradbury and colleagues to cast the findings against the backdrop of BEST-CLI. Moakes, who was the statistician for BASIL-2, explained that the team are planning to conduct an individual patient data meta-analysis to answer questions around any relevant differences between the two trials.
“A trial of two strategies”
Also during the discussion, the panel touched on the evolving landscape of endovascular treatment, with moderator Andrew Holden (Auckland City Hospital, Auckland, New Zealand) asking Bradbury and colleagues whether they had noted a significant change in endovascular practice in the period between BASIL-2 and its eponymous predecessor.
Bradbury noted in his interpretation of the data that “there is a much greater willingness now that if you do an endo[vascular], and you are not happy with it, the interventional radiologists will go back and have another go, whereas what we tended to see, I think, in BASIL-1, was that if endo[vascular] did not work, [treatment would] quickly go over to bypass. I think that is the difference.”
Moderator Dittmar Böckler (Heidelberg University Hospital, Heidelberg, Germany) urged the audience to keep in mind the various options that remain open when undertaking an endovascular-first approach. Greenhalgh underscored the point. “It also came out with BEST-CLI that the quality of the vein is important,” he said. “It is very, very crucial that whatever you do first, it does not have to be the last word.”
Böckler said vascular specialists “need to learn from this trial which patient deserves which treatment”. It is not a case of surgery versus endovascular therapy, but rather a case of learning from the data, he added. Bradbury concurred. “It is a trial of two strategies,” he said. “That was what BASIL-1 was. It is quite a difficult concept to get across. We are not comparing a vein bypass with an endovascular treatment. We are in a sense—but what we are saying is, ‘What do you do first?’ If you have got equipoise, if you are really on the fence, and you do not know which to do, this trial suggests fairly strongly, I would suggest, that in this subgroup of patients, that you should go endo[vascular] first.”
Bentley has bought its main supplier, the Switzerland-based Qmedics, Bentley has recently announced in a press release. It also announced its plan of initial public offering (IPO), which is planned for autumn/winter 2023/2024, depending on market conditions.
Qmedics manufactures approximately 80% of all balloon catheters used in conjunction with Bentley’s covered stents. Bentley, in turn, is responsible for about 70% of the Swiss company’s sales.
The acquisition, which was signed on 21 April and will come into effect on 3 July, will enable Bentley to secure the central supply chain for balloon catheters in the long term. In addition to balloon catheters, Qmedics has a complete portfolio of self-expanding stents for peripheral endovascular procedures. The acquisition of Qmedics thus represents an opportunity for Bentley to accelerate its expansion into the field of interventional radiology (IR).
Anita Patteet, CEO of Qmedics, said—”I am very pleased that the future of Qmedics is in good hands with Bentley. Together, we will certainly be able to celebrate further market successes.”
Sebastian Büchert, CEO at Bentley, said—”With the acquisition of Qmedics, we not only ensure the availability of one of our most important components, but at the same time complete our newly created product portfolio for [IR].”
Bentley’s planned IPO intends to be completed on the Swedish stock exchange, a part of Nasdaq Nordic, an offshoot of the US technology exchange Nasdaq. A Swedish holding company was set up for the upcoming IPO, which is temporarily called BeThundered AB. This holding company becomes 100% owner of both Bentley Innomed GmbH from Hechingen and Qmedics AG, which thus operates as Bentley’s sister company. The pre-IPO, the first step in an IPO, is scheduled for the summer 2023. The actual IPO is
planned for the autumn/winter 2023/2024, depending on market conditions.
Bentley is also launching a €15million employee program to make all of its employees shareholders. Every employee has received a promise to receive shares worth around 400€ (±100€) per month of their affiliation with the company at the time of the IPO.
Büchert explained—“Bentley’s management is very pleased that the previous shareholders have agreed to give the Bentley staff this share gift. Our employees really deserve this for their great work over the past few years.”
Vestibular schwannomas related to neurofibromatosis type 2 (NF2) are difficult to manage and are sometimes treated with a noninvasive option—stereotactic radiosurgery. A retrospective study conducted by an international, multicentre team and reported in Neurosurgery found that stereotactic radiosurgery is effective for patients with these tumours while preserving serviceable hearing and not causing radiation-related tumour development or malignant transformation.
NF2 is a genetic condition that results in the growth of tumours of the brain, spinal cord, and peripheral nerves. A vestibular schwannoma (also known as acoustic neuroma, acoustic neurinoma, or acoustic neurilemoma) develops from the nerves of the inner ear that control balance and hearing. Many people with NF2 develop vestibular schwannomas in both ears that are very difficult to manage, often requiring multiple surgeries and/or other procedures. Vestibular schwannomas can lead to hearing loss, facial weakness or numbness, and in large tumours, compression of cranial nerves and the brainstem leading to weakness, disequilibrium, difficulty swallowing, and hydrocephalus.
To better understand the effectiveness and safety of stereotactic radiosurgery for NF2-related vestibular schwannomas, Hussam Abou-Al-Shaar (University of Pittsburgh Medical Center, Pittsburgh, USA) and colleagues reviewed data on 267 patients (328 vestibular schwannomas) who underwent single-session stereotactic radiosurgery at 12 centres across the world.
The researchers report multiple positive outcomes:
Tumour control likelihood of 77% at 10 years and 52% at 15 years
Likelihood of not requiring additional treatment of 85% at 10 years and 75% at 15 years
Likelihood of preserving serviceable hearing of 64% at five years and 35% at 10 years.
The only significant predictor of tumour progression was tumour volume, with each 1cm3 increase in tumour volume increasing the relative risk of tumor progression by 8%. The tumour progression rate was 48% at 15 years after stereotactic radiosurgery, but only 25% of patients required additional treatment by that time point, suggesting that despite radiographic progression, only half merited treatment.
Significant predictors of loss of serviceable hearing were older age (3% greater risk per year of age after stereotactic radiosurgery) and presence of bilateral vestibular schwannomas (4.56 times greater risk).
Abou-Al-Shaar and colleagues report that during the median 59 months of follow-up, “we did not observe any event of radiation-induced tumour development or NF2-associated vestibular schwannoma malignant transformation.” This has been a concern in patients with NF2 given their underlying propensity to develop tumours. The authors note that despite the benefits of stereotactic radiosurgery and its good safety profile, its use in patients with NF2 “remains an area of controversy and concern among physicians. We hope that the findings of this study address some of these concerns.”
Abou-Al-Shaar’s group concludes that their results point to the need for early treatment of vestibular schwannoma in patients with NF2. “Tumour volume appeared to significantly impact tumour control and freedom from additional treatment, advocating for early stereotactic radiosurgery to maximise benefits and delay clinical deterioration.”
Dimitrios Filippiadis (image credit: CIRSE on demand)
Dimitrios Filippiadis (image credit: CIRSE on demand)
Dimitrios Filippiadis (National and Kapodistrian University of Athens [ATTIKON], Athens, Greece) was the final speaker to take to the podium at the European Conference on Interventional Oncology’s (ECIO; 16–19 April, Stockholm, Sweden) advanced musculoskeletal (MSK) session. His presentation drew on the subtopics within MSK oncology addressed by previous speakers to underline the importance of multidisciplinary collaboration to treat a range of MSK tumours or metastatic disease. Echoing the takeaways of preceding sessions, Filippiadis underlined that, despite the good work already being done to prove the value of a multidisciplinary approach to treating patients with MSK tumours or metastatic disease, gaps in the data persist from a clinical evidence point of view.
“Stating the obvious,” Filippiadis began, he advocated for cancer patients being managed at multidisciplinary tumour board meetings, “ideally with orthopaedic and neurosurgeons, medical and radiation oncologists, and, of course, interventional radiologists”.
The speaker then homed in on the value of shared terminology, and mutual understanding of what keywords mean—in the National Comprehensive Cancer Network (NCCN) 2023 guidelines, in relation to management of pain in adult cancer patients, ‘interdisciplinary’ was replaced by ‘multidisciplinary’, Filippiadis detailed. “We need to have both—to be able to offer a patient-tailored, or, even better, a lesion- or tumour-tailored approach.” The presenter elaborated how “everything in theory seems to work if you can have a multidisciplinary approach, but there are theoretical and practical gaps that we need to fill in”.
Moving on to focus on a location-specific example of where multidisciplinary treatment has worked well, Filippiadis suggested that “we can all agree that [Wallace et al’s paper in The Oncologist on treating metastatic spine disease in a multidisciplinary manner] was a success”. The essence of this, the speaker summarised, is having “therapies proposed from different disciplines”, adding that it “goes without saying that interventional radiology [IR] was at the core of these multidisciplinary approaches”. Filippiadis listed the advantages of IR treatments which render it so well suited to featuring in the multidisciplinary approach—“it is minimally invasive; well tolerated even in patients with comorbidities or extensive disease; the overall morbidity of the procedures is low; and there is impressive and reliable pain relief in the vast majority of cases”.
Furthermore, Filippiadis mentioned, among other examples of specific treatments for specific tumour types, systemic therapies to treat desmoid tumours or sarcoma metastatic disease—it is a “good example of how you can combine with local treatments”.
However, the speaker made sure to note “clear gaps” in knowledge surrounding a multidisciplinary approach to treating MSK tumours or metastatic disease. Yet Filippiadis outlined how data on the immuno-oncological effect of ablation on a tumour, including when combined with immunotherapy, plus the interplay and timing between systemic therapy and MSK oncology interventions and techniques” is coming to “[fill] these gaps”.
Filippiadis then took the opportunity to recommend distinct approaches depending on “whether the goal of your therapy is local tumour control or pain palliation”—the time interval between treatments can be adjusted accordingly. A pain palliation specific knowledge gap, the speaker supplemented, is around “the effect of ablation combined with radiation therapy for pain palliation”. A phase I or II trial for painful skeletal metastases could be a first step, he suggested.
To conclude, Filippiadis reiterated that IR treatments for MSK tumours have a “significant role to play because they are simple and effective [and afford great benefits to practitioners, to the cancer patients and to the wider field of oncology, including the healthcare system and its economics.” As the presenter sees it, he conveyed to delegates, “high-quality data [can] fill in these gaps, [but] the prerequisite for this is that people from different specialties are speaking the same language”.
IceCure, developer of the minimally-invasive cryoablation ProSense System which has shown promise in the treatment of renal masses, has announced that it has been used in a single-site study conducted at the Sorbonne University Department of Interventional Radiology and Oncology, Tenon Hospital in Paris, France by lead investigator François H Cornelis, (Memorial Sloan Kettering Cancer Center, New York, USA) and a team of doctors.
The study, titled “Pain-Free Survival After Percutaneous Image-Guided Cryoablation of Extraperitoneal Endometriosis” was published in the Journal of Vascular and Interventional Radiology (JVIR). The independent study and published paper were not sponsored by IceCure. Cornelis presented the study data at the Society of Interventional Radiology 2023 Annual Scientific Meeting (4–9 March, Phoenix, USA).
Cryoprobes used in the study were of two types: IceCure’s ProSense cryoprobe and Varian’s V-probe. The purpose of the study was to retrospectively evaluate the pain-free survival of percutaneous image-guided cryoablation of symptomatic extraperitoneal endometriosis (EE). In total, 42 patients with 47 lesions were treated. Patients were made aware that cryoablation was offered as a minimally invasive alternative to surgery, and that a surgical procedure may be performed if cryoablation failed. According to the published study, the therapeutic options to avoid the progression of endometriosis and reduce symptoms have been limited thus far to hormonal agents and wide surgical excision. In recent decades, minimally invasive techniques such as cryoablation have been suggested as a promising option to treat abdominal wall endometriosis with satisfactory outcomes and low morbidity.
Based on the following study outcome data, the study concluded that percutaneous cryoablation is a safe and effective procedure that significantly reduces pain and obtains local control of EE. The median follow-up was 13.5 months after cryoablation. The study’s conclusions included:
Efficacy rate of cryoablation to avoid secondary surgery was 92.8% per patient and 93.6% per nodule treated.
Median pain-free survival rates were 93.75% at six months and 82.72% after 12 months, 24 months, and 36 months.
Pain decreased from a median of 8/10 on the visual analogue scale to 0/10 at the last follow-up (p<0.0001).
Four patients had an adverse event in the days following the procedure, while one patient had a severe adverse event.
“We are grateful to Cornelis and the team of doctors at Sorbonne University and Tenon Hospital, where the data was collected, for having used our ProSense system, in addition to those from another company, as part of this independent study. Tenon Hospital institution is highly regarded in the field of interventional radiology,” stated Eyal Shamir, IceCure’s chief executive officer. “The ProSense system has regulatory approval in several countries, including US Food and Drug Administration (FDA) clearance for use as a cryosurgical tool in gynaecology, and we are pleased that doctors now have more evidence of cryoablation’s efficacy in patients with extraperitoneal endometriosis.”
Surmodics has announced enrolment of the first patient in PROWL, the Pouncethrombectomy system retrospective registry. PROWL is an open-label, retrospective, multicentre US registry of the Pounce system for the non-surgical removal of emboli and thrombi in the peripheral arterial vasculature.
The registry will collect real-world efficacy and safety outcomes data for endovascular interventions using the Pounce system for up to 500 patients at up to 30 sites. Sean Lyden, chairman of the Department of Vascular Surgery, Cleveland Clinic (Cleveland, USA) and Joseph Campbell, interventional cardiologist, OhioHealth (Columbus, USA) are national co-principal investigators. The first site to enrol a patient in the registry study was Baton Rouge General Medical Center (Baton Rouge, USA).
“We are delighted to be the first site to enrol a patient in the PROWL registry,” said Joseph Griffin, vascular surgeon at the Vascular Specialty Center and Baton Rouge General Medical Center. “In our experience, the Pounce system promptly removes peripheral arterial clot in a single treatment session while reducing the need for thrombolytic drugs and subsequent intensive care unit stays. We are eager to help track outcomes in this important study.”
“We have long needed better tools to help us resolve acute limb ischaemia in a simple and effective manner, without the use of multiple adjunctive treatments,” he added. “In this respect, our experience with the Pounce system has been quite positive.”
PROWL’s primary efficacy endpoint is procedural success, while the primary safety endpoint is the incidence of device-related major adverse events in the 30 days post-procedure.
“Acute limb ischaemia from arteries blocked by thrombus or embolus is an urgent threat to both limb and life,” said Gary Maharaj, president and CEO of Surmodics. “With hospitals increasingly short on staff and beds, physicians need a simple and effective tool that lets them restore arterial flow right on the table without resorting to time-consuming and costly adjunctive treatments. We are confident the PROWL registry will demonstrate these exceptional attributes of the Pounce system in real-world clinical practice.”
Day two of the European Conference on Interventional Oncology (ECIO; 16–19 April, Stockholm, Sweden) opened with a session dedicated to posing and responding to the most burning questions regarding colorectal cancer (CRC) metastases. Alessandro Vitale (University of Padua, Padua, Italy) presented current advice and practice concerning bridging colorectal liver metastases (CRLM) to liver transplantation.
A “difficult” subject to tackle, Vitale first pointed out that liver transplant has gained new indications in recent years, enumerating “not only HCC [hepatocellular carcinoma],” but perihilar cholangiocarcinoma, liver metastases from neuroendocrine tumours, intrahepatic cholangiocarcinoma, and CRLM as tumours which are now among the tumours for which liver transplant can be indicated. However, Vitale proceeded to note that there is a “low” level of evidence concerning liver transplants for patients with CRLM. “Excluding case reports,” the presenter shared, “the expected long-term outcomes of liver transplants for CRLM [between 1981 and 2023] can be extrapolated from less than 100 cases”.
Data on CRLM—then versus now
He then acknowledged that there are ongoing trials across Europe, including TRANSMET out of France and SOULMATE from Sweden, the results of which are expected shortly. Vitale also mentioned his centre’s MELODIC study, which is among the same group of trials.
Before 2000, Vitale stated that it was only one team out of Vienna, Austria, to have gathered any data on liver transplant for CRLM, but that “history changed about 10 years ago” when the Norway-based Hagness et al published their paper which reported an overall survival rate at five years among 21 patients of 60%. They found “some important prognostic factors,” the speaker added, listing lesion size and progressive disease after chemotherapy among these. At 10 years, this year, Vitale informed the audience that the study had found a 42.9% overall survival rate among the original patient cohort.
In addition, Vitale underlined findings from Maspero et al published in 2023 in Cancers that suggest the main risk factors for poor prognosis post-liver transplant for CRLM patients are related to molecular biomarkers, the presence of extrahepatic disease, the size, number, and progression of the liver metastases, as well as “some parameters” relating to the primary tumour, such as it being right-sided, or it having been resected less than two years before transplant.
With this in mind, Vitale described the ideal CRLM patient candidate for transplant—they are fit, with unresectable CRLM but high tumour burden, without any extrahepatic metastases, and have a left-sided primary CRC.
Potential for expanding transplant offering
Looking to the future, the speaker mused that patients with unresectable CRLM, yet “not good” tumour biology—their disease had progressed on all standard lines of chemotherapy, or patients with single extra-hepatic metastasis—may become candidates for transplant. These patients may face “very poor outcomes” without the transplant, so the potential for benefit with transplant is “very good,” Vitale summarised. “The more interesting future transplant [CRLM] patients,” Vitale went on to say, are those whose metastases are “borderline unresectable.” If the patient is considered “borderline” for poor fitness, the presenter said they would not be good transplant candidates. However, for those who are “borderline” because the surgery would be technically complex or those whose cancer is “highly likely” to recur intrahepatically, a liver transplant may be viable in the future. Furthermore, “patients with a high tumour burden but good [oncologic] biology have an important transplant benefit,” Vitale proffered, referring to a 2021 study published in Transplant International by Lanari et al.
The role of ablation and locoregional therapies
“Ablation, now, is competitive with resection for small lesions,” the speaker averred, homing in on the interventional radiology (IR) side of bridging CRLM patients to transplant. “But there is no evidence on [its] use before liver transplantation,” Vitale lamented. “And the situation is completely different for CRLM compared to HCC,” he added, implying that one cannot directly relate the use of ablation in the latter patients to the former. “Ablation and locoregional therapy play a big role in selection for transplant and bridging to avoid dropout from the waiting list,” Vitale said of the situation with regard to HCC. On the other hand, “only systemic therapy” is used for selection and bridging for CRLM currently due to the high tumour burden in comparison to HCC. This is reflected in the guidelines, the speaker supplemented.
“A potentially important role is possible,” Vitale volunteered, speaking of ablation in bridging CRLM patients to transplant, “only if we extend our indication to initially unresectable patients with a very good response to chemotherapy.” Other potential patient demographics currently not receiving ablation to bridge to transplant are those who are oncologically borderline unresectable or technically borderline, Vitale suggested, as ablation would remove the need for challenging surgery. The same would be true of patients with repeatedly recurring CRLM—“We can choose to ablate,” the speaker asserted.
Concluding, Vitale spoke to the ethical dilemma of increasing the number of liver transplant candidates in countries where demand due to liver disease is already high. He put forward using more cadaveric livers for transplantation than is the case currently as one solution to the donor liver shortfall. On the subject of ablation as a bridge to transplant once more, Vitale conceded that it would become relevant “strictly linked to future indications, namely borderline resectable CRLM,” but with the current indications for transplant, this is not the case. From this perspective, the “transplant radiologist figure will become fundamental in the multidisciplinary evaluation of these patients.”
Surmodics has announced that Ankur Lodha (Cardiovascular Institute of the South, Lafayette, USA) and Pradeep Nair (Cardiovascular Institute of the South, Houma, USA) were the first physicians to use the company’s Sublime radial access microcatheter.
The Sublime microcatheter is in limited market evaluation, a press release notes. The full suite of Sublime microcatheters will be launched in 2024. The Sublime portfolio will include the industry’s first suite of 0.014”, 0.018”, and 0.035” high-performance peripheral microcatheters.
“For peripheral as well as coronary interventions, radial access is safer than femoral access and much preferred by patients,” said Lodha. “I am pleased to report that the Sublime microcatheter performed exceptionally well during our first uses of the device in treating peripheral arterial disease.”
“The lack of long-length, high-performance catheters for peripheral procedures has slowed adoption of radial access for treatment of lower extremity artery disease,” added Nair. “Sublime microcatheters will fill a major gap in the peripheral-intervention toolkit, including for procedures from access sites other than the wrist.”
Available in five lengths from 65 to 200cm and compatible with 0.014”, 0.018”, and 0.035” guidewires, the press release details that the Sublime microcatheters Surmodics’ Pristyne hydrophilic coating for lubricity to optimise device trackability through vessel tortuosity. The device’s dual stainless steel, locked-braid layers work in unison to optimise torque control, push transmission, and deliverability to distal target lesions, the company adds.
The microcatheters are available in straight or angled tip configurations. The Sublime 0.014” and 0.018” microcatheters can be telescoped through the 0.035” Sublime microcatheter to provide additional back up support when navigating extreme tortuosity or heavily stenosed lesions, the press release continues.
“This successful first use of our Sublime microcatheters is a major milestone, not only for Surmodics, but for the countless patients who stand to benefit from peripheral arterial treatment,” said Gary Maharaj, president and CEO of Surmodics. “For years, torqueable microcatheters have enabled coronary operators to overcome the most extreme challenges presented by complex arterial disease. We are pleased to bring this industry-first capability to peripheral interventions.”
GE HealthCare is further advancing its precision care strategy with CT-Navigation, which offers clinicians detailed, real-time, 3D computed tomography (CT) images for stereotactic needle guidance across an array of care areas, including interventional and oncological procedures, as well as biopsies, ablations, drainage, and therapeutics.
Providing highly detailed images of internal structures such as bones, organs, and tumours, CT-guided interventions can assist clinicians in performing minimally invasive procedures that guide stereotactic needles through the anatomy to biopsy or deliver treatment directly to affected tissue. As a result, interventionalists benefit from greater visibility and confidence in needle placement, while patients benefit from more accurate and precise care.
“Consistent and accurate navigation through the body is key in delivering precision care,” explained Laura Crocetti, associate professor of Radiology, Division of Interventional Radiology, University of Pisa (Pisa, Italy) and deputy chairperson of the European Conference on Interventional Oncology (ECIO). “CT-Navigation is an intuitive technology that helps us achieve this by enabling clinicians to select and follow an out-of-plane trajectory for a safer path that avoids critical organs and reaches deep-located targets with impressive accuracy, while reducing procedure time and possibly radiation dose. All together, it helps us ensure better patient outcomes while expanding the boundaries of our practice.”
CT-Navigation enables a more comfortable and safe experience than some of the alternative solutions. Instead of working wholly within the CT system’s narrow bore, interventionalists using CT-Navigation can place a sensor on the patient inside the gantry. After scans are complete and the patient is removed from inside the system, interventionalists have full range of motion while navigating a needle more easily and safely through the patient’s anatomy using the placed sensor and detailed CT images.
CT-Navigation was developed by IMACTIS and became part of the GE HealthCare portfolio of solutions upon close of the previously announced acquisition of the France-based company.
The GE HealthCare system, which includes a mobile workstation, guidance software, and disposable procedure kit, is approved under the European Union’s Medical Devices Regulation (MDR) and has US Food and Drug Administration clearance for use within the USA.
BlackSwan Vascular, a privately held company that is developing innovative therapies in endovascular embolization, is has announced it has received US Food and Drug Administration (FDA) Premarket Approval (PMA) of its Lava Liquid Embolic System (Lava LES) for treatment of peripheral arterial haemorrhage.
Lava LES—a non-adhesive injectable—is the first liquid embolic product approved by the FDA for use in the peripheral vasculature and is specifically indicated for embolization of peripheral arterial haemorrhages. Liquid embolic agents, which are injected as a liquid and solidify after entering the vasculature, are used to treat a variety of conditions.
“Lava LES was purpose-built to provide interventional radiologists with an important tool to rapidly address challenging active arterial bleeds, including gastrointestinal bleeding and bleeding from trauma,” says BlackSwan CEO Suresh Pai. “Arterial bleeds frequently present in an emergent setting and can be life-threatening. We are delighted to bring this important technology to fruition to safely and effectively treat these patients.”
Premarket approval was granted based on clinical evaluation of Lava LES in a prospective, multicentre, single-arm study (the “LAVA study”) evaluating safety and efficacy in acute peripheral arterial haemorrhages. The study utilised composite outcomes as a measure of safety, documenting the percentage of cases that were free from major adverse events within a 30-day period following treatment. Effectiveness was determined by the percentage of cases that were clinically successful, with no bleeding from the target lesion after embolization with the Lava LES, and no need for emergency surgery, re-embolization, or other target lesion reinterventions within 30 days of the index procedure. Results of the study, which followed 113 patients at 20 centres demonstrated safety and efficacy outcomes that exceeded the pre-established performance goals of the study.
“Lava LES has been optimised for use in the peripheral circulation” based on viscosity, radiopacity, and volume, explains Mahmood K Razavi (Vascular & Interventional Specialists of Orange County, Orange, USA). As co-principal investigator of the LAVA study, Razavi presented the study findings at the 2023 Society of Interventional Radiologists Annual Meeting (SIR, 4–9 March, Phoenix, USA). “The study confirms that there are clear advantages to liquid embolics in peripheral applications,” he says. With this approval, “practitioners can be trained to use this highly effective form of embolization, to the benefit of patients.”
Lava LES was developed by BlackSwan, leveraging the infrastructure, resources and ISO 13485 and FDA QSR compliant quality systems of LamaMed, a med-tech venture studio with a successful track record of capital-efficient product development from concept to commercialisation.
Two of the sessions from day one of the 2023 European Conference on Interventional Oncology (ECIO; 16–19 April, Stockholm, Sweden) drew delegates’ focus to what the evidence in interventional oncology (IO) and immuno-oncology is indicating in 2023. Specifically, hepatocellular carcinoma (HCC) featured as the subject of presentations—the promise of locoregional and immunotherapy in tandem for advanced HCC among them. On the immuno-oncology side, the audience was privy to an examination of the potential role IO can play in treating oligoprogression and oligoresistance.
A key takeaway from the presentations in question was that there will always be a need to consider different types of tumour and different patients in different ways—homogeneity will not yield desired outcomes—and therefore, the continued pursuit for more evidence is crucial.
Bruno Sangro (Clínica Universidad de Navarra, Madrid, Spain) was among the speakers who addressed advanced HCC evidence, beginning by outlining that “one of the main reasons why, twenty years ago, we were doing locoregional therapies for everyone, even for patients with metastases [is that] we had nothing else to offer patients with advanced tumours”. Sangro then turned to address combining locoregional therapies with immunotherapy: “We have two drug combinations that are able, no question, to improve the survival of patients in the advanced stage. We started from a point where we were able to improve survival for the majority of patients—when it comes to three-year survival rate, we were able to get 15–20% of patients alive at that time. Now these figures have doubled.”
The benefit of checkpoint inhibitors
A discovery that changed the field, according to Sangro, were checkpoints inhibitors—”unlike with tyrosine kinase inhibitors (TKIs), these treatments can induce responses irrespective of tumour location or burden, [whether] small tumours, large tumours, [those] invading the portal vein, metastases. The most important point is that patients who respond, have a very prolonged survival.” Expanding further on his experience, Sangro shared that “when we looked at checkpoint inhibitors versus TKIs as a first-line therapy, consistently we were able to see that single agents were able to increase the number of long-term survivals but were not able to significantly improve the overall survival of the population”.
The promise of systemic therapy
Sangro went on to explain that “because of the success of immunotherapy in the advanced stage, more patients in earlier stages of the disease are reaching systemic therapy [and are] no longer kept on repeated locoregional therapies. Now, all poor candidates for selective transarterial chemoembolization (TACE) or transarterial radioembolization (TARE) are being moved onto systemic therapies, increasing their survival.” This led Sangro to underline what one of the key messages from his presentation is—overall, the survival of patients treated with systemic therapy is improving. This improvement, the speaker supplemented, is seen in tolerability, and in terms of patient-reported outcomes, including quality of life. The next step, Sangro stated, is to make the most of “the opportunity to test whether [systemic therapy] improves the outcomes and survival for other earlier [HCC] stages”.
Providing a counterpoint, the presenter pointed to other tumour types, and the fact that where there are good systemic therapies for patients with these, this also “has to be translated into early-and intermediate-stage patients otherwise, as it happened with TKIs, it would not be the kind of systemic therapies we would like to have.” This was echoed in the question and answer session that followed Lambros Tselikas’ (Institut Gustave Roussy, Villejuif, France) presentation by Antonia Digklia (Centre hospitalier universitaire de Lausanne, Lausanne, Switzerland), who emphasised to the audience the importance of focusing on each tumour subject across IO.
Distinguishing oligoresistance from oligoprogression
Tselikas began his presentation by defining oligoresistance, which means that “you only have control of some of the lesions”. Some lesions may also have primary resistance to immunotherapies, Tselikas elaborated—even though it is the same disease, it is a different immune microenvironment surrounding the different tumours. Oligoprogression, in distinction is when some of the multiple lesions “regrow or recur in other places”. This, therefore, constitutes secondary resistance, which is a “completely different scenario”.
Whether a patient’s cancer is oligoresistant or oligoprogressive can “impact on the results you expect,” Tselikas averred, explaining that in the case of the former, “you hope to be curative”. However, with the latter, “you delay the resistance, and it can last for a while”.
The question of how and whether to treat
The next question is then how you treat the two types of oligometastases. In the case of oligoresistance, there is some evidence of ablation and radiation’s efficacy, but “this can be variable,” Tselikas acknowledged. In the case of oligoprogressive lesions that follow initial treatment, the presenter expressed doubts as to whether there is benefit to treating them, from an increased toxicity point of view. “We do not really know if there is any added value in local treatments [for these lesions], such as ablation, or radiation therapy,” Tselikas added, while pointing out that “oligoprogression under immunotherapy is quite rare, [but] it is very frequent under TKIs”.
The speaker went on to share his experience from his centre, where they have had eight patients over last 10 years who were treated with immunotherapies and received ablation treatment. “We have both [oligo]resistant and progressive,” Tselikas informed delegates—some [received] cryoablation, some radiofrequency ablation, and some microwave, and safety is perfect”. Regarding efficacy, the presenter observed better results for the patients with an oligoresistance profile, he shared.
Concluding, Tselikas noted the importance of “real-time, easy-to-obtain biomarkers […] for those to whom we can offer local treatments”. This will facilitate the idea that “IO can help immuno-oncology to help overcome these oligoresistance and oligoprogressive patterns,” as Tselikas sees it.
The study is coordinated by Thierry de Baere (Gustave Roussy, Villejuif, France) and will evaluate the clinical performance and safety of the Epione device for the treatment of these tumours.
Epione is a robotic platform capable of assisting interventional radiologists in planning and performing minimally invasive procedures for the percutaneous ablation of tumours in the abdomen. Available in France and the USA, the Epione robot has already been used in procedures on more than 150 patients with liver or kidney cancer. With this study, Quantum Surgical aims to obtain an extension of its marketing authorisations in Europe and the USA with an indication extended to the treatment of lung tumours.
“This study sets a new milestone in the development of Quantum Surgical, and I am proud that it is being done in collaboration with Gustave Roussy, whose teams see the full potential of our technology. This is another step towards the dissemination of our innovation to other cancer patients”, said Bertin Nahum, president and co-founder of Quantum Surgical.
Christos Georgiades (Johns Hopkins University, Baltimore, USA), delves into the various national society guidelines for treating renal cell carcinoma (RCC), what the ‘gold standard’ of treatment is currently considered to be, and what he believes is the route to ensuring the best outcomes for patients.
The answer to the question of “where do we stand on cryoablation for stage 1A RCC?” can best be found by deploying the ultimate litmus test. Ask those who treat RCC what they would choose for themselves if their life depended on it. And in the case of RCC, it would. I would not be going out on a particularly long limb if I presumed to answer for them—“cryoablation”. This, however, may not satisfy the data-driven, or more accurately, data-dominated decision-makers. So, let us look at the ‘guidelines’. With or without qualifications, all major relevant associations—the National Comprehensive Cancer Network, American Urological Association (AUA), European Association of Urology (EAU), Society of Interventional Radiology (SIR), and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE)—include ablation as a treatment option for stage 1A RCC. The guidelines worth exploring a bit deeper, however, are those from the American Society of Clinical Oncology, which recommends ablation for stage 1A RCC “if a complete ablation can be achieved”.
The wisdom of this last statement is that it gets to the heart of an important issue. Implicitly, it brings up the crucial factor for good oncologic outcomes—operator experience. While no study addresses this issue rigorously, there is a common understanding among interventional radiologists and urologists on “where we currently stand”—for stage 1A RCC, an experienced interventional radiologist will deliver the same oncologic outcomes as an experienced surgeon. Yet, admittedly, this is not the case everywhere. Many places, especially community settings, lack experienced interventional radiologists. But then again, the same holds true for surgeons experienced in partial nephrectomy, the current ‘gold standard’ of treatment. Which brings us to the second part of the question—“where are we going?”
Twenty years ago, partial nephrectomy was the new ‘gold standard’ for treating stage 1A RCC. Yet, due to the unavailability of experienced surgeons, nearly 54% of patients had radical nephrectomy, which led to them unnecessarily losing a lot of healthy nephrons. Today, after a 20-year push for nephron-sparing options, the situation is not much better, with about 42% of patients with stage 1A RCC still receiving radical nephrectomy. What a disappointment! More relevantly, while 3% of such patients were treated with ablation 20 years ago, today, and despite the evolving guidelines, only 12% are. One could very well argue we are going nowhere. But at the same time, it ought to be clear where we should be going. If we are truly committed to patient care, our collective efforts should be focused towards offering all stage 1A RCC patients a nephron-sparing option, whichever one that may be.
The practical solution is neither easy nor obvious. The most feasible and logical answer seems to be the setup and promotion of regional centres that provide these nephron-sparing options—small, incentivised groups of interventional radiologists and urologists working together to offer nephron-sparing options to their respective population parcel. A committed effort by the AUA/EAU and SIR/Society of Interventional Oncology (SIO)/CIRSE/European Society of Interventional Oncology (ECIO) would indeed have tremendous benefits for patients, many of whom would be spared short-term complications and, importantly, potential renal failure and the need for chronic renal replacement treatment.
In closing, reading between the (guide)lines, one appreciates the essence of them can be distilled down to the oncological equivalence of ablation and surgery for stage 1A RCC. This is provided that interventional radiologists possess the necessary expertise to maintain published oncological outcomes. More crucially, however, the question “where are we going?” reveals a failing, an opportunity, and a challenge to interventional radiologists and urologists—make nephron-sparing options available to the nearly-50% of stage 1A RCC patients who unnecessarily undergo radical nephrectomy.
Christos Georgiades is professor of vascular and interventional radiology at Johns Hopkins University. Georgiades is a consultant for Boston Scientific.
Adept Medical has launched the Adducted Arm Scoop—an improved solution for supporting the adducted arms of supine patients during image-guided procedures.
Adept’s new, “extremely durable” Adducted Arm Scoops are purpose-designed, providing security and comfort on narrow imaging tables, as per a press release.
Moulded with gentle, curved edging to reduce the likelihood of pressure injury and improve handling, the ergonomic design allows patients to comfortably rest their arms at their side with assurance. The ideal height, extending just above the arm, allows access and ease of cable and line management during procedures, Adept also claims.
“After 10 years developing solutions for interventional cardiology/radiology teams, listening to their needs, and observing how they care for their patients, it became obvious that existing arm supports could be improved immensely,” said Mike Oxborough, lead product designer at Adept. “Typically made from folded plastic sheet, they appeared to have very little thought put into design and were almost an afterthought, which is strange given they are an essential component for achieving patient comfort and safety on narrow imaging tables.
“Common complaints from nurses and MRTs [medical response teams] were that the arm boards would crack or break too easily, were expensive to replace, or were simply too flexible to support the heavy arms of larger patients. Improving durability was key, so selecting a material with superior chemical resistance was critical to prevent stress-cracks resulting from exposure to disinfectants used between patients.
“We wanted to create a product that would be more rigid, more durable, would look and feel like it had been designed for the job, and could be purchased for the same price or less than existing boards. With the Adept Medical Adducted Arm Scoop, we have achieved that.”
The Adducted Arm Scoops are quick and easy to install, according to the release. They simply slide under the mattress and are secured by the patient’s weight. Designed for use with existing lab and imaging equipment, they are compatible with any magnetic resonance (MR), computed tomography (CT) or C-Arm imaging tables.
Tanzanian faculty and staff with visiting faculty and students from Emory, University Hospitals Cleveland, Duke, Michigan, MSKCC, USC, UVA, and Yale in front of Muhimbili National Hospital in Dar es Salaam, Tanzania.
Fabian M Laage Gaupp is assistant professor of radiology and biomedical imaging at Yale School of Medicine (New Haven, USA) and a recipient of the Yale Institute for Global Health’s winter 2023 Spark Awards. This monetary prize will see Laage Gaupp and his team at Road2IR make frequent trips to Uganda to help set up the country’s first interventional radiology (IR) training programme—based on the sub-Saharan region’s very first, which the organisation established in Tanzania in 2018. Laage Gaupp, who is one of Road2IR’s founding members, speaks to Interventional News about the challenges of growing IR in sub-Saharan Africa and the impact Road2IR’s work to date has had on healthcare in this region.
What prompted the foundation of Road2IR? Why were you so keen to dedicate yourself to this outreach work?
Road2IR started as a WhatsApp group in 2017 when I first visited Tanzania with my friend and mentor Dr Frank Minja, who is himself a neuroradiologist, originally from Tanzania. During that visit, I met three peers in Tanzania, who were in their second year of radiology residency at the time—Drs Azza Naif, Erick Mbuguje, and Ivan Rukundo. Together, we assessed the current status of IR in Tanzania—it was non-existent. We came up with the goal of establishing an IR service and training programme in Tanzania, which would make it the first and, at the time, only, IR training programme in all of sub-Saharan Africa (a region with over one billion people). In October 2018, we started doing a two-week teaching trip to Tanzania every month. Another year later, Muhimbili University of Health and Allied Sciences (Dar es Salaam), the university affiliated with Muhimbili National Hospital, where Azza, Erick, and Ivan were training in diagnostic radiology, started a two-year Masters of Science course in IR. Those three enrolled as the first trainees and graduated in September 2021. We have come a long way, with several thousand procedures performed, 10 interventional radiologists graduated (eight from Tanzania, one from Rwanda, and one from Nigeria), and growing demand and procedure numbers. The reason why I do this is because I see the extreme demand for IR in Tanzania and sub-Saharan Africa overall and I know that we can have immense impact, even with relatively limited resources. All the advantages IR provides in countries like the USA are even more pronounced in sub-Saharan Africa, where surgical and anaesthesia complication rates are often higher.
How did the COVID-19 pandemic impact your work over in Tanzania? In spite of this, what has Road2IR achieved since its inception in 2018?
The COVID-19 pandemic only halted our progress for about six months (March until October 2020). We decided early on that we could not justify stopping an entire service line and training programme because of a viral disease with relatively low mortality. At the time, the IR service in Tanzania was already saving lives every day, so stopping it was not an option. We resumed our monthly teaching trips in November 2020, and have done at least one trip per month since. This is in contrast to many other global health organisations, who seemed to remain in a state of paralysis until recently. We graduated the first class of three fellows in 2021, the second class of seven in 2022, and are about to graduate the third class of three in August 2023. The reason why the second class was so large is that several Tanzanians, who were supposed to do IR training in China, got kicked out of the country when the pandemic started, and we took them into the programme in Tanzania. This should serve as a cautionary tale for countries relying on China and other nations to train their physicians. The safest way is always to train in-country and every country should aim to have at least one IR training programme of its own.
What are the challenges associated with trying to help establish IR services in a less economically developed part of the world?
Our main challenge has always been, and remains, disposable equipment. This is an obvious problem, since there was never any demand and, therefore, nobody to supply equipment. Now that demand is growing, we are trying to convince equipment companies supplying this part of the world. So far, some companies have been eager to expand their market to sub-Saharan Africa, while others, not so much. This probably depends on their overall strategy, their willingness to take risk, and their size—some companies can barely keep up with demand in the USA. That being said, I do think it is important that companies make an effort to supply their products to sub-Saharan Africa. The demand is huge and we as IR physicians cannot do our work without equipment. If Western companies do not act, Chinese and Indian companies will certainly take the market. Tanzania is an example of how quickly a supply chain can be established—we can get a company’s entire device catalogue approved in a week by the Tanzanian health authorities, who have been supportive collaborators with us throughout the process. All we need is for companies to be open-minded.
Evaluating a patient for nephrostomy tube placement, Muhumbili National Hospital, Dar es Salaam, Tanzania.
How was the Road2IR open letter to the World Health Organisation (WHO) in 2021 received?
To be honest, I have no idea. WHO never responded. Prior to the letter, we have reached out to WHO for several years. At one point, we had a Zoom call with some of their radiology and surgery leadership and discussed extensive plans and suggestions. After that, they never followed up and it went nowhere. Sadly, I think that WHO has no real understanding or appreciation of what IR is and how much impact it could have in resource-limited settings. I am hoping that with a growing body of evidence on IR in these settings, WHO will take note. We could greatly benefit from their support, but IR is still not a focus for global health, unfortunately.
What are your immediate plans for putting the Spark Award funding to use?
I will travel to Tanzania and Uganda every few months in the coming year to help set up the partner programme in Uganda. We are essentially creating a copy of the Tanzania programme, but now have the advantage of having a regional partner programme in Tanzania. This means that we will not only have visiting teams going to Uganda from Europe and the USA, but also from Tanzania. This should help the Uganda programme evolve even more quickly and robustly. I am really excited for the next year and I am hopeful that, by 2024, we can do most basic IR procedures in Uganda and, by 2025 or 2026, we will be able to do most complex procedures there. In addition, Ivan Rukundo is now back in his homeland Rwanda and has started the first IR service in this country of 10 million. He is getting over 100 phone calls from referring physicians a day! As you can see, demand for IR is high everywhere, and we are trying to reach the goal set by the Society of African Interventional Radiology and Endovascular Therapy (SAFIRE) of at least one interventional radiologist per million people. This means we need at least 60 in Tanzania, at least 40 in Uganda, and at least 10 in Rwanda.
Further discussion: IR societies and funding awards
Probed further on SAFIRE’s role in expanding IR coverage in sub-Saharan Africa, Laage Gaupp states how it is a very new society, having had its first official meeting in 2021 in Cape Town, South Africa. Nonetheless, he asserts his belief that there is “lots of promise and potential” as far as the society’s work is concerned. Laage Gaupp suggests that SAFIRE plans to set up a continental examination board to allow for uniform IR training standards.
Regarding the continued work of Road2IR, the Spark Award is one of several funding sources that the organisation has secured, Laage Gaupp avers. For example, it has recently received £25,000 from the UK’s Academy of Medical Sciences, but in order to continue to gain much-needed financial backing, Laage Gaupp stipulates the need to tailor funding applications to the promise of solving disease-specific problems, as opposed to a larger gap in procedural medicine.
Recent advances in immuno-oncology are transforming the practice of medical oncology. Currently, antibodies directed against negative regulators of T-cell function, the so-called checkpoint inhibitors, oncolytic virus, and engineered cell therapies such as chimeric antigen receptor (CAR)-T products have received market approval in treating more than 16 types of haematological and solid malignancies and two tissue-agnostic cancer indications including tumours with microsatellite instability (dMMR/MSI-H) and high tumour mutation burden (TMB).
In 2022, the first randomised phase III trial of adoptive cell therapy with tumour-infiltrating lymphocyte (TIL) treatment was presented. This trial was led by The Netherlands Cancer Institute in collaboration with the National Center for Cancer Immune Therapy in Copenhagen, Denmark and compared the ex vivo modified patient’s own immune cells versus ipilimumab alone in patients with stage IV melanoma. TIL treatment led to a significant progression-free survival benefit of four months (seven versus three months) and in 20% of patients, the metastases disappeared completely (vs. 7% in the ipilimumab arm). Although the comparator arm is not the current standard of care (ipilimumab plus nivolumab) and the data are immature for evaluating overall survival benefit, authors reported a difference in two-year survival of 10% (54.4% vs. 44.1%).
Reprogramming patient or donor T-cells that are designed to express chimeric antigen receptors on their surface (the so-called CAR-T cell) to recognise and target specific tumour-associated antigens has revolutionised haematologic malignancies such as leukaemia and lymphoma, leading to six approved CAR-T cell treatments since 2017. Several clinical trials are underway focusing on this type of therapy option for solid tumours. A recent phase I trial of CAR-T cell and mRNA vaccine targeting carcinoembryonic antigen claudin 6 (CLDN6) in solid tumours that expressing this protein showed a highly impressive objective response rate of 57% and a disease control rate up to 85% in patients with testicular cancer.
Since 2021, two bispecific antibodies, a new form of immunotherapy, have been approved for the treatment of advanced uveal melanoma (Kimmtrak) and metastatic non–small cell lung cancer with certain EGFR mutations (Rybrevant). These antibodies bind onto two specific proteins—one on the surface of the cancer cell and one on the T-cell. Thus, they bring the two cells closer together, allowing the T-cell to better recognise and kill the cancer cell.
Although personalised immunotherapy is an obvious strategy to pursue, its high cost as well as frequent serious toxicities, including cytokine-release syndrome, make them not applicable to all cancer patients. Combining immune therapies with other types of treatment—such as chemotherapy, targeted therapy, radiotherapy, and interventional radiology—many of which are standard of care, can provide additional benefit, as has been shown in several trials. Finally, it is increasingly obvious that other characteristics of the host including sex, microbiome, obesity, and smoking play a role in inducing different responses in immunotherapies.
For the future, the challenge remains—learn how we can identify the patients who will respond to current immune-based cancer therapies and increase the rate of durable clinical responses.
Antonia Digklia is a specialist in medical and interventional oncology at the Centre hospitalier universitaire de Lausanne (Lausanne, Switzerland).
At the Society of Interventional Oncology (SIO) annual scientific meeting (19–23 January, Washington DC, USA), Sean Tutton (University of California San Diego Health, San Diego, USA) presented evidence on treatment for musculoskeletal (MSK) metastases, while urging those involved in these patients’ care, as well as collecting data on their experiences, to “harmonise the nomenclature” they use to optimise data and care quality.
Tutton began by suggesting that a reason for inconsistent terminology where bone cancer treatment is concerned, among interventional radiologists, is that it is a “young” part of the interventional radiology (IR) space. “We need to start talking about skeletal-related events—both the cancer as well as the cancer therapies are having a significant impact on the skeleton,” he urged. An example of why this issue is relevant for interventional radiologists, which Tutton gave, was that of a post-menopausal patient who, after chemotherapy, underwent “an 8% year-on-year bone loss”. This increases the risk of fracture, the speaker underlined.
Moving on to focus on pelvic metastases specifically, the presenter noted that they are the second most common type of skeletal metastasis after spinal. In Tutton’s view, it is crucial to understand that patients with cancer metastatic to the pelvis may experience different types of pain—mechanical pain is not the same as bone-tumour interface pain, which, in turn, is not the same as neuropathic pain. “We address them differently,” Tutton emphasised.
Likewise, there are different classifications of disease stage depending on the type of skeletal metastasis. In the pelvis, the Harrington scale runs from one to four, with complete pelvic discontinuity at the end of the gradation, Tutton informed delegates. Treatment for these metastases differs based on the classification—Harrington 1 is “ablation alone”, 2 is a combination of ablation and osteoplasty, and for profound Harrington 3 and 4, the preferred treatment modality is “osteosynthesis, which is a combination of cement and screws,” the presenter outlined.
Tutton proceeded to run through the biomechanics behind using cement and screws, stating that he and IR and orthopaedic colleagues had seen in their experience that using screws alone is “very similar to not treating at all”. While “cement alone only deals with compressive forces”—and the pelvis also has to be able to deal with “bending, sharing and tortional forces,” Tutton detailed—cement and screws work in conjunction with one another to “shift the load-bearing away from the bad bone to the good bone”. He supplemented this by saying that “the key concept is that you are fixing bicortically if possible”. With the two materials combined, you achieve “the highest stiffness and greatest yield strength”. A further point Tutton made was regarding working with orthopaedic colleagues and how there, uniform nomenclature is key.
The speaker was keen to highlight that the cement plus screw combination is for progressive disease, with Nick Kurup and Matt Callstrom having reported on their experience with Harrington 1 and 2 lesions. Tutton labelled their use of balloon-assist osteoplasty and ablation as a “very novel way of dealing with periacetabular lesions”.
Regarding the body of data that exists within IR for treating skeletal metastases, Tutton acknowledged that there are “a lot of great retrospective data,” which help interventional radiologists build their “toolbox” and stipulate how to use cone beam computed tomography (CT), how to plot navigation lines and how to improve accuracy.
Speaking on his and colleagues’ experience, Tutton averred that the aforementioned pelvic procedures are “safe”, with no significant blood loss or infection reported. Following treatment, the patients he studied saw an improvement in terms of function and narcotic use. At one-year follow-up, the presenter shared that they were able to obtain “good data” on 42 of 105 participants—“we are in the process of reporting,” Tutton told attendees.
“The value” of studies like his is that “as we treat these patients and they survive, which is great […] 43% will need some form of additional procedure—you are going to need to see these folks [again],” was one of Tutton’s main messages for the audience. In order to add to their value, he opined that there needs to be, again, “harmonisation” of the outcome metrics, patient-reported and otherwise, “so that when we publish we all speak the same language”.
In conclusion, Tutton expressed how patients living longer with pelvic metastases is a “huge win”, but that in order to give them the best possible quality of life, it is necessary to continue along “the right track” that IR is on with evidence surrounding osteosynthesis. “Skeletal metastases are common and devastating for quality of life,” so harmonised evidence reporting and use of nomenclature will contribute to “[allowing patients] to continue their cancer therapies and to get walking and actually enjoying life”.
Nima Kokabi (Emory Healthcare, Atlanta, USA) addressed the “uncomfortable truth” of healthcare disparities in the USA specifically within interventional radiology (IR) in a presentation at the Society of Interventional Radiology 2023 annual scientific meeting (4–9 March, Phoenix, USA). He referenced a Journal of Interventional Radiology (JVIR) publication from 2022 to share with delegates the extent of the disparities at play within IR, before putting forward suggestions as to why IR care is as unequally received as it is in the USA, and what interventional radiologists can and should be doing to redress the imbalance.
‘Unequal Treatment’ is a 2003 US Institute of Medicine report on implicit bias and racial disparities in medicine in the USA, that Kokabi began by highlighting. The presenter lamented the fact that the reality of implicit bias and healthcare disparities has not changed as much as one might have hoped in the 20 years since the report was published. In Kokabi’s view, it contains “uncomfortable truths” that he believes all healthcare providers should have awareness of. A key point from the report, he went on, is that “although Black people are disproportionately [affected] by poverty […] that alone cannot explain why they are sicker and have shorter lives compared to their white counterparts”. What is more, “even if they have the same income, age, and severity of condition”, this is still the case. “The lower quality of healthcare is down to us as physicians,” Kokabi opined.
Beyond healthcare more widely, Kokabi then drew audience attention to a recent JVIR article that dissects the disparities that exist within IR in the USA. The article examines the unequal treatment that members of minority groups receive across different disease areas, but Kokabi chose to home in on those most relevant to his practice—these included uterine interventions and hepatocellular carcinoma (HCC). “If you are Black, you are two to three times more likely to undergo hysterectomy for fibroids [over embolization],” Kokabi relayed, adding that those in the Hispanic and rural-dwelling communities also experience a “significantly higher rate” of hysterectomy. This is further exacerbated if you are Black and live rurally, Kokabi shared. When it comes to postpartum haemorrhage, the same phenomenon occurs, according to the article—the aforementioned communities have a higher likelihood of hysterectomy as opposed to embolization, with “Asians suffering from the same trend,” Kokabi said.
In terms of HCC treatment, the presenter then conveyed, “if you are Black or Hispanic, even adjusting for tumour stage, you are less likely to receive any treatment”. In addition, Black, Native American, and Hispanic patients are less likely to undergo certain IR procedures, such as transarterial chemoembolization (TACE) and thermal ablation. Black patients with HCC also have a lower survival rate, which, Kokabi explained, is due to “more fragmented care, lower screening rates, and less access to treatment”.
The disparities extend beyond race, the JVIR article details, to patients of a less favourable socioeconomic background. Those with non-private medical insurance are “less likely to receive IR treatments”.
Regarding finding solutions to the disparities present in IR care, the article recommends “identifying and understanding the underlying causes” first. “If you are a realist or pessimist like myself, you know that finding solutions is very difficult […] it is hard to intervene and be successful,” Kokabi lamented. “One thing that we could all do better with is implicit bias and we are lying to ourselves if we say we are not affected by it.” The presenter urged delegates to seek out implicit bias training, which, in his experience is “very eye-opening—you realise things that you may not have thought you do subconsciously”.
Equally, Kokabi advocated for “[trying] to learn about those who you have biases towards” and then “[engaging] in dialogue with them”. He sees it as “the least we can do [to] reduce the gap [in IR service access],” the reasons for which he sees as being multifactorial. Kokabi suggested that “a lack of uniform access” to IR services in the USA is at play, as well as a lack of understanding from healthcare leaders and insurance companies of the value of IR, which creates inequalities in access. “We are not working hard enough,” were Kokabi’s concluding words, encouraging interventional radiologists to “do a better job” of promoting what IR can offer patients of all demographics.
A session at the recent Society of Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA) put the focus on the landscape of interventional radiology (IR) in Latin America. Members from the affiliate societies Sociedad Iberoamericana de Intervencionismo (SIDI), which is region-wide and the Brazilian Sociedade Brasileira de Radiologia Intervencionista e Cirurgia Endovascular (SOBRICE) took to the podium to speak about IR in their respective countries, and SIR’s International Division councillor Constantinos Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA) shared with delegates the initiatives that SIR has implemented to strengthen IR worldwide, including in South and Central America.
“Our main goal is to empower interventional radiologists, wherever they are, wherever they practise,” Sofocleous stated, including strengthening local IR societies under that umbrella. “Hopefully we are able to create targeted training programmes,” he expressed, as well as “increasing awareness of IR not only among referral services, but also patients”. Citing an example of an SIR initiative geared towards fulfilling these goals, Sofocleous spoke about the Give Back Project, from which Latin America has benefited in the past. “We approve a project that an affiliate society has identified as an important programme for their country, in a specific disease or field,” the speaker explained. “In partnership with SIR, certain faculty members will go and create a programme for the local population, with local faculty.” An example of this project’s work was the symposium on uterine fibroid embolization in September 2019 in El Salvador, Sofocleous shared, labelling it a “great success” that “needs to be replicated […] now we are post-pandemic”.
In addition, Sofocleous listed the “exciting” SIR International Scholar Programme, which takes place every year to provide “outreach to young people interested in IR”. These efforts, alongside others from SIR, will help “raise our voice at a governmental level”, Sofocleous concluded.
Another speaker in the session was SOBRICE President Gustavo Pipoca Andrade (Hospital da Restauração, Recife, Brazil), who walked the audience through the current state of Brazilian IR, before highlighting the challenges his country faces when it comes to improving recognition of the role it can play in healthcare. “We have 24 [IR training] centres certified by SOBRICE,” Andrade relayed, emphasising that this homogenisation of the qualification took place in 2002. In terms of numbers of practising interventional radiologists, the speaker admitted that there is “a long way to go” in Brazil—they comprise only 3% of radiologists.
Regional differences make for “completely different realities” in terms of healthcare, Andrade went on to underline—under 10% of those living in the north of Brazil have private health insurance, whereas in the wealthier southeast region, for example, this figure is over 30%. Showing the audience a heatmap of interventions performed across the country, Andrade demonstrated these are concentrated in the higher-population areas, with the number of training centres distributed accordingly too.
“As a society we have tried to introduce IR everywhere in Brazil,” Andrade asserted. “We have almost everything—yttrium [Y]90, reversible electroporation, hybrid suites—much like the USA”. Yet, awareness of IR is not as good as it could be, he admitted. With this in mind, SOBRICE has launched several campaigns to improve understanding of IR procedures. These include holding social media livestreams during which patients can ask interventional radiologists questions and an annual course for medical students. Andrade homed in on the importance of helping students understand that IR is more than “stopping bleeding or treating a tumour”.
The speaker proceeded to clarify that “in Brazil, we do have industry—we produce wires, catheters, sheaths, coils, filters, stents, and prostheses.” There is also a SOBRICE-published, Portuguese-language collection of IR textbooks available to interventional radiologists and trainees, Andrade added, before leaving the audience with the fact that “finally, in the big centres, we are established as a clinical service, but beyond the big centres, we are not known yet and that is the biggest challenge”.
“My interest in understanding and tackling health disparities has grown while here in Alabama as I have become increasingly aware of the imbalance of opportunities for patients in this state.” Theresa Caridi is an interventional radiologist based at the University of Alabama at Birmingham (UAB; Birmingham, USA), where she is Interventional Radiology (IR) Division director. Caridi’s career has also seen her practise across the USA, take on roles which have included the chair of the Society of Interventional Radiology (SIR) Foundation Board of Directors (2022–23), and has now led her, as a passionate patient advocate, to make the move away from academic IR into a principal industry position. She recounts some of the key points on her IR career journey to date for Interventional News.
What attracted you to a career in IR?
Some individuals know exactly what they want to do from the start, but I was not one of those people. I was fascinated by general surgery, but the environment was not ideal at the time I was a student. I was very fortunate to have the benefit of my dad’s perspective—he highlighted for me all those who were switching from surgery into IR and diagnostic radiology (DR). There really was not the reverse happening—nobody switched from radiology into surgery—which I found very telling.
I did a rotation in radiology, and I loved it, including the diagnostic component. It was so fascinating to piece the whole puzzle together for the teams in the hospital. I ultimately attended radiology residency and when I rotated through IR, I loved the ability to combine what I valued in diagnostic work with a procedural solution. I was fascinated by taking care of complex diseases through tiny incisions and sending patients home the same day with very few side-effects. It spoke to me that we could significantly impact someone’s health and healthcare in such a positive way. It could not be more at the forefront of medicine and ideal patient care.
Who were your mentors?
There have been many who have been pillars along my path—mentors, sponsors, and champions. I think it is important to have a variety of mentors of varying career stage, gender, and geography. I always want at least one strong critic who will have the difficult conversations. I am particularly grateful to Jim Benenati, Jim Spies, Cheri Canon, Frank Facchini, David Hahn, and too many peer mentors to count, including, but not limited to, many of the women in IR leadership. Now, I have mentees that began working with me as students and are graduating and becoming peer mentors themselves. Each reference point has its own value.
Credits: NB Illustration/Andy Watt
Could you describe a particularly memorable case of yours?
I was on call while 38–39 weeks pregnant with my second of three children. I was called in overnight for biliary sepsis in a patient with a bile leak needing diversion. The biliary system was non-dilated. My fellow at the time performed a single blind stick into a peripheral biliary duct. When we saw how tiny it was, I hip-checked him and moved my big belly over to first operator for the remainder of the case. I was so far from the table because of my term belly (I ended up having a 9lbs, 1 ounce bundle of joy) that we laughed quite a bit watching me in action. Fortunately, all went smoothly!
How does being associate professor of obstetrics and gynaecology (ob/gyn) complement being an IR? What led you to pursue both specialties?
I appreciate having a secondary appointment in ob/gyn. At the minimum, it is a symbol of the collaboration we have with our ob/gyn colleagues at UAB. They have truly met us in the middle where we have treatment overlap. It has been a phenomenal experience for me and I feel it has added a lot of value to a truly comprehensive women’s health practice in IR.
What was it that earned you the 2022 Brewer-Heslin Award for Professionalism in Medicine?
The Brewer-Heslin Award recognises those who exhibit excellence in patient care and is named for the late Alabama Governor Albert P Brewer, and Martin Heslin, a long-time UAB surgeon leader. Brewer made the gift for the endowment in appreciation of the professionalism he observed and admired in Heslin, who had been his surgeon. I was unaware of the nomination for this—it was all done behind the scenes— until I was notified of my award by the dean. As I understand it, my nomination was based on efforts made to create a comprehensive clinical IR service with a focus on quality and improving health disparities. It was really special to accept the award at the white coat ceremony. It is truly a reflection of great mentors, sponsors, champions, and a hard-working team.
“It is my goal to stay true to my purpose and show other women in IR that this path is possible!”
How is practice in Alabama different to practising in Washington DC where you were based before coming to UAB?
The practice is very different in that UAB is a larger organisation with a much bigger catchment area. There is no patient population that we do not treat. My individual practice areas have been heavily supported by colleagues in ob/gyn, urology, and surgery, and I think that has a lot to do with tremendous leaders who have shown a true sense of collaboration.
My interest in understanding and tackling health disparities has grown while here in Alabama as I have become increasingly aware of the imbalance of opportunities for patients in this state. There are so many individuals and organisations doing good work here to bridge these gaps, including our team, which has looked at disparities in fibroid treatments and interventional oncology therapies.
Your father, James G Caridi is a posthumous recipient of an SIR Gold Medal this year—what is it like being a second-generation interventional radiologist? Are there any downsides to it as well as the obvious positives?
Being second-generation to someone like my father is all an upside. Dad believed in helping others, even if in a small way. This made him beloved as a physician and patient advocate, which was only enhanced by his own personal diagnosis. I love that I learned so much about being a patient advocate from him.
Where being a second-generation IR is challenging is similar, I would imagine, as in any career – in the stages of defining yourself, your path, and your individual impact. It is been many years since I have felt that burden. Dad and I had a tremendous mutual respect for one another’s careers and allowed plenty of space between our paths.
What inspired a pivot from a purely academic career to a role in industry? Are there other women in IR who have done this?
I have partnered a fair amount with industry as an individual and via national society work. I have always felt that we need strong industry colleagues and physicians to partner to provide the best products for our patients. Our corporate partners have incredible minds and resources. I think we need to continue to align and have patient-centred voices in leadership within these corporate entities. I admire the companies who are seeking this physician perspective. It was a very difficult decision to pivot away from academia and a traditional IR practice, but I feel it absolutely suits where I am in my career. I have an opportunity for a major stretch— to understand the corporate world, while bringing the physician/patient voice, and all the while, get to continue to have a clinical IR practice. I am thrilled and filled with gratitude to have this opportunity.
I am unaware of other women in IR that have truly worked as a leader in the medical device world. I am amongst amazing male colleagues as I make this pivot, many of whom gave me guidance as I considered this decision. It is my goal to stay true to my purpose and show other women in IR that this path is possible!
What are your hobbies and interests outside of medicine?
I take pride in being a partner to my husband Reggie and a mother of three children (Corinne who is eight years old, Jude, five, and Giuliana, two). I love nothing more than to fill the bellies of loved ones with food from my kitchen (my staple is preparing Italian food, as this is my heritage). Breaking bread with friends and family is the best. A perfect day for me involves exercise, scenic views, time with my family, cooking and sharing wonderful food, and reading (on a chill day) or seeing live entertainment—maybe a concert, Broadway musical, or a ballet—on a more elaborate day.
Consultant interventional radiologist Damian Mullan (The Christie NHS Foundation Trust, Manchester, UK) speaks to Interventional News about his experiences with Merit Medical’s Temno Elite™ biopsy system at his hospital, the largest single-site cancer centre in Europe. Among the benefits of using the product for cancerous and non-cancerous soft tissue biopsies alike, Mullan emphasises its ability to yield a larger and less fragmented sample with better macroscopic and microscopic visibility compared to other biopsy needles. This advantage is complemented by the intuitiveness of the design, allowing even those using the system for the first time to do so while reaping the benefits of the Temno Elite’s “unique” features.
Mullan first outlines the obstacles that he and colleagues have historically faced when it comes to carrying out soft tissue biopsies. “Our main challenge is getting a sufficient volume of tissue to satisfy needs for histological diagnosis, for clinical trials and for tissue banking. A good-quality sample is vital, as every biopsy has inherent risks, and you do not want to repeat a biopsy simply because the sample is insufficient despite accurate biopsy placement. The Temno Elite enables the clinician to take a good-quality sample first time, and in a safe manner for the patient”, according to Mullan.
Moving on to speak on the key features Temno Elite boasts, Mullan mentions the “cored-out” bevel, which “produces up to a 72% larger sample1 than previous side-notch needle systems. This can provide a similar bulk of tissue with fewer biopsy passes or allow confidence that a smaller gauge biopsy will give you a similar bulk of tissue to current needle systems. You now do not have to upsize your needle and puncture hole to get a better quality sample,” he underlines.
In addition, he explains how the sample assist feature is key to allowing delivery of a non-fragmented sample to your histopathologist. “It allows you to atraumatically slide the biopsy sample off the bevel, avoiding having to scrape it off with a scalpel or swirl in formalin, and this avoids fragmentation. A non-fragmented sample is crucial for liver and renal biopsy where you are looking for a continuous piece of tissue to ascertain the number of continuous portal triads or the ratio of glomeruli to fibrosis.” In combination, he summarises, these two features aid the diagnostic yield when sampling, for cancer and non-cancer patients alike. He adds: “It is visually and microscopically better and appears as if you are getting a sample from a traditional forward-cutting needle—they are good, solid cores.”
Ease of use is a further consideration that the Temno Elite accounts for, Mullan avers, dubbing it “very intuitive”. This is in contradistinction, he notes, to “some other needle systems, which, if you handed to a colleague with no experience of that system, they would find it difficult to understand how to load and fire the system until they had used it 10 or 20 times. However, if you hand over a Temno Elite, it is a case of ‘point-and-click biopsy’, it is ergonomic intuition.” Mullan describes the new system overall, in this regard, as “a nice, stepwise evolution of the previous Temno systems. You do not need instruction or repetition to become immediately familiar with it”.
Temno Elite
Regarding the safety profile, Mullan refers to unique advantages offered by the Temno Elite. Lung biopsy, specifically, is “a procedure that can carry significant morbidity.” There are well recognised risks of pneumothorax and haemothorax, and the rare, but very serious, risk of air embolism, which can be fatal. There can be a certain amount of stress to the operator because you are cognisant of those risks, so having the confidence of using a system that is designed to prevent some of these risks is very reassuring,” he conveys.
“Lung biopsies can be technically challenging if you are a single operator, as you will perform the biopsy, and then perform a little ‘dance’ around the sample pot, either plugging the Coaxial Introducer with one finger, or resheathing with the Introducer stylet needle, all whist trying to simultaneously get the sample into a pot by any means necessary. The Temno Elite valved Coaxial Introducer has a one-way valve mechanism which means you have the luxury of knowing that you are not going to get air ingress or an air embolism, or any bleeding to the outside, during transfer of biopsy specimen into a sample pot. The one-way valve could also, theoretically, reduce the track bleeding which is an inevitable consequence of inserting and removing the biopsy needle—as the blood is not going to egress, and is more likely to form a clot within the biopsy site,” Mullan posits.
“[IT] produces up to a 72% larger sample than previous side-notch needle systems.”
“This all makes for a much less stressful procedure because you have confidence that you are not rushing through [it]. The Temno Elite lends itself nicely to how you should want to do a procedure, which is in a controlled, concise, methodical and safe fashion.” Mullan follows this up by stating that the Temno Elite is geared towards use for multiple types of biopsy, with a range of gauge and length options. “The quality of the sample and the size means that it is relatable to any biopsy, [not only lung and liver] because you will get a better quality sample than with traditional flat-cutting bevel needles. It is an evolution of previous needle systems, so it is not too different, just better. Across the board, whether for renal, peritoneal, [or others], it does seem to give a better sample.”
On the topic of testing, Mullan proceeds to share his experience—“we have performed bench-side tests, ex vivo, with a calf’s liver to assess the number of portal triads, and it did give us a significant increase in the number compared to older flat-cutting bevel systems.” In theory and in practice, “fragmentation is significantly less with the Temno Elite system”.
Commenting on real-life use, Mullan explains how the cored-out bevel does make the needle tip slightly more prone to bending and distortion (in comparison to a flat bevelled needle), but “only if you are aggressive with manipulation in tissue. One would argue that any biopsy should be precise and targeted, avoiding excess torque and aggressive manipulation.”
Concluding, Mullan provides anecdotal evidence, proving that the Temno Elite “tells its own story” when it comes to the advantages it bestows upon the operator. Recently, when going to take the needle system off the shelf in preparation for a biopsy procedure, he discovered that he had used up the stock of Temno Elite faster than expected and was waiting for new Temno Elite stock inventory to arrive—“I was really disappointed to not be able to use it, and genuinely very frustrated that I did not have the needle to hand. It is so intuitive, that once you start using it and seeing the better sample that it gives you, it becomes difficult not to use it.”
DISCLAIMER:Before using any product, refer to the instructions for use2 (IFU) for indications, contraindications, warnings, precautions, and directions for use. Temno Elite Biopsy System is intended for use in obtaining biopsies from soft tissues such as liver, kidney, breast, prostate, spleen, lung, lymph nodes, thyroid, and various soft tissue masses. It is not intended for use in bone. The valved Coaxial Introducer needle and standard Coaxial Introducer needles are intended for use as guiding needle in obtaining core biopsy samples from soft tissue such as liver, kidney, prostate, spleen, lung, lymph nodes, thyroid, and various soft tissue masses. It is not intended for use in bone.
Justin Guan is an interventional radiologist practising at the Cleveland Clinic (Cleveland, USA), who is also involved in the Society of Interventional Radiology’s (SIR) International Division. He and other members of the division are currently conducting a survey of interventional radiologists and interventional radiology (IR) trainees worldwide with the goal of better understanding the challenges and priorities in IR internationally. Guan took some time to speak to Interventional News about his reasons for getting involved in the global-facing side of SIR, why the survey is so important, and what he and colleagues working on it hope the results will yield for IR and its patients in the not-too-distant future.
How did you get involved in the survey and how did it come to be?
I was born in China and my family moved to the USA when I was seven, so I have always been exposed to different countries’ perspectives and travelled to different places. So I am really interested in the international relations aspect of my work, helping to develop international cooperation. This Global Trainee Network that I am heading was a new subcommittee created under the International Division [of SIR] and our chancellor Dr Constantinos Sofocleous. We had started working on this project under Dr Brian Stainken a few years back when he was the chancellor, and this year, we finally got it approved by SIR to be distributed internationally.
What are the goals of the survey? What questions is it asking?
The main goal is to understand what IR training and practice is like throughout the world, as we do not have much data on what it is like in most countries. Once we have these gaps in the data filled, our hope is that we will be able to better direct resources to areas where we feel these will make the most impact—helping to create training programmes, provide continuing medical education resources, or imaging/procedural devices, for instance. We will also know how to direct different companies and players within industry who can provide the tools for this. Another goal is being able to increase awareness of IR among patients across the world.
The survey includes questions like ‘where do you practice?’; ‘does your centre offer training?’; ‘what sort of procedures do you do?’; and ‘what are the main factors preventing expansion of IR in your region?’
What is the plan in terms of a practical response in places where the survey shows there is most demand for outreach or collaboration to improve and expand IR services?
We do not quite have the infrastructure in place at this moment to send delegations to regions where there is most need, but we could set up industry partnerships to do that. We could potentially create exchange programmes like the SIR delegation that went to Central America a few years back, and there are groups such as Road2IR who are currently setting up training programmes in sub-Saharan Africa. We want data on the state of IR services as is, so we know how to develop initiatives going forward.
Do you foresee SIR collaborating with other societies to implement a training provision-focused response to the survey data?
We could, and definitely should, have intersociety collaboration to fill in the gaps once we have the data on where there is IR training and where there is not. On the trainees side, there is already the IR Juniors global summit, initially set up by trainees in the UK and Middle East, which is flourishing. We just had the third annual summit, which was sponsored by SIR this year. Trainees from different societies came together to discuss what IR is about and the potential is for it going into the future. We will continue this collaboration going forward.
How are you intending to share the data from the survey?
We are going to summarise the data in an article, hopefully by the end of the year. The plan is to have the data collected and ready by late summer. Depending on what we find, there is scope to have additional projects in the works focusing on specific areas of IR practice, for example.
To take part in the short ‘Global assessment of the status of IR’ survey, go to the following link—https://www.surveymonkey.com/r/JYPVZKJ—or scan the QR code.
Example of histotripsy technology targeting kidney tissue.
Histotripsy technology targeting kidney tissue
HistoSonics has announced the first kidney patient has been treated using its histotripsy platform. The procedure was performed at the Leeds Teaching Hospitals NHS Trust (Leeds, UK) by Tze Min Wah, senior consultant radiologist and clinical lead for interventional oncology programme. This procedure marks the initial treatment in the HistoSonics-sponsored CAIN trial, which is a Phase I prospective, multicentre study designed to evaluate the safety and technical success of the company’s histotripsy system in targeting and destroying primary solid renal tumours without the need for incisions or needles.
“This first treatment is a significant milestone for the company as it represents expansion into our second active clinical application (after liver) and supports our mission to deliver histotripsy to patients who may potentially benefit from its unique capabilities,” commented Mike Blue, president, and CEO of HistoSonics. Blue added, “our goal is to enable physicians to precisely target and destroy kidney tumours with our novel, non-invasive solution, avoiding the morbidity and complications seen with current invasive surgery or ablative techniques.”
Current kidney therapies such as partial nephrectomy and thermal ablation are invasive and exhibit complications from bleeding and infection that non-invasive histotripsy may avoid. While surgical intervention is the “gold standard” in removing kidney tumours, a non-invasive approach with histotripsy provides the potential to destroy targeted tissue without damaging non-targeted kidney tissue. Additionally, histotripsy’s purely mechanical mechanism of cellular destruction could preserve function of the kidney’s urine-collecting system and eliminate certain complications seen with existing invasive approaches.
Wah commented—”I was delighted to lead the clinical team in carrying out this world’s first kidney tumour treatment using histotripsy and a real privilege to have the trust of the patient and their family in translating this innovative technology into our clinic. The CAIN trial represents a significant milestone for treatment of solid renal tumours with histotripsy as a needle-less technology and is a paradigm shift from this point onwards.”
HistoSonics’ image-guided sonic beam therapy system uses advanced imaging and proprietary sensing technology to deliver non-invasive, personalised treatments with precision and control. The science of histotripsy uses focused sound energy to produce controlled acoustic cavitation that mechanically destroys and liquifies targeted tissue at subcellular levels. The company believes that the novel mechanism of action of their proprietary technology provides significant advantages to patients, including the ability of the treatment site to recover and resorb quickly. Uniquely, the HistoSonics’ platform also provides physicians the ability to monitor the destruction of tissue under continuous real-time visualisation and control, unlike any modality that exists today.
HistoSonics histotripsy systems are not currently available for sale, HistoSonics advises.
AVS, an early-stage medical device company focused on safely and effectively treating severely calcified arterial disease with its pulsatile intravascular lithotripsy (PIVL) therapy, has announced that it closed an additional US$8.8 million in new financing, bringing its Series B round to US$28.8 million total.
A press release reports that the funding will continue to support clinical trials for the company’s device for PIVL in peripheral cases, while advancing preclinical work for an expanded indication in coronary cases.
“We are pleased to see the investor excitement around this technology,” said Mark Toland, chairman of the board for AVS. “Intravascular lithotripsy represents an emerging therapy that demands new solutions for patients with severely calcified arterial disease. With the support of our partners, we can continue our work toward US approval for both peripheral and coronary applications.”
AVS notes that it successfully enrolled, treated and collected positive 30-day follow-up with patients in a first-in-human study, the POWER PAD I clinical trial, in September 2022. The prospective, single-arm, multicentre feasibility study is evaluating the technical and clinical success of the Pulse IVL system for treating patients with calcific femoropopliteal arteries.
The Pulse IVL system is a novel, balloon-based platform that expands calcified lesions by gently shattering calcium with pressure waves in frequent bursts, all through a single device, a press release details.
BioStar Capital, an investor in transformational medical technologies, led the Series B financing with CUE Growth Partners, a private equity firm focused on healthcare.
“AVS’s technology has demonstrated promise in treating peripheral arterial disease and we are excited to play a role in future trials in the coronary space,” said Louis Cannon, founder and senior managing partner of BioStar Capital. “We have supported AVS through both of its funding rounds because we firmly believe in the company’s potential to improve the options available to patients and ultimately drive improved health outcomes for patients.”
“Cardiovascular disease remains the leading cause of death globally and requires continued investment in novel technologies,” said Ben Cannon, co-founder and partner at CUE Growth Partners. “We are committed to supporting medical devices, such as the Pulse IVL system, that can impact areas of need in medicine through innovative new solutions.”
Interventional News’ most popular stories from March included those covering new embolization and radiofrequency ablation data presented at the Society of Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA); news of the launches of a new peripheral intravascular lithotripsy (IVL) catheter and steerable microcatheter; and the receipt of US Food and Drug Administration (FDA) premarket approval for a new covered stent to be used to treat iliac artery occlusions.
Large bore mechanical thrombectomy with the FlowTriever system (Inari Medical) in patients with high-risk pulmonary embolism (PE) was associated with a significantly lower occurrence of meaningful in-hospital adverse clinical outcomes compared to other contemporary treatments.
The final results of the RAVI prospective registry study demonstrated the safety and efficacy of radial access in visceral interventions in standard embolization procedures for uterine fibroids, benign prostatic hyperplasia, and hypervascular tumours.
Genicular nerve radiofrequency ablation is a minimally invasive treatment for knee pain due to osteoarthritis of the knee, and can significantly reduce pain, especially for adults who are 50 and older, according to new research.
Prostate artery embolization (PAE) provides long-term effectiveness in treating urinary symptoms from an enlarged prostate gland, according to new research presented at the SIR annual scientific meeting.
Results of a recent bariatric arterial embolization study at show that the procedure was associated with “significant” weight loss that did not affect muscle mass, as detected by whole-body magnetic resonance imaging anthropometry.
In a first-in-human, compassionate use case approved by the US Food and Drug Administration (FDA), radiologists David M Williams and Minhaj S Khaja successfully used VeinWay’s Traversa for venous recanalisation to save a patient’s leg that was close to being amputated.
Merit Medical has announced the expansion of its SwiftNinja steerable microcatheter product line. New sizes include a low-profile 2.4Fr distal diameter option in 125-cm and new longer 150-cm lengths.
Argon Medical introduces the Traveler portal vein access series. The product line is designed to meet the needs of physicians accessing the portal vein through the liver during transjugular intrahepatic portosystemic shunt procedures.
Getinge’s iCast covered stent system has received premarket approval from the US FDA for the treatment of patients with iliac arterial occlusive disease.
A new investigation into the association between end-stage renal disease (ESRD) and major adverse limb events (MALEs) has found that not only is it strong, but ESRD is particularly associated with below-knee amputation. The details of the study were presented at the Society of Interventional Radiology (SIR) Annual Scientific Meeting (4–9 March, Phoenix, USA).
The authors, led by Yonatan Babore (Perelman School of Medicine at the University of Pennsylvania, Philadelphia, USA), state in their abstract that their focus was on uncovering the likelihood of MALEs and amputation with ESRD specifically in chronic limb-threatening ischaemia (CLTI) patients who were undergoing percutaneous vascular intervention (PVI) for their condition. They therefore designed a study in which they performed propensity score matching with the data from two contemporaneous cohorts, both of whom were undergoing PVI for symptomatic CLTI. The data was gathered from 2012 to 2022, and the cohorts were differentiated by ESRD status.
The database used included 628 patients, who underwent 1,297 lower extremity revascularisation procedures. These were then matched to 147 patients. Outcomes from procedures on 180 limbs were considered in total—90 limbs for each group—while both Kaplan-Meier and Cox proportional hazard analyses were performed with the data, intended to examine the effect of the presence of ESRD on the probability of MALEs. MALEs themselves were stratified into reintervention, meaning PVI or bypass surgery, as well as major amputation. This latter category was subdivided into above-knee amputation and below-knee amputation.
Babore et al found that, following a PVI procedure, 31.3% of patients in the matched cohorts experienced a MALE. Among those experiencing ESRD, 45.7% experienced a MALE while only 18.2% of those without ESRD did so. On major amputation, patients without ESRD experienced an event at a rate of 5.2%, while those with the condition did so at the higher rate of 27.1%. The proportional hazard analysis, the authors outline, found that ESRD “was an independent predictor of MALE” (hazard ratio [HR] 3.15; 95%, confidence interval [CI] 1.58–6.29; p ¼ 0.001), major amputation (HR 7.00; 95% CI 2.06–23.79; p ¼ 0.002), and below-knee amputation (HR 7.56; 95% CI 1.71–33.50; p ¼ 0.008).
Summarising the findings, the authors state that ESRD is “strongly predictive” of both MALE and major amputation for CLTI patients who are receiving PVI procedures, and particularly so in the case of below-knee amputation. Finally, they look forward, calling for more research: “These patients warrant closer follow-up, and new methods may become necessary to predict and further reduce their amputation risk.”
The publication confirmed an amputation-free survival rate of 66% at six months, which exceeded the trial’s primary endpoint target of 54%, as reported by co-principal investigator Daniel Clair (Vanderbilt University, Nashville, USA) at the 2022 Vascular Interventional Advances (VIVA) meeting (31 October–3 November, Las Vegas, USA).
PROMISE II—multicentre, prospective and single-arm—included 105 patients with CLTI. The pool bore a median age of 70, 33 (31.4%) were women and 45 (42.8%) were Black, Hispanic, or Latino.
Transcatheter arterialisation of the deep veins was performed successfully in 104 patients (99.0%), the researchers report in NEJM. At six months, 66.1% of the patients had amputation-free survival. “Limb salvage (avoidance of above-ankle amputation) was attained in 67 patients (76.0% by Kaplan–Meier analysis),” they write. “Wounds were completely healed in 16 of 63 patients (25%) and were in the process of healing in 32 of 63 patients (51%). No unanticipated device-related adverse events were reported.”
Patients enrolled in PROMISE II “were representative of real-world patients,” including those with dialysis-dependent chronic kidney disease (CKD) and Rutherford class 5 or 6 wounds—groups “routinely excluded” from vascular device studies, the triallists noted in the discussion section of their paper.
Prespecified subgroup analyses indicated a difference between the 19 patients with dialysis-dependent CKD—who had amputation-free survival of 36.8%—and the 86 patients who did not (72.7%), the authors report. Similarly, the mortality rates among these groups of patients were 36.2% (dialysis dependent) and 8.6%, they show.
“Results of a prespecified subgroup analysis were aligned with those of previously published outcomes indicating an increased risk of death after peripheral arterial revascularisation procedures among patients who were undergoing dialysis,” they write. “Although the incidence of limb salvage was similar between patients who had dialysis-dependent chronic kidney disease and those who did not, mortality appeared to be greater in the population with dialysis-dependent disease. The decision to offer transcatheter arterialisation of the deep veins to patients with dialysis-dependent chronic kidney disease should take into consideration life expectancy and patient preferences.”
The LimFlow transcatheter arterialisation system is designed to re-establish blood flow in deep veins for end-stage CLTI patients who have exhausted all other treatment methods and face major amputation of their lower limb. Trial subjects will be followed out to three years.
“The publication of PROMISE II in the New England Journal of Medicine reinforces the transformational value of [transcatheter arterialisation of deep veins] for a patient population in great need,” stated Mehdi Shishehbor (Harrington Heart and Vascular Institute, University Hospitals, Cleveland, USA) PROMISE II’s other co-principal investigator, who is president of the and lead author of the NEJM paper. “The introduction of this therapy provides the possibility of limb salvage for a no-option CLTI population previously consigned to primary amputation, potentially reducing the suffering, mortality, and economic burden in this ever-growing segment of patients.”
“These results establish [transcatheter arterialisation of deep veins] as a real alternative to major amputation for patients facing inevitable limb loss from no-option CLTI,” added Clair. “This therapy will enable us to redefine the concept of a ‘no-option’ CLTI patient by giving us a treatment that offers patients limb salvage and hope.”
The LimFlow system—an investigational device in the USA—attained a CE mark for use in the European Union in 2016.
Researchers found that a minimally invasive procedure combined with epidural steroid injection treatment led to superior pain reduction and disability improvement over one year in patients with sciatica. The results of the study were published in Radiology, a journal of the Radiological Society of North America (RSNA). The combined treatment performed better than steroid injections alone.
Sciatica is pain that originates along the sciatic nerve, which extends from the back of the pelvis down the back of the thigh. The sciatic nerve is the largest nerve in the body. Treatments to relieve pain include nonsteroidal anti-inflammatory medications, applying heat or cold, and exercising to help minimise inflammation. When the pain is caused by a lumbar disc herniation, surgery is often the treatment option for pain relief.
“The goal of nonoperative care is to provide the most effective means of symptom resolution, while still avoiding the need for a surgical procedure,” said the study’s lead author, Alessandro Napoli, associate professor of radiology and interventional radiology at Policlinico Umberto I at the Sapienza University of Rome (Rome, Italy). “However, in many cases conventional approaches are ineffective.”
Minimally invasive interventional therapy has become increasingly popular in patients with sciatica who have become resistant to conservative treatments. Among the available options, transforaminal epidural steroid injection (TFESI) is the only interventional procedure recommended in clinical guidelines. However, the duration of benefit is usually short, and additional treatments are often necessary.
Another treatment that researchers have studied for sciatica pain relief is pulsed radiofrequency—a minimally invasive procedure in which pulses of energy from a probe are applied directly to nerve roots near the spine.
For the multicentre, randomised trial, researchers wanted to determine the difference in effectiveness between pulsed radiofrequency combined with TFESI versus the steroid injection alone for sciatica pain lasting 12 weeks or longer and not responsive to conservative treatment in patients with due to lumbar disc herniation.
A total of 351 participants (223 men) with sciatica were randomly assigned to receive a single computed tomography (CT)-guided pulsed radiofrequency treatment combined with TFESI (174 patients) or TFESI alone (177 patients). Participants were recruited at two tertiary university hospitals and one spine clinic. All procedures were carried out in an outpatient clinic, took only 10 minutes, and were performed without general anaesthesia.
At four, 12, and 52 weeks, there was greater leg pain reduction and greater disability improvement in participants who received pulsed radiofrequency combined with TFESI, compared to the participants who only received the steroid injection.
“The results of our trial demonstrate that a combined treatment of pulsed radiofrequency and TFESI leads to better outcomes at one year following a single 10-minute procedure,” Napoli said.
IceCure Medical, developer of minimally invasive cryoablation technology, the ProSense System (marketed under the brand name IceSense3 in China), that destroys tumours by freezing as an alternative to surgical tumour removal, has announced the National Medical Products Administration (NMPA) of China approved the company’s IceSense3 disposable cryoprobes for commercial use, to be used in combination with the company’s IceSense3 console, which was previously approved by the NMPA.
With this latest approval, the company and its partners in China can address a significant market with its novel and proven technology to treat malignant and benign tissue of the breast, lung, bone, liver, and kidneys, as well as palliative interventions.
“With approximately 430,000 new breast cancer cases in 2022 alone, and a healthcare system readily adopting new technologies that produce improved outcomes, we see China as a prime market for our cryoablation system,” stated Eyal Shamir, IceCure’s chief executive officer. “Having received regulatory approval for commercial sales of both our console and cryoprobes, we expect to effectively monetise our distribution agreement in the Chinese market.”
Data and discussion on revascularisation treatment strategies for patients with chronic limb-threatening ischaemia (CLTI) will take centre stage at the CX 2023 Consensus update, with results from the BASIL-2 (Bypass versus angioplasty in severe ischaemia of the leg-2) randomised controlled trial (RCT) to be presented for the first time.Chief investigator Andrew Bradbury (University of Birmingham, Birmingham, UK) speaks to Interventional News about the background, context and significance of the trial ahead of this year’s meeting.
Bradbury notes that BASIL-2 has its origins in the original BASIL-1 trial, the short-term results of which were published in The Lancet in 2005. BASIL-1 randomised (1999–2003) patients with severe limb ischaemia, mainly due to femoropopliteal disease, to either a plain balloon angioplasty-first or a bypass surgery-first revascularisation strategy. With “fairly limited follow-up,” Bradbury recalls, there did not seem to be much of a difference in the primary outcome of amputation-free survival. There was, however, a suggestion that the data from both groups were “beginning to diverge,” which prompted the team to follow the patients up for longer. Reporting the key finding from these later outcomes, Bradbury summarises that “people randomised in BASIL-1, and who were likely to live for more than two years, and who had a good vein, were best served by having a vein bypass first rather than a plain balloon angioplasty first”.
Speaking on his motivation for starting the BASIL-2 trial, Bradbury recollects how it became clear there were a number of gaps in peripheral arterial disease (PAD) research during his involvement in the UK National Institute for Health and Care Excellence (NICE) guideline expert group on PAD. One such gap had to do with infrapopliteal, or below-the-knee, disease, and Bradbury notes that NICE made a research recommendation to undertake a randomised controlled trial compare a ‘vein bypass-first’ with a ‘best endovascular treatment-first’ strategy for people who required an infrapopliteal procedure. This is what BASIL-2 endeavoured to achieve.
“Endovascular techniques and technologies for lower limb revascularisation are very different now from what they were 15–20 years ago when we did BASIL-1,” Bradbury remarks, noting for example better guidewires, better balloons, more skilful entry and retrograde cannulation to name just a few developments. As a result, the team are keen to see how the two treatment modalities compare in this new treatment landscape.
In addition, the question at the centre of BASIL-2 represents a “massive global problem” and therefore an important one to solve, Bradbury comments. He elaborates: “I have had the opportunity to visit hospitals in many different countries, and vascular wards wherever you go are essentially full of people with CLTI.” Bradbury explains that BASIL-2 is his and his team’s “attempted contribution” to try and improve the evidence base for the treatment of these patients who are “very challenging” and often “very poorly,” with multiple comorbidities.
BASIL-2 is a superiority trial, Bradbury explains, noting that the hypothesis the investigators started with was that vein bypass would be superior due to the fact that BASIL-1 “seemed to show that vein bypass had advantages over endovascular intervention”. He adds that it is a pragmatic trial, and thus surgeons and interventional radiologists are permitted to use their preferred techniques and equipment, with the primary outcome being amputation-free survival (time to major—above the ankle—amputation, or death from any cause, whichever occurs first).
Considering the BASIL-2 trial in its wider context of randomised data in this space, Bradbury notes that the investigators have been in “friendly dialogue” with the BEST-CLI team “from the get-go”. Results of the BEST-CLI trial were presented late last year, with the headline finding being that surgical bypass with adequate single-segment great saphenous vein is a more effective revascularisation strategy for patients with CLTI who are deemed to be suitable for either an open or endovascular approach.
Bradbury notes that there are a number of differences between the two trials, highlighting for example that BASIL-2 included a different group of patients. “Only about 40% of [BEST-CLI] patients has a below-the-knee intervention,” he says. “We are focused in BASIL-2 on below the knee, and [BEST-CLI] did not pre-specify an only below-the-knee analysis.” While BEST-CLI is “not exclusively a femoropopliteal trial,” it has similarities to BASIL-1 in that it is more of a femoropopliteal trial with or without infrapopliteal disease, whereas BASIL-2 is specifically looking at infrapopliteal revascularisation, Bradbury explains.
BASIL-2 and BEST-CLI are both RCTs, however Bradbury is keen to stress the limitations of this high level of evidence. “An RCT is not a GPS, it is more like a wobbly compass near the North Pole, and all it can try and do is push you in a certain direction of travel,” he comments. He adds that while both the BASIL-2 and BEST-CLI teams are “huge enthusiasts” for RCTs, this type of research must still be scrutinised.
Looking ahead to CX, Bradbury expresses his excitement at the prospect of presenting the BASIL-2 data for the first time at what he describes as “the big UK vascular and endovascular meeting”. “I am really looking forward to seeing everyone at CX 2023 and it is going to be a great meeting. It is a pleasure and a privilege for us to be part of it and have the opportunity to present our trial data for the first time.”
Bradbury hopes that once the audience hear the results, as well as the limitations, which “every RCT has,” they will “go away and reflect” on the data and think about them “in the context of their own practice, their own healthcare system and come to a decision as to whether these new data are going to influence their practice, or not, as the case may be”.
Ultimately, Bradbury believes, CLTI treatment “is all about team-working” to determine what is best for the patient. “We sit in an MDT [multidisciplinary team meeting] and there is a discussion about a leg and whether we are going to do endo or vein bypass. It does not necessarily mean the same person has to do both procedures, and I think that is a positive. I do not think people see that as a threat […] and I think most people would think it was better for the patient.”
Join the conversation at CX 2023
During the CX session, Bradbury will deliver the results of the BASIL-2 trial, with co-investigators Catherine Moakes, Gareth Bate and Matthew Popplewell (all University of Birmingham, Birmingham, UK) and Lewis Meecham (University Hospital Cardiff, Wales), set to present on the journey from BASIL-1 to BASIL-2, methodology, study limitations and future work, among other topics.
Attendees in London and remote participants will have the opportunity to pose questions to the BASIL-2 investigators, who—along with an expert panel and in the presence of the US Food and Drug Administration (FDA) and Secretary of State for Health—will interrogate the evidence in a roundtable discussion to reach consensus on this hotly debated topic.
You can watch the BASIL-2 Podium First presentation 11:10–11:40 on Tuesday 25th April and the roundtable discussion 12:00–13:00.
Delcath Systems has announced in a company press release that the US Food and Drug Administration (FDA) has accepted its (Delcath’s) new drug application resubmission for Hepzato Kit (melphalan hydrochloride for injection/hepatic delivery system) seeking approval for the treatment of patients with unresectable hepatic-dominant metastatic ocular melanoma (mOM).
The US FDA also communicated to Delcath that its considers the submission a complete class 2 response and the Prescription Drug User Fee Act (PDUFA) date for the resubmission is 14 August 2023.
“The FDA’s acceptance of the [new drug application] resubmission is a significant milestone for Delcath and we look forward to working with the agency throughout its review of the application,” stated Gerard Michel, Delcath’s chief executive officer. “We believe that Hepzato, if approved, will be an important option for treating patients with mOM.”
Getinge‘s iCast covered stent system has received premarket approval from the US Food and Drug Administration (FDA) for the treatment of patients with iliac arterial occlusive disease.
Iliac arterial occlusive disease is a type of peripheral arterial disease (PAD), which affects 8 million people in the USA. As the world population ages and rates of diabetes and obesity rise, it is estimated that more people will be affected with iliac artery disease.
“We are pleased that the iCast stent system is approved in the USA for use in iliac arteries to benefit an even greater number of patients,” says Elin Frostehav, president of acute care therapies at Getinge. “The global market for covered stents is growing at an annual rate of 5%. Getinge will continue to ramp up capacity throughout the year in order to meet the demand.”
The iCast covered stent system, which is sold outside the USA under the brand name Advanta V12, has been used by clinicians for 20 years and is the most clinically evaluated balloon expandable polytetrafluoroethylene (ePTFE)-covered stent in the world, with clinical data published in more than 550 articles.
A range of experts, including Koen Deloose (Dendermonde, Belgium), Thomas Zeller (Bad Krozingen, Germany), Marianne Brodmann (Graz, Austria) and Antonio Micari (Messina, Italy), talk to Vascular News about how the latest data supporting the cost-effectiveness of the IN.PACT Admiral drug-coated balloon (DCB; Medtronic) is helping to drive the adoption of this treatment strategy in chronic limb threatening ischaemia (CLTI) patients.
The physicians also discuss whether or not these data, combined with those showing long-term safety and efficacy of the Admiral DCB, are enough for this treatment option to becoming standard of care in this challenging patient population.
SurgVision, a company developing pioneering solutions for fluorescence-guided surgical and interventional oncology, part of the Bracco Group, has announced that it has received 510(k) clearance from the US Food and Drug Administration (FDA) for the Explorer Air II for use with pafolacianine (Cytalux, On Target Laboratories) during intraoperative fluorescence imaging.
This is designed to achieve high-sensitivity and imaging fidelity, meeting the needs of oncological intraoperative fluorescence imaging. The system allows real-time imaging during surgery and its prototype has been tested by academic centres for a variety of indications.
“We are very excited about this important milestone. Our goal is to make the Explorer Air II available to surgeons, supporting them in their mission to fight cancer,” quoted Stefan Schorling, managing director and COO of SurgVision.
The Explorer Air II is also cleared in the USA and CE-marked in the EU for visual assessment of blood flow and tissue perfusion.
Currently, the identification of tumours during surgery or interventional endoscopy relies on visual inspection and palpation. Tumour tissue is sometimes difficult to distinguish from healthy tissue. As a consequence, surgical resection of the tumour is often incomplete. This has medical as well as financial implications, impairing patient treatment outcomes.
EDAP TMS, a global leader in robotic energy-based therapies, has announced a recent presentation of positive results from a large, multicentre, noninferiority study comparing Focal One high-intensity focused ultrasound (HIFU) versus radical prostatectomy (RP) at the 38th annual congress of the European Association of Urology (10–13 March, Milan, Italy).
The study, which ran from April 2015 to September 2019, compared Focal One HIFU versus RP as a first-line treatment for patients with localised prostate cancer (grade groups <3). A total of 3,328 patients from 42 treatment centres were included: 1,967 were treated with Focal One HIFU and 1,361 underwent radical prostatectomy surgery. Patients were followed for 30 months.
Among the data that the study produced were the following points:
At 30 months, the salvage treatment-free survival rate was higher in the HIFU arm (90.1%) compared with RP arm (86.8%);
Risk of salvage treatment was greater than 1.2-fold higher after RP (HR: 0.75, 95% CI [0.64-0.96], p = 0.02);
ICS score, a measure of urinary incontinence, was significantly lower after HIFU (0 vs 1, p < 0.001);
IIEF-5, a measure of erectile function, decreased significantly less after HIFU than after RP despite (median Δ = -4 vs -9 p < 0.001);
Postprocedural benefits of HIFU for both erectile function and urinary continence were demonstrated despite patients in the HIFU-treated group being an average of 9.6 years older (median age was 74.7 years for HIFU vs 65.1 years for RP, p>0.0001).
Pascal Rischmann (Rangueil University Hospital, Toulouse, France), who is lead investigator of the study, commented, “I was very pleased to present, for the first time, the final consolidated results from this major academic study which was sponsored by the French Association of Urology. This is the largest study ever done to prospectively evaluate HIFU against radical prostatectomy. The aim of this postapproval, noninferiority study was to compare the survival rates without salvage treatment in both arms, as well as to confirm reimbursement of HIFU in France. These results confirm the growing importance of HIFU in the management of localised prostate cancer.”
Koen Deloose (Dendermonde, Belgium) talks to Vascular News about the key one-year data from the BIOPACT randomised controlled non-inferiority trial, which evaluated the safety and efficacy of the Passeo-18 Lux drug-coated balloon (DCB) catheter (Biotronik) compared to the IN.PACT Admiral DCB (Medtronic).
Speaking at the 2022 Paris Vascular Insights (PVI) conference (23–25 November, Paris, France), Deloose notes that there was “no difference between the balloons” in terms of the primary efficacy endpoint (freedom from clinically-driven target lesion revascularisation at 12 months) as well the primary safety endpoint (a composite of freedom from device- and procedure-related death through 30 days post-index procedure, freedom from major target limb amputation and clinically-driven target vessel revascularisation through 12 months post-index procedure).
Deloose outlines the factors that dictate which device he chooses, including latest data, available sizing and economic considerations. He explains why these types of randomised head-to-head trials are so important, noting that “the more data we have available to show the safety of these kind of technologies, the better”.
A total of £10 million has been awarded to the Medicines and Healthcare products Regulatory Agency (MHRA)—an executive agency of the UK Department of Health and Social Care (DHSC)—to help bring innovative new medicines and medical technologies to UK patients more quickly, His Majesty’s (HM) Treasury has announced.
The funding will be used to accelerate routes for bringing innovative medical products developed in the UK onto the market, as well as those made and approved by other trusted regulatory partners globally.
Over the next two years, the MHRA will use the money to support development of a thorough but shortened process to speed up the approval process for cutting-edge treatments developed in the UK with the greatest opportunity to meet the country’s healthcare priorities, such as cancer vaccines and artificial intelligence (AI)-based therapeutics for mental ill-health.
It will also support the establishment of an international recognition framework, allowing the MHRA to capitalise on the expertise and decision-making of trusted regulatory partners, and provide patients with fast-track access to best-in-class medical products that have been approved in other countries.
The MHRA will still be responsible for the approval of all ‘recognition route’ applications, ensuring that all products are of sufficient quality to be licensed in the UK, and it will operate a robust process promoting patient safety and access to improve the health of the UK population.
Using the agency’s pre-existing international partnerships, developed through the Access Consortium and Project Orbis, the first regulatory partners that the MHRA intends to build new recognition routes with are the Food and Drug Administration (FDA) in the USA and the Pharmaceuticals and Medical Devices Agency (PMDA) in Japan.
June Raine, MHRA chief executive, said: “We greatly welcome the £10 million funding announced by HM Treasury today, which will be used to fund our ongoing innovation work and to accelerate the development of ground-breaking global recognition routes, which will give UK patients faster access to the most cutting-edge medical products in the world.
“This cash injection will ensure that we have access to the best resources, talent, and infrastructure to deliver this ambitious vision for patients across the UK.”
Steve Barclay, UK Secretary of State for Health and Social Care, added: “Technology is transforming our care for patients, delivering faster and more accurate diagnoses. This new funding will accelerate the delivery of cutting-edge treatments like cancer vaccines and new artificial intelligence technology that will make therapy more accessible to those who suffer from mental health conditions.
“It will also fast-track access to medical products that have been approved in other countries by trusted regulatory partners, ensuring we continue to provide the best, most innovative and safest treatments in the UK.”
Merit Medical has announced the expansion of itsSwiftNinja steerable microcatheter product line. New sizes include a low-profile 2.4Fr distal diameter option in 125-cm and new longer 150-cm lengths.
The 180-degree articulating microcatheter is designed to provide access to challenging peripheral and coronary vasculature without the use of a guidewire. It is part of the broader Merit Vascular portfolio that includes sheath introducers, inflation devices, embolics, and other procedural solutions.
“Unlike conventional microcatheters that are limited to a set shape, the steerable SwiftNinja is really a game-changer,” said Jason Hoffmann, interventional radiologist at New York University (New York, USA), and consultant for Merit Medical. “The tip shape and angle can be changed in real time while inside a patient, allowing for shorter procedures with less radiation exposure. Without the need for a guidewire, there is the potential for significant cost savings as well—all of which benefit the patient. The SwiftNinja has paved the way for better embolization care.”
“The SwiftNinja is the only widely offered steerable microcatheter in the USA,” said Fred P Lampropoulos, Merit Medical’s chairman and CEO. “By providing the additional sizes that physicians require, the SwiftNinja can be used with a range of devices in a greater number of procedures, diagnosing and treating more complex cases.”
The Society of Vascular and Interventional Neurology (SVIN) has released its first global analysis of access to mechanical thrombectomy for the treatment of large vessel occlusion (LVO) stroke. Findings from MT-GLASS—a study conducted as part of the SVIN Mission Thrombectomy 2020-plus (MT2020+) initiative—have been published in the journal Circulation.
The MT-GLASS study looked at worldwide access to life-saving thrombectomy treatments, and the factors that contribute to global access, including income class of the country, based on the World Bank classification; proportion of gross domestic product (GDP) spent on healthcare; availability of thrombectomy infrastructure, including operators and centres; availability of reimbursement for thrombectomy; and other relevant stroke systems of care policies.
The study ultimately found an “extremely low” global rate of mechanical thrombectomy access, with an “enormous disparity” between countries by income level.
“The study findings validate why we founded Mission Thrombectomy in 2016 and our continued mission that has now grown to include 95 countries,” said Dileep Yavagal (University of Miami, Coral Gables, USA), corresponding author of the study, chair of the MT2020+ initiative, and past president and co-founder of SVIN. “The global access to thrombectomy is dismally low, with the countries’ income level, prehospital protocols to bypass non-thrombectomy centres, and operator and thrombectomy centre availability, all playing critical roles in thrombectomy access in a given region.”
MT-GLASS was conducted throughout 75 countries using the Mission Thrombectomy global network of regions between November 2020 and February 2021, and received 887 responses from across 67 countries, a SVIN press release details.
It found a median global thrombectomy access rate of 2.79% (interquartile range, 0.7–11.74%), and revealed a <1% rate of thrombectomy access in 18 countries and 0% in seven countries. In addition, there was a 460-fold disparity between the highest and lowest non-zero thrombectomy access regions, while low-income countries had an 88% lower rate of access compared to high-income countries.
The global rate of availability for thrombectomy-capable operators and centres were found to be 16.5% and 20.8%, respectively, of what is considered to be the “optimal” rate, the authors report. Multivariable regression analyses showed that country income level (low/lower-middle versus high); operator and centre availability; and presence of prehospital acute stroke bypass protocols, were all “significantly associated” with increased odds of thrombectomy access.
“Mechanical thrombectomy has proven to be a highly effective therapy for mitigating death and disability since 2015, and it is the largest advancement in stroke treatment in 30 years,” said SVIN president Ameer Hassan (Valley Baptist Neuroscience Institute, Harlingen, USA). “Given the widely distributed global burden of stroke, it is critical to have rapid access to mechanical thrombectomy, worldwide, in an equitable manner. In the USA, stroke is now the number-five killer—but, in the rest of the world, it is still number two! The findings highlight distressing results on a global scale, and represent many lives that could have been saved or significantly improved with better access to thrombectomy treatments.”
“We believe that insights gained from this study would inform global interventions to improve access to this life-saving treatment and enable researchers to study nuances of the obstacles to it further,” added Kaiz Asif (University of Illinois, Chicago, USA), corresponding and first author of the study. “While we continue to work on innovations in surgical treatments and technologies, we are also determined to expedite their dissemination—through Mission Thrombectomy—to a large majority of people across the world to whom they are not yet available.”
When receiving treatment for abdominal aortic aneurysm (AAA), female patients have a higher risk for kidney damage after endovascular repair, a Michigan Medicine study finds.
Researchers from Michigan Medicine designed an algorithm that can be used prior to endovascular AAA repair to identify risk for kidney damage. They tested the algorithm using data from over 7,000 patients through the Blue Cross Blue Shield of Michigan Cardiovascular Consortium database.
The risk prediction algorithm, according to findings published in Annals of Vascular Surgery, demonstrated that women receiving endovascular aneurysm repair had 1.4 times higher odds of developing acute kidney injury after aneurysm repair.
“While we have seen higher risk of acute kidney injury in female patients who have undergone coronary stenting or renal stenting, this is the first time we are seeing a higher risk after endovascular abdominal aortic aneurysm repair,” said senior author Peter Henke (University of Michigan Health Frankel Cardiovascular Center, Ann Arbor, USA).
Patients with reduced glomerular filtration rate, an indicator of kidney disease, had 4.7 times higher odds of developing acute kidney injury after aneurysm repair. Those with larger aneurysms were also at increased risk. These findings are less surprising than the higher odds of kidney injury in women, investigators say, given patients’ decreased renal function at baseline and the possible prolonged procedures and intraoperative contrast loads that come with larger aneurysms.
The Michigan Medicine research team hopes to implement the algorithm in clinical practice to provide at-risk patients with optimisation before an operation.
“Kidney injury after surgery can be benign, but for some patients it leads to permanent renal failure and, in some instances, dialysis,” said first author Drew Braet (University of Michigan Health Frankel Cardiovascular Center, Ann Arbor, USA). “This algorithm shows that we can use easily attainable factors prior to surgery that may help identify patients at risk of complications during their surgery and, thus, ensure we are optimizing these patients accordingly. If we can protect patients and decrease their risk of permanent renal failure, then we have truly provided them a benefit.”
Shockwave Medical today announced the full US commercial availability of the Shockwave L6 peripheral intravascular lithotripsy (IVL) catheter following clearance by the US Food and Drug Administration (FDA).
A press release details that the Shockwave L6 catheter is purpose-built to modify calcification in otherwise difficult-to-treat lesions in large peripheral vessels, including the iliac and the common femoral arteries.
“The Shockwave L6 catheter pushes the boundaries of what IVL can help physicians achieve for patients with severe peripheral arterial disease,” said Frank Arko (Sanger Heart and Vascular Institute, Charlotte, USA). “The characteristics of the new catheter allow physicians to optimise IVL therapy in large peripheral vessels, which represent over 20% of peripheral interventions performed in the USA each year. The Shockwave L6 catheter may also be beneficial when IVL is utilised to facilitate transfemoral access for large bore procedures like TAVR [transcatheter aortic valve replacement], TEVAR [thoracic endovascular aortic repair] and EVAR [endovascular aortic repair] to minimise the risks of rupture and dissection.”
According to Shockwave Medical, the L6 IVL catheter’s compact emitter configuration, in conjunction with four new device sizes (8, 9, 10 and 12mm diameters), enables effective delivery of sonic pressure waves in larger vessels.
“Shockwave L6 is another example of our team’s commitment to developing technologies to address specific market needs while still maintaining the safety, effectiveness and ease of use of our core IVL technology,” said Doug Godshall, chief executive officer of Shockwave Medical. “We are pleased with the success of our limited release and the great feedback we have received from our customers. We now look forward to offering Shockwave L6 as an additional IVL option for the most complex and high-risk large vessel cases.”
The final results of the RAVI prospective registry study demonstrated the safety and efficacy of radial access in visceral interventions in standard embolization procedures for uterine fibroids, benign prostatic hyperplasia, and hypervascular tumours. The findings of the Terumo Medical-sponsored study were presented at the Society of Interventional Radiology (SIR) 2023 annual scientific meeting (4–9 March, Phoenix, USA).
The results of the RAVI registry—the largest, prospective, multicentre, observational study in vascular and interventional radiology (VIR)—were shared on behalf of study investigators by Marcelo Guimarães, professor of radiology and surgery, Division of Vascular and Interventional Radiology, Medical University of South Carolina (MUSC; Charleston, USA). It showed that radial access (RA) can be used as the primary access site for highly relevant and emerging embolization procedures, regardless of disease state (benign or malignant).
Of the 105 patients screened for the study, 99 were successfully enrolled in six US hospitals and treated between February 2020 and January 2022. In addition to MUSC, the other leading IR centres that participated were: Mount Sinai Hospital (New York); St Louis University (St Louis); University of North Carolina at Chapel Hill; Rush University (Chicago); and the University of California, Los Angeles.
The primary safety endpoints included RA-related complications, stroke, myocardial infarction and death at 30 days. The procedural endpoint was defined as successful completion of the intended procedure using RA (i.e. without femoral bailout), which was achieved in 100% of patients. Technical success was 100%, defined as the successful embolization of the target lesion/organ. This prospective registry confirmed the safety and efficacy of RA at 30 days’ follow-up in visceral embolization procedures. Of the 99 patients in the study, 74 (74.7%) were able to be discharged the same day of their procedure, demonstrating that RA for embolization procedures can create efficiencies in cost management. In addition, newly presented one-year results focus on 70 patients where UFE was performed. The data showed that UFE done transradially allows for fast recovery, presents low risk of bleeding and other complications, and demonstrates sustained improvement in quality of life.
“We are proud to announce the one-year results from the biggest cohort of patients where UFE is performed using radial access,” said Guimarães. “Safety and effectiveness of this procedure, as shown in this study, should encourage us in our belief that radial access could potentially become preferred for all common embolization procedures.”
A new trial of endovascular ultrasound-based renal denervation technology has found that it reduced blood pressure in hypertensive patients at two months. The RADIANCE II study, published in The Journal of the American Medical Association (JAMA), was carried out by a team led by Michel Azizi (Université Paris Cité, Paris, France). The international, multicentre, sham-controlled randomised clinical trial was aimed at determining the procedure’s safety and efficacy “in the absence of the potentially confounding influence of antihypertensive medications”.
Azizi et al sketch out some background to the trial in their introduction, where they state that the widespread availability of pharmacotherapy for hypertension, which is at the core of existing treatment for the condition, has not prevented many patients from being inadequately treated. Endovascular renal denervation using radiofrequency or ultrasound technology for renal nerve ablation, they say, has been examined as an adjunct to pharmacotherapy and lifestyle change, but that earlier studies with the radiofrequency technology including the DENERHTN randomised controlled trial, also led by Azizi, and the Simplicity HTN3 trial reported “inconsistent results”. They also refer to the further RADIANCE-HTN SOLO trial using ultrasound renal denervation led by Azizi to place RADIANCE II in context.
RADIANCE II took place across 37 centres in the USA and 24 in Europe, enrolling a total of 1,038 patients of whom 224 met all criteria for randomisation. Of these 224, 150 were randomised to a group receiving ultrasound renal denervation and 74 to a sham procedure group. The mean age was 55 years, while 28.6% of patients were women. Antihypertensive medications were being taken by 147 patients (65.6%) at the time of their enrolment, while the rest had previously received but ceased taking them. Those patients receiving renal denervation underwent a procedure of an average length of 77 minutes, compared with 44 minutes for the sham procedure. Bilateral ablation was successfully carried out in 148 of 150 patients (98.7%), with 30 (20.0%) of these having accessory renal artery ablations.
The primary efficacy outcome of the trial was the mean change in daytime ambulatory systolic blood pressure (SBP) at two months, with patients of both groups maintained off medications except for when blood pressure exceeded a certain level. There was also a primary safety outcome which was a composite of major adverse events including “death, kidney failure, and major embolic, vascular, cardiovascular, cerebrovascular, and hypertensive events at 30 days and renal artery stenosis greater than 70% detected at six months”. There were a number of secondary outcomes—these included mean change in 24-hour ambulatory SBP, home SBP, office SBP, and all diastolic blood pressure parameters at two months”.
Turning to the results, the study authors found that ultrasound renal denervation brought a greater reduction in daytime ambulatory SBP (mean, −7.9mmHg [standard deviation (SD), 11.6mmHg]) vs. the sham procedure (mean, −1.8mmHg [SD, 9.5mmHg]; baseline-adjusted between-group difference, −6.3mmHg [95% CI, −9.3 to −3.2mmHg], p<0.001), which the study authors reported to be consistent throughout the 24-hour circadian cycle. “Among the seven secondary blood pressure outcomes,” Azizi and colleagues also reported, “six were significantly improved with ultrasound renal denervation vs. the sham procedure.”
Discussing the findings, the authors note that patients in RADIANCE II had more severe hypertension than those in RADIANCE-HTN SOLO, while they also state that “the homogeneity of the blood pressure-lowering effect of ultrasound renal denervation, independent of the method of blood pressure measurement, reinforces the strength of the results”. In further results that reflect a strong performance for denervation, SBP decrease in the ultrasound renal denervation group was found to be present “as early as one month after undergoing the procedure”. The procedure was found to be safe, with no adverse events, which was also found in the RADIANCE-HTN SOLO results.
Azizi et al pointed to several limitations of RADIANCE II. The first noted was the limited period of follow-up of two months—though plans for further follow-up are mentioned. The trial was also “limited to those at low cardiovascular risk with an estimated glomerular filtration rate (eGFR) of 40 mL/min/1.73m2 or greater and without significant comorbidities”, something that owed to the trial’s design, which required the withdrawal of blood pressure medications. Therefore, they suggest, the generalisability of the trial’s results to patients with the most severe hypertension could be limited—though its results are promising for those with hypertension which is resistant to existing treatments, as previously shown by Azizi et al in the RADIANCE TRIO trial.
The authors add too that the effects of the procedure on any given individual patient may be “difficult to predict as a result of the “variability in the prevailing state of sympathetic hyperactivity or variable renal nerve ablation”. In an editorial accompanying the study in JAMA, Clyde W Yancy (Northwestern University Feinberg School of Medicine, Chicago, USA) and colleagues say there remain questions over “patient selection, anatomic or physiologic barriers to denervation, durability of the blood pressure response, and operator or institutional requirements” which demand further investigation. Renal denervation, they say, must be one element in “a more comprehensive disease-management algorithm”.
Distal embolic protection using a filter has been associated with improved transfemoral carotid artery stenting (tfCAS) outcomes in terms of in-hospital stroke and death risks—underpinning current Society for Vascular Surgery (SVS) guidelines recommending routine use of distal embolic protection during carotid stenting, and supporting the notion that, “if a filter cannot be placed safely, an alternative approach to carotid revascularisation should be considered”.
Sophie Wang, Patric Liang (both Harvard Medical School, Boston, USA) and colleagues deliver this message in a recent Journal of Vascular Surgery (JVS) publication detailing a retrospective, propensity score-matched cohort analysis of tfCAS patients in the Vascular Quality Initiative (VQI) across a 16-year period.
“Transfemoral carotid stenting without use of embolic protection is associated with a significant increase in in-hospital stroke/death compared with tfCAS performed with distal filter placement,” the authors write. “Failed attempted filter placement is associated with worse outcomes after tfCAS, but stroke/death rates are no different than those seen in patients in whom a filter was never attempted.
“These findings support the current guideline recommendation for routine use of distal embolic filters during tfCAS. However, the proportion of non-protected tfCAS performed annually is increasing, and there is significant variability in routine filter usage across physicians and centres in the VQI.”
In an effort to assess in-hospital outcomes in patients undergoing tfCAS with and without embolic protection using a distal filter, Wang, Liang and colleagues identified all patients undergoing this procedure in the VQI from March 2005 to December 2021—excluding those who received proximal embolic balloon protection. As well as creating propensity score-matched cohorts of patients who underwent tfCAS with and without attempted filter placement, they performed subgroup analyses of patients with ‘failed’ versus ‘successful’ filter placement, and ‘failed’ versus ‘no attempt’ at filter placement.
In-hospital outcomes were assessed using log binomial regression, adjusted for protamine use, the authors detail. Their outcomes of interest were composite stroke/death, stroke, death, myocardial infarction (MI), transient ischaemic attack (TIA), and hyperperfusion syndrome.
Among 29,853 patients who underwent tfCAS, 28,213 (95%) had a filter attempted for distal embolic protection and 1,640 (5%) did not. After propensity-score matching, 6,859 patients were identified.
In comparison to cases in which a filter placement was attempted, no attempted filter was associated with a significantly higher risk of in-hospital stroke/death (6.4% vs 3.8%)—constituting a more than two-fold increase in stroke/death risk, as per the analysis’ key outcome of interest. Similar trends were observed regarding stroke (3.7% vs 2.5%) and mortality (3.5% vs 1.7%) too.
In a secondary analysis of patients who underwent a failed attempt at filter placement—versus successful filter placement—failure was associated with worse outcomes (stroke/death: 5.8% vs 2.7%; stroke: 5.3% vs 1.8%, respectively). However, Wang, Liang and colleagues observed no statistical difference in outcomes in patients with failed versus no attempted filter placement (stroke/death: 5.4% vs 6.2%; stroke: 4.7% vs 3.7%; death: 0.9% vs 3.4%) after adjusted analysis.
“Distal embolic protection confers a benefit in stroke/death rates following tfCAS compared to unprotected stenting,” the authors conclude, putting forward their ‘take-home message’ in JVS. “Failure to place a filter should prompt exploration of alternative carotid revascularisation approaches.”
NeoDynamics, a medical device company dedicated to advancing the diagnosis and care of cancer, recently announced that the company has been granted a Chinese patent for the needle design employed in the NeoNavia FlexiPulse probe.
The front-loaded, open-tip sampling needle is designed to enable maximum tissue yield, with minimal patient trauma. The patent is an important milestone that opens up for a future commercial launch in China and strengthens the protection of the NeoNavia biopsy system. NeoNavia with FlexiPulse addresses biopsies in the axillary lymph nodes, which can be a technically and anatomically challenging site due to the proximity to blood vessels and nerves.
The Chinese patent comes on top of a similar patent granted in the USA in August 2021, followed by US Food and Drug Administration (FDA) clearance received in September 2022.
“The novel needle design has shown great results in PULSE, our German multicentre study evaluating the safety and performance of the device in the axillary lymph nodes of breast cancer patients,” says Kai-Uwe Schässburger, director of clinical development and medical affairs, NeoDynamics.
Michel Reijnen (Arnhem, The Netherlands) presents the results of a study that sought to assess the potential cost-effectiveness of a urea-based drug-coated balloon (DCB; IN.PACT Admiral, Medtronic) as standard of care treatment for those with chronic limb threatening ischaemia (CLTI) within the Dutch and German healthcare settings.
Reijnen looks at the rising trend in national healthcare spending which he notes indicates that “cost-effectiveness is becoming more and more important” and goes on to outline the study design and some of the key results of the quality-adjusted life year (QALY) analysis. In fact, although the procedure costs were slightly higher in the DCB group, the target lesion revascularisation and amputation costs were found to be higher in the status quo group. This ultimately meant a cost saving for DCB use across both healthcare communities.
New interventional oncology data from Galvanize demonstrate positive preclinical and early clinical study results using the Aliya pulsed electric field (PEF) system.
The Aliya PEF system, which has US Food and Drug Administration (FDA) clearance for soft tissue ablation, is being studied in Europe and Asia to treat solid tumours by inducing PEF-mediated cell death and neoantigen creation, designed to stimulate the patient’s own immune system to activate against the tumour. Results from two Aliya PEF studies were presented during oral sessions at the Society of Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA).
The INCITE-ES clinical study is a treat and resect study conducted outside of the USA, designed to assess safety, including impact on sensitive structures such as vessels, airways and pleura; and examine immune activation in patients with non-small cell lung cancer (NSCLC) (NCT04732520). Results demonstrated high technical success with a favourable safety profile in delivering PEF energy with a single needle with no PEF-related adverse events and no impact on planned surgical resections. PEF treatment significantly reduced malignant tissue, and 95% of the assessed sensitive structures within the PEF treatment zone remained viable and unaffected by the PEF energy. Additionally, PEF increased tertiary lymphoid structure accumulation, indicating potential immunoactivation with PEF.
A preclinical study, which was featured by SIR as an SIR 2023 exceptional abstract, compared tumour response with incomplete ablation using PEF vs radiofrequency ablation (RFA) in mice with breast cancer tumours. Results showed that PEF induced a greater infiltration of immune cells in the ablated zone and increased tumour recruitment of antigen cells as compared to RFA. PEF also showed greater suppression of tumour growth and had a synergistic effect in combination with immunotherapy, unlike RFA.
“Galvanize’s unique approach to improving cancer outcomes through electrosurgical immunotherapy continues to show compelling promise, and we are excited to share our newest study results with leading interventional radiologists and other medical experts around the world,” said Jonathan Waldstreicher, founder and CEO of Galvanize Therapeutics. “We are making additional investments to expand our Aliya clinical research programme, including a US clinical study of patients with NSCLC.”
Traveler 16 is a 16Ga needle and is one of three variations in the Traveler series
Traveler 16 is a 16Ga needle and is one of three variations in the Traveler series
Argon Medical, a leading provider of device solutions for interventional radiology (IR), vascular surgery, interventional cardiology, and oncology, introduces the Traveler portal vein access series as the newest addition to its portal vein access product portfolio. The product line is designed to meet the needs of physicians accessing the portal vein through the liver during transjugular intrahepatic portosystemic shunt (TIPS) procedures. Traveler supplements Argon’s 2021 launch of Scorpion, which also supports TIPS procedures.
Traveler is designed to improve component visualisation and durability, which are common challenges of the TIPS procedure. “Several innovative features of the Traveler set make it easier to access the portal vein compared to other sets on the market. Firstly, the metal cannula is very robust, and the shaping tool allows it to be curved to great degrees without compromising component integrity. Secondly, the puncture needle is longer and seems sharper, making it easier to pass through severely fibrotic liver parenchyma and reach the portal vein, even when there is very distorted anatomy” said Donna D’Souza, an interventional radiologist at the University of Minnesota (Minneapolis, USA).
“Our mission is to improve the lives of patients and caregivers through the innovation, manufacturing, and delivery of best-in-class medical devices. Thus, we were compelled to act when we identified an opportunity to simplify complex portal vein access procedures for our customers. We are excited to launch our new Traveler products for this purpose and see the positive impact they have on portal access procedures and outcomes in accordance with our mission,” said George Leondis, president and CEO of Argon Medical.
The Traveler Series, which includes Traveler 16, Traveler 21, and Traveler 38, is now available in the USA and Canada.
The European Union’s Council of Ministers has today adopted a resolution to extend the deadline for the certification of medical devices under the Medical Devices Regulation (MDR).
Producers of medical devices will have until 31 December 2027 for higher risk devices and until 31 December 2028 for medium and lower risk devices to meet the legal requirements.
The extension of the transition period will be granted under certain conditions, ensuring that only devices that are safe and for which manufacturers have already started the certification procedure will benefit from the additional time.
The regulation—which changes the way that medical devices are certified for use in the European market—first came into effect in 2021 with an initial three-year transition period, having been delayed by one year in 2020 due to the onset of the COVID-19 pandemic. However, challenges in the implementation of the legislation led to concerns about a potential shortfall in the availability of certain devices, which prompted a rethink in the timetable for the regulation as proposed by the European Commission in December.
Today’s adoption of the resolution by EU Council members, comprising ministers from each of the EU’s member states, means that the decision to extend the implementation period will enter into force on the day of its publication in the Official Journal of the EU.
“Today we have agreed on measures that will allow the industry to continue bringing essential medical devices to the market and ensure that patients have safe access to medical devices,” Acko Ankarberg Johansson, Sweden’s minister for healthcare, was quoted saying.
MedTech Europe, which represents the continent’s device manufacturers, has welcomed the adoption of the amended transitional provisions, which it said will help mitigate the immediate risk that medical devices across all areas of medicine, which are still on the EU market, would no longer be available after May 2024.
“The amendment of the Medical Devices Regulations’ transitional provisions is a needed step forward to help ensure that more medical devices remain available to patients and healthcare systems across Europe. This decision grants Notified Bodies more time to complete certification of more than 500.000 medical devices and accelerates efforts to certify innovative devices in the pipeline,” says Oliver Bisazza, CEO of MedTech Europe.
As soon as the amendment comes into force, MedTech Europe said that alongside its members it will work toward its implementation according to the new provisions and extended deadlines.
“In that regard, it is important that all stakeholders have an aligned and clear interpretation of the amendment, including the process for submitting applications to Notified Bodies, and how the extended validity of certificates can be concretely demonstrated,” the organisation’s statement adds.
Data from a new prespecified analysis of the phase III VOYAGER PAD clinical trial show that low-dose rivaroxaban plus aspirin resulted in a 33% reduction in acute limb ischaemia and a 15% reduction in major adverse limb and cardiovascular events, with or without dual antiplatelet therapy (DAPT).
The new findings reinforce the benefits of the Xarelto (rivaroxaban; Janssen Pharmaceutical Companies of Johnson & Johnson) vascular dose (2.5 mg twice daily plus aspirin 100 mg once daily) over standard of care (aspirin alone), demonstrating consistent benefit at 30 days, 90 days and up to three years following lower extremity revascularisation in patients with peripheral arterial disease (PAD).
“These data demonstrate an evolution in the medical therapy of patients undergoing lower extremity revascularisation for symptomatic [PAD],” said Marc P Bonaca (University of Colorado Anschutz Medical Campus, Aurora, USA), lead study author of the VOYAGER PAD analysis. “We hope these data assist clinicians in understanding how to implement antithrombotic therapy in practice and overall support initiation of rivaroxaban in the first days after revascularisation regardless of whether or not DAPT is utilised.”
Those treated with Xarelto plus aspirin after lower extremity revascularisation saw a 33% reduction in acute limb ischaemia, with a trend toward greater benefit observed early (≤30 days hazard ratio [HR]=0.45; 95% confidence interval [CI] 0.24–0.85) vs. late (>90 days HR=0.75; 95% CI 0.60–0.95).
Xarelto plus aspirin was more effective than antiplatelet therapy alone in preventing acute limb ischaemia after lower extremity revascularisation (Kaplan-Meier estimate from 0 to 90 days 1.02% vs. 2.10%, respectively, and 4.3% and 5.7% from 91 days to three years). The hazard ratio for the rate of thrombolysis in myocardial infarction (TIMI) major bleeding at 0 to 90 days was HR 2.01 (range 0.9–4.47) and from days 91 up to three years was HR 1.28 (range 0.82–1.99), neither of which were statistically significant.
Janssen Pharmaceutical Companies of Johnson & Johnson note in a press release announcing the new results that the Xarelto vascular dose is the first and only approved anticoagulant for PAD.
Lead researchers Clifford Weiss and Daniel Giraldo Herrera (Johns Hopkins University School of Medicine, Baltimore, USA) presented their recent bariatric arterial embolization (BAE) study at the Society of Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA). Their research found that the procedure was associated with “significant” weight loss that did not affect muscle mass, as detected by whole-body magnetic resonance imaging anthropometry.
The authors note in the study abstract that the purpose of their research was “to evaluate the early effects of BAE on multicompartment fat and muscle body composition”, which constitutes the pilot phase of the BEATLES trial (bariatric embolization of arteries with imaging visible embolics).
BEATLES is a US Food and Drug Administration (FDA)-approved, physician-initiated investigational device exemption (IDE) study that, Weiss, Herrera, et al stipulate in their abstract, “evaluates tightly calibrated 100–200μm radiopaque microspheres” (BT-001933-01, Boston Scientific) delivered transarterially into the gastric fundus, supplied by the left gastric and left gastroepiploic arteries. Adult participants with obesity—defined as those with a body mass index [BMI]≥35 kg/m2—were scanned at zero (baseline), three, and six months post-BAE from neck to knee using a Siemens Skyra 3T magnetic resonance imaging (MRI) scanner. The researched employed a dual-echo Dixon water-fat vibe protocol, and a single-slice multiecho Dixon proton liver density acquisition.
Anthropometrics were gathered using AMRA Researcher (AMRA Medical), a semi-automated cloud-based MRI segmentation tool, and statistical testing was performed via repeated measures correlation (Rrm).
Regarding the results, the researchers shared in their write-up that seven patients (six female, one male) with a mean age of 39.6 ± 11.0 years and Centers for Disease Control and Prevention-defined class II–III obesity underwent BAE. At zero, three, and six months, mean body weight was 125.9±24.4, 113.5±21.2, and 110.7±23.3kg (R rm=-0.694 [95% confidence interval (CI) -0.921–-0.113], P value=0.012). Weight-to-thigh muscle volume ratios were 10.3±1.9, 10.0±0.5, and 9.2±1.3 kg/L (Rrm =0.89 [95% CI 0.64–0.97], P value =0.001), respectively.
Weiss, Herrera, et al were able to conclude that “BAE using 100–200μm microspheres is associated with significant postprocedural muscle-sparing weight loss via subcutaneous and intramuscular fat reduction.”
Robert A Lookstein, who is executive vice chair, Diagnostic, Molecular and Interventional Radiology at the Icahn School of Medicine at Mount Sinai Hospital (New York, USA) today presented the results of a subanalysis of Thrombolex’s National Heart, Lung and Blood Institute (NHLBI)-sponsored RESCUE trial during the late-breaking trial session at the Society for Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA).
The core laboratory analysis of this investigational device exemption (IDE) trial demonstrated that pharmacomechanical catheter-directed thrombolysis (PMCDT) therapy using the Bashir endovascular catheter from Thrombolex led to a significant reduction in segmental arterial occlusions (71%; p<0.0001), which correlated with the reduction in right ventricular to left ventricular (RV/LV) ratio (p= 0.0026). There was also a significant reduction in main pulmonary artery (PA) occlusions (61%; p<0.0001) but this did not correlate significantly with the reduction in RV/LV ratio. This reduction in occlusions of not only the main PAs but also the segmental arteries explains why the overall reduction in PA obstruction as assessed by the refined Modified Miller Index is greater with the Bashir endovascular catheter than that which has been reported in contemporary thrombectomy or thrombolysis trials for the treatment of acute pulmonary embolism (PE).
The magnitude of effect of these other treatments on segmental arterial occlusions has not previously been reported.
The RESCUE trial is a prospective, multicentre trial evaluating the Bashir catheter in 109 patients with intermediate-risk acute PE at 18 sites in the USA. The Bashir catheter was used to deliver 7mg of recombinant tissue plasminogen activator (r-tPA) into each PA over a five-hour infusion period. The primary efficacy endpoint was the core lab-assessed change in the computed tomography angioplasty (CTA)-derived mean RV/LV diameter ratio at 48 hours, and the primary safety endpoint was serious adverse events, including major bleeding, at 72 hours. The median device placement time was 15 minutes and length of hospital stay, 2.8 days.
“The RESCUE trial demonstrated rapid resolution of obstruction in the main, and especially segmental, arteries, with less than a 1% major bleeding rate. It is imperative that future PE trials assess the reduction in obstruction in more distal PAs since it has been shown that both the degree of residual PA obstruction and reduction in pulmonary vascular volumes, presumably due to reduced PA inflow, are significant predictors of late PE-related mortality. This novel approach with the Bashir catheter and low-dose tPA represents a major advance in the treatment of acute PE,” said Lookstein.
During the late-breaking session at SIR 2023, Lookstein answered a question about total procedure time, which he stipulated as having been six hours as per protocol. He noted, however, that there may be potential for this to be reduced, but that this would necessitate prospective research in order to be validated. A further comment from one of the delegates present drew attention to the fact that it was “interesting” that RESCUE found the bleeding rate to be “lower” than in some mechanical thrombectomy trials.
“We are pleased to be able to share this important new information from our RESCUE trial and thank all those who made this possible, especially our physician investigators and their patients. We would also like to thank the National Institutes of Health and the Commonwealth of Pennsylvania Department of Health for their support,” said Brian G Firth, chief scientific officer of Thrombolex and Principal Investigator of the NHLBI-funded grant to Thrombolex.
Large bore mechanical thrombectomy with the FlowTriever system (Inari Medical) in patients with high-risk pulmonary embolism (PE) was associated with a significantly lower occurrence of meaningful in-hospital adverse clinical outcomes compared to other contemporary treatments, data presented at the American College of Cardiology (ACC) 2023 Scientific Sessions (4–6 March, New Orleans, USA) indicate.
These were among the results of the FLAME study, a prospective, non-randomised study of interventional treatment in high-risk PE, a patient population with a historical mortality rate of 25-50%, which were presented at ACC 2023 by Mitchell Silver (OhioHealth Heart and Vascular, Mansfield, USA).
The study collected data on patients treated with the FlowTriever and on those treated with other therapies in a context arm. The primary endpoint measured a composite of meaningful in-hospital clinical outcomes, including mortality, major bleeding, clinical deterioration, and escalation to an alternate therapy.
Silver reported that FLAME was stopped early after meeting the pre-specified interim analysis criterion at 50 FlowTriever patients. Sharing the results of the study, Silver noted that the endpoint was met in the FlowTriever arm, in which a mortality rate of 1.9% was recorded, compared to 29.5% in the context arm. In all, the composite primary endpoint occurred in 17% of patients in the FlowTriever arm, compared to 63.9% in the context arm.
“The remarkably low mortality seen with FlowTriever demonstrates the benefit of rapidly identifying PE patients and getting them to an interventionalist for assessment,” Silver was quoted as saying in a press release issued shortly after the presentation of the results at ACC 2023. “It is time for our hospital systems to develop standardized care pathways for PE, similar to what has been done in other major cardiovascular diseases such as heart attack and stroke.”
“High-risk PE persists as one of the deadliest cardiovascular diseases,” James Horowitz (NYU Grossman School of Medicine, New York, USA), FLAME national principal investigator was also quoted in the same release. “Outcomes have remained unchanged for decades. The FLAME data shows that [the] FlowTriever is an important new treatment option that offers a dramatic improvement in survival.”
Viz.ai has announced it will use its Viz Recruit platform to optimise patient enrolment for the National Institutes of Health (NIH)-funded Pulmonary embolism—thrombus removal with catheter-directed thrombolysis (PE-TRACT) clinical trial.
The company claims that PE-TRACT will be the most rigorous randomised controlled clinical trial to date of catheter-directed therapy for PE, with plans to enrol 500 patients across 30–50 sites.
The PE-TRACT trial is designed to address whether catheter therapy should be routinely used to treat intermediate-risk PE versus anticoagulants alone.
“The PE-TRACT trial will offer a deeper knowledge of PE by providing a comprehensive comparison of catheter-directed therapy plus anticoagulation to anticoagulation alone,” said Akhilesh Sista (Weill Cornell Medical College, New York, USA), principal investigator of the PE-TRACT trial. “PE-TRACT will provide valuable insights to patients and providers regarding which approach best maintains cardiopulmonary health in the year following PE. Viz.ai’s Recruit tool has the potential to efficiently identify potential participants and help this important trial complete enrolment on time.”
Participating research institutions in the PE-TRACT trial will use Viz Recruit to find, screen, and enrol clinical trial candidates. Viz Recruit, an artificial intelligence (AI)-powered clinical trial enrolment platform, automates the identification and triage of eligible candidates for pre-trial review, while reducing the burden on the research team. Using Viz Recruit, sites will be able to automatically screen patients based on PE and high right ventricular to left ventricular diameter (RV/LV) ratio. The cloud-based technology helps to broaden the recruitment funnel in both size and diversity and streamlines the trial enrolment workflow. To date, Viz Recruit has been used to screen nearly 300,000 patients and identify over 14,000 clinical trial candidates across 100 healthcare facilities, a press release reports.
Viz.ai advises that information on the PE-TRACT trial and the Viz Recruit platform will be presented at the upcoming Society of Interventional Radiology (SIR) meeting (4–9 March, Phoenix, USA).
Mr. Jordan Pollack, CEO, VeinWay (left) and Dr. Minhaj S. Khaja (right) on the day of the procedure.
Jordan Pollack, CEO, VeinWay (left) and Minhaj S Khaja (right) on the day of the procedure
In a first-in-human, compassionate use case approved by the US Food and Drug Administration (FDA), University of Michigan Health (Ann Arbor, USA) interventional radiologists David M Williams and Minhaj S Khaja successfully used VeinWay’s Traversa for venous recanalisation to save a patient’s leg that was close to being amputated.
Traversa, a newly developed tool for crossing tough occlusions in veins, enabled the physicians to recanalise a previously uncrossable vascular pathway, which included a 20cm-long blocked vein with four occluded stents.
Williams made the following comment on the procedure—“I had crossed the segment in this patient three years ago, but today it would have been impossible with existing devices. The patient’s leg was in a desperate condition. Traversa not only made this procedure possible, but also much easier and impressively faster.”
Khaja said that “the device allowed us to take the path that we wanted rather than being forced to troubleshoot the path chosen by the sharp recanalisation devices available today. With Traversa, we were able to choose the angle and the length of the throw of the needle. This enabled us to pick the pathway and if we did not like it, we were able to readjust. I think that allowed us to safely get through the occlusions and the stents.”
VeinWay CEO Jordan Pollack stated that his company’s “mission is to give surgeons the control they need to recanalise the veins of their patients safely, in a timely manner, and successfully. In doing so, we hope to inspire physicians to perform more venous recanalisations for the patients that need it to relieve pain and improve mobility. The procedure at University of Michigan Health was a huge step in changing the medical landscape of venous recanalisation. We would like to thank the US FDA for approving the use of Traversa in this first compassionate use case as well as Drs Williams and Khaja for their agreement to try something new. We were honoured to be of service.”
Interventional News’ most popular stories for the month of February included news from the Pan Arab Interventional Radiology Society annual meeting (PAIRS; 11–14 February, Dubai, UAE), along with other global meetings from the first couple of months of 2023; the announcement of Abbott’s acquisition of Cardiovascular Systems; and two articles from interventional radiologists themselves about the cutting-edge of ablation and embolization in their areas of the specialty—women’s health and interventional oncology (IO).
Biotronik announced the US Food and Drug Administration (FDA) 510(k) clearance and CE mark of its Oscar (One Solution: Cross. Adjust. Restore) multifunctional peripheral catheter.
Abbott and Cardiovascular Systems (CSI) have announced a definitive agreement for Abbott to acquire CSI. Under terms of the agreement, CSI stockholders will receive US$20 per common share at a total expected equity value of approximately US$890 million.
Karim Abd El Tawab (Ain Shams University Hospitals, Cairo, Egypt) wrote about his experiences using interventional radiology (IR) techniques, including ablation and coil embolization, to treat pelvic varicosities in women.
The Magic Touch percutaneous transluminal angioplasty (PTA) sirolimus drug-coated balloon catheter (DCB) has received investigational device exemption (IDE) for the treatment of below-the-knee (BTK) atherosclerotic lesions in peripheral arterial disease (PAD).
A number of speakers took to the stage at the International Symposium on Endovascular Therapies (ISET; 16–19 January 2023, Miami Beach, USA) to debate the ‘ambulatory shift’ that is currently taking place in the interventional space.
Riad Salem (Northwestern University, Chicago, USA) took to the PAIRS podium to give insight into a new frontier in IO—yttrium 90 (Y90) microspheres to deliver targeted radiation to glioblastoma.
Mina S Makary (Ohio State University Wexner Medical Center, Columbus, USA) and Warren A Campbell IV (Ohio State University, also Columbus) share their take on the impact histotripsy stands to make on the ablation space within IO.
Few adverse events are connected to the use of inferior vena cava (IVC) filters to help prevent deep vein blood clots from developing into pulmonary embolisms (PE), according to the findings of the PRESERVE trial.
Clinical Laserthermia Systems Americas (CLS)’s Tranbergthermal therapy system will be evaluated for safety and efficacy in treating low- to medium-risk prostate cancer patients outside of a hospital setting.
During the Society of Interventional Oncology (SIO) 2023 annual scientific meeting (19–23 January, Washington DC, USA), a panel of speakers delivered presentations on why patient-centred care is important, and how to provide it most effectively.
Jafar Golzarian
Copyright: 2019 Solares Photography Inc.
Jafar Golzarian Copyright: 2019 Solares Photography Inc.
The keynote lecture on day one of the Pan Arab Interventional Radiology Society annual meeting (PAIRS; 11–14 February, Dubai, UAE) advocated a simultaneously global and local approach when it comes to conducting research in interventional radiology (IR), and when innovating. Jafar Golzarian (University of Minnesota, Minneapolis, USA) talked delegates through the rationale for basing ideas for research and new medical devices or products on what is already familiar—or ‘local’—while bearing in mind that international collaboration with societies and individuals from other geographical regions can lead to more cost-effective innovations.
Citing the USA as an example of a country that invests a relatively large proportion of gross domestic product (GDP) in its healthcare system and health research, Golzarian made the point that “clearly, putting more money in […] is not the answer,” adding that “the current [system] is not sustainable”. According to the speaker, “it takes somewhere between US$5 and 10 million to get a US Food and Drug Administration [FDA] 510(k) class II approval” for a new medical device, hence the need, he believes, for a new way of innovating and researching in healthcare, and more specifically the IR field.
Golzarian conveyed his optimism despite this high financial burden on innovators—“innovation does not have to come with a cost”. Illustrating this, he cited the Fairembo concept—the use of suture fragments as an embolic—which is “feasible, safe” and “inexpensive”. With this in mind, Golzarian urged budding innovators among the delegates to ask themselves “how can [their idea] help other people across the globe while being affordable?” Posing questions, he continued, is “important for the younger generation”, as is getting “frustrated” and “out of your comfort zone”, as this can often lead to finding a solution to the clinical problem that has elicited the questions and frustration in the first place. The solution, Golzarian supplemented, as exemplified by Fairembo, is to “always consider cost” and “material availability locally”. This being said, it is key not to sacrifice quality, was the presenter’s final words on innovation, before transitioning to speak on the similar issue faced by those wishing to pursue research—the high cost of doing so.
“Usually what people think,” the presenter averred, is that research is not worth their while—because of a “lack of ideas”, but also sometimes because they consider it to be too time-consuming and expensive. However, Golzarian assured, “research is not as complex as we think […] we need to demystify [it].” Conceding that multicentre, randomised trials are valuable, the speaker opined that, in IR, what is “probably most significant is real-world research”, but that knowing the outcomes of one’s procedure is vital. “Reflecting on complications is a very good start,” Golzarian shared.
Addressing the younger interventional radiologists in attendance once again, the speaker advocated for beginning a research endeavour with the procedures “you perform the most”, as well as doing a “thorough literature search”. Then, “you can start to fill the gap” if there seems to be one in the existing evidence. Golzarian then returned to a previous point—that “cost should always be a consideration”. This may prompt research into cheaper materials that could substitute those used currently, and, even better, those which could be “useful globally”.
A personal anecdote led Golzarian to emphasise how crucial cost and collaboration considerations are when it comes to research—over the last 10 years, he has sought to conduct a trial with 110 patients comparing prostate artery embolization [PAE] to a sham procedure. Despite generous funding from the Society of Interventional Radiology (SIR) Foundation, Golzarian admitted that “we could not find enough money”. With this in mind, the presenter concluded that he was “sure” that current prohibitive costs associated with research and innovation need not continue to pose a barrier to entry for aspiring investigators and innovators—rather it is a case of harnessing this issue creatively to seek a solution in international collaboration. The status quo is “not sustainable,” the speaker reaffirmed, and that this necessitates a “change in the landscape”.
ReCor Medical and its parent company, Otsuka Medical Devices, recently announced that primary endpoint results from the RADIANCE II pivotal trial were published in the Journal of the American Medical Association (JAMA). Study results showed that the Paradise ultrasound renal denervation (uRDN) system successfully reduced blood pressure compared to sham. In addition, pooled analysis results from the combined primary efficacy endpoint and safety data from RADIANCE SOLO, RADIANCE TRIO, and RADIANCE II were concurrently published in JAMA Cardiology. Results of the pooled analysis showed a consistent blood pressure lowering effect across a broad range of hypertension, including mild to moderate and resistant hypertension.
RADIANCE II is a randomised, sham-controlled US Food and Drug Administration (FDA) investigational device exemption (IDE) pivotal trial of the Paradise uRDN system in the treatment of patients with uncontrolled hypertension. Conducted as an international multicentre study at more than 60 study centres in eight countries, 224 patients with uncontrolled hypertension were randomised 2:1 to uRDN or a sham.
Patients were to remain off antihypertensive medications throughout the two months of follow-up unless specified blood pressure criteria were exceeded. At the two-month primary efficacy endpoint, patients treated with the Paradise uRDN system had a mean reduction in daytime ambulatory systolic blood pressure of -7.9 mmHg, compared to a reduction of -1.8 mmHg in the sham arm, corresponding to a statistically significant and clinically relevant between-group difference of -6.3mmHg (p<0.0001). The study also achieved its primary safety composite outcome with no major adverse events observed.
Concurrently published in JAMA Cardiology, the RADIANCE pooled analysis includes data from more than 500 patients randomised in the three studies from ReCor’s RADIANCE global programme: RADIANCE-HTN TRIO, which studied patients with resistant hypertension, and RADIANCE-HTN SOLO and RADIANCE II, which studied patients with mild-moderate hypertension.
The combined dataset showed an overall reduction in daytime ambulatory systolic blood pressure in the uRDN group of -8.5mmHg with a difference between treatment and sham at two months of -5.9mmHg (p<0.0001), favouring uRDN. Blood pressure results were similarly positive in the 24-hour, night-time, home, and office measures. A favourable safety profile was consistently observed following uRDN treatment across the studies.
“The results of the RADIANCE clinical trials are meaningful in that they solidify the role of the Paradise uRDN system as an adjunctive therapy for hypertension treatment, in addition to medications and lifestyle modification. Having three consistent sham-controlled clinical trials demonstrating that the Paradise uRDN system can safely lower blood pressure across a range of patients is a very high bar to have met,” said co-principal investigator Ajay Kirtane (New York-Presbyterian Hospital, New York, USA).
Co-principal investigator Michel Azizi (Université Paris Cité, Hôpital Européen Georges Pompidou, Paris, France) added: “The pooled analysis of RADIANCE SOLO, TRIO, and RADIANCE II shows a remarkable consistency of effect in patients with mild to moderate hypertension and those with resistant hypertension. These results are in line with the new 2023 consensus statement of the European Society of Cardiology (ESC) Council on Hypertension and the European Association of Percutaneous Cardiovascular Interventions (EAPCI). The publication of these results in JAMA and JAMA Cardiology will bring the evidence of the performance of uRDN in the treatment of hypertension to a broad audience of physicians.”
“With hypertension being a leading cause of cardiovascular disease worldwide, it is vital that we help patients with an effective therapy to reduce blood pressure. We are pleased that the RADIANCE clinical trials have repeatedly shown that the Paradise uRDN system can successfully reduce blood pressure in a broad range of patients,” said ReCor president and CEO, Lara Barghout. “ReCor is focused on bringing the Paradise uRDN system to patients and their physicians as a treatment option in the near future.”
Genicular nerve radiofrequency ablation is a minimally invasive treatment for knee pain due to osteoarthritis of the knee, and can significantly reduce pain, especially for adults who are 50 and older, according to new research to be presented the Society of Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA). This is the first time a study has examined patient demographics, prior surgical history and other clinical characteristics that may predict the level of pain reduction after treatment.
“We know this treatment has clear benefits in reducing pain and improving the ability to do everyday activities for patients,” said Kaitlin Carrato, chief resident in interventional radiology (IR) at MedStar Georgetown University Hospital (Washington DC, USA). “But now that we know it is particularly helpful for those over 50 years old, it may mean that those with chronic pain conditions, like arthritis, would benefit more from this treatment than patients suffering acute pain, such as an injury.”
Interventional radiologists perform genicular nerve radiofrequency ablation by image guidance to place probe needles next to the nerves of the knee that can send pain signals to the brain. The probes generate radio waves, creating a ball of heat to dull or destroy the pain nerve endings. These nerves do not control muscles or affect balance, making the procedure safe. Furthermore, patients leave with plasters, not stitches. The treatment in other studies has been shown to last for approximately six months to up to two years.
The study examined pain reduction for 36 patients using the visual analogue scale and the Western Ontario McMaster Universities Osteoarthritis (WOMAC) pain scale. Researchers evaluated whether pain reduction levels were influenced by demographics and clinical characteristics, such as age, gender, body mass index, history of prior surgery and history of fibromyalgia.
Before treatment, patients had a mean baseline VAS of 8.58 and a mean baseline WOMAC of 66.6. After treatment, all study participants experienced a statistically significant reduction in pain. The mean VAS of 8.58 decreased to 5.02, while the mean WOMAC score decreased from 66.6 to 41. The greatest increase in functionality and decrease in pain was recorded for patients 50 and older compared to younger participants.
“Roughly one in four US adults have knee pain,” said John B Smirniotopoulos, an interventional radiologist at MedStar Georgetown University Hospital. “This treatment can offer many of those people a chance to enjoy everyday activities and regain a higher quality of life by decreasing the pain that they experience on a daily basis.”
During a dedicated media briefing held by SIR, Smirniotopoulos commented on how “rewarding” it is to see the patients return to the clinic for follow-up at regular intervals following their ablation treatment. The progress seen now, overall, at over a year in most cases is “possibly to a degree that [patients] did not expect and maybe that we did not even expect”.
The researchers are currently conducting long-term studies into this treatment that dive deeper into what other factors could predict how well the treatment will work. The same treatment is also conducted with shoulder, hips and sacroiliac joints, where the spine connects to the pelvis.
A minimally invasive treatment that injects allograft disc tissue into the spine to relieve pain associated with degenerative disc disease provides significant improvement in pain and function over a sustained period, according to new research to be presented at the Society of Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA).
The treatment, known as viable disc allograft supplementation, injects specialised cells and fluid into a patient’s damaged disc. The cells of the injected fluid encourage the cells in the damaged disc to regenerate with healthy tissue.
“The significant improvement in pain and function is promising for patients living with chronic low back pain—a condition that can greatly impact a person’s quality of life,” said lead author Douglas Beall, chief of radiology at Clinical Radiology of Oklahoma (Oklahoma City, USA). “Back pain is the leading cause of limited activity and workplace absenteeism. This treatment may help patients return to a normal activity level for a longer period of time.”
Fifty patients at nine sites participated in this three-year voluntary extension of the randomised control ‘Viable allograft supplemented disc regeneration in the treatment of patients With low back pain’ (VAST) trial, with 46 receiving allograft treatment and four receiving saline. The treatment group was similar to the patient population at the start of the trial in age, sex, race, ethnicity, body mass index and smoking status. Pain levels were evaluated using the visual analogue scale and functionality was measured using the Oswestry Disability Index (ODI).
Sixty percent of patients who received allograft treatment for chronic low back pain reported a greater-than-50% improvement in pain and 70% of patients reported more than a 20-point improvement in their ODI scores. There were no persistent adverse events reported.
Degenerative disc disease is the leading cause of chronic low back pain, one of the world’s most common medical conditions. It occurs when the discs that cushion the spine’s vertebra begin to wear away. Because the discs help to facilitate movement and flexibility, the condition leads to pain and reduced functionality.
“Existing treatment for chronic low back pain due to degenerative disc disease is often ineffective or the effects are short-lived,” said Beall. “We need better treatments for this condition since conservative care is not providing the long-term outcomes that patients deserve. Injectable allograft treatment might be the answer for many people.”
Use of allograft could even help decrease opioid use among patients with chronic low back pain, researchers said, which would be especially meaningful for younger patients who have years of function and quality of life to look forward to. In a media briefing held by SIR ahead of the annual meeting, Beall expanded on this to say that the potential impact of the treatment is “huge”, as this type of chronic back pain is “very common—maybe even one of the most common disease processes known to man”.
The treatment requires no incisions and patients are able to go home on the same day.
Prostate artery embolization (PAE) provides long-term effectiveness in treating urinary symptoms from an enlarged prostate gland, according to new research to be presented at the Society of Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA).
In the largest long-term North American study, 1,000 patients who underwent PAE reported significant sustained relief, up to six years, from lower urinary tract symptoms (LUTS) or urinary retention due to benign prostate hyperplasia (BPH).
“Our study shows that PAE is a highly effective treatment whose long-term outcomes include sustained LUTS relief and significant improvement in quality of life,” said senior author Shivank Bhatia, chair of Interventional Radiology (IR) at the University of Miami Miller School of Medicine (Miami, USA). “Of 18 million men in the USA eligible for BPH treatment, many avoid all treatments because of the widely known risks of surgery, particularly sexual side effects and leakage. PAE avoids these risks while achieving long-term clinical results.”
With PAE, interventional radiologists inject tiny particles into arteries that feed the prostate gland, reducing its blood supply and thereby shrinking it. Researchers characterised the treatment as showing “great short- to mid-term results” and positive long-term outcomes in self-reported symptom relief. In a media briefing organised by SIR ahead of the annual meeting, Bhatia responded to a question on the nature of the particle used for his six-year study—”they are acrylic polymer coated with gelatine”. He added that while the particles are permanent, as opposed to resorbable, they carry a positive charge, where blood is negative, thereby ensuring that they do not move through the bloodstream “to the brain, but stay within the organ itself”.
Participants reported dramatic improvements on the 35-point International Prostate Symptom Score, which ranks symptoms as mild, moderate or severe. Preprocedure, patients reported a mean score of 23, in the “severe” range. But in less than a year, they achieved a score of six, with “mild” symptoms persisting throughout the six-year study – a response similar to that following surgery for BPH. However, PAE does not negatively impact sexual function. Study participants were also asked a quality-of-life question: “If you were to spend the rest of your life with your urinary condition just the way it is now, how would you feel about that?” Preprocedure, the mean score was 5 or “mostly dissatisfied,” but within a year, the score was 1, or “mostly satisfied,” a ranking that also continued throughout.
PAE has a well established safety profile, as shown in repeated studies in the 10 years since it was first used. But interventional radiologists said most men are unaware of this treatment option. Most will avoid surgery and may instead take medication for years, even as BPH worsens, potentially leading to bladder failure.
“Patients choose PAE to avoid the side effects of current medications for BPH, which can include erectile dysfunction, painful or difficult urination, constipation, dizziness or fatigue,” said the study’s lead author Andrew Richardson, a senior resident at Jackson Memorial Hospital (Miami, USA). “PAE is an alternative not just to surgery but also to lifelong medication.”
Among the study’s findings was a persistent, years-long reduction in prostate size. However, Bhatia noted that prostate size reduction is not the only goal in long-term effectiveness. “Treatment should make the prostate softer as well as smaller – as opposed to smaller but remaining hard, which will still cause urinary symptoms.”
Bhatia and Richardson encourage patients to learn about all options for enlarged prostate symptoms, talk to various physicians and then decide what is best for them. Bhatia says, “One size does not fit all when it comes to treating BPH.”
The Journal of Vascular and Interventional Radiology (JVIR) published a paper in January 2023 examining the potential barrier that the name of the interventional radiology (IR) specialty poses to the US public’s understanding of the role of interventional radiologists. Mina Makary et al (The Ohio State University Wexner Medical Center, Columbus, USA) found that “less than half” of those surveyed were able to identify interventional radiologists as doctors.
Their findings also revealed that most IR referral patients who ended up having surgery “stated that a lack of IR awareness played a role in their decision”. The authors make recommendations, in their paper titled ‘Public awareness of IR: Population-based analysis of the current state and pathways for improvement’, of how to improve recognition and understanding of IR among the general public, which include patient education delivered by primary care providers.
The authors embarked on the study in order to “evaluate IR awareness among the public and identify methods for improvement”. One thousand participants responded to 69 questions anonymously on Amazon’s Mechanical Turk crowdsourcing platform, which required either Likert Scale or free text answers. The authors justified their choice of platform “to obtain a more accurate and reliable assessment of the current rate of IR awareness”, compared to previous study samples. The questions prompted respondents on their “medical and IR-specific knowledge, preferred methods of medical information acquisition, and suggestions for improving IR awareness”.
The study’s results
With regards to study results, 39.8% of participants were able to place IR as a medical specialty in and of itself—this specialty status is the case in the USA, where it is not elsewhere, such as in the UK. This is “improved” from 2000, when data demonstrated that only 2% of the US population knew what interventional radiologists did. Less than half of respondents knew that IR involved medical procedures, with over half feeling that the name of the IR specialty was “too ambiguous” and 458 stated that they wanted to “learn more” about it. Makary et al also specify that they found “no correlation between age, income level, residence, or race” and level of IR awareness.
As stated above, there were respondents who themselves had been offered an IR procedure, numbering 113, and of these, 66 also had the option of undergoing surgery. Twenty patients then went on to say that their choice of surgery over minimally invasive IR treatment was influenced by a “lack of IR awareness”, which amounted to 71% of those who chose a surgical procedure. This is despite the finding that “92% of participants preferred undergoing a minimally invasive procedure over surgery”.
Suggested solutions
Regarding the solutions to the lack of awareness proposed to participants, in terms of an alternative name for IR, ‘minimally invasive radiology’ was “most preferred”, opted for by 21.3% of respondents. ‘Procedural radiologist’ and ‘radiological surgeon’ also featured among the top choices, garnering 18.4% and 14.6% of responses, respectively. “Short (<10-min) educational videos and increased patient education by primary care providers (PCPs) were among the most suggested ways to improve awareness,” the authors detail. Other suggestions posed to respondents, in order of popularity as per the study, included websites dedicated to the dissemination of information on IR, increased social media presence, and some form of advertising campaign promoting the specialty.
Based on their study, Makary et al were able to conclude that “a lack of IR awareness may underlie underutilisation. When presented with the knowledge that IR improves patient outcomes, minimally invasive procedures with an interventional radiologist are more often desired by the public over surgical options.” Moreover, the authors posit that the current level of IR awareness among the general populace is “further exacerbated by low IR awareness within PCPs, which has led to low referral rates and underexposure of patients to IR”. Makary and his co-authors make the point that “initiating and maintaining professional relationships [between interventional radiologists and] local PCPs is the first step to improving patient referrals to IR. As IR awareness is low amongst PCPs, strong emphasis should be placed on educating PCPs about common pathologies such as peripheral artery and venous disease, fibroids, [and] chronic pain, that IR physicians treat.”
The importance of continued conversation
Speaking to Interventional News about the results, Makary noted how “the overall low level of awareness was not surprising as most patients who come to us for care are not familiar with our specialty or our procedures until we meet them and explain what we can offer.” However, he went on to add that he “did find it interesting that most found the name ‘interventional radiology’ ambiguous, and that ‘minimally invasive radiologist’ was the most preferred alternative”. Expanding on the appetite for a possible name change for the specialty, Makary expressed hope that his and colleagues’ work could “[support] the conversation [in the USA] regarding the identity and name of [the IR] specialty and [provide] helpful insight as the specialty evolves”—not just in terms of nomenclature, but also “educating the public and other healthcare providers about IR and the value of our care”.
Microbot Medical has announced that Japan is the most recent global jurisdiction to recognise the unique interface design of the Liberty robotic system’s remote controller. The design patent, which was issued by the Japan Patent Office (JPO), complements similar design patent allowances in the USA and Europe, further strengthening the company’s global intellectual property (IP) portfolio.
“We believe the ability to perform an endovascular procedure remotely, while reducing radiation exposure and the physical strain due to wearing a lead vest for an extensive period of time, is a major benefit to the physician and patients,” commented Eyal Morag, the company’s chief medical officer. “By eliminating these issues, it allows the healthcare provider to better focus on delivering the best patient care to achieve better outcomes.”
During the recent animal study, as well as other physician-sponsored lab sessions in Europe and the Americas, when using the Liberty robotic system, physicians were given the option to use the remote-controlled activation from the safety and convenience of the interventional suite control room.
“The research and development team spent a considerable amount of time designing the remote controller for the Liberty robotic system and the recognition by Japan, along with other jurisdictions, proves that the design is unique and innovative,” commented Simon Sharon, general manager and chief technology officer at Microbot Medical. “We developed a controller that is ergonomic, and we believe is ready to meet the demands of the interventional radiologist community, aimed to allow users to perform procedures, safely and away from the radiation source.”
Sarah White (Medical College of Wisconsin, Milwaukee, USA) opened the liver interventional oncology (IO) session at the Pan Arab Interventional Radiology Society (PAIRS) annual meeting (11–14 February, Dubai, UAE) with a presentation that set out what she believes to be the salient points of the latest Barcelona Clinic Liver Cancer (BCLC) guidelines. Last updated in early 2022, White emphasised the fact that “many key aspects of hepatocellular carcinoma [HCC] treatment are still missing”, including combination therapy with transarterial chemoembolization (TACE) and ablation and transarterial radioembolization (TARE).
White began by outlining a “historical overview” of the BCLC guidelines. “Initially published as a prognostic system in 1999,” it was not “designed” to stage liver cancers, the presenter shared with attendees. Neither was it formulated using “guideline methodology,” White added. “Many recommendations are not supported by high-quality data.” Other limitations include metastatic and non-metastatic patients being combined into one category and treatment modalities “not [being] unique to disease stage,” White furthered, before stating that BCLC oncologic outcomes “are worse than other staging systems”. Providing a counterexample, White stated that the National Comprehensive Cancer Network (NCCN) guidelines, which have a “strict policy of who sits on the committee” and a “strict conflict of interest policy”, as well as a “methodological way to review all of the data [it deals with]”.
Nevertheless, the most recent update to the BCLC guidelines is “much more” in-depth compared to the first set, “largely because now we have nine drugs that we did not have in the past,” White attested.
What is new in the guidelines?
A first example of the 2022 additions is the focus on the “potential candidacy for liver transplantation” for patients with early-stage malignancies, which, White said, before had “never really been put in the guidelines”. Within the scope of this addition is recommendations on eligibility for transplant and alternatives for those who are not suitable, for reasons such as heart disease, for example, the presenter relayed. “Ablation is really frontline for a patient who is not a transplant candidate, whereas before, it was resection that was frontline,” White said, expanding on the latest change to advice. Now, the consensus is that ablation and resection are “really on a par”, according to the speaker, with some concerns surrounding recurrence after resection, which was not the case two decades ago.
Next, White addressed what the guidelines now recommend for patients unable to have any of the aforementioned treatments. “You will see that the algorithm recommends TACE and TARE. What this really is talking about is when you cannot do ablation because of the location of the tumour.”
For stage B liver cancers, White proceeded to convey to delegates, “instead of having one category there are now three. There are now multiple treatment approaches, whereas it used to be straight to chemoembolization.” The speaker also noted that for patients in this category, overall survival used to be 20 months with the old guidelines, but this is now “up to five years”. In summary, “no matter what [treatment you receive] the outcome is much better than it used to be,” White celebrated.
There is now also a “vast difference” when it comes to treatment guidelines for advanced-stage liver cancer, White said, elaborating by saying that “before, with portal vein invasion and metastatic implants, sorafenib was our only choice”. Overall survival was 11 months, whereas it is now greater than two years for these patients, the speaker underlined.
And what is missing?
“So, what did they fail to include?” White moved on to answer her own question, emphasising that one “really important” omission is the use of prospective data to compare ablation directly to resection. Moreover, she added, “the difference between ablation modalities—maybe that does not matter as long as you are in good hands, but there is no differentiation” between using a particular modality in a patient, versus choosing another.
“They [also] did not talk about liver-directed therapy [LDT] as a bridge to liver transplant,” White lamented. “At my centre, it is an 18-month waiting period,” she explained, going on to say that waiting for a patient with 3cm HCC for that duration may take them outside of the transplant criteria—LDT can ensure they remain eligible, on the other hand. LDT is also an option for those who are not on the transplant waiting list, White went on, as it can confer an increase in overall survival, yet this too is not referenced in the 2022 update. Likewise, LDT in the setting of advanced or extrahepatic disease—the guidelines recommend “systemic therapy only”, the prudence of which in the context of an isolated lesion White invited the audience to question.
Adding to her list of important omissions in the most recent iteration of guidelines, White stated that radiation segmentectomy “either by itself or in addition to ablation” would have merited inclusion as “we have some pretty good data surrounding that”. Similarly, TACE and ablation for lesions over 3cm—”I do not think that anyone in this room would use a [single modality alone]” on a lesion greater than 3cm, White averred.
“They do not even talk about stereotactic body radiation therapy [SBRT], or the different TACE modalities. Drug-eluting beads are not the same as conventional TACE. And there is no stratification of when we should be using which one,” White continued. “[Neither do they] talk about radioembolization in the setting of intermediate disease [although] there are really good data,” the presenter said, rounding off the section of her presentation addressing the 2022 edition omissions.
On a final note, White acknowledged that “[failure] to mention any kind of combination therapy is likely because there are still data coming out—with many trials in the pipeline”. The speaker anticipated that the release of new data will continue to ”drastically change the BCLC guidelines,” which, while evolving in line with research findings, “has many limitations as a staging system”.
Matthew S Johnson (Copyright: The Trustees of Indiana University)
Few adverse events are connected to the use of inferior vena cava (IVC) filters to help prevent deep vein blood clots from developing into pulmonary embolisms (PE), according to the findings of the Predicting the safety and effectiveness of inferior vena cava filters (PRESERVE) trial, published jointly in the Journal of Vascular and Interventional Radiology (JVIR) and the Journal of Vascular Surgery Venous and Lymphatics (JVS-VL).
PRESERVE is a US Food and Drug Administration (FDA)-directed multicentre, prospective, open-label, non-randomised trial that studied the safety and efficacy of IVC filters from six manufacturers. It was a joint effort of the Society of Interventional Radiology (SIR) and the Society for Vascular Surgery (SVS). The study was conducted at 54 sites in the USA between 10 October 2015 and 31 March 2019. During that time, filters were implanted in 1,421 patients, of whom 1,019 patients had an existing deep vein thrombosis (DVT) or pulmonary embolism (PE).
Researchers found that IVC filters were effective in helping to prevent PEs in patients experiencing a DVT where anticoagulation medicines failed or were not an option for the patient. Approximately half of the patients in the study had their filters removed within three months of placement without complication or recurrence of DVT or PE, according to study authors.
“The question should not be only ‘should we place a filter?’ but ‘how should we offer comprehensive filter-inclusive care of patients with venous blood clots, comprised of a detailed patient evaluation, a plan for retrieval after placement, and frequent follow-up with evaluation for filter removal or replacement,’” said Matthew S Johnson, an interventional radiologist and professor of radiology and surgery at Indiana University School of Medicine (Indianapolis, USA) and co-principal investigator on PRESERVE. “PRESERVE showed what questions we should ask as clinicians: ‘does this person continue to require protection against PE, and, in light of changing clinical status and available therapies, is the current filter needed?’ and then make an informed decision on how to continue care.”
David L Gillespie spoke exclusively on the PRESERVE trial at VEITHsymposium 2022.
“DVTs and PEs are a significant cause of death worldwide and understanding fully how tools like IVC filters can be used to prevent the progression of a DVT into a PE allow physicians to safely treat patients at risk of death from venous thromboembolism [VTE]” said David L Gillespie, a vascular surgeon at Beth Israel Deaconess Medical Center (Brockton, USA), and co-principal investigator on PRESERVE. “Now that the study is complete, we now have a roadmap for better filter utilisation. We need to solidify a clearer set of practice guidelines for venous thromboembolic disease, based on its symptoms, location and complications. Further studies will focus on how the different manifestations of venous thromboembolic disease may benefit from filter-inclusive care.”
Speaking at VEITHsymposium 2022 (15–19 November, New York, USA), Gillespie outlined that “approximately ten years ago or so, the clinical management of patients with VTE and the prophylaxis of potential VTE in trauma patients was not well studied with regard to the use of IVC filters”. The result of the PRESERVE trial has been that “essentially, these filters are safe and effective for therapeutic [and prophylactic] use in the patient population [in question],” Gillespie continued, and this, despite the “challenges” of the COVID-19 pandemic, the “high dropout rate”, and the fact that “a large number of patients” had their filters removed.
To date, PRESERVE is the largest prospective study investigating the real-world patient outcomes of IVC filter use. “This trial represents an important step in collaborating across specialties to benefit the health and safety of our patients,” said SIR President Parag J Patel (Medical College of Wisconsin, Milwaukee, USA). “Thanks to the work of Drs Johnson and Gillespie and all the investigators and patients involved in the trial, we now have higher quality evidence to support appropriate utilisation and management of IVC filters in patients with venous thromboembolic disease.”
“Congratulations to Dr Gillespie, Dr Johnson and their many colleagues for shepherding this large collaborative multispecialty, multicentre clinical trial to completion,” said Michael C Dalsing (Indiana University Health, Indianapolis, USA), president of the SVS. “This highly impactful study provides the real-world evidence needed when recommending IVC filter placement to protect our patients from a potentially lethal disease and when to remove that filter after it has accomplished the desired effect. It is a stellar example of collaboration across specialties for the betterment of patient care.”
David Gillespie (Boston, USA) talks to Interventional News about the PRESERVE study—established by the Society for Vascular Surgery and Society of Interventional Radiology—which is the largest prospective study to investigate real-world outcomes with contemporary use of inferior vena cava (IVC) filters in patients who are at risk for venous thromboembolism.
A total of 1,421 patients were enrolled at 54 sites across the USA and had IVC filters from seven different manufacturers placed. “It was a monumental task to enrol patients and get them to complete” states Gillespie, who goes on to outline some of the key challenges the study faced, including the changing regulatory landscape, COVID-19 and a large patient drop-out rate.
Despite these hurdles, PRESERVE has essentially shown in a non-randomised study that IVC filters “are safe and effective for therapeutic use” as well as in prophylactic use “with continued monitoring and early removal”.
Humacyte, a clinical-stage biotechnology platform company developing universally implantable bioengineered human tissues and advanced tissue constructs and organ systems at commercial scale, today announced the publication of “Six-year outcomes of a phase two study of human-tissue engineered blood vessels for peripheral arterial bypass,” in the Journal of Vascular Surgery-Vascular Science.
The publication describes the long-term analysis of the company’s phase two clinical trial evaluating the bioengineered human acellular vessel (HAV) as a conduit in patients with symptomatic peripheral artery disease (PAD). The researchers concluded that “the infection-resistant, off-the-shelf human acellular vessel could provide a durable alternative conduit in the arterial circuit setting, to restore lower extremity blood supply in patients with peripheral artery disease”.
This paper reports a 60% overall secondary patency rate for the phase two study at 72 months, including all patients originally enrolled, and was estimated by Kaplan Meier analysis. There was no evidence of graft rejection or infection. Additionally, no patients underwent amputation of the affected limb out to six years—a meaningful clinical and quality-of-life result, as amputation is a common outcome in many severe PAD patients. Furthermore, no patients reported pain at rest or ischemic ulcers on the affected legs. Researchers reported that “these data have demonstrated the durability of the HAV and suggest the occurrence of cellular remodelling by the host.”
Piotr Gutowski (Pomeranian Medical University, Szczecin, Poland), lead manuscript author, commented: “Synthetic grafts can be limited due to poorly matched mechanical compliance, risk of infection, and variable patency rates. Furthermore, cryopreserved allogenic grafts are limited due to poor durability, thrombosis, and mechanical degradation. The HAV is designed to be consistent in size, durable in high-pressure circulation, show no clinical immunological response, and remodel with the patient’s own cells.”
“With an increasing global prevalence of PAD and more than 200 million people living with the disease, there still remains a major unmet need for long-term solutions,” said Laura Niklason, chief executive officer of Humacyte. “Key findings of this publication show that the HAV was durable and performed well in a medically complex patient cohort for long-term treatment of PAD. The HAV is designed to be available off-the-shelf, has the potential for a regenerative capacity and low infection risk, all of which are particularly important in this patient group.”
The HAV has been evaluated in eight clinical studies in the USA, Europe, and Israel, including an ongoing phase two/three clinical trial in vascular trauma and an ongoing phase three trial as a haemodialysis access in end-stage kidney disease. The HAV is an investigational product and has not been approved for sale by the US Food and Drug Administration (FDA) or any international regulatory agency.
Shape Memory Medical has announced the first patient treated in Germany as part of the EMBO postmarket surveillance registry (EMBO-PMS), the company’s prospective, multicentre registry study of its Impede and Impede-FX embolization plugs when used for peripheral vascular embolization.
The patient was treated by Götz Martin Richter, chairman of the Clinics for Diagnostic and Interventional Radiology at the Center for Minimally Invasive Medicine, Klinikum Stuttgart (Stuttgart, Germany) in cooperation with the Clinic for Vascular Surgery, Endovascular Medicine and Transplant Surgery in the Klinikum Stuttgart.
The EMBO-PMS has been initiated at two centres in the UK and has now expanded to include up to ten centres in Germany, with the goal of treating up to 125 patients. Results thus far in the UK reflect treatment for conditions including iliac artery aneurysm, type II endoleak after thoracic endovascular aneurysm repair (TEVAR), type 1b endoleak after endovascular aneurysm repair (EVAR), gluteal artery aneurysm, and splenomegaly. “We are pleased to participate in this important study and look forward to the follow-up from our treated patients,” said Richter, who is also the principal investigator for the EMBO-PMS.
Both the Impede and Impede-FX embolization plugs incorporate Shape Memory Medical’s shape memory polymer, which is a porous, radiolucent, embolic scaffold that is crimped for catheter delivery and self-expands upon contact with blood, enabling conversion to organised thrombus followed by gradual healthy tissue formation. Preclinical and clinical studies have shown that shape memory polymer offers effective and predictable space filling, stable clot formation for embolization, and progressive healing as the material is absorbed.
“We look forward to collaborating with colleagues from Germany to add to the experience within EMBO-PMS,” said Robert Morgan, consultant vascular and interventional radiologist, St George’s NHS Trust (London, UK) and principal investigator, EMBO-PMS UK registry. “We are continuing to obtain data to support the safety and effectiveness of the Impede devices across a variety of peripheral vascular anatomies with technical success and target vessel thrombosis achieved in all cases,” continued Morgan.
What is the background to the ESC/EAPCI consensus statement on renal denervation?
This consensus document was deemed necessary because a significant amount of new sham-controlled trial evidence has become available. In the 2018 guidelines of the ESC and the European Society of Hypertension (ESH), device-based hypertension treatment was graded with a class 3 recommendation, not to be used routinely in clinical practice. There was a sentence added to the statement that until further evidence regarding the safety and efficacy becomes available these devices should not be used outside of clinical trials.
We felt it was important to re-evaluate the evidence that has aggregated after publication of the guidelines, and by now we have five sham-controlled clinical trials that have indeed proven the efficacy and safety of renal denervation in the presence and absence of antihypertensive drugs.
What have the recent trials shown and how are these reflected in the consensus statement?
We know it works in patients with and without antihypertensive medication, but this is a very broad potential patient population. We felt it is also important to provide some guidance on where denervation may be used in clinical practice and felt this should be reserved as a treatment option for patients with so-called “resistant” hypertension, meaning despite treatment with three antihypertensive drugs, they still have uncontrolled blood pressure values, as confirmed by office and ambulatory blood pressure.
Despite the fact that we have evidence that this works in a very broad potential patient population, we nailed it down, first and foremost, to patients with resistant hypertension. There is another potential indication for renal denervation and that is in patients where drugs are not tolerated, patients who are not willing or able to take antihypertensive drugs, and patients who express a preference to be treated with a device-based approach.
How significant a development is the consensus statement?
It is not the intent of the consensus statement to change people’s perception. The perception needs to be adapted according to the published trial evidence. This is really more to inform clinical practice.
What we did here is reach consensus on different statements. The challenge is who to treat within clinical practice, and this is the overall objective of such consensus statements. Which patients in which centres? How should the centres be trained? What are the potential complications of the procedure that interventionalists need to be informed about?
Are there “ideal” patients for renal denervation?
What we have to accept is that this is a treatment possibility for patients with uncontrolled blood pressure. It is not replacing drugs, it is not replacing lifestyle modification—that this is another approach available in our armamentarium to lower blood pressure. But, it is not exclusive. It is not renal denervation or nothing. Most patients we treat have undergone lifestyle modification, but it was unsuccessful. They have been treated with several drugs, are still uncontrolled and have high blood pressure and have high cardiovascular risk. In these patients it is another treatment that may bring blood pressure down.
You have studied renal denervation in great detail, how excited are you by this treatment?
We started the scientific evaluation of this approach 15 years ago. It is among the very, very few device-based treatments that has been investigated against and has beaten sham control. This is something we have to keep in mind. There has been a very rigorous evaluation of procedure, which is not available for other techniques that we are using every day. This is something we have to acknowledge, that we have a lot of clinical data, a lot of robust methodologically defined and properly designed studies conducted around the world and they have proven that this technology lowers blood pressure. You cannot question whether or not it works—it works—that is a statement, and now it is our responsibility as physicians to offer this to certain, but of course not all, patients at risk.
I am excited, of course, because it is about science, but this is probably among the last steps in the evaluation of this technology and this technique. We are working on a US Food and Drug Administration (FDA) submission so hopefully this will become available in the USA sometime soon. I think overall we are in good shape moving forward with this technology.
We are now looking into new indications such as heart failure, atrial fibrillation and ventricular tachycardia. We have registry data confirming that in those populations it is safe, and now we are heading off to new shores and among those are heart failure, certainly and arrhythmias are very interesting also.
Where are the gaps in our knowledge regarding renal denervation?
Identification of responders is the unmet need, something that we are investigating in clinical studies to get further insights, and has never become available even for antihypertensive drugs. I am not sure if we will succeed in this with renal denervation, but we are still trying.
The second question is whether or not this blood pressure lowering translates into improvements in outcomes. We know that blood pressure as LDL [low-density lipoprotein] cholesterol closely associate with cardiovascular morbidity and mortality, and when you lower blood pressure or LDL cholesterol, it is believed that it lowers morbidity and mortality too, so I am pretty confident that this will translate into improved outcomes—but it has not yet been shown.
Compared to other races, African American patients are more likely to experience premature arteriovenous (AV) graft failure in the treatment of advanced kidney failure, according to a study published in Radiology, a journal of the Radiological Society of North America (RSNA).
One treatment option for advanced kidney failure is haemodialysis, or dialysis; to aid with dialysis treatment, physicians need to create access to the bloodstream by installing either an AV fistula, catheter or an AV graft.
An AV graft is the placement of a flexible tube to create a path between an artery and a vein. While AV fistulas are the preferred method for dialysis access, some patients may need to receive an AV graft when their veins are too small or weak for a fistula.
“Patients with renal failure often receive an AV graft to facilitate dialysis,” said study co-author Hillary J Mull, an investigator for the Center for Healthcare Organization and Implementation Research for the VA Boston Healthcare System and associate professor of surgery at Boston University Chobanian & Avedisian School of Medicine (Boston, USA). “These grafts can fail over time, requiring an interventional radiologist to perform a maintenance procedure. If the procedure has a complication within 30 days, the patient will need another procedure right away to fix the problem.”
Prior studies have found racial and ethnic disparities in the treatment of chronic kidney disease and dialysis access. Additionally, women and minority populations are more likely to receive AV grafts rather than other forms of grafts that are less likely to have complications.
“The literature has clearly illustrated higher rates of access failure with AV grafts, as well as the disappointing disparities in outcomes for African Americans undergoing dialysis access interventions,” said the study’s lead author Mikhail CSS Higgins, assistant professor from the Department of Radiology at Boston University Chobanian & Avedisian School of Medicine.
To identify the racial disparities among premature AV graft failures, researchers used medical data from the Veterans Health Association (VHA).
In this retrospective cohort study, researchers identified 1,950 AV graft procedures in 995 patients (mostly men) across 61 VHA facilities. The average age of the patients was 69 years. Most of the procedures (60%) involved African American patients and patients residing in the southern portion of the USA (51%). A majority of the procedures were performed by interventional radiologists.
Premature graft failures occurred in 11% of the procedures. After controlling for a variety of factors, such as socioeconomic and comorbidities, African American race was associated with premature graft failure.
“African American patients are more vulnerable to experiencing early dialysis access dysfunction and failure when compared to their other racial counterparts. This relative predisposition to this complication represents a disparity in care and adverse outcomes in a largely understudied population, namely the VHA system,” Higgins said.
Out of the 61 VHA facilities included in the study, 30 of them had interventional radiology (IR) resident training programmes, which had lower rates of premature graft failure. Notably, there was no evidence of racial disparities in the outcome of the 1,057 procedures that were conducted in facilities with an IR resident training programme. However, the researchers stress that the association between facilities with teaching programmes and health outcomes should be studied further.
“We cannot say that patients should find hospitals with teaching programmes, as our results do not show this direct relationship,” Mull said. “Rather, teaching is associated with equitable patient outcomes for dialysis access maintenance procedures and there are likely unmeasured factors associated with teaching programmes that influence this relationship.”
According to Higgins, the results of this study suggest that there are environmental and cultural characteristics of teaching sites that help to reduce racial disparities in patient care and health outcomes.
The researchers believe that future studies should investigate the occurrence of graft failures in non-VHA populations as well as other factors, such as provider, facility, and regional practices, that reduce racial disparities in premature graft failure.
Mechanical thrombectomy appears to be a safe and technically feasible treatment option for ischaemic strokes caused by primary isolated anterior cerebral artery (ACA) occlusions in more distal locations. The procedure—which is more traditionally used in large vessel occlusions (LVOs) of the middle cerebral artery (MCA) and internal carotid artery (ICA)—has also demonstrated similar clinical outcomes to best medical management with or without intravenous thrombolysis (IVT).
These are the key findings of an international registry study published recently in the journal Radiology by Lukas Meyer (University Medical Center Hamburg-Eppendorf, Hamburg, Germany) et al.
As Meyer and his co-authors point out in their introduction, despite thrombectomy being a potential therapeutic option in distal occlusion stroke, current evidence supporting its benefits specifically for primary, isolated distal medium vessel occlusions (MeVOs) in the ACA is, to their knowledge, “generally unknown”.
They aimed to elucidate this issue through a case-control study of the TOPMOST registry—an international, retrospective, multicentre, observational registry of patients treated for distal cerebral artery occlusion stroke. Meyer et al analysed the clinical and safety outcomes of thrombectomy for primary, isolated ACA occlusions of the more distal A2–A4 segments, compared to best medical management with or without IVT, in daily clinical practice between January 2013 and October 2021.
In this study, endovascular reperfusion was evaluated using the modified thrombolysis in cerebral infarction (mTICI) scale. The number of reperfusion manoeuvres was counted—including first-pass effect (mTICI 3 after first attempt)—and a final reperfusion result of mTICI 2b–3 was considered a successful thrombectomy, with intervention times and the rate of intervention-related serious adverse events also being detailed.
Regarding clinical measures, early outcome was assessed via the median improvement of National Institutes of Health Stroke Scale (NIHSS) scores at 24 hours, while functional outcomes were defined as favourable (modified Rankin Scale [mRS] score of 0–2) or excellent (mRS 0–1) at 90 days. Safety was assessed by the occurrence of mortality—during hospitalisation and at day 90—as well as symptomatic intracerebral haemorrhages (ICHs).
From a total of 154 patients who met the inclusion criteria, Meyer et al detail that 110 patients (median age=76 years, 50 men) underwent propensity score matching, with 55 having received a thrombectomy and 55 receiving best medical management. Distal MVOs were located in the A2 (53% of patients), A3 (45%) and A4 (2%) segments.
Prior to propensity score matching, the authors observed a median time from symptom onset to groin puncture of 195 minutes across 94 patients who received a thrombectomy. The median number of reperfusion attempts was one, and successful thrombectomy (mTICI grade 2b–3) was achieved in 81% of patients. Complete reperfusion (mTICI 3) was achieved in 67% of patients—including a first-pass effect rate in 41%. Symptomatic and asymptomatic bleeding events were observed in 2% and 14% of patients, respectively, before propensity score matching.
The authors report a median 24-hour NIHSS point decrease of 2 in the thrombectomy cohort compared to 1 in the best medical management cohort. In addition, the distribution of mRS scores at 90 days showed “no evidence of a statistically significant difference” between the thrombectomy and non-thrombectomy cohorts regarding mRS scores of 0–1 (38% vs 33%, respectively) and 0–2 (49% in both groups).
“There was no evidence of statistically significant differences when clinical and safety outcomes were stratified by occlusion site,” Meyer et al add. “This finding remained stable if we included the last known mRS scores in patients with missing long-term follow-up.”
Functional outcomes stratified across several subgroups—including age, sex, occlusion site, NIHSS on admission, and whether IVT was given—showed no evidence of a difference in 90-day mRS score distributions between the two cohorts. Ninety-day mortality rates were similar with (22%) and without (31%) thrombectomy too, as were in-hospital mortality rates (11% and 10%, respectively).
“We did not find a treatment effect in favour of one therapy option after propensity matching,” Meyer et al conclude. “These results show the potential efficacy of [best medical management] in the subgroup of ACA distal medium vessel occlusion. Mechanical thrombectomy may be considered a technically feasible treatment option for acute ischaemic stroke due to primary isolated occlusions in the A2 and A3 segments because it can lead to high rates of successful reperfusion associated with favourable long-term outcome and did not result in increased rates of symptomatic bleeding events compared with [best medical management] if patients were treated at tertiary stroke centres.
“Nevertheless, patient selection for treatment allocation requires further investigation to identify patients who will benefit the most from available treatment options.”
And, in spite of their study’s potential limitations—including its retrospective design, small sample size, and absence of some clinical data—the authors assert that these results “reinforce clinical equipoise, and encourage ongoing and upcoming randomised trials investigating treatment options for distal MeVO stroke”.
Xeltis has raised €32 million in a Series D2 equity fundraise, backed by a syndicate of current and new investors, which the company says will enable it to progress its clinical programmes into pivotal trials.
Investors include Grand Pharma, DaVita Venture Group, EQT Life Sciences, Invest-NL and others.
Xeltis’ proprietary endogenous tissue restoration (ETR) platform utilises an advanced polymer-based material which triggers the body’s natural healing response to regenerate the patient’s own tissue around it, forming new, living and long-lasting vessels and valves.
The company’s most advanced program, aXess, is a vascular access graft for patients with chronic kidney disease (CKD) requiring haemodialysis. Xeltis is also pursuing clinical programmes in pulmonary valve replacement and coronary artery bypass grafts.
Alongside the equity fundraise, Xeltis and Grand Pharma have completed a license deal, covering Greater China, for aXess and other potential haemodialysis products developed under the same technology platform. Under the agreement, Grand Pharma will have exclusive rights to develop, produce and commercialise these products in Greater China.
“The strategic support of Grand Pharma and DaVita alongside our existing investor base represents a strong validation of our technology and potential to transform the landscape of cardiovascular surgery. We remain focused on progressing our aXess clinical trials, as well as exploring our next steps in other indications,” commented Eliane Schutte, CEO of Xeltis. “Securing this financing is an important milestone for Xeltis. We are proud to have attracted such high-profile investors to our company and look forward to leveraging their respective insights—from clinical expertise to the product development lifecycle—as we continue on the next phase of growth.”
Rana Tarek M Khafagy is a consultant interventional radiologist based at Ain Shams University Hospital (Cairo, Egypt). In her capacity as head of the Pan Arab Interventional Radiology Society (PAIRS) residents, fellows and students (RFS) section committee, she sat down with Interventional News at the PAIRS annual meeting (11–14 February, Dubai, UAE) to discuss her journey into interventional radiology (IR), and how it is for those in training now, both in her home country and across the Middle East-North Africa (MENA) region.
“At my institution, we have one department, radiology and IR […] During your residency and fellowship you are obliged to do rotations in [diagnostic and IR],” Khafagy explained, setting the scene for the discussion. However, she went on, “when I entered in 2014, the IR department was not open to [all] the residents and fellows. There were no females at that time in the IR unit—I had wanted to have training at the IR unit since my first year in residency, however only a few male seniors agreed to help me. I used to finish my daywork duties in the department then go and stay there [and observe].”
The significance of being a woman in IR in the MENA region
Khafagy proceeded to recount how most of those in the IR unit at the time thought that “she [would] get bored and leave,” but, as is evident now given her position, she did not. “Most of the consultants were not accepting females in the unit,” she elaborated, describing the situation as “very challenging”. Khafagy believes that this is due to stereotyping women as unable to cope with the stress of a specialty like IR and the on-calls that they bring, and as too squeamish to deal with blood. “However, to be honest,” she conceded, “I did meet some male consultants who supported me, including my mentor.”
In 2021, “me and another woman in my class the first [women] to be consultants at the IR unit,” Khafagy shared. “Our presence as residents and fellows and now consultants has encouraged many females after us to join the IR unit and has helped to open the gate to them—if you were to come to the department now you would see a lot of women training at the IR unit.” Khafagy illustrated how much of the initial negativity towards female interventional radiologists at her hospital has dissipated since—women are now “welcomed” and “no one is offending [us], no one is avoiding [us]”.
On the subject of the IR procedures that she specialises in, Khafagy emphasised the importance of being skilled in all of them, not only in women’s health-related procedures. For example, she does prostate artery embolization, and bronchial artery embolization, presenting on the latter at PAIRS 2023. However—and this is a point that was echoed in an information session later on during the meeting, on routes into IR in the MENA region—there is a particular demand in the region, given the religious and cultural environment, for female interventional radiologists, as female patients often require their doctor to be a woman. Therefore, women’s health procedures, such as uterine fibroid embolization make up more of a female interventional radiologist’s caseload than they do a male’s in the region.
Training in IR in the MENA region
Khafagy then moved on to discuss her role in PAIRS’ RFS section—“ the team is very active and there are also many females on the team.” Team members are “mainly from Egypt, Saudi Arabia, also from Algeria, Syria, Qatar, UAE and Morocco—many countries,” she detailed. There are even members involved in the section’s activities despite currently being based outside of the MENA region—“the UK, USA, Canada and Germany,” she added.
This prompted the question of whether she had spent time during her training outside of Egypt—“I spent a few months in the UK,” she replied. Contextualising this fact, she explained that it is “not that common to do fellowships abroad in Egypt” but more common in Saudi Arabia and the UAE. “Officially, in the UAE they do not have an IR training programme. So they have to go abroad, do their training and come back as a consultant.” The implications of this reality were addressed in the aforementioned information session—attendees expressed their concern that interventional radiologists-in-training often leave the region for an IR programme and do not return. Khafagy shed further light on this subject, clarifying that it is mainly in Saudi Arabia and Egypt, of all the MENA countries, that trainees embark on IR training.
Khafagy then segued into addressing awareness of her specialty in the MENA region—”Maybe five, six years ago, if you asked medical students [in the region] if they knew anything about IR, they would definitely say no. As for now, I cannot say that everyone knows about it, but I believe they have heard about it. And this is very important regardless of the specialty they will go into eventually —they need to know about IR so they can refer patients.” The progress towards more widespread recognition of IR in the MENA region is, in part, due to the efforts of PAIRS , who “had a vision” that involved a focus on “promotion” of IR. An example of this is the ‘I am PAIRS’ campaign done in several Middle Eastern countries, for which Khafagy is a regional leader in Egypt, she shared. This has centred around gathering students at a dedicated event “so that [medical students would know about [IR]”. Many of the students were “amazed, giving very good feedback,” Khafagy supplemented.
PAIRS’s residents, students and fellows focus
The inspiration for tailored RFS initiatives came from “peers at the Society of Interventional Radiology [SIR] and Cardiovascular Interventional Radiological Society of Europe [CIRSE],” Khafagy went on to say. The committee itself started as “just a little chat”—with Ayah Megahed (Yale New Haven Hospital, Bridgeport, USA). “She is a colleague of mine training in the USA and she is working for the SIR RFS. She said to me, why do we not have something like this for PAIRS?” Khafagy relayed by way of an origin story for the section. They agreed that the concept had “very good potential,” given the success of the US and European counterparts. “Being interested in working with the juniors and as a regional leader in Egypt of ‘I am PAIRS’, I spoke to Ayman Al Sibaie [Rashid Hospital, Dubai, UAE], the president of PAIRS and Karim Abd El Tawab [also Ain Shams University Hospital], the secretary,” Khafagy recounted, the PAIRS board was supportive and thus the PAIRS RFS section came into being. “I led it when I was a fellow and still [am leading it],” she added.
“Our vision, which is matching with PAIRS’s vision ‘Investing in Youth’ is mainly to increase awareness of IR among students and to support the residents and fellows because in a lot of countries, they are also involved in diagnostic work […] so we are working to encourage them [towards IR],” Khafagy summarised. Also of central importance to her though, as reflected throughout the discussion, is boosting the image of women in IR in the MENA region. She celebrated the fact that the section members say they “see many females presenting—this enhances their vision of females being able to [work in IR].” The goal is to continue what the section has achieved to date with supporting the students and juniors, Khafagy concluded.
Danial Jilani is an interventional radiologist based at Northwestern Medicine Palos Hospital (Chicago, USA), who uses the SKATER™ drainage catheter (Argon Medical) as his “go-to” catheter for a range of both “bread and butter” and more complex interventional radiology (IR) procedures. He spoke to Interventional News about why SKATER works so well for him and his patients, and the findings of a recent bench test that compared SKATER to other percutaneous drainage catheters on the market.
For Jilani, SKATER’s “all-purpose” suitability means he can use it for pneumothoraxes, chest tubes, pleural effusions, nephrostomy and biliary procedures. Moreover, SKATER works for sclerotherapy too. Ethyl alcohol and doxycycline used in this type of treatment can “break certain catheters down”, Jilani explains, however SKATER “can tolerate both these agents—having the luxury to handle both is one of the advantages of this catheter.”
There are multiple “subtle differences” that set SKATER apart, Jilani goes on to tell Interventional News. The recent findings of a bench test1, which compared a range of percutaneous drainage catheters on the points of kink resistance, flow rate and ‘pushability’ shed light on these, he reports. Among those tested, SKATER, made of a blend of durable polyurethane material, was found to be the most kink-resistant, in turn improving flow rate. Jilani notes that SKATER demonstrated a high flow rate during the bench test, with 8Fr catheters and mini pigtail catheter loops—in spite of their small size, which would typically reduce flow rate. The large, skived holes are one of the features that allow for maximal drainage.
Jilani then speaks to the ‘intrinsic mechanisms’ of SKATER that, in the bench test, helped it fare more favourably than other drainage catheters. One was the “locking shoulder tip, which decreases buckling during insertion.” The hydrophilic coating also reduces friction as it is being inserted. The force required to insert the SKATER was 22% less than for some of the other catheters, and 70% less with the mini-loop catheter, Jilani relays, opining that this is an “underrated” feature of drainage catheters across the board.¹
Case study 1: Nephrostomy tube placement for malignant obstruction
Clinical presentation: Renal failure secondary to obstruction from bladder mass; Imaging findings: CT scan demonstrating severe hydronephrosis (top arrow) from malignant bladder mass (bottom arrows)Imaging findings: Image-guided 8Fr percutaneous nephrostomy tube placement. Faint contrast opacifies the obstructed right kidney/renal collecting system
Citing a further benefit of using SKATER, Jilani goes on to elucidate how the position markers on the SKATER are “especially helpful when doing a procedure under CT [computed tomography] guidance, as you are stepping in and out of the room and do not have your hands on the catheter the whole time”. Precision, as facilitated by these markers, is key as in a few millimetres “you can be in a structure you do not want to be in,” Jilani elaborates.
In addition, the low-profile locking system SKATER offers is, Jilani says, “so easy to use that I was able to teach myself [how to use it]”. Providing anecdotal context for these positive data, Jilani then explains how inserting a drainage catheter into a cirrhotic liver can feel like “pushing up against a rock”, making buckling more likely. Hence, SKATER’s proven ‘pushability’ is advantageous. “The more difficulty you have [overall] during the case, the more things can go wrong and the more time the patient spends on the table,” Jilani admits, suggesting a further reason why having a drainage catheter that can perform as SKATER did in the bench test, across all the aspects assessed, is beneficial.
Case study 2: Chest tube placement for spontaneous pneumothorax in patient with COPD
Imaging findings: Chest radiograph after placement of an 8Fr pigtail chest tube demonstrating resolution of pneumothoraxClinical presentation: Shortness of breath, increasing oxygen requirement, chest pain; Imaging findings: Chest radiograph demonstrates large right pneumothorax
Jilani goes into detail about how using SKATER can yield advantages for patients and their outcomes—“I am a firm believer that the faster you can drain an abscess, the less risk there is of recurrence.” Chronic abscesses can last for months, which, in turn, requires long-term drainage. However, with SKATER’s “large skived holes and fast flow rates”, catheter drainage is more efficient. “For the majority of patients with abscesses, we place these [SKATER] catheters and within a week, we can remove it, sometimes even faster,” Jilani relays.
Inadequate flow rate, such as seen in other types of catheters that kink more readily, means drainage takes longer, Jilani reiterates. “We follow our patients closely,” he asserts, meaning that he can say with some confidence that he has noticed “far fewer instances of kinking” compared to earlier in his career when he used other drainage catheters. Longer drainage time can lead to occlusion from bacteria and fibrin build-up and more catheter exchanges, prolonging the overall time the patient has a catheter in. Even without complications, Jilani explains that having a drainage catheter in for a long time is “very inconvenient” for patients—“they are attached to a bag […] which can make day-to-day activities hard.”
Case study 3: Percutaneous drainage of infected bladder/acute cholecystitis
Clinical presentation: Right upper quadrant/epigastric pain, fever, elevated liver enzymes; Imaging findings: CT of gallbladder showing pericholecystic inflammatory changes, gallbladder wall thickening, and small gallstones consistent with acute cholecystitisImaging findings: Intraprocedural image related to 8Fr percutaneous transhepatic cholecystostomy drainage. Contrast opacifies obstructed gallbladder. Faint filling defects noted, consistent with gallstones
The improved patient outcomes—faster drainage and therefore fewer complications related to chronic abscesses and catheterisation—that SKATER facilitates, reduce healthcare costs, Jilani is also keen to acknowledge.
To round off the discussion, Jilani summarises what it is about SKATER that makes it his “go-to” drainage catheter. “The subtle differences make an impact,” he states, referring back to SKATER’s high level of performance in the bench test: for kink resistance, flow rate and ‘pushability’. The evidence the test produced supports Jilani’s own clinical experience that “[the SKATER catheter] works well and is associated with better patient outcomes”, meaning he can continue to use it with confidence.
References: 1. Data on File. Bench Testing Comparative Data Relative to Drainage Catheter Performance: An analysis of pigtail drainage catheter systems.
Renal denervation represents another treatment option in patients with uncontrolled resistant hypertension and may be used in selected patients deemed intolerant to antihypertensive drugs.
These are among the messages of a new consensus statement published in EuroIntervention following a review of evidence by the European Society of Cardiology (ESC) Council on Hypertension and the European Association of Percutaneous Cardiovascular Interventions (EAPCI).
Initial excitement over the potential for renal denervation as a treatment for hypertension was dampened following the release of initial results of the SYMPLICITY HTN-3 trial in 2014 in which it was shown that at six months, renal denervation did not elicit significant incremental blood pressure lowering benefit compared with a sham procedure.
Subsequently, joint ESC and European Society of Hypertension (ESH) guidelines on the management of arterial hypertension, published in 2018, advocated against the routine use of device-based therapies for hypertension, until further evidence of their safety and efficacy came to light. However, newer sham-controlled trials have revitalised hope in the potential of renal denervation, with a number showing statistically significant and clinically meaningful reductions in blood pressure.
In producing the latest consensus statement, the ESC and EAPCI expert panel have reviewed evidence from several “second-generation” randomised, sham-controlled trials, which, they say, demonstrate the safety and the blood-pressure lowering efficacy of radiofrequency and ultrasound renal denervation. The second generation of trials have involved either the Symplicity Spyral (Medtronic) multi-electrode radiofrequency device or the Paradise (ReCor Medical) ultrasound system.
“Since the publication of the 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension, several high-quality, randomised, sham-controlled trials have been published, demonstrating a blood-pressure-lowering efficacy over 24 hours for both radiofrequency and ultrasound renal denervation in a broad spectrum of patients whose hypertension ranges from mild-to-moderate to severe and resistant,” Emanuele Barbato (University of Rome, Rome, Italy) and colleagues write in EuroIntervention.
“This expert group proposes that renal denervation is an adjunct treatment option in uncontrolled resistant hypertension, confirmed by ambulatory blood pressure measurements, despite best efforts at lifestyle and pharmacological interventions,” the statement notes. Renal denervation may also be used in patients who are unable to tolerate antihypertensive medications in the long term, the writing committee has concluded.
The authors of the paper suggest that a shared decision-making process, taking into account the patient’s global cardiovascular risk and the presence of hypertension-mediated organ damage, should be followed when considering renal denervation as a treatment option.
Furthermore, they state that interventionalists require expertise in renal interventions and specific training in renal denervation procedures. “Centres performing these procedures require the skills and resources to deal with potential complications,” Barbato et al state.
Presently both the Symplicity Spyral and Paradise system carry a CE mark, and Medtronic and ReCor both filed premarket approval applications to the US Food and Drug Administration (FDA) in late 2022 for their respective devices.
“To date, there are at least 18 societal and/or expert consensus documents published, and the increasing number of citations seems to parallel the mounting evidence for renal denervation therapy,” David Kandzari (Piedmont Heart Institute and Cardiovascular Services, Atlanta, USA), a member of the writing committee for the ESC/EAPCI consensus statement and prinicipal investigator in the SPYRAL HTN-ON MED trial, told Cardiovascular News. “In all, these documents are important for providing clinicians with guidance regarding the evidence basis for renal denervation safety and effectiveness, patient selection, and procedural technique. Many of the documents also underscore the need for shared-decision making and accounting for patient preference.
“The ESC/EAPCI document offers the most contemporary evidence and informed clinical considerations for renal denervation, including recommendations for not only patient selection but also for institutions related to renal denervation programme development, patient selection, and operator proficiency.”
Delcath Systems has announced it has submitted a new drug application (NDA) resubmission to the US Food and Drug Administration (FDA) for the Hepzato Kit (melphalan hydrochloride for injection/hepatic delivery system, or melphalan/HDS) seeking approval for the treatment of patients with unresectable hepatic-dominant metastatic ocular melanoma (mOM).
The resubmission is in response to a Complete Response Letter (CRL) from the US FDA. The NDA resubmission contains comprehensive data and information to address all issues identified in the CRL. The US FDA is expected to determine whether the resubmission constitutes a complete response and is eligible for review within 30 days. Once accepted for review by the US FDA, a new prescription drug user fee amendments (PDUFA) action date will be established for the Hepzato Kit application.
The FOCUS trial
The FOCUS trial evaluated the safety and efficacy of treatment with Hepzato Kit for patients with mOM. The primary endpoint of overall response rate (ORR) was assessed by an independent review committee per RECIST (Response evaluation criteria in solid tumours) version 1.1. Per protocol, patients were treated every six to eight weeks for a maximum of six cycles. Tumour responses were assessed every 12 weeks (+/- 2 weeks) until disease progression.
As previously reported, treatment with Hepzato Kit in the treated population resulted in an ORR of 36.3% (95% confidence interval [CI]: 26.44, 47.01) including 7.7% of patients with a complete response (CR). The median duration of response was 14 months (95% CI: 8.31, 17.74) and the disease control rate (DCR) was 73.6% (95% CI: 63.35, 82.31).
In addition, the NDA resubmission includes updated estimated median overall survival (OS) of 20.53 months (95% CI: 16.79, 25.26) and updated estimated OS at one year of 0.80 (95% CI: 0.70, 0.87). Delcath Systems will continue to follow patients until May 2023 (24 months after the last patient’s last treatment).
There were no treatment-related deaths in the trial. This is consistent with Chemosat, the HDS device component of Hepzato Kit, approved in Europe under a CE mark to deliver melphalan to the liver. The safety data submitted in the NDA is consistent with the Chemosat safety data documented in numerous European single-centre and multicentre publications.
Guerbet has shared in a press release that it has commercially launched Elucirem (gadopiclenol) and the first patient has received a dosing. This is following US Food and Drug Administration (FDA) approval in 2022. The first dosing took place at the Hospital of the University of Pennsylvania (Philadelphia, USA).
“Having the ability to use a lower dose of gadolinium, while seeing the diagnostic value and good tolerance during the magnetic resonance imaging [MRI] would be a significant improvement for the practice of neuroradiology,” said Laurie A Loevner, Division Chief, Neuroradiology and Professor of Radiology at the Perelman School of Medicine, University of Pennsylvania.
Biotronik has announced the US Food and Drug Administration (FDA) 510(k) clearance and CE mark of its Oscar (One Solution: Cross. Adjust. Restore) multifunctional peripheral catheter.
The company notes in a press release that Oscar is intended for percutaneous transluminal interventions in the peripheral vasculature. The device was developed to provide support during access into and to dilate stenoses in femoral, popliteal and infrapopliteal arteries.
The Oscar peripheral multifunctional catheter is comprised of three user-adjustable components:
The Oscar system will be available in 11 total size configurations with either 0.014″/4Fr or 0.018″/6Fr guidewire/introducer sheath compatibility, Biotronik states. Additional standalone Oscar PTA balloons are also available separately to be used with the Oscar support catheter.
The company details that the Oscar support catheter and dilator are used in tandem to enable lesion access and crossing with a compatible guidewire, offering a wide range of support strength, adjusted with the extension of the dilator. At its strongest support level, Biotronik claims, the combination provides up to 55% more pushability than the leading 0.035″ support catheter.
The first procedure with the Oscar system in the USA was performed by Jihad A Mustapha (Advanced Cardiac & Vascular Centers for Amputation Prevention, Grand Rapids, USA). “Oscar is a game-changing product. In cases where we had previously failed with multiple treatment approaches, the Oscar catheter made it possible to succeed, while also saving time and reducing how long the patient needs to spend on the table. This is one of the best support systems I have ever used, and the length-adjustable balloon functionality is exceptional,” stated Mustapha.
More than 70 cases have been performed in US hospitals with the Oscar device as part of Biotronik’s pre-launch evaluations. Despite highly complex disease, the Oscar catheter demonstrated a 90% crossing success rate and a PTA technical success rate of 95%, the company reveals. In some cases, physicians had previously tried and failed with traditional crossing devices and strategies.
Biotronik advises that the product will be commercially available in the USA starting in the Spring of 2023 and in CE mark accepting regions in the second half of 2023.
In a recent study of patients with intermittent claudication (IC) caused by isolated superficial femoral artery (SFA) lesions, researchers found that primary stenting conferred benefits in health-related quality of life (HRQoL) at 36 months from treatment compared with best medical therapy (BMT) alone, which were lost at the 60-month mark, where a high crossover rate affected the power of the final analysis.
Results of the study were recently published online in the European Journal of Vascular and Endovascular Surgery (EJVES). The investigators—led by Thordur Gunnarsson (Lund University, Lund, Sweden)— highlight their previous finding that primary stenting of the SFA in IC increased HRQoL after 12 and 24 months in this trial. The current paper, they note, presents an extended follow-up of HRQoL 36 and 60 months after randomisation.
This was a multicentre randomised controlled trial conducted at seven vascular clinics in Sweden between 2010 and 2020, which included 100 patients randomised to either primary stenting and BMT (n=48) or BMT alone (n=52) followed for 60 months.
Gunnarsson et al detail that HRQoL—which they assessed using the Short-Form Health Survey (SF-36) and EuroQoL 5 dimensions (EQ5D) 36 and 60 months after randomisation—was the primary outcome. Walking Impairment Questionnaire (WIQ) score, reinterventions, progression to chronic limb-threatening ischaemia (CLTI), amputation, and death were secondary outcomes.
The authors report that, at 36-month follow-up, the stent group (n=32) had “significantly better” scores in the SF- 36 domain Role Physical (RP, p=0.023) and the Physical Component Summary (PCS, p=0.032) compared to the control group (n=30), however, there was no significant difference in EQ5D scores (p=0.523).
In addition, they reveal that WIQ was also “significantly better” compared to the control group (p=0.029) at 36 months.
At 60-month follow-up, Gunnarsson and colleagues found no significant difference in HRQoL between the stent (n=31) and the control group (n=32), and that there was no difference in progression to CLTI, amputation (2.1% vs. 1.9%) or mortality (14.6% vs. 15.4%) between groups. The authors point out that crossover from control to stent group was 25% at this later follow-up point.
The authors recognise that their study has some limitations. They note, for example, that as the study was originally designed to detect differences in the primary outcome at 24 months with an expected 10% loss to follow-up, both the prolonged follow-up and additional loss of patients at 36 and 60 months and the 25% crossover from the control group to stent at 60 months “negatively affected the power of the analysis”. In future trials of invasive treatment of IC, they write, crossover and loss to follow-up “need to be taken into account”.
“We interpret the trial results in favour of stent treatment for at least 36 months for physical HRQoL measures for the [IC] patient,” Gunnarsson et al write in the discussion of their findings. While they acknowledge that the trial does not give robust evidence for a lasting effect of stenting until 60 months, it suggests instead that a “transient period” of improved HRQoL “might be valuable” for an elderly vascular patient.
They summarise the wider impact their results might have: “This trial provides information relevant when presenting treatment options for patients as well as for health authorities.”
“When I relocated to Lebanon, I was the only person with practical experience and expertise in EVAR [endovascular aneurysm repair] in the Middle East.” It was thus that Aghiad Al-Kutoubi became the first in the Arab world to perform this procedure, in doing so changing the face of interventional radiology (IR) practice in the region. Now adjunct professor of diagnostic and interventional radiology at the American University of Beirut Medical Center (AUBMC; Beirut, Lebanon), Al-Kutoubi tells Interventional News how he came to embark on his IR career; recounts the obstacles he overcame to develop an IR service in Beirut, as well as those encountered in practising IR in the country more broadly; and imparts his knowledge on how best to train interventional radiologists.
What attracted you to a career in IR?
This really happened by chance. I was attracted to radiology because of the potential of contributing to the diagnosis of disease in multiple organs and the interaction with different medical teams. My career in radiology started when I was accepted for training at St Mary’s Hospital (London, UK) in September 1977. The head of the department was David Sutton, a pioneer of angiography and its application in systems including the heart and central nervous system. I was mesmerised by the art of diagnostic angiography.
Interventional procedures were only just emerging—treatment of gastrointestinal bleeding with vasoconstrictive medication, preoperative embolization of renal tumours, venous procedures, etc. I still vividly remember the first iliac angioplasty procedure that I assisted in as a registrar in 1978 and the impressive result. At the same time, ultrasound and computed tomography (CT) scanning became established tools. These modalities offered opportunities for biopsy and drainage procedures. I think I benefitted from these developments and unconsciously became an interventionalist as well as a diagnostician.
Who were your mentors?
In my earlier years, I was influenced by many people—my parents, some teachers at school and university, and close associates in my home country, Syria. In my radiology career, I owe gratitude to David Sutton for inspiring me and Oscar Craig for his wisdom and guidance. I must also mention Averil Mansfield, who provided the best collaboration, knowledge and support.
Could you describe a particularly memorable case of yours?
There are so many, but I will mention two. The first was in the UK—a patient who developed an arteriovenous fistula between the origin of the left carotid artery and innominate vein after pinning for clavicular fracture. Suitable stent grafts were not available commercially and the case was treated with the combined efforts of IR and vascular surgery, who provided a segment of the saphenous vein that I attached to a Palmaz stent and placed it at the origin of the left carotid artery through a direct carotid approach with balloon occlusion of the innominate vein. A second similar stent was needed but we were elated that the procedure was clinically successful, and the patient avoided thoracotomy.
The second was in Lebanon, a few months after I performed the first endovascular aortic case. A patient presented to the emergency room with type B dissection and a large leak from the distal aortic arch into the left thorax, as well as lower limb ischaemia. As luck would have had it, I had a thoracic stent graft for another elective case that was the appropriate size for sealing the point of bleeding. Balloon fenestration of the abdominal aorta treated his limb ischaemia. I saw this patient repeatedly until he passed away 20 years later from complications of lymphoma.
What were the challenges involved in building up the IR service at the AUBMC?
Although some IR procedures were being performed by colleagues, there were challenges at multiple levels. These included acceptance of new procedures; perception of competition by other specialties such as vascular surgery; acceptance of new treatment methods by insurance and third-party payers; the cost of procedures to patients; availability of appropriate equipment and paramedical staff; anaesthesia and sedation requirements; availability of devices; and the volume of cases versus training requirements for residents. Some of these challenges required a gentle approach, with firmness and perseverance required in others. The result was of benefit not only to the AUBMC, but to the practice of IR in other centres in Lebanon and in the Middle East as experiences were exchanged and knowledge shared.
Having practised in both the UK and Lebanon, what are the main differences/similarities associated with IR in these two geographical areas?
I think the fundamental difference is financial. In the UK, my practice was mainly in the UK’s National Health Service (NHS), where the person with the most expertise would be the one to perform the medical procedure and this was also true in the private sector. In Lebanon, the health system is spearheaded mainly by established and respected private institutions, for example, the American University of Beirut. In contrast, the public sector provides a relatively small proportion of healthcare with limited resources and lags behind in terms of state of-the-art treatments. Private healthcare requires someone to pay for the treatment of the patient be it the patients themselves, insurance companies or other third-party payers who have to accept the value of the treatment procedure and frequently find reasons for not paying in full.
The other issue is remuneration of medical staff. Whereas in the NHS the physician is not paid per procedure, in Lebanon, the income of the physician is dependent on referral and case numbers. Therefore, a surgeon may choose not to refer the patient for an IR procedure because he would lose income. Joint arrangements for management became necessary to provide a balanced approach to the treatment of patients and to avoid ‘competition’.
How did you come to be the first to carry out an EVAR in the Arab world? What do you remember about how it came about, and the impact it has had since?
At St Mary’s, we had embraced this new approach to the treatment of aortic aneurysms early on, and I, with my vascular surgical colleague John Wolfe, treated a few patients with stent grafts for aortic aneurysms using the first-generation devices. When I relocated to Lebanon, I was the only person with practical experience and expertise in this field in the Middle East. Despite this, I had a hard time convincing colleagues of the value of this method and was, in fact, the target of efforts to stop its introduction until we had a patient who developed a false aneurysm of the thoracic aorta after coarctation surgery. I had, by that time, modernised the angiography suite and was able to convince the cardiothoracic surgeon Munir Obeid that this was an ideal case for stent graft placement. With his help, and that of Ghattas Khoury, another surgical colleague, I treated this patient successfully and she went home the following day. The publicity that followed resulted in referrals and soon patients were treated by various EVAR devices—the people who had resisted were now interested! I was able to present my work at various regional fora and got colleagues in other Arab countries to pursue this approach. The rest is history!
As someone who has a passion for educating the next generation, both in the UK and in the Arab world, what would you say are the priorities when it comes to making sure interventional radiologists-in-the-making receive the highest standard of training possible?
Interesting question! I think one of most important factors is the commitment of the trainers to training! Commitment of the trainee is no less important. Secondly, establishment of a comprehensive curriculum to take into account the modern, and ever-changing IR landscape—this is pivotal to ensuring the standard of training. After these first two steps, finding training centres that have the breadth of practice and case volume to meet the curriculum objectives is relatively easy. It may prove necessary for trainees to visit other centres to observe/train in procedures that are not done at their primary training centre.
What are your hobbies and interests outside of medicine?
I have pursued many sporting hobbies over the years but had to give some up after injuries. I now do scuba diving and golf, which I wish I could play better and more! Arabic calligraphy is a skill I was taught by my grandfather and I practise it occasionally, but I hope to spend more time at it. I guess grandparenting is the main ‘hobby’ now.
The Magic Touch percutaneous transluminal angioplasty (PTA) sirolimus drug-coated balloon catheter (DCB) has received investigational device exemption (IDE) for the treatment of below-the-knee (BTK) atherosclerotic lesions in peripheral arterial disease (PAD). Concept Medical received its first IDE approval for the Magic Touch for coronary in-stent restenosis (ISR) indication in September 2022. The Magic Touch has also been granted with a breakthrough device designation in BTK by the US Food and Drug Administration (FDA).
Currently, plain balloon angioplasty (POBA) is the standard of care for the treatment of the BTK arterial occlusion disease, along with paclitaxel-coated balloons, as well as stents. The IDE approval will allow Concept Medical to gather safety and effectiveness data for the Magic Touch PTA sirolimus-coated balloon to support a future premarket approval (PMA) in the USA, providing patients and physicians with an alternative product for the treatment of BTK arterial disease.
The CE-marked Magic Touch has already been widely studied in multiple clinical trials outside the USA and has shown promising safety and efficacy results. The product is currently being investigated in Europe in two randomised controlled trials (RCTs) for the BTK indication. The LIMES RCT is a study designed to compare the Magic Touch with POBA, while the Debate BTK Duell is compares the Concept Medical catheter with a paclitaxel-coated balloon catheter.
Sahil Parikh (Columbia University Irving Medical Center, New York, USA) stated that, “Concept Medical’s proposed clinical trial studying the Magic Touch PTA in BTK indication will collect significant data on safety and efficacy of the device, thus paving its way to treat patients in USA. With the sirolimus-coated balloon having already received an IDE approval in coronary arteries, and breakthrough device designations for multiple indications, along with the vast clinical data [outside the USA], it will surely be looked up to by the US physicians and patients with PAD.”
Edward Choke (Sengkang General Hospital, Singapore), one of the early investigators of the Magic Touch PTA balloon, is also conducting a RCT against POBA (FUTURE BTK) adds, “the field of BTK angioplasty needs effective solutions to its problem of poor patency rates. This is an exciting phase III trial that will determine whether the novel Magic Touch PTA can maintain the patency of BTK arteries for a longer period of time, compared with our current gold standard of POBA. This is a key goal in our efforts to reduce the number of repeated interventions and to save the legs of our patients with the severest form of PAD. If successful, this has the potential to be a game-changer.”
On day two of the Pan Arab Interventional Radiology Society annual meeting (PAIRS; 11–14 February, Dubai, UAE), Riad Salem (Northwestern University, Chicago, USA) took to the podium to give insight into a new frontier in interventional oncology (IO)—yttrium 90 (Y90) microspheres to deliver targeted radiation to glioblastoma (GBM). Drawing on experience treating liver cancer in such a way, Salem introduced delegates to how this neuro-oncological concept came about and informed them of the currently-recruiting FRONTIER trial—a feasibility study to evaluate the safety of the Therasphere GBM device in patients with recurrent GBM).
Salem began by clarifying for the audience that the glass Theraspheres (Boston Scientific) “are not an embolic-type therapy”, as some microspheres are, but rather, they deliver Y90 radiation. “Now the natural discussion [point would be] what about external beam radiotherapy [for GBM]?” Arguments against this approach, Salem countered, include the fractionated nature of the radiation, with multiple treatments, as well as the dose limits, “depending on how much brain you want to expose.” Non-target radiation is, equally, a reason that limitations exist in external beam radiation, the speaker added. On the other hand, he acknowledged that radiotherapy delivered transarterially can “precisely deliver” radiation exactly as predicted by cone-beam computed tomography (CBCT). There are “no major issues with adjacency to other structures, so that provides you with a therapeutic option”.
“What have we learned in the liver?” was Salem’s rhetorical question that reflected the subject of the session as a whole—IO outside the liver—and the answer was that “we can see exactly where [the Y90] has been deposited”. This means that one can accurately predict where necrosis will occur, the presenter explained, “in contradistinction” to external beam radiotherapy, which applies radiation to a “much larger area”. Applying these learnings in an area of “unmet need” is how the FRONTIER trial came about, as, Salem noted, “there are between 10,000 and 12,000 GBM cases in the USA and treating these patients can be “quite challenging”.
“One of the goals of treatment, initially, is debulking the tumour,” Salem went on, adding that unlike in the hepatic and other spaces, “R0 resections are rare because you want to limit how much brain you take out.” Recidivism around the area of resection is the result, the speaker detailed. “And there really are very few treatments that are effective and accepted second-line standards-of-care,” according to Salem—“you can re-resect, re-radiate, but there is no protocol”.
“So, the options that we currently have are surgical,” but as seen on flare images with magnetic resonance imaging (MRI), “there is [often] disease around the tumour”. Whether micrometastases or oedema, there is “a challenge” associated with dealing with this in addition, according to Salem. “How much are the surgeons going to resect?” The need to cover this larger zone also means that external beam radiotherapy comes with the risk of non-target radiation, the speaker supplemented. Recurrence and recidivism are problems in this disease condition no matter the approach, in Salem’s opinion.
“Credit is due to the Hopkins group, who completed a six-canine study on dogs having seizures,” the presenter went on to say, which “opened the door” to using Y90 for GBM. Compared to humans, the cerebral anatomy in dogs does not allow for “selective injections” when delivering the Y90, yet, Salem shared, “the dogs were able to tolerate these hemispheric treatments”.
Regarding the FRONTIER trial, Salem confirmed that “in humans, of course, we want to get much more selective, and this is something we will be able to share once data starts coming out”. In the Hopkins study, “all canines demonstrated initial reduction in tumour volume” and therefore, it is proof of concept, the speaker summed up.
“The FRONTIER trial is open and recruiting,” Salem told the audience, conceding that he was unable to divulge much more about the trial’s progress. Summarising the use of Y90 for GBM, the presenter relayed that “imaging is much more critical than in hepatic space and there is a level of cerebral vascular complexity that does not exist in the liver”. There are challenges to applying this product in the brain, such as the need to “re-engineer the microspheres” so as to use fewer than in the liver, however, “there is a lot of excitement [including] at prospect of treating meningiomas [in the future]”.
Clinical Laserthermia Systems Americas (CLS) and HALO Precision Diagnostics (HALO) have announced a letter of intent to evaluate the safety and short-term efficacy of CLS’s Tranbergthermal therapy system for treating low- to medium-risk prostate cancer patients with focal laser ablation (FLA) therapy outside of a hospital setting.
HALO will conduct an initial postmarket study treating up to 25 patients at one or more of its HALO ambulatory surgery centres. Upon completion of its evaluation, HALO and CLS will enter into discussions regarding HALO’s acquisition of the Tranberg laser system for use in some of its nationwide system of approximately 16 clinics.
Focal laser ablation of prostate tumours has demonstrated high levels of precision and accuracy with low risk of side effects, such as erectile dysfunction and urinary incontinence.
“CLS Americas is excited to begin this initial collaboration with HALO Precision Diagnostics to bring our minimally invasive, image-guided FLA treatment to patients in the convenience of their local urology doctor’s office or clinic,” said Michael Magnani, president of CLS Americas.
“HALO Precision Diagnostics is pleased to announce a formal relationship and initial postmarket study with CLS to evaluate its Tranberg laser for treating patients with image-guided, laser focal therapy,” stated Bernadette M Greenwood, chief research officer, HALO Precision Diagnostics. “CLS has a strong track record of safety and innovation with its Tranberg system and a history of successful clinical studies with leading academic and research institutions in the USA and European Union. We look forward to working with their team to help more patients access focal therapy.”
Abbott and Cardiovascular Systems (CSI) have announced a definitive agreement for Abbott to acquire CSI. Under terms of the agreement, CSI stockholders will receive US$20 per common share at a total expected equity value of approximately US$890 million.
CSI is a leader in devices for atherectomy, the procedural use of which can help maximise the benefits of standard balloon angioplasty or stent treatments in restoring blood flow in complex arterial disease. CSI also has an early-stage pipeline of complementary vascular intervention devices in development.
“The acquisition of CSI will add new, complementary technologies to Abbott’s leading vascular device offerings,” said Lisa Earnhardt, executive vice president, Medical Devices, Abbott.
“We are pleased to have reached an agreement with a leading global company that shares our passion for the development and commercialisation of innovative solutions for treating complex peripheral vascular disease and coronary artery disease,” said Scott Ward, CSI’s chairman, president, and chief executive officer.
Financial impact of the transaction
Upon closing, the transaction is expected to be neutral to Abbott’s recently issued 2023 ongoing earnings per share guidance.
The transaction, which has been approved by the boards of directors of CSI and Abbott, is subject to the approval of CSI stockholders and the satisfaction of customary closing conditions, including applicable regulatory approvals.
JP Morgan Securities LLC is serving as financial advisor to CSI.
Northeast Scientific announced this week it has received US Food and Drug Administration (FDA) 510(k) clearance for reprocessing the intravascular ultrasound (IVUS) Eagle Eye Platinum RX digital catheter (Philips).
CEO and founder, Craig Allmendinger shared his thoughts on the impact of adding another device to Northeast Scientific’s growing product portfolio: “The reprocessed Eagle Eye catheter is another high-cost complex interventional device that will bring considerable savings to office-based labs and hospital cath labs nationwide. Having reprocessed multiple sizes of the peripheral IVUS device for the last three years to great success, it was an easy choice to pursue the Eagle Eye version.”
Director of product development, Matt Farley commented: “As always, it is a testament to our team, from R&D to Product Development, Quality and Regulatory and the technicians helping do the work on validations. We’ve spent a lot of time honing in how we work through our product pipeline to submit 510(k)s and expect to have multiple submitted in 2023, the Eagle Eye is just the start.”
The company has said that it will have an additional announcement soon regarding when the NES Reprocessed Eagle Eye Platinum RX Digital IVUS Catheter device will be available for sale.
In the past two decades, there has been a shift in varicose vein management from conventional surgical treatments to outpatient interventional procedures. Depending on the type and site of the affected vein, patients now have many other treatment options—namely with ablation, glue, coil embolization and sclerotherapy. These minimally invasive options offer better disease control with maximal safety, less pain and less recurrence.
With increasing patient awareness, one of the common clinical scenarios interventionalists encounter now is female patients with pelvic varicosities associated with the presence of vulvar, perineal, inguinal, or gluteal varicose veins, sometimes also associated with lower-extremity varicosities.
The prevalence of vulvoperineal varices in the general population is still unknown. Yet, in a series of over 4,000 female vein clinic patients, as written about by J T Hobbs et al in a 1990 British Journal of Hospital Medicine paper, the incidence of vulvar varices was about 4%, rising to 40% in patients with pelvic venous insufficiency. These latter patients are typically multiparous women between 20 and 40 years of age suffering from coital aches, genital heaviness, discomfort, continuous arousal, as well as lower urinary symptoms in severe cases.
Despite it being a common problem, there are few publications discussing vulvoperineal varices management. Most of the treatment approaches are derived from case reports or very small case series. Management options include compression, ovarian and internal iliac veins embolization, surgical ligation or phlebectomy and ultrasound-guided sclerotherapy. The latter is becoming both the doctor and patient’s favourite treatment where suitable—being safe and almost painless. It involves injecting a sclerosing agent like polidocanol foam, which causes a biochemical reaction in the diseased vein that, in turn, causes the vein to collapse and harden, before it is then absorbed by the body. The use of vulvoperineal sclerotherapy has little evidence and is done under ultrasound guidance alone, which despite being sufficient for symptom improvement in most cases, does not allow full assessment of the veins going up to the pelvis.
This was our motive when developing direct fluoroscopic-guided sclerotherapy for vulvoperineal varices, which combines ultrasound guidance for vein puncture followed by contrast injection under real-time fluoroscopic guidance to assess all external genitalia veins and how they interact with pelvic and lower-limb veins.
We published the results on our first 70 patients in the Arab Journal of Interventional Radiology (AJIR) in 2021 and we have now treated more than 160 patients using this procedure.
Varices most commonly drain into the internal iliac veins through perineal and internal pudendal veins, and connections with the vaginal and external iliac veins were also noted. Ovarian venous connections were not as common as most of these patients had already undergone ovarian vein embolization prior to vulvar sclerotherapy.
Technical success was achieved in all cases, with all patients showing short-term improvement in their symptoms, whether from one or two sessions of sclerotherapy. For patients who completed a one-year follow-up, recurrence was found in only 7%. The rest of the patients showed a stable therapeutic effect with no recurring varices, pain, or labial swelling.
This new procedure will be discussed at the Pan Arab Interventional Radiology Society (PAIRS) annual congress that will take place in Dubai, UAE from 11–14 February. The congress provides the opportunity for all those interested in interventional radiology (IR) to network and improve their practice by attending sessions and workshops covering all categories of IR, including like interventional oncology, venous, embolization, aortic, women’s health and musculoskeletal, as well as a dedicated track for juniors with more than 150 speakers from all over the world.
Karim Abd El Tawab is a consultant interventional radiologist at Ain Shams University Hospitals, Cairo, Egypt.
Disclosures: Abd El Tawab is a member of PAIRS 2023’s Scientific Committee.
Interventional News’ most popular stories in the opening month of 2023 included news of first enrolments in clinical studies of peripheral arterial disease (PAD) and deep vein thrombosis (DVT), respectively; key takeaways from a conference myth-busting session centring on being a woman in interventional radiology (IR); and an update on patients treated with tumour-specific electroporation (TSE) in Ukraine.
Cardiovascular Systems Inc (CSI) recently announced initiation of the KAIZEN clinical study of its Diamondback 360 peripheral orbital atherectomy system (OAS) for the treatment of calcified plaque in patients with PAD.
Cardiovascular Systems (CSI) announced that Innova Vascular (Innova) has submitted a 510(k) premarket notification to the US Food and Drug Administration (FDA) for its thrombectomy devices intended to treat peripheral vascular disease.
Paula Novelli (University of Pittsburgh Medical Center, Pittsburgh, USA) put her own spin on a British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK) presentation titled ‘Women are more likely to work part-time’. She brought the perspective of ‘the only girl in the gang’—the gang being her IR team at Pittsburgh.
Inari Medical has announced that the first patient has been enrolled in DEFIANCE, a prospective randomised controlled trial (RCT) comparing the clinical outcomes of patients with iliofemoral DVT treated with the ClotTriever system versus anticoagulation only.
AVS has announced that it raised US$20 million in Series B financing, which the company says will accelerate clinical trial timelines for its device for peripheral application in pulsatile intravascular lithotripsy (PIVL) cases and advance development and preclinical work on a PIVL device for coronary cases.
Rivermark Medical has announced the successful first-in-human (FIH) use of its FloStent System as part of the company’s RAPID-1 FIH clinical study, which is evaluating the delivery, safety, and clinical effectiveness of the FloStent System for treating the symptoms of benign prostatic hyperplasia (BPH).
In a newly released “focused update” to its 2019 recommendations, the European Society for Vascular Surgery (ESVS) abdominal aortic aneurysm (AAA) guidelines writing committee has published advice on the surveillance and management of patients treated with the Nellix endovascular aneurysm sealing (EVAS) system (Endologix).
GE Healthcare announced it has entered into an agreement to acquire Imactis, an innovator in computed tomography (CT) interventional guidance across an array of care areas.
A team of specialists at Ulis Hospital (Ulis, Ukraine) has recently reported that the quality-of-life of the two pancreatic cancer patients treated with TSE in September 2022 continues to improve.
Radioactive (ionizing radiation) round yellow and black danger symbol painted on a massive steel checker metal diamond plat pattern wall with dark rustic grungy texture background.
Researchers at Moffitt Cancer Center (Tampa, USA) are investigating new treatment approaches for the primary lung neuroendocrine tumour patient population. In a new article published in the International Journal of Radiation Oncology, Biology and Physics, a team of physicians, led by Daniel Oliver and Stephen Rosenberg, suggests that stereotactic body radiotherapy (SBRT) could be an effective treatment for patients with early-stage lung neuroendocrine tumours.
SBRT is a treatment approach that delivers high doses of radiation to precise areas of a tumour, minimising damage to surrounding normal cells. Patients receiving SBRT often have less toxicity and side-effects compared to treatment with conventional radiotherapy that is delivered in smaller doses each day over several weeks.
“SBRT is commonly used as a treatment for early stage non-small cell lung cancer, and our results show strong tumour control. This suggests that SBRT may also be effective for lung neuroendocrine tumours,” said Oliver, assistant member of the Department of Radiation Oncology at the Moffitt Cancer Center. “In fact, SBRT is increasingly being used to treat early-stage lung neuroendocrine tumours in clinical practice, despite the lack of consensus recommendations for this approach and very limited data on its effectiveness and toxicity in lung neuroendocrine tumour patients.”
Because of the lack of data, Oliver and his team wanted to assess the efficacy and long-term outcomes of SBRT in patients with lung neuroendocrine tumours. They performed a retrospective analysis of 48 lung neuroendocrine tumours from 46 patients who were treated with SBRT from 11 institutions across the USA. The researchers discovered that SBRT provided strong local/regional tumour control. The three-, six- and nine-year local control rates with SBRT were 97%, 91% and 91% respectively, and only one regional recurrence occurred. The treatment was also well tolerated with only one case of SBRT-related toxicities reported, which was considered low-grade.
“The current study is the largest and first multi-institutional series evaluating local control, toxicity and dosimetric outcomes with SBRT for early-stage lung neuroendocrine tumours. Our results suggest that while surgery provides excellent outcomes, SBRT should be considered another treatment option for this patient population,” said Rosenberg, study senior author and director of magnetic resonance imaging (MRI)-guided radiotherapy in the Moffitt Cancer Center’s Department of Radiation Oncology.
Guerbet has announced the first production batch has been manufactured and released for Elucirem (gadopiclenol) injection following US Food and Drug Administration (FDA) approval in September 2022, after priority review. The highly stable macrocyclic gadolinium-based contrast agent (GBCA) has the highest relaxivity in its class for magnetic resonance imaging (MRI) and is indicated for use in adults and children aged two years and older.
Elucirem injection is used to detect and visualise lesions with abnormal vascularity in the central nervous system (brain, spine, and associated tissues) and the body (head and neck, thorax, abdomen, pelvis, and musculoskeletal system).
GBCAs improve the contrast between lesions and surrounding tissues by accelerating the relaxation of protons thanks to interaction with gadolinium atoms. Gadopiclenol, the active drug substance of Elucirem, has been designed to enable twice as much interaction, resulting in the highest relaxivity among all non-specific GBCAs. This allows use at half the conventional gadolinium dose to reveal high-quality images.
A number of speakers took to the stage at the International Symposium on Endovascular Therapies (ISET; 16–19 January 2023, Miami Beach, USA) to debate the ‘ambulatory shift’ that is currently taking place in the interventional space.
Aaron Mauck (Advisory Board, Washington DC, USA), began with a keynote lecture describing the factors driving the migration of procedures away from the hospital towards ambulatory surgery centres (ASCs) and office-based labs (OBLs)—describing this as a “seismic shift” that “everyone is preparing for”. New reimbursement policies and regulations, provider competition and innovation are among major drivers of this trend. However, Mauck stated that “the future is not etched in stone” when it comes to the ambulatory shift, adding that industry investment and purchaser/referrer steerage are among factors that could accelerate this shift, while certain data indicating poorer outcomes with peripheral vascular procedures performed in the OBL—as well as US state legislatures not being amended—constitute barriers that may slow the process.
Jeffrey Carr
For ambulatory practices
Several key points extoling the virtues of more ambulatory, office-based practices were delivered by Jeffrey Carr (CardiaStream, Tyler, USA). Drawing on a 15-year experience of cardiac and vascular procedures in the ambulatory environment, Carr averred that greater control of their (his team’s) schedule and patients’ clinical care was among the initial motivations behind establishing an OBL in 2008, which was then transitioned to a hybrid lab—an OBL-ambulatory surgery centre (ASC)—in 2014. Here, the speaker cited the possibility for diversification and optimisation of revenue, a minimised impact on reimbursement cuts, and “higher standards” for existing OBLs as among the most important benefits.
After detailing the myriad peripheral vascular, cardiac and venous interventions that can currently be performed in his centre’s office-based settings—and touching on other future possibilities, such as aortic repairs and carotid stent placements—Carr concluded that it is “vital” to follow standardised processes/protocols, while also exercising transparency and reporting outcomes accurately. He further stated that “the future is bright” for expanding procedures, reducing costs and creating high value in office-based and ASC settings.
Jason Greis
This session also yielded additional tips for those wishing to establish outpatient practices—Jason Greis (Benesch, Friedlander, Coplan & Aronoff, Cleveland, USA), advised prioritising “quality of care, not volume of cases”; maximising the number of interventionalist owners and the percentage of equity they hold; and taking patient, payer and investor complaints seriously.
Against ambulatory practices
This talk was immediately followed by Dipankar Mukherjee’s (INOVA Fairfax Hospital, Falls Church, USA) presentation entitled: “Why I chose not to work in an outpatient lab”. Mukherjee noted that, since the 2011 approval of atherectomy codes for peripheral vascular interventions, migration of talent has become a problem, as “some of our best interventionalists” have moved from hospitals to OBLs. In addition to leaving some of the sickest hospitalised patients in the hands of less experienced operators, and contributing to a “serious manpower crisis” across much of the USA, the speaker stated that these interventionalists have “abandoned their responsibility” in educating future generations as well.
Dipankar Mukherjee
On top of this “immense loss” facing trainees, surgeons working exclusively in OBLs are also likely to “lose all open repair skills”, according to Mukherjee, who asked the ISET audience, ‘where would you and I be now’ if pioneering interventionalists of the past had gone to work in these ambulatory settings? He further called for the “rules of the game” in OBLs to change and for the restoration of “the values that attracted us to the profession and specialty”.
Crossing chronic total occlusion (CTO) lesions are challenging procedures. The BeBack crossing catheter—Bentley’s first product to be available in both Europe and the USA following the company’s acquisition of Upstream Peripheral Medical Technologies’ GoBack crossing catheter in September 2022—offers a new solution in this space. Andrej Schmidt (University Hospital Leipzig, Leipzig, Germany), one of the first to use the catheter, shares his clinical experience with the BeBack, noting how it has been a “game-changer” in his endovascular peripheral arterial disease (PAD) practice.
What does your PAD practice look like, and what do you think are the most difficult aspects to overcome when treating CTO lesions?
The University Hospital Leipzig is one of the larger centres in Germany for the endovascular therapy of peripheral arterial occlusive disease, and we receive a lot of very complex cases, many of them failed in other hospitals. These are very often patients with severely calcified infrainguinal disease, but also complex iliac total occlusions.
Could you talk us through your first experience with the BeBack catheter?
We were struggling with a CTO of the common iliac artery in an abdominal aneurysm patient and failed to get through the CTO coming from retrograde, cross-over and antegrade using an arm-access. Nothing worked, until eventually we used the BeBack catheter via the retrograde approach. With this, device passage through the CTO back into the aorta succeeded immediately. This experience was an eye-opener for us with regard to the success of the BeBack catheter.
Can the BeBack also be used as a support catheter?
In addition to its main purpose as a crossing catheter for complex, calcified CTOs, the BeBack indeed can be used as a support catheter since it is quite stable and stiff. This feature is very helpful in difficult total occlusions. It also can be used as a re-entry catheter, for example during a recanalisation of a CTO of the femoropopliteal segment. In the typical situation of being stuck subintimally, unable to pass the guidewire back into the true lumen distal to the CTO, the BeBack reliably helps to re-enter the distal patent segment of the artery.
How is the BeBack part of your recanalisation strategy?
This depends on the type of lesion and the problem encountered during the intervention. For example a typical femoropopliteal CTO is usually approached from antegrade. In case of inability to penetrate the guidewire into the CTO, either due to dense fibrosis of the proximal cap or severe calcification, the BeBack catheter is used as a crossing device by pushing the adjustable needle just a little bit out of the tip of the 4Fr catheter. More frequent however is the situation that the guidewire passes the CTO subintimally and reconnection to the patent lumen distal to the CTO fails. As mentioned above, the BeBack catheter is then used as a re-entry-device by protruding the curved inner needle further out of the tip of the catheter. Different to other re-entry devices is that the BeBack is 4Fr compatible, instead of 6Fr, and introduction into calcified, tight lesions may be easier. Yet it can be used over a 0.018” guidewire, which is often the guidewire of choice in difficult CTOs, improving stability and success compared to 0.014” guidewires.
Another situation, where the BeBack is our device of choice, is a reocclusion of the femoropopliteal segment with previous spot-stenting. Usually, the guidewire passes subintimally and entering into the occluded lumen of a stent within a longer CTO is not possible. In this situation the BeBack indeed reliably and fast allows the guidewire to enter into the proximal end of the occluded stent and to finalise the procedure successfully.
Below the knee we mainly use the 2.9Fr BeBack device, although also the 4Fr device is used in the proximal third of the calf for penetrating through calcific CTOs or for re-entering after subintimal guidewire passage. In some cases of severely calcified infrapopliteal lesions it can happen, that the GW passes easily intraluminally through a stenosis, but no balloon would follow due to the tightness and calcification of the lesion. In this situation, the 2.9Fr BeBack is inserted over the guidewire and, with the needle slightly protruded from the tip of the catheter, it is drilled into the problematic plaque. This technique, mimicking the Japanese technique of transcutaneous plaque-piercing, is very successful in facilitating introduction of balloons into the lesion and finalising the procedure.
Has the BeBack changed your practice and if so, how?
For many years, we and other centres have helped to develop techniques to improve the success rate in difficult peripheral CTOs. The retrograde and bidirectional approach became standard in case of inability to pass a CTO from antegrade. However, in some cases it can be anticipated that establishing a retrograde access will be cumbersome or time consuming. In these cases we now prefer the BeBack to keep the intervention simple. Furthermore, a bidirectional recanalisation can be time consuming and may even fail. In this situation the BeBack helps to speed up and may even be the only way to finalise the procedure successfully.
During CTO recanalisations, do you think that sometimes physicians start too late to switch from one to another technique?
Not infrequently physicians try different guidewires and different catheters many times to pass a difficult CTO or to re-enter back into the patent distal lumen. This increases the risk of protruding the dissection distal to the CTO, destroying healthy segments which sometimes worsens the clinical situation. Furthermore radiation dose and the amount of contrast medium increases. Complications correlate with the duration of the procedure. The retrograde approach and the BeBack catheter are our technique and technology to shorten the procedure time.
How much time or how many attempts would you give yourself with conventional techniques before using the BeBack crossing catheter?
It depends on the complexity of the lesion. If we see a chance to be successful using an antegrade approach, we may proceed for some minutes. In very complex lesions, where it can be anticipated, that a conventional approach has a high risk to fail or may take time, we switch to the BeBack catheter within a minute.
If a colleague were to ask you about the BeBack, how would you describe it?
The BeBack is a reliable crossing and re-entry device. It is very slim (2.9Fr or 4Fr), yet very stable and can easily be used not only in larger diameter arteries like iliacs, but also in small arteries, even via a retrograde pedal access through a 2.9Fr sheath. Furthermore, it is possible to use it over a 0.014” and over a stable 0.018” guidewire, which is usually the wire of choice in more complex lesions. Due to its straightforward design, it is easy to position and reposition the device and control the depth and direction of the 360 degree adjustable needle from the tip of the catheter. It is helpful in quite a large variety of difficult situations and handling is easy to learn.
Case images1. CTO of the left superficial femoral artery in a male patient suffering from severe claudication left calf. 2. After subintimal passage it was impossible to redirect the guidewire into the patent lumen distal to the CTO. 3. Positioning of the BeBack catheter to re-enter the guidewire. Arrow indicates an orientation-marker. 4. Marker appearing as a “C” indicates the direction of the needle, needle protruding maximally out of the BeBack catheter. 5. A 0.018” guidewire passing into the patent distal lumen. 6. Result after stenting.
Mina S Makary, assistant professor at the Division of Vascular and Interventional Radiology/Department of Radiology at the Ohio State University Wexner Medical Center (Columbus, USA) and collaborator Warren A Campbell IV from Ohio State University’s medical scientist training programme share their take on the impact histotripsy stands to make on the ablation space within interventional oncology (IO).
Ablation techniques utilise thermal stress to induce cell death, which is accomplished using currents, cryotherapy, microwaves, lasers, or ultrasound. While effective, these ablation techniques have limitations. Transducer placement requires percutaneous or laparoscopic access. Reliance on temperature can prevent effective targeting near sensitive structures, and uniform necrosis often cannot be achieved because of the heat-sink effect near vascular structures. The advent of histotripsy as an ablative modality has the potential to cause a shift in ablation therapies by addressing existing limitations. Histotripsy creates targeted cavitations with large amplitude pulses to mechanically disintegrate tissue1—cavitations are transient steam-filled microbubbles that form when high amplitude waves travel through fluid. Rapid expansion and implosion during cavitation causes significant sheer stress to break cells into subcellular components.
Histotripsy has technical advantages over traditional ablation methods. First, renal, hepatic, and intracranial masses can be targeted transdermally. Second, the primary mechanism is mechanical tissue destruction, which improves accuracy and focus on smaller targets.2 Third, connective tissue is more resistant to histotripsy, reducing the likelihood of collateral damage to blood vessels or biliary structures.3 Lastly, the area of destruction creates hypoechogenicity which is efficient to monitor in real time.4 With the principles of histotripsy, there exists the potential to target any tissue in the body for ablation in a precise, rapid approach, sparing non-targeted tissue and without percutaneous incisions or forms of dangerous ionising radiation.
Histotripsy is showing promise in the treatment of cancer. Preclinical animal studies demonstrated histotripsy’s ability to treat liver, prostate, breast, kidney, oesophageal, pancreas, and brain tumours through necrosis.5 For metastatic tumours, data have also detected an abscopal effect, where untargeted tumours decrease in growth rate. Targeted ablation disrupts the tumour’s evasion of the immune system. Mechanical perturbation of the tumour’s microenvironment increases the exposure of immunological epitopes and removes anti-inflammatory regulatory cells, permitting immune cell infiltration and improved anti-tumour immunity.6 Recent developments include the phase 1 clinical trial of histotripsy on nonresectable hepatic tumours (THERESA), which was successful7—all eight patients experienced no procedural complications two months after the procedure, and tissue was effectively targeted and destroyed in both primary and secondary tumours.
Warren A Campbell IV
The future of histotripsy is currently being developed in the lab, with a focus on improving the safety, efficacy, and versatility of the procedure. Utilisation of microbubbles and fluid-filled polymer capsules can make histotripsy safer by reducing the energy required for cavitation. Liposomes could also transport drug payloads (i.e. chemotherapies), where histotripsy initiates targeted release. Histotripsy may also permit the diffusion of larger nonpermeable biopharmaceuticals like heparin and insulin through skin via histotripsy of the stratum corneum, eliminating the need for regular injections. The debulking and tumour-targeting functions have already been proven in clinical trials, but these advancements will increase its synergistic effects with other oncological therapies.
Histotripsy is the most recent development of high-intensity focused ultrasound techniques, which have the added benefit of mechanical tissue destruction with increased precision and targeting that is less invasive than alternative techniques. Histotripsy may also have the added benefit of increasing tumour immunogenicity in metastatic disease. Preclinical models in multiple cancers have been effective, and the first human trial targeting hepatic tumours was safe and effective. The future of histotripsy includes a range of applications to treat patients increasingly safely and non-invasively.
References:
Bader, KB, Vlaisavljevich, E & Maxwell, AD For whom the bubble grows: Physical principles of bubble nucleation and dynamics in histotripsy ultrasound therapy. Ultrasound Med. Biol.45, 1056–1080 (2019).
Nault, J-C, Sutter, O, Nahon, P, Ganne-Carrié, N & Séror, O Percutaneous treatment of hepatocellular carcinoma: State of the art and innovations. J. Hepatol.68, 783–797 (2018).
Wang, Y-N et al. Mechanical decellularisation of tissue volumes using boiling histotripsy. Phys. Med. Biol.63, 235023 (2018).
Wang, T-Y et al. Quantitative ultrasound backscatter for pulsed cavitational ultrasound therapy-histotripsy. IEEE Trans. Ultrason. Ferroelectr. Freq. Control56, 995–1005 (2009).
Izadifar, Z, Izadifar, Z, Chapman, D & Babyn, P An Introduction to High Intensity Focused Ultrasound: Systematic Review on Principles, Devices, and Clinical Applications. J. Clin. Med.9, 460 (2020).
Hendricks-Wenger, A, Hutchison, R, Vlaisavljevich, E & Allen, IC Immunological Effects of Histotripsy for Cancer Therapy. Front. Oncol.11, 681629 (2021).
Vidal-Jove, J et al. First-in-man histotripsy of hepatic tumours: The THERESA trial, a feasibility study. Int. J. Hyperthermia39, 1115–1123 (2022).
Disclosures:The authors declared no relevant disclosures.
During the Society of Interventional Oncology (SIO) 2023 annual scientific meeting in Washington DC, USA, a panel of speakers delivered presentations on why patient-centred care is important, and how to provide it most effectively. The session comprised perspectives beyond interventional radiology—a nurse practitioner and a patient offered complementary and valuable insight—yet there were commonalities across the different presenters’ talks. All emphasised how crucial open communication between the patient and their family and healthcare professionals is. Only with this approach will patients receive the best care, which extends beyond clinical intervention to incorporate caring for the emotional and mental needs of the patient and their loved ones—this was a key takeaway from the session.
Physicians are co-narrators in the patient’s story
Eric Keller (Stanford University, Stanford, USA), whose presentation was delivered in his absence by Isabel Newton (University of California San Diego, San Diego, USA), underlined how “there is more to healing than what we do with our catheters and our wires”. Keller conveyed that “patients’ perspectives of the quality of our work has a lot to do with […] how nice the facility is, our body language, tone of voice and [whether] they can get hold of you for questions and concerns”. Therefore, how a patient feels their experience with a healthcare practitioner has gone is influenced by how it is framed—Keller gave the example of how it is better to tell a patient their biliary drain will be in for a year and for it to come out after six months, than it is to overpromise that it will in
three months.
Keller published a study in 2018 in the Journal of Vascular and Interventional Radiology (JVIR), the presenter went on to share, which illustrated that physicians’ and patients’ perceptions of the quality of their care depend on different variables. “[Interventional radiologists] valued minimising side effects and complications,” Keller averred, whereas from the patient’s point of view it is “not so much the actual outcome as much as not being surprised [by it]”. With this in mind, Keller wished to inform delegates that a physician’s role is as a “co-narrator” who seeks to “understand [the patient’s] story” and to help them “write those next few pages”.
Keller then put forward “three important non-procedural interventions that we can do to help maximise our patients’ experiences”. The first was advanced care planning, comprising an assessment of the patient’s goals and preferences for their care. The recommendation is “to facilitate this at the beginning of serious disease”, with scope to revise in line with the patient changing their mind, the presenter relayed. “It does not have to be us [who has these conversations],” Keller continued, “but we can advocate for them to occur as part of the preprocedural work-up”.
The second recommendation from Keller was to share alternatives to clinical interventions, to move away from what the presenter dubbed “old-school paternalism”. He made the point that “often we do a great job at discussing our interventions but not at doing the procedure. We are also inconsistent in how we handle preprocedure [‘do not resuscitate’] DNR orders.” As a remedy, the presenter suggested that these are dealt with “well ahead of time”.
Eric Keller
Finally, Keller emphasised that “healing is a multifactorial process—it can be easy to forget the impact of nutrition, spirituality and social determinants of health [including] the patient’s socioeconomic status, living situation, race, etc.” Detailing that physicians tend to be sceptical of alternative modes of treatment, Keller vouched for talking to patients about their use of these so as to be more “inclusive”. The concluding note was that interventional radiologists should put a greater emphasis on the precise context in which a patient is being cared for—which is shaped by the aforementioned social factors. Examples of how to maximise these contextual aspects of cancer care, according to Keller, include advanced care planning, shared decision-making, and engaging patients about other aspects of their healing to become co-narrators with patients.
Multidisciplinary interventions make a difference
The second presenter was Angela Laffan, a nurse practitioner based at the University of California San Francisco (San Francisco, USA), who runs a survivorship programme for patients who have finished treatment with curative intent. “Cancer survivorship is to help optimise patients’ overall wellness,” she outlined for the audience. She works primarily with patients with metastatic neuroendocrine tumours and used them to illustrate why survivorship matters—many live with their cancer “for years or decades” and thus “miss out on a lot of resources” by virtue of not fitting the “standard model” of a survivorship cancer patient.
Laffan explained that those who work within the programme look at patients’ individual needs, which are affected by “age, gender, stage of life, treatment, diagnosis, and goals for treatment”. Key for consideration, the presenter continued, are whether a patient prioritises quality over quantity of life, or vice versa, as well as the financial and caregiver burden that their illness is having. “This conference is looking at increasing quantity of life, but there are things we can do as healthcare providers to increase quality”. Echoing Keller on acknowledging with patients the multiplicity of lifestyle factors that can impact their healing, Laffan cited an American College of Sports Medicine consensus paper from 2019, which recommended exercise as a means of improving cancer patients’ “quality of life, mental health, sleep”, among other factors. “Despite this, the majority of patients say healthcare providers are not routinely telling them not to exercise […] we should refer patients to exercise counselling if it is available”.
Laffan then expressed her certainty that “you all know the huge mental toll” on patients, who will often be living “from scan to scan” and footing “exorbitantly expensive” bills. Meditation can be a means of assuaging this psychological burden, and also improving symptom profile and pain levels, the presenter supplemented, recommending that physicians working with cancer patients should also offer this form of therapy where possible.
Beyond the patients themselves, Laffan then turned her focus to caregivers—a 2016 National Alliance of Caregivers study found that this group is 60% women, and 50% reported high levels of emotional stress. Half were also working in paid employment alongside their caregiving. “So, what do caregivers need from healthcare providers?” Laffan posed as a rhetorical question. “Recognition, detailed education and support with their role […] the vast majority of the time, they are not doctors or nurses,” Laffan stated, underlining that they are still “asked to perform medical tasks.”
In summary, there needs to be an “individualised approach for patients living with cancer as chronic illness,” Laffan advocated. “It is important we check in with patients and caregivers, particularly at times of transition […] Often they smile and say they are fine but that might not be their reality.” Reiterating, Laffan’s parting note was that “extending life does not necessarily equate to living well” and therefore, the focus should also be on quality of life, intervening early with a multidisciplinary approach. An example of the success of this is Laffan’s neuroendocrine wellness clinic, where patients are referred proactively, “rather than reactively, which is what we often do”.
Lynn Lazzaro speaking about her patient experience
Patient point of view: treatment as a “miraculous” tapestry
Lynn Lazzaro (a financial advisor based in Sparks, USA) gave her patient perspective on the care that saved her life mirrored much of what Laffan’s presentation covered. Diagnosed with a 13.5cm mass on her liver in January 2016, Lazzaro told delegates how her interventional oncology (IO) team gave her a year to live, “maybe two with treatment”. Living from scan to scan as Laffan had described was Lazzaro’s reality, the presenter acknowledged. “Looking back on the journal I kept […it] almost seems to reel as if it happened to someone else”. But Lazzaro recognised her experience in the previous presenters advocating for conversations—about treatment plans, goals and how to achieve them. “My treatment team asks me these questions often,” Lazzaro affirmed, referencing Atul Gawande’s book ‘Being Mortal’, which outlines how the “ultimate goal is not a good death but living a good life all the way to the end”.
Lazzaro described her life during treatment like a “beautiful tapestry—maybe if you pulled one string the whole thing would fall apart”. However, IO, she avowed, “was the miracle that began by adding years to my life, which ultimately gave me the chance at a cure—transplant after downstaging.” Her relationship with her multidisciplinary team, as mentioned by Laffan, was instrumental in reducing hers and her family’s stress—“treating me as a whole person gave me the resilience to get up and do it all again. They kept me informed always of my prognosis—an easier conversation for some than others—but factual honesty was key for family.”
“If treatment was an art or tapestry then the outcome is really the result of the art form of your profession—your judgement, your risks, your compassion saved my life,” was Lazzaro’s thanks for the work that the IO community, drawing attention to how the clinical and non-clinical aspects of a patient’s care play complementary roles.
Thierry De Baère (Gustave Roussy; Villejuif, France) talks to Interventional News about the rationale behind setting up the Initiative on Superselective Conventional Transarterial Chemoembolization (INSPIRE), which aims to bring Asian and European experts together in order to collaborate on standardising cTACE across the globe.
Speaking at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual meeting (10–14 September 2022, Barcelona, Spain), De Baère discusses whether or not TACE/cTACE will remain a choice for hepatocellular carcinoma (HCC) patients in the future. “I think cTACE will survive only in very select populations,” he says.
De Baère concludes by highlighting why it is important to improve cTACE, before outlining how he hopes the paper will impact the interventional radiology community.
The Society of Interventional Oncology (SIO) has declared Mayo Clinic, Rochester, USA as the first of 10 sites in the USA and Europe approved for enrolment on the society’s primary clinical trial ‘Ablation with Confirmation of Colorectal Liver Metastases (ACCLAIM), Prospective Trial for Microwave Ablation as a Local Cure.’
Constantinos T Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA), the study’s global primary investigator presented the background to the trial, as well as its aims, to attendees of the SIO 2023 annual scientific meeting (19–23 January, Washington DC, USA). The Mayo Clinic site study investigators include Grant D Schmit as the principal investigator, and Matthew R Callstrom and Anil N Kurup as co-investigators (all Mayo Clinic, Rochester, USA).
ACCLAIM is the first global, prospective trial to use an objective and reproducible technical endpoint in its design, which SIO believes will drive important changes to future colorectal liver metastases (CRLM) treatment guidelines, the society announced in a press release. In this multicentre, international trial, SIO aspires to establish microwave ablation (MWA) as the preferred local curative treatment option for selected CRLM that can be ablated with sufficient margins. The study mandates the use of 3D software to assess the ablation zone and margins and determine if achieving complete margins during an ablation equates to procedural success, where the primary outcome is local tumour progression-free survival at two years post-ablation. This trial is funded through SIO grants from Boston Scientific, NeuWave Medical (part of Ethicon) and Varian (a Siemens Healthineers company). Participants of the trial will have a diagnosis of CRLM for which they would be offered ablation as standard of care. MWA will be performed using a combination of US Food and Drug Administration (FDA)-cleared or CE marked, commercially available MWA system and margin confirmation (visualisation) 3D software. Upon its launch, the ACCLAIM study is expected to have a three-year enrolment period of approximately 275 participants across sites in the USA and Europe.
Speaking at SIO 2023, Sofocleous began by stating his opinion that the ACCLAIM study was “way overdue” as currently, “surgery is the preferred treatment for synchronous and metachronous CRLM”. Hence, posing the rhetorical question “Why do we need the ACCLAIM?”, the presenter answered that the trial aim is “to prove that [MWA] can be the preferred treatment ahead of surgery for selected CRLM that can be ablated with margins, and to create the evidence to support the use of [MWA] for this indication.” Furthermore, Sofocleous emphasised the importance of “standardising ablation treatment” through mandatory steps involved in image-guided thermal ablation for CRLM.
Sofocleous then referred to ablation’s recent past—when confirming the success of ablation margins was not common practice. Recent software developments, namely 3D assessment software, has facilitated the confirmation of margins, the speaker noted, adding that “if we have this ability intraoperatively, as work using 3D software assessments showed, we may [be able] to retreat intraoperatively and avoid local treatment failures.”
Thanks to two National Institutes of Health (NIH) grants, Sofocleous went on to explain how he has been able to interrogate prospectively the efficacy of achieving complete tumour eradication and creating sufficient margins with tissue sampling. “You can document a minimum of 5mm margin with tissue evidence of no residual viable disease at the end of the ablation treatment,” Sofocleous clarified, furthering that this is “regardless of modality or energy” and “biopsy-proven”. Continuing, Sofocleous informed attendees that “comparisons of intraoperative assessments using contrast-enhanced CT (CECT) with the guideline standard of care—assessment at four to eight weeks post-ablation—have shown that the intraoperative CECT assessment yielding margins of less than 5mm is “the most reliable
factor to predict local tumour progression”.
Sofocleous circled back to underline what “ACCLAIM is mandating to do”. Enrolment mandates “immediate 3D software assessments of the ablation zone and margins”, with a need to create an ablation margin of at least 5mm in order to avoid local tumour progression”. Once the 3D assessment has confirmed a margin greater than 5mm, Sofocleous concluded, “we believe that regardless of centre, country, operator, this unified endpoint (of ablation with minimal margin of at least 5mm) will result in high rates of sustained, long-term tumour control.”
The presenter ended by stating that the trial is anticipating opening in 10 centres, and that any FDA- cleared or CE-marked 3D margin assessment software and ablation device is “acceptable” for use in the trial.
Cagent Vascular has announced the results of a comparative subanalysis of the PRELUDE-below-the-knee (BTK) study versus plain balloon angioplasty.
The study was led by Marianne Brodmann (Medical University of Graz, Graz, Austria). This subanalysis compared their PRELUDE-BTK subset to a consecutive plain balloon angioplasty group.
The Serranator-treated lesions had an average final residual stenosis of 17.2±8.2% vs. 33.7±15.7% in the plain balloon angioplasty group. This represents a 49% average improvement in final residual stenosis. In chronic total occlusions (CTO), there was a 62% improvement in final residual stenosis compared to the plain balloon angioplasty group. The average balloon inflation pressure was 5atm in the Serranator group vs. 9atm in the conventional balloon angioplasty group. Additionally, Serranator-treated arteries demonstrated 2.4 times greater calculated flow improvement versus plain balloon angioplasty. These data, analysed by the same independent core lab, were recently published in the Journal of Endovascular Therapy.
Brodmann stated: “As an early user of serration angioplasty, it was meaningful to quantify through this subanalysis what we have experienced using the Serranator device. William Tang (UC Irvine, Irvine, USA) developed a novel model, anchored by Poiseuille’s law, from which we were able to derive the volumetric blood flow from lumen gain achieved with the Serranator compared to conventional balloon angioplasty. These results suggest an advantage for serration technology that should allow for superior wound healing and patient outcomes, while minimising the need for stent placement.”
Raman Sharma (Mount Sinai Medical Center, New York, USA) was an early adopter of serration technology, and added: “When it comes to BTK interventions, there simply have not been great options for physicians to treat patients, who are often in jeopardy of limb loss. In these cases, our goal is to restore sufficient blood flow to allow a patient’s wound to heal, without leaving anything behind. The results from this subanalysis study support what we have seen in our experience; the Serranator provides greater lumen gain and blood flow versus conventional technology.”
Photon-counting detector computed tomography (CT) reduces the amount of contrast needed for CT angiography (CTA) while maintaining image quality, according to a new study published in Radiology: Cardiothoracic Imaging, a journal of the Radiological Society of North America (RSNA).
The portion of the aorta that passes through the chest and abdomen is prone to aneurysms. Risk increases with age. Doctors use CTA with contrast media to examine this region of the artery. While the iodinated contrast media used in these exams is considered very safe, there is a higher risk of adverse reactions in patients with kidney disease, or nephropathy.
“Many patients undergoing CTA of the aorta are elderly, and some may suffer from a certain degree of nephropathy,” said senior author Hatem Alkadhi from the Department of Diagnostic and Interventional Radiology at University Hospital Zurich in Zurich, Switzerland. “Thus, they might be at risk for a further reduction of their kidney function due to contrast media administration.”
Using less contrast media is also good for the environment, as iodine breakdown products have harmful environmental effects. In addition, the supply of contrast media has suffered from shortages due to COVID-19-related disruptions in the pharmaceutical supply chain.
Photon-counting detector CT is a new technology that can acquire high-quality images at lower contrast media volume than conventional CT scanners that rely on energy-integrating detectors. It also offers diagnostic quality images at lower radiation dose than those of conventional CT.
Alkadhi and University Hospital Zurich colleague Kai Higashigaito led a study that looked at a low-volume contrast media protocol with photon-counting detector CT for CTA of the aorta in the chest and abdomen.
The study included 100 people, mean age 75. Patients underwent CTA with photon-counting detector CT of the aorta in the chest and abdomen. The patients had received a previous CTA with conventional CT at equal radiation doses.
Photon-counting CT had a higher contrast-to-noise ratio, a key measure of image quality, which translates to a low-volume contrast media protocol. Contrast media volume was reduced by 25%.
Two independent readers rated the image quality of photon-counting CT as higher than that of conventional CT at an equal radiation dose.
“We showed that the improved image quality of CTA with photon-counting detector CT systems can be used to reduce the amount of administered contrast media to the patients, without reducing the diagnostic yield of the examination,” Alkadhi said. “Image quality remained at the same level as that of previous CT angiography examinations in the same patients using a conventional CT, despite the fact that we reduced the contrast media volume.”
Surmodics recently announced it has received a letter from the US Food and Drug Administration (FDA) related to its premarket approval (PMA) application for the SurVeil drug-coated balloon (DCB).
In the letter, the FDA indicated that the application is not currently approvable, while providing specific guidance as to a path forward. The letter stated that certain information within two general categories—biocompatibility and labelling—must be added by an amendment to the company’s PMA application to place it in approvable form. Although the information identified by the FDA to put the PMA application in approvable form would require additional testing and analysis, the letter did not question the human clinical data submitted nor request any further human clinical data.
“We are disappointed by the FDA’s response to our PMA application and continue to have confidence in our SurVeil DCB including its compelling performance in the TRANSCEND clinical study,” said Gary Maharaj, chief executive officer of Surmodics. “We are evaluating the issues raised in the FDA’s letter and plan to meet with Agency representatives regarding its contents. Based on our discussion with the Agency, our team and external advisors will determine the appropriate path forward. Concurrently, we will be evaluating options to reduce our use of cash given this development. We expect to address these topics further in connection with our upcoming first quarter fiscal 2023 earnings call.”
Surmodics notes in a press release that the SurVeil DCB is a next-generation device for the treatment of peripheral arterial disease and includes a proprietary drug-excipient formulation using an innovative process to improve coating uniformity. The company advises that, in the USA, the SurVeil DCB is an investigational device, limited by Federal law to investigational use.
IceCure Medical has shared in a press release that it has received a Notice of Allowance from the US Patent and Trademark Office for its patent application titled ‘Cryogen Pump’. The patent will be in effect until February 2040 and was recently granted in the European Union and allowed in Japan.
“ProSense is gaining increasing commercial traction in the USA in the indications for which it already has regulatory approval and reimbursement, as well as increased visibility in breast cancer following our October 2022 regulatory filing with the [US Food and Drug Administration] FDA. This Notice of Allowance in the USA is very well timed to protect our intellectual property as we develop the next generation of cryoablation systems to perform minimally invasive procedures for new indications,” stated Eyal Shamir, IceCure’s chief executive officer.
The cryogenic pump enables IceCure to bring to market a new generation of cryoablation systems with a small footprint for a wide range of clinical applications. Moreover, this pump expands IceCure’s portfolio of products with a broader range of thinner cryoprobes and catheters.
IceCure’s cryogenic pump is submersible in liquid nitrogen, works in a closed circuit, enables temperature control of the cryoprobe, improves the cooling rate during a procedure, and is designed to be used for multiple procedures or longer-duration procedures without the need to refill liquid nitrogen.
Delcath Systems has shared in a press release the publication of updated results from the phase 1b CHOPIN Trial, conducted at Leiden University Medical Center (Leiden, The Netherlands) on the use of the Delcath Chemosat hepatic delivery system with melphalan (Chemosat) in combination with the immune checkpoint inhibitors (ICI) ipilimumab and nivolumab to treat patients with metastatic uveal melanoma with liver metastases.
The publication is titled ‘Combining melphalan percutaneous hepatic perfusion with ipilimumab plus nivolumab in advanced uveal melanoma: First safety and efficacy data from the phase 1b part of the CHOPIN trial’ and was published in CardioVascular Interventional Radiology (CVIR).
Updated CHOPIN phase 1b trial results
The goal of the CHOPIN trial is to study the safety and potential synergistic effects of systemic ICI therapy ipilimumab plus nivolumab (IPI+NIVO) when combined with Delcath’s proprietary liver-targeted percutaneous hepatic perfusion (PHP) treatment in metastatic uveal melanoma patients. The phase 1b portion of the trial enrolled seven patients, each of whom were treated with two courses of PHP (melphalan 3mg/kg, max. 220 mg per cycle) combined with four courses IPI+NIVO escalating the dosing from 1mg/kg each IPI+NIVO (cohort 1) to IPI 1mg/kg + NIVO 3mg/kg (cohort 2). The best overall response included one complete response, five partial responses and one stable disease accounting for an objective response rate of 85.7% and a disease control rate of 100% (figure 1). At the cut-off date of 15 November 2022, the median follow-up was 29.1 months (range 8.9–30.2), the median progression-free survival was 29.1 months (95% confidence interval [CI] 11.9–46.3) and the median duration of response was 27.1 months (range 7.4–28.5).
The ongoing randomised phase 2 part of the CHOPIN trial comparing M-PHP alone with M-PHP plus IPI+NIVO, which will include another 76 patients (38 per arm), is approximately 50% enrolled and will provide more insight to the efficacy.
The determination of a safe and effective dose was a primary goal of the Phase 1b portion of the CHOPIN trial. Grade 1/2 adverse events were seen in all patients and 71.4% experienced grade 3/4 toxicities. In this phase 1b dose-escalation study combining M-PHP with IPI+NIVO, the safe treatment dose was established at IPI 1mg/kg and NIVO 3mg/kg. The phase 2 part of the CHOPIN study will provide more information on both hepatic and systemic toxicity associated with the combination therapy.
“If similar results are observed in the larger, randomised, second phase of this trial, it would represent a meaningful improvement over current treatment options for this patient population,” said Johnny John, the company’s senior vice president, Medical and Clinical Affairs. “In addition, further investigation of this combination protocol may be warranted in patients with liver dominant disease in other tumour types currently treated with ICI agents.”
figure 1: % change of target lesions from baseline by response Category
Rationale for combination therapy
The rationale for combining ICI therapy with M-PHP in metastatic uveal melanoma is based on both uveal melanoma’s specific characteristics and the unique immunomodulatory role of the liver. Uveal melanoma is characterised by a different set of driver mutations and lower mutational load compared to cutaneous melanoma, leading to limited neoantigen presentation and lower efficacy of ICI. By combining M-PHP with IPI+NIVO, the authors noted that they aim to increase the efficacy of ICI by turning a ‘cold tumour’ into a ‘hot tumour’. In addition, while PHP can provide long-lasting disease control in the liver, it does not control extrahepatic disease. Conversely, IPI+NIVO treatment shows a trend towards control of extrahepatic lesions, but hepatic disease progression regularly occurs. With combined treatment, the authors aim to control hepatic disease, as well as prevent extrahepatic disease in follow-up. In addition, it is well documented that the liver has a unique immune-modulating role and liver metastases diminish ICI efficacy systemically regardless of the type of primary tumour and in animal models, it has been shown that this effect can be overcome by localised hepatic therapy Current available evidence from studies on isolated limb perfusion (ILP) and isolated hepatic perfusion (IHP), which is the surgical counterpart of M-PHP, show that ILP and IHP can lead to T-cell activation following the procedures. The authors hypothesise that this is also the case for M-PHP leading to an improved activation of the immune system together with ICI.
A team of specialists at Ulis Hospital (Ulis, Ukraine) has recently reported that the quality-of-life of the two pancreatic cancer patients treated with tumour-specific electroporation (TSE) in September 2022 continues to improve. These two unresectable, locally advanced pancreatic cancer patients had both received TSE treatments in combination with a low dose of chemotherapy, using the IQwavedevice (ChemoTech).
In the follow-up computed tomography (CT) scans, the patients had shown almost a 50% decrease in tumour mass. Both patients are ambulatory and capable of self-care with no pain and are not on analgesics.
After seeing the promising achieved results, the Ulis Hospital team will continue to perform treatments on similar cases and has also invited cancer researchers internationally to join forces and take this treatment forward.
A press conference is planned in the coming weeks by Ulis researchers to interact with the media and attract other researchers to collaborate and explore the full potential of the TSE technology.
Alexei Kovalev of the Ulis Hospital team gave the following statement to press—”Almost five months after treatment, the response of our patients seems lasting and we are optimistic that it can sustain for many more months, with a positive impact on overall survival. We would like to invite cancer researchers internationally to join hands with us in our pursuit of exploring the TSE technology further, possibly in combination with immune-oncology drugs.“
Both the Andreas Gruentzig Lecture at this year’s Cardiovascular and Interventional Radiological Society of Europe meeting (CIRSE; 10–14 September, Barcelona, Spain) and a presentation of interim data at the ‘New Frontiers’ FIRST@CIRSE session informed delegates of the innovative future liver remnant (FLR) hypertrophy technique, liver venous deprivation (LVD).
As Remon Korenblik (Maastricht University Medical Center, Maastricht, The Netherlands) and Boris Guiu (Hôpital Saint-Eloi, Montpellier, France) explained in the context of the data presentation and lecture respectively, LVD involves combining hepatic and portal vein embolization (HVE/PVE) to cause FLR growth. Guiu referred to the ongoing DRAGON 1 trial on which Korenblik presented as an example of “pushing the limits” and a key takeaway message from these presentations was that there is a “place [for] LVD in the future”, and that further studies will “define” exactly what that is.
Portal and hepatic vein embolization in metastatic colorectal cancer treatment
DRAGON 1, as Korenblik conveyed to attendees, is a multinational, multicentre, prospective and single-arm trial, of which the purpose is to “assess training, implementation, safety and feasibility of combined PVE and HVE to accelerate FLR hypertrophy in patients with borderline resectable colorectal cancer liver metastases [CRLM]”. Korenblik alluded to the importance of the trial—“the cornerstone [of CRLM] treatment is resection” but in cases of “insufficient FLR” this is not an option, hence, investigating whether the FLR can be increased in size, so that resection is possible.
The primary endpoint for the DRAGON 1 trial is “a composite of the safety of combined PVE and HVE, 90-day mortality, and one-year accrual monitoring of each participating centre.” Secondary endpoints feature feasibility of resection, FLR hypertrophy, overall survival and disease-free survival.
The interim results from the trial so far, which Korenblik shared with delegates, seem to demonstrate that combined HVE and PVE “induces fast and extensive FLR hypertrophy and leads to high rates of resectability”. The definitive analyses after the DRAGON 1 trial completion are needed to confirm these assumptions. “We also found this in a recent pooled analysis, which will be published shortly,” Korenblik reported, “in which we saw statistically significant higher resectability rates after PVE/HVE compared to PVE alone.”
Next for the DRAGON Initiative, which is behind a series of trials to determine the safety and efficacy of combined PVE and HVE, is the beginning of recruitment for DRAGON 2, Korenblik asserted. This study “will investigate the efficacy and survival of patients after PVE alone compared to PVE and HVE combined in a multinational, multicentre randomised controlled trial”.
Guiu first acknowledged in his lecture, as did Korenblik, the relative clinical success of PVE alone and how it has been considered “really efficient” for decades—but that appetite to improve this further has led to the development of techniques capable of increasing FLR hypertrophy, and thus resection rates. From 2016, when Guiu and colleagues carried out the first study of combined PVE and HVE, yielding “attractive initial results”, cohort studies have confirmed the technique’s outperformance of any other preparation technique, including ALPPS (associating liver partition and portal vein ligation for staged hepatectomy)—historically regarded as “the most efficient technique in terms of volumetric gain [in the FLR]”—or even hepatectomy, in terms of functional gain. Functional increase, Guiu duly noted, is, in addition to volumetric gain, “very important” in the context of liver preparation for hepatectomy.
“There is probably a place for [liver venous deprivation] but we need definitely more data”
“Now we are five or six years on [from the first study], we have now several [more…] from different teams,” Guiu elaborated for attendees. “All but one is showing that LVD outperforms PVE in terms of volumetric gain”, and the presenter went on to acknowledge that there is evidence that LVD also leads to fewer post-resection complications.
With “enthusiasm sparked” by the aforementioned findings, the next step, Guiu averred, is to go about obtaining multicentre, prospective study data. An example the presenter gave is the French HYPERLIV-01 randomised controlled trial comparing PVE with LVD, using glue in the hepatic veins in addition to proximal plugs. As Guiu noted, the trial “has already completed more than two-thirds of its accrual in 11 centres,” and the DRAGON Initiative will also provide key evidence of the value of performing LVD, through its series of trials, as relayed by Korenblik. “There is probably a place for LVD but we need definitely more data […] the objective is to define more precisely the place of this technique,” was Guiu’s conclusion regarding LVD versus PVE for FLR hypertrophy.
The presenter’s final remarks were on innovation within clinical practice more broadly and how to achieve “wide acceptance” of a new technique, such as LVD within the IR community. “I firmly believe that our role should not be limited to [research and innovation]”, Guiu stated, emphasising the “need to disseminate knowledge as part of our mission—new ideas would certainly be pointless if they were to remain confidential.” The goal, the presenter concluded, is to “ignite interest” in the latest innovations, as this is ultimately for patients’ benefit.
From left: Chiang Chi-Leung, Albert Chan Chi-yan, patient Wan Ying-Keung
A phase II clinical study on a trimodality therapy (START-FIT), conducted by the Departments of Surgery and Clinical Oncology, School of Clinical Medicine, University of Hong Kong (HKUMed; Hong Kong), has found that nearly 50% of patients with inoperable, locally advanced liver cancer, can be cured through this approach, which includes stereotactic body radiation therapy (SBRT) and transarterial chemoembolization (TACE). The results have been published in The Lancet Gastroenterology and Hepatology.
A total of 33 patients were screened and enrolled in this treatment method from March 2019 to January 2021, for tumour diameter ranging from 5 to 17.5cm. Just under two thirds (64%) of patients had tumours with major vascular invasion that precluded them from a curative surgical procedure. The research team developed a new approach termed ‘reduce and remove’—a trimodality therapy (START-FIT)—for these 33 patients. Patients received TACE on day one for local tumour control, followed by SBRT on day 28, and then immunotherapy administered 14 days following SBRT and every two weeks thereafter. This trimodality approach is to downstage the tumour status so that it is amenable to curative surgical intervention.
After this trimodality therapy, 55% (18 patients) became suitable to receive curative surgery, of whom four patients (12%) underwent this surgery, and 14 patients (42%) had complete tumour necrosis and are receiving ongoing monitoring with regular scans. After up to 2.5 years of follow-up, two-year survival among these patients exceeded 90%, with mild side effects experienced throughout the treatment process. The advantages of this approach are that it is minimally invasive with a short hospital stay and a relatively high safety profile.
This treatment strategy provides the opportunity for curative surgery with promising long-term outcomes to patients who would otherwise be unsuitable. “This treatment strategy provides a definite treatment schedule. Most patients could have an idea on the treatment effect within six months after the start of treatment and be able to have better planning for themselves and their family. Now the team is looking forward to expanding the treatment coverage to more patients, especially those with poor liver function, to help downstage the tumour status and hence, increase the chance of fitting into the criteria for liver transplantation in the future.” This statement was shared by Albert Chan Chi-yan, clinical professor at HKUMed’s Department of Surgery at the School of Clinical Medicine, who initiated this world-first trimodality therapy.
Interventional News’ most popular stories as 2022 came to a close included news of a US Food and Drug Administration clearance for a new radiofrequency ablation (RFA) system; CE mark approval for a radiation protection system; results of a retrospective analysis of a percutaneous hepatic perfusion (PHP) system; and a report from the current Royal College of Radiologists president on where she thinks interventional radiology (IR) will be in 2030.
A minimally invasive treatment for carpal tunnel syndrome provides long-term relief to patients without the use of corticosteroids, according to research presented at the annual meeting of the Radiological Society of North America (RSNA; 27 November–1 December, Chicago, USA).
Boston Scientific has announced that it will make a partial offer to acquire a majority stake, up to a maximum of 65%, of shares of Acotec Scientific, a Chinese medical technology company that offers solutions designed for a variety of interventional procedures.
Delcath Systems announced the publication of a retrospective analysis of patients who underwent a PHP procedure with Chemosat for the treatment of either inoperable intrahepatic cholangiocarcinomas (iCCA) or extrahepatic cholangiocarcinoma (eCCA) with liver metastases.
RF Medical is a Korean thermal ablation system manufacturer and the creator of the Mygen M-3004 generator and specialised electrodes including Myoblate. Both of these products have been cleared by the US Food and Drug Administration (FDA) and are now commercially available in the USA.
Europe’s health commissioner, Stella Kyriakides, has announced that proposals to extend the transition period for the implementation of the European Union’s (EU) Medical Device Regulation (MDR) will be put forward in early 2023.
Cook Medical announces John A Kaufman (Cook Medical, Bloomington, USA) will be joining as its chief medical officer, effective July 2023. With Kaufman’s expertise and new appointment to this position, Cook is taking a significant step in its clinical and product-related goals.
Egg Medical, a medical device company commercialising technologies to reduce scatter radiation exposure during interventional angiographic procedures, has announced that it has achieved CE mark for the EggNest XR radiation protection system.
Corindus has been rebranded to Siemens Healthineers Endovascular Robotics and will sit as a dedicated business within the Advanced Therapies area of Siemens Healthineers, the company has announced.
The Society of Interventional Radiology (SIR) published a position statement deeming endovascular thrombus removal “an acceptable treatment option in selected patients with acute iliofemoral deep vein thrombosis [DVT].”
RCR president Kath Halliday (Nottingham University Hospitals, Nottingham, UK) gave a presentation to the British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK) exploring how new technologies and infrastructural reforms can improve outcomes for patients under IR department care.
Inari Medical has announced that the first patient has been enrolled in DEFIANCE, a prospective randomised controlled trial (RCT) comparing the clinical outcomes of patients with iliofemoral deep vein thrombosis (DVT) treated with the ClotTriever system versus anticoagulation only. The trial is led by principal investigators Xhorlina Marko, interventional radiologist at Beaumont Health (Dearborn, USA), Steven Abramowitz, chair of vascular surgery at MedStar Health (Washington DC/Leonardtown, USA), and Stephen Black, consultant vascular surgeon, Guy’s and St. Thomas’ Hospital (London, UK).
The first DEFIANCE patient was enrolled by Abdullah Shaikh, interventional radiologist at Allegheny Health Network (Pittsburgh, USA). DEFIANCE will enrol 300 DVT patients at up to 60 centres worldwide. DEFIANCE is Inari’s second RCT, enrolling in parallel to the PEERLESS pulmonary embolism trial.
“We are thrilled to enrol the first patient and officially kick off this important clinical trial,” said Shaikh. “ClotTriever is fundamentally different to other DVT treatments. This trial is designed to produce definitive evidence to change standard of care.”
“DEFIANCE is an important step forward and will answer critical questions about how we manage DVT patients,” said Abramowitz. “Prior RCTs have focused on thrombolytic-based interventions, which have known downsides and limited effectiveness. This ClotTriever RCT is the first to compare lytic-free thrombectomy to anticoagulation for DVT.”
“With six major clinical studies, including two ongoing RCTs, Inari is wholly committed to [venous thromboembolism] patients and producing definitive evidence to support our technologies,” said Thomas Tu, Inari’s chief medical officer. “None of this is possible without the collaboration and dedication of our clinical trial investigators, who continually push the field forward in the name of better patient outcomes.”
In a newly released “focused update” to their 2019 recommendations, the European Society for Vascular Surgery (ESVS) abdominal aortic aneurysm (AAA) guidelines writing committee has published advice on the surveillance and management of patients treated with the Nellix endovascular aneurysm sealing (EVAS) system (Endologix).
The committee advises that all patients in whom a Nellix device has been implanted “should be identified, properly informed and enrolled in enhanced surveillance.” If device failure is detected, it states that “early elective device explant should be considered in surgically fit patients”.
Boyle and colleagues note that they performed a scoping review of risk for late serious aortic-related adverse events in patients treated with EVAS for AAA based on a literature search in PubMed up to 7 December 2022. Following synthesis of the available evidence, the writing committee agreed on recommendations graded according to the European Society of Cardiology (ESC) grading system.
“EVAS has a very high incidence of late endograft migration resulting in proximal type 1 endoleak with risk of rupture, requiring open conversion with device implant,” the authors write, detailing their key finding from the review. They add that the reported mortality for elective explantation varies between 0% and 14%, while acute conversion for rupture has a “very dismal prognosis” with 67–75% mortality.
The authors detail that ESVS guidelines are renewed every five years or so, and that ESVS focused updates are issued “to convey important new data that have emerged in between the publication of the full guidelines, that affect patient safety or impact decision-making or management of the patients”.
In their 2019 guidelines on the management of abdominal aortoiliac artery aneurysms, the writing committee recommended that “conceptual new technologies, such as [EVAS], should only be used within studies approved by research ethics committees and with informed consent, until properly evaluated”.
In May of last year, Endologix ended production of the Nellix EVAS system, based on reportedly higher rates of leaks around the device’s implantation, endograft migration and aneurysm sac enlargement. The guideline committee recognised, however, that there was no clear guidance on surveillance and management of patients who have already undergone AAA repair with an EVAS device. It was for this reason that the ESVS AAA guidelines writing committee initiated a literature review on the topic. “The current accumulated knowledge suggests that patients treated with EVAS for AAA may be at high risk for serious aortic-related adverse events, which justified an updated guidance on the surveillance and management of patients already treated with EVAS,” they write in the new paper.
Commenting on the timing of the alert, the committee note that they decided it was important to publish before the fully updated guidelines will be available in 2024, “to highlight the issues with EVAS failure, to promote patient safety and to encourage clinicians to identify all patients in whom a Nellix device has been implanted”.
Viz.ai has announced the launch of Viz Vascular Suite—artificial intelligence (AI)-powered software enabling vascular care teams to automatically detect and triage care for suspected pulmonary embolism, right heart strain, aortic dissection, and abdominal aortic aneurysm (AAA). The company submitted a new 510(k) application to the US Food and Drug Administration (FDA) for the AAA algorithm, a press release notes.
“Recognising the symptoms of serious vascular conditions, such as aortic dissections, is hugely important because any delay in treatment can have a direct impact on patient outcomes,” said Philip Batista (Cooper University Health Care, Camden, USA). “When Viz identifies an abnormal scan, it quickly notifies the appropriate specialists regardless of their location, facilitating seamless communication via mobile application. We have been using the Viz software for the last several months and have seen improvements in patient care across our institution.”
Viz.ai claims that the Viz Vascular Suite uses AI to automatically analyse an array of imaging modalities, including computerised tomography (CT), electrocardiogram (ECG), and more for suspected vascular diseases. If a suspected pathology is found, the app automatically alerts and displays high-fidelity patient scans on providers’ mobile devices. Clinicians can use Viz Vascular Suite to remotely coordinate vascular pathology care within a hospital system’s hub and spoke network and enable synchronous, HIPAA-compliant communication among specialists. The platform is enhanced by AI for immediate team activation and facilitates informed, efficient treatment decisions.
“We set out to build a solution where any patient with life threatening diseases can benefit from AI-powered care coordination with triage and real-time mobile communication. The Viz Vascular Suite will bring the advantages of intelligent care coordination to even more patients and help clinical teams achieve better clinical outcomes,” said Chris Mansi, CEO of Viz.ai. “The feedback from our early adopters has been highly positive, and we look forward to expanding access to this solution to our over 1,300 hospital customer base.”
Cardiovascular Systems Inc (CSI) recently announced initiation of the KAIZEN clinical study of its Diamondback 360 peripheral orbital atherectomy system (OAS) for the treatment of calcified plaque in patients with peripheral arterial disease (PAD). The study is intended to support regulatory approval in Japan.
The first KAIZEN patient was enrolled by Tatsuya Nakama at Tokyo Bay Urayasu Ichikawa Medical Center (Urayasu, Japan).
Nakama said: “I felt that the Diamondback 360 peripheral OAS offered both effective treatment and ease of use. I was able to observe significant vessel compliance change, which permitted satisfactory balloon expansion at low pressure. Additionally, I felt that minimal distal embolism compared to other devices throughout the procedure was greatly comforting. I look forward to further evaluation of the device, but believe it will be seen as a highly welcomed tool in the battle against calcified vessels.”
CSI notes that the Diamondback 360 peripheral OAS is a minimally invasive, single-use, catheter-based device that is designed to differentiate between hard, diseased plaque and healthy, compliant arterial tissue. The OAS orbiting crown reduces and modifies calcified plaque while preserving the healthy vessel wall in order to restore blood flow, the company claims.
KAIZEN is a prospective, single-arm, multicentre study led by Hiroyoshi Yokoi (Fukuoka Sanno Hospital, Fukuoka, Japan). The study is designed to evaluate the safety and efficacy of CSI’s Diamondback 360 peripheral OAS in the treatment of de novo symptomatic calcified occlusive atherosclerotic lesions in the superficial femoral artery and/or popliteal artery. According to CSI, OAS has demonstrated safety and efficacy in the US population and this study is designed to confirm this in Japan. The study is expected to enrol up to 100 subjects at up to 12 study sites.
Yokoi said: “Severely calcified peripheral vessels continue to be a significant challenge for both patient and caregiver, and the need for new treatment devices is greater than ever. I believe the Diamondback 360 peripheral OAS has great potential for this underserved patient population, and I look forward to evaluating it in Japan. In addition, the high use of imaging by practitioners in Japan will provide greater insight into lesion morphology, and I am confident that this will also help us optimise treatment and safety using OAS.”
Scott R Ward, CSI’s chairman, president and chief executive officer, said: “We look forward to completing KAIZEN and working with the investigators and regulators so that we may offer peripheral OAS therapy to physicians in Japan.”
Medtronic has announced the first patient enrolment in the ADVANCE Trial, a head-to-head randomised controlled trial of two leading aortic stent graft systems, the Medtronic Endurant II/IIs stent graft system and GORE Excluder AAA device family systems. The ADVANCE Trial is a global, post-market, prospective, interventional, multicentre, randomised study that will enrol a minimum of 550 patients at up to 50 centres globally. Patients will be randomised to receive endovascular aneurysm repair (EVAR) with either the Endurant family or Excluder family grafts and will be followed at one month, one year, and annually through five years.
The first patient in the ADVANCE Trial was enrolled by the team led by Ray Workman at Novant Health Forsyth Medical Center (Winston-Salem, USA).
“Through the ADVANCE Trial, we are working to deepen our evidence of sac regression as a key indicator of long-term EVAR patient outcomes,” said Hence Verhagen, professor of Vascular Surgery at Erasmus Medical Center (Rotterdam, Netherlands) and co-principal investigator of the trial. “Our hope is that the findings will allow physicians to make evidence-based clinical decisions to improve long-term patient outcomes.”
The ADVANCE Trial aims to further the understanding of sac regression by robust evaluation of CT imaging utilising an independent core lab through five years. The trial will provide a comparison of aneurysm sac regression outcomes between the Medtronic Endurant II/IIs stent grafts and the GORE Excluder AAA device family stent grafts with additional evidence to analyse risk factors related to aneurysms that fail to regress. The trial will also compare other key clinical outcomes between the two stent grafts, including endoleaks, migration, secondary interventions, mortality, and renal complications.
“We are pleased to announce the first patient enrolled in the ADVANCE Trial,” said Marc Schermerhorn, chief of vascular and endovascular surgery, Beth Israel Deaconess Medical Center (Boston, USA) and co-principal investigator of the trial. “This milestone underscores the commitment to rigorous study of the long-term data around the durability of the Endurant system for patients in need of EVAR. The results of the trial aim to demonstrate contemporary outcomes and our overarching goal to deliver superior aortic patient care through robust and rigorous clinical data.”
The ADVANCE Trial draws on clinical data showing that one-year sac regression is an early indicator of improved long-term survival. The outcomes were consistent with the eight-year results from the ENGAGE OUS Registry, published in January 2022, which demonstrated the long-term clinical safety and effectiveness of the Endurant Stent Graft System. The ENGAGE OUS Registry followed subjects through 10 years.
The Endurant II/IIs bifurcated stent graft is indicated for the endovascular treatment of infrarenal abdominal aortic or aorto-iliac aneurysms. Endovascular stent grafting may be an option for patients who have an abdominal aortic aneurysm as determined by a vascular specialist.
Rivermark Medical has announced the successful first-in-human (FIH) use of its FloStent System as part of the company’s RAPID-1 FIH clinical study. The procedures were performed on 15 patients by Principal Investigator (PI) and urologist Ingrid Perscky Arravanti (Universidad de Panamá, Panama City, Panama) and proctored by Primary Clinical Advisor and urologist Dean Elterman (University of Toronto, Toronto, Canada) at the Pacifica Salud Hospital and the Panama Clinic in Panama City, Panama. The study evaluates the delivery, safety, and clinical effectiveness of the FloStent System for treating the symptoms of benign prostatic hyperplasia (BPH).
“I am pleased to be a part of the initial cases and remain very impressed by the performance of the FloStent System. I was able to easily position and deploy the implant with standard equipment, using familiar endoscopic techniques,” stated Perscky Arravanti, who is also founder of the Global Men’s Health Foundation. “This therapy is extremely attractive as it offers patients instant improvement in BPH symptoms without the inconvenience and discomfort of traditional treatments.”
The Flostent System is intended to be the preferred first-line device treatment for BPH. The outpatient procedure involves the placement of a nitinol stent during a routine flexible cystoscopy with minimal patient recovery time and no need for a urethral catheter. The stent gently holds the prostatic urethra open to restore normal urinary function, preserve sexual function, and improve a patient’s overall quality of life. If desired, the device can be easily retrieved or repositioned after implantation.
“Watching the FloStent procedures first-hand, I am enthusiastic about the ease of use and immediacy of BPH symptom relief,” said Dean Elterman, faculty member at the University of Toronto’s Division of Urology. “Being able to perform this procedure quickly using common flexible cystoscopes will allow urologists worldwide to offer the FloStent System in a variety of outpatient settings, making it easier for patients to seek and receive device treatment.”
“Today marks an important milestone as Rivermark transitions into a clinical-stage company,” commented Adam Kadlec, CEO of Rivermark Medical and practising urologist at Advocate Health in Milwaukee, USA. “We are excited at the prospect of being able to offer the most accessible BPH device therapy in the world—a first-line, minimally Invasive outpatient therapy that can be performed with existing equipment, offering BPH patients immediate and reliable relief. In the coming months, we look forward to building upon the momentum of our FIH experience by gathering additional clinical evidence demonstrating the value of the FloStent System.”
GE Healthcare announced it has entered into an agreement to acquire Imactis, an innovator in computed tomography (CT) interventional guidance across an array of care areas. Imactis is a France-based company that was founded in 2009 by Stéphane Lavallée and Lionel Carrat, who created CT-Navigation, an ergonomic universal solution that provides stereotactic needle guidance, enabling intuitive pre-planning and continuous control throughout a wide range of procedures, from diagnosis to treatment.
“We are thrilled to take this step in strengthening our interventional guidance offering for patients and customers,” said Jan Makela, president and CEO of imaging, GE Healthcare. “The Imactis CT-Navigation system is designed to improve workflow for interventional radiologists and hospitals by increasing procedural accuracy, while helping to reduce procedure time and radiation dose for patients and physicians. It is an innovative navigation solution for image-guided percutaneous procedures that aims for better patient outcomes, by reducing variability for simple and complex procedures and improving reproducibility.”
“The timing to join GE Healthcare is perfect,” said Pierre Olivier, president and CEO of Imactis. “Our solution, which is already deployed in leading healthcare systems in Europe and the USA, is ready to scale and become a standard of care, thanks to GE Healthcare’s market access. Our product development team also sees significant opportunities to integrate our hardware and software into GE Healthcare solutions and make the workflow of the interventional radiologists and oncologists even simpler and faster.”
While this innovation currently focuses on CT, GE Healthcare plans to expand the technology to its image-guided therapy (IGT) business to drive further growth.
The Imactis CT-Navigation, which includes an integrated workstation, guidance software, and disposable procedure kit, is currently approved under the European Union’s Medical Devices Regulation (MDR) and has US Food and Drug Administration (FDA) clearance for use within the USA.
The consummation of the transaction is subject to customary closing conditions, including review by the relevant governmental authorities in France. Financial details of the transaction have not been disclosed publicly.
Today, Penumbra announced the US Food and Drug Administration (FDA) clearance and launch of its Lightning Flash mechanical thrombectomy system.
“Lightning Flash features Penumbra’s novel Lightning intelligent aspiration technology, now with dual clot detection algorithms,” the company notes in a press release, adding that the system is designed to quickly remove large blood clots in the body, including venous thrombus and pulmonary emboli (PE).
“Penumbra’s Lightning Flash gives physicians a highly torqueable, larger catheter that is designed to remove a large clot burden in the pulmonary arteries or deep venous system more efficiently while maintaining an excellent safety profile because of Lightning’s computer-aided algorithms,” said James F Benenati, chief medical officer at Penumbra. “We believe that patients can have improved outcomes with this new technology because of the exceptional trackability and unique ability to distinguish flowing blood from clot.”
The company details that Lightning Flash, powered by the Penumbra Enging, uses both pressure and flow-based algorithms to detect blood clot and blood flow. The catheter is made with MaxID hypotube technology, allowing an inner diameter similar to large-bore catheters while maintaining a lower profile and a soft, atraumatic tip designed to help navigate the complex and delicate anatomy of the body. When used together, the device is intended to help remove blood clots quickly while minimising potential blood loss.
“Lightning Flash will fundamentally change how blood clots are removed from the body,” said Adam Elsesser, president and chief executive officer of Penumbra. “With this latest advancement, physicians are more likely to adopt mechanical thrombectomy because a broad spectrum of blood clots can be removed much quicker and less invasively than current interventional or surgical methods. This means that we are able to help even more patients with our technology, which is core to who we are as a company.”
Lightning Flash is part of Penumbra’s Indigo system with Lightning portfolio. The company claims that Lightning products are the only computer-aided mechanical thrombectomy systems currently available in the USA and early data have shown improvement in clinical outcomes and quality of life.
“Penumbra’s commitment to innovation and clinical excellence enables us to pioneer interventional therapies that have a significant impact on patients,” said Sandra Lesenfants, president of interventional at Penumbra. “Innovations such as Lightning Flash will continue to transform the standard of care for these difficult conditions, ultimately improving patient outcomes and allowing patients to return home quickly.”
Instylla has announced the enrolment of the first patient in the HALT study for the treatment of peripheral arterial bleeds. The HALT study is a prospective, multicentre, single-arm study to evaluate the safety and effectiveness of the Embrace hydrogel embolic system (HES) for the embolization of arterial bleeding in solid organs and peripheral arteries.
According to the American Association for the Surgery of Trauma (AAST), injury is a major public health problem accounting for over 150,000 deaths and over 3 million non-fatal injuries annually. Traumatic injuries, specifically pelvic and hepatic injuries, are the leading causes of haemorrhage in trauma patients. Transcatheter arterial embolization (TAE) has played an increasingly significant role in controlling haemorrhage, with an efficacy rate of 81%–100% in unstable pelvic fractures for example.
Acute gastrointestinal bleeding has a mortality rate ranging from 4% to 10%. TAE facilitates highly selective embolization of bleeding vessels, with clinical success rates of 74.7% in treating acute upper gastrointestinal bleeding.
“We are excited to have enrolled the first patient nationally in the prospective HALT study, evaluating an innovative, in situ-forming liquid embolic for haemorrhage control in patients,” commented David Tahour, chief of vascular and interventional radiology at MemorialCare Long Beach Medical Center (Long Beach, USA). “Embrace HES has demonstrated rapid and durable haemostasis in preclinical studies while reducing the risk of non-target embolization. I look forward to being involved with this innovative technology which will change the standard of care for future embolizations.”
The HALT study is led by Suvranu Ganguli, section chief, interventional radiology at Boston Medical Center (Boston, USA). The study is estimated to enrol 118 patients at up to 25 US sites. Patients with upper gastrointestinal bleeds, kidney, liver, or spleen bleeds, spontaneous haematomas, or other peripheral arterial bleeds such as pelvic haemorrhage may be considered suitable for this study.
“I would like to thank Dr Tahour and his team for their effort in achieving this significant clinical milestone,” said Amar Sawhney, Instylla CEO. “We are excited to study the performance of the Embrace HES in this additional indication, which reflects the versatility of this novel liquid embolic.”
Synchron has announced that the medical journal JAMA Neurology has published peer-reviewed, long-term safety results from a clinical study in four patients with severe paralysis implanted with the company’s first-generation Stentrode neuroprosthesis device. The study found that it is possible to use the neuroprosthesis device to transmit neural signals from inside a blood vessel in the brain over a long-term period without any serious adverse events related to the device.
The SWITCH (Stentrode with thought-controlled digital switch) trial—a first-in-human study—evaluated four patients implanted with Synchron’s Stentrode. Patients participating in the study completed a 12-month follow-up with no persistent neurological deficits. There were no clots or migrations of the device, a Synchron press release reports, and signal quality remained stable with no evidence of significant deterioration.
In addition, each participant successfully controlled a personal computing device with the brain-computer interface (BCI). They were able to use the implant to generate digital switches under intentional control for routine digital activities, such as texting, emailing, personal finance, online shopping, and communication of care needs, the release adds.
The study was led by Peter Mitchell, the neurointerventionist who performed the procedures, and vascular neurologist Bruce Campbell (both University of Melbourne, Melbourne, Australia). The procedures were performed in a neurointerventional angiography suite.
“We carefully conducted this first-in-human study with a primary focus on safety. The patients all tolerated the procedure well and were typically discharged home within 48 hours,” said study co-principal investigator Mitchell. “The widespread availability of the angiography suite for this procedure could promote a rapid translation of BCI for people with paralysis.”
As a Synchron press release notes, paralysis may result in a loss of control of muscles in the body, while the brain can remain intact. Motor intent is the brain signal underlying the physical will to move, and a BCI is designed to restore the lost motor intent signal transmission associated with paralysis. The device is implanted in the motor cortex of the brain via the jugular vein in a minimally invasive endovascular procedure. Once implanted, it detects and wirelessly transmits motor intent in order to control personal digital devices.
In the SWITCH trial, motor intent was detected using a robust decoder that searches for power changes in certain frequency bands. The digital switches were executed under the volitional control of frequency band shifts by the users.
Synchron’s first-generation system was developed in partnership with Ripple LLC and utilised Ripple’s neural sensing technology to provide core signal acquisition, data telemetry and signal processing capabilities, the release also states.
“This technology holds great promise for people with paralysis who want to maintain a level of independence,” added co-principal investigator Campbell. “The Stentrode enables a form of motor restoration, with individuals able to use the switches to communicate and engage with their digital world.”
“The SWITCH study is an early demonstration of safety in a low number of participants using a commercial grade BCI. The decoder was simple and robust, meaning that patients did not have to train hard to execute switches,” said Tom Oxley, CEO and founder of Synchron. “Our view is that a motor neuroprosthesis should be safe and easy to use. Digital switches controlled by motor intent could translate into a meaningful restoration of motor capability for patients with paralysis and the return of things we take for granted, like texting loved ones or turning on a light.”
The publication of this study follows Synchron’s announcement of ongoing patient enrolment in the COMMAND trial at Carnegie Mellon, the University of Pittsburgh and Mount Sinai Hospital in the USA to assess safety and explore quantified efficacy measures of Stentrode. Three out of six participants have been enrolled in the COMMAND trial, with the clinical trial sites still actively looking for the next participants.
Fluidx Medical has released information regarding the success of the IMPASS Embolic Device in in vivo research related to middle meningeal artery (MMA) embolizations which can be used to treat chronic subdural haematomas (CSDH) on the surface of the brain.
CSDH is a common pathology that can result in death and/or disability in patients. The typical treatment of CSDH involves drilling a hole in the skull and draining the blood. Minimally invasive catheter-based MMA embolization can be an alternative to surgical treatment.
“We have been listening to clinicians and they need better tools to treat CSDH,” says Danny Smith, vice president of research and development for Fluidx. “We designed the IMPASS embolization device to work with standard embolization catheters and embolize microvasculature in the MMA. Our results are encouraging and the IMPASS product could be a great solution to unmet patient needs.”
MMA embolization is a promising option to address CSDH and is particularly appealing for elderly patients and others who cannot undergo invasive surgical procedures. Hundreds of thousands of patients with CSDHs may benefit from this minimally invasive procedure. During the procedure, a small catheter is navigated into the MMA located within the dura mater which covers the brain, then an embolic material is delivered into the vessel to block arterial flow.
The Fluidx embolic platform is expected to bring simple preparation and controllable material delivery to a range of applications. The IMPASS device is packaged in a ready-to-use syringe, can be prepped tableside by the clinician in about 30 seconds, and may be delivered through standard microcatheters (no complex mixing systems or special delivery catheters are necessary).
Speaking to Interventional News at the recent Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain), Arthur Rocha (São Paulo, Brazil), from professor Carnevale’s team, shares the development of an optimised imaging workflow—which consists of “cone-beam computed tomography (CBCT) from the internal iliac artery as the main imaging and the use of embolization planning and guidance software such as Embo ASSIST (GE HealthCare) to improve anatomy assessment and prostate artery embolization (PAE) planning and navigation.
Arthur Rocha outlines some of the advantages of CBCT with software such as Embo ASSIST compared to digital subtraction angiography (DSA), noting that it helps “avoid misleading identification of the origin of the prostatic artery, which would make navigation difficult, as well as identify secondary prostatic arteries which, if not embolized, may lead to symptoms recurrence”.
He examines past literature on PAE and how it relates to a recently conducted study which showed that CBCT helped find almost four times more secondary arteries than previously described based on DSA only. “We recommend routine use of CBCT imaging with augmented planning and guidance software to improve PAE outcomes,” concludes Arthur Rocha.
Lydus Medical is pleased to announce that the Vesseal has received US Food and Drug Administration (FDA) 510(k) clearance. The Vesseal is a microvascular anastomosis suture deployment system, for standardised omnivessel anastomoses, enabling simple, fast, safe, and effective procedures.
An anastomosis is one of the most complicated steps of microvascular surgery and fundamental to the success of these demanding surgical interventions. Varied clinical fields require microvascular anastomosis, including breast reconstruction; head and neck reconstruction; surgical lymphoedema treatment; and vascular access for haemodialysis.
Until now, microvascular anastomoses have been performed manually. Manual microanastomoses are time- and labour-intensive, require a long learning curve, a unique skill set and great surgical dexterity. The Vesseal is designed to mimic the skill set and dexterity needed to deliver quality patient care in microsurgical anastomoses. It provides, simple, accurate, dependable and consistent results through symmetrical placement of eight microsutures at the anastomosis site.
“FDA clearance of the Vesseal is a significant milestone both for innovation in microvascular anastomoses, and for Lydus Medical. It is common knowledge that there are large clinical unmet needs around microvascular anastomosis,” said Jessica Weiss, CEO of Lydus Medical. “Clinicians who used the Vesseal stated that it shows a significant advantage over the manual anastomosis and provides more consistency in the procedure. We believe that the Vesseal will support enhanced outcomes in microsurgical procedures, as well as improved patient care.”
Paula Novelli, who is associate professor of interventional radiology (IR) at the University of Pittsburgh Medical Center (Pittsburgh, USA) put her own spin on a British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK) presentation titled ‘Women are more likely to work part-time’. The ‘myth-busting’ session as a whole saw speakers weigh in on how gendered perceptions and, in some cases, realities, can impact women interventional radiologists’ careers. Novelli in particular, bringing the perspective of ‘the only girl in the gang’—the gang being her IR team at Pittsburgh—left delegates with the salient message that “on all levels”, women are not overinvesting in education, despite the fact that, in the USA, “women practise fewer total hours than men due to significant household responsibilities.”
Novelli began her presentation remarking that, based on a 1970s survey of 97 male and 95 female doctors, 59% of the female respondents and 87% of the men had been working full-time from graduation, with 17% of the women not working due to taking on a traditional ‘female’ role instead. The prevailing thought at the time was that medical education of women in the USA was a poor investment due to the likelihood of women practising fewer hours over their professional lifetimes. Yet, despite these figures, Novelli conveyed that the findings demonstrated “women spent 90% as much time in medical work as did men, accounting for childbearing responsibilities.” This points to the idea of the “superwoman”, the presenter elaborated—female doctors may be working fewer overall hours, but they work with increased productivity.
More current than the previous data, Novelli then highlighted a British Medical Journal (BMJ) op-ed from 2008, which professed the opinion that women doctors were concentrated in “family-friendly” specialties, including paediatrics, psychiatry and family medicine. This was considered to be a “ticking timebomb” since women are more likely to work part-time, and this “feminisation” of these family-friendly specialties would mean that the specialties would disproportionately suffer the implications of part-time working and maternity leave, such as lack of continuity of care and resource use.
However, recent data on the state of women in academic medicine from the Association of American Medical College (AAMC) Novelli countered, while “difficult to interpret” because of varying definitions of what percentage of full-time work part-time constitutes, suggests that among part-time doctors, there is an almost equal male-female split. The figures she cited were 50.1% of male part-time medical faculty, versus 49.9% women.
The “leaky pipeline” in IR
Bringing the focus to IR specifically, Novelli noted that radiology and surgery are “up there” when it comes to the specialties in which the aforementioned part-time doctors are concentrated, but that, as shown by the statistic, this is not due to a higher number of women faculty members in these specialties.
Yet, according to a Journal of the American Medical Association (JAMA)-published study of parental status among early-career physicians, the object of which was to determine which factors influence doctors’ decisions to work part-time or full-time, 75% of female participants said they were considering reducing their hours. Novelli underlined the importance of this “early gap” in hours practised between men and women, reaffirming the definite gender imbalance in this regard with anecdotal evidence: “I have never worked with another female IR [interventional radiologist] in my entire 18-year [IR career]”. The leaky pipeline will perpetuate the gender imbalance in medicine for the foreseeable future, Novelli posited.
The mental “toll” on women in IR
Novelli then brought burnout among interventional radiologists into the picture, flagged how, as found in a recent Society of Interventional Radiology (SIR) questionnaire, burnout was “significantly higher” than among diagnostic radiologists, and, pertinent to the current discussion, also among women over men. Similarly, Novelli added, another JAMA study assessing depression among doctors just post-medical school found that the rate was also higher among the female respondents.
A theory Novelli brought to explain this phenomenon was that, perhaps, women need to work harder: “I do believe that we need to work harder in any academic setting just to prove ourselves.” This “toll” medicine takes on women is multifactorial, the presenter furthered, stating that female doctors are more likely to be reported, have fewer advancement opportunities, and less likely to become full professors or academic leaders. “We are not really learning from the past,” Novelli lamented, explaining that since the seventies, there have been calls for women to receive more flexibility and respect to foster their advancement. “We need to eliminate biases and harassment,” was one of Novelli’s own calls regarding how to successfully support women in their medical careers.
Women are currently supported to some extent, Novelli acknowledged, mentioning the BSIR’s pamphlet that informs women of the scope for flexibility around training and provides guidance on radiation exposure for those of childbearing age who may be concerned about this aspect of an IR career.
Investment in women in medicine not misplaced
“Today, the total training cost per diagnostic radiology resident is US$99,000 a year on top of the half-a-million that they pay to become a physician academically,” was Novelli quantifying for the audience members the extent to which embarking on becoming a radiologist in the USA is a significant financial undertaking. Be this as it may, she opined that women are not “overinvesting” in their medical education, as their practices, even if they do not work full-time hours, provide the same level of patient care.
Novelli’s parting words were that “as the only girl in the gang” she has been “called into the principal’s office” many times—this refers back to how it is harder to be a woman in medicine, how the standards to which women are held are higher. “But I have been able to maintain the support of family and work/life responsibilities,” she celebrated. Novelli then admitted that she is “still waiting for her ‘Me Too’ moment and is “not sure” that her 16-year-old daughter should pursue a career in medicine as “there is still a lot of work to do.”
Subsequent discussion around the subject of Novelli’s presentation drew out the sentiment that her point about not necessarily encouraging her daughter to go into medicine was “[disheartening]”. This then raised the question of whether women could be the predominant source of negative comments dissuading fellow female doctors or trainees from pursuing IR. Mentorship was suggested as an antidote for women’s reticence about entering into a field which may have seemed, traditionally, not to be a good “fit” for women. “[The mentor need not] be a woman,” was Shilpi Pal’s (Ninewells Hospital, Dundee, UK) view—“[just] someone who has been in your shoes”.
Interventional News covered a whole range of the specialty’s news during 2022, but readers’ attention was most piqued by acquisitions (Boston Scientific’s of Obsidio and Bentley’s of the GoBack catheter); study results from meetings that highlighted the “potential” and “promise” of both renal denervation and prostatic artery embolization (PAE); and the launch of a first-in-human trial of a sirolimus drug-coated balloon (DCB) for peripheral indication.
In August, Inari Medical announced planned enrolment of the DEFIANCE randomised controlled trial (RCT), which is designed to compare the clinical outcomes of patients with iliofemoral deep vein thrombosis (DVT) treated with the ClotTriever system versus anticoagulation only.
Also in August, Boston Scientific shared the news of the acquisition of Obsidio, a privately held company that has developed the Gel Embolic Material (GEM) technology used for embolization of blood vessels in the peripheral vasculature.
Late-breaking trial data presented at EuroPCR 2022 (17–20 May, Paris, France) underscored the potential of renal denervation as an adjunctive therapy to treat hypertension, complementing existing first-line treatments including lifestyle modifications and medication, attendees of the conference heard.
Tiago Bilhim (Saint Louis Hospital, Lisbon, Portugal) presented during the Scientific Paper session at this year’s European Conference on Embolotherapy (22–25 June, Nice, France), and won the award of best abstract for his and co-authors’ ‘Long-term outcome of prostatic artery embolization for patients with benign prostatic hyperplasia’.
Again in August, BD announced the start of enrolment in the PREVISION first-in-human trial, a prospective, multicentre, single arm, non-randomised study designed to evaluate the safety of the BD sirolimus DCB in the treatment of peripheral arterial disease (PAD) in the femoropopliteal arteries.
In November, Otsuka Medical Devices and ReCor Medical, a subsidiary of Otsuka, shared the news that they had filed a pre-market approval (PMA) application to the US Food and Drug Administration (FDA) for the Paradise ultrasound renal denervation (uRDN) system in the treatment of uncontrolled hypertension.
September also saw Medtronic share that it received CE mark for its Radiant balloon-expandable covered stent, the first and currently, only, covered stent indicated for use in chimney endovascular aneurysm repair (ChEVAR) with the Endurant II/IIs stent graft system.
AVS has announced that it raised US$20 million in Series B financing, which the company says will accelerate clinical trial timelines for its device for peripheral application in pulsatile intravascular lithotripsy (PIVL) cases and advance development and preclinical work on a PIVL device for coronary cases.
BioStar Capital, the lead investor in the company’s Series A round, also led the Series B round. BioStar Capital is focused on transformational investments in medical technologies with an emphasis on cardiovascular and orthopaedics.
“AVS is one step closer to offering a new treatment solution for patients with severely calcified peripheral arterial disease and progressing toward preclinical studies for coronary cases,” said Mark Toland, managing director for BioStar Capital and executive chairman/CEO of AVS. “Patients in this disease state too often face the prospect of limb amputation due to a lack of treatment options. We see a significant opportunity to address that need and advance the intravascular lithotripsy space through minimally invasive technology in both peripheral and coronary therapy.”
AVS’s novel balloon-based platform, the Pulse IVL system, shatters calcium with pressure waves in frequent bursts and expands calcified arteries, all with a single device.
“We are proud to support AVS in both its successful Series A and Series B funding rounds,” said Louis Cannon, founder and senior managing partner of BioStar Capital. “The preclinical results of the Pulse IVL System have shown the potential to raise the standard of care and significantly impact the wellbeing of patients with calcified arterial disease. We are excited to partner with AVS as it looks to future clinical trials and development.”
In September 2022, AVS announced enrolment, successful treatment, and positive 30-day follow-up data of the first patients in its POWER PAD I clinical trial, a first-in-human study. Jon George (University of Pennsylvania Health System, Philadelphia, USA) an interventional cardiologist at the and medical advisor to AVS, assisted in trial cases in the Dominican Republic.
“Our early trial results showed that we can successfully treat patients with multiple lesions using a single device,” said George. “We saw patients report a reduction in leg pain, increase in blood flow to the leg, and improvement in their ability to walk in our initial study. This is a patient population that needs easier access to advanced therapies and this platform has the potential to provide that access.”
Cardiovascular Systems (CSI) announced that Innova Vascular (Innova) has submitted a 510(k) premarket notification to the US Food and Drug Administration (FDA) for its thrombectomy devices intended to treat peripheral vascular disease.
CSI intends to acquire and commercialise each of the novel thrombectomy devices from Innova targeting peripheral vascular disease. Commercialisation of the thrombectomy devices will be complementary to CSI’s broader portfolio of advanced technologies used in the treatment of cardiovascular disease.
Sanjay Shrivastava, CEO of Innova, said, “the FDA submission of the thrombectomy devices for use in the peripheral vasculature marks an important milestone in our commitment to develop innovative technologies targeting large, underserved markets. We are excited to partner with CSI, which has been serving the interventional cardiology, interventional radiology, and vascular surgery communities that will be the primary users of this thrombectomy system.”
Pending regulatory clearance in the USA and completion of the acquisition of the first Innova system, CSI could begin to commercialise a portfolio of aspiration catheters and clot retrieval devices for use in peripheral vasculature in approximately six months. The portfolio and corresponding indications for use will be expanded to include the treatment of deep vein thrombosis and pulmonary embolism following completion of the respective clinical trials and subsequent 510(k) clearances. These trials are expected to begin enrolling later in 2023.
Scott R Ward, chairman, president and CEO of CSI said, “CSI’s strong commercial presence, with over 150 peripheral sales representatives, will make thrombectomy an excellent fit as we seek to reach more patients and drive increased revenue through our sales channel beginning later this year.”
Under the terms of the agreements signed with Innova, CSI has provided financing to Innova for the development of the thrombectomy devices. Under an acquisition option agreement, upon Innova’s completion of key technical, regulatory and clinical milestones in the development program, CSI will have exclusive rights to acquire the thrombectomy devices, subject to the satisfaction of closing conditions set forth in the agreement.
IceCure Medical, developer of the minimally-invasive ProSense System for cryoablation, which destroys tumours by freezing, today announced interim results from the ICESECRET study for the treatment of patients with small renal masses (SRM) who cannot be offered kidney-preserving surgery. Data were presented at the Urological Association Conference (14 December, Eilat, Israel). The presentation, titled “Renal Mass Cryoablation – Interim Analysis ICESECRET Study”, was delivered by Nasir Said (Bnai Zion Medical Center, Haifa, Israel).
According to the presentation, out of the 115 patients enrolled, 107 patients (112 lesions) returned for follow-up with a mean duration of 22.8 months and a range 12-60 months. In a subgroup of patients with no previous history of kidney cancer on the same kidney and a lesion ≤3cm, an 89.5% recurrence-free rate was observed at a mean follow-up time of 22.2 months when the procedure protocol was followed.
The recurrence-free rate was 85.1% for the 107 patients (91 patients, including 13 patients who underwent a second cryoablation), at a mean follow-up period of 16.5 months. Five serious adverse events were reported, four of which were of mild severity and were treated conservatively and resolved within one to five days, with one severe complication of a new onset of ipsilateral hydronephrosis seven months after the cryoablation procedure that led to nephrectomy.
Cryoablation time and hospitalisation time were relatively short, up to approximately 25 minutes and two days, respectively. The presentation concluded that, based on these interim results, cryoablation is safe and effective for treating renal masses under five centimetres.
According to the American Journal of Roentgenology, small renal masses, which may be malignant or benign tumours in the kidney, have been rising in incidence over the past two decades. According to the American Cancer Society, in 2022, in the US, an estimated 79,000 new cases of kidney cancer will be diagnosed, with about 14,000 dying from the disease. Globally, there were more than 430,000 new cases of kidney cancer in 2020 and about 180,000 deaths according to World Cancer Research Fund International.
“These impressive interim results demonstrate the value of ProSense for urologists and interventional radiologists as a therapeutic alternative when patients are not eligible for surgery,” stated IceCure’s Chief Executive Officer, Eyal Shamir. “We believe the findings will support further use of ProSense in the jurisdictions in which our cryoablation system is approved for use with benign and malignant tissues of the kidney. The growing body of data on ProSense’s efficacy and safety across a broad range of indications supports commercialization momentum, particularly in facilities that benefit from one device that can be used across multiple specialties.”
ICESECRET, a prospective, multicentre, single-arm clinical trial is being performed at Bnai-Zion Medical Center, Haifa, Israel, and Shamir Medical Center, Zerifin, Israel, and led by principal investigator Halahmi Sarel (Bnai Zion Medical Center, Haifa, Israel). The trial included 115 patients (138 lesions) with localized SRM of ≤5cm who were treated with ProSense cryoablation under computed tomography (CT) guidance. Full engulfment of the renal lesion, including a safety margin of 0.5cm was achieved in approximately 96% of the procedures where there was no anatomical limitation. Follow-up visits are performed 6 weeks, 6 months, 1 year, and then annually up to 5 years after the procedure. During the follow-up visits, data related to local recurrence, based on CT imaging, is collected. Safety was determined by monitoring procedure-related adverse events throughout the study.
ReCor Medical and its parent company Otsuka Medical Devices have announced the appointment of Lara Barghout as president and chief executive officer of ReCor.
Barghout will lead the ReCor business strategy and organisation in the global commercialisation of ReCor’s Paradise ultrasound renal denervation system for the treatment of hypertension. She brings more than 20 years of experience leading global businesses in the medical device industry, joining ReCor from Siemens Healthineers, where she was senior vice president and head of advanced therapies, leading the image guided therapy business in North America. Prior to Siemens Healthineers, Barghout held several roles at Terumo Cardiovascular.
“I am honoured to lead the extraordinary team at ReCor at an exciting time in the company’s growth,” said Barghout. “High blood pressure is a leading contributor to cardiovascular disease burden worldwide, resulting in increased patient risk and higher costs to health systems. I look forward to leading our focus to advance ultrasound renal denervation as a treatment for hypertension and the global commercialisation of the Paradise ultrasound renal denervation system. We believe our Paradise ultrasound renal denervation technology to be a true game changer in improving hypertension therapy, with the potential to offer a new option for physicians to help improve blood pressure outcomes for their patients on a global scale.”
“We are delighted to name Ms Barghout President and CEO of ReCor. She is a highly experienced leader with a track record of commercial success across a range of medical device businesses, coupled with extensive experience in global leadership,” said Noriko Tojo, executive director of Otsuka Holdings and president of Otsuka Medical Devices. “We are very excited for Ms Barghout to lead ReCor into its next phase of global growth. Her deep commercial experience and adept leadership make her ideal to build on the technology development and clinical trial successes of the ReCor team, guiding the business to realise its therapeutic and commercial potential. I would like to thank Andy for his outstanding leadership and countless contributions over the past 10 years.”
The Paradise system bears the CE mark for the treatment of hypertension in Europe and is an investigational device in the USA and Japan.
Lung nodule biopsies performed with new robotic bronchoscopy technology may be safer and more effective than those done by traditional methods, a study by researchers at the University of Texas Southwestern (UTSW; Dallas-Fort Worth, USA) suggests.
UTSW was among the first in the country to use robotic-assisted bronchoscopy (RAB) to biopsy pulmonary lesions. Paired with advanced imaging that provides real-time 3D visuals, the technology enables UTSW’s Interventional Pulmonology team to navigate an ultra-thin, ultra-flexible tube with light and camera capabilities into a patient’s lungs to pinpoint and test suspicious abnormalities.
The increased dexterity of the steerable tube makes it possible to safely reach areas in the lungs that could not be accessed through traditional bronchoscopy and other sampling tools.
A retrospective analysis of 200 of those procedures found that shape-sensing, robotic-assisted bronchoscopy (ssRAB), when combined with technologies such as intraprocedural cone beam computed tomography imaging (CBCT) and radial endobronchial ultrasound, offers high diagnostic accuracy, sensitivity, and specificity with an excellent safety profile. The findings were published in Lung.
“The goal of advanced bronchoscopy is to diagnose lung nodules and perform mediastinal staging in a single procedure, while achieving a comparable diagnostic yield to percutaneous biopsy and at the same time, minimising complications,” said Kim Styrvoky, assistant professor of internal medicine in the Division of Pulmonary and Critical Care Medicine at UTSW, and Muhanned Abu-Hijleh, professor of internal medicine in the Division of Pulmonary and Critical Care Medicine.
“The diagnostic yield of current bronchoscopic techniques is limited, and there is about a one-in-four chance of pneumothorax, or collapsed lung, with percutaneous biopsy,” Styrvoky said. “Our study showed that this new technology provided accuracy of 91.4%, on par with traditional biopsy methods, while reducing the risk of pneumothorax complication to 1%.”
Lung cancer remains the leading cause of cancer-related deaths for both men and women in the USA. Each year, between 1.5 million and two million pulmonary nodules are identified through diagnostic imaging. UTSW is using robotic bronchoscopy in cases where traditional biopsies present a higher risk of complications, including patients with lesions deep in the lung, near major blood vessels, or adjacent to a portion of diseased lung.
This was UTSW’s first reported study detailing the usage of ssRAB-CBCT, but other trials focusing on various aspects of robotic bronchoscopy are underway.
If further studies confirm the findings, ssRAB-CBCT has the potential to become the standard of care for targeted lung sampling, Styrvoky and Abu-Hijleh said.
RF Medical is a Korean thermal ablation system manufacturer and the creator of the Mygen M-3004 generator and specialised electrodes including Myoblate. Both of these products have been cleared by the US Food and Drug Administration (FDA) and are now commercially available in the USA.
RF Medical’s chief executive officer Mike Jun imparted that the company is delighted to extend some of its finest medical equipment to the American market. Jun is confident that Mygen and Myoblate will empower US-based medical facilities and practices, and will modernise the standard of care for minimally invasive practices in the USA.
According to Jun, RF Medical’s commitment to developing effective, affordable, and minimally invasive medical devices is embodied in its latest inventions, communicating the following:
“The world’s medical device market is showing remarkable growth driven by cutting-edge minimally invasive technology and its industrial value is limitless. RF Medical is working diligently in an effort to keep pace with the advanced medical market. Improving the health and safety of mankind is our top priority and we are dedicated to carrying our mission as a leading medical device company through continuous investments in superior workforce and research and development.”
The Mygen M-3004 is a medical device that enables a combination of monopolar and bipolar modes. In addition to delivering radiofrequency energy more effectively, it also supports optimised algorithm modes for use in a variety of lesions depending on their size and shape.
The clearance of the Myoblate system is expected to bring another option to women suffering from uterine fibroids. A recent study showed that approximately 70-80% of women will experience this condition at some point; the Myoblate system will then be a less invasive, and more patient-friendly alternative to hysteroscopy or myomectomy.
Myoblate electrodes are intended for soft tissue coagulation and ablation to treat fibroids in a minimally invasive manner.
Myoblate utilises radiofrequency ablation to safely treat fibroids individually while keeping the uterus intact. According to Ben Ovenden, Business Director of RF Medical, USA, “Myoblate is the only RFA system for the treatment of uterine fibroids that utilises a wide range of approaches, unlike existing ablation technology.”
VentureMed Group, a privately held medical device innovator in access management for arteriovenous (AV) fistulas and grafts and vessel preparation for interventional treatment of peripheral arterial disease (PAD) announced data presented at the VEITHsymposium, (15–19 November, New York, USA). Overall, the data presented demonstrated that Flex vessel prep used prior to balloon angioplasty improves 12-month outcomes both in PAD and AV fistulas and grafts.
“AV Access management is a critical component of successfully treating AV patients over time,” said John Aruny (Dialysis Access Institute, Orangeburg, USA), primary investigator of the Flex Vessel Prep AV registry clinical study, the 12-month outcomes of which he presented at VEITH. “The FLEX AV Registry 12-month outcomes shows that utilising Flex vessel prep provides more time between interventions and continues to excel in the very difficult cephalic arch lesions.”
The study was a single arm, prospective study conducted in eight centres in the USA with 114 real world patients.
The Flex AV Registry 12-month outcomes demonstrate sustained patency across most patients and particularly good results specifically in the cephalic arch.
49% patency for all AV fistula patients (comparable historical data 26%)
59.7% patency for cephalic arch lesions (comparable historical data 0–33.9%)
AV grafts had average time to target lesion revascularisation of 228 days (41.2% patency at nine months)
No observed serious adverse events.
“Vessel preparation has become a necessary step for better patient outcomes,” said Eric Secemsky, director of vascular intervention, Beth Israel Deaconess Medical Center (Boston, USA), who presented the 12-month results of the Belong study with Flex vessel prep system prior to drug-coated balloon (DCB). “Vessel preparation in PAD with Flex creating longitudinal microincisions prior to DCB therapy had impressive freedom from clinically driven target lesion revascularisation and looks to improve outcomes by lowering balloon inflation pressures and potentially enhancing drug delivery.”
The Belong study was a single-centre, single-arm, prospective study conducted with 41 patients in Fribourg, Switzerland.
12-month efficacy results:
97.5% (39/40) freedom from clinically driven target lesion revascularisation
84.2% (32/38) freedom from target lesion restenosis via duplex
Corindus has been rebranded to Siemens Healthineers Endovascular Robotics and will sit as a dedicated business within the Advanced Therapies area of Siemens Healthineers, the company has announced.
This brand unification is the final step of the company integration process that commenced in 2019 with the acquisition of Corindus by Siemens Healthineers, the company says in a press release. The aim of the Endovascular Robotics business is to advance interventions with robotics and change the way that care is delivered through innovations that enhance physician technique and bring precision to interventional procedures, the press release adds.
Siemens Healthineers Endovascular Robotics says it will continue to offer the CorPath GRX system to support endovascular procedures while working to revolutionise treatment of emergent conditions by developing technologies to provide specialised and timely medical care to more patients around the world.
Wayne Markowitz, worldwide executive vice president of Siemens Healthineers and head of endovascular robotics, said: “The completion of our brand evolution marks the final step to becoming a united company and we remain focused on pioneering breakthroughs for everyone, everywhere. Our flagship product, the CorPath GRX system, is designed to support endovascular interventions, and we look forward to working with our customers as Siemens Healthineers Endovascular Robotics while fuelling our vision to connect more patients to advanced care.”
Efemoral Medical has today announced the closing of its US$4.9 million preferred Series A1 round. Supported by existing investors as well as an experienced cohort of new investors, the proceeds will further Efemoral’s device development and expand enrolment in its ongoing first-in-human clinical trial, EFEMORAL I, investigating the Efemoral vascular scaffold system (EVSS) with FlexStep technology.
The new funds will also complement Efemoral’s recently announced phase II Small Business Innovation Research (SBIR) grant award, which will support pre-clinical studies.
The EVSS with FlexStep technology offers a new approach to treating peripheral arterial disease (PAD) by addressing the specific anatomical challenges and complex biomechanics of patients with athero-occlusive disease in the leg, Efemoral states in a press release. Through the use of inter-scaffold spaces, the patented FlexStep technology combines flexibility with support to accommodate tortuosity and skeletal movement, while the balloon-expandable deployment system is designed to open vessels and sustain healthy blood flow. The novel bioresorbable scaffold with long-term Sirolimus elution aims to restore normal vessel diameter at the time of the procedure, deliver therapeutic benefits across all lesion lengths and morphologies, prevent restenosis, and maintain patency while leaving no permanent implant behind, the company’s statement adds.
“The implantation of strong, balloon-expandable, drug-eluting stents has conclusively been shown to be the best therapy for diseased human arteries. Their results in the coronary arteries of the heart have been no less than spectacular,” said Lewis B Schwartz, co-founder and chief medical officer (CMO) of Efemoral Medical. “However, these rigid devices cannot be safely implanted into the arteries of the legs because they would be crushed as the patient walks or sits. The EVSS uses a unique design of alternating dissolvable scaffolds and spaces that, for the first time, allows the long arteries of the legs to be treated with the same, effective, balloon-expandable technology proven to be successful in other human vascular beds.”
“The initial clinical experience in EFEMORAL I has demonstrated that the EVSS has the potential to be a highly effective treatment for femoro-popliteal disease,” said Christopher Haig, co-founder and chief executive officer (CEO) of Efemoral Medical. “This new funding will allow us to build additional confidence in our device by taking it to multiple hospitals and enrolling more patients. We remain committed to advancing the science behind our device and are excited about the potential of our technology to offer a durable clinical solution to patients and physicians.”
Cook Medical announces John A Kaufman (Cook Medical, Bloomington, USA) will be joining as its chief medical officer, effective July 2023. With Kaufman’s expertise and new appointment to this position, Cook is taking a significant step in its clinical and product-related goals.
Kaufman is an interventional radiologist with 30 years of experience. In 1982, he earned his doctor of medicine from the Boston University School of Medicine. He interned at the hospital of the University of Pennsylvania. Then, he finished a residency at Boston University/Boston City Hospital, later becoming chief resident in radiology, completing a fellowship in vascular and interventional radiology there as well.
Throughout his career, his research has focused on aortic aneurysms, venous diseases, vascular malformations and image guide treatment of liver cancers and uterine fibroids. Then, in 2010, he earned an MS degree in healthcare management from the T.H. Chan School of Public Health at Harvard. Kaufman is the inaugural chair of the Dotter Department of Interventional Radiology, director of the Dotter Interventional Institute and the Frederick S Keller professor of Interventional Radiology at the Oregon Health & Science University (OHSU) in Portland, Oregon.
In addition to practicing medicine and being a professor, Kaufman has been involved in many societies. He is active in the American Heart Association, American Board of Radiology, American College of Radiology, American Roentgen Ray Society and Radiological Society of North America. As a long time fellow of the Society of Interventional Radiology (SIR), Kaufman served as SIR president. SIR named him as the 2012 Dotter lecturer. Additionally, he is a fellow of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE). Both SIR and CIRSE awarded Kaufman gold medals for his research and his passion for education.
“We are honoured to have Kaufman join Cook Medical and add his unique expertise to our leadership team. We’ve followed Kaufman’s work for years and it’s evident that we share the same value of putting patients first. He will bring a unique insight into the needs of clinicians, patients, and scientists as we work together to move the practice of medicine forward,” said Pete Yonkman, president of Cook Medical and Cook Group.
In his role as chief medical officer, Kaufman will represent the company to regulatory and legislative agencies, advise on the educational needs of the clinical community and patients, serve as voice of the patient to ensure understanding and promote the future of minimally invasive interventions within Cook. The chief medical officer will also serve as clinical resource for engineers, marketing and ethics and compliance officers, as well as provide strategic input on current devices and programs.
“I look forward to sharing my perspective from the front lines of patient care,” said Kaufman. “One thing I am particularly passionate about is education. Teaching and learning have been staples in my career, and medical education is integral to Cook’s product philosophy. Most importantly, joining Cook is a beautiful opportunity to be a liaison between the scientific community and patients as we learn together how we can improve patient lives.”
Kaufman will continue his clinical practice part-time at OHSU.
Boston Scientific has announced that it will make a partial offer to acquire a majority stake, up to a maximum of 65%, of shares of Acotec Scientific, a Chinese medical technology company that offers solutions designed for a variety of interventional procedures.
The proposed price is HK$20 per share, which represents a total upfront cash payment consideration of approximately US$523 million for the 65% stake at current exchange rates.
Acotec is a leader in medical solutions, including drug-coated balloons (DCBs), which are used in the treatment of vascular and other diseases. In 2016, the company launched the first peripheral DCB in China after receiving approval from the National Medical Products Administration. The Acotec portfolio also includes radiofrequency ablation technologies and thrombus aspiration catheters, as well as more than 20 other products in various stages of development across a range of specialties. In the 12-month period ending June 30, 2022, Acotec generated sales of RMB 339 million (approximately US$53 million), growing 25% year-over-year in the first six months of 2022 with strong double-digit growth in each of the two years prior.
“Acotec is a profitable, fast-growing company with a strong portfolio and innovative pipeline of medical technologies, and we believe this investment will generate growth opportunities for both companies,” said Art Butcher, executive vice president and group president, MedSurg and Asia Pacific, Boston Scientific. “We expect completion of the partial offer to further strengthen our presence in China and create the potential for commercialisation of Acotec products globally, providing an increased number of physicians and patients access to our robust and complementary product portfolios.”
Boston Scientific expects the impact to adjusted earnings per share to be immaterial in 2023 and the impact to generally accepted accounting principles (GAAP) earnings per share to be less accretive, or dilutive, as the case may be, due to amortisation expense and acquisition-related net charges.
The completion of the transaction, which is anticipated in the first half of 2023, is subject to acceptance and approval by Acotec shareholders and other conditions set forth in related filings.
Europe’s health commissioner, Stella Kyriakides, has announced that proposals to extend the transition period for the implementation of the European Union’s (EU) Medical Device Regulation (MDR) will be put forward in early 2023.
Kyriakides informed health ministers from the EU’s 27 member states of the plan at a meeting of the Employment, Social Policy, Health and Consumer Affairs Council in Brussels on Friday (9 December), where the council members discussed the current status of the implementation of the MDR.
The regulation—which changes the way that medical devices are certified for use in the European market—first came into effect in 2021 with an initial three-year transition period, having been delayed by one year in 2020 due to the onset of the COVID-19 pandemic.
Concerns have been raised over the impact of the transition to the new regulatory regime, with the European Society of Cardiology (ESC) last week calling upon ministers to act to prevent a “shortfall of essential medical devices for cardiovascular patients”, which the Society warned could include diagnostic and ablation catheters and some stents.
At Friday’s meeting, Kyriakides informed ministers that she will propose an extension to the transition period for the implementation of the MDR in early 2023—with the measure then to be voted upon by the European Council and Parliament.
“Patients rightly expect to have safe and high-quality medical devices,” Kyriakides told journalists at a press conference that followed the council meeting, where she acknowledged it is now a “crucial time” for the transition to the new rules.
“We have been following the progress achieved towards this goal very closely in the past months and, while the number of notified bodies have increased and actions have been taken to prepare manufacturers, this is not enough,” Kyriakides added. “In addition, we are now experiencing supply shortages on the global market. We are still feeling the impacts of the pandemic, and now also the Russian war in Ukraine, where several manufacturers of devices are located. This is creating additional complications.
“This is why I announced today to ministers that we will propose to extend the transition period to mitigate any short-term risks. This targeted amendment will take into account the risk class of different devices and address the sell-off date. At the same time, we will work on medium- and long-term solutions to address the more structural issues that have arisen with the new rules.
“Our citizens do not only expect medical devices to be safe, they also expect them to be available. We will do everything in our power to ensure that this transition does not create any disruptions.”
Reto Bale (Innsbruck, Austria) talks to Interventional News at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain) about some of the key benefits of using navigation and robotics during interventional radiology and oncology procedures, such as the ability to “increase reliability and reproducibility” and “improve workflow”.
Bale discusses his initial experience of using an early robotic system for cone beam computed tomography (CBCT)-guided procedures for bone interventions, noting that, with this technology, “you can precisely reach nearly every target in the body from head to toe”.
One of the major strengths of the Micromate robotic system (Interventional Systems) “is that it is very flexible” states Bale, who concludes that “it is a very interesting tool to do all types of CT-guided procedures, including radiofrequency ablation”.
This video is sponsored by Interventional Systems.
Interventional News’ most popular stories last month included news of a US Food and Drug Administration pre-market approval submission of an ultrasound renal denervation system, as well as that of receipt of aforementioned approval for a drug-coated angioplasty balloon for peripheral artery disease; and a report of a British Society of Interventional Radiology presentation on the state of genicular artery embolization practice in the UK.
Otsuka Medical Devices and ReCor Medical have announced the filing of the pre-market approval application to the US Food and Drug Administration for the Paradise ultrasound renal denervation system in the treatment of uncontrolled hypertension.
The first trial participant has been treated as part of GENESIS II, a study of Embozene microspheres for genicular artery embolization as treatment of mild-to-moderate knee osteoarthritis.
The US Food and Drug Administration (FDA) has approved the Chocolate Touch drug-coated balloon (DCB) percutaneous transluminal angioplasty catheter for the treatment of patients with peripheral artery disease in the superficial femoral artery and the popliteal artery.
The Sundance (Surmodics) sirolimus drug-coated balloon (DCB) has an “excellent” safety profile in a “challenging, real-world, predominantly CLTI [chronic limb-threatening ischaemia] population,” and has a primary patency rate of 80% at 12 months in a per-protocol analysis population.
The British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK) featured a presentation on the existing body of evidence for GAE’s safety and efficacy and the roadmap for growing this further in order to gain UK National Institute of Health and Care Excellence (NICE) recommendation.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual meeting (10–14 September, Barcelona, Spain) discussion participants underlined that while vying to make your voice heard at multidisciplinary team meetings is vital, this should not be motivated by ego, rather, by the common goal of what is best for the patient based on clinical effectiveness and patient outcome.
The Society of Interventional Radiology (SIR) published a position statement deeming endovascular thrombus removal “an acceptable treatment option in selected patients with acute iliofemoral deep vein thrombosis [DVT].”
The latest results from CLOUT and a propensity score-matched analysis of CLOUT versus ATTRACT bolster the evidence base for mechanical thrombectomy in the field of deep vein thrombosis (DVT) management.
Delcath Systems announced the publication of a retrospective analysis of patients who underwent a percutaneous hepatic perfusion procedure (PHP) with Chemosat for the treatment of either inoperable intrahepatic cholangiocarcinomas (iCCA) or extrahepatic cholangiocarcinoma (eCCA) with liver metastases.
Sixteen of the 17 patients were evaluable for response as one patient died without follow-up imaging 13 weeks after the first PHP with no identifiable relationship to the PHP treatment. After the first PHP, one patient (6%) presented with a complete response (CR). Three patients (18%) had a partial response (PR) in the first follow-up exam and seven patients (44%) presented with stable disease (SD). Five patients (31%) had progressive disease (PD), one of which was limited to extrahepatic progression only. In total, in 17 treated patients had an overall response rate (ORR) of 25% and a disease control rate (DCR) of 75% was achieved. Two patients with PR, six patients with SD and the patient with PD limited to extrahepatic progression received further PHP treatments. In the subsequent follow-up exams, the overall best therapy response in these patients was PR in 78% and SD in 22%. One patient was treated in total with eighy PHP treatments within 30 months.
The median progression-free survival (PFS) was 3.5 (95% CI:2.2–7.4) months with a similar median hepatic PFS of 3.6 [95% CI: 2.6–9.5] months. Calculated from first diagnosis of iCCA (or CCA liver metastases), the median survival was 27.6 [95% CI: 16.5–37] months. From first PHP, a median survival of 9.9 [95% CI: 3.8–21] months was observed, with a one-year survival rate of 41%. For context, the authors noted that for inoperable CCA, the treatment options are limited and a median survival of 2.5–6 months is to be expected, which can be extended to approximately 12 months under first-line chemotherapy with gemcitabine and cisplatin. In this study all patients were previously treated with at least systemic therapy and the authors note that the results of their analyses confirm the potential for survival extension by PHP treatment even after the exhaustion of systemic therapies.
The authors highlighted the increasing importance of locoregional forms of therapy in the treatment of CCA and that the new edition of the German S3 cancer guideline ‘Diagnostics and Therapy of Hepatocellular Carcinoma and Biliary Carcinomas’ now includes PHP with melphalan for the treatment of inoperable iCCA or eCCA liver metastases. Based on the results of this study, the authors concluded that for patients with inoperable, treatment-refractory iCCA and CCA liver metastases, PHP is an effective and safe treatment option that has the potential to prolong life in a palliative setting.
Data have been presented for the first time at the Paris Vascular Insights (PVI) conference (23–25 November, Paris, France) from the ABISS trial, which compared drug-coated balloon (DCB) with plain-balloon angioplasty for arteriovenous fistula (AVF) stenosis.
ABISS was a physician-designed prospective, randomised, double-blind trial that included 12 centres in France. The study enrolled 150 adult patients who had a native autologous AVF stenosis already punctured for haemodialysis. Following predilatation, patients were randomised 1:1 between DCB (Lutonix, BD) and placebo balloon application. The study was mainly funded by the French government clinical research programme (PHRC).
The primary outcome of the study was cumulated incidence of loss of primary patency of AVF at six months. The study authors, led by Raphaël Coscas (Ambroise Paré Hospital and Paris-Saclay University, Paris, France) found in an intention-to-treat analysis DCB was superior to plain-balloon angioplasty at six months but not in a statistically significant way, with a p value of 0.09. It was however statistically significant at three months (p=0.002). In a prespecified per-protocol analysis, the DCB was superior to a statistically significant degree at the intervals of three (p=0.0004), six (p=0.008) and 12 months (p=0.029) for the main outcome. There was no difference in terms of mortality or rates of adverse events between the groups. Coscas noted that the secondary outcomes, which included dialysis circuit patency, restenosis, and thrombosis, will be presented in future meetings.
The presenter drew attention to the difference between the intention-to-treat analysis results and those of the per-protocol analysis. He said that “the way data of the study were analysed will need to be discussed because, in the intention-to-treat analysis, patients lost to follow-up or who waived consent were imputated to the worst-case scenario (loss of patency if DCB arm and patency if placebo arm),” suggesting a “disadvantage” for the DCB in the intention-to-treat results. “This was less the case in the per-protocol analysis—I think we will discuss that later on”. He added that post-hoc analyses based on similar criteria of other major DCB in AVF trials are ongoing.
Egg Medical, a medical device company commercialising technologies to reduce scatter radiation exposure during interventional angiographic procedures, has announced that it has achieved CE mark for the EggNest XR radiation protection system. The EggNest protects the entire interventional team in hospital X-ray labs (cardiac catheterisation, electrophysiology, interventional radiology, and operating rooms) from the harm of long-term exposure to scatter radiation.
“Occupational exposure of hospital staff to X-rays during medical procedures is an important workplace risk. Almost everyone in the interventional cardiology and radiology profession knows someone with a radiation-related illness. There have been minimal improvements in X-ray shielding over the past 30 years, leaving the medical teams working in these environments exposed to scatter radiation every day,” said Robert Wilson, Egg Medical CEO. “The EggNest platform addresses the problem of hospital personnel radiation exposure for everyone working in these environments by reducing scatter radiation by an average of 91 per cent.”
With the CE mark certification, Egg Medical will continue expansion into all markets recognising the CE mark.
“At Egg Medical, our belief is that everyone deserves protection, meaning the entire interventional team,” said Wilson. “With CE mark approval of the EggNest platform, we are bringing this protection to more interventional teams worldwide.”
Royal College of Radiology (RCR) president Kath Halliday (Nottingham University Hospitals, Nottingham, UK) gave a presentation to the British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK) exploring how new technologies and infrastructural reforms can improve outcomes for patients under interventional radiology (IR) department care. Drawing attention to the problems with IR practice in the National Health Service (NHS), particularly with regard to capacity, she suggested harnessing artificial intelligence (AI), collecting data and recourse to dedicated day case units and hybrid theatres could reduce waiting times and drive more effective interventions.
She drew attention to the fact that “there are no data” widely available on IR procedures. The Getting It Right First Time (GIRFT) programme reviews services and procedure outcomes across the NHS but, Halliday said, provides little in the way of information on the outcomes of IR procedures. “We need to be able to identify IR procedures from our radiology codes,” she argued, stating that these in turn need to link to the codes used in Hospital Episode Statistics (HES), a database of NHS admissions records covering comorbidities, length of stay and outcomes.
According to Halliday, a similar problem exists in informing patients of their options around IR procedures, as those who present the information are often not radiologists themselves. Often, this is due to a lack of a dedicated area within radiology departments in which to see patients. Integrating IR procedures into a more comprehensive data management system means interventional radiologists and their patients can make more informed decisions about procedures. This will also require improvements to NHS IT infrastructure, Halliday suggests.
Capacity was another focus of Halliday’s talk. She described how “lack of capacity too often results in poor outcomes for patients,” adding that “for instance, some people wait so long for angioplasty that they end up with amputation,” then referring to the situation in some hospitals where capacity is so limited that radiologists are forced to come in to perform procedures when they are not on call. Improving capacity is difficult because those radiologists required to teach trainees are already overworked, she argued. It would also require creating a more hospitable workplace in terms of morale and working hours to encourage radiologists to stay in the field. For a technology-driven solution Halliday pointed to procedure simulators, which are still underused in training new radiologists. AI would also be useful for diagnostics in IR—though she said she did not believe robots would be performing procedures any time soon.
Halliday concluded the question and answer that followed her presentation by advocating for expanded IR training.
A minimally invasive treatment for carpal tunnel syndrome provides complete and long-term relief to patients without the use of corticosteroids, according to research presented at the annual meeting of the Radiological Society of North America (RSNA; 27 November–1 December, Chicago, USA).
Carpal tunnel syndrome is a form of nerve entrapment neuropathy, involving the pressing or squeezing of a peripheral nerve. It occurs when the median nerves and tendons inside the carpal tunnel, a narrow and rigid passageway that runs from the forearm to the palm of the hand, are being pressed or squeezed at the wrist. This results in tingling, numbness and/or weakness of the fingers and hands. Carpal tunnel syndrome is the most common and widely known form of entrapment neuropathy, affecting about 3% of the USA’s population.
Surgery is often required to treat carpal tunnel syndrome when non-surgical methods, such as physical therapy or corticosteroid injections, are insufficient. The most common and widely used surgical method involves cutting the carpal ligament to reduce pressure on the median nerve. This method requires making an incision into the wrist.
The study’s findings show that a technique called hydrodissection effectively treats nerve entrapments without the need for surgery or corticosteroids. It involves the injection of a liquid, usually saline, into a nerve to separate it from the surrounding tissue. Ultrasound guidance is used to accurately identify nerves.
Lead author Anindita Bose (University College of Medical Sciences, Delhi, India) comments “previously, the studies that have been done on ultrasound-guided hydrodissection for carpal tunnel syndrome have used corticosteroids either alone or as a part of the injection, making it difficult to assess whether hydrodissection alone was beneficial, or if it was due to the effect of the steroids.”
For this randomised controlled trial, Bose and colleagues enrolled a total of 63 patients suffering from carpal tunnel syndrome. Researchers used the Boston Carpal Tunnel Questionnaire (BCTQ), the Visual Analog of Pain (VAS), and cross-sectional area ultrasounds of the median nerve to assess patient pain and symptoms before and after the procedure. The 63 patients were divided into three groups. Group one received ultrasound-guided hydrodissection with just a saline injection. Group two received ultrasound-guided hydrodissection with an injection mixture of saline and corticosteroid. Group three received just an ultrasound-guided corticosteroid injection with no hydrodissection.
Follow-up was done at four weeks, 12 weeks and six months. At the four-week mark, all three groups of patients showed a reduction in pain. By the 12-week and six-month mark, both groups that received ultrasound-guided hydrodissection showed further improvement while the group that received just a corticosteroid injection reported a recurrence of symptoms and an increase in BCTQ and VAS scores.
Additionally, ultrasounds showed a significant reduction of median nerve cross-sectional area in both hydrodissection groups. Group one showed a reduction of 43%, and group two showed 46%. Group three showed only an 11% reduction.
The procedure is short, requiring only 10 to 15 minutes, which can reduce costs for treatment facilities. Anupama Tandon (University College of Medical Sciences, Delhi, India) a co-author of the study notes, “it came as a pleasant surprise when this simple procedure of ultrasound-guided hydrodissection provided patients with long-term relief.” She continues, “the patients were highly satisfied, as the cost was low, no anaesthesia or hospitalisation was needed, and they could go back in an hour’s time and resume their routine work.”
Neurologica, a subsidiary of Samsung Electronics, has announced that its head-to-toe trauma imaging solution—the BodyTom 64 point-of-care mobile computed tomography (CT) scanner—has received 510(k) clearance from the US Food and Drug Administration (FDA) for commercial use in the USA.
Based on customer feedback, the company designed the BodyTom 64 to enhance the user experience and improve clinical workflows through revisions to both the software and the data acquisition system (DAS), a press release states. Such revisions include incorporating Linux as the operating system and having the ability to generate up to 64 cross-sectional CT images of a patient’s body, versus the 32 images produced by the predicate BodyTom Elite system.
A Neurologica press release also details that, with indications for both paediatric and adult imaging, the BodyTom 64 is a multi-departmental imaging solution that can be utilised for various needs, including:
Neurosurgery/surgery—when combined with any radiolucent skull fixation device, it can transform an operating room into an intraoperative neuroimaging suite to enhance neuro-navigation and surgical outcomes, including clinical utility for extracranial procedures
Trauma/emergency room (ER)—its unique combination of internal lead shielding and battery operation allows any standard trauma bay to be transformed into an advanced CT imaging suite
Interventional radiology (IR)—it can also help optimise workflows by remaining ready to rescan for each stage of needle guidance, and bring the power of multi-slice CT to the interventional suite
“We are thrilled to build off our expertise and elevate point-of-care imaging with our BodyTom 64, which can transform any room in a hospital into an advanced imaging suite,” said Jason Koshnitsky, senior director of Global Sales and Marketing at Neurologica. “This full-body 64-slice CT scanner is an upgraded version of the BodyTom Elite CT scanner, providing enhanced functionality with the same high-resolution imaging capabilities.”
“In contrast, for patients with RCCs smaller than 3cm, either cold-based or heat-based therapy is just as effective in reducing cancer-specific mortality,” comments lead author Gabriele Sorce (San Raffaele Scientific Institute, Milan, Italy). “The findings may help us to better tailor the choice of ablation technique for patients with small RCCs.”
Lower risk of cancer death with cryoablation versus heating
Renal cell carcinoma is the most common type of kidney cancer. For patients with early-stage RCCs smaller than 4cm, an increasingly popular treatment option is destroying the cancer by freezing it or heating it. For these clinical stage T1a RCCs, ablation can provide high survival rates without the need for more extensive kidney surgery.
However, the outcomes of ablation appear “less favourable” for a subset of patients with clinical stage T1a RCCs: those whose tumours are between 3 and 4cm in size. Current European guidelines recommend cryoablation over thermal ablation for these cancers measuring 3 to 4cm, while US guidelines state that either treatment can be used. Both sets of guidelines state that either freezing or heating can be used for T1a RCCs measuring 3cm or smaller.
To clarify the issue, an international research group analysed patients with stage T1a RCCs treated with freezing or heating between 2004 and 2018. Patients were drawn from the US National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program. The study focused on two matched groups of patients with cancers measuring between 3 and 4cm: 757 treated with cryoablation and 388 treated with thermal ablation.
Median age at treatment was 71 years. Follow-up data on cancer-specific mortality were available for 422 patients treated with freezing and 238 treated with heating.
Eight years after treatment, estimated cancer-specific mortality among patients with RCCs measuring 3 to 4cm was 8.5% for patients treated with cryoablation versus 12.9% for those undergoing heat-based thermal ablation. With both treatments, about 40% of patients died from causes other than cancer.
Implications for treatment decisions in ‘small, potentially curable’ kidney cancers
After adjustment for non-cancer-related death and other characteristics, patients undergoing thermal ablation for RCCs between 3 and 4cm were twice as likely to die of kidney cancer. In contrast, for patients with cancers smaller than 3cm, estimated cancer-specific mortality was similar between groups: 6.8% after cryoablation and 6.1% after thermal ablation.
The study is one of the first to directly compare clinical outcomes for freezing versus heating in patients with stage T1a RCCs measuring between 3 and 4cm. The results suggest that thermal ablation has “a highly statistically significant and clinically meaningful” disadvantage in terms of the long-term risk of death from kidney cancer, compared to cryoablation.
“Conversely, in patients with tumours 3cm or smaller, either ablation technique is equally valid,” says Sorce. “We believe our findings have important implications for clinical decision-making and informed consent for patients with these small, potentially curable kidney cancers.”
The Swiss Federal Assembly has voted in favour of accepting medical devices with US Food and Drug Administration (FDA) marketing authorisation in Switzerland.
A motion for ‘more freedom of action in the procurement of medical products for supply of the Swiss population’ was discussed and put to a vote in the country’s parliament on Monday 28 November, with many industry groups, including Swiss Medtech, supporting the acceptance of FDA-approved devices.
In a press release, Swiss Medtech described this as a “necessary and urgently needed decision”, and stated that it is “essential” for this order to now be implemented swiftly and pragmatically. It further draws on Australia and Israel as examples of countries in which “efficient procedures” to recognise FDA approvals in parallel with the CE mark have “proven successful”, and “can be achieved in an uncomplicated manner”.
“Swiss Medtech very much welcomes the policymakers’ important and forward-thinking decision,” added Peter Biedermann, managing director of Swiss Medtech. “It is a response to circumstances that could no longer be ignored. Specifically, problems with the implementation of the new European Medical Device Regulation [MDR], and the negative consequences concerning availability, product range and quality of medical devices throughout Europe. As innovations are increasingly being introduced first to the market in the USA, new products reach Europe with a delay, at best.”
The Swiss Federal Council—the executive body of the country’s federal government—opposed this proposition, citing the administrative burden that would be brought about by this regulatory shift, and patient safety concerns caused by risk classification discrepancies between the USA and Europe.
On 30 May 2022, the potential acceptance of US FDA products was voted on by the 46 members of the Swiss Council of States (the upper house of the country’s Federal Assembly), with 23 voting to accept and 12 voting to reject.
Shortly following this decision, the Federal Council asserted in a press release that there was no need to accept non-CE-marked medical devices, such as US FDA-approved devices, at that time—describing the extension of simplified market access to other countries outside of the EU as “disproportionate”—before noting that it would re-evaluate this situation at the end of 2024. It added that the supply of safe medical devices in Switzerland was “currently guaranteed”, referencing various backup measures it took back in 2021 to ensure this “even without an updated MRA [Mutual Recognition Agreement]”.
The parliamentary vote that took place earlier this week was borne out of the introduction of the European MDR on 26 May 2021, with the MRA and all related trade-facilitating effects for medical devices between the EU and Switzerland also ceasing to apply from the same date.
And, while devices ‘in conformity’ with the MDR can be certified and placed on the market until 25 May 2024, marketed devices must be certified directly under the MDR from the following day (26 May) onwards. With this deadline drawing ever closer, concerns have been raised regarding regulatory challenges, supply chain gaps and device shortages, and the impact this could have on patient care and industry alike.
As a statement from Swiss Medtech notes, “more than 1,000 of the approximately 5,000 foreign manufacturers have already stopped supplying Switzerland with their products—they are not prepared to meet the additional requirements for the limited Swiss market, and patients in Switzerland are the ones to suffer”.
The motion to accept US FDA approval of devices in Switzerland was brought up to the 200-seat Swiss National Council (the lower house of the country’s Federal Assembly) on Monday, with 100 votes in favour and 79 against being cast. As such, both chambers of Switzerland’s national parliament have now voted to adopt the initiative, and will instruct the Swiss Federal Council to adapt legislation to allow devices with US FDA clearance onto the market.
Details of this new system and the logistics of implementing it, as well as when it will come into effect, are yet to be confirmed.
Otsuka Medical Devices and ReCor Medical, a subsidiary of Otsuka, announce the filing of the pre-market approval (PMA) application to the US Food and Drug Administration (FDA) for the Paradise ultrasound renal denervation (uRDN) system in the treatment of uncontrolled hypertension.
The Paradise uRDN system is designed to reduce sympathetic nerve activity by denervating nerves which surround the renal arteries with the goal of reducing blood pressure, and uses a combination of ultrasound energy to denervate the renal nerves and a water-filled balloon to protect the renal artery. The system employs an interventional procedure in which a catheter is placed in each of the main renal arteries, following which two to three seven-second ultrasound emissions are delivered to denervate the surrounding renal nerves, thereby reducing blood pressure.
Since 2009, ReCor has been focused on developing and testing the Paradise uRDN system to treat hypertension safely and effectively. ReCor has three global, independently powered, sham-controlled randomised clinical trials of the Paradise uRDN system in more than 500 patients with uncontrolled hypertension: RADIANCE-HTN SOLO, RADIANCE-HTN TRIO and RADIANCE II. Each RADIANCE trial met its prespecified primary efficacy endpoint of blood pressure reduction, with positive safety.
RADIANCE II is the USA FDA’s investigational device exemption (IDE) pivotal trial. In September 2022, ReCor and Otsuka Medical Devices announced that the trial successfully reached its primary efficacy endpoint. Results showed a reduction in daytime systolic ambulatory blood pressure of -7.9 mmHg in those treated with uRDN and a difference between uRDN and sham of -6.3 mmHg (p <0.0001). The results from the all three RADIANCE clinical trials have been included in the submission for approval to the FDA.
The uRDN system bears the CE mark for the treatment of hypertension in Europe and is an investigational device in the USA and Japan.
L to R: Clare Bent, Peter Littler, Robert Morgan, Raman Uberoi (at BSIR 2022)
L to R: Clare Bent, Peter Littler, Robert Morgan, Raman Uberoi (at BSIR 2022)
In the opening session of the British Society of Interventional Radiology (BSIR) annual scientific meeting 2022 (2–4 November, Glasgow, UK) titled ‘What’s up, Doc?’, four faculty members spelt out for attendees what they consider to have been the most noteworthy advancements in the specialty of late, as well as their forecasts for interventional radiology’s (IR) direction of travel. Advances from the vascular, interventional oncology (IO), non-vascular, and non-clinical spheres featured in the session, with the latter consisting of a call to encourage trainees into IR to meet the current workforce shortfall.
In Robert Morgan’s (St George’s Hospital, London, UK) vascular-focused presentation, he first drew attention to a paperthat had reported favourable results of the use of paclitaxel-coated balloons below the knee for patients with peripheral arterial disease (PAD) including no risk of death. He reminded the audience that a previous meta-analysis of studies involving paclitaxel-coated devices had suggested an increased risk of all-cause death, which had been ascribed to paclitaxel-coated device use. During his presentation, he stated that no study published since 2018, looking at single-cause mortality and involving the use of paclitaxel-coated devices above or below the knee, had found an increased risk of death associated with paclitaxel-coated devices.
Morgan also described the IMPERIAL randomised study comparing the Eluvia (Boston Scientific) and the Zilver PTX (Cook Medical) drug-eluting stents (DES), which had concluded that there was no significant difference in patency at two years between the two DESs. However, there was a slight benefit in target lumen revascularisation rate for the Eluvia DES, which just reached significance.
Morgan discussed the positive results of the randomised controlled trial DISRUPT PAD III, which compared Shockwave Medical’s peripheral lithoplasty system plus drug-coated balloon (DCB) for treating moderate and severely calcified femoropopliteal arteries with standard balloon angioplasty. He described the findings as “providing proof of concept for intravascular lithotripsy” as a treatment for heavily calcified femoropopliteal occlusive lesions.
Robert Morgan presenting at BSIR 2022
Another study that Morgan referenced was an analysis of Medicare data from 2011 to 2019 published in the Journal of Vascular and Interventional Radiology (JVIR) in November 2022. This study examined clinicians’ use of medical devices including drug-eluting balloons (DEBs), DESs and atherectomy in treating PAD patients in the USA. Morgan described an attached commentary as being relatively “scathing” of existing practice with excessive non-evidence based used of atherectomy compared with DEB/DES. Morgan concluded by stating that the evidence supports much more widespread use of DCBs and DESs compared with atherectomy devices, although the two techniques may be complementary in selected patients.
Peter Littler’s (Freeman Hospital, Newcastle upon Tyne, UK) focus was on IO, detailing advances in the techniques used in selective internal radiation therapy (SIRT), noting that for the first time, this type of cancer treatment has been included in international guidelines. Advanced catheters like the SWIFTNinja steerable catheter (Merit Medical) and personalised dosimetry, where individual cancer patients can be given amounts of radiation catered to the nature of the tumour, are among the developments in SIRT. Littler cited a study in The Lancet that evidences considerable improvements in survival rates after such tailored treatment.
Advances have also been made, Littler said, in ablation. Littler, who carries out ablation procedures on the liver, noted the benefits of stereotactic needle guidance technology. He then shared details of the novel ablation technology histotripsy, a non-invasive, ultrasound-based technique that works “like 3D sculpting” that is currently only being used in the HOPE4LIVER trial. Littler offered the suggestion that many of the technologies he detailed would be more widely available in the immediate future.
Clare Bent (University Hospitals Dorset, Bournemouth, UK) then gave her take on the “exciting new interventions and applications” in the benign non-vascular world of IR—an area that is “expanding at a fast pace”.
Clare Bent presenting at BSIR 2022
Musculoskeletal (MSK) embolization has grown as a discipline, Bent informed the BSIR audience, with genicular artery embolization (GAE) having the largest evidence base. Experimental studies have demonstrated a link between angiogenesis and pain, shown as hyperaemia on angiographic imaging, Bent detailed, enabling targeted therapeutic embolization. Bent also described several other applications including embolization of plantar fasciitis, with reductions in both plantar fascial thickness and pain following treatment. The next step for MSK embolization, she advised, is for the IR community to secure investment into further scientific research, the results of which may then help move these techniques from “marginal” to “mainstream”.
Bent also gave an overview on the use of glue, over coil, embolization to reduce cost, radiation dose and increase durability of the embolic endpoint, using pelvic vein and prostate artery embolization as examples of where this alternative technique may be advantageous. Moreover, and despite its “slow uptake in the UK”, radiofrequency ablation for benign symptomatic thyroid lesions has been endorsed by many societies worldwide. News of National Institute of Health and Care Excellence (NICE) guidance stating that microwave ablation can be used provided standard arrangements are in place for clinical governance, consent, and audit has been released since Bent gave her presentation.
“Expanding on existing techniques can change lives,” Bent concluded, adding cryotherapy for Morton’s or amputation stump neuromas to her list of novel IR applications.
Raman Uberoi (Oxford University Hospitals, Oxford, UK) rounded off the first session of the meeting by addressing the non-clinical side of IR, choosing to home in on recruitment of interventional radiologists in line with achieving a fit-for-purpose national service specifically as worthy of focus. He began by outlining the “huge range and complexity – has grown and grown, is exploding” of IR procedures, and how this has seen interventional radiologists branch into different subspecialties. However, the small numbers in these subspecialties make providing a 24/7 IR service challenging, the audience heard. Therefore, Uberoi incited delegates to “think carefully” about how the “next generation” of interventional radiologists can and should work.
Raman Uberoi presenting at BSIR 2022
The speaker made some suggestions as to how the specialty can “make things better for future interventional radiologists”. Among these was the adoption of specific IR training and formal assessment, as the subspecialty increasingly diverges from diagnostic radiology, Uberoi explained. The European Board of Interventional Radiology (EBIR) examination is an example of an accreditation model that has been proven to work worldwide, with a dedicated curriculum to match the exam content.
Future improvements to training, the presenter went on to note, could include in non-operative, more “human factors that are pertinent to our practice”, as well as coverage of day-to-day catheter skills.
Although the IR workforce has, on average, grown by 4% year on year over the last five years, Uberoi underlined the “unacceptable risk for patients” that the insufficient number of interventional radiologists in the UK is causing—50% of UK trusts were “unable to provide adequate 24/7 IR services in 2021,” Uberoi stated.
Therefore, the presenter left the audience on a to-do list for future-proofing IR services, involving increasing advertising to attract more IR trainees, protecting time for specific IR training, and ensuring trainees are exposed to ‘on-call’ earlier—“you should not be doing your first independently once you have become a consultant”.
“There are opportunities to collaborate across the spectrum,” Uberoi concluded, highlighting stroke as an area that lends itself to cross-disciplinary working. However, he emphasised how “we [in BSIR] have to drive the changes” and “work with the [Royal College of Radiologists]” so that improved patient quality of care is the outcome.
This article was amended on 30th November to correct an error.
Findings from a recent prospective study show promising safety and patient outcomes data for locally advanced and borderline resectable pancreatic cancer treatment using ablative stereotactic magnetic resonance imaging (MRI)-guided on-table adaptive radiation therapy, also known as SMART. Approximately 25% of the study’s participants were patients treated at the Henry Ford Pancreatic Cancer Center (HFPCC; Detroit, USA).
“As a pioneering institution in the field of MRI-guided adaptive radiation therapy, Henry Ford Health is thrilled to have led this novel study, which was the largest international study of ablative radiation for pancreatic cancer in the world,” said Ben Movsas, Medical Director of Henry Ford Health Cancer and Chair of Radiation Oncology. “Henry Ford was first in the world to treat a patient using the MRIdian MRI-Guided Radiation Therapy system back in 2017. Since then, we have treated many cancer patients with MRI-guided radiation therapy.”
The primary endpoint outcomes from the study were presented at the 64th annual meeting of the American Society for Radiation Oncology (ASTRO; 23–26 October, San Antonio, USA) by Parag Parikh, the principal investigator of the study and Director of Gastrointestinal Radiation Oncology and MR-Guided Radiation Therapy at Henry Ford Cancer.
“In this study, 136 patients were treated with ablative MRIdian SMART at 13 international centres,” said Parikh. “The study’s primary outcome measured grade 3 or higher gastrointestinal toxicity, such as nausea, vomiting or abdominal pain, in the first 90 days after treatment. The study’s primary safety objective was met, with zero incidence of acute grade 3 or higher gastrointestinal toxicity definitively related to SMART treatment.”
Secondary measures of the study include overall survival, local control, distant progression-free survival, and changes in patient-reported quality of life, Parikh explained. While study patients are still early in the follow-up period, preliminary clinical outcomes data of one-year local control and distant progression-free survival were 82.9% and 50.6% respectively. One-year overall survival from diagnosis was 93.9%.
NOTE: This video is ONLY available to watch in selected countries and geographies
Lambros Tselikas (Villejuif, France) speaks to Interventional News about a recent retrospective study evaluating Liver ASSIST Virtual Parenchyma—the results of which he presented at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain).
The software simulated the perfused parenchyma from a virtual selective injection point on the proximal cone-beam computed tomography (CBCT). It was compared to the corresponding selective CBCT considered as the ground truth.
“You can have very easily the vascular extraction, tumour-feeding vessels, and more interestingly, you can now test multiple injection points and simulate the associated liver parenchyma,” says Lambros Tselikas.
“If it were easy, this session would not be here.” These are the words of Jens Ricke (University Hospital Munich, Munich, Germany), who drew attention to the self-evident nature of the difficulties involved in multidisciplinary collaboration during an expert roundtable discussion at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual meeting (10–14 September, Barcelona, Spain). Titled ‘If you are not at the table, you will be on the menu’, the discussion participants, who presented perspectives on multidisciplinary work from their various societies, kept returning in the subsequent question and answer section of the session to one key message. They underlined that while vying to make your voice heard at multidisciplinary team meetings is vital, this should not be motivated by ego, rather, by the common goal of what is best for the patient based on clinical effectiveness and patient outcome.
Eric Verhoeven
Raman Uberoi (John Radcliffe Hospital, Oxford, UK) began the discussion with a question for vascular surgeon Eric Verhoeven (General Hospital Nuernberg, Paracelsus Medical University Nuernberg, Nuernberg, Germany) and Stefan Müller-Hülsbeck (Academic Hospitals Flensburg, Flensburg, Germany) on the “stresses and strains” that arise from multidisciplinary collaboration. “You have both made the point that we ‘forget patients’—how much do you think that is driven by egos?” Verhoeven was first to acknowledge that a little bit of ego may not be a bad thing, pointing out that “without that [type of] personality”, it can be difficult to convey your specialist perspective effectively and persuasively. He recounted how he was able to influence the clinical setup at his hospital, so as to have “the whole personnel working together in the same location”—this includes radiologists, vascular surgeons, and nurses and technicians specially trained in radiology and endovascular techniques. Emphasising the “big benefit” this approach affords their patient-centric service, Verhoeven went on to share how they have a daily “vascular patient meeting”—even the name puts the focus on the patient, as opposed to the interdisciplinary makeup of the clinical team behind the care.
Raman Uberoi
Müller-Hülsbeck picked up the discussion to label this multidisciplinary way of working as “an ideal playground”, which should be harnessed to “put the patient first”. Collaboration can yield highly successful outcomes, which, at Müller-Hülsbeck’s centre, takes the following form: “if we need, for certain reasons, surgical cutdown, we call the vascular surgeon, and vice versa, if they need help from the interventional radiologist”. This collaborative way of operating is how they go about treating thoracic and abdominal aneurysms in Nuernberg and Flensburg, delegates heard, with a strong emphasis on “speaking a clear language” to facilitate cross-specialty communication for the benefit of the patient.
Part of this clarity when communicating, Müller-Hülsbeck detailed, is establishing “clear rules that are defined in advance”. This is so that the answer to the question of “who does what with the patient?” is not dictated by egos, or other factors that may render patient outcome a secondary consideration. In contrast, Verhoeven relayed how, at his hospital, “it is completely irrelevant who is doing what”, elaborating on this to say that “we decide together as a team who is the best suited” for taking on each individual case. This statement then gave way to Ricke making the point that different people’s definitions of collaboration will be different, and that what multidisciplinary involvement looks like in a particular hospital needs to be defined— ‘involved’ does not necessarily mean doing the procedure, as he added that it could mean only taking part in decision-making beforehand.
Stefan Müller-Hülsbeck
In addition to keeping the patient at the forefront of a procedure and “[putting] ego aside”, as Valérie Vilgrain (Assistance Publique-Hôpitaux de Paris, Paris, France) drove home in her presentation, Ricke summed up another takeaway from the session as a whole: “What I have learned today is that we need communication training in medical school.” He went on to contextualise this by making clear that “Nuernberg is not the rule” and that collaboration may not occur in a multidisciplinary manner as effectively in other hospitals. His hope, therefore, is that by starting early, the next generation of clinicians can learn while still at medical school to communicate in a way that is conducive to collaborative, yet patient-centred work.
Jens Ricke
Antonin Krajina (Charles University Hospital, Hradec Kralove, Czechia) then called upon the societies, such as those represented round the discussion table, to “take responsibility for interdisciplinary education.” Examples of this already occurring were heralded throughout the session, including the European Society for Minimally Invasive Neurological Therapy’s (ESMINT) theoretical stroke course (EXMINT).
Valérie Vilgrain
Stroke treatment and by whom it is delivered formed a further part of discussion during the session, with the panel shining a light on the differences in stroke thrombectomy services between the UK and The Netherlands in particular. Beyond the theory, as courses such as EXMINT teach, there is a question of how much training an interventionalist should be required to do before they can independently carry out thrombectomies for stroke patients. Wim van Zwam (Maastricht University Medical Center, Maastricht, The Netherlands) explained how “in The Netherlands, we have a requirement that if you want to do thrombectomies, you have to do at least 25 under the guidance of an experienced interventionalist, and your centre has to do at least 50 thrombectomies per year. These are very simple and straightforward guidelines.” However, Van Zwam acknowledged that, while there are more centres that can and want to do stroke thrombectomy than the country needs in The Netherlands, such is not the case in the UK. Uberoi labelled the latter as a “chicken and egg situation”, whereby “until you start doing the procedure, how can you have enough cases to train in it.”
Wim van Zwam
Van Zwam followed up to ask whether a solution could be to allow adequately trained cardiologists to perform stroke thrombectomy, to which Uberoi responded: “I do not really think the patients care who does their procedure], as long as it gets done and it is a safe service. Ultimately, you want the best trained person, but there has got to be a reality check in terms of what is achievable. Do you want zero service, or could a ‘silver’ or ‘bronze’ service be good enough to improve outcomes without compromising safety? That is the kind of balance I feel we need to look at in the UK.”
The session closed with all participants agreeing that “the clinical aspects of patient care are the same whether you are a vascular surgeon, interventional cardiologist or interventional radiologist.” This can, therefore, be a unifying motivation in multidisciplinary collaboration scenarios, and, as Vilgrain summarised, “we are better doctors when we work together”. This necessitates leaving egos at the door and working communication skills into education for medical students and trainees.
Hospices Civils de Lyon (HCL; Lyon, France) has acquired Epione, the robotic platform developed by Quantum Surgical (QS) that is designed to enable minimally invasive ablations of tumours in the abdomen. This was announced by QS in a press release.
This partnership between HCL and QS will allow more patients to benefit from Epione, a platform allowing clinicians to plan, target, deliver and confirm ablation treatment in a more secure and precise manner. Epione is currently used to target liver and kidney tumours but will be expanded to the treatment of lungs and bones as radiologists at HCL expand their robotic interventional oncology practice.
HCL is the second hospital in the world to offer this platform. The first Epione robot was acquired by Institut Gustave Roussy (Villejuif, France) in January 2022 and the team is approaching their 100th robotic procedure.
“This new acquisition of Epione is a major step for QS and a full validation of the key benefits that Epione offers. It is a great honour to have our robotic system acquired by one of the top medical institutions in France. The most exciting part of this story is that patients will now have a powerful new technology that can offer curative treatments by robotically navigating to destroy tumours while sparing surrounding healthy tissue,” explains Bertin Nahum, QS chief executive officer.
“Epione is a unique percutaneous robotic solution […] Currently, only few expert radiologists perform these treatments. Robotics will allow us to standardise these treatments and more radiologists will thus be able to perform these cases, especially the more complex ones, on tumours that would not be treated. This will allow us to help and cure more patients,” underlines Laurent Milot, deputy head of medical and interventional imaging department at HCL.
Varian, a Siemens Healthineers company, announced today that the first trial participant has been treated as part of GENESIS II, a study of Embozene microspheres for genicular artery embolization (GAE) as treatment of mild-to-moderate knee osteoarthritis. GENESIS II is the largest randomised clinical trial of GAE to assess pain relief from this condition.
GENESIS II is being conducted at the University Department of Radiology, Royal Berkshire NHS Foundation Trust, in Reading, UK. The trial targets mild-to-moderate osteoarthritis (OA) of the knee joint, a common condition and a leading cause of chronic disability. GAE involves a small catheter being advanced into the genicular arteries and Embozene microspheres are delivered through the catheter to reduce the blood supply to the areas of greatest inflammation in the knee, with the goal of reducing pain.
In the GENESIS II clinical trial, patients with knee OA will either receive treatment with the Embozene microspheres or a sham control; they have the option to receive Embozene treatment later in the clinical trial. This clinical trial design allows more accurate assessment of pain relief from the new treatment.
In October 2021, the US Food and Drug Administration (FDA) granted breakthrough device designation for Embozene microspheres for GAE for OA. Currently, Embozene is used to treat hypervascular tumours, arteriovenous malformations, uterine fibroids, and benign prostatic hyperplasia. Embolics are not yet authorised for marketing anywhere for GAE.
Mark Little, consultant diagnostic and interventional radiologist at the University Department of Radiology at the Royal Berkshire NHS Foundation Trust, is the principal investigator of the GENESIS II study. “In GENESIS, our previous 38-patient prospective study, GAE in patients with mild-to-moderate knee OA was found to be safe and effective at early follow-up,” Little noted. “We are excited to build upon this foundation with GENESIS II, which has the potential to improve our understanding of the clinical applications for the procedure. Including a sham-treated group provides the opportunity to validate the findings of GENESIS as well as to gain insight into longer-term follow-up and patient quality of life.”
“Varian is committed to supporting research that has the potential to improve outcomes and enhance the quality of life for patients around the world, and we view the GENESIS II study as an important opportunity to do this,” said David Hahn, chief medical officer, Interventional Solutions, at Varian. “Interventional radiology is defined by minimally invasive techniques, and we believe the treatment of chronic pain is a natural fit for this specialty, particularly given the World Health Organisation’s guidance on this subject. We look forward to better understanding the possible role of GAE in addressing a pressing challenge for care providers and patients.”
The Sundance (Surmodics) sirolimus drug-coated balloon (DCB) has an “excellent” safety profile in a “challenging, real-world, predominantly CLTI [chronic limb-threatening ischaemia] population,” and has a primary patency rate of 80% at 12 months in a per-protocol analysis population. Ramon Varcoe (Prince of Wales Hospital, Sydney, Australia) presented these findings from the SWING first-in-human study at the VEITHsymposium 2022 (15–19 November, New York, USA).
Varcoe, who is co-lead investigator of the trial, added that the research team observed no major amputations, “very low” rates of major adverse events, and “impressive” luminal gain, which was sustained out to six-month angiogram. In addition, Varcoe reported that Rutherford category and the functional outcome measures were improved.
“The Sundance sirolimus-coated balloon is a novel device,” Varcoe informed VEITH attendees. He elaborated: “It has a microcrystalline surface, but also a very sophisticated proprietary excipient, which, rather than using nanoparticles or microreservoirs uses chemistry to deliver the drug into the blood vessel wall and have it retain that much more so than the other devices on the market.”
The presenter noted that SWING is a prospective, multicentre, single-arm feasibility study that looked at patients with stenotic or occluded lesions. The researchers enrolled 35 patients over eight sites in Australia, New Zealand, and also in Europe.
Noting some key inclusion criteria, Varcoe detailed that patients had to be either Rutherford 4 or 5. He added the caveat that Rutherford 3 patients were included, but numbers were capped at 20% of the total cohort. Furthermore, patients had to have de novo or restenotic lesions and at least 50% stenosis by visual estimate of the investigator. They could have up to two distinct lesions in the same or different below-the-knee (BTK) artery, and had to have successfully treated inflow, as well as an unimpaired outflow artery in continuity to the ankle or foot.
The investigators performed both an intention-to-treat and a per-protocol analysis, Varcoe informed the audience. “The reason for that was because [the trial] was conducted over the COVID-19 pandemic period, so we lost seven patients to the primary endpoint of angiography,” he noted, adding that there were also three post-protocol deviations. For these reasons, the research team focused on the 25 patients who had the per-protocol analysis.
The presenter stressed that the patients included represent a “real-world” population, including a high proportion of patients who are smokers and have diabetes, as well as a majority of patients with Rutherford 4 or 5 disease. “They also had high proportions of moderate-to-severe calcification in excess of 18%, and around a third of these patients had total occlusions,” he added.
The study had two primary endpoints. The first was a safety primary safety endpoint—freedom from major adverse limb event (MALE) and perioperative death at 30 days following the index procedure. The primary efficacy endpoint was the rate of late lumen loss at six months, as assessed by quantitative vascular angiography. Both primary endpoints of the SWING trial were achieved, Varcoe revealed.
Varcoe reported that, in the per-protocol population, there were no major amputations, no major reinterventions, and complete freedom from perioperative death, “so it was a safe device”.
The team also saw a rate of all-cause death that was 0%, target lesion amputations were 0%, and a “very low” rate of clinically driven target lesion revascularisation at 8%.
Varcoe added that the minimal luminal diameter at the end of the procedure was “very high”, which he thinks “represents modern-day angioplasty techniques”, and reported a late lumen loss of 1mm at six months—results that compare “very favourably” to other equivalent DCB trials below the knee, he remarked.
As six months, the researchers observed a primary patency of 88.5%. Varcoe noted that primary patency was retained and consistently retained out to 12 months at 80%—a figure that he said is “very good for this part of the vasculature”.
Varcoe added that, “pleasingly,” the team also saw improvement in Rutherford Becker classification, which was sustained and improved out to 12 months. Regarding quality of life, he noted that patient-reported outcome measures were again consistently improved out to that 12-month endpoint.
In closing, Varcoe shared his belief that the Sundance device has “great promise” and “warrants evaluation in a large-scale pivotal trial” based on these latest findings.
Amanda Smolock (Medical College of Wisconsin, Milwaukee, USA) discusses how her practice operates, using microwave ablation nearly exclusively for primary and metastatic liver tumours targetable under ultrasound (US) and/or computed tomography (CT) guidance.
Patients are typically discussed at a multidisciplinary liver tumour conference and referred to the interventional radiology (IR) clinic for evaluation. At consultation, a full history and physical exam is completed along with updated laboratory studies, including complete blood count, liver function studies, and coagulation tests. Patients with good performance status and preserved liver function are considered appropriate for percutaneous liver ablation. Contrast-enhanced (CE) CT images or magnetic resonance images (MRI) are obtained within one month of evaluation and procedure. US assessment is performed at the clinic visit to ensure sonographic visibility and percutaneous approach for ablation. The approach is communicated with the procedure team and helps to streamline preparation on the procedure day.
Procedures are scheduled for general anaesthesia in the interventional CT suite and proper patient positioning for the procedure is a team effort: a posteriorly located tumour may require oblique positioning of the patient, and safe positioning of arms overhead improves CT image quality.
Non-contrast and multiphasic CE-CT are typically obtained prior to probe placement. This helps to review anatomy pre-procedure, confirm tumour location and size, and optimise the percutaneous approach. When possible, probes are placed under direct US guidance. Few cases have tumours visible only on CT or only after lipiodol staining with transarterial chemoembolization (TACE). In these cases, CT navigation software is used to optimise probe placement, which is often best in double oblique approaches to maximise both safety and efficacious tumour treatment. Respiratory manoeuvres in concert with the anaesthesiology team are utilised as needed to accurately and precisely target tumours with ablation probes. A non-contrast CT is obtained to confirm and document probe position. Hydrodissection and/or biopsy, if being performed, are done after securing ablation probe position(s). CT and US are complementary imaging to confirm appropriate tumour targeting and predict ablation zone coverage. Activated probes and ablation zone formation are monitored in real time with US and intermittent CT. This allows for confirmation of ablation zone formation and coverage.
Another CE-CT is obtained at the conclusion of the ablation. Total contrast volume is split between pre- and post-ablation CE-CT, not to exceed 150–200ml of iodinated contrast agent. Post-ablation CE-CT assesses ablation zone coverage of the tumour with adequate margins and also evaluates for any complications. If margins are inadequate, additional ablation can be performed at this time.
A recent addition to our practice is MR-guided cryoablation. This technology allows ablation of small liver metastases that are visible only on MRI. Patient positioning and tumour targeting require additional considerations to maintain safety in the MR environment.
Patients receive a check-up telephone call from a nurse the day after the procedure and are then seen one month post-procedure in clinic along with CE-CT/MR. Follow-up with imaging occurs every three months, which may be extended to every six months after one year of documented complete response.
Amanda Smolock is assistant professor at the Division of Vascular and Interventional Radiology, Department of Radiology, Medical College of Wisconsin (Milwaukee, USA).
Relevant disclosures: consultant/speaking faculty and grant recipient/research support, Neuwave Medical.
Terumo Europe has announced in a press release that it welcomes the guidance released by the National Institute for Health and Care Excellence (NICE) mentioning that microwave ablation can be used provided standard arrangements are in place for clinical governance, consent, and audit. This has the potential to broaden access to minimally invasive alternatives to surgery available to patients with symptomatic benign thyroid nodules.
The guidance describes ultrasound-guided percutaneous microwave ablation for symptomatic benign thyroid nodules as a minimally invasive procedure that can be performed in an outpatient setting using local anaesthesia. The aim is to reduce symptoms and improve cosmetic appearance by making the nodule smaller while preserving thyroid function, and with fewer complications than surgery.
This guidance is part of NICE’s interventional procedure programme which considers whether interventional procedures are safe and work well enough for wider use in the NHS. A comprehensive review of the literature and consultations with clinical experts and patient representatives informed the decision.
This is a positive endorsement of the treatment and a complement to the 2020 European Thyroid Association clinical practice guideline for the use of image-guided ablation in benign thyroid nodules.
The NICE document also reports that using uncooled microwave ablation devices means thinner needles can be used.
“Nowadays microwave technology is widely used in liver, lung, and kidney ablation” says Eduardo Crespo, chief of the radiology department at Hospital Universitario Fundación Jimenez Diaz (Madrid, Spain). “So far, the main gap to approach thyroid ablation has been the lack of thinner and shorter probes, to avoid potential damage to the adjacent nerves, which could lead to complications. Within the TATOpro antennae range, Terumo Interventional Systems introduced a dedicated thyroid antenna as thin as 18G with a length of 8 cm, to be used at limited power. Moreover, a 17G antenna is also available to treat larger nodules in one session, avoiding the need for patients to come back for multiple treatments.”
Soundbite Medical Solutions announced that it has entered into an exclusive license agreement with VFLO Medical (VFLO).
Pursuant to the agreement, Soundbite has granted VFLO an exclusive license for certain proprietary products including its SoundBite crossing system and the Active microcatheter system. Under the Agreement, VFLO is entitled to manufacture, develop, and commercialise the products in mainland China, Hong Kong, Macau, and Taiwan. Soundbite is, in return, entitled to receive an upfront fee, subsequent milestone payments, plus royalties from sales of such products. The terms also allow cross-licensing on future improvements of the products, aligning both companies’ focus on innovation.
“The growing prevalence of atherosclerotic vascular disease burdened by calcium has become a serious public health problem in China. We are excited to partner with the Soundbite team and look forward to bringing the unique technology and portfolio of treatment solutions to patients in Greater China that suffer from calcified arterial disease,” commented Dong Wu, president and CEO of VFLO.
“We are thrilled to work with VFLO to bring our revolutionary shock wave technology to patients in China, opening a key market for our company with an experienced partner like VFLO. Bringing non-dilutive capital to our shareholders provides us with the opportunity to build meaningful value while serving patients in the growing Chinese market,” said Lori Chmura, president and CEO of Soundbite.
VentureMed Group has announced new data presentations on the treatment of peripheral arterial disease (PAD) with drug-coated balloon (DCBs) in addition to 12-month AV Registry Data. These presentations will be given as part of the VEITH Symposium Annual Scientific Meeting 2022 (15–19 November, New York, USA).
Data presented will cover the use of FLEX Vessel Prep System in both PAD treatment with DCB and also in arteriovenous (AV) access interventions. The AV Access presentation will expand the six-month AV Registry data presented at VASA in June with 12-month results.
The first of two presentations will be titled “Late Breaking Trial with FLEX Vessel Prep and DCBs Show Better 12-Month Results With FemPop” and be presented by Eric A Secemsky (Beth Israel Deaconess Medical Centre, Boston, USA).
The second is titled “FLEX Vessel Prep System: Clinical Outcomes and Utility in HD Access Practice—AV Registry 12-Month Study Results,” and will be shared by primary investigator John E Aruny (Dialysis Access Institute, Orangeburg, USA).
Interventional News’ most popular content last month featured a report on the need for greater interventional radiology (IR) service coverage in rural areas of the USA; news of a US Food and Drug Administration (FDA) premarket approval (PMA) submission by Endologix; new restorative haemodialysis access graft data from Xeltis; and the release of three-year effectiveness data for the Abre stent (Medtronic).
A new report from a joint taskforce of the American College of Radiology (ACR) and the Society of Interventional Radiology (SIR) recommends improved access to interventional radiologists in small and rural areas.
Xeltis today announced what it describes as “very promising” preliminary efficacy and safety results from one of the centres participating in the AXESS study—a first-in-human (FIH) clinical trial of its restorative haemodialysis access graft, Axess.
Roberto Luigi Cazzato speaks to Interventional News about the emergence of IR outpatient clinics (IROCs) and his view that IR hospitalisation clinics (IRHCs) will soon begin being established too.
XACT Robotics announced that its ACE Xtend remote control unit received US FDA clearance, allowing users to robotically insert and steer the XACT ACE Robotic System remotely from the control room.
Medtronic has announced the 36-month final results from the ABRE clinical study, the puropse of which was to evaluate the safety and effectiveness of the Abre venous self-expanding stent system, intended for the treatment of symptomatic iliofemoral venous outflow obstruction.
In the USA, atherectomy use in peripheral vascular interventions (PVIs) “more than doubled” from 2010 to 2019, with office-based procedures a “major driver” of this increase. This is according to published US data from the Vascular Quality Initiative (VQI).
Mark Little (Royal Berkshire Hospital, Reading, UK) brought delegates up to speed on genicular artery embolization (GAE) for knee osteoarthritis over two sessions at the recent British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK). Little led audience members through the existing body of evidence for GAE’s safety and efficacy, before outlining the roadmap for growing this further in order to gain UK National Institute of Health and Care Excellence (NICE) recommendation.
“We set up the first European study [GENESIS] back in 2017 and the interim analysis was published in CVIR [CardioVascular and Interventional Radiology] last year.” Little began his presentation by offering the BSIR audience background to his research. The participants in the study, he explained, were “patients with mild-to-moderate knee osteoarthritis [OA]”, numbering 38, and who “had to have had at least an attempt at conservative treatment in the six months preceding referral.”
Regarding the method and materials used, Little shared that for GENESIS, he used 100–300-micron Embosphere particles, and “skin-to-skin”, the embolization procedure took “about an hour”.
For both GENESIS and the now-enrolling GENESIS II studies, Little stated the primary outcome as being knee pain and function, assessed according to the Knee Injury and Osteoarthritis Outcome Score (KOOS). The measure of technical success, the presenter elaborated, was carrying out the embolization, which, according to the GENESIS interim analysis was 84%.
Posing the rhetorical question “Why was it not 100%?”, Little gave by way of an answer that they did not embolize six patients. The reasons in each case varied among a “risk of non-target embolization to the skin, anastomotic communication between the genicular and popliteal arteries posing an unacceptable risk of non-target embolization, and a lack of hyperaemia”.
Interim results show “initial improvement sustained to follow-up”, Little declared, before alluding to the fact that, for the one-year data, due for publication in 2023, “the trends are the same”.
Little then addressed the NICE appraisal for GAE that he undertook 18 months ago. NICE recommend research preferably in the form of randomised controlled trials against sham or current best practice. Patient-reported outcome data will also be key, Little reported.
Brain scans and a neuropsychometric questionnaire were also included in the GENESIS trial to evaluate the impact of chronic pain on procedure outcomes. The finding, Little relayed, was that “there is a strong signal between patient catastrophising and poor outcomes” in terms of pain.
Rounding off his coverage of GENESIS, Little concluded that the trial demonstrated that GAE for mild-to-moderate knee OA is “safe with potential efficacy” and has “good scientific rationale”. To prove efficacy and heed NICE’s request for more data, there is GENESIS II, to which the presenter then turned.
This trial began two weeks ago, and is using the same KOOS primary endpoint, with a placebo comparison, the presenter outlined. Patient-reported outcome data will constitute a secondary endpoint, Little added. GENESIS involved a patient questionnaire, from which the results showed that “75% [of participants] would be more than happy to have [the procedure] again”.
Session chair Rob Morgan (St George’s Hospital, London, UK) asked Little whether anyone in the field had gathered data over more than a year—“there are Japanese data to four years,” the presenter replied, following up by affirming that “the effects [are] maintained”.
In the second session of GAE coverage, Little spoke to deepened understanding of knee OA anatomy that has come in the last decade, citing discoveries about vessel formation as “pivotal”.
Pre-empting the question of where GAE fits into the treatment strategy, Little asserted that the majority of knee OA patients are treated by their general practitioner but that many of those will fail conservative therapy, including injections and physiotherapy. Moreover, the presenter went on, “there is a treatment gap between those [whose conservative treatment has] failed and those who are eligible for joint replacement surgery—orthopaedic surgeons do not like to operate on young patients, [for example].”
The current ideal patient, Little communicated, is one with mild-to-moderate knee OA, as these are the individuals in whom the procedure has been trialled to date. There is good data concordance despite slight differences in technique and embolic agent across various centres—“patients get better and then there is a plateau”.
Conrad von Stempel (University College London Hospitals, London, UK) put the question to Little, following his presentation, of how to convince orthopaedic colleagues to refer patients for GAE. According to Little, “these are difficult to treat patients as they will have failed conservative treatments but are not surgical candidates”. Orthopaedic colleagues “are delighted” to have another potential treatment option in the form of GAE. “It is a completely different mindset to traditional turf wars,” Little emphasised.
The Society of Interventional Radiology (SIR) published a position statement deeming endovascular thrombus removal “an acceptable treatment option in selected patients with acute iliofemoral deep vein thrombosis [DVT].” The position statement is published online on the Journal of Vascular and Interventional Radiology (JVIR) website.
SIR convened a multidisciplinary writing group that conducted a comprehensive literature review. The group used evidence from 84 studies—including randomised trials, systematic reviews and meta-analyses, prospective single-arm studies, and retrospective studies—to develop 17 recommendations to guide the use of endovascular venous intervention for the care of patients with acute iliofemoral DVT.
Among the key recommendations were for physicians to quickly identify DVT and provide prompt and adequate anticoagulation, symptom control and functional recovery at the time of diagnosis. For those with anatomically extensive and clinically severe DVT and low bleeding risk, a form of catheter-directed thrombolysis (CDT) is reasonable to use in carefully selected patients after evaluating their comorbidities and personal preferences.
“Endovascular management has been used to treat select patients with acute iliofemoral DVT for more than 25 years, but newer and better designed studies have shown us that such interventions are most effective and safest when applied to younger patients with severe DVT symptoms,” said Suresh Vedantham lead author and an interventional radiologist with the Washington University in St Louis (St Louis, USA).
“Most DVT patients will benefit from anticoagulation alone, and can be spared anything more invasive, but for those who are suffering from severe symptoms or are at the highest risk of developing lifestyle-limiting post-thrombotic syndrome, catheter-directed therapies are appropriate and effective in reducing symptom severity early and late,” said Vedantham.
Vedantham was the primary investigator on the ATTRACT trial, the findings of which were published in 2017 and informed the new recommendations. Vedantham lauded the efforts of the international thrombosis research community in conducting several pivotal randomised trials to enable well informed guidelines, and the strong support of the SIR Foundation in the development and conduct of ATTRACT.
Based on the findings of the ATTRACT trial, the position statement authors recommend against the use of CDT for most patients with DVT that is limited to the tibial, popliteal, and femoral veins, for patients with clinical factors that confer a moderate or high risk for bleeding, and for patients with only mild lower extremity symptoms.
“Patient selection is the most important factor for success in the application of interventional treatments,” said, Kush R Desai, chair of SIR’s Venous Disease Clinical Specialty Council, a co-author of the statement, and an interventional radiologist with Northwestern Medicine (Chicago, USA). “Our recommendations follow the evidence so those who may benefit from endovascular treatment options are quickly identified to receive care and ensure positive outcomes.”
“Timing of intervention for acute deep vein thrombosis is important to optimise outcomes,” said Ronald S Winokur, vice chair of SIR’s Venous Disease Clinical Specialty Council, co-author of the statement, and an interventional radiology with Weill Cornell Medicine (New York, USA). “Clear guidance on patient selection including an understanding of extent of disease and accounting for flow dynamics helps patients receive the best treatment at the right time.”
As further research proceeds, SIR believes that adherence to the recommendations in the position statement allow for the use of endovascular therapy in a manner that optimises benefit and minimizes harm.
“SIR is dedicated to the evidence-based practice of interventional radiology and ensuring our position statements and guidelines reflect the findings of the latest science so patients receive the best possible care,” said SIR President Parag J Patel, an interventional radiologist with the Medical College of Wisconsin (Milwaukee, USA). “Thank you to the authors for their time and energy to ensure that DVT patients have access to the care appropriate for their case and medical history.”
The Chocolate Touch drug-coated balloon angioplasty balloon
Genesis MedTech Group announced that the US Food and Drug Administration (FDA) has approved the Chocolate Touch drug-coated balloon (DCB) percutaneous transluminal angioplasty (PTA) catheter developed by TriReme Medical for the treatment of patients with peripheral artery disease (PAD) in the superficial femoral artery (SFA) and the popliteal artery.
The Chocolate Touch DCB was shown to have statistically superior patency and non-inferior safety at 12 months as compared with Lutonix DCB based in a head-to-head, randomised trial of patients with symptomatic femoropopliteal disease.
The Chocolate Touch showed statistically superiority in its primary efficacy endpoint of 12-month true DCB success—a measure of the target vessel remaining patent without the need for bail-out stenting. Primary patency by Kaplan-Meier (KM) estimate was 83.3% for the Chocolate Touch and 73.0% for Lutonix DCB at 12 months.
The primary safety endpoint of 12-month freedom from major adverse events (MAEs) was 88.9% for those treated with the Chocolate Touch versus 84.6% for Lutonix DCB.
Additionally, Chocolate Touch results reported the lowest all-cause KM mortality value as compared to reported mortality for FDA-approved DCBs in pivotal studies. Mortality rates for Chocolate Touch using KM estimates at three years were 6.7% for the Chocolate Touch and 11.1% for the Lutonix DCB.
“I am very excited to see the Chocolate Touch, a next-generation DCB, is now available for patients across the USA. This technology is an important tool in the armamentarium for the treatment of patients with PAD,” stated Mehdi H Shishehbor, interventional cardiologist at University Hospitals Harrington Heart and Vascular Institute (Cleveland, USA) and the Chocolate Touch trial’s co-principal investigator.
Chocolate Touch is designed to open in small sections using pillow-like structures coated with a therapeutic agent with the goal of providing patients suffering from PAD with an alternative treatment to traditional DCB angioplasty.
“This next-generation paclitaxel DCB is based on the chocolate mechanism of pillow-and-groove formation resulting in an increased balloon surface facilitating effective drug release to the vessel wall and potentially reducing the need for permanent implants. The recently completed randomised, controlled study demonstrated excellent primary results, with statistical superior effectiveness as compared to the control DCB. The Chocolate Touch is a DCB category of its own,” commented co-principal investigator Thomas Zeller of Universitaets-Herzzentrum (Bad Krozingen, Germany).
Xeltis announced today the initiation of a pivotal trial with the “first-ever” restorative synthetic haemodialysis access grafts, dubbed ‘Axess’.
The first two patients have been successfully implanted as part of the AXESS European pivotal trial at AZ Sint-Jan Brugge-Oostende AV (Bruges, Belgium) by vascular surgeon Jan De Letter, and discharged from hospital.
The AXESS EU pivotal trial is a prospective, single-arm study to evaluate the safety and performance of Axess in patients with end-stage kidney disease who need haemodialysis. The study will enrol 110 patients at up to 25 centres in Europe and will follow them for five years.
The Axess graft has been previously successfully implanted in 20 patients, as part of the AXESS first-in-human (FIH) trial, which completed enrolment in September 2022. AXESS FIH full cohort data are expected in 2023.
“A device that enables immediate use, as seen with the existing synthetic ePTFE [expanded polytetrafluoroethylene] grafts, and turns into a living blood vessel that recovers promptly after puncturing from each dialysis session may become the safer and longer-lasting solution that patients on haemodialysis need,” explained De Letter, who also has previous experience with Axess, having implanted it during the FIH trial. “We are encouraged by the promising preliminary experience with this device from the FIH trial, and confirmation in a larger trial involving more patients and implanting sites is an important next step.”
The Axess graft is a restorative, synthetic, electrospun blood vessel for arteriovenous haemodialysis access. Once implanted, its porous microstructure gets colonised by the patient’s own tissue cells through the body’s natural healing process, turning into a living vessel made of their own tissue over time.
“Life for patients on haemodialysis means multiple hospital visits each week, involving puncturing, bleeding, waiting, healing and risk of infections from all of the above, in addition to poor renal function,” added An De Vriese, head of Nephrology and Infectious Diseases at AZ Sint-Jan Brugge-Oostende AV, and one of the coordinating investigators of the AXESS EU pivotal trial. “If a novel device can spare part of this burden through reduced bleeding, prompt coagulation and healing, lower infection risks and longer durability, it would be a life-changing experience for most patients.”
HYBRID - fluorescent Neon tube Sign on brickwork - Front view - 3D rendered royalty free stock picture. Can be used for online banner ads and direct mailers.
Chris Titze Imaging/stock.adobe.com
Chris Titze Imaging/stock.adobe.com
Year three of the COVID-19 pandemic and yet much now feels unrestricted and ‘back to normal’. This can certainly be said of meetings—at least in Europe and the USA—which, throughout 2020 and some of 2021, took place online, but have returned to in-person in recent months. However, transatlantic, intra-European and American travel, though possible and permitted, has not been plain sailing (flying?), even this year. Therefore, many societies, within interventional radiology (IR) or otherwise, for 2021/2022, have opted for a hybrid setup, where delegates have had the choice of accessing sessions, or to travel to the physical venue. Several society spokespeople relay to Interventional News their plans for the hybrid and in-person evolution of some of the IR calendar’s main meetings, based on how those from the last couple of years have panned out.
Parag J Patel (Medical College of Wisconsin, Milwaukee, USA), president of the Society of Interventional Radiology (SIR), provides the perspective of a society that has, deliberately, not offered hybrid attendance options. The reason being, he explains, that “this allows us to provide a consistent experience to all who participate, ensuring valuable learning, interactions with speakers, and connection to the materials.” So, this year’s Society of Interventional Radiology annual meeting (SIR; 11–15 June, Boston, USA) was in-person only, and 2021’s exclusively online, after the 2020 meeting, scheduled for late March, was cancelled. However, Patel notes, the SIR 2022 plenary sessions were available via livestream, and saw 230 viewers tune in.
This reflects where the society stands on the question of a hybrid future for meetings right now, and Patel details how the hybrid model has, by no means, been discounted by SIR, which is “exploring the possibility of deploying hybrid models at future meetings to allow more IRs to participate in the way in which they prefer to or are able to attend. We know that travel and time off can be a challenge, and hybrid models enable accessibility from an attendance standpoint.”
In contrast, the European Society of Radiology (ESR)’s director of communications David Zizka tells Interventional News, that his society has taken a hybrid approach to its annual meeting, the European Congress of Radiology (ECR) since 2013 when it started streaming educational content. “Our participants are used to having the option to attend the event either onsite or online, but in many cases, they choose to attend in both ways,” Zizka notes, qualifying this statement with the following: “What we have learned this year is that there is no strict distinction between an onsite or online visitor anymore, as many of our participants visit us in Vienna, but not for the entire five days, and then continue their ECR experience online.”
Concerns for superiority of in-person experience not universal
Patel expresses concerns that moving away from in-person only, may not be solely positive for the SIR meeting—as the rationale for not offering SIR 2022 in a hybrid format suggests. “We want to ensure that what we deliver does not create silos in the audience based on the format through which the attendee chose to participate. There is a risk with a hybrid approach that one group receives a lesser experience because they are not in the audience,” Patel acknowledges, before highlighting what underpins this reservation. “We do not just want to broadcast content to a passive audience. We want to actively engage our audience in discussion and learning, whether in-person or online.”
Zizka appears not to share such concerns, stating that “we are stepping away from differentiating participants according to [whether they are online or onsite attendees], as ECR is not a single event anymore but a year-long one with a variety of ways of participating.” He expands upon this assertion, pointing to the fact that “watching sessions on-demand during the actual congress period and especially afterwards for the rest of the year has become very popular amongst our participants.”
Adding his voice to the discussion, the Radiological Society of North America (RSNA) associate executive director for meetings services and corporate relations John Jaworski, whose opinion comes from the position of having 40% of RSNA attendees come from outside of North America, is therefore aware of the constraints that prevent people from travelling to the physical event space. Luckily, he acknowledges that “RSNA is fortunate to have a great team able to support both [the in-person and virtual] events,” which enables the society to fulfil the important objective of “[reaching] a greater number of healthcare professionals across the globe and providing them with important educational content to assist in patient care.”
Shared observations of post-pandemic attendance upswing
Patel underlines that all societies are having to consider how to keep optimal engagement from attendees the foremost priority. Interestingly, Zizka underlines that there was already “a regressive trend in onsite meeting attendance before COVID-19”, but that a reduction in appetite for attending in person may have been “accelerated” by the pandemic. In the eyes of the ESR spokesperson, “onsite attendance must be a special experience for the participant [if the meeting has a remote attendance option], something that adds unique benefit in comparison to online-only participation,” justifying this with the point that offering hybrid meetings means “you will see a decrease in onsite participation.”
But, right now, in the immediate aftermath of lockdowns, Patel recounts witnessing “a chorus of excitement and eagerness to be completely in-person,” at SIR 2022. “Screen fatigue is real,” Patel adds, attributing the “[palpable] desire to continue to meet in person” to this fact. Jaworski has observed the same enthusiasm for the in-person RSNA annual meeting: “Currently, our in-person registration is up 54% from this time last year, while our virtual meeting is on a par with 2021,” he relays to Interventional News. This follows an RSNA 2021 meeting for which attendance was “in line with our expectations”—30,000 attendees, of whom 6,000 attended virtually.
ECR received similarly positive feedback about their 2022 meeting, including from those who made last-minute decisions to attend remotely instead of in Vienna, and vice versa. “A big benefit of our registrations system is that every ECR ticket allows for full onsite and online access,” Zizka emphasises, “so participants can make that decision at any time without any bureaucratic efforts.”
Priorities for a bright future of IR meetings
Quizzed on how SIR plans on fulfilling the aforementioned goal of maintaining high levels of engagement, Patel refers to the possibility that SIR 2023 will livestream “at least some in-person sessions and in ways to ensure that any online audiences are actively engaged in the lessons happening on site in Phoenix.” After the fact, an on-demand library will enable attendees to revisit sessions, or view those they missed, Patel adds, stating that this “will also be available for purchase after the meeting for those who could not attend in person.”
The priority for the RSNA meeting logistics-wise, Jaworski brings to Interventional News’ attention, is to “better connect the virtual attendee to the in-person meeting.” For him this means “[looking] at almost every session like a TV studio and [considering] what the virtual attendee will be seeing and hearing.” One example of a simple but pivotal consideration in this regard is checking that in-room microphones are switched off during breaks “so personal conversations are not broadcast virtually”. Jaworksi adds that the RSNA is also “working on a way to better connect the virtual attendee with the speaker during session question and answer sessions, which will require some re-training of session moderators.” Finally, he alludes to the longer-term goal of RSNA “[improving] virtual networking between attendees and engagement opportunities with virtual exhibitors.”
Patel appears optimistic about the future of SIR meetings, in whatever variation on a hybrid form they may take, based on the 4,000-strong attendance at the 2022 meeting. Even if in-person attendance is set to decrease, as Zizka predicts, he believes that the strategies the ESR is adopting will mitigate this, at least in part, with “state-of-the-art online participation possibilities that live up to the latest technical trends, and [by reinventing] our event every year [to make it] a unique experience […] that people are always drawn to take part in onsite.” Jaworksi sees the meetings trend going the way of fewer attendees overall “in the short-term”, before increased comfort with travel leads to an uptick in attendance once more. “Nothing is better than face-to-face meetings for connecting with colleagues and developing relationships,” he professes, suggesting too that “competition from virtual meetings will lead to better in-person meetings […] with experience and engagement opportunities for attendees, such as interactive and hand-on experiences.”
ReCor Medical and its parent company, Otsuka Medical Devices, announced consistent and significant blood pressure-lowering results across a range of patients with uncontrolled hypertension, including across differences in age, sex, baseline blood pressure, medication level and ethnicity. The results come from analysis of the pooled data from ReCor’s RADIANCE global clinical trial programme: three prospectively powered, randomised and sham-controlled clinical trials which evaluated the endovascular Paradise ultrasound renal denervation (uRDN) system in patients with uncontrolled hypertension.
The results were presented at the 2022 American Heart Association (AHA) annual meeting (5–7 November, Chicago, USA) by Ajay Kirtane, professor of medicine at Columbia University and an interventional cardiologist at New York-Presbyterian/Columbia University Irving Medical Center (both New York, USA).
The RADIANCE pooled analysis includes data from more than 500 patients randomised in the three studies from ReCor’s RADIANCE global programme: RADIANCE-HTN TRIO, which studied patients with resistant hypertension, and RADIANCE-HTN SOLO and RADIANCE II, which studied patients with mild-moderate hypertension. The combined dataset showed an overall reduction in daytime ambulatory systolic blood pressure in the uRDN group of -8.5mmHg (p<0.0001) with a difference between treatment and sham at two months of -5.9mmHg (p<0.0001), favouring uRDN. Blood pressure results were similarly positive in the 24-hour, nighttime, home, and office measures. A favourable safety profile was consistently observed following uRDN treatment across the studies.
“Pooling the data from the RADIANCE programme demonstrates that treatment with the Paradise uRDN System results in a consistent reduction in blood pressure across differing severities of hypertension. The consistent and clinically meaningful blood pressure reduction across multiple patient groups increases our interest in the use of uRDN as a potential therapeutic option, when added to lifestyle modification and medications for our patients with uncontrolled blood pressure,” said Kirtane, study co-principal investigator.
“It is very important that the RADIANCE pooled analysis demonstrated a consistent blood pressure reduction in patients across a range of hypertension and both with and without antihypertensive medication, thus broadening the potential applicability of uRDN. Just as important, more than 50% of patients treated with uRDN in the pooled analysis either achieved daytime ambulatory blood pressure control or had a greater-than-10mmHg decrease in daytime ambulatory systolic blood pressure at two months, showing the potential benefits of uRDN as an element of a treatment regimen for patients with uncontrolled hypertension,” said study principal investigator Michel Azizi, professor of medicine at Université Paris Cité, Hôpital Européen Georges Pompidou, Paris, France.
The RADIANCE global programme is an international, multicentre initiative designed to explore the benefits of ultrasound renal denervation in hypertension. The RADIANCE studies are double-blind, randomised, sham-controlled trials designed to provide information about the ability of the Paradise uRDN System to treat high blood pressure. All three studies in the RADIANCE global programme were individually powered for efficacy with a primary endpoint of daytime systolic ambulatory blood pressure at two months, and all three met their primary efficacy endpoint with statistical significance at two months.
If maintained in the long-term, the blood pressure reductions demonstrated in the RADIANCE pooled analysis correlate to a potential 25% reduction in cardiovascular risk as shown in a meta-analysis of the cardiovascular benefits of antihypertensive medications.
Medtronic has announced the six-month results from the full cohort of the SPYRAL HTN-ON MED clinical trial. The late-breaking data were presented at the American Heart Association (AHA) Scientific Sessions 2022 (5–7 November, Chicago, USA). With this news, Medtronic has submitted the final module of the Symplicity Spyral premarket approval (PMA) package to the US Food and Drug Administration (FDA) for review and approval.
Subjects who were prescribed antihypertensive medications and were treated with the Medtronic Symplicity Spyral renal denervation (RDN) system had a statistically significant and clinically meaningful reduction in office-based systolic blood pressure (OSBP), a key secondary endpoint, compared to subjects in the sham control group. However, in the primary endpoint, RDN did not demonstrate a statistically significant reduction in 24-hour ambulatory systolic blood pressure (ABPM) due to increased medications in the sham control group and the potential impacts of the COVID-19 pandemic on the clinical trial environment. The study also included win ratio, a pre-specified secondary endpoint that combines reduction in blood pressure with reduction in medication burden, which enables assessment of the overall beneficial effect of RDN. The win ratio demonstrated significance in favour of RDN versus a sham procedure. Finally, the study met its primary safety endpoint, with a low incidence of procedure-related and clinical adverse events.
“The ON MED study demonstrated significant reductions in office-based blood pressure, the most commonly used measure in clinical practice. Additionally, we saw reductions in absolute blood pressure that were consistent with earlier RDN studies,” said David Kandzari, chief, Piedmont Heart Institute and Cardiovascular Services (Atlanta, USA) and SPYRAL HTN-ON MED principal investigator. “Surprisingly, 24-hour ABPM declined with RDN but did not differ from the sham group, and the primary endpoint was not met. More than 80% of patients in the ON MED expansion group experienced follow-up during the COVID-19 pandemic. Compared with patients enrolled before the pandemic, significant differences in baseline 24-hour ABPM were observed that may reflect changes in patient behaviour and lifestyle during the pandemic. Additionally, patients treated with the sham procedure increased the amount of medication they were taking compared to those treated with RDN. These factors likely contributed to the smaller-than-expected differences in ABPM.”
SPYRAL HTN-ON MED is a global, randomised, sham-controlled trial investigating the blood pressure-lowering effect and safety of RDN with the radiofrequency (RF)-based Symplicity Spyral RDN system in hypertensive patients who have been prescribed up to three antihypertensive medications, including diuretics, calcium channel blockers, ACE/ARB inhibitors or beta blockers. A total of 337 patients with uncontrolled hypertension were enrolled at 42 sites across the USA, Europe, Japan, Australia, and Canada, and were randomised 2:1 to RDN (n=205) versus sham control (n=132). Results were as follows:
The primary Bayesian efficacy endpoint of 24-hr systolic ABPM reduction was not met, with a 51% probability of superiority for the RDN group versus those who received a sham control procedure. However, nighttime systolic ABPM reduction was statistically significant.
6.5 mmHg 24-hr systolic ABPM reduction in the RDN group versus 4.5 mmHg in the control group (treatment difference of -1.9 mmHg, p=0.119)
6.7 mmHg nighttime systolic ABPM reduction in the RDN group versus 3.0 mmHg in the control group (treatment difference of -3.7 mmHg, p=0.01)
The study met the prespecified secondary endpoint, which was the change in OSBP from baseline to six-month follow-up between the RDN group (n=199) and the sham control group (n=126).
Statistically significant 9.9 mmHg OSBP reductions in the RDN group versus a 4.9 mmHg reduction in the sham control group (treatment difference of -4.9 mmHg, p=0.001)
The study met the primary safety endpoint, evaluating major adverse events at one month post-procedure, and renal artery stenosis at six months, pooled across the SPYRAL HTN-ON and OFF MED studies (p<0.001)
RDN demonstrated a low incidence of procedure-related and clinical adverse events at six-months in the SPYRAL HTN-ON MED study specifically.
The win ratio demonstrated significance in favour of RDN versus a sham procedure (p=0.005).
Overall burden of medications was higher in the sham control group at six months (p=0.04).
L-R: Alik Farber, Matthew Menard, and Kenneth Rosenfield
L-R: Alik Farber, Matthew Menard, and Kenneth Rosenfield
The first results from the BEST-CLI randomised controlled trial (RCT) of 1,830 patients show that surgical bypass with adequate single-segment greatsaphenous vein (GSV) is a more effective revascularisation strategy for patients with chronic limb-threatening ischaemia (CLTI) who are deemed to be suitable for either an open or endovascular approach. Researchers also found that both strategies can be accomplished safely and are effective for treatment for CLTI.
Further, the triallists urge that patients with CLTI who are candidates for limb salvage should undergo an evaluation of surgical risk and conduit availability. “Bypass surgery with adequate single-segment saphenous vein should be offered as a first-line treatment option for suitable candidates with CLTI as part of a fully informed shared decision-making. Level one evidence from BEST-CLI does not support an endovascular-first approach to all patients with CLTI. In patients without a suitable single-segment saphenous vein, both surgical and endovascular strategies are effective in treating patients with CLTI, so we believe that there is a complementary role for both revascularisation strategies in these patients,” they say, bringing the “quality of vein” back into the centre of discussion on revascularisation strategy.
The co-principal investigators—Alik Farber (Boston Medical Center, Boston, USA), Matthew Menard (Brigham and Women’s Hospital, Boston, USA), and Kenneth Rosenfield (Massachusetts General Hospital, Boston, USA)—note that this is the largest RCT comparing revascularisation treatment strategies in patients with CLTI and will provide important information regarding the management of these patients.
BEST-CLI (Best endovascular versus best surgical therapy for patients with CLTI) randomised patients with CLTI and infrainguinal peripheral arterial disease (PAD) to receive either infrainguinal bypass or endovascular intervention. The trial consisted of two parallel trials: Cohort 1 included patients with single-segment great saphenous vein; Cohort 2 included patients who lacked single-segment GSV and therefore alternative autogenous vein or prosthetic was used in those randomised to the open arm.
According to Farber, the best way to evaluate whether a patient has single-segment GSV—one he says needs to be at least 2.5mm in diameter, but ideally above 3mm, and must be free of thrombus—is by using duplex ultrasound. Speaking to Vascular News on this topic, Menard notes that while assessment of the vein is common practice for vascular surgeons, it is not for other specialties. In the wake of BEST-CLI, he suggests that evaluation of the GSV—a “very important” part of the assessment for treatment—should be included in the guidelines.
Farber tells Vascular News: “We are not claiming to bring down the 10 commandments here; all we are saying is that we are introducing some level one data into a space that has almost no Level one data.[…]. Here is another study that says the endovascular-first [approach] is a great thing for some people, but [it is not] for everybody. So, if a patient is a candidate for surgery and [..] has a good single-segment saphenous vein, there should be a conversation about surgery, for that individual.”
Key results
The investigators found that surgery was more effective than endovascular therapy in the Cohort 1 patients. At AHA, Farber revealed that there was a reduced rate of major adverse limb event (MALE) or all-cause death—the primary endpoint—in patients with good single-segment GSV who underwent open surgery, as well as fewer major reinterventions, at median follow-up of two point seven years. The maximum follow-up time in these patients was seven years.
Going into the details, Farber noted that Cohort 1 included 1,434 patients with single-segment GSV who were randomised 1:1 to either surgical or endovascular treatment. At median follow-up, the rate of MALE or all-cause death was 42.6% in the surgery arm compared to 57.4% in the endovascular arm (hazard ratio, 0.68; 95% confidence interval [CI], 0.59 to 0.79; p<0.001). In terms of secondary endpoints, he revealed that 10.4% of patients in the surgery arm underwent above-ankle amputation of the index limb versus 14.9% in the endovascular arm, in addition to rates of 9.2% vs. 23.5% for major reintervention on the index limb and 33% vs. 37.6% for all-cause death for patients in the open and endovascular arms, respectively.
In patients who did not have adequate saphenous vein, i.e. those in Cohort 2, there were no significant differences in the primary endpoint. Farber detailed that that this group included 396 patients who were randomised 1:1 to either surgical or endovascular treatment. The median follow-up was 1.6 years and maximum follow-up, 5.1 years. Farber reported that the rate of MALE or all-cause death in this cohort was 42.8% vs. 47.7% in the open and endovascular arms, respectively (hazard ratio, 0.79; 95% CI, 0.58 to 1.06; p=0.12). The corresponding figures for the secondary endpoints were as follows: 14.9% vs. 14.1% for above-ankle amputation of the index limb; 14.4% vs. 25.6% for major reintervention on the index limb; and 26.3% vs. 24.1% for all-cause death.
Farber added that there were no differences in perioperative mortality or major adverse cardiovascular events (MACE), and that mortality and MACE were similar between treatment strategies over the course of follow-up.
The presenter concluded that surgery with adequate saphenous vein “should be offered as a first-line treatment option for suitable candidates with CLTI, as part of fully informed, shared decision-making”. He added that level one evidence from BEST-CLI “does not support an ‘endovascular-first’ approach to all patients with CLTI,” and instead supports a “complementary role” for both revascularisation strategies. He noted that further studies are needed to better elucidate the comparative outcomes in subsets of patients.
While the primary focus of the trial was clinical outcomes in the comparison of open surgery versus endovascular therapy, Menard tells Vascular News that the investigators planned two “very important” ancillary assessments: cost-effectiveness—which the team is yet to conduct—and quality of life. With regards to the latter, he noted that the team used a number of different metrics for this, including the vascular disease-specific VascuQoL, as well as the EQ-5D and the SF-12.
According to Menard, the baseline scores for quality of life speak to the impact of CLTI on patients’ everyday lives: “The quality of life for all patients at baseline on entry into the trial was extremely poor and low, and that is consistent with what is known about the devastating impact of CLTI on patients’ overall function, the mental status, their physician limitations, and their high degrees of pain.”
Menard reports that both revascularisation strategies resulted in “significant gains” across every metric studied, noting also that there was not any significant difference between the two treatment arms.
Making the case for the benefits of the endovascular approach, Rosenfield emphasises: “This is the first trial that really shows that when you compare ‘endo’ to surgery, certainly in the disadvantaged vein group, they both actually had durable outcomes. A lot of us had questions about how durable outcomes for the ‘endo’ approach would be. And it should be clear that it is an approach, because sometimes touch-ups are needed on both sides and those are not considered MALE events. You really had to have a major reintervention to reach an endpoint of MALE, or an amputation. But I think that this for the first time shows that, in a head-to-head trial, that both are durable and that, on the ‘endo’ side, once you achieve successful technical outcome, it is comparable even in the group that had reasonable vein in cohort one.”
BEST-CLI meets “astronomic” need for high-quality, practice-changing data
At AHA, Farber noted that data from the Vascular Quality Initiative (VQI) from centres of excellence in North America revealed “tremendous” centre-specific variability in treatment strategy in the use of bypass versus endovascular for CLTI patients, which BEST-CLI national trial manager Michael Strong tells Vascular News attributes to the lack of evidence-backed guidelines in the space.
Speaking to this newspaper, the investigators express their confidence that the results of BEST-CLI will change practice and impact the Global Vascular Guidelines published in 2019. Menard believes there is “no question” that guidelines will change, partly because the current guidelines are “riddled with gaps”. He notes that anywhere from 10–15% of current guidelines are based on level one data—a “miserably low” figure in his opinion. “The need for quality data that the BEST-CLI represents is astronomic,” he says.
Rosenfield remarks that the trial will “definitely change practice” as it provides the clear message that “surgery is not dead, in fact it is very much alive and well for the appropriately selected patients”. He stated that the data “should be described to patients—simple as that,” and that patients “should have the option of deciding, but they should be knowledgeable that they will do better with surgery [in selected cases], and that is an appropriate response to [these results].”
Farber concurs, noting that there is now level one evidence to support the role of bypass in certain patients. “It supports a body of literature that is not as strong, and so I think [guidelines] will change,” he comments.
“I think it is nice for us to have all these arrows in our quiver to treat CLTI patients, and that is what this is; it is about saying this arrow does work and it should be used in some situations,” Farber summarises. “That is a great thing to add because, before BEST-CLI, the data were not as strong.”
“The first step”
While the investigators agree that BEST-CLI will be practice changing, they acknowledge that it represents “the first step” in a long trajectory of future investigations and discussions in CLTI research.
At AHA, Farber noted some limitations of the trial, including selection and operator bias in enrolment and intervention, the fact that equipoise and eligibility were determined locally and were variable, and that anatomic complexity is yet to be evaluated. In addition, cohort 2 was likely underpowered, anatomic complexity yet to be evaluated, percentage of female patients lower than targeted, and use of paclitaxel balloons or stents affected by the Katsanos meta-analysis during enrolment, they elaborate.
“We need to dig deeper,” Rosenfield says. He describes the trial as a “game-changer in many respects,” but stresses that “this field is still a moving target” and so BEST-CLI must be seen as “the first foray into developing very solid level one evidence”. Specifically, he notes that techniques will “continue to improve and get better”. Looking ahead, Rosenfield believes that those who treat CLTI will “learn a lot more over the course of the next couple of years as we peel back the layers of the onion”.
According to Menard, the trial stimulates two topics that will take centre stage in the “great discussions that are going to be had” in the coming months. “We are all trying to figure out exactly how we are going to interpret the results for our own practices, and in order to do that, you really need to understand the patients enrolled into the trial, and that is a big focus of the future work—defining what their anatomy was […] and a bit more about overall demographics. You can have selection bias, but you cannot imply or in any way get around the fact that at that institution they were deemed appropriate for both [open and endovascular strategies],” he tells Vascular News.
Farber stresses that further investigation might also elucidate how an operator decides between adopting an open or endovascular approach in certain patients. “We all know that if it is an easy ‘endo’, then of course the patient should have an ‘endo’, there is no equipoise, and then on the other extreme there are cases where everything is blocked from the groin to the foot and somebody might say of course surgery is the way to go, and then there is everything in between,” he says. What remains, according to Farber, is for the investigators and others in the field to “dig deep” into these data to answer the question of how to define appropriateness for a certain treatment.
For now, Rosenfield notes that the investigators are “really excited” about analysing the “treasure trove” of data that BEST-CLI provides and seeing what they can learn. Looking beyond this, Menard expresses the team’s hope that “many more trials will come along and build on what the trial has laid as a foundation”.
Two datasets presented during the late-breaking clinical trials session at The VEINS (Venous Endovascular Interventional Strategies) 2022 (30–31 October, Las Vegas, USA)—the latest results from CLOUT and a propensity score-matched analysis of CLOUT versus ATTRACT—bolster the evidence base for mechanical thrombectomy in the field of deep vein thrombosis (DVT) management. However, discussion at the meeting pointed to the need for further, high-quality data to solidify the role of this treatment modality.
The latest analysis from the now fully-enrolled CLOUT registry demonstrates the “excellent safety profile and effective thrombus removal” of mechanical thrombectomy with the ClotTriever system (Inari Medical) in a “real-world” DVT population of 500 patients. This is according to David Dexter (Sentara Vascular Specialists, Norfolk, USA), who presented in-hospital and 30-day outcomes from this multicentre, prospective registry at The VEINS 2022. Steven Abramowitz (MedStar Washington Hospital Center, Washington DC, USA) also presented data on the ClotTriever system, sharing results of a propensity score-matched analysis of early clinical outcomes from the CLOUT and ATTRACT studies.
The CLOUT (ClotTriever outcomes) registry is an all-comer, multicentre study evaluating patient outcomes following treatment of proximal, lower extremity DVT with the ClotTriever system, and, according to Dexter, represents the largest mechanical thrombectomy study in the field of DVT. All-comer patients were enrolled, irrespective of symptom duration, thrombus age, prior failed treatment of the current DVT, or bilateral disease. The primary endpoint was complete or near-complete (≥75%) thrombus removal, assessed by an independent core laboratory.
Dexter reported that the primary endpoint was achieved in 91.2% of limbs, and the 30-day device-related severe adverse event rate was 0.2%. Nearly all procedures were single session (99.4%), median estimated blood loss was low (40mL), and only 2.2% of patients received overnight post-thrombectomy intensive care unit monitoring, he added. Furthermore, patient symptoms (e.g. pain and oedema) were significantly reduced at discharge and showed sustained improvement through 30 days.
The presenter also revealed recovery of vessel flow and compressibility as measured by duplex ultrasound, improvements in revised Venous Clinical Severity Score and EuroQoL five dimensions quality-of-life score, median 5.5-point reduction in Villalta score, and <10% of patients with a moderate or severe Villalta score (≥10).
A question from the panel probed what is next for the field of mechanical thrombectomy in light of these results. Dexter pointed to the need for more studies, and also stressed what the focus of future research should be: “We need to show a real, long-term result on post-thrombotic syndrome”.
CLOUT versus ATTRACT
Steven Abramowitz at The VEINS 2022
In Abramowitz’s presentation of the propensity score-matched analysis, the presenter summarised that CLOUT patients showed better thrombus extraction and improvement in 30-day Villalta scores than ATTRACT patients. Specifically, the presenter revealed that nearly two times more CLOUT patients had complete thrombus removal, and that 13% fewer CLOUT patients had Villalta scores ≥5 at 30 days.
Abramowitz explained that ATTRACT is a reference trial evaluating interventional treatment for DVT that showed no added benefit compared to anticoagulation. “New interventions have emerged since the completion of ATTRACT, and their comparative effectiveness is unknown,” he said. Using propensity score-matched data, the investigators compared outcomes from the CLOUT registry with those from the treatment arm of the ATTRACT trial.
To adjust for differences in study design, patients with bilateral DVT, symptom duration >4 weeks, or incomplete case data were excluded. Propensity score matching (1:1) on 11 baseline covariates (age, sex, body mass index, sidedness, prior venous thromboembolism, race, symptom duration, DVT location, presence of provoked DVT, Villalta score, and Marder score) was performed between the remaining CLOUT and ATTRACT patients, resulting in 166 matched pairs.
No significant differences in baseline characteristics remained after matching, the presenter noted. Rates of stenting and venoplasty were similar between the groups and, as expected based on differences in mechanism of action, rates of thrombolytic use (0% vs. 100%, p<0.0001), single-session treatment (98.2% vs. 25.3%, p<0.0001), and postprocedural hospital overnights (mean, 1.7 vs. 3.4, p<0.0001) were significantly different.
Abramowitz reported that thrombus extraction as measured by core laboratory-assessed Marder scores was 22.3% better in CLOUT patients (p<0.0001), and 22.2% more CLOUT patients achieved ≥75% thrombus clearance (p<0.0001). Similarly, 12.7% fewer CLOUT patients had Villalta scores ≥5 at 30 days (p<0.05). Logistic regression on ATTRACT showed that 30-day Villalta scores significantly predicted post-thrombotic syndrome at six months, one year, and two years (odds ratios, 1.37, 1.32, and 1.43; p<0.0001), which the presenter said highlights the potential long-term effect of these differences.
Closing his presentation, Abramowitz echoed Dexter’s call for more data, noting that randomised controlled trials such as the recently announced DEFIANCE trial “will further clarify the role of the ClotTriever system in treating DVT”.
The first of four presentations was delivered by Rosario Grasso (Campus Biomedico University Hospital Foundation, Rome, Italy), who argued that percutaneous thermal ablation approaches like radiofrequency ablation (RFA) or cryoablation are an option for the management of patients with clinical-stage T1 renal lesions—primarily in masses <3cm in size, but potentially for larger masses in select patients too.
Grasso stated a belief that percutaneous ablation represents a safe and effective alternative to surgery in treating T1a renal cell carcinomas due to the “excellent” functional and technical outcomes seen with the procedure. The “very low” complication rate these procedures hold also compares favourably to those associated with nephrectomy, he added.
The speaker concluded that there is currently Level C evidence that, in selected patients with suspected T1a renal cell carcinoma, percutaneous thermal ablation should be offered over active surveillance owing to the “acceptable” long-term oncological and survival outcomes it has demonstrated to date. Grasso also said RFA, cryoablation and microwave ablation are all appropriate treatment modalities, and claimed that the choice of ablation method “should be left to the discretion of the operating physician”.
Treatment planning
Arian van Erkel (Leiden University Medical Center, Leiden, The Netherlands) followed this by discussing treatment planning in renal ablation—a “well-established” treatment for small T1a tumours. He posited that the first step here is to choose between surgery, ablation or active surveillance, and that this decision is an individualised one influenced by patient preference, age and life expectancy, renal function, the location and size of the tumour, and multiple other factors.
“Planning the treatment of your RFA is very important in getting complete ablation, with a sufficient margin, and in avoiding complications,” van Erkel asserted. “This planning involves image guidance, the ablation modality and protective measures.” He further claimed that axial diameter, bowel proximity, adjacency to the ureter, and several other characteristics of the tumour, should be taken into account.
“An immediate CT [computed tomography] after ablation is, of course, important, to evaluate your complications and your ablation margins especially,” van Erkel concluded. “And, there is software on the market that can help you make these estimations in a more scientific and exact way.”
Different modalities
A closer look at the different approaches to percutaneous ablation for renal cell carcinoma was then provided by Esther Gálvez González (Hospital Severo Ochoa, Madrid, Spain). The speaker corroborated many of her colleagues’ earlier points, noting that ablative treatment is as effective as surgery in T1a tumours—adding that it can also help to preserve renal function, and is associated with low complication rates.
Gálvez González further asserted that a key advantage held by RFA is the wealth of experience and high volume of published papers associated with the technique, but also noted two important limitations: thermal tissue conductivity and the ‘heat sink effect’. In contrast, she continued, bigger tumours can be ablated more quickly, and at higher temperatures, with microwave ablation, while its relative insensitivity to the heat sink effect allows it to be used in target areas located closer to larger blood vessels. The major limitation of microwave ablation, however, is the increased risk of complications in more central locations, which restricts its use to peripheral lesions, she added.
The speaker also touched on the various advantages and limitations of two other approaches—cryoablation, and a non-thermal technique (on which there are minimal published data) called irreversible electroporation—stating that both are essentially unaffected by impedance and the heat sink effect, but are limited by smaller ablation volumes and longer procedure times as well. Gálvez González concluded by asserting the importance of selecting the correct approach based primarily on the size and location of the target tumour.
Combined therapies
The session’s final talk was given by Marco van Strijen (St Antonius Hospital, Nieuwegein, The Netherlands), who outlined several combined treatments in cryoablation. “Combined treatment in renal cryoablation, in my opinion, consists of either embolization—which is a safe treatment but for which scarce literature is available—or thermoprotection by liquid; air or CO2 dissection; or pyeloperfusion,” he stated. Homing in on the former technique, the speaker said that, despite the limitations around previous studies and a lack of prospective data, percutaneous embolization is considered a safe procedure that is “most effective” in reducing periprocedural blood loss, and holds potential benefits in local tumour control and procedural visibility.
Van Strijen went on to highlight two further, more recently introduced tools that he also considers among the options for combined approaches: robotic needle placement, and the use of integrated controls and augmented reality to perform ablations virtually with the aid of a HoloLens device (Microsoft). In concluding his presentation, van Strijen added: “Robotic needle placement is currently one of my favourite techniques.” Here, he cited the fact it is “very simple”, and enables steep angulations, as well as reducing radiation exposure and speeding up the procedure “considerably”.
Concept Medical has announced the successful completion of enrolment for the SIRONA randomised controlled trial (RCT) investigating the use of its Magic Touch PTA sirolimus drug-coated balloon (DCB) versus paclitaxel DCB angioplasty for the treatment of peripheral artery disease in the femoropopliteal vessel segment.
The prospective, multicentre, head-to-head, corelab adjudicated RCT enrolled a total of 480 patients across 28 sites in Germany and Austria. The target patient was enrolled on September 23, at Hanusch Hospital Vienna (Vienna, Austria) by principal investigator (PI) Martin Werner and team.
Coordinating principal investigator, Ulf Teichgräber, said: “I am thrilled to work with 28 highly dedicated and motivated study sites that have managed to complete enrolment much earlier than expected. SIRONA represents a breakthrough head-to-head RCT with the potential to usher in a new era of sirolimus DCB in peripheral arterial disease (PAD) to replace an old technology.”
SIRONA will be a game changer trial, considering its bold design and the direct comparison against paclitaxel, say Concept Medical. The trial enrolled all patients with a disease in the superficial femoral artery (SFA) segment, whether de-novo or restenotic, falling into Rutherford classes 2–4, and experiencing intermittent claudication to critical limb ischaemia (CLI).
The 12 month results will feature patency (defined as the absence of target lesion revascularisation (TLR) or restenosis), and the primary safety endpoint is assessed as the composite of freedom from device or procedure-related death at 12 months as well as major target limb amputation.
The University Heart Center (Bad Krozingen, Germany) topped the enrolment under the lead of Thomas Zeller.
“It is exciting that enrolments into the first head-to-head comparative study between a sirolimus coated DCB and a variety of marketed paclitaxel coated DCB for femoropopliteal indication could be finished in such a short time”, said Zeller. “The study has sufficient size and the power to demonstrate if there is at least equivalent performance between the Magic Touch DCB and a range of paclitaxel coated DCB and if so, if there are potential lesions which may even benefit from the use of a sirolimus coated DCB,” he added.
Magic Touch PTA has already been granted a breakthrough device designation by the US FDA for below-the-knee indication.
Gerd Grözinger (Tübingen, Germany) chats with Bernhard Gebauer (Berlin, Germany) at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain) about some of the difficulties associated with treating patients with pulmonary embolism (PE) and deep vein thrombosis (DVT). Gebauer states that “the options we have at the moment with either anticoagulation or lysis are very limited”. One of the problems with systemic thrombolysis for example, explains Gebauer, is that “you could have some complications” with the high dose, in addition to the fact that lysis “is contraindicated in a lot of patients”.
Grözinger agrees with Gebauer that the age of the thrombus is very important. Asked about the perfect time window to treat those with DVT, Grözinger states that “in the old days we had to tell our patients that beyond two to four weeks there is no chance of getting rid of the clot”. However, “this strict timeframe can be overcome with new technology like the ClotTriever (Inari Medical) which can address thrombus of various ages” and ultimately “extend our treatment window”, he adds. The pair conclude by discussing which patients benefit most from interventional treatment for DVT or PE.
Synchron has announced that enrolment in the COMMAND trial has commenced at the University of Pittsburgh in Pittsburgh, USA.
The COMMAND trial is an early feasibility study funded by the National Institutes of Health (NIH) that will primarily assess safety while beginning to explore quantified efficacy measures of Synchron’s brain-computer interface (BCI) technology—the Stentrode—in severe paralysis patients, with the goal of enabling them to control digital devices, hands-free.
COMMAND is being conducted under what Synchron claims is the first investigational device exemption (IDE) awarded by the US Food and Drug Administration (FDA) to a company assessing a permanently implanted BCI. This new site at the University of Pittsburgh marks the second approved COMMAND trial location, joining Mount Sinai in New York, USA, where patients are also currently being enrolled, a company press release notes.
“Synchron’s Stentrode has the potential to restore functionality to the millions of people worldwide suffering from paralysis,” said Raul Nogueira, director of the University of Pittsburgh Medical Center (UPMC) Stroke Institute. “Giving patients the option to receive this device without the need for open brain surgery may open endless possibilities into the application and scalability of this promising technology.”
“This exciting technology may open up the possibility for patients with paralysis to use digital devices to communicate with loved ones again, and restore independence back into their lives,” said David Lacomis, COMMAND principal investigator and chief of the University of Pittsburgh’s Neuromuscular Division. “Something as simple as surfing the web or doing online grocery shopping can seem mundane to some, but it can change the world for someone who previously had those fundamental abilities taken away.”
The Stentrode is implanted within the motor cortex of the brain via the jugular vein in a minimally invasive endovascular procedure. Once implanted, it detects and wirelessly transmits motor intent, restoring a capability for severely paralysed patients to control personal devices hands-free with ‘point-and-click’. COMMAND will assess the Stentrode’s impact on tasks like texting, emailing, online shopping and telehealth services. The US FDA granted Breakthrough Device designation to Synchron in August 2020 and an IDE in July 2021 for this trial.
“Today marks an important milestone in our mission to advance technology access for the millions of people who have lost the ability to use digital devices,” said Tom Oxley, CEO and founder of Synchron. “We are excited to expand the COMMAND trial with enrolment at the University [of Pittsburgh] as we look to advance a scalable BCI solution to market.”
Transit Scientific has announced that the XO RX 2.2Fr and XO RX 3.8Fr platform has received US Food and Drug Administration (FDA) clearance to crack, break and dilate stenoses in peripheral arteries and arteriovenous dialysis fistula-associated lesions.
“We have demonstrated XO’s rotating strut technology can crack, break, and dilate intimal and medial calcium,” said Jihad Mustapha (Advanced Cardiac and Vascular Centers for Amputation Prevention, Grand Rapids, USA). “The new 3.8Fr XO RX has a low profile and accommodates 20cm balloons, making it a good option for PAD [peripheral arterial disease] and CLI [critical limb ischaemia] disease. The lower-profile 2Fr version helps address gaps in treatment options currently available for BTK [below-the-knee], tibiopedal and pedal loop stenoses.”
XO RX and XO OTW (over-the-wire) exoskeleton devices include up to 22 rotating struts that slide onto a broad range of off-the-shelf angioplasty balloons, according to a press release from Transit. During balloon inflation, the struts rotate 90 degrees to crack, break and dilate calcified stenotic atherosclerotic lesions, and intimal hyperplastic lesions, and can be used for vessel prep for other treatment options.
“We have seen good results in PTA [percutaneous transluminal angioplasty]-resistant intimal hyperplastic and elastic venous lesions in patients with dialysis fistulas with the XO at low nominal or near-nominal pressures,” said Richard Saxon (Tri-City Medical, San Diego, USA). “The new XO RX presents a unique and versatile option for prepping and dilating longer lesion types in patients with severe PAD during limb salvage procedures.”
The XO RX and XO OTW technology is designed to reduce shear and facilitate balloon rewrap by counter-rotating 90 degrees upon deflation. Clinicians can deliver fluids from the hub to the balloon before, during or after inflation with XO OTW. No consoles, new capital equipment, or complex learning curve are required, the release adds.
“The XO RX platform sets new standards for low-profile, flexibility and performance,” said Jennifer Arnold, Transit’s chief operating officer. “Patients and clinicians need more tools to crack, break and dilate occlusive lesions in patients with cardiovascular disease. XO RX allows clinicians to add XO technology to hundreds of angioplasty balloons covering a wide range of diameters and lengths with just a few SKUs [stock-keeping units].”
The XO RX PTA system is intended to be used in conjunction with a PTA balloon to facilitate dilation and apposition of the scoring surface to the stenotic material in the iliac, femoral, ilio-femoral, popliteal, infra-popliteal, and renal arteries, and for treatment of obstructive lesions of native or synthetic arteriovenous dialysis fistulas. However, it is not for use in the coronary or neuro vasculature, according to Transit.
XO RX is available in 2.2Fr and 3.8Fr sizes, which accommodate 1.5–7mm outer diameter standard PTA balloons of lengths from 20–200mm, reducing inventory requirements, the release also notes.
Matthew Gibson (Royal Berkshire Hospital, Reading, UK) will be delivering this year’s British Society of Interventional Radiology (BSIR; 2–4 November, Glasgow, UK) Wattie Fletcher Lecture ‘Survive and thrive in interventional radiology [IR]’. Interventional News spoke with Gibson to glean some of the details of his talk, in which he will address the “psychological and non-medical stresses and strains of being an interventional radiologist and even suggest some things we can do to improve the situation.”
From Gibson’s preview, it would appear that he intends to underline in the lecture how “just trying to get through to the next day is not enough” as an interventional radiologist. A self-professed enthusiast who, from personal experience, knows the value of enjoyment and laughter at work, Gibson makes a compelling case for thriving over mere survival in IR.
“I have an interest in several areas of IR, for example below-the-knee angioplasty, dialysis access, and deep venous intervention but I am sure there are plenty of people better qualified than me to talk on these topics,” Gibson begins, talking through how he chose his lecture topic. He wanted to make it relevant and interesting to a wide audience. In a career of 25 years as a consultant interventional radiologist, he has “retained his enthusiasm for the job and IR in general”. This has surprised his contemporaries and younger colleagues, who have seen stress and burnout lay claim to many medical professionals’ enjoyment of their job. He felt he was well placed to produce a talk on the all-too-common stresses of IR, rather than a more specific procedure or medical talk about a certain area of IR.
Before delving into burnout and the many contributing factors that make this a reality for many interventional radiologists, Gibson states his keenness to work discussion of serious adverse events (SAEs) into his lecture. Namely, he expresses a desire to examine beyond the important impact of SAEs on the patient’s safety: the effect involvement in a SAE can have on medical professionals. “It is something we do not talk about enough, but SAEs produce a definite adverse effect on medical staff”. This can result in, according to Gibson, damage to confidence and self-esteem and anxiety about making another mistake and, he adds, “you are more likely to be involved in another adverse event if you have already had one.”
“Death by 1,000 arrows” is the metaphor Gibson uses to characterise how the UK healthcare system investigates adverse events. “Although it is supposed to be a no-blame medical culture, being under investigation at any level can be damaging and upsetting. Anyone can refer a doctor to the General Medical Council [GMC], which can be extremely stressful,” Gibson relays, emphasising that doctors have taken their own lives after being referred.
Opening the issue of stress and burnout back up, Gibson again suggests that “[he does] not think we have talked about it enough in IR”, suggesting that this “[may be because] some of us think we are immune to it.” However, “we are all at risk”, he counters, moving on to list multiple explanations for this. Paperwork, emails, directly looking after our own patients”, work-life balance and “time poverty”. In addition, the public’s attitude plays a role, Gibson notes—“the medical profession is less respected than previously and patients and relatives may not understand the subtleties of why mistakes occur and the effect making mistakes, and being the subject of complaints, can have on the medical staff involved.”
In addition, lack of professionalism and rudeness at work “can make your IR team dysfunctional and negatively impact on patient care”.
Yet, there are positive steps that can be taken to mitigate the strain of working in modern medicine and IR, Gibson points out. “Governments, employing organisations, managers, interventional radiologists and their team members can take steps to redress work-life imbalance, time poverty, improve resilience and, hopefully, reduce the risk of burnout and also improve patient safety.”
Interventional radiologists would also stand to gain from understanding that “being vulnerable is not a weakness,” Gibson advises, labelling this as “a real issue for us—we are expected to be invulnerable, to ride into high-stress situations and know what to do with no doubt in our mind.” Be this as it may, “you probably also need to be vulnerable at times in order to have a caring, empathetic relationship with your patients,” Gibson admits, elaborating on the importance of “shedding this armour”. Being invulnerable also “spills over into your private life—doctors can have issues with depersonalisation and desensitisation and thus cut themselves off from their loved ones.”
“Having a laugh with staff and patients might seem frivolous because medicine is a serious business, but it can have some very positive effects,” Gibson offers as part of the explanation for his having staved off burnout 30 years into his IR career.
“I cannot pretend that I have all the answers but stress and burnout are very much with us now and are probably only going to get worse.” This is what he expects the BSIR’s first survey into burnout among interventional radiologists to show and is why “it can be quite difficult to convince junior doctors or medical students how much of a privilege it is to care for patients.” Such, Gibson says, is his “humble opinion”, but he is convincing in how he conveys a need to address the issues that will form the basis for his lecture.
Above: Roger Greenhalgh, Tilo Kölbel, Markus Steinbauer, Heinz Jakob; Below: Jans Heyligers, Michele Antonello
Above: Roger Greenhalgh, Tilo Kölbel, Markus Steinbauer, Heinz Jakob; Below: Jans Heyligers, Michele Antonello
The second day of the CX Aortic Vienna 2022 Digital Edition (24–26 October) saw presentations on dynamic computed tomography angiography (CTA), a device with the potential to bring hologram guidance to vascular procedures and an edited case highlighting the role of intravascular ultrasound (IVUS) intraoperatively in thoracoabdominal branched endovascular aneurysm repair (BEVAR). The multidisciplinary moderating panel, which included a cardiac viewpoint from Heinz Jakob (Essen, Germany), questioned these technological developments for imaging in the post-presentation discussions—in terms of the limited access to them for cost reasons, and whether the reduction in radiation exposure the technologies offer can justify hospitals assuming the financial burden.
The first presentation came from Alan Lumsden (Houston, USA), who demonstrated why dynamic CT imaging might be considered the “new gold standard” for diagnosis and interventional planning. “It is obviously important to choose the right diagnostic tool at the right phase of the treatment modality,” the presenter began, declaring CT as a “very flexible” modality. This means that it can lend itself to dynamic imaging, Lumsden explained—static imaging and the single “view” it offers is sometimes akin to “no view” at all.
Lumsden then detailed how and why time-resolved CTA, developed for cardiac imaging, can be advantageous for use in endovascular aneurysm repair (EVAR) follow-up. The approach involves “moving the patient in and out the scanner, taking snapshots”, which can then be “put together” to form a three-dimensional composite image over time, Lumsden relayed, likening it to a “movie”. This allows the surgeon to see the contrast dye’s flow pattern and how long it takes to “arrive”, meaning “you can work out what type of endoleak you have.”
Furthermore, the presenter asserted that there is no radiation exposure increase as compared to triphasic CTA. His concluding remarks were that dynamic CTA can be applied to “guide subsequent interventions” and can be “widely performed on conventional scanners”.
It was whether this imaging approach can, in fact, be “widely performed” that featured in the discussion that followed. Moderator Markus Steinbauer (Regensburg, Germany) acknowledged its potential as a “valuable tool”, but that he does not currently have access to it in his practice. Anchor Roger Greenhalgh (London, UK) concurred—“we encourage the concept, but it needs to be more widespread”.
Another point the discussion raised was whether the reduced radiation exposure facilitated by dynamic CTA warrants shouldering the financial cost of implementing the requisite technology. For this reason, moderator Tilo Kölbel (Hamburg, Germany) posited that it would “take a while until this is standard practice”.
The result from the interactive audience poll suggested that dynamic CTA could indeed become the gold standard for diagnosis and interventional planning, with 88% of respondents voting in the affirmative.
The edited case presented by Michele Antonello (Padua, Italy), which shed light on intraoperative intravascular ultrasound (IVUS) in thoracoabdominal branched endovascular aneurysm repair (BEVAR), also yielded noteworthy discussion. Fellow presenter Jan Heyligers (Tilburg, The Netherlands) again posed a question on radiation exposure to Antonello—“is it mainly a reduction of radiation that you are aiming at?”—to which the response was that IVUS can “reduce contrast [use] by 30%”. Kölbel queried the impact IVUS has on procedure time, highlighting that this is also a factor when evaluating the cost-effectiveness of the approach as compared to the standard of care.
Heyligers’ own presentation demonstrated the scope for holographic augmented superposition of patient-specific imaging. The device in question, Heyligers suggested, could, with further development, solve the “problem” in vascular surgery of having to interpret three-dimensional information from a two-dimensional display. With smart glasses projecting directly onto the exact location on the patient, Heyligers shared with delegates that thus far, the technology has proved promising in static applications such as in a foot or wrist. Future iterations will be “smarter”, and capable of assisting in a “moving environment”, such as the vasculature, the presenter ventured.
Once more, the hologram technology elicited lively discussion, with Kölbel keen to hear how this could work in endovascular procedures. Heyligers underlined that other technologies could be harnessed “once inside vessels”, reiterating that the holographic capability to “recognise patient-specific surroundings” can help fulfil the “ambition” to have “faster, more precise” procedures, with “less radiation”.
Steinbauer pointed to the potential for applying the technology in educational settings, such as to project guidelines onto a patient to show where and where not to operate. This was an idea with which Heyligers agreed— a “remote experience” is possible, he added, thanks to the device’s internet connectivity, which could allow a seasoned surgeon “to help younger colleagues out” even if they are not in the room.
The thread running through this session on thoracic imaging was that practising at the forefront technological and procedural advancements in vascular surgery does not come without significant financial cost, ultimately constituting a barrier to entry for many centres. The moderating panel emphasised that radiation reduction is a priority when considering whether or not to implement a new procedure and shoulder the cost of the technology required to perform it.
“The spine is an area where interventional radiologists play a crucial role in both diagnosis and therapeutic management of a variety of pathologies”.
Dimitrios Filippiadis is associate professor of diagnostic and interventional radiology (IR) at the National and Kapodistrian University of Athens (Athens, Greece) whose practice centres around musculoskeletal (MSK) interventions and diagnostics, and interventional oncology (IO) and cancer pain management. Beyond this, he is passionate about IR education, which has seen him, this year, take up the position of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Online Education Committee chair. From his research on discomanometry, to personal experience at the forefront of adopting ablation procedures within Greece, Filippiadis speaks to Interventional News about the “intrinsic rewards” and “lifelong memories” that being an interventional radiologist has given him in his decorated career thus far.
What attracted you to a career in IR?
When I started my residency in diagnostic radiology, I had a lot of second thoughts about sitting in front of a computer monitor dictating reports. Then, a fellow resident came to me and suggested I register for a postgraduate course in IR, which was organised by Professor Dimitrios Kelekis in Greece. From the introductory courses onwards, I knew that this was the clinical career path I wanted to follow. Some years later, a visit to Strasbourg on a CIRSE grant made me realise that interventional oncology (IO) and pain management would be my specialist practice.
Who are, or were, your mentors?
I was fortunate enough to have had wonderful mentors early on in, and throughout, my career. During my residency, Alexis Kelekis introduced me to spinal and MSK procedures and influenced me greatly. Elias Brountzos taught me that providing patient care is one aspect of our work, with the other being to bolster the IR community by volunteering our time and expertise to help our specialty to flourish further. Nikolaos Kelekis gave me the opportunity to work almost exclusively in the field of ablation and I will always be grateful to him for this chance. Last but not least, even though I have never worked with him, Loukas Thanos, a Greek pioneer in the field of ablation, has had a great influence on my career.
Could you describe a particularly memorable case of yours?
I will never forget the first time I treated a paediatric cancer patient. He was 16 years old with a history of right paraganglioma and right nephrectomy due to renal cell carcinoma (RCC) and presented with an endophytic RCC lesion in the lower pole of his left kidney. The stress obtaining the parents’ consent and preparing for the ablation was unbearable, at least for me. The night before the ablation, I was not able to sleep, imagining only the worst-case scenario. However, after the procedure, when I informed the parents that everything had run smoothly, that we had totally ablated the tumour without any adverse events, they started crying. It is a moment I will never forget.
What led you to pursue your PhD in quantitative discomanometry? How is it complementary/relevant to your role as an interventional radiologist?
The spine is an area where interventional radiologists play a crucial role in both diagnosis and therapeutic management of a variety of pathologies. Specifically for intervertebral disc herniation, what I have always found fascinating is the fact that the success rate of percutaneous decompression techniques is around 80% no matter which technique you use. Discomanometry could serve as a diagnostic tool to escalate patients, leading to an improved patient-specific, or even better, hernia-specific, approach.
Your paper on pain management in cancer patients, recently published in Current Oncology Reports, is one of many you have authored on the subject—what innovations do you see on the horizon in this area?
Management of cancer pain is one of the most interesting topics in my everyday clinical practice. We have published numerous papers on the topic, but myself and the rest of the co-authors are actually particularly proud of this publication, which has been included in the National Comprehensive Cancer Network 2021 guidelines for adult cancer pain. As far as innovations in the field of pain management are concerned, I am convinced that cryoneurolysis is the ideal technique for pain palliation, as it offers more confined and more organised nerve regeneration alongside pain reduction. Although, at present, there is no standardised ablation protocol, given the wide range of variables that affect intraprocedural temperature at the ablation site, a more palatable solution will be a new device with information-gathering capabilities, to form and perform individual cryoneurolysis protocols.
You were appointed to the position of associate professor of diagnostic and interventional radiology at the National University of Athens Medical School—what has changed the most about your practice since your early senior consultant days over a decade ago?
Being an educator offers intrinsic rewards and brings with it lifelong memories. Providing real-life clinical experiences and context to medical students is an essential part of today’s medical education—whereas I had only very minimal obligations towards medical students and teaching when I started as a senior consultant. Integrating the role of medical students into the healthcare system provides added value, both to clinical care and medical education. You need to change your workflow in order to allow students to contribute before, during, and after visits, and to engage them holistically in patient care. Last but not least, you need to strike a balance between apprenticeship and an academic model, and choose which approach works best for whom.
You were at the forefront, at your centre, when it came to integrating microwave and navigation-guided ablation into IR services, yours being the first in Greece to adopt both procedures—why do you think it is important to lead the charge in adopting new techniques and procedures?
New techniques and procedures go hand in hand with IR, which is a discipline born of innovation; adopting new technologies is essential for the growth and flourishing of our specialty. Early adoption results in improved efficacy, ability to offer what no one is offering at the moment, and empowering practice with new and improved systems that make for better services. From our first experience with microwaves in 2008 to today, it has been evident for us that this technology offers unique advantages and has a role in today’s ablation practice. Ideally, when it comes to locoregional therapies, we want to have all the ablation techniques available in our armoury and to be able to take a lesion-tailored approach. Application of navigation tools as well as simulation and verification software significantly contribute to standardisation of ablation; I strongly believe that in the near future, these tools and software will be part of all interventional radiologists’ everyday practice. The tools will prove their value by allowing for better comparison of percutaneous ablation to surgical and radiation oncology.
In (also) becoming the first Greek hospital to enrol in the International Accreditation System for Interventional Oncology Services (IASIOS), what has the impact on your practice and patients been?
Even though the second department of radiology is in the process of acquiring the IASIOS accreditation, the benefits for patients and in terms of practice performance are more than evident. The whole process of patient care and treatment is improved. During the IASIOS accreditation process, we have analysed our service, improved its coordination and monitoring, and the end result is improved delivery of high-quality IO care, with the patient receiving the best possible treatment for an optimal, individual clinical outcome. This improvement has been throughout the department, affecting not only IO but all IR services.
You recently became the CIRSE Online Education Committee chairperson—what do you hope to do in this role that has not been done before?
Education extends beyond practical knowledge. Educated physicians develop thinking and skills, which help them make good decisions for the benefit of the patients. The Online Education Committee deals with the CIRSE Library, Academy and Webinars as well as with everything included in these three main pillars of virtual and online education provided by our scientific society. To leave your own footprint on this position I must admit is a very difficult task, since my predecessor Stefan Müller-Hülsbeck has done a superb job in organising almost everything from scratch. I am positive though, that along with my deputy chairperson Julien Garnon and all the members of the Committee, we will rise to the challenge and structure education in order to foster a love of learning among our IR community.
What are your hobbies and interests outside of medicine?
Before and during my medical studies, I worked as a DJ. What I have left from these days and nights are thousands of vinyl records and CDs of all kinds of music, which I love listening to in my free time. Apart from listening to music, I love reading books, especially historical novels (Bernard Cornwell, Wilbur Smith and Ken Follett are my favourite authors). My other main hobbies are playing basketball and swimming, especially on my beloved island of Lefkada where we have a beach house.
1-3) Preoperative CT scan views. The lateral left lung lesion is clearly visible; 4) Definition of the planned needle path. The red contour corresponds to the borders of the segmented lesion; 5) Alignment of Micromate to the planned needle path under live imaging; 6) Insertion of the biopsy needle through the guidance needle and tissue harvesting.
This advertorial is sponsored by Interventional Systems.
Marco van Strijen
Marco van Strijen is an interventional radiologist at St Antonius Ziekenhuis (Nieuwegein, The Netherlands) who specialises in non-vascular interventions and interventional oncology. Image-guided procedures feature heavily in his practice, Van Strijen tells Interventional News, enabling him to “[draw] needle paths, [define] targets and [introduce] needles”. Micromate(Interventional Systems) provides robotic assistance for these tasks, Van Strijen reports, detailing how “it is three years that we have been using Micromate”, following on from a successful stint with the early prototype that “functioned so well” that “the rest was history”.
On how Micromate fulfils its role within his practice, Van Strijen begins by acknowledging that for any percutaneous biopsy “it is very important to have a stable needle”, and therefore, “a device that helps you keep the needle stable while advancing the device through the skin to the desired target,” such as Micromate does, is valuable. “This is especially true in […] areas where there is not that much overlying skin or soft tissue [to] hold your needle while you are trying to centre it in the direction of your target,” Van Strijen adds, before exemplifying how unwieldy some of the former approaches to intraprocedural needle stabilisation were: “we were using our own hands, sterile towels draped around the needle insertion point, or sterile forceps, making adjustments until we had the needle in a holding position, but these were not that stable, especially when you have a patient who is still breathing or maybe even starts to move because of their discomfort on the table: you always have the risk of dislodging the needle.”
Van Strijen then enumerates the precise advantages of having a completely stable needle, as achieved with Micromate—“not only will it help in reducing the number of [needle] re-positionings, but it reduces the need for imaging, as you can advance the needle as quickly as possible. And this is [of…] benefit in reducing the amount of radiation, not only for the patient but also for yourself as the operator.” Furthermore, Van Strijen speaks of the procedural time reduction that this results in, and, consequently, the discomfort the patient is subjected to on the table.
In a particular case of Van Strijen’s—that of a percutaneous lung biopsy close to the pleura in a 52-year-old patient referred with suspected rectal carcinoma—in which Micromate was used under live imaging, the procedure time was 43% faster than previously reported, Interventional Systems states. The radiation level decrease measured 70%. Greater needle stability facilitates greater procedural accuracy, which, Van Strijen shares, makes “[working] in areas that rely on needles being positioned to millimetre or sub-millimetre accuracy” possible. For example, this could be “in the vicinity of critical structures such as the neck or the face or close to the major vessels of the thorax”. Van Strijen asserts that “this is where this type of robotic device comes in very handy.”
1-3) Preoperative CT scan views. The lateral left lung lesion is clearly visible; 4) Definition of the planned needle path. The red contour corresponds to the borders of the segmented lesion; 5) Alignment of Micromate to the planned needle path under live imaging; 6) Insertion of the biopsy needle through the guidance needle and tissue harvesting.
To the question posed by Interventional News of how Micromate reduces complications in lung biopsy cases, such as the aforementioned, Van Strijen states that “a quick in-and-out is the ideal strategy”, and with Micromate, the biopsy is possible “during one single breath-hold”. The incidence of pneumothoraces, which Van Strijen notes is the “most encountered complication in this procedure”, is “[reduced] significantly” by virtue of being able to avoid unnecessary pleura punctures. Where the needle is less stable, the necessary multiple attempts and sometimes, leaving the needle in, can cause tears in the pleura, Van Strijen explains.
Micromate may be responsible for something akin to his team becoming victims of their own success, Van Strijen then admits—”I think that by having this type of technology available, we are challenged quite a bit by our referring clinicians who are asking for more and more challenging lesions to be biopsied.” In practice this means “trying to get histology from a lesion of just a few millimetres,” in contrast to a decade ago, when, Van Strijen says “a two- or three-centimetre lesion was common”.
Likewise, because of the development of robotic technology, Van Strijen now carries out biopsies “next to very challenging structures—close to major vessels, close to the beating heart”.
Van Strijen is also keen to mention a further advantage of Micromate and the impact it has in his teaching hospital. “This type of device should be very easy to use, one that any user immediately understands without a lot of training—after only one or two demo cases,” he opines. And, with Micromate satisfying such an expectation, Van Strijen sees it as “[bridging] the gap between inexperienced and experienced users […] Young doctors are challenged in trying to perform the same procedures as their tutors,” but, as Van Strijen informs Interventional News, “one of the things I find very helpful [about Micromate]” is how doctors of different levels of experience can use it successfully.”
In the USA, atherectomy use in peripheral vascular interventions (PVIs) “more than doubled” from 2010 to 2019, with office-based procedures a “major driver” of this increase. This is according to published US data from the Vascular Quality Initiative (VQI), which also revealed wide regional variability in the use of atherectomy.
According to authors Tonga Nfor (Aurora St Luke’s Medical Center, Milwaukee, USA) and colleagues, small, older studies have indicated that the use of atherectomy devices has become common in PVIs despite what they describe as the “paucity of strong clinical guidelines”.
The study, published in the Journal of Vascular Surgery (JVS), was a retrospective analysis of prospectively collected data from the VQI registry, which the investigators say provides a “unique opportunity” to fill knowledge gaps in this field of research using “real-world” data originating from across the USA. The team identified all patients who had undergone endovascular PVIs for occlusive lower-extremity arterial disease from 2010 to 2019. Procedures in which an atherectomy device had been used as the primary or secondary device were classified as the atherectomy group, Nfor et al write.
In the study period, the authors note that 205,377 PVIs were performed for 152,693 unique patients. They report in JVS is that, during the 10-year study period, 16.6% of the PVIs had used atherectomy, with the data showing that use “significantly increased” from 8.5% in 2010 to 19.7% in 2019.
Geographic variation was evident in the study results, with Nfor and colleagues stating that they found a significant difference in the prevalence of atherectomy use across 17 geographic regions, ranging from 8.2% to 29%. These regions were further split into North, East, South, and West, the authors write, revealing that the observed frequency of atherectomy use in PVIs during the 10-year period was highest in the South at 22.5%, followed by the West (19.9%), North (17.3%), and East (12.6%; p<0.0001).
The 10-year VQI data also clarified predictors of atherectomy use. According to the study authors, the strongest predictor of use was performance of PVI in an office setting (odds ratio [OR], 10.08; 95% confidence interval [CI], 9.17–11.09) or ambulatory centre (OR, 4; 95% CI, 3.65–4.39) versus a hospital setting. Furthermore, the geographic trend in atherectomy use followed the distribution of the proportion of office-based PVI procedures—South (6.1%), followed by the West (4%), North (3.9%), and East (0.5%).
They note that the presence of severe (OR, 2.6; 95% CI, 2.4–2.85) or moderate (OR, 1.5; 95% CI, 1.4–1.69) lesion calcification was also predictive of atherectomy use, as well as some other factors including elective status, insurance provider, lesion length, prior PVI, claudication symptoms, and diabetes mellitus.
The researchers also examined the reimbursement aspect of the atherectomy discussion, highlighting differences in compensation levels for hospital-based versus office-based procedures, and for angioplasty versus angioplasty with atherectomy. For angioplasty performed in a hospital, the physician total relative value units (RVU) was 12.94, averaging about US$466, they report. For the same procedure performed in an office-based laboratory [OBL], the total RVU was 100.68 (procedure total), translating to US$3,628. Nfor et al further reveal that, when angioplasty was performed with atherectomy in a hospital, the physician RVU was 17.61, averaging US$635. However, when atherectomy with angioplasty was performed in an OBL, the reimbursement increased to 345 RVU— approximately US$12,444. The authors, however, point out that these total RVU reimbursement figures for office and ambulatory centre procedures includes the technical and facility fees.
“To provide patients with the highest quality of care, physicians must allow their decision-making to be guided only by the clinical factors and the best interest of the patient, and should be mindful of any biases that might influence their practice, including the reimbursement structure and financial incentives,” the researchers stress.
Despite the financial incentives that exist, the authors acknowledge that clinical considerations “play an important role in interventional decisions that guide patient care”. For example, they note that patients in the hospital setting will tend to have more acute disease with greater urgency and a greater risk of complications. “It follows naturally that operators might want to avoid long, complicated procedures that will subject patients to more risk, which might partly explain the lower use of atherectomy,” the investigators remark.
There are a number of limitations to the present study which the authors address in their discussion. For example, while the VQI database offers researchers a “large sample of patients from multiple regions,” they acknowledge that a selection bias could still occur because the nature of the database is “dynamic” and different centres were added cumulatively over time.
Despite this and other drawbacks, Nfor and colleagues claim that, to the best of their knowledge, the present study was “the largest to investigate specific clinical and non-clinical predictors of atherectomy use and also to examine the trend and geographic distribution”.
Routine use of atherectomy for infrainguinal PVI called into question
Caitlin Hicks
In a commentary on Nfor and colleagues’ report, Caitlin Hicks (Johns Hopkins University School of Medicine, Baltimore, USA) underscores the “overwhelming message” of the analysis: that atherectomy is being overused in the USA.
“This is not an attack on physicians who work in OBLs,” Hicks stresses at the outset of her commentary—titled ‘Atherectomy overuse is a real problem’—but rather a “statement of the facts,” of which she assembles four from this latest addition to the available research:
Atherectomy use for infrainguinal PVI has been “increasing rapidly” in the USA
No high-quality evidence that atherectomy improves outcomes compared with alternative endovascular therapies is available
Atherectomy is much more frequently used in OBL settings than in hospital-based settings
Reimbursement for atherectomy procedures is substantially higher than that for stenting and balloon angioplasty in the outpatient setting
“Based on these facts, the routine use of atherectomy for infrainguinal PVI is suspicious at best,” Hicks remarks. She acknowledges that cases exist for which atherectomy has proven beneficial—calcific disease, popliteal lesions that cannot or should not be stented, and recalcitrant lesions, for example. However, Hicks also notes that the data have shown the use of atherectomy in up to 100% of cases by some physicians—a fact that is “not right” in her view.
Hicks concludes: “As a field, vascular surgeons need to come together and unite on this issue. If we do not police ourselves regarding the appropriate use of high-cost technologies, the Centers for Medicare and Medicaid will most certainly do it for us.”
Cordis is a global interventional vascular technology company
Cordis today announced its acquisition, subject to customary closing conditions including regulatory approvals, of MedAlliance.
A press release notes that the agreement includes an initial investment of US$35 million and US$200 million payment upon closing in 2023, regulatory achievement milestones up to US$125 million and commercial milestones up to US$775 million through 2029. Cordis will immediately begin co-promotion of MedAlliance’s Selution SLR drug-eluting balloon in markets where it is commercially available.
The Selution platform leverages spherical MicroReservoirs made from biodegradable polymer mixed with the drug to control the sustained release of sirolimus. The continuous manufacturing process produces millions of precisely formed, miniature drug delivery systems. According to Cordis, Selution SLR is the only drug-eluting balloon using MicroReservoirs and is designed to provide the longest and most effective pharmacokinetics release profile of any device on the market.
“Nearly twenty years ago, Cordis introduced Cypher, the first drug-eluting stent, transforming cardiovascular treatment for patients around the world,” said Shar Matin, Cordis CEO. “Today, we are furthering that legacy of innovation and market disruption with MedAlliance and the first MicroReservoir sirolimus drug-eluting balloon, Selution SLR.”
Duke Rohlen, executive chairman of Cordis added: “The acquisition of MedAlliance illustrates our vision to maximise patient impact by pairing highly innovative growth drivers with Cordis’ trusted brand and extensive global commercial capabilities.”
Jeffrey B Jump, chairman and CEO of MedAlliance, commented: “When looking for a partner to bring our ground-breaking Selution SLR technology to market, Cordis was the perfect fit with its proven record in the industry. Our sirolimus drug-eluting balloon programme provides a flagship product that complements Cordis’ existing portfolio and will benefit greatly from its deep marketing and distribution expertise.”
Selution SLR received CE mark approval for the treatment of peripheral arterial disease in February 2020 and for the treatment of coronary artery disease in May 2020. In addition, MedAlliance has obtained investigational device exemptions for peripheral below-the-knee (BTK) and superficial femoral artery (SFA) interventions. Two IDE clinical studies are already underway.
“I have had the privilege to meet with clinical experts around the world and review hundreds of angiograms demonstrating the impact of Selution SLR in both cardiovascular and peripheral vascular patients,” said George Adams, chief medical officer for Cordis. “The clinical outcomes are remarkable, to say the least—especially for patients with few if any other treatment options.”
CSI notes in a press release that the 2.00 Max Crown is uniquely designed to enable simultaneous modification of both intimal and medial calcium. The device features an increased 70-micron diamond coated crown that creates more efficient engagement in mixed plaque, helping to achieve optimal luminal gain in mild to moderately calcified lesions above the knee.
Amit Srivastava (Bay Area Heart Center, St Petersburg, USA), who was one of the first physicians in the USA to incorporate the 2.00 Max Crown into his practice, commented: “The new 2.00 Max Crown greatly expands the lesions that can be treated with CSI’s orbital atherectomy. This device delivers exceptional luminal gain in mixed morphology lesions above the knee.”
Scott R Ward, chairman, president and chief executive officer of CSI, said: “The full commercial launch of the 2.00 Max Crown represents another important product launch for CSI as we broaden and diversify our product offering. Our peripheral orbital atherectomy systems can now treat a wider range of plaque morphologies throughout the leg. Combining this new device with our full line of interventional support devices, we continue to advance the ability of physicians to improve outcomes for patients undergoing peripheral interventions.”
Medtronic has announced the 36-month final results from the ABRE clinical study. The purpose of the ABRE clinical study was to evaluate the safety and effectiveness of the company’s Abre venous self-expanding stent system, intended for the treatment of symptomatic iliofemoral venous outflow obstruction.
The study results were presented in a late-breaking clinical trial session at the American Vein and Lymphatic Society (AVLS) 2022 annual meeting (13–16 October, New Orleans, USA). Stephen Black (Guy’s and St Thomas’ Hospital, London, UK), co-principal investigator for the ABRE study, presented the data.
“The 36-month ABRE data have continued to demonstrate the long-term durability of interventions in patients suffering from deep venous disease,” Black said. “The results show a sustained result in both technical aspects, but more importantly, in patient outcomes.”
The ABRE study included a complex set of patients. Within this patient group:
47.5% of patients were categorised as having post-thrombotic syndrome (PTS),
35.8% of PTS patients presented with a complete venous occlusion confirmed by the core lab
Mean lesion length of patients was 112.4mm
44% of patients had stents that extended below the inguinal ligament.
Of note, the study results showed:
Overall, effectiveness following treatment with the Abre venous stent was sustained through 36 months as evidenced by a Kaplan-Meier estimated primary patency rate of 81.6% and a Kaplan-Meier estimated freedom from clinically driven target lesion revascularization (CD-TLR) rate of 89.3%.
No stent fractures or delayed stent migrations were reported through 36 months.
Sustained and clinically meaningful improvements were observed through 36 months compared to baseline as measured by EQ-5D and VEINES-QoL quality of life.
Sustained and clinically meaningful improvements through 36 months as measured by Villalta and VCSS venous functional assessments indicates less severity of PTS disease and venous disease overall.
“Medtronic is strongly committed to the deep venous market. As the 36-month results show, the Abre venous stent system safely and effectively treats venous disease,” said Dave Moeller, president of the Peripheral Vascular Health Operating Unit at Medtronic. “This study included many patients with highly challenging cases, showing that Abre is meaningfully able to improve patients’ quality of life—including those with severe disease—for a long period.”
Interventional radiology (IR) was officially born on January 16, 1964, when Charles Dotter performed the first arterial angioplasty at the Department of Radiology at Oregon Health and Science University (Portland, USA). We still can see the prescription Dotter received from the referring physician, which stated: “VISUALISE BUT DO NOT TRY TO FIX!!!” Roberto Luigi Cazzato speaks to Interventional News about the emergence of IR outpatient clinics (IROCs) and his view that IR hospitalisation clinics (IRHCs) will soon begin being established too.
The above phrase summarises what interventionalists are—dreaming souls looking for innovation. For this reason, it is not surprising that in the last few decades, IR has evolved so rapidly that today, at least one type of IR procedure can be done on any and every organ. Moreover, devices and imaging guidance are becoming so sophisticated and precise that new interventions and clinical outcomes are presented yearly. Therefore, as interventional radiologists, we are succeeding in providing innovation in healthcare.
Our willingness for innovation is not only due to our love for novelty and technology. In our minds, innovation has a purpose, and it is a noble one—to serve our patients! For this reason, we stay in close contact with patients before and after interventional procedures.
It is not a surprise that in the last decade, IR initiatives intended to increase contact with our patients and improve their care have flourished. From this perspective, two main measures can be adopted: the IROC for consulting patients before and after the intervention; and on the other side, the IRHC, which provides hospital beds for patients undergoing challenging interventions.
Both of these solutions are desirable for the development of our specialty. However, the clinical, administrative, and financial input to establish IROCs versus IRHCs differs— it is much less costly to establish an IROC compared to an IRHC. In the last decade, newly built IROCs have flourished, with IRHCs less of a priority. The creation of IROCs is the first step, but we are confident that IRHCs will soon become more common.
In the meantime, we can analyse the performance of the IROC so far. In a paper published in CardioVascular and Interventional Radiology (CVIR), the addition of an IROC at the University Hospital of Strasbourg (Strasbourg, France) has had a positive effect on patient care. The results have been quite surprising:
The total number of consultations steadily increased from the first to the last year of the study period (from 693 consultations performed in 2011, to 1595 consultations performed in 2019, which accounts for an increase of 130%); the rate of unattended consultations remained stable throughout the entire study period (around 7%); in the 2018–2019 period, the cumulative procedure conversion rate, namely, the rate of first consultations that led to an IR procedure, was higher than 85%; among the 159 patients being surveyed to evaluate their satisfaction with the IROC, 99.2% highly appreciated their IROC experience, and pointed out that the main aspects they took into account to evaluate their IROC experience were the quality of secretarial and medical services.
These results represent another successful chapter for IR in its so far short, but bright, history. This study points out that as interventional radiologists, we are succeeding in taking care of our patients and that our clinical role is being affirmed, which may pave the way to establishing IRHCs in the near future.
Nevertheless, with patients looking for high-quality secretarial and medical services, these results also show that specific training is required for the employees involved in running the IROC.
The entire IR community is becoming increasingly interested and focused on developing this topic; for this reason, the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) dedicated a lecture to ‘How to establish and run an outpatient clinic’ at its annual meeting (10–14 September, Barcelona, Spain).
Roberto Luigi Cazzato is associate professor at the Department of Interventional Radiology, University Hospital of Strasbourg (Strasbourg, France).
Disclosures: The author declared no relevant disclosures.
Interventional News’ most popular content last month included news of the acquisition of a new catheter by Bentley, the announcement of the final patient enrolled in a liquid embolic study, latest data from the SAVAL trial of a drug-eluting stent, and a video discussion of the current landscape of deep vein thrombosis (DVT) treatment.
Bentley announced that it has acquired the rights of the GoBack catheter from Upstream Peripheral Technologies. The catheter will simplify crossing and re-entry in occluded arteries.
Medtronic announced that it has recently received CE mark for its Radiant balloon-expandable covered stent, the first and currently, only, covered stent indicated for use in chimney endovascular aneurysm repair (ChEVAR) with the Endurant II/IIs stent graft system.
Stryker has announced in a press release that its OptaBlate bone tumour ablation system (OptaBlate) has received 510(k) clearance from the US Food and Drug Administration (FDA). The addition of the OptaBlate technology to Stryker’s Interventional Spine (IVS) portfolio expands on its core competencies in vertebral augmentation and radiofrequency ablation and completes its portfolio of treatment options for metastatic vertebral body fractures.
Andrew Wigham (Oxford, UK) and Rick De Graaf (Friedrichshafen, Germany) discuss the current state of DVT treatment at the Leipzig Interventional Course (LINC) 2022 (6–9 June, Leipzig, Germany), with both noting that “a massive problem” in Europe is the lack of awareness around treatment.
Fluidx Medical announces completion of trial enrolment for its GPX embolic device. In this multicentre trial, GPX was used to treat a variety of primary and metastatic tumours, renal adenoma tumours, and a range of other arterial and venous applications.
Philips announced new milestones in the development of the world’s first spectral detector angio computed tomography (CT) solution— Philips Spectral Angio CT suite—bringing the company’s breakthrough spectral CT imaging technology into an integrated hybrid angio CT suite.
Penumbra and Asahi Intecc, a Japanese medical device manufacturer, announced that they will collaborate to introduce Penumbra’s Indigo Aspiration System into the Japanese market upon regulatory approval.
Reto Bale (Medizinische Universität Innsbruck, Innsbruck, Austria) gave a presentation titled ‘Stereotactic thermal ablation—can it break the current limits?’ at the 2022 European Conference of Interventional Oncology (ECIO; 24–27 April, Vienna, Austria). A key takeaway was that the stereotactic procedure yields “excellent” results.
Ablation is used to destroy or shrink tumours in the liver, lung, kidney, bone, and other organs. In recent decades, image-guided ablation has become integral to modern cancer therapy with curative or palliative intent. Although a promising treatment option, the main challenge is the accurate and safe positioning of the ablation probes to achieve complete tumour coverage, especially in difficult-to-access localisations.
XACT Robotics announced that its ACE Xtend remote control unit received US Food and Drug Administration (FDA) clearance, allowing users to robotically insert and steer the XACT ACE Robotic System remotely from the control room. The first-of-its-kind feature for computed tomography (CT)-guided percutaneous procedures is designed to improve physician workflows while limiting physician and other users’ exposure to radiation, and to reduce physical strain.
“The XACT ACE Robotic System has already allowed users to make percutaneous procedures, such as ablations, drainages and biopsies, more accurate, consistent and efficient,” said Shai Meltzer, chief executive officer of XACT Robotics. “The addition of ACE Xtend has the potential to further increase efficiencies for the care team with a streamlined workflow that helps reduce the time during which physicians and other users are exposed to harmful radiation during standard procedures.”
“Interventional radiology is among the medical specialties that are facing a physician shortage in the coming years and technologies that can improve their efficiencies are crucial,” said Jeffrey Solomon, vice president of Medical Affairs at XACT. “By equipping different users with tools that can standardise the procedure and potentially shorten procedure times, we can maximise the number of patients they see.”
The comprehensive XACT ACE Robotic System combines image-based planning and monitoring with patented S-Drive technology, which enables the system to quickly adapt from a linear to a non-linear trajectory with its robotic insertion and steering of instruments during interventional percutaneous procedures.
The XACT ACE Robotic System has been proven to achieve 1.7mm tip-to-target average accuracy upon first insertion based on data obtained from company clinical studies for biopsy procedures. By providing accurate and actionable results for medical diagnosis, the system aims to enhance early detection and improve patient outcomes.
Six-month data from the Surmodics SWING first-in-human (FIH) study of the company’s Sundance sirolimus drug-coated balloon (DCB) were shared at the 2022 Amputation Prevention Symposium (AMP; 9–11 October, Lugano, Switzerland).
The SWING study is a prospective, multicentre, single-arm feasibility study to evaluate the safety and performance of the Sundance sirolimus DCB when used to treat occlusive disease of the infrapopliteal arteries.
The study’s primary safety endpoint data showed no perioperative deaths or major amputations at 30 days and just one major reintervention was reported among the 35 trial subjects, a Surmodics press release reports. Data for the primary efficacy endpoint show a late lumen loss (LLL) of 1mm (±0.79mm) across 35 lesions at six months, indicating that the large luminal gain achieved immediately after the procedure was sustained six months post-treatment.
“At six months we observed a consistent improvement in Rutherford category and functional measures, as well as an excellent primary patency of 88.5%, which compares favourably to other DCBs used in the infrapopliteal circulation,” said SWING trial co-lead investigator Ramon Varcoe, vascular surgeon at the Prince of Wales Hospital and associate professor of vascular surgery at the University of New South Wales (Sydney, Australia).
The SWING trial enrolled subjects with stenotic or occluded lesions of the infrapopliteal arteries, a reference vessel diameter (RVD) of 2mm to 4mm, and a total lesion length of ≤230mm for treatment with the Sundance sirolimus DCB at eight sites in Australia, New Zealand, and multiple locations in Europe. They will be followed for 36 months following the index procedure.
“The novel coating on the Sundance sirolimus DCB was evaluated in a challenging, predominantly CLTI [chronic limb-threatening ischaemia] population with a high proportion of diabetes and moderate-severe calcification,” said trial co-lead investigator Andrew Holden, director of interventional radiology at the University of Auckland (Auckland, New Zealand). “This first-in-human study demonstrates that the Sundance sirolimus DCB could be a safe and promising treatment for occlusive disease of the infrapopliteal arteries.”
The Sundance sirolimus DCB utilises a “next-generation” coating technology consisting of microcrystalline sirolimus and a proprietary excipient to maximise drug transfer, which, according to Surmodics, enhances sirolimus delivery and sustains therapeutic levels in the artery.
In a press release, Surmodics notes that sirolimus is a potent anti-inflammatory and anti-proliferative compound, has been used successfully in coronary drug-eluting stents. “The delivery of sirolimus to the vessel wall during mechanical dilatation provides an ancillary action of inhibiting the proliferation of cells, with the intended purpose of reducing restenosis,” the company adds. Surmodics advises that the Sundance sirolimus DCB is not available for sale anywhere in the world, and currently is for investigational use only.
A new report from a joint taskforce of the American College of Radiology (ACR) and the Society of Interventional Radiology (SIR) recommends improved access to interventional radiologists in small and rural areas. The taskforce was formed to explore strategies for recruitment and retention of interventional radiologists in rural areas, which have the greatest challenges with access to interventional radiologic care.
“Interventional radiologists play a key role in improving patient health outcomes and creating healthier communities,” said Alan H. Matsumoto, vice chair of the ACR Board of Chancellors and a member of the joint taskforce. “The recommendations should be beneficial for practices in small and rural areas that hope to recruit interventional radiologists and provide the care patients deserve.”
“Access to an interventional radiologist’s care can be the difference between life and death.”
The taskforce focused on improving training opportunities, creating templates to help radiology practices and hospitals provide interventional radiology (IR) services in small and rural communities, and developing appropriate financial models to recruit interventional radiologists to these areas and retain their services.
“Access to an interventional radiologist’s care can be the difference between life and death, yet millions of Americans living in rural communities do not have access to the image-guided treatments interventional radiologists perform to literally save life and limb,” said SIR President Parag J. Patel, professor of radiology at the Medical College of Wisconsin (Milwaukee, USA). “Access to IR services improves the care offered within a hospital or health system. The recommendations outlined in this paper will help practices attract IR talent and expand IR services where they are often needed the most, eliminating IR deserts and improving patients’ access to the care they need.”
The report was published online in the Journal of the American College of Radiology (JACR).
Endologix has announced the submission of a premarket approval (PMA) application requesting approval for the Detour system to the US Food and Drug Administration (FDA).
The Detour system, which earned FDA Breakthrough Device Designation, is a unique therapy that allows the creation of a fully percutaneous femoropopliteal bypass that is routed through the femoral vein. The Detour system uses the Endocross Device and Torus Stent Graft to treat patients with moderate to severe peripheral arterial disease with long blockages of the superficial femoral artery (SFA).
The PMA application includes the results of the DETOUR2 IDE study, which were presented at the 2022 Annual Meeting of the Society for Vascular Surgery (SVS; 15–18 June, Boston, USA). Sean Lyden (Cleveland Clinic, Cleveland, USA), one of the study’s principal investigators presented results that included 12-month primary patency of 72.1% in SFA lesions with a mean length of 32.7cm. The trial demonstrated technical success of 100% in 202 patients, with a 30-day major adverse event rate of 7%.
“This submission is a significant milestone in our mission to expand our therapeutic products into the large peripheral vascular market opportunity. Patients with long SFA blockages have compromised treatment options at present due to high rates of failure with conventional endovascular techniques and the morbidity associated with open femoropopliteal bypass surgical procedures,” said Matt Thompson, president, and chief executive officer of Endologix. “Once approved, offering a fully percutaneous femoropopliteal bypass, will provide a disruptive, innovative therapy to physicians for the treatment of long-segment SFA disease and expand the treatment options available for these patients.”
Thomas Rand (Klinik Florisdorf, Vienna, Austria) recently presented on the preliminary results to 12 months of the Motiv bioresorbable scaffold (Reva Medical) postmarket trial at the recent Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain). With the objective of evaluating safety and efficacy for the treatment of patients with rest pain or minor tissue loss due to the presence of lesions of a maximum length of 100mm at the level of the below-the-knee (BTK) arteries, Rand shared in a FIRST@CIRSE session that at 12 months, primary patency—the efficacy endpoint—was 88%, and the technical success rate, 99%.
The MOTIV BTK study is a prospective, single-arm, multicentre trial, in which 58 patients with BTK artery lesions of a maximum length of 100mm have been enrolled. The study is being carried out on 60 limbs with 76 Motiv scaffolds, Rand specified. The Motiv scaffold has been approved for use in Europe since 2018 when, according to Reva Medical, the device became the first bioresorbable scaffold to receive CE mark for use below the knee.
“The special thing with the Motiv scaffold,” Rand opined, “is that it is sirolimus-eluting and bioresorbable, so you have two good things.” The presenter noted that this is in keeping with the ‘leave nothing behind’ concept. “The scaffold itself is made from TyroCore, which is derived from tyrosine amino acid,” Rand then detailed, and this design is responsible for “low inflammation and irritation during degradation and [no calcification].” The thin struts “have been evaluated as best-in-class,” Rand supplemented.
Moving on to address the preliminary study outcomes, Rand described them as “really very good, [with] a 99% technical success in all patients.” Primary patency at six months was 90%, and the 12-month preliminary result 88%. The limb salvage rate until now at 12 months, as conveyed by Rand was 97%, and the 14% (n=8) death rate was entirely unrelated to the device or procedure. The freedom from clinically driven target lesion revascularisation (CD-TLR) was “a very nice” 98.3% at 12 months, Rand also underlined, with a “decline in Rutherford stages observed during this time.”
“As a conclusion, already, we can say with the Motiv scaffold we had excellent tracking and visibility and a problem-free delivery.” Rand proceeded to emphasise the scaffold’s ease of use and the 90% vessel patency rate, before sharing that the CD-TLR and limb salvage rates remained stable from six to 12 months.
“The major concept behind this study, which I really like, is the ‘nothing left behind’ concept, and this is really fulfilled in this study,” Rand finished by informing delegates.
Enrolment in MOTIV IDE clinical trial begins
In the weeks following CIRSE 2022, Reva Medical announced that enrolment in the MOTIV pivotal trial has been initiated at clinical centres in both the USA and Europe. The study, which is being conducted under a US Food and Drug Administration (FDA) investigational device exemption (IDE), will evaluate the use of the Motiv sirolimus-eluting bioresorbable vascular scaffold for treatment in patients suffering from chronic limb-threatening ischaemia (CLTI).
The MOTIV study is a global, randomised controlled trial (RCT) that was designed to evaluate the safety and efficacy of the Motiv scaffold for the treatment of infrapopliteal lesions in patients with CLTI by randomised comparison with standard balloon angioplasty. The study, led by co-principal investigators Ehrin Armstrong (Adventist Health, St Helena, USA) and Andrej Schmidt (Universitätsklinikum Leipzig, Leipzig, Germany) will follow up to 292 patients at approximately 35 clinical centres in the USA and Europe.
Schmidt recently recorded a live case using Motiv scaffolds that was shown at the 2022 Transcatheter Cardiovascular Therapeutics (TCT) conference (16–19 September, Boston, USA). During the procedure, Schmidt implanted three 60mm Motiv scaffolds in a patient with CLTI below the knee, and the patient has demonstrated positive postoperative results.
“The absence of an approved device as a dedicated treatment option for the estimated 20 million patients worldwide suffering from CLTI is a significant unmet need,” commented Jason Ricci (Bellin Health Cardiology Associates, Green Bay, USA), the physician who enrolled the first US patient. “I am delighted to play a role in this important trial and evaluate its potential to advance the science and therapies available to this highly complex patient population.”
“The Motiv scaffold has a demonstrated history of positive clinical results, and I am honoured to have performed the first procedures with the device in this trial,” stated Henrik Schröder (Ihre Radiologien MVZ, Berlin, Germany), who enrolled the first European patients. “The scaffold was easily delivered, and the procedure was aided by visibility of the device under fluoroscopy, which is beneficial to confirm proper placement.”
Xeltis today announced what it describes as “very promising” preliminary efficacy and safety results from one of the centres participating in the AXESS study—a first-in-human (FIH) clinical trial of its restorative haemodialysis access graft, Axess.
The company has also reported that enrolment in the trial is now complete, with 20 patients having been successfully implanted with the Axess graft.
During haemodialysis, the Axess device demonstrated 100% cumulative primary and secondary patency, with an average follow-up time of 5.8 months and no device-related complications, in patients implanted by Matteo Tozzi and his team at the University of Insubria (Varese, Italy)—one of six European sites participating in the trial.
These data will be presented at the Porto Vascular Conference (PVC; 7–8 October 2022, Porto, Portugal), organised by the European Society of Vascular Surgery (ESVS). To date, Axess has enabled more than 1,200 haemodialysis sessions in just over a year as part of the AXESS FIH trial. Sixty of these sessions have taken place in Varese, a Xeltis press release states.
“Our initial clinical experience with Axess is very promising, from implanting to puncturing, and the data on functionality observed so far are very encouraging,” Tozzi commented.
Xeltis’ Axess device is a synthetic, bio-restorative vessel graft that enables early puncturing needed to connect to the haemodialysis machine. Unlike any currently available options—according to Xeltis—it is also designed to turn into a patient’s own living blood vessel, like an arteriovenous fistula, as its porous structure gets gradually colonised by patient’s own tissue cells.
According to the experience in Varese, Axess improved compliance over time, which may result from new tissue forming in the device.
After the disappointment of a few failed randomised controlled trials (RCTs), transarterial radioembolization (TARE) is finally back in the spotlight. And interventional radiologists (IRs) are learning from these past failures to shape the future.
Despite negative results, former trials have taught us that TARE is a highly effective treatment option if some essential rules are respected. Firstly, thoughtful selection of patients, with careful evaluation of the liver function reserve. Secondly, adequate arterial vascularisation, with a preference for no harm caused by prior therapy. The third rule is to carry out personalised dosimetry tailored to the vascular anatomy, tumour type and extension, the patient’s characteristics and the goal of treatment.
Irene Bargellini
Learning from the past, the current decade has finally started with successful trials, showing the efficacy and safety of TARE in primary tumours (such as the DOSISPHERE-01 [Boston Scientific], TRACE and LEGACY [Boston Scientific] trials for hepatocellular carcinoma (HCC) in advanced, intermediate and early stages, respectively) as well as metastatic lesions (such as the EPOCH [Boston Scientific] study in second-line colorectal cancer metastases).
Personalised dosimetry has become a central focus of investigation in an attempt to identify the most adequate administered activity for achieving tumoricidal tumour-absorbed doses without harming the surrounding liver parenchyma. With high tumour-absorbed doses, complete tumour necrosis may be achieved, translating into a durable response, conversion to surgery and ultimately significant survival advantage. However, obtaining a high tumour-absorbed dose implies limited dose to the non-tumoral parenchyma— in other words, a high tumour-to-liver ratio. If all or almost all the activity is concentrated selectively in the tumour cells, there is, potentially, no limit to the radioactivity level we could administer!
But what do IRs have to do with this? There is no doubt that good dosimetry starts with a good angiographic work-up, by understanding anatomy, flow distribution and haemodynamics, so that the tumour can be targeted selectively. Over the years, the preliminary angiographic work-up has adapted to increasingly refined dosimetry calculations. From whole-liver and hemi-liver treatments, in which the main challenge was the identification of extrahepatic vessels, we are moving towards selective and super-selective treatments and, where these are not possible, we are learning how to exploit and modify the arterial flow.
While selectivity can be relativity easy to obtain when dealing with hypervascular lesions, and well demarcated and limited tumour burden, it becomes challenging in patients with infiltrative lesions, hypovascular tumours and multifocal extensive disease. How can we obtain a selective intratumoral concentration of particles in these cases?
Several computational studies have shown that even minimal modifications in injection parameters and position, shape and orientation of the supporting catheters and of the microcatheters may have a meaningful impact on the distribution of flow in the target volume. As an example, when the catheter is close to an arterial bifurcation, a preferential flow into one of the two branches is frequently observed, influenced by the size of the distal vessels, their area of distribution, and the morphology and the orientation of the catheter’s tip. The challenge for the operator is to select the most appropriate position for the catheters and, if needed, exploit specific pre-shaped microcatheters, to obtain a homogeneous flow distribution in the entire target liver volume.
The capacity of the arterial branches to receive the right quantity of spheres is another matter of concern, particularly in tumours with multiple feeding vessels and in pre-treated patients with impaired arterial vascularisation. Minor tumour-feeding vessels may require coil embolization to promote flow redistribution. However, redistribution requires an in-depth knowledge of the possible intra- and extrahepatic arterial connections; it may be tricky and unpredictable, varying by specific vascular anatomy, the tumour type and tumour location. The success of flow redistribution has been reported to be lower in certain conditions, such as when parasitised arteries are embolized proximally, or when it is difficult to predict which vessels are going to be recruited after embolization— in centrally located tumours if unilobar treatment is planned, and in hypervascular bulky lesions. As a result, flow redistribution is now recommended only when strictly needed.
Specific microcatheters, such balloon and anti-reflux microcatheters, have recently become available, and through different mechanisms, they are able to modify the haemodynamics and flow distribution, potentially enhancing the intratumoral uptake and reducing the risk of reflux and non-target embolization. These tools may be of particularly useful for treating hypovascular lesions and multifocal disease. How effective they are for radioembolization is still being investigated.
In conclusion, we have learned over the years that, to be successful, radioembolization requires a high level of expertise—it is a truly multidisciplinary treatment modality. Dosimetry is key to success; yet, personalised dosimetry requires personalised angiographic planning based on flow analyses and where possible, flow modification, to achieve selective tumour uptake.
Irene Bargellini works within the Division of Vascular and Interventional Radiology at Florence University Hospital (Florence, Italy).
Disclosures:Bargellini declared having received an institutional research grant from Boston Scientific; consulting fees from AstraZeneca, EISAI, GE Healthcare, Guerbet, Merck, Sirtex, Terumo; honoraria for lectures from AstraZeneca, Bayer, Boston Scientific, Eisai, Guerbet, Merck, Sirtex, Sobi, Terumo; having been part of the Independent Data Safety Monitoring Board for AstraZeneca.
Results of the FLASH registry demonstrate the “excellent safety profile” of the FlowTriever system (Inari Medical) in 800 “real-world” patients. This is according to Catalin Toma (University of Pittsburgh Medical Center, Pittsburgh, USA), who presented outcomes for the full US cohort of FLASH at the 2022 Transcatheter Cardiovascular Therapeutics meeting (TCT; 16–19 September, Boston, USA). The results were simultaneously published in EuroIntervention.
Toma reported a 1.4% major bleeding rate and 0.4% rate of other major adverse events (MAEs) in what the presenter described as the largest prospective interventional study in pulmonary embolism (PE). All-cause mortality was <1% at the 30-day visit in this “real-world” population with prevalent baseline predictors of mortality, the presenter added, noting also that haemodynamics improved on-table, acute vitals and right ventricular (RV) strain normalised, and clinical recovery continued through six months.
The presenter noted that acute all-cause mortality following PE has remained high (>10%) over two decades, adding that, following PE, the 30-day readmission rate is nearly 25%, and up to half of patients report persistent dyspnoea, exercise intolerance, and/or functional limitations at three to six months.
According to Toma, guidelines suggest considering advanced therapies, including mechanical thrombectomy, when thrombolytics fail or are contraindicated, or haemodynamic deterioration occurs. However, he said, major bleeding risks with thrombolytic-based treatment strategies remain a concern, and their use is limited by corresponding contraindications and consequent intensive care unit (ICU) monitoring.
Mechanical thrombectomy can rapidly extract thrombus and relieve RV strain without thrombolytics, the presenter informed the TCT audience, stating that “additional data on the risk-to-benefit ratio could shift the standard of care”. One example of a mechanical thrombectomy device is FlowTriever, he highlighted, noting that this system is 510(k)-cleared by the US Food and Drug Administration (FDA) and CE mark-approved for the treatment of PE.
FLASH is a prospective, multicentre, single-arm registry designed to evaluate the safety and effectiveness of the FlowTriever system for treatment of PE through six months, with the decision to intervene being at the discretion of treating physicians or local PE response team (PERT). The primary endpoint is an MAE composite endpoint of device-related mortality within 48 hours, major bleeding within 48 hours, and intraprocedural device- or procedure-related adverse events.
At TCT, Toma reported outcomes for the full US cohort. In terms of the primary outcomes, he relayed a primary MAE rate of 1.8% (14/788), which combined a 0% rate of device-related deaths (0/788), 1.4% rate of major bleeding (11/788), and 0.4% rate of intraprocedural adverse events (3/788). The presenter also communicated all-cause mortality data, noting rates of 0.3% at the 48-hour visit (2/794), 0.8% at the 30-day visit (6/734), and 5% rate at the six-month visit (28/588). Importantly, the procedure led to significant improvement in invasive haemodynamics with decreased pulmonary pressures and improved cardiac output. Finally, Toma revealed that the rate of all-cause readmissions at the 30-day visit was 6.2%, with 1.4% related to PE treatment (10/711) and 4.8% unrelated to PE treatment (34/714).
Looking ahead, Toma highlighted that “data from the ongoing PEERLESS randomised controlled trial will provide important evidence regarding the safety and effectiveness of FlowTriever mechanical thrombectomy compared with catheter-directed thrombolysis”.
Paediatric interventional radiologist Alex Barnacle (Great Ormond Street Hospital, London, UK) gave the Josef Roesch Lecture at the Cardiovascular and Interventional Radiological Society of Europe 2022 meeting (CIRSE; 10–14 September, Barcelona, Spain), choosing to present on the subject of ‘Developing excellence in interventional radiology (IR) for our youngest patients’.
The presenter used various case examples to demonstrate to non-paediatric interventionalists that they “still need to think about [paediatric IR]—children grow up and graduate into adult practice”. A take-home message from Barnacle was how cross-specialty collaboration on issues such as establishing standards of practice, especially with the wider IR community, will help paediatric IR grow and “[change lives]”.
Barnacle’s presentation began with the story of a patient of hers, who was the first to receive orbital sclerotherapy at Great Ormond Street Hospital. Highlighting the life-changing impact of the treatment on her patient, Barnacle also underlined the importance of her network in providing the care her patient required—“[David Lord] talked me through [the procedure] over the telephone and we did [it].” This success is proof of the value of tapping into “the very small pool of expertise around the world”—Lord is based in Sydney, Australia—however “if we do not know each other, we cannot share our expertise and data,” Barnacle acknowledged.
How crucial cultivating a network within paediatric IR is, is complemented by the need to communicate and work together with other specialties so that they better recognise where paediatric IR can play a key role in patient care. “Just as with IR […] paediatric IR is massively under-recognised by other specialties,” Barnacle stated, going on to explain the impact this has—”we get late referrals because other teams do not know what we can do”. An example of where increased awareness and implementation of paediatric IR expertise could make a difference to current practice is, as illustrated by Barnacle, central venous access. “We all know that children should not need to be going through repeated painful, distressing cannulations […] that will mentally and physically scar them and their families for the rest of their lives.” What is a “bread and butter” procedure for a paediatric interventional radiologist will enable their patients to “get on with dealing with [everything else] that they need to, without having to think about those repeated cannulations.”
Barnacle presenting her Josef Roesch Lecture at CIRSE 2022
In contrast to the day-to-day roles paediatric interventional radiologists can play, such as by providing central venous access, Barnacle touched on the “supportive care” that they can give patients with rarer conditions, including those with rapidly involuting congenital haemangioma, and those who have swallowed button batteries, and may require dozens of interventions to “get through”.
Protocols and guidelines are also a factor in limiting the extent to which paediatric IR can fulfil its potential in such cases, as Barnacle also flagged. The presenter illustrated her point with a trauma case example, which saw the 15-year-old patient requiring a partial splenic embolization bypass a major trauma centre, as protocol would not allow (non-paediatric) interventional radiologists to carry out the treatment. “[It] just feels wrong”, Barnacle admitted, before suggesting that, as with the “limited” existing standards of practice for paediatric IR, “we need more”. As a potential solution to the paucity of paediatric IR-specific practice guidelines, the presenter offered the approach of adding paragraphs to existing guidelines on how to nuance well established adult practice for children.
A further barrier to widespread recourse to paediatric IR that Barnacle brought to the audience’s attention was the increase in paediatric contraindications for some devices—“we have had to change the inferior vena cava [IVC] filter we use,” the presenter lamented. This is symptomatic of a “small toolbox that is being emptied very quickly,” which, in addition to affecting paediatric IR practice, also has a knock-on effect for training, as device companies feel obliged to pull out of events such as the hands-on device training offered at meetings.
Nevertheless, Barnacle rounded off her presentation on a positive note, taking stock of the increasing interest in paediatric IR, of which there is ample evidence. The scope of the paediatric IR programme at CIRSE was one example Barnacle drew upon, including a sell-out hands-on session in spite of one company pulling out for the aforementioned reason of contraindications. “Things are changing,” according to the presenter, proceeding to celebrate the fact that CVIR Endovascular’s most downloaded paper of the past year was on paediatric IR, and how the remote Society of Paediatric Interventional Radiology annual meeting in 2020 saw attendees from 43 different countries.
Key now, Barnacle believes, is to “build on this interest”, which, she believes, extends to trainees looking for more of a “human side” to their work and “greater job satisfaction”—requirements that, she opines, being a paediatric IR can meet. As relayed throughout her presentation, efforts to grow paediatric IR, and interest and awareness of it, can take the form of establishing clearer guidelines and protocols, drawing on professional networks to aid innovation and optimal patient care, and working with colleagues in other specialties “so that children get referred to us sooner—this is better than picking up the pieces,” Barnacle concluded. “[After all], we are all here because we believe that minimally invasive procedures are the way to go” was the presenter’s salient final remark.
Terumo Medical Corporation has announced late-breaking data showing the safety and efficacy of radial to peripheral (R2P) interventions with the R2P Misago self-expanding peripheral stent in lower extremity endovascular interventions via a radial approach. The results were presented at this year’s Transcatheter Cardiovascular Therapeutics (TCT) conference (16–19 September, Boston, USA).
Presented by Yulanka Castro-Dominguez (University Hospitals’ Harrington Heart & Vascular Institute, Cleveland, USA), the study results showed that using a radial approach in treatment of complex lower extremity peripheral arterial disease (PAD) allowed 92.3% of patients to be discharged the same day. In addition, there were no serious access site complications for any of the patients enrolled in the study.
“In the invasive management of patients with PAD, the ‘radial first’ approach is beginning to gain momentum,” said Michael Martinelli, chief medical officer of Terumo Medical Corporation. “Radial artery access has been shown to minimise bleeding and vascular complications, lessen mortality rates, reduce costs, and shorten length of stay compared to femoral access in patients undergoing percutaneous coronary intervention (PCI), and we are now seeing growing evidence for similar benefits in peripheral arterial intervention. Our study contributes significantly to this expanding body of evidence as it clearly demonstrates the safety and efficacy of radial access in PAD intervention.”
The study was a prospective, multicentre, core-lab reviewed, clinical endpoint committee (CEC) adjudicated, single-arm study aimed at evaluating the safety and feasibility of radial access when used in the treatment of complex lower extremity PAD. A total of 120 PAD patients with Rutherford classification 2–5, from eight medical centres from across the USA were enrolled from 29 June, 2020 to 24 June, 2021 and followed up to one year.
In the final analysis, the primary safety endpoint included evaluation of radial access related complications, to include: access site bleeding, hand ischemia, hematoma, nerve damage, perforation, pseudoaneurysm, radial artery occlusion, embolic stroke or transient ischemic attack (TIA). Based on CEC adjudication, primary safety events categorized as serious access site-related adverse events did not occur in any patient. Radial access was successfully achieved in 100% of patients.
Patients who received R2P Misago self-expandable bare metal stent were later followed up to 12 months and the reintervention on the target lesion was required only in two patients.
The study was sponsored by Terumo Medical Corporation. Dedicated Terumo radial devices used in this study included: R2P Destination Slender guiding sheath, R2P Metacross RX percutaneous transluminal angioplasty (PTA) balloon dilatation catheter, R2P Crosstella RX PTA balloon dilatation catheter, R2P Misago self-expandable bare metal stent and TR Band radial compression device.
Truveta announced a strategic collaborative agreement with Boston Scientific to improve long-term patient care and gain insights into healthcare disparities. Through this collaboration, Boston Scientific researchers will be able to access data from Truveta, which contain de-identified medical records from more than 65 million US patients.
“Truveta will enable us to gather insights on a breadth of devices and disease states, including peripheral artery disease (PAD), venous thromboembolic disease, and segments of interventional oncology,” said Michael Jaff, vascular medicine specialist and chief medical officer and vice president, Medical Affairs, Innovation and Technology, Peripheral Interventions, Boston Scientific. “The first analysis will focus on gaining a deeper understanding of the long-term patient outcomes relating to the use of our products indicated for treatment of PAD.”
According to the US Centers for Disease Control, PAD affects approximately 6.5 million people aged 40 and older in the USA. This month is PAD Awareness Month, and Truveta recently shared new insights from its de-identified data, including findings that of the more than 11,000 PAD patients who received revascularisation procedures, Black or African American patients with PAD (1.0%) were less likely to undergo revascularisation than white patients diagnosed with PAD (2.6%). Of those who are treated with an interventional procedure, Black or African American patients were also less likely to receive drug-eluting stents than their white counterparts. Additionally, insights into major adverse outcomes, like lower-limb amputation, were discovered. For example, patients treated with drug-eluting stents had lower rates (4.8%) of amputation compared to all patients who received revascularisation (8.5%).
“Device manufacturers realise it is critical to have data on the clinical outcomes for patients treated with their devices following regulatory approvals, yet those data can be messy, fragmented, and difficult to obtain and analyse,” said Terry Myerson, chief executive officer of Truveta. “Truveta solves this problem, empowering researchers with real-world data on how any drug or device is currently being used every day across the USA.”
Truveta data provide the most up-to-date picture of US health across age, race, ethnicity, geography, socioeconomic factors, and more. Data are updated daily and include the full Electronic Medical Record (EMR), including device-specific data, not just the medical bill from claims data, all de-identified and aggregated
These clinical data are linked across providers and with medical claims when care is provided outside Truveta’s network. Every patient record is enhanced with comprehensive socioeconomic data and daily mortality data for a complete picture of each patient’s health journey without risk of re-identification.
“The COVID-19 pandemic put a spotlight on the importance of data to inform and improve patient care. It also put a glaring spotlight on the inequities in accessing and receiving equitable healthcare that are prevalent among people of colour and low-income communities throughout the USA,” said Debbie Salas-Lopez, Community and Population Health at Northwell Health and Truveta Ethics and Health Equity Board of Governors member.
Guerbet announced that the US Food and Drug Administration (FDA), after priority review, has approved Elucirem (Gadopiclenol), a new macrocyclic gadolinium-based contrast agent (GBCA) for use in contrast-enhanced magnetic resonance imaging (MRI).
Elucirem (Gadopiclenol) is a new macrocyclic GBCA with high relaxivity indicated for use in adults and children aged two years and older, for contrast-enhanced magnetic resonance imaging (MRI). The product is used to detect and visualise lesions with abnormal vascularity in the central nervous system and the body (head and neck, thorax, abdomen, pelvis, and musculoskeletal system).
Gadopiclenol, the active substance of Elucirem, has been designed with two sites for water molecule exchange to increase relaxivity and contrast, allowing it to be used at half the conventional dose of gadolinium compared to other non-specific GBCAs.
The efficacy and safety of Gadopiclenol have been assessed as part of Guerbet’s clinical development plan, with marketing authorisation being targeted worldwide (cf. phase III trial results below).
The FDA is the first health authority to have approved Elucirem. It is currently in the process of examination by the European Medicines Agency via a centralised procedure.
“As a pioneer in MR imaging, thanks to the success of our first gadolinium-based macrocyclic contrast agent, we are delighted with the FDA approval of Elucirem. This approval allows patients and practitioners to benefit from the innovations brought by Elucirem,” said David Hale, chief executive officer of Guerbet Group.
Phase III clinical trials for Elucirem
The approval was primarily based on data from two phase III studies completed in March 2021 which demonstrated that Elucirem leads to non-inferior results in brain and body MRI at half the gadolinium dose of Gadobutrol. The endpoints were met in terms of the diagnostic benefit of injecting Gadopiclenol (0.05 mmol/kg) during MRI examinations, based on two criteria:
The superiority of the examination with Gadopiclenol compared to the examination with no contrast agent
The non-inferiority of Gadopiclenol (0.05 mmol/kg) compared to Gadobutrol (0.1 mmol/kg) for the visualisation and detection of lesions of the central nervous system and in the other anatomical areas studied
No major safety signals were reported during the development of Gadopiclenol, and the adverse reactions reported during the two phase III studies were similar for both products administered.
Penumbra and Asahi Intecc, a Japanese medical device manufacturer, announced that they will collaborate to introduce Penumbra’s Indigo Aspiration System into the Japanese market upon regulatory approval.
“By bringing together our newest innovations with Asahi’s leadership and expertise in the Japanese medical device market, we can provide physicians in Japan with technology that has been proven highly effective, helping patients to return home quickly and in good health,” said Adam Elsesser, president and chief executive officer of Penumbra.
Penumbra’s Indigo Aspiration System can be used to remove emboli and thrombi from vessels of the peripheral arterial and venous systems, and for treatment of pulmonary embolism. A minimally invasive device, Indigo enables the restoration of blood flow in such cases as acute limb ischaemia and venous thrombus.
Penumbra’s newest generation offering combines hypotube-based Indigo Aspiration Catheters with Lightning Intelligent Aspiration, a unique computer-aided clot detection technology that can differentiate between clot and blood, designed to reduce blood loss and the need for clot-dissolving drugs, which may lower the risk of bleeding complications.
“Our companies share the mission of helping expand the available treatment options for serious conditions that impact an increasing number of people in Japan,” said Masahiko Miyata, president and chief executive officer of Asahi Intecc. “We believe that, together, we are able to provide physicians with the latest innovations that best meet their patients’ needs and help advance patient care.”
Penumbra’s neurovascular thrombectomy and neurovascular and peripheral embolization devices will continue to be distributed by its long-time partner, Medico’s Hirata. This includes the latest RED reperfusion catheters, which are designed with optimised trackability and aspiration efficiency to help navigate the complex anatomy of the brain and deliver efficient aspiration for the removal of blood clots in a broad range of stroke patients.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain) saw presenters explore artificial intelligence (AI), its current role in interventional radiology (IR), and how the two will evolve together to shape innovative practice in a session named “IR: The most tech of the medical specialties”. Among the key takeaways was reassurance that AI will not “replace” human interventional radiologists, rather that it is a question of understanding how AI can be useful in IR, learning how best to harness it as a tool for improving practices, and combining it with the knowhow and abilities of interventional radiologists to achieve ‘hybrid intelligence’.
Discussion of virtual reality (VR) and augmented reality (AR) also featured in the session, as well as wider commentary on what it takes to become a technological innovator in the IR space.
AI can lead to “truly patient-focused, individualised medicine”
The first speaker, Fernando Gómez Muñoz (Netherlands Cancer Institute, Amsterdam, The Netherlands; Hospital Clinic and Hospital Sant Joan de Déu, Barcelona, Spain), provided a comprehensive overview of how AI is currently being applied in IR and how he predicts this landscape will look in the coming years. Referring to the results for ‘artificial intelligence interventional radiology’ that a pubmed.gov search yields, the presenter demonstrated that AI in IR has been a topic of growing research focus—in 2016 there were 16 publications on the subject, and in 2021, 290.
Fernando Gómez Muñoz presenting at CIRSE 2022
Defining AI as “a combination of algorithms to provide machines with the capability to solve problems in a similar way to humans”, and machine learning as “a subtype of AI that uses computer algorithms to build predictive models,” Gómez Muñoz gave the example of how the latter can be used to predict type 2 endoleaks. The importance of this capability is, he shared with delegates, that “if you can predict [these], you can embolize the vessels that may cause the endoleak beforehand, avoiding a more complex procedure later, or an aneurysm rupture, which can happen if there is no adequate follow-up”.
Among the other applications of AI is in predicting local tumour progression post-thermal ablation, classifying peripheral arterial disease (PAD) in conjunction with computed tomography (CT) angiography, 3D planning for ablation procedures, as well as intraprocedural verification. The presenter then spoke to the advantages that AI offers for limiting unnecessary radiation exposure, such as during fluoroscopy-guided endoscopic procedures. Gómez Muñoz relayed his experience using verification software after ablation of liver tumours. It can “lead to early retreatment in some situations”, he explained, and can “dramatically reduce the recurrence rate of colorectal liver metastases”.
A further take-home message from Gómez Muñoz’s presentation was that he sees haptic perception in robots as a key area of future development with relevance to IR procedures. “Pressure, vibration, temperature and viscosity” are among the types of perception that the presenter hopes to see in robots used in IR settings, bringing the interventional radiologists who will make use of these innovations in a position to practise, increasingly, “truly patient-focused, individualised medicine”.
VR: the potential to reduce radiation exposure
Bradford Wood (National Institutes of Health Center for Interventional Oncology, Bethesda, USA) focused on VR in IR now, and its future directions. An important message he had for delegates was regarding the precise ways in which VR can benefit IR, which “can be poor” when reproducibility is concerned: by standardising practice and “equalising” the care patients receive. VR also has the potential to reduce interventional radiologists’ and patients’ radiation exposure through providing real-time mapping during cases, such as in conjunction with cone beam CT, to increase accuracy. This will also, in turn, reduce procedural complications and the time the given procedure takes. Related to this, VR can track patient movements so registration—the matching of images to the patient—remains accurate throughout the procedure.
Bradford Wood presenting at CIRSE 2022
However, Wood admitted that there are hurdles to adopting VR technologies in an IR practice. For example, goggles—a common means of accessing VR for use in a procedure—can bring on cybersickness, which discourages its use. However, handheld and projector-based tools can be a way around this ergonomic issue—Wood cited a smartphone app that can aid precise needle placement, even for interventional radiologists who are less experienced. Cost-effectiveness, Wood explained, is another barrier to healthcare providers incorporating VR into IR procedures, even though the benefits of increased accuracy and therefore reduced radiation exposure and intraprocedural complications, as Gómez Muñoz outlined, are highly valuable.
Technological innovations at lower cost
Luigi Solbiati (Humanitas University, Milan, Italy) gave his presentation on technological innovations in IR, what it takes to get them off the ground, and the obstacles that innovators can come up against in trying to do so. Solbiati also covered the benefits and pitfalls involved in developing these types of innovations and what he foresees the next disruptive IR technologies being. In terms of the latter, Solbiati cited histotripsy as already showing significant “world-changing” potential as a non-invasive, non-thermal, non-ionising procedure, where high-intensity focused ultrasound (HIFU) has been less successful.
Luigi Solbiati (image credit: CIRSE)
Image fusion technology, which came into being around 20 years ago, was an example Solbiati gave of game-changing technology innovation in IR—“nowadays, we have wonderful rooms where you can do [ultrasound, angiography, CT and cone beam CT] together”.
However, he was keen to acknowledge the lack of accessibility of these types of advancements throughout the world, due to the cost involved. Therefore, Solbiati concluded, “we should find alternative solutions”. Among these, he listed “the fusion of real-time ultrasound (US), contrast-enhanced CT and positron emission tomography (PET) in the US room,” which he qualified by stating that it is “a simple and significantly lower-cost alternative to interventional PET-CT rooms.”
The presenter also opined that robots that facilitate remote needle placement will be a crucial future development in AI for IR, and that ablation confirmation software that should become mandatory after every ablation.
Solbiati himself, as highlighted by his co-presenters, has successfully created technology that can thermally ablate liver tumours using AR alone, and no radiation. One of the ideas behind this is to solve the aforementioned issue of the high cost associated with installing sophisticated multifunction CT suites.
To round off the session, moderator Laetitia Saccenti (Hôpital Paris Saint-Joseph, Paris, France) asked a question on behalf of those who may be concerned about AI capabilities exceeding those of interventional radiologists, and thus reducing or eliminating the scope of human practitioners’ roles in IR. “You cannot change the way things are going, you just have to surf the wave […] the more you learn, the more useful [a tool] it will be,” Gómez Muñoz answered.
Wood reiterated that “[AI and VR] will not replace” interventional radiologists. Certainly, a key takeaway from all three speakers was that technology will evolve to complement the work of interventional radiologists; enhancing what they are able to achieve and far from rendering their role obsolete.
Comparing the Saval drug-eluting stent (DES) below-the-knee (BTK) vascular stent system (Boston Scientific) and percutaneous transluminal angioplasty (PTA) in the infrapopliteal lesions of chronic limb-threatening ischaemia (CLTI) patients, the trial failed to meet its primary effectiveness and safety endpoints.
The primary objectives of the SAVAL study were to evaluate one-year primary vessel patency and safety following use of the Saval DES, which is designed specifically for BTK interventions, Van Overhagen asserted. The stent is made of nitinol and polymer-coated, with paclitaxel.
The presenter then explained that the SAVAL trial is a prospective, multicentre, randomised superiority trial of patients with symptomatic infrapopliteal artery lesions and Rutherford category 4–5 CLTI. The patients were assigned 2:1 to treatment with Saval DES or PTA.
The primary safety endpoint (non-inferiority) is 12-month major adverse event (MAE)-free rate, defined as a composite of above-ankle amputation of the index limb, major reintervention and 30-day mortality, the presenter elaborated.
Providing further details of the study, Van Overhagen stated that a total of 201 patients were enrolled and randomly assigned to treatment (n=130 DES, n=71 PTA) at 39 study centres in Belgium, France, The Netherlands, the USA, and Japan.
In terms of primary results, Van Overhagen reported a high technical success rate of 100% in the DES group and 98.7% in the PTA group.
However, “the primary effectiveness endpoint of superior 12-month primary patency was not met,” the presenter relayed—the figure was 68% in the DES group and 76% in the PTA group. “The primary safety endpoint of non-inferior 12-month MAE-free rate was [also] not met,” Van Overhagen supplemented, citing the results of 91.6% and 95.3% respectively for the DES and PTA groups, while freedom from all-cause mortality was 92.2% versus 89.9%.
Van Overhagen shared the rationale behind conducting the study: CLTI is a condition with “few effective endovascular options for infrapopliteal artery revascularisation” and DESs have yielded positive results in previous studies. This reflects what Van Overhagen highlighted in an earlier presentation he gave on DESs—both an endovascular approach and revascularisation are key to optimal treatment of CLTI.
In view of the primary results, Van Overhagen told delegates that “patient follow-up will continue through three years in-office with vital status assessment through five years, as specified in the study protocol […] We believe that given the impact of CLTI on limb and life, continued innovation to provide minimally invasive treatments is needed”.
In another PAD day session, Van Overhagen presented on the devices currently available and evidence to support the use of DESs specifically.
Van Overhagen began his first presentation of the day by underlining that the “cornerstone” of CLTI is revascularisation—”we try to get unobstructed blood flow all the way into the foot and avoid amputation”. The presenter went on to acknowledge that “we all know that endovascular treatment is less invasive. This is why, where possible, we use an endovascular approach”.
The presenter then proceeded to explain the origin of drug-eluting balloons (DEB) and DES: “[they] have been introduced in order to try to reduce restenosis […] we try to diminish the amount of intimal hyperplasia”. The Dutch PADI trial, for which Van Overhagen was principal investigator, compared PTA with bare metal stents (BMS) to DES and, at two-year follow-up, there were almost twice as many major amputations in the former group, a trend which was also observed at five years.
“Our initial conclusions were that DES BTK in CLTI achieved improved patency, a trend towards fewer major amputations [and indicated] a need for dedicated self-expandable and longer stents,” Van Overhagen reported. Further analysis out to ten years has also shown DES BTK to be safe and cost-effective, the presenter concluded.
Stryker’s first bone tumour ablation system with patented microinfusion technology
Stryker has announced in a press release that its OptaBlate bone tumour ablation system (OptaBlate) has received 510(k) clearance from the US Food and Drug Administration (FDA). The addition of the OptaBlate technology to Stryker’s Interventional Spine (IVS) portfolio expands on its core competencies in vertebral augmentation and radiofrequency ablation and completes its portfolio of treatment options for metastatic vertebral body fractures.
“Stryker’s new bone tumour ablation (BTA) system is a significant improvement on existing technology and builds on Stryker’s IVS portfolio,” said Anthony Brown, a vascular and interventional radiologist at Radiology Imaging Associates (Englewood, USA).
As Stryker’s first interventional oncology technology, OptaBlate optimises all aspects of the procedure, from set-up to ablation. Featuring four probes and Stryker’s patented microinfusion technology, OptaBlate allows physicians to customise their procedure and reduce ablation time by three minutes.
Specific key features of the system include:
Treatment of two vertebral body levels at once using a bipedicular approach
Quicker, more consistent ablation
Microinfusion technology, which keeps the zone hydrated, reducing impedance errors and preventing charring
“The collaboration has helped us to develop a more efficient bone tumour ablation system to address their unmet needs,” said Greg Siller, vice president and general manager, interventional spine business, Stryker. “OptaBlate will help our customers provide another treatment option for those suffering from painful metastatic cancer.”
Medtronic announced that it has recently received CE mark for its Radiant balloon-expandable covered stent, the first and currently, only, covered stent indicated for use in chimney endovascular aneurysm repair (ChEVAR) with the Endurant II/IIs stent graft system.
Used together, the Endurant II/IIs stent graft and Radiant covered stent offer a standardised, fully on-label, off-the-shelf solution for short-neck, juxtarenal abdominal aortic aneurysms (AAA). This enables safe and effective endovascular repair in both urgent and elective juxtarenal AAA cases.
The Radiant product’s design offers predictable, accurate delivery and deployment, while providing the flexibility and radial strength necessary for a chimney covered stent.
The covered stent is intended to maintain perfusion to the renal arteries when used in combination with the Endurant II/IIs stent graft system for AAA patients with inadequate sealing zones.
With this CE mark, Medtronic will roll out a comprehensive training programme and continue to invest in clinical data to optimise ChEVAR outcomes for physicians and the patients they treat.
“Having a stent graft specifically approved for ChEVAR reflects a milestone towards standardisation of the technique and the materials used. In combination with the strict preoperative protocol regarding planning and sizing, ChEVAR will stabilise its role and approach in the existing endovascular alternatives to treat aneurysms with inadequate infrarenal sealing zones,” Konstantinos Donas, head of the Department of Vascular Surgery and director of the Research Vascular Centre, Asklepios Clinic Langen, University of Frankfurt (Frankfurt, Germany) said of the Radiant stent graft.
In partnership with Getinge
The Radiant product comes from the long-term collaboration between Medtronic and Getinge, leveraging Getinge’s proven Advanta V12 design and eight sizes of the Getinge (Atrium Medical) stent portfolio. It will be produced by Getinge and distributed by Medtronic.
“To support this business expansion, Getinge has invested in doubling our stent production capacity in order to provide all of our global customers with the devices needed to treat patients,” the company’s senior director of Global Marketing and Product Management, Vascular Systems, Patty Burns, said of the partnership.
Findings from the RADIANCE II randomised pivotal trial, presented at the 2022 Transcatheter Cardiovascular Therapeutics meeting (TCT, 16–19 September, Boston, USA), “confirm that ultrasound renal denervation lowers blood pressure across the spectrum of hypertension”.
RADIANCE II—results of which were described as “important data for the field” by discussants—was the first of two major renal denervation trials reporting results at TCT 2022, with the treatment having seen a renaissance following successive sham-controlled trials showing statistically significant and clinically meaningful in blood pressure.
The trial’s primary result was presented during a late-breaking clinical science session by Ajay Kirtane (Columbia University Irving Medical Center New York-Presbyterian Hospital, New York, USA). Kirtane reported that ultrasound renal denervation using the Paradise (Recor Medical) system was superior at lowering blood pressure when compared to a sham procedure.
Patients with hypertension (seated office BP ≥140/90 mmHg and <180/120 mmHg) on no more than two anti-hypertensive medications underwent a four-week observation time during which they were taken off all hypertension medications. Those who remained clinically stable after the observation period and whose blood pressure remained elevated with daytime ambulatory systolic blood pressure (ASBP) greater than or equal to 135/85 mmHg but less than 170/105 mmHg underwent anatomic screening with CTA/MRA. Those with qualifying renal artery anatomy proceeded to renal angiography, and if angiography re-confirmed suitability for ultrasound renal denervation, they were then randomised 2:1 to receive bilateral uRDN of the main and accessory (≥3 mm) renal arteries or a sham procedure.
Between March 2019 and May 2022, a total of 150 patients received the renal denervation procedure and 74 underwent a sham procedure. Baseline characteristics including ambulatory blood pressure and the number of anti-hypertensive medications were similar between both groups.
The primary efficacy endpoint was the change in ambulatory systolic blood pressure at two months. The change in ambulatory systolic blood pressure was -7.9 mmHg for the ultrasound renal denervation group compared to -1.8mmHg for the sham group. The between group difference was -6.3 mmHg (95%CI, -9.3 to -3.2, p<0.0001. In addition, the secondary efficacy endpoints of change in 24-hour, nighttime, home, and office systolic blood pressure showed statistically and clinically significant reductions (∆5-7 mmHg versus sham). There were also no major adverse events in either group through 30 days, Kirtane reported.
Kirtane’s presentation preceded the delivery of long-term results from the SYMPLICITY HTN-3 trial, assessing radiofrequency renal denervation using Medtronic’s Symplicity system.
Deepak Bhatt
Investigator Deepak Bhatt (Brigham and Women’s Hospital Heart & Vascular Center and Harvard Medical School, Boston, USA) commented that the findings indicate that durable blood pressure reductions with radiofrequency renal denervation in combination with maximal medical therapy can be safely achieved.
In the primary report of the SYMPLICITY HTN-3 trial, at six months, renal denervation was found to be safe but did not show any significant incremental blood pressure lowering benefit compared with a sham procedure. The present analysis reports long-term blood pressure changes in both initially treated renal denervation patients as well as in a composite control group consisting of sham-treated patients as well as sham-treated patients who crossed over to renal denervation after six months (but using blinded, pre-crossover data as the control).
Eligible patients had an x ≥160 mmHg and 24-hour ambulatory systolic blood pressure ≥135 mmHg. In addition, they were on stable, maximum tolerated doses of three or more antihypertension drugs.
A total of 535 patients at 88 sites in the USA were randomised 2:1 to renal denervation using the Symplicity Flex catheter (n=364) or sham control (n=171). Unblinding occurred after six months, and eligible control patients could crossover to renal denervation. For the 101 patients who crossed over and received renal denervation, their most recent blinded pre-crossover BP measurement and medication data were used as controls. Treatment differences were adjusted for baseline blood pressure.
At 12 months, renal denervation patients had significantly greater office systolic blood pressure reductions compared with sham control after crossover imputation (-18.9 mmHg vs -6.3 mmHg, p<0.0001, respectively). In addition, the number of antihypertension drugs were similar between patients in the RDN and control groups (4.7±1.4 vs. 4.7±0.9, p=0.22). The office systolic blood pressure reductions continued each year following the procedure, and at 36 months, the reduction in blood following renal denervation was -26.4 mmHg compared with -5.7 mmHg for the control group (p<0.0001). Similar results were observed in other measures of blood pressure (office diastolic blood pressure, 24 hour systolic and diastolic blood pressure).
Sirtex Medical announced that the Brazilian National Agency of Supplementary Health (ANS) approved SIR-Spheres Y-90 resin microspheres for the treatment of intermediate- and advanced-stage hepatocellular carcinoma (HCC) in Brazil.
In an update to its List of Health Procedures and Events, ANS recommends SIR-Spheres for use in selective internal radiation therapy (SIRT), a minimally invasive treatment that delivers high doses of radiation directly to tumours while sparing surrounding healthy liver tissue. Sirtex received product approval from the Brazilian Health Regulatory Agency (ANVISA) for SIR-Spheres in 2014.
“This milestone represents the close collaboration we have fostered with Brazilian colleagues, interventional radiologists and respected regulatory entities like ANS over the last six years,” said Kevin R Smith, chief executive officer of Sirtex. “We celebrate the recognition of SIR-Spheres to advance care for HCC patients, and we also reaffirm our commitment to global growth and partnership for more effective cancer treatment worldwide.”
The proposals for incorporation into the ANS List of Health Procedures and Events underwent broad social participation and careful technical analysis by the ANS, using the methodology of health technology assessment, similar to England, Canada, Australia and Germany.
“The ANS recommendation of SIR-Spheres solidifies it as a valuable treatment option, especially since 76% of HCC patients in Brazil are diagnosed at an advanced stage when treatments of curative intent are no longer an option,” said Joaquim Maurício da Motta Leal Filho (Universidade de São Paulo, São Paulo, Brazil), president of the Brazilian Society of Interventional Radiology and Endovascular Surgery (SOBRICE). “As we continuously strive to improve outcomes for patients, we are proud of this achievement and feel gratitude to the many people who contributed to this decision.”
In addition to Brazil, SIR-Spheres are approved for use in Argentina, Australia, Switzerland, Turkey, and several countries in Asia for the treatment of unresectable liver tumours. In the USA, SIR-Spheres Y-90 resin microspheres have a Pre-Market Approval (PMA) from the US Food and Drug Administration (FDA) and are indicated for the treatment of unresectable metastatic liver tumours from primary colorectal cancer with adjuvant intrahepatic artery chemotherapy (IHAC) of FUDR (floxuridine).
L-R: Rainer Bregulla, director R&D; Sebastian Büchert, CEO; Thomas Morawek, Arnold Schwarzenegger double; Hartmut Grathwohl, director Operations; Andrew Brabner, director Finance & IT; Christian Bader, director Quality & Market Access
L-R: Rainer Bregulla, director R&D; Sebastian Büchert, CEO; Thomas Morawek, Arnold Schwarzenegger double; Hartmut Grathwohl, director Operations; Andrew Brabner, director Finance & IT; Christian Bader, director Quality & Market Access
Bentley today announced that it has acquired the rights of the GoBack catheter from Upstream Peripheral Technologies.
“The acquisition of the GoBack catheter marks the start of inorganic growth for Bentley,” said Sebastian Büchert, Bentley’s CEO. “We launched our first of six existing product families to the market in 2012 and have experienced significant growth since then. Now, only 10 years later, we are able to acquire this very innovative product. This strategic move further completes our product offering to hospitals and physicians to the benefit of our joint patients.”
The GoBack catheter will simplify crossing and re-entry in occluded arteries. A press release notes that the product’s unique feature is a curved nitinol needle that can be manipulated by the physician using the device handle. Thanks to its small profile, the device can even be used in the smaller arteries in the lower leg.
“Bentley acquiring the GoBack makes me feel proud. I am sure that with Bentley’s global footprint more physicians will have access to the catheter,” said Dan Rottenberg, CEO of Upstream Peripheral Technologies. “Our vision is to save limbs and reduce the number of amputations. With Bentley’s strong network more patients will have access to such treatment.”
The GoBack catheter is CE marked and US Food and Drug Administration (FDA) cleared. Launched in 2019, the device is now available in 23 countries. It is Bentley’s intention to extend the global availability to all of the 80 markets in which the company is already active, the press release details.
Martijn Nugteren, director Sales & Marketing, Bentley, says, “We will be really busy in the months ahead. Not only because we want to make the product commercially available in additional markets, but also due to the fact that we are going to rebrand the GoBack to BeBack. This is to make sure that our new product will be recognised as another leading product underneath Bentley’s brand umbrella.”
Currently produced in Israel and initially shipped from there, a production transfer to the Bentley production facility in Hechingen, Germany, will be completed by 2025.
Merit Medical Systems has announced the US commercial release of the Prelude Roadster guide sheath. The Prelude Roadster is the newest addition to the Merit Vascular-Peripheral Access portfolio, which includes introducers and other products, including access kits, vessel dilators, and accessories.
The device is designed for deliverability, visibility, and resilience in tortuous peripheral vasculature anatomies. Indicated for use in a variety of procedures, the device will also help deliver devices used to diagnose and treat the large patient population who suffer from peripheral artery disease (PAD).
“Patients with peripheral vascular disease often have complex vessel anatomies that make treatment challenging,” said Sandeep Nathan, interventional cardiologist and director of the Coronary Care Unit at the University of Chicago Medicine (Chicago, USA) and a consultant of Merit Medical. “The Roadster sheath is designed to help physicians deliver the diagnostic and therapeutic devices needed to achieve successful outcomes.”
“The Prelude Roadster is an example of Merit’s commitment to understanding, innovating, and delivering products to meet the needs of physicians. After decades of offering vascular access products, we are always searching for ways to help physicians diagnose and treat successfully, improving the lives of patients worldwide,” said Fred P Lampropoulos, Merit Medical’s Chairman and CEO.
ABK Biomedical has announced US Food and Drug Administration (FDA) 510(k) clearance of Easi-Vue embolic microspheres for the treatment of patients suffering from arteriovenous malformations and hypervascular tumours.
Aravind Arepally, chief medical officer of ABK Biomedical said: “The evolution of embolic therapies to treat these complex disease states has been notable in recent years. Now, with Easi-Vue embolic microspheres, interventional radiologists have a highly calibrated, see-and-do technology capable of visually targeted placement using conventional X-ray and fluoroscopy systems. This microspheres technology and proprietary controlled-concentration delivery system have the potential to improve patient outcomes.”
“We are excited to achieve FDA 510(k) clearance for this new technology that has the potential to advance the field of embolic therapies”, said Gary Donofrio, chief business officer of ABK Biomedical. “This represents a major milestone for ABK as our team continues to execute our product development objectives. We will partner with key physicians to understand the range of clinical utilisation and optimisation of Easi-Vue therapy. Additionally, ABK continues to significantly advance the development programme of our Eye90 microspheres radioembolic technology that is being investigated for the treatment of patients with unresectable hepatic cellular carcinoma (HCC). Easi-Vue embolic microspheres share core technologies and design characteristics with Eye90 microspheres. Both devices continue to add to our knowledge base regarding the clinical experience of the first glass radiopaque embolic microspheres therapy.”
Interventional News’ popular stories last month included acquisitions by Boston Scientific and Gore, studies of deep vein thrombosis and peripheral arterial disease treatments and, on the subject of the latter, research into the racial disparities affecting patients who receive peripheral vascular interventions. Stories covering data presented at two of the summer’s meetings—Society of Interventional Radiology (SIR) and the European Conference on Embolotherapy (ET)—also garnered ample views.
Boston Scientific has announced the acquisition of Obsidio, a privately held company that has developed the Gel Embolic Material (GEM) technology used for embolization of blood vessels in the peripheral vasculature.
Inari Medical has announced planned enrolment of the DEFIANCE randomised controlled trial (RCT), which is designed to compare the clinical outcomes of patients with iliofemoral deep vein thrombosis (DVT) treated with the ClotTriever system versus anticoagulation only.
BD has announced the start of enrolment in a first-in-human trial of a peripheral sirolimus drug-coated balloon (DCB). The PREVISION trial is a prospective, multicentre, single arm, non-randomised study designed to evaluate the safety of the BD sirolimus DCB in the treatment of peripheral arterial disease (PAD) in the femoropopliteal arteries.
Fluidx Medical disclosed study results examining extent of vessel filling using the GPX embolic device compared to microspheres, a common treatment for many types of tumours.
A database study titled ‘Unplanned 30-day readmissions and in-hospital outcomes for the management of submassive and massive acute pulmonary embolism: Catheter-directed versus systemic thrombolysis’ has produced results that could provide some of the evidence base for preference of catheter-directed over systemic thrombolysis in treating the more severe cases of pulmonary embolism (PE).
Mark Little (Royal Berkshire NHS Foundation Trust, Reading, UK) described the emergence of, and advancement within, musculoskeletal (MSK) embolotherapy as “fast-paced” during a presentation at this year’s ET (22–25 June, Nice, France). The take-home message was that the “signs are encouraging” when it comes to MSK embolotherapy’s integration into more mainstream practice.
Ramona Gupta (Northwestern University, Chicago, USA) addresses the issue of recurrent varicose veins, highlighting in particular the “multiple tools” now at physicians’ disposal to treat the problem.
Gore has announced the acquisition of InnAVasc Medical, a privately held medical technology company focused on advancing care for patients with end-stage renal disease who utilise graft circuits for dialysis treatment.
Interventional News spoke to Eric A Secemsky and Anna K Krawisz (Smith Center for Outcomes Research in Cardiology, Beth Israel Deaconess Medical Center, Boston, USA)—about the motivations for carrying out their study into racial disparities in peripheral vascular interventions, the results it yielded, and where this research might lead.
Concept Medical has announced the initiation of the LIMES trial, which has enrolled 15 patients to evaluate the safety and efficacy of the company’s Magic Touch sirolimus-coated percutaneous transluminal angioplasty (PTA) balloon for the treatment of peripheral arterial disease (PAD).
This advertorial is sponsored by Interventional Systems.
At the onset of the COVID-19 pandemic in early 2020, healthcare systems across the globe were forced, almost overnight, to adapt to a new reality. No corner of the healthcare landscape has been left untouched, and the ripple effects of the pandemic have changed the financial reality for care providers everywhere.
“Capital equipment sales are always a long-term process, with budgeting and approval processes,” Scott Peairs, vice president of Global Sales at Interventional Systems, tells Interventional News. “The pandemic made that worse with a diversion of capital assets towards the treatment of COVID-19 patients.”
This has prompted a realignment in the way that hospitals and healthcare facilities approach the procurement of new technologies and devices, and creates a potential hurdle to investment in cutting-edge treatment solutions. For Interventional Systems, the developer of Micromate—a table-mounted medical robot for interventional procedures—this represents a particular challenge as hospitals refocus their spending priorities, and capital expenditure on new technologies becomes more difficult.
Micromate suite
“Only equipment that was broken or was desperately needed was being purchased under the capital price,” comments Peairs, adding that since the start of the pandemic, many providers have become wary of making capital investments, seeking more flexible solutions instead. “We are starting to come out of that cycle now and hospitals are starting to get back on more of a standard capital cycle, but we are probably another year away from normal.”
As a result of this, hospitals may be missing out on the opportunity to access new technologies that will smooth workflows and improve outcomes for patients through high-quality care. To address this, Interventional Systems has sought to deliver a service that will allow hospitals to still have the opportunity to offer the innovative Micromate robotic system to their patients, albeit without the initial capital outlay that is usually involved in this kind of procurement.
“We wanted to offer a way that, if the hospital does not have the budget but wants to use a robotic system, we can offer them a subscription model,” Peairs explains. The subscription model—which Peairs says is relatively unique to the healthcare technology setting—works in a similar way to how users purchase software packages.
“Microsoft or Adobe are the best examples,” he explains. “You used to have to go and buy the software, it was loaded to a hard drive on a computer, and then you would have to go and buy an upgrade for it. The software companies have completely moved to the subscription model, where it is virtual. You get the free upgrades, it is accessible, and you can turn it on and off when you want to.”
A flexible option
One of the potential advantages of this model is, according to Peairs, the fact that healthcare providers will have the flexibility to incorporate an emerging technology into their practice, without the long-term outlay that comes with a commitment to capital expenditure on new equipment. And, with a subscription-based service, getting hold of a robotic system may be a more streamlined process, Peairs says, as the subscription may not fall into the capital expenditure category, meaning that the physician can incorporate the cost into the budget that they already control.
Scott Peairs
“The idea is that we want to give them access to it,” Peairs tells Interventional News. “They can have a system and they are not obligated for the long term, that gives the physician access to it. From there, they can explore internally if it adds value to the procedures within their facility.” Additionally, without the initial outlay of the capital cost of the system, hospitals can potentially reap the efficiency gains that can be achieved by deploying the Micromate system, quicker.
Interventional Systems offers three different subscription models that are structured depending on the volume of procedures to be performed using the robotic platform and the duration that the healthcare provider wishes to sign up to. The centre pays a fixed amount per month, which covers the disposable components that are needed for each procedure, as well as software updates that may occur during the subscription time and technical assistance during the first cases.
As these core services are essential, they are covered within each of the three packages on offer, however, customers can opt to get access to more whenever needed, and have the option to upgrade or downgrade their subscription at any time. Furthermore, the system requires no preventive maintenance and the customer pays for service only outside warranty, and when needed. “To go back to the Microsoft analogy—it updates itself, you do not have to do service, you do not have to do training—it is all included in that subscription,” says Peairs.
Setup and training are also important aspects of the provision, which are delivered to clients at the outset of the subscription. Interventional Systems offers service support to troubleshoot any issues that may arise, and can centrally access the system via a remote interface. If hardware repairs are needed, Interventional Systems offers a “swap-out” facility whereby faulty components are replaced to reduce downtime.
Learning curve
As Micromate is a system that can be used in a number of different procedures on different organs, Interventional Systems says that there are several factors that will affect how long it may take to master the system. “A lot of it depends upon the type of procedure that they are doing,” says Peairs, adding that learning to use the platform in lung, kidney or liver tissues—the primary interventional radiology target areas—may have different requirements. From experience, and though it changes from physician to physician and centre to centre, five procedures is generally a good rule of thumb for getting to grips with the system, that he describes as a “third arm” for the operator.
“Some of the interventional radiologists have told us that they would use it on the hard cases because that is where they would think they would have the need,” Peairs adds, commenting on the learning curve involved in mastering the robot. “Now the mindset has shifted and several of them have told us that they are going to use it on every case, even the simplest of biopsies, because of its fast setup.
“They want to use it on easy cases so the staff know the workflows and the setup using the robot, so that once they get to the hard cases that is not a stressor. I really see that is where a subscription model is going to help, because it is going to allow them to use it on all cases,” he says.
The subscription model will be available to Interventional Systems’ customers in the USA and Europe from Autumn 2022.
The European Society of Cardiovascular and Interventional Radiology (CIRSE) will host its 38th annual meeting in Barcelona from September 10 until September 14. Around 5,000 healthcare professionals from around the world are expected to attend more than 400 lectures in person, while a custom-built online platform will allow full digital access to all lectures and symposia for those unable to make it to Barcelona.
Living up to its motto “Science for people”, CIRSE 2022 will have two main foci: increasing the evidence base for interventional radiology, and continuing to make interventional radiology (IR) a clinical, patient-centred discipline. Two FIRST@CIRSE session will contribute to IR’s evidence base with the largest number of data releases of IR studies to date—one session focusing on studies in peripheral arterial disease treatment and a second session presenting data releases on other treatments.
Other session highlights will include those comprising PAD Day, the Interdisciplinary Endovascular Aortic Symposium (IDEAS), as well as various sessions focusing on paediatric interventions.
The CIRSE 2022 Local Host Committee headed by Mariano Magallanes Bas (Hospital Ribera Povisa, Vigo, Spain) has organised a patient information exhibition with the title “The medicine of today”, which will take place throughout the congress in the nearby shopping mall Diagonal Mar with the aim of increasing popular awareness of the specialty. Using laymen’s terms and appealing images, the exhibition will give the general public an introduction to the wide array of conditions that can be treated by interventional radiologists, from uterine fibroids to benign prostate hyperplasia, highlighting both the state-of-the-art nature of IR treatments as well as the specialty’s human, clinical side.
The Micromate robot for percutaneous interventions
The Micromate robot for percutaneous interventions
Interventional Systems haslauncheda newsubscription servicefor Micromatewith three package levelsofferingthe miniature robotic system including the latestplanning and navigation station, as well as disposable accessories and specialised services. The subscription fee is fixedand there are nomandatory service agreements, making the costs as predictable and low as needed.
“The cost of technology is responsible for half of the increase in healthcare–related costs worldwide. This can help explainwhy only up to 3% of surgeries and interventions are performed with robotic assistance, despite its obvious advantages”, says Pedro Costa, chief product officerat Interventional Systems.“The word democratisation is ubiquitous in brochures, publications,slide decks,and websites. Every new player in MedTech democratises something, just to proceed by charging you a million euros for a robot, disposables that cost you thousands,and mandatory service agreements of at least 8% capital cost. Our understanding is different. We want to ensure true access to every physician and, ultimately, patient.”
“Healthcare providers are looking for more flexible solutions”, adds Scott Peairs, vice president of global sales at Interventional Systems. “With a subscription–basedservice,they canhavetherobotic systemfor as long and as many procedures as they need.And because they are spending each month only a fraction of the capital cost of the robot, they can also leverage the increase in efficiency to generate profits faster and get a better return on investment.”
The Micromate subscription is available in the USA and Europe as of September 12022, with plans to expand globally.
Penumbra announced today that its RED reperfusion catheters have secured a CE mark and are now commercially available in Europe. The catheters are part of the company’s Penumbra system, which is a fully integrated mechanical aspiration thrombectomy system designed to restore blood flow in acute ischaemic stroke patients.
“When addressing stroke, our goal is to remove the blood clot as quickly as possible for patients to have the best outcome,” said Saleh Lamin (Queen Elizabeth Hospital, Birmingham, UK). “With RED catheters, we will be able to get up to the clot quickly and efficiently remove it, most of the time within a single pass. Restoring blood flow promptly is key as it is associated with less damage to the brain and better outcomes.”
The RED family of catheters is engineered with the latest technology in trackability and aspiration to address a wide range of large vessel occlusions via mechanical aspiration thrombectomy, a Penumbra press release notes.
The RED catheters feature the company’s REDglide technology—which enhances the trackability of the catheters as they navigate the challenging vessel anatomy of the brain while also maximising aspiration efficiency to remove blood clots. Additionally, the RED catheters have a full-length polytetrafluoroethylene (PTFE) liner designed to maintain their true lumen size under powerful vacuum, the release adds.
“Penumbra’s commitment to advancing technology allows us to have one of the most expansive aspiration stroke portfolios on the market, enabling physicians to have the latest innovations with the most options to provide the best care to their patients,” said Joan Kristensen, vice president and head of the Europe, Middle East and Africa region for Penumbra. “With enhanced trackability and powerful aspiration, initial data have shown that Penumbra’s RED catheters can restore blood flow quickly across all clot types, which would potentially have a significant impact on patient outcomes here in Europe.”
Royal Philips today announced new milestones in the development of the world’s first spectral detector angio computed tomography (CT) solution— Philips Spectral Angio CT suite—bringing the company’s breakthrough spectral CT imaging technology into an integrated hybrid angio CT suite. By combining its Spectral CT 7500 system and the image-guided therapy system—Azurion with FlexArm—in a fully integrated interventional suite solution, Philips aims to give physicians immediate access to these two key imaging modalities in a single room, enabling innovation in minimally-invasive procedures in areas such as oncology, stroke, and trauma care.
Expanding Philips’ clinical network
Leiden University Medical Center (Leiden, The Netherlands) has joined Philips’ global network of clinical partners to investigate how its spectral detector angio CT solution could offer new treatment opportunities and improve patient care.
“We are excited to co-create an innovation that could play a defining role in improving patient care in the space of interventional oncology,” said Mark Burgmans, head of Interventional Radiology at Leiden University Medical Center. “Adding spectral CT imaging to the interventional suite will enable us to offer new treatment opportunities, avoid moving patients from one imaging suite to another, and offer the unique benefits of spectral CT information when you need it.”
Philips is also working on its innovation with Mayo Clinic (Rochester, USA) and Baptist Health’s Miami Cardiac & Vascular Institute (Miami, USA).
Philips Spectral Angio CT suite combines the company’s latest diagnosis and treatment technologies. Philips Azurion with FlexArm is the company’s next-generation image-guided therapy platform, integrating best-in-class imaging systems, software, and specialised diagnostic and therapeutic devices to support exceptional treatment for the most complex procedures. The addition of Philips’ award-winning Spectral CT 7500 system means physicians only need one scan to capture all the spectral information required to differentiate and quantify different tissues. Spectral CT enables improved detection, delineation, and quantification of lesions, leading to better-informed planning for minimally invasive procedures and more precise interventions.
It has already demonstrated higher sensitivity in detecting malignant findings and improved readings of incidental findings. With its ability to improve tissue characterisation, the Spectral CT 7500 offers significant benefits over conventional CT, the company states.
Research results show better targeted biopsies using spectral CT guidance
At this year’s Cardiovascular and Interventional Radiological Society of Europe Annual Meeting (CIRSE 2022; September 10–14, Barcelona, Spain) Filippo Piacentino, interventional radiologist at the University of Insubria (Varese, Italy), is giving a presentation on the value of spectral CT imaging guidance for performing high-confidence tumour biopsies. The results being presented illustrate the potential for Philips’ spectral CT technology to better guide biopsies by distinguishing between active and non-active regions in a tumour.
“With conventional CT, large masses may appear as a largely uniform mass, making highly targeted biopsy difficult,” said Filippo Piacentino. “By fusing images from Philips’ XperGuide live needle guidance with images from spectral CT, that are colour-coded based on the effective atomic number of tissues, and provide a large amount of additional information, we can now investigate the possibility of obtaining better defined biopsy targets with a fewer number of inconclusive biopsies.”
New clinical collaboration on reduction of the risk of tumour recurrence
Philips also announced a research collaboration with the University of Pennsylvania (Philadelphia, USA) to study the practicality of using spectral CT-based tissue temperature mapping to provide real-time feedback during tumour thermal ablation procedures to confirm its effectiveness before the patient leaves the room. This will potentially reduce the risk of localised tumour recurrence.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) recently incorporated transarterial chemoembolization with degradable starch microspheres (DSM-TACE) into its guidelines for hepatic transarterial chemoembolization.¹ In addition to society backing, experts are also in favour of this treatment modality, underlining its role as a game-changing addition to the liver cancer care paradigm.
Speaking to Interventional News, Roberto Iezzi, associate professor of Radiology at the Catholic University of Rome (Rome, Italy) and Christiane Kuhl, head of the Department of Radiology at Aachen University (Aachen, Germany), share their clinical experiences with EmboCept® (PharmaCept®) and how the European guideline update solidifies its place in liver cancer treatment by TACE.
Roberto Iezzi
“EmboCept consists of a suspension of starch microspheres that are rapidly and completely degradable within 90–120 minutes² (in vitro half-life time 30–40 minutes) from the arterial infusion, allowing a temporary occlusion of the arterial microcirculation at the tumour level,” Iezzi explains, giving an overview of EmboCept’s mechanism of action. This, he says, improves the therapeutic effect by reducing the immediate wash-out of the cytostatic agent, and decreasing the risk of systemic toxicity and post-embolic syndrome.
EmboCept is also characterised by a cross-linked, partially hydrolysed starch matrix that allows the interventionalist to obtain a ready-to-use solution with different chemotherapeutic drugs being mixed with them. Iezzi recalls how this feature positively impacted his practice: “This option allowed us to open the door in the last few years for new indications, for liver metastases from lung, breast and gynaecological tumours, for example. You can now use EmboCept with any cytostatic that can be given intra-arterially, allowing [the interventionalist] to be much more flexible and broadening the range of indications.”
Christiane Kuhl
Kuhl notes that the current CIRSE recommendation reflects the current level of evidence, but is still conservative regarding the patient cohort included. She states: “Maintaining liver function is decisive for a patient’s treatment as well as survival. A patient needs a working liver, both to survive, but also because an adequate liver function is a prerequisite for most systemic treatment protocols.” In patients with metastatic solid tumours, metastatic overgrowth of the liver can thus become the driver of a patient’s prognosis. Kuhl highlights that interventionalists now have the tools to help the liver fight against this metastatic overgrowth in addition to systemic treatment. “With systemic treatment, often in the liver, the dose is simply not high enough to stop the cancer,” she says, stressing that in these patients, palliation of liver function through local treatment is key, and is the major goal of liver-directed treatment. “This is similar to the local treatment of osseous metastasis to a vertebral body, where the intention is to palliate the static function of the bone,” Kuhl adds. “Similarly, in patients with secondary liver cancer, the aim is to palliate the liver. We are able to do that with EmboCept-driven transarterial chemotherapy”.
In the field of embolic agents, both interventionalists are in agreement that EmboCept holds its ground, providing a solid treatment option and in some cases offering advantages over alternatives. “I think the most obvious advantage of EmboCept compared with other embolic agents is the fact that it only causes a temporary occlusion, maintaining the route to the tumour,” Kuhl opines. She believes this is crucial in the treatment of liver cancer other than hepatocellular carcinoma (HCC), where the main method of action may not be devascularisation, but in bringing the chemotherapeutic agents into the tumour. Kuhl elaborates: “Everywhere we want to treat chemo-sensitive cancer in the liver, these agents must be applied not only once, but repetitively—just as is usual practice with their systemic use. In such patients, temporary occlusion of vessels by degradable starch microspheres allows one to keep the route to the tumour patent for several courses of transarterial chemotherapy.” Such TACE should only temporarily occlude the vessels to avoid passage of the chemotherapeutic or cytotoxic agent through the tumour, but ideally keep it inside the tumour.” This is what EmboCept achieves in a perfect way,” Kuhl remarks.
According to Iezzi, DSM-TACE can offer benefits where other TACE options, namely drug-eluting bead TACE (DEB-TACE) and conventional TACE (cTACE), are not indicated. “DSM-TACE is safe, without side effects or worsening of liver function. It is also safe in advanced HCC patients, with the worst clinical conditions (Child-Pugh>B7), vascular invasion (portal vein thrombosis), high bilirubin level or ascites—patients in whom DEB or cTACE could be contraindicated,” he relays.
Overall, however, it is Iezzi’s opinion that DSM-TACE is not necessarily in competition with DEB or cTACE, but provides another treatment option that interventionalists can offer to their patients, thereby widening clinical indications and improving disease prognosis overall. Iezzi adds that DSM-TACE “could also be used as a bridge to other locoregional or surgical options as it is effective and repeatable (so called bridging and downstaging) being able to maintain vessel patency”.
Figure 1. Preprocedural (A, B) and postprocedural (C, D) CT images of a 68-year-old patient with unresectable multinodular bilobar HCC treated successfully with DSM-TACE. The patient showed >6 hepatic lesions, the largest of which was 7cm (A and B). DSM-TACE procedures were performed with a selective lobar catheterisation and with a coaxial technique placing a 2.7Fr microcatheter in the right or left hepatic artery that was feeding the tumour lesions. A solution of 450mg in 7.5ml of EmboCept S mixed with 50mg of Doxorubicin and non-ionic contrast medium was slowly infused. The patient experienced no adverse events, with dismission after 24 hours, without any pain or periprocedural complications. Since the CT follow-up performed after three months showed an almost complete response with necrosis of almost all multinodular liver lesions (C, D), the patient received two more DSM-TACE sessions. (Case: R. Iezzi)
CIRSE’s approval of DSM-TACE has solidified its place as “an important pillar of tumour treatment,” says Kuhl. In recent years, a number of papers have been published that highlight the role of DSM-TACE in HCC, and all of these have contributed to the acceptance of DSM-TACE in the CIRSE guidelines. For example, Iezzi was part of a team that recently published a multicentre European study confirming that DSM-TACE is well tolerated with no major clinical adverse events and only limited major laboratory events.³ He tells Interventional News that preserved liver function was observed after repetitive DSM-TACE treatments in this study. “Our results confirm that repetitive DSM-TACE is a safe, well tolerated and effective treatment option for HCC patients with high tumour burden, ineligible for, or failing other palliative therapies,” said Iezzi, relaying the key take-away message from the paper.
“Guidelines are what drive clinical patient care,” Kuhl states, underlining the significance of the CIRSE update. DSM-TACE is now an accredited treatment option and this, according to Iezzi, “widens indications for locoregional treatments and gives new opportunities to patients”. In addition, he believes that the guideline update might convince all interventional radiologists, hepatologists and oncologists who were doubtful of the important role of DSM-TACE in the treatment of liver cancer.
References 1. Lucatelli P, Burrel M, Guiu B, et al. CIRSE standards of practice on hepatic transarterial chemoembolisation. Cardiovasc Intervent Radiol. 2021; 44 (12): 1851–1867. DOI: 10.1007/s00270-021-02968-1. 2. Wiggermann, P, Heibl M, Niessen C, et al. Degradable starch microspheres transarterial chemoembolisation (DSM-TACE) of HCC: dynamic contrast-enhanced ultrasonography (DCE-US) based evaluation of therapeutic efficacy using a novel perfusion software. Clin. Hemorheol. Microcirc. 2012; 52 (2–4): 123–129. DOI: 10.3233/CH-2012-1590. 3. Ludwig, JM, Iezzi R, Theysohn JM, et al. European multicenter study on degradable starch microsphere TACE. The digestible way to conquer HCC in patients with High tumor burden. Cancers. 2021; 13 (20).
Andrew Wigham (Oxford, UK) and Rick De Graaf (Friedrichshafen, Germany) discuss the current state of deep vein thrombosis (DVT) treatment at the Leipzig Interventional Course (LINC) 2022 (6–9 June, Leipzig, Germany), with both noting that “a massive problem” in Europe is the lack of awareness around treatment.
Wigham highlights some of the major challenges associated with treating this patient population, including that “traditional devices have a limited window of effective treatment of acute DVT”, as well as “limited operating room time and bed availability” due to the COVID-19 pandemic, and “significant bleeding risk to the patient” with thrombolysis. “We are really in need of solutions to address these issues”, he adds.
“We do not want to do thrombolysis anymore,” states De Graaf, when questioned on his preferred treatment modality. “We went through all the devices out there and my major problem was always that I could not get all the thrombus out,” he says, adding that “thankfully now I am finally very confident that I have a device [ClotTriever, Inari Medical] that takes out all the thrombus.” Wigham himself adds that ClotTriever is “a very effective device that helps us to clear the thrombus and potentially limit the amount of stents we are using in a young patient cohort.”
Wigham goes on to say that one of the principle advantages of the device is that he has found it to be “effective out beyond six weeks”. De Graaf adds that this is “a huge benefit that we see as well”, with the pair concluding that the device is a real “gamechanger” for the treatment of DVT.
This video is sponsored by Inari Medical.
Rick de Graaf and Andrew Wigham will be sharing their experiences with ClotTriever® for the treatment of deep vein thrombosis during the Inari symposium at CIRSE 2022 (Sunday, 11th September, 1pm–2pm, room 114).
Fluidx Medical announces completion of trial enrolment for its GPX embolic device. In this multicentre trial, GPX was used to treat a variety of primary and metastatic tumours, renal adenoma tumours, and a range of other arterial and venous applications.
“We are pleased to announce the enrolment of the final patient in the trial and look forward to participating in future trials using this promising technology,” stated the trial’s principal investigator, Andrew Holden (Auckland City Hospital, Auckland, New Zealand.) “In the trial, GPX showed significant potential to advance liquid embolics, penetrating very distally, providing profound embolization, and demonstrating excellent radiopacity which helped to avoid non-target embolization and preserve healthy adjacent tissue.”
GPX has shown promising results for tumour embolization and other uses where there is a desire for distal vessel bed penetration. Embolization is a procedure in which arterial or venous blood supply to an organ, malformation, aneurysm, bleed, tumour, and/or other abnormal area of issue is blocked.
L: baseline image of contract flowing through tumour-feeding vessels of pelvic tumour. R: GPX embolization of a pelvic tumour’s largest feeding vessel.
Interim results of the GPX study have been presented at recent annual congresses including Global Embolization Symposium & Technologies (GEST), Society of Interventional Radiology (SIR), and Leipzig Interventional Course (LINC).
Holden concluded, “We’ve only touched on some of the applications. Further trials will provide opportunities to look at broader applications of this product. We believe it will be an exciting addition to the embolic portfolio for interventionalists.”
GPX is an innovative embolic designed for simple preparation and controllable material delivery. The device is packaged ready-to-use in a syringe, can be prepped tableside by the clinician in about 30 seconds, and may be delivered through standard microcatheters (no complex mixing systems or special delivery catheters are necessary). GPX technology is a low viscosity, aqueous-based solution in a syringe that solidifies into a durable embolus upon delivery without polymerisation or dimethyl-sulfoxide (DMSO) precipitation.
Inari Medical has announced planned enrolment of the DEFIANCE randomised controlled trial (RCT), which is designed to compare the clinical outcomes of patients with iliofemoral deep vein thrombosis (DVT) treated with the ClotTriever system versus anticoagulation only.
The trial will enrol 300 patients at up to 60 centres worldwide. DEFIANCE is Inari’s second RCT and it will run in parallel to the PEERLESS trial. PEERLESS commenced earlier this year and compares FlowTriever to catheter-directed thrombolytics in pulmonary embolism.
“Anticoagulation is still the predominant therapy used in the management of DVT and in some studies has been associated with post-thrombotic syndrome (PTS) in up to 50% of patients,” said Steven Abramowitz (MedStar Health, Washington, DC, USA), co-principal investigator. “PTS is a debilitating condition with symptoms including swelling, difficulty walking, skin changes and poorly healing open wounds. Research has shown PTS quality of life scores can be as low as those of patients suffering from heart failure or cancer. Mechanical thrombectomy procedures, using technology like ClotTriever, rapidly remove large volumes of DVT and may thereby reduce the risk of PTS.”
“DEFIANCE is the first RCT to compare mechanical thrombectomy to anticoagulation for the treatment of DVT,” said Xhorlina Marko (Beaumont Health, Dearborn, USA), co-principal investigator. “The primary endpoint for the trial is a hierarchical composite of treatment failure and PTS severity at six months. The trial has the potential to influence guidelines and change the standard of care.”
“Physicians need to know in which patients to use our devices and what outcomes to expect. This is our basic responsibility,” said Thomas Tu, Inari’s chief medical officer. “We have studied over 2,000 patients, published 250 peer reviewed publications, and DEFIANCE marks our sixth major clinical study. These high-quality studies will establish a new standard of care for patients and further distance us from competition.”
Ablation is used to destroy or shrink tumours in the liver, lung, kidney, bone, and other organs. In recent decades, image-guided ablation has become integral to modern cancer therapy with curative or palliative intent. Although a promising treatment option, the main challenge is the accurate and safe positioning of the ablation probes to achieve complete tumour coverage, especially in difficult-to-access localisations. The CAS-One® IR system (CASCINATION AG) and its AblaSure®margin assessment software aim to improve the reproducibility, reliability and accuracy of ablation procedures for liver, lung, pancreas, kidney and bone. It enables more patients, and those whose cases are more challenging, to be treated, and to reduce rates of recurrence and procedural complications.
Quality Ablation with the CAS-One IR System
Martin Hoffmann (St Claraspital, Basel, Switzerland) and Shaheen Noorani (Hampshire Hospitals NHS Foundation Trust, Basingstoke, UK) have experience using CAS-One IR with AblaSure to ablate advanced tumours where single or multiple electrodes are required to treat the tumour adequately. They believe that lesions can be targeted more accurately using the navigation system compared to the traditional manual ablation. Hoffmann and Noorani spoke to Interventional News about their experiences using CAS-One IR with AblaSure and contextualise these in the broader landscape of ablation, as well as detailing how, and for which patients, the CASCINATION offering yields advantageous ablation results.
Hoffmann begins by stipulating that he has around five years’ experience with CAS-One IR, which contrasts with Noorani’s more recent incorporation of it into her practice. Hoffmann recalls being asked, when he started in his current hospital, whether he could find some way of treating large kidney- and liver-dominant tumour masses? This stemmed from the fact that, as Hoffmann elaborates, “we would see patients [who could not be treated systemically] declined from our surgical services.” So, CAS-One IR provides a solution for treating these “more challenging lesions in challenging locations” as Noorani puts it, illustrating that the pair share motivations for using the technology. Both Hoffmann and Noorani spoke of the advantage of achieving standardised ablation that is consistent from one patient to the next, and also from one interventional radiologist (IR) to the next.
Martin Hoffmann
Asked about the challenges involved in using conventional ultrasound or computed tomography (CT) freehand ablation, Hoffmann reframes his response from the outset: “it is not so much a limitation of CT or ultrasound,” but the ablation modalities. He then explains that “one of the prerequisites of [using NanoKnife electrodes] is that they must be arranged parallel around the tumour,” which is very challenging manually. The CASCINATION system also has the advantage of allowing the use of “an un-bordered array of microwave antennae” that work in tandem “to cover a large tumour volume, [ablating] section by section” in many different positions during the same procedure. Similarly, Noorani points to the issue of having “[to eyeball] the targeted ablation zone and needle position” when carrying the procedure out manually, which means that the “technical ability” of the IR is a “huge factor” in dictating how successful the outcome is. Furthermore, IRs encounter the issue of not being able to see the “invisible lesions” on CT that do show up on magnetic resonance imaging (MRI) scans—ablation of those lesions freehand is, consequently, impossible. Yet, Noorani clarifies that CAS-One IR resolves this problem, “[fusing] the MRI scans to the CT images.”
Shaheen Noorani
While CAS-One IR is versatile and usable with all ablation modalities and suitable for liver, kidney, lung, bone and other organs, it is AblaSure that adds value for patients, Noorani then shared, as being able to do margin assessment alongside the ablation means “we can re-treat on the same day, rather than bringing the patient back.”
Continuing in a similar vein, Noorani outlines where CAS-One IR holds potential economic value for healthcare providers. “Patients with deep-seated lesions would, in the past, have had a hepatectomy,” she begins, but as there is now the option for ablation with CAS-One IR, “[there will be fewer large operations, which] will ultimately mean reduced length of stay, [less] need for intensive care beds, and reduced wait for open theatre procedures.” Workflow can also be managed better in a hospital with the length of procedure time being shorter and less variable, as “more challenging lesions can be done in a timelier manner,” and the increased accuracy of ablation with CAS-One IR means that, in time, Noorani “[hopes] to see a reduction in patients having repeat ablations.” Moreover, “a larger cohort of patients can be treated with curative intent,” to the same end.
A case from Noorani: Trajectory plan, needle verification, AblaSure confirmation
On the hot topic of attaining sufficient margin, Hoffmann emphasises that there is, indeed, “huge demand for safety margin verification and that can only be achieved with a navigation system, such as CAS-One IR.” Image overlay, which is the means of verifying margins without such a system, is flawed, Hoffmann continues: “it can torque the kidney and liver,” and only works where there are “very advanced algorithms” at play. Noorani concurs, adding that post-ablation assessment is also “becoming more and more important […] economically to reduce re-ablation rates.”
A summarising remark from Noorani is that CAS-One IR allows for targeting lesions “at angles not previously achievable,” and this advantage is supplemented those conferred by the fusion software capabilities. Hoffmann’s own parting message is that, where in the past, ablation may have been prized by its practitioners as an art form, what IRs want now is to have “reproducible and accurate results.” Backing up his assertion with anecdote, Hoffmann stated that he finds it “embarrassing to go to a multidisciplinary tumour board meeting and be presented with evidence that there is a new tumour growing at the back of the ablation scar.” CAS-One IR is a means to avoiding such unsavoury scenarios, he concludes.
You can read more about Quality Ablation and CAS-One IR at www.cascination.com
Alban Denys is a French-Swiss interventional radiologist who was one of the founding members of the Society of Interventional Oncology (SIO). He has held the position of chairman of the European Conference on Interventional Oncology (ECIO) and developed and patented a chemoembolization method that includes anti-angiogenic agents. Passionate about mentorship and giving up-and-coming interventional radiologists quality fellowship opportunities, Denys is head of diagnostic and interventional radiology (IR) at the Centre Hospitalier Universitaire Vaudois (CHUV) in Lausanne, Switzerland. Interventional News spoke to him about his career highlights, research interests, and what is required to succeed as an interventional radiologist.
What attracted you to a career in IR?
I actually discovered IR by chance during my residency. I was lucky enough to be working at the Gustave Roussy Institute (IGR) under the supervision of Alain Roche with a bunch of other young fellows. At the IGR, I discovered a brand new field of medicine where image guidance could facilitate effective, yet less minimally invasive treatment. I had also found myself a little frustrated by diagnostic radiology, where there is not much close patient contact. IR was a way to be more directly involved in patient care.
Who were your mentors?
I am lucky to have had fantastic radiology mentors. Alain Roche in Paris and Michel Lafortune in Montreal have really impacted my work. Both are extremely patient-centred and are highly respected both in and outside of their specialty. Michel Lafortune has also shown me that academic medicine—coming up with ideas, and designing a study, and then publishing it—can bring me a lot of joy. I also love the interventional oncology (IO) family that I have met over the years: Bradford Wood, Riad Salem, Ricardo Lencioni, Patrick Chevallier, Thierry de Baere, Afshin Gangi, they are more than colleagues; we have had this shared adventure in the development of IR and IO. I have also welcomed fantastic fellows to Lausanne—the stars of today and tomorrow—including Rafael Duran and Boris Guiu, who are working together on CIRSE’s (Cardiovascular and Interventional Radiology Society of Europe) Interventional Oncology for Immuno-oncology (IO4IO) initiative.
Could you describe a particularly memorable case of yours?
The day that my oldest daughter came to the world, I received a call from my chief nurse whose daughter-in-law had just given birth to twins in a small clinic in a Parisian suburb. She had had a very severe form of postpartum haemorrhage, and she also had a coagulation disorder. The obstetrician had already left for the weekend and the ambulance could not transport her to the hospital because she was so haemodynamically unstable. I ended up embolizing her successfully in a very basic radiology room without any angiographic facilities, in the small clinic she was in. This was probably the most emotionally intense day of my entire life— there was the extreme happiness I felt at the arrival of our newborn, and then the stress of this intervention. I have kept a ‘basic embolization kit’ in my car ever since.
What are the most challenging aspects of using IR techniques to diagnose and treat liver cancers?
The real challenge is to develop an oncologic approach; to work out when best to perform an IO treatment, you actually have to develop skills and knowledge in both surgery and oncology. Our techniques have had to demonstrate their validity through strong medical evidence, too. Designing a trial, finding the money to run the trial and recruiting patients, all of these are tricky tasks.
Alban Denys
This year’s ECIO featured the first IO foundation course—what is the significance of this for the future of IO and its practitioners?
This brings me back to my previous comment. We have to have an open dialogue with the oncologists we work with. This means understanding how they work and seeing things from their perspective, to then offer our solutions for the patients, at the right point in their treatment. But we should also be able to challenge oncologists’ decisions sometimes. And you can only do this if you have an in-depth knowledge of oncology. The IO foundation course is intended to equip our younger colleagues with this knowledge.
You patented chemoembolization composition including anti-angiogenic agents, which was then licensed for use in the VERONA study, now completed. What was the patent process like from your researcher’s standpoint?
Developing a new therapeutic concept, and building the preclinical evidence was extremely challenging. However, this was a lot of fun, even if finding money for experiments, going through the process of patenting, and then trying to license the product, was as exciting as it was difficult. In the end, the product licensed to BTG was approved for use in a clinical trial, which yielded interesting results. I also learned a lot from my exchanges with the industrial partners. Unfortunately, the project was not considered enough of a priority to be continued.
You recently published, in the Journal of Hepatology, a report on your experience with portal vein recanalisation? What do you think your results brought to the medical community?
This is actually the first large single-centre study of portal vein recanalisation in symptomatic chronic portal obstruction. This study reflects 15 years of practice in this rare and often misdiagnosed disease and demonstrates that this technique can be offered even after decades of portal obstruction. It leads to symptom and clinical improvement in 70% of cases and improves the nutritional status of patients. On the other side of the Atlantic, Riad Salem developed another treatment for the same disease. Time will tell whose is better.
During your professorship at CHUV Lausanne, what would you say the biggest shift in IR practice has been, both in your hospital and more widely? How has this impacted interventional radiologists’ approaches to cases and the consequent patient outcomes?
In 2018, we acquired an angiosuite combined with a computed tomography (CT) scanner in the same room. This kind of interventional suite has been used in Japan for years under the leadership of Professor Arai, but not much in Europe. This has been a game-changer in our practice for all procedures that require both angiography and percutaneous intervention. Of course, cone beam CT is also an option, but it has the disadvantage of being way more limited in term of imaging quality. We use our combined angiosuite and CT everyday and it has made us feel more secure and confident in our techniques, and probably also improved our clinical results.
Mentorship was the subject of this year’s Charles T. Dotter lecture at the Society of Interventional Radiology (SIR) Annual Meeting—why is this so important in IR and how can interventional radiologists seek to be better mentors?
Mentorship in every interventional or surgical activity is crucial; it is so important to be at young colleagues’ sides in the angiosuite. The transmission of all the tips and tricks of IR can only be done this way. The development of phantom and robotic IR will certainly change this approach in the near future, just like it did for laparoscopic surgery.
What are your hobbies and interests outside of medicine?
One of my main hobbies is biking, either in the Swiss mountains or in my beloved Normandy where we have a beach house. I also try to listen to live jazz music whenever I get the chance and I love reading books (particularly modern American authors like Jim Harrison). I am lucky enough to have been married for 30 years now, to a painter, and we enjoy visiting the museums and galleries in the places we visit on our travels, often with our children too.
Indrajeet Mandal, a second-year radiology registrar at Oxford University Hospitals NHS Foundation Trust (Oxford, UK), speaks to Interventional News about the interventional radiology (IR) awareness initiative that he co-founded in 2019—IR Juniors.
Mandal along with Niall Burke (NHS Lothian, Edinburgh, UK), Sachin Modi (Royal Free London NHS Foundation Trust, London, UK) and Navin Nagesh (Oxford University Hospitals NHS Foundation Trust) under the guidance of Gregory Makris (Guy’s and St Thomas’ NHS Foundation Trust, London, UK) and further support by Jim Zhong (Leeds Teaching Hospitals NHS Trust, Leeds, UK), launched the website to further awareness of the specialty. IR Juniors is now partnered with the British Society of Interventional Radiology (BSIR). The group aims to educate those at the start of their medical career about how they can pursue IR, become involved in the initiative’s affiliated research collaborative (UNITE) and embark on an elective in IR abroad—and much more besides.
Q: How did you end up as a radiology trainee with a passion for IR?
A: Just one day of a vascular surgery placement I did as a medical student was in IR, and that day changed my life. The consultants there probably do not know that they inspired me this much, but I am going to namedrop them anyway—Nick Woodward and Neil Davies at the Royal Free Hospital in London. I just had a fantastic experience—they let me scrub and explained exactly what IR was. Before, I had thought that it was just cardiologists who did stents, and this showed me a whole other world. Independently of that, I then did a placement in radiology towards the end of medical school and my supervisor happened to be an interventional radiologist. I really got inspired by the concept of ‘minimally invasive procedures under image guidance’—there is no other specialty like it.
Q: Why do you think that there tends not to be much awareness of IR among medical students? What specifically led you to set IR Juniors up?
A: In my opinion, the medical school curriculum is already very congested, and IR does not really fall among the priorities, which was fair enough a few decades ago. However, it has now become such a vital cog of healthcare. Even with some medical school teaching, it is hard to get a full grasp of what radiologists do, and this was partly the ‘why?’ for IR Juniors. It was also personal—before my IR elective I was searching for a basic website or book to help me prepare and I felt like there was a gap. We hope IR Juniors, as a solution to this, is accessible and not too advanced.
Q: UNITE—National IR Trainee REsearch Collaborative—is IR Juniors’ affiliated research group, which you also set up. Why was encouraging research involvement among students and trainees a priority?
A: Education is important, but research is too—IR has been one of the most innovative specialities. There are not that many avenues in the UK to explore IR research, and while not everyone is going to be an investigator or a researcher, it is still key to show that a career in research in IR is possible.
Q: You have carried out COVID-19-related projects through UNITE, among others—what has come from this research so far?
A: Our first project was on the impact COVID-19 had on IR training and services. As a trainee-led research collaborative, it was important to start with this. We found that, while a lot of surgical services had to stop because of the anaesthetic risk during the pandemic, a lot of IR services carried on, which highlights the importance of IR in the patient pathway. The next project was a multicentre study on the outcomes of cholecystostomy and over 30 centres collaborated—that work was presented at the BSIR meeting in 2021. It was great proof that we could mobilise trainees across the country, which had been done in other specialties, but never until then in IR. The papers from this study have now been accepted for publication.
Q: The Global IR section of IR Juniors shows your commitment to widening access to all that IR has to offer, for clinicians and patients alike—what does this look like in practice?
A: As a specialty, IR has always been collaborative—among different specialties but also countries—and we wanted to show that as an IR, you are part of a huge network around the world. There are two parts to the Global IR section, the first being highlighting opportunities for training in countries such as Canada and Australia. You can learn new techniques during these fellowships, while sharing how things are done in the UK too. Secondly, IRs can help set up training programmes and infrastructure in less developed countries. Road2IR is a great initiative as part of which trainees from the UK and USA go to Uganda to set up an IR training programme. This teaches participants that the specialty is not just about fancy, expensive equipment.
Vascular Therapies has announced that the first patient in the ACCESS 2 clinical trial was enrolled by Nikhil Kansal at Harbor-UCLA Medical Center in Torrance, USA.
The Phase 3 prospective randomised ACCESS 2 study will enrol 120 patients from centres in the USA and UK. The study is being conducted to validate an encouraging subgroup analysis from the first Phase 3 (ACCESS) study that showed that Sirogen use in end-stage renal disease (ESRD) patients 65 years and older resulted in clinically meaningful improvement in arteriovenous fistula (AVF) maturation and durability.
Kansal commented: “We are excited to participate in this randomised clinical trial that addresses an important unmet clinical need. The elderly population is the fastest growing segment of the haemodialysis population and these patients urgently need a solution to improve AV fistula maturation.”
Sriram Iyer, chief scientific officer of Vascular Therapies commented: “Initiating enrolment of the ACCESS 2 clinical study is an important milestone for Vascular Therapies. We would like to thank our investigators and their research teams for their interest in Sirogen and desire to evaluate a new potential therapy for haemodialysis patients.”
Vascular Therapies advises that the Sirogen drug development programme has received Fast Track status from the US Food and Drug Administration (FDA).
Reto Bale (Medizinische Universität Innsbruck, Innsbruck, Austria) gave a presentation titled ‘Stereotactic thermal ablation—can it break the current limits?’ at the 2022 European Conference of Interventional Oncology (ECIO; 24–27 April, Vienna, Austria). A key takeaway was that although the 3D planning and other elements of the stereotactic procedure may require more effort than conventional ultrasound (US)- and computed tomography (CT)-guided ablation approaches, the results that it yields are “excellent.“
His presentation covered an explanation of stereotactic thermal ablation, the logistical challenges of implementing it, and the outcomes it can achieve. Bale underlined to Interventional Newsthat “interventional oncology must become reliable and reproducible,” and that this is what underpins the stereotactic approach.
Bale’s stereotaxy workflow, he detailed, begins with “precise planning of multiple overlapping ablation zones”, to determine isotherms and to cover the whole tumour plus a safety margin. The next step, Bale relayed, is to place needles/probes in accordance with the plan, using respiratory triggering.
Planning CT showing colorectal liver metastases in segment VIII with 3cm diameter
Bale expanded on his previous explanation, conveying how a stereotactic approach is key when dealing with tumours greater than three centimetres, as, larger than this, and ablation from a single-probe position may not be possible, hence the need for multiple needles, and the careful 3D planning that precedes their use.
Since his very first stereotactic radiofrequency ablation (SRFA) in 2001, Bale has used the image fusion software of the stereotactic navigation system to superimpose the intraoperative contrast-enhanced control CT to the planning CT for verification of complete coverage of the tumour by the ablation zone. With regard to obtaining the results of the procedure, image fusion enables the interventional radiologist to see the results of stereotactic thermal ablation before the patient even wakes up. This intraoperative verification is an advantage that stereotaxy has over radiation therapy, which necessitates waiting until long-term follow-up imaging has been completed.
Planning of eight needle trajectories
Speaking to the outcomes of treating his patients with stereotactic thermal ablation, Bale stated that they very obviously demonstrate how “the additional efforts” necessary in order to conduct 3D planning, stereotactic needle placement and image fusion “lead to excellent results”. He expanded upon this assertion, explaining that his team treated more than 3,500 tumours in this way between 2001 and 2020, in more than 1,100 patients, and that even patients with multiple lesions and lesions greater than 10cm respond well. The complication rate after 2011, Bale underlines, was 0.5% mortality and 6% major complications. Of particular note is that more than half of these major complications “could be treated in the same session by the interventional radiologist.” The same is true when treating multiple lesions—they can often be treated simultaneously, in a single session.
Verification of precise coaxial needle placement by image fusion
Referencing histopathological evidence of the treatment’s success, Bale acknowledged the results of his study, which evaluated 188 hepatocellular carcinomas (HCCs) in 96 patients—the residual tumour rate was 2.7%. In lesions greater than three centimetres, the residual tumour rate is still as low as 3.8%, Bale added.
Consequently, Bale concluded, SRFA is now regarded the first-line treatment by the Innsbruck Tumour Board for most patients with primary and secondary liver tumours, encouraging clinicians first to ask themselves whether ablation could be an alternative to resection in HCC and colorectal liver metastasis patients. The advantages of the additional use of stereotaxy and image fusion are that it enables the interventional radiologist to treat more patients more consistently, with curative intent, minimally invasively, and while sparing tissue. Moreover “the beauty of the technique,” Bale emphasised, that “it is easy to teach” and that “training of three-dimensional needle trajectory planning can be done in your own lab on virtual patient datasets.”
Final contrast enhanced CT showing large ablation zone with sufficient margin as confirmed by image fusion
The logistical obstacles that stand in the way of more widespread current rollout of the treatment, Bale concedes, are the need for general anaesthesia, more than three hours per patient in the CT suite, the stereotactic neuronavigation system, and “there is still a problem, also, with reimbursement.”
Bale left the audience on the note that he hopes his excellent results will encourage those responsible for reimbursement guidelines to make changes to improve the accessibility of SRFA.
ŌNŌCOR has announced in a company press release that the ŌNŌ endovascular retrieval system was used to remove a large central-line-associated thrombus from the right atrium in a teenage patient.
The team at Children’s Hospital Los Angeles (CHLA; Los Angeles, USA) led by Darren Berman, Director of Congenital Interventional Catheterisation with CHLA’s Heart Institute, percutaneously removed a large fibrotic thrombus from a 14-year-old patient using a combination of ŌNŌ, endovascular snares, and electrocautery.
“This procedure was inspired by the Seattle procedure recently performed at the University of Washington, and represents the first time that a large haemodynamically problematic thrombus was captured and removed non-surgically, and without fragmentation or distal embolization of particulate matter,” said Berman. “The ŌNŌ was key to securing the mobile mass and subsequently removing it from the vasculature atraumatically.”
Berman continued, “Intra-atrial thrombus formation associated with indwelling central lines is a common problem. Typically, the approach is to treat with anticoagulants in the hopes that the clot reabsorbs. When this doesn’t work, and the thrombus burden remains substantial, it represents an ongoing risk for pulmonary and systemic emboli.
“Our patient today is representative of a clinical dilemma that we often face. Up until this point, the only options that we had were ‘watchful waiting’ or open-heart surgery,” said Berman.
The ŌNŌ designed to receive, align, compress, and remove material (non-biologic and biologic) from the vascular system. ŌNŌ is intuitive to use and is compatible with commercially available vascular sheaths, endovascular snares and other graspers.
“We are delighted that ŌNŌ was able to help the team at Children’s Hospital Los Angeles,” said Mark Piper, CEO of ŌNŌCOR. “ŌNŌ was designed to help safely remove material from the vascular system, so it’s rewarding to hear that the patient in Los Angeles has done well and recovered nicely from this procedure.”
Teleflex has announced a new agreement with FundamentalVR, a company providing virtual reality (VR) integration for medical simulation. The agreement will provide Teleflex with a VR training platform to accelerate the effective use of the company’s UroLift 2 system, a technology for treatment of benign prostatic hyperplasia (BPH), commonly known as enlarged prostate. The VR training platform integrates tactile feedback and a digital representation of the UroLift 2 system to provide urologists with a ‘hands-on’ VR experience that can accelerate their learning.
By leveraging the capabilities of FundamentalVR’s Fundamental Surgery platform, Teleflex aims to increase access and standardisation of clinical training of the UroLift 2 system in the USA and around the world, including Japan, where the UroLift 2 system was recently approved for use. The customised solution from FundamentalVR will enable urologists globally to practice the procedure remotely in a virtual environment.
Teleflex showcased the Fundamental Surgery platform at the company’s UroLift system booth at the 2022 American Urological Association (AUA) meeting in New Orleans.
“We are delighted to offer our customers this leading VR platform for surgical and procedural education which offers advanced, realistic graphics to help demonstrate the ease of use of the UroLift 2 system in a variety of prostate anatomies,” said Kevin Hardage, president and general manager of Teleflex Interventional Urology. “FundamentalVR’s Fundamental Surgery platform is versatile and scalable, making them an ideal supplier to meet our customers’ needs for training for the UroLift 2 system around the world.”
Chris Scattergood, co-founder at FundamentalVR said, “We are delighted that Teleflex, a market leader in urology, has chosen FundamentalVR as their partner for their future vision. Integrating extended reality education solutions can have a positive impact on surgeons and patients.”
A study recently published in the World Journal of Surgery claims to be the first to provide comprehensive population-level data on the epidemiology of lower extremity amputation (LEA) in a Latin American low- and middle-income country (LMIC). The investigators write that their data, which focus on the Brazilian state of Sao Paulo, are “crucial to plan strategies to reduce the burden of LEA”.
“Lower limb amputations represent a high social, economic and health burden,” Rodrigo Bruno Biagioni (Hospital do Servidro Público Estadual de São Paulo, São Paulo, Brazil) et al write. According to the authors, most lower limb amputations are preventable, and reflect areas for improvement in healthcare. For these reasons, they stress that it is “essential” to know the epidemiology of these amputations, underscoring the rationale behind their study.
The investigators detail that LEA rates are “highly variable” across the world and that LEA trends are “conflicting”. These factors, they say, necessitate population-based studies in particular, “not only to truly know the local epidemiology of LEA, which reflects the quality of the health system, but also to build a global panorama in order to establish standards and goals.”
According to the authors, several countries in Europe, North America and Australasia have reported their amputation epidemiology, with most data coming from high-income countries (HICs). “Data from [LMICs] are scarce,” they write, noting that in Latin America no such study existed before the present analysis, to the best of their knowledge. “The paucity of data on LEA in LMICs is of particular concern,” the researchers note, “as the burden of PAD and [diabetes mellitus] is increasing in rates higher in LMICs than those observed in HICs.”
Biagioni et al’s study was a retrospective, population-based, cross-sectional analysis on all lower limb amputations performed in public hospitals in Sao Paolo—the most populous Brazilian state—between 2009 and 2020. The authors relay that they used a public database to evaluate types, rates and trends of the amputations performed, main aetiologies leading to the indication for amputation, hospital length of stay and in-hospital mortality rates, demographics of the amputees and procedure costs.
The study included data on 180,595 lower limb amputations and surgical revisions of amputations, with toe amputations (45%) and major amputations (33%) being the most frequent types of surgeries. Biagioni and colleagues report a significant increase in the rates of both of these procedures. They add that peripheral arterial disease (PAD) was found to be the most frequent underlying diagnosis for LEA, followed by diabetes mellitus, with an increasing trend for both over the last 12 years. Furthermore, they also observed seasonality in procedure rates, with peaks in August in all years.
The authors also reveal that most patients were male (69.3%), Caucasians (55.6%) and elderly. Other findings included a 6.6% rate of in-hospital mortality and lower limb amputations and total of US$67,675,875.55 reimbursed by the government.
Based on these findings, the authors propose some preventive strategies—namely foot ulcer screening, multidisciplinary diabetic foot care, and encouraging revascularisation procedures, which, they claim, have not significantly increased in the city of São Paulo, the capital of the state of Sao Paulo, since 2008.
In the discussion of their results, the research team considers some possible explanations for PAD being the main underlying diagnosis for all LEA in Sao Paulo, one of which is that Brazil is “late in the epidemiological transition concerning LEA”. They predict that it is likely Brazil will reach similar statistics to those found in most recent nationwide studies—which point to diabetes mellitus as the most common underlying cause of LEA—in the coming years, as the prevalence of smoking is reducing and that of diabetes mellitus is rising.
Furthermore, Biagioni et al address the finding that August showed the highest number of amputations in all years of their study. They write that, although this contrasts a previously reported finding from Hong King of higher LEA frequency due to diabetes mellitus during the summer, in this study the main underlying diagnosis was PAD, and it is possible there may be a worsening in PAD during winter. They elaborate: “Even though impaired circulation of lower limbs is documented for venous insufficiency, it is reasonable to think it may also play a role in arterial insufficiency.”
The authors recognise there are some limiting factors to their study, including the accuracy of their findings being “susceptible to inherent miscoding or data entry errors,” as with any database-driven study. In addition, they acknowledge that their data represent only the state of Sao Paulo, which depends solely on the public health system. “An integrated database covering data from public and private health systems would be more comprehensive,” they note.
Speaking to Vascular News, corresponding authors Louzada and Nelson Wolosker (Hospital Israelita Albert Einstein, São Paulo, Brazil) comment on the study findings: “Knowledge of the data is essential for decision-making by public policy managers. Knowing the real amputation rates, increased investment in risk factor controls, and increased access to revascularisation become the most obvious attitudes. Soon, adopting such attitudes, amputation rates will probably decrease. This way, Brazilian society can evolve, an example for other countries.”
The first US patient has been enrolled in the US Food and Drug Administration (FDA) SELUTION4BTK (below-the-knee) clinical trial evaluating Selution SLR, MedAlliance’s novel sirolimus-eluting balloon. This follows investigational device exemption (IDE) approval in the USA in May 2022, with enrolment of the first patient occurring in Germany one week after approval.
“We are very excited to finally have drug-eluting technology in the USA to treat this difficult patient population,” commented the trial’s principal investigator (PI) Ehrin Armstrong (University of Colorado, Denver, USA). “We are encouraged by the positive early outcomes with this novel Selution SLR sirolimus drug-eluting balloon (DEB) in Europe and Asia. We hope this FDA IDE trial will demonstrate significant benefit for patients who currently have limited treatment options.”
The aim of the SELUTION4BTK clinical trial is to demonstrate the superior efficacy and equivalent safety of Selution SLR compared to plain (uncoated) balloon angioplasty in the treatment of BTK arteries in chronic limb-threatening ischaemia (CLTI) patients. The trial is a prospective, multicentre, single blinded, randomised study.
377 subjects are being randomised 1:1 to either Selution SLR or control treatment. This is the first study of its kind where ‘real-world’ patients with CLTI can be included. Patients are being enrolled at approximately 40 sites across the USA, Europe and Asia. This first US patient was enrolled at Vascular Solutions in Cary, USA, by Siddhartha Rao.
“We are very pleased to be participating in this ground-breaking study,” said Rao. “We hope that this promising technology will fulfil a huge need for our patients with CLTI, saving life and limb. We look forward to the rapid enrolment of this trial.”
“We were the first company to be granted Breakthrough Device designation for a DEB by the FDA and are proud to enrol the very first US patient in a sirolimus DEB study,” added Jeffrey B Jump, MedAlliance chairman and CEO. “Many companies have been trying for years to bring sirolimus to the USA and we are very pleased with our team for achieving this significant milestone. US patients will now have an alternative to paclitaxel DEB, addressing the concerns expressed by the FDA.”
MedAlliance advises that Selution SLR is available in Europe and all other countries where the CE mark is recognised.
BD has announced the start of enrolment in a first-in-human trial of a peripheral sirolimus drug-coated balloon (DCB).
The PREVISION trial is a prospective, multicentre, single arm, non-randomised study designed to evaluate the safety of the BD sirolimus DCB in the treatment of peripheral arterial disease (PAD) in the femoropopliteal arteries.
A company press release notes that BD initiated this trial to determine the viability of sirolimus as a future treatment option for patients with PAD. The first patient was successfully treated by principal investigator Andrew Holden at Auckland City Hospital (Auckland, New Zealand).
“It is an honour to enrol the first patient in the PREVISION study,” said Holden. “The burden of PAD continues to impact patients and challenge physicians around the globe. A continued focus on developing next-generation technology is important for the patients suffering from PAD.”
PREVISION is being conducted across multiple sites in Australia, New Zealand, and Singapore. The trial will enrol and follow-up on approximately 50 patients over the coming months.
Building upon “pioneering work” at University of Texas Southwestern (UTSW) Medical Center (Dallas, USA), investigators recently reported the results of a clinical trial exploring the role of stereotactic ablative radiation therapy (SAbR) for patients with a handful of metastases, or so-called oligometastatic disease.
As per a UTSW press release, the study represents the first clinical trial for patients with untreated oligometastatic kidney cancer.
“There has never been a clinical trial for these patients. It is unclear whether these patients should be treated with medication, surgery, or another approach. This represents an unmet medical need,” said Raquibul Hannan (UTSW, Dallas, USA), lead author of the study along with Robert Timmerman and James Brugarolas (both UTSW).
As per the release, kidney cancer encompasses a wide spectrum and can present with extensive metastases, or just a handful. However, today, all patients are treated the same way—with medication. Metastatic kidney cancer is typically treated with immunotherapy agents or targeted drugs, which are toxic and diminish quality of life. For most patients, the disease ultimately progresses, necessitating a change in treatment, until patients exhaust their options. When metastatic, most patients eventually succumb to the disease, and the quality of their remaining lifespan is negatively impacted by the cancer drugs.
The phase 2 clinical trial tested SAbR, a treatment that delivers potent, narrow beams of radiation to tumours, in 23 kidney cancer patients with oligometastases (up to five metastases) at UTSW and the affiliated county hospital, Parkland Health. Patients received SAbR to metastatic tumours at the outset and while the disease remained oligometastatic. Overall, 57 metastases were treated.
The primary goal was to control the metastatic cancer in at least 60% of patients at one year. The study was successful, with more than 90% of patients demonstrating disease control at one year without systemic therapy.
“It appears that most patients will be free of systemic therapy for at least two years,” said Hannan.
None of the patients experienced serious side-effects either, the release notes, and periodic questionnaires showed no negative impact on quality of life. A large, phase 3 randomised clinical trial evaluating SAbR for oligometastatic kidney cancer has now been approved by the National Cancer Institute and will also be led by Hannan.
“If successful, this phase 3 trial will establish, for the first time, a standard of care for patients with oligometastatic kidney cancer,” added Brugarolas. “The hope is that the treatment will help patients by delaying progression while preserving their quality of life.”
A new imaging device at University of Texas (UT) Southwestern (Dallas, USA) is making complex aortic repairs safer for patients and operating room staff by dramatically reducing their exposure to radiation. The device, known as Fiber Optic RealShape (FORS; Philips), uses light to visualise blood vessels, nearly eliminating the need for X-rays typically used during minimally invasive vascular procedures.
“Complex aortic repairs tend to be long operations that require frequent in-procedure imaging. Every time a surgeon presses on the X-ray pedal, the patient and staff including assistants, nurses, scrub techs, anaesthetists, and X-ray techs gets a dose of radiation,” said Carlos Timaran, professor of surgery at UT Southwestern. “The safety of each of these individuals is paramount, so reducing radiation exposure during these procedures is an important goal.”
UT Southwestern was one of about a dozen medical centres in the USA and Europe chosen to participate in the early implementation of FORS. Timaran has completed more than 300 fenestrated endovascular aortic repairs as part of his physician-sponsored investigational device exemption study, in which a patient-specific graft is used to support the aorta and its main branches.
As an alternative to conventional imaging, the FORS device uses light travelling through hair-thin optical fibres built in specially designed catheters and wires to display its position and shape inside the body. Once this device is placed within a blood vessel, the strain on the optical fibres changes the light’s pathway. By analysing how light reflects back along the fibres, a computer algorithm reconstructs and visualises the full shape of the device. The result is a real-time, three-dimensional view of the blood vessel that surgeons can overlay on computed tomography images taken before the procedure, providing a roadmap that surgeons can view in any angle to guide the surgery. Timaran said that far fewer X-rays are necessary when using FORS, significantly reducing patients’ and staff’s exposure.
He expects FORS use to expand to other vascular procedures over time. “This technology could potentially be used for any cardiovascular procedure,” he said. “This will eventually be the goal.”
Iodinated contrast media agents, namely Omnipaque (iohexol) and Visipaque (iodixanol), are frequently used in imaging studies for both diagnosis and treatment. GE Healthcare, the manufacturer, had to shut its plant in Shanghai, China, due to local COVID-19 policies, which created a domino effect in the supply chain, as seen in recent months. In May and June of 2022, clinicians were offered guidance on alternative imaging methods for interventional radiology procedures
Speaking to Interventional News about hers and colleagues’ article, which was published in the Journal of Vascular and Interventional Radiology (JVIR), lead author Nikki A Keefe (Department of Radiology, University of North Carolina at Chapel Hill, Chapel Hill, USA) outlines the current iodinated contrast media supply situation, and what the response to her recommendations has been among radiologists.
Taking the American College of Radiology (ACR) Committee on Drugs and Contrast Policy’s guidelines statement as a starting point, Keefe and her co-authors recommended using a priority matrix to help manage radiology services in the face of the contrast media shortages. The matrix should encompass the following types of procedures: those requiring iodinated contrast media versus procedures that can be deferred; those that can be performed with alternative imaging modalities such as intravascular ultrasound; and those that can be performed with an alternative contrast media.
Keefe first underscores to Interventional News the impact of the shortage on radiology services: there were many cancellations and delays for non-emergent procedures, and alternative agents used. “Many procedures were transitioned,” she expands, citing how the traditional gastrostomy tube placement replaced the balloon-assisted gastrostomy tube placement, non-contrasted computed tomography (CT) replaced sinogram, and ultrasound-guided saline injections replaced fluoroscopy-guided contrast injections for tube placements.
The article’s lead author also relays how she, personally, “received many questions about using gadolinium, gastrografin and carbon dioxide in unique methods such as within angioplasty balloons.”
From a patient point of view, Keefe details how they were often “not familiar with the cases performed in the usual manner”, so remained largely unaware of procedural changes caused by the shortage, such as the employment of different imaging modality. Many, however, were acutely aware of the delays in imaging and their procedures.
“It would be interesting to see how radiation doses changed during this period, as perhaps patient doses decreased due to increased utilisation of ultrasound,” Keefe muses, while also contemplating how doses may actually have increased “if interventionalists were less familiar with alternative contrast agents and therefore the procedure was made more challenging and lengthier”
Regarding the current state of contrast media availability, Keefe asserts that it seems to be at “pre-shortage levels”, owing to Bracco’s increased production and importation to the US market and GE Healthcare’s production having returned “to normal”.
However, “it may be prudent to continue to utilise some of the mitigation strategies full-time,” Keefe advises, citing that nephrology colleagues of hers are in support of such an approach. “Use of air, carbon dioxide, and intravascular ultrasound where applicable can decrease both patient and provider radiation dose during the procedure,” the lead author suggests. Keefe goes on to say that “this may not increase procedural time but perhaps [even] decrease it, while providing [higher-quality] diagnostic imaging in certain situations.”
In a study recently published in Circulation, researchers found that Black adults underwent significantly more endovascular peripheral vascular interventions (PVI), were treated for more advanced disease and were also more likely to experience adverse outcomes following PVI procedures, including amputation and death. Interventional News spoke to two of the authors—Eric A Secemsky and Anna K Krawisz (Smith Center for Outcomes Research in Cardiology, Beth Israel Deaconess Medical Center, Boston, USA)—about their motivations for carrying out the study, the results it yielded, and where this research might lead.
Asked what led them to study race-related disparities in PVI treatment and outcomes, Secemsky and Krawisz explain that the Vascular Research section at the Smith Center is “deeply invested in improving care for patients with peripheral artery disease (PAD).” This, they assert, means “confronting the healthcare disparities that are prevalent in the vascular field.” PVI is now a common means of revascularisation and, therefore, the authors state their desire to “to understand whether racial disparities exist in different aspects of PVI”, knowing, as they do from their study, that “Black adults have a higher prevalence of PAD than white adults and they are more likely to have adverse outcomes such as amputation.” Moreover, the authors sought to identify what underpins the differences in outcomes for Black versus white patients.
Eric A Secemsky
Secemsky and Krawisz relay their findings as follows— Black race was associated with worse one-year outcomes following PVI, with adjustment for age and sex, owing, in large part, to the “disproportionate burden of advanced comorbidities among Black adults.” A further finding, the authors communicate, was that Black adults have more advanced PAD than white adults when they are referred for PVI.
“These results were not necessarily surprising,” they admit, but it is nonetheless, “critically important” that the vascular community be aware of them, given how much PVI is used to manage symptomatic PAD. However, what did surprise them was how few patients, regardless of race, received guideline-directed medical therapies following PVI—”we would have expected that medical therapy would be optimised prior to moving towards revascularisation,” they state.
The authors’ hope for their findings is that the vascular community better understands how “critically important” it is to detect, and effectively treat, comorbidities early. This is particularly crucial in Black adults, they affirm, so as “to reduce health disparities and improve limb outcomes.”
Regarding where this research will lead, Secemsky and Krawisz convey that they “continue to untangle the interplay between many types of disparities that impact care and outcomes in PAD, including poverty, gender, regional wealth, and geographic location.” Krawisz will give special focus to better understanding why women, like Black patients, tend to present for treatment with more advanced PAD, and why, when they require amputation, it is, generally, “more proximal”. Her research programme, she explains, will centre around PAD management for female patients. She reports that clinical trials in PAD “tend to underrepresent female patients”.
CX Aortic Vienna returns in October for its third edition (24–26 October, Digital), bringing together world-leading specialists from the cardiac and vascular fields to discuss all facets of aortic care from selection to investigation, diagnosis, techniques and technologies. The meeting will showcase the latest approaches—open and endovascular—for the treatment of complex aortic problems spanning the aortic valve to the iliac arteries.
Having attracted a global, online audience during its first two editions, CX Aortic Vienna will continue to reach out to the worldwide aortic surgery community. The 2022 edition features three days of high-quality digital programming, to be broadcast live from 24–26 October for the wider global audience, delivering a total of 15 hours of aortic education, which will also be available on-demand to registered attendees after the event.
The format for the digital edition will follow the CX style of short talks, debates, and audience interaction, presented live via broadcast. The programme includes open and endovascular aortic techniques and technologies, including edited aortic cases.
For the first time, the meeting will also offer an in-person component from its home city, Vienna, Austria, where CX Aortic Vienna has been invited to provide two 90-minute primetime cutting-edge English-language sessions for attendees of the Dreiländertagung—the joint meeting of the Austrian Society of Vascular Surgery (ÖGG), the Swiss Society for Vascular Surgery (SGG) and the German Society of Vascular Surgery (DGG)—on Thursday, 20 October.
World-leading faculty
The full programme has been curated by a Vascular, Endovascular and Cardiothoracic Executive board comprised of leaders in the field of aortic care including CX Aortic Vienna founding chair Roger Greenhalgh (London, UK), alongside Tilo Kölbel (Hamburg, Germany) who will moderate the in-person session at Dreiländertagung, Afshin Assadian (Vienna, Austria), Roberto Chiesa (Milan, Italy), Martin Grabenwöger (Vienna, Austria), Stéphan Haulon (Paris, France), Gustavo Oderich (Houston, USA), Markus Steinbauer (Regensburg, Germany) and Alexander Zimmermann (Zürich, Switzerland).
“This is, as always, a focus upon the aorta as managed by cardiac aortic surgeons, open vascular surgeons and endovascular surgeons; from the aortic valve at one end, to the iliacs at the other end,” says Greenhalgh of the event’s 2022 edition. “CX Aortic Vienna, for those of you who have been to it before, is for all of those who manage the aorta,” he adds. “This is not just the surgeons, but the physicians—we have radiologists, imaging experts, vascular scientists and vascular nurses. All who manage aortic patients are welcome to come and join us for the digital edition on 24, 25 and 26 October this year.”
“October is the time for aortic disease and to discuss newest trends, technologies and features in aortic therapy,” comments Kölbel. “We are focusing on both open and endovascular techniques and we are inviting the cardiovascular and vascular communities to come to CX Aortic Vienna, with a presence during the Dreiländertagung, and very much to the virtual event that happens a few days later.”
Multidisciplinary approach
The importance of multidisciplinary aortic approaches will be a key strand running through CX Aortic Vienna’s content and discussion, and the 2022 event will continue its mission to bring together specialists of all skills—be they cardiac, vascular or endovascular—to provide a comprehensive overview of cutting-edge aortic treatment.
“CX Aortic Vienna is the unique chance to get together with cardiac surgeons and all kinds of vascular specialists that are treating the aorta,” says Zimmermann, discussing the importance of the multidisciplinary focus at the heart of CX Aortic Vienna. “The problem is that we have a transition zone in the arch and we—as vascular surgeons—move further and further into the ascending aorta with our endovascular techniques. This can only be done with the support of the cardiac surgeons, and this is the reason why we really look forward to CX Aortic Vienna because everyone comes together addressing this complex field.“
Talking points
The programme encompasses discussion and debate spanning key talking points in the aortic space including aortic arch interventions, thoracic dissection, thoracic imaging, thoracoabdominal techniques, juxtarenal, abdominal aortic and iliac artery therapies.
“I have had the honour and the privilege during my career to treat the aorta from the aortic valve all the way to the femoral arteries,” notes Joseph Coselli (Houston, USA), who has been among the expert speakers to have participated in previous editions of CX Aortic Vienna and is returning in 2022. “The entire history of aortic surgery, and vascular surgery to the same extent, has been one of technical and clinical evolution.”
Coselli adds: “The Charing Cross meetings are among the best with regard to the broad spectrum of technology and clinical information and sharing among experts. I would invite everyone to take the opportunity to learn a lot about vascular and aortic surgery at CX Aortic Vienna.”
From 2023 onwards, CX Aortic Vienna will be held annually in October as a hybrid meeting in-person in Vienna whilst simultaneously livestreaming globally.
Boston Scientific has announced the acquisition of Obsidio, a privately held company that has developed the Gel Embolic Material (GEM) technology used for embolization of blood vessels in the peripheral vasculature.
Recently cleared by the US Food and Drug Administration (FDA), the GEM technology is a semi-solid, proprietary material packaged in a ready-to-use form, thus reducing the preparation time required for many embolization procedures. Physicians deliver the GEM agent through a catheter, and its gel-like composition enables controlled placement within patient anatomy. Unlike solid and liquid embolics that can take time to form an obstruction to blood flow, once placed, the GEM technology conforms to the targeted vasculature, immediately creating a barrier.
“The GEM technology combines benefits of currently available embolics, such as precise control of a solid and malleability of a liquid, to create a unique technology that offers procedural efficiency and a more personalised therapy for patients,” said Peter Pattison, president, interventional oncology and embolization, Peripheral Interventions, Boston Scientific. “This acquisition strengthens our interventional oncology and embolization portfolio with a differentiated solution for physicians and their patients suffering from haemorrhages, cancer and other debilitating conditions.”
Ramona Gupta (Northwestern University, Chicago, USA) addresses the issue of recurrent varicose veins, highlighting in particular the “multiple tools” now at physicians’ disposal to treat the problem.
Superficial venous insufficiency and varicose veins affect approximately 23% of adults worldwide. Treatments have significantly evolved from surgical ligation and stripping to less invasive endovascular ablative procedures. However, recurrent varicose veins are common with both surgical and endovascular techniques. Durability is an important long-term outcome measure. Recent studies have examined recurrences following endovenous procedures and delineated the rates of recurrence, the patterns of recurrence, and factors associated with recurrence.
Recurrence rates following endovenous ablation procedures has consistently proven lower in long-term studies when compared to ligation and stripping. Multiple studies have confirmed durable closure rates approaching 95% after five years with the thermal and non-thermal ablative technologies. Recurrent rates after ligation and stripping have been described ranging from 20–80% with incidence increasing over time.
Importantly, the recurrence patterns following endovenous ablation are significantly different from those following ligation and stripping. The REVAS (Recurrent varices after surgery) study evaluated a large cohort of patients and found that 20% of recurrences were due to saphenofemoral neovascularisation, 19% of recurrences were secondary to incorrect junctional ligation and 55% of recurrences originated from perforator reflux. Neovascularisation after endovenous ablation is rarely seen. Instead, the majority of recurrences are due to recanalisation of a segment of previously treated vein or new reflux in an accessory saphenous vein or alternate truncal pathway. Specifically, recanalisation of a previously treated great saphenous vein (GSV) or reflux in the anterior accessory great saphenous vein (AAGSV) are common causes of recurrent disease in patients.
Treating these patterns of recurrence often involves employing non-thermal techniques. Recanalised short segment GSV can be effectively treated with ultrasound-guided foam sclerotherapy (USGFS) with special attention to newly refluxing perforator veins frequently noted in the thigh. Recurrent disease with new reflux in the GSV below the knee can be treated with cyanoacrylate adhesive closure or USGFS to avoid nerve injury. The AAGSV frequently becomes superficial, tortuous and outside the sheath after only a few centimetres. Endovenous laser ablation is successful in treating to the saphenofemoral junction although tumescing outside the sheath and achieving adequate depth to prevent a skin burn can be difficult. Cyanoacrylate adhesive closure requires 10cm of straight segment to treat. USGFS is an option but has routinely demonstrated lower closure rates. The short saphenous vein is also a common culprit for disease recurrence and can be successfully treated with most of the newer technologies, thermal or non-thermal.
Factors related to varicose vein recurrence after endovenous ablation include: 1) obesity with increased abdominal pressure increasing the likelihood of venous reflux, 2) increase in the diameter of the vein to be treated and 3) treated refluxing venous segment below the knee.
While awareness of these factors is important, they rarely cause me to alter my treatment or post-treatment plan. However, I do council patients that recurrence may be more likely in these situations and I encourage vigilant use of compression in the immediate- and long-term post-treatment period.
In my practice, recognising and treating recurrent disease is an important factor in overall long-term leg health and patient satisfaction. Our practice does not routinely bring patients back at one year for follow-up ultrasound so most recurrences are noted solely due to return of symptoms or new visible varicosities. In addition, recurrences can be a significant cause of morbidity as seen in the case below.
Figure 1. Map of a patient treated with endovenous radiofrequency ablation of the GSV at an outside clinic five years prior to her presentation in Gupta’s clinic.
Figure 1 is the map of a patient who was treated with endovenous radiofrequency ablation of the GSV at an outside clinic five years prior to her presentation in my clinic. Her standing duplex ultrasound examination demonstrates several important patterns of recurrence: perforator reflux and new small saphenous vein (SSV) reflux. Moreover, she had a large non-healing wound at the medial malleolus, which had been present for six months (Figure 2).
Figure 2: Ulcer at left medial malleolus at presentation.
I treated her in a single session with endovenous laser ablation of the SSV and USGFS of the refluxing varicosities in the thigh and calf. She followed a strict regimen of compression and wound care following the procedure. At six months, the wound showed significant healing and the patient reported meaningful improvement in her swelling and heaviness (Figure 3).
Figure 3: Ulcer six months post treatment.
While recurrent varicose veins can be frustrating for the patient and the physician, rates of recurrence are low with newer techniques and patterns of recurrence are easily recognisable. Physicians have multiple tools available to treat these new refluxing veins and are able to achieve excellent clinical outcomes.
Ramona Gupta is associate professor of radiology at Northwestern University in Chicago, USA.
Gore has announced the acquisition of InnAVasc Medical, a privately held medical technology company focused on advancing care for patients with end-stage renal disease who utilise graft circuits for dialysis treatment.
Jeffrey Lawson and Shawn Gage from Duke University School of Medicine’s Department of Surgery (Durham, USA) have developed the InnAVasc device, which is specifically designed to allow for safe, easy, reproduceable and durable access for dialysis treatment of patients with graft circuits.
The investigational InnAVasc device is designed to protect the graft from backwall punctures and reduce the damage associated with frequent needle sticks which occur over the lifespan of a dialysis graft. This can lead to circuit failure and shortened circuit life. “To be stuck with two needles three times a week for haemodialysis for 52 weeks, that’s 312 times a needle goes into a patient’s graft each year,” said Stephen Hohmann, vascular surgeon at Texas Vascular Associates (Dallas, USA). “So having a graft that has the ability to decrease risk potential and long-term injury is definitely something that would be a game-changer.”
“Backwall punctures and damage due to excessive needling are painful and can cause unwanted bleeding, delay or stoppage of treatment, and reduced graft durability,” said Prabir Roy-Chaudhury, professor of medicine at the Division of Nephrology and Hypertension at the University of North Carolina (Chapel Hill, USA). “I greatly appreciate how this technology is intended to be so patient-centric, addressing this important interface need, for both clinicians and home caregivers.”
“We see an array of synergies working with Gore. The company is well recognised for its advanced material capabilities. [It has a] long history of designing graft solutions […] used in dialysis access procedures today, and we are excited to collaborate on future innovations,” said InnAVasc CEO Joseph Knight.
Royal Philips today announced an important milestone in the evolving standard of care for treating patients with peripheral vascular disease: the establishment of the first-ever global consensus for the appropriate use of intravascular ultrasound (IVUS) in lower extremity arterial and venous interventions.
Published in the August 2022 issue of the Journal of the American College of Cardiology: Cardiovascular Interventions, the new consensus document from 30 global vascular experts recommends routine use of IVUS as a preferred imaging modality in all phases in many peripheral vascular disease procedures.
“The voting panellists considered a variety of clinical scenarios and based on their extensive experience, arrived at a strong consensus,” said lead author Eric A Secemsky (Beth Israel Deaconess Medical Center, Boston USA). “They recommend routine use of IVUS as a preferred imaging modality in all phases for many peripheral interventions, both diagnostic and therapeutic, as it enables such exquisite visualisation of the target vessel and lesion. Their recommendations, which withstood the rigour of peer review, can now be considered in the formulation of clinical guidelines for the diagnosis and treatment of peripheral vascular disease.”
Peripheral vascular disease affects an estimated 200 million people worldwide, including approximately 40 to 45 million Americans, according to the American Heart Association. The authors noted that minimally invasive approaches for peripheral vascular disease interventions are increasingly common, but traditional imaging techniques like angiography have limitations, including two-dimensional projections of three-dimensional vasculature, which can complicate diagnosis and intraprocedural optimisation.
“As the global leader in providing vascular solutions to physicians and the patients they serve, we especially value the rigour and independence of this cross-specialty expert consensus,” said Heather Hudnut Page, general manager and business leader for peripheral vascular image guided therapy devices at Philips. “It is exciting to know that this initiative has the potential to standardise the use of IVUS in peripheral interventions and guide clinical decisions to further improve the quality of care procedures for patients.”
Supported in part by research grants from Philips and Boston Scientific, the study was conducted and analysed independently by Smith Center for Outcomes Research, gathering a wide spectrum of vascular expert opinion to ascertain the role of intravascular imaging in contemporary clinical practice.
Delcath Systems has announced the publication of a retrospective analysis of patients who underwent a percutaneous hepatic perfusion procedure (PHP) with Chemosat at three European centres, one in the Netherlands and two in Germany, between February 2014 and December 2019. The study, published in CardioVascular Interventional Radiology (CVIR) involved 101 patients who completed a minimum of one PHP procedure for the treatment of unresectable uveal melanoma (UM) liver metastases.
The study by T. M. L. Tong, et al, included a total of 212 PHP procedures for the 101 patients included in the study. Of the 101 patients, 66 received PHP as first-line treatment and 33 had received prior therapy (status of two patients was unknown). Approximately 50% of patients had greater than nine metastases. Seventy-seven patients underwent at least two procedures and 25 patients received more than two PHP procedures. After a median follow-up time of 15 months, a complete response (CR) was reported in five (5.0%) patients; partial response (PR) in 55 (54.5%), and stable disease (SD) in 30 (29.7%), resulting in an objective response rate (ORR) of 59.4% and a disease control rate (DCR) of 89.1%.
The median progression-free survival (PFS), liver progression-free survival (LPFS), and overall survival (OS) were 9.0 months (95% CI 7.7–10.3); 11.0 months (95% CI 9.0– 13.0); and 20.0 months (95% CI 13.7–26.3), respectively. Twelve patients who were lost to follow-up were censored in the survival analyses. The study also found statistically significant differences in median PFS, median LPFS, and OS between patients who had CR, PR, or SD; and patients with progressive disease (PD). For example, for patients with CR or PR the median OS was 27 months (95% CI 17.5–36.5); for patients with SD the median OS was 21 months (95% CI 11.2–30.8); and 8 months (95% CI 5.7–10.3) for patients with PD.
Although the study did not find a statistically significant difference in either median PFS and LPFS for patients treated with two or more PHP procedures compared to patients treated with one PHP procedures, the study did find a statistically significant difference in OS (20 months vs. 8 months) for patients who had two or more PHP procedures compared to patients who were treated with one PHP procedure.
The safety analysis was conducted on the first treatment cycle (183 PHP procedures). The most common adverse events were haematological toxicities which were grade 1/2 and self-limiting in the majority of patients and consistent with previous reports on PHP. Other adverse events were thromboembolic in nature. The mortality rate was 1.1% within 30 days after PHP.
AngioDynamics recently announced that it has received US Food and Drug Administration (FDA) 510(k) clearance of an expanded indication for the Auryon atherectomy system to include arterial thrombectomy.
The FDA recently cleared the expanded indication for the Auryon system’s 2mm and 2.35mm catheters to include adjacent thrombus aspiration when treating stenoses in native and stented infrainguinal arteries. Both catheters have aspiration capabilities as atherectomy devices, including in-stent restenosis (ISR).
“AngioDynamics is pleased to have received these expanded indications for the Auryon atherectomy system,” said Scott Centea, senior vice president and general manager, Global Endovascular Therapies. “Since launching commercially in September 2020, the Auryon atherectomy system has become an essential tool for providers across the USA in the treatment of peripheral arterial disease (PAD) and related conditions. These expanded indications further validate the extensive capability and effectiveness of the Auryon technology offering our providers an advanced and efficient treatment option for PAD.”
The Auryon laser can be used to treat all infrainguinal lesion types, including above-the-knee (ATK), below-the-knee (BTK), and ISR, and to date, has been used to treat more than 21,000 patients in the USA, a company press release reports.
“Combining the 2mm and 2.35mm Auryon laser atherectomy with the aspiration capability has changed our practice. We now treat acute limb ischaemia in a single session where we remove the acute component as well as treat the underlying lesion. Patients are now discharged in less than 24 hours without the need for an ICU bed or overnight lysis,” said Carlos J Guevara (Washington University School of Medicine, St Louis, USA).
Fluidx Medical disclosed study results examining extent of vessel filling using the GPX embolic device compared to microspheres, a common treatment for many types of tumours.
“GPX is demonstrating deep distal vessel penetration,” said Ryan O’Hara, interventional oncologist at the University of Utah (Salt Lake City, USA). “The ability to fill the smallest tumour-feeding vessels and reach distal vessel beds is very important in effective treatment of hypervascular tumours and in other therapeutic embolic procedures.”
Embolizing blood supply to tumours is a high-growth procedure to block blood supply to certain tumours. Transarterial chemoembolization (TACE) includes delivering chemotherapy with embolization. Tumour embolization may also be performed prior to resection.
“GPX exhibited effective and thorough embolization throughout the renal cortical vasculature,” according to a pathology assessment conducted by study pathologist James Stanley. “GPX filled the smallest arteries/arterioles of the distal cortex which was not observed with 40-micron microspheres.”
GPX and microspheres were studied in selected small branches of renal arteries. The GPX embolic device was found to fill vessels more completely and penetrate deeper into smaller vessel beds than the smallest microspheres commonly used for tumour treatments.
“The extent of distal penetration of GPX, combined with its potential as a drug-loadable oncology solution, make this a unique technology with an exciting future in advancing cancer care,” said Danny Smith, Fluidx Medical vice president of research and development.
Selution SLR, MedAlliance’s sirolimus-eluting balloon, has received conditional US Food and Drug Administration (FDA) investigational device exemption (IDE) approval to initiate its pivotal clinical trial for the treatment of occlusive disease of the superficial femoral artery (SFA).
This comes only a few months after the company received IDE approval for Selution SLR in the treatment of below-the-knee (BTK) indications (May 2022).
Enrolment will begin in the SELUTION SLR IDE SFA study later this year. It will be conducted at over 20 centres in the USA and an additional 20 centres around the world. This study will enrol 300 patients to demonstrate superiority over balloon angioplasty (POBA). The principal investigator of this study is George Adams, the director of cardiovascular and peripheral vascular research at Rex Hospital (Raleigh, USA).
“We are very excited that US patients suffering from PAD [peripheral arterial disease] will have the opportunity to receive this novel sirolimus drug coated balloon technology. This is yet another advancement in the field of treating vascular disease and we are confident that this study will enrol quickly,” Adams commented.
“This is a significant milestone for MedAlliance: we are the first non-paclitaxel drug coated balloon to receive IDE approval, and now the first to have two applications approved. This is the culmination of a multi-year research and development programme to provide the comprehensive non-clinical data required to satisfy the very high standards expected by the US FDA,” added Jeffrey B Jump, MedAlliance chairman and chief executive officer. “We are very pleased with the rapid level of sales growth we are experiencing in Europe, Asia and South America and very much look forward to entering the US market.”
Selution SLR was awarded CE mark approval for the treatment of PAD in February 2020 and for the treatment of coronary artery disease in May 2020. The US FDA has awarded Selution SLR with four breakthrough designations: for the treatment of atherosclerotic lesions in native coronary arteries; coronary in-stent restenosis; peripheral below-the-knee and AV-fistula indications.
In August 2021, the first of over 3,000 patients was enrolled in a ground-breaking coronary randomised controlled study comparing Selution SLR with any limus drug-eluting stent [DES]. This is the largest drug-eluting balloon (DEB) study ever initiated.
MedAlliance’s DEB technology involves MicroReservoirs made from biodegradable polymer intermixed with the anti-restenotic drug sirolimus. These MicroReservoirs provide controlled and sustained release of the drug for up to 90 days. Extended release of sirolimus from stents has been proven highly efficacious in both coronary and peripheral vasculatures. MedAlliance’s proprietary CAT (Cell Adherent Technology) enables the MicroReservoirs to be coated onto balloons and adhere to the vessel lumen when delivered via an angioplasty balloon.
Shape Memory Medical announced today that its 1,500th patient has been treated, marking a significant milestone for the company’s portfolio of shape memory polymer embolotherapy devices—the Impede embolisation plug family and the TrelliX embolic coil. The patient was treated by Thomas Maldonado (NYU Grossman School of Medicine and NYU Langone Health, New York, USA).
“We were excited to perform our first case using shape memory polymer technology, and in this particular case for the occlusion of the internal iliac artery for prevention of post-EVAR [endovascular aneurysm repair] type II endoleak,” said Maldonado.
According to a company press release, shape memory polymer is a new concept in medical devices, built on 25 years of polymer research and expertise initiated at Lawrence Livermore National Laboratory (LLNL; Livermore, California) and further developed at Texas A&M University (College Station, USA). Shape memory polymer features a porous, compliant polyurethane embolic material that enables conversion to organised thrombus followed by gradual healthy tissue formation. In 2009, Shape Memory Medical was formed to develop and commercialise devices for use in the peripheral and neurovascular embolisation markets. An emerging alternative to traditional, bare metal embolisation devices, shape memory polymer is soft and conformable, and the material is radiolucent which improves visibility of the surrounding anatomy during and after the procedure.
“This milestone is especially significant for Shape Memory Medical,” said Ted Ruppel, chief executive officer. “This accomplishment is only the beginning of our plans for this emerging technology, with a product pipeline focused on the development of shape memory polymer solutions for aortic aneurysms and aortic dissection.” The company is also pursuing research and development and corporate licensing partnerships for potential applications across multiple therapeutic areas such as aortic therapies, structural heart, biopsy, and drug delivery.
Since the launch of the Impede embolisation plug family in the USA, Europe, and Japan and the TrelliX embolic coil in Europe, these novel devices have been used by vascular surgeons and interventional radiologists in over 25 countries. The growing body of evidence presented from the podium and in the literature has raised physician awareness and interest in the Impede and TrelliX devices, including data from the TrelliX APEX study and the IMPEDE EMBO postmarket surveillance study. The Impede-FX RapidFill device is also currently being evaluated in a first-in-human safety and efficacy trial for a potential new indication for abdominal aortic aneurysm (AAA) sac management during elective endovascular aneurysm repair (EVAR). “Early AAA-SHAPE results are encouraging,” said Michel Reijnen (Rijnstate Hospital, Arnhem, The Netherlands), principal investigator, AAA-SHAPE Netherlands. “Shape memory polymer technology has the potential to improve post-EVAR sac regression, reduce secondary interventions, and reduce the burden for our patients as well as for healthcare systems.” The AAA-SHAPE trial is ongoing, with one-year results expected to be announced in 2023.
Prostate conditions and their treatment proved popular reading topics during the month of July. Interventional News reported on this subject from various angles—from an award-winning abstract on prostatic artery embolization for benign prostate hyperplasia (BPH) and the US Food and Drug Administration (FDA) 510(k) clearance of a new high-flow microcatheter, to new data to support a minimally invasive procedure to treat BPH, and a US FDA investigational device exemption for high-intensity ultrasound therapy for prostate cancer.
Tiago Bilhim (Saint Louis Hospital, Lisbon, Portugal) won the award of best abstract for his and co-authors’ ‘Long-term outcome of prostatic artery embolization for patients with benign prostatic hyperplasia’ at this year’s European Conference on Embolotherapy (ET; 22–25 June, Nice, France).
Embolx, a company developing microcatheters for arterial embolization procedures to treat cancerous tumours, benign prostatic hyperplasia, and uterine fibroids, has announced that the company has filed a 510(k) to the US FDA for its new line of high-flow microcatheters, Soldier.
Merit Medical has announced the successful enrolment of the first patient in its WRAP registry study, which will evaluate the clinical benefits associated with the use of the Wrapsody cell-impermeable endoprosthesis in patients receiving haemodialysis that experience stenosis or occlusion of blood vessels required for dialysis.
The University of Texas at Arlington (UTA; Arlington, USA) announced in June 2022 that Kytai Nguyen, a UTA bioengineering professor, had received National Institutes of Health (NIH) funding to develop a dual-capability biodegradable nanoparticle for use in treating peripheral arterial disease (PAD).
As part of the ‘Trauma and Emergencies’ session at this year’s European Conference on Embolotherapy (22–25 June, Nice, France), conference deputy chairman Otto van Delden (Amsterdam University Medical Centers, Amsterdam, The Netherlands) presented blunt abdominal trauma cases to delegates “to underscore the teaching points” that these types of clinical scenarios offer.
Ra Medical Systems has announced receipt of US FDA 510(k) clearance for the company’s Dabra 2.0 catheter as part of the Dabra excimer laser system. The catheter features enhancements including a six-month shelf life.
Instylla, a company developing liquid embolics for peripheral vascular embolotherapy, recently announced two publications that evaluated the Embrace hydrogel embolic system (HES) in preclinical porcine haemorrhage models.
Teleflex has announced the results of several research studies that further support the safety and efficacy of the UroLift system for men living with enlarged prostate, benign prostatic hyperplasia (BPH), or those who have a wide range of prostate sizes and/or a median lobe obstruction.
Northeast Scientific, a company that reprocesses single-use peripheral vascular catheters, announced recently in a press release that it has received US FDA clearance for reprocessing the Philips Spectranetics 0.9mm over-the-wire Turbo-Elite laser atherectomy catheter.
Insightec, a global healthcare company dedicated to using acoustic energy to transform patient care, announced that it has received US FDA approval for an investigational device exemption (IDE) for a clinical comparative study of the Exablate Prostate system used to treat diseased prostate tissue.
Study team at the University Hospital Münster Germany
Study team at the University Hospital Münster
Concept Medical has announced the initiation of the LIMES trial, which has enrolled 15 patients to evaluate the safety and efficacy of the company’s Magic Touch sirolimus-coated percutaneous transluminal angioplasty (PTA) balloon for the treatment of peripheral arterial disease (PAD).
A Concept Medical press release elaborates that LIMES is a prospective, multicentre, randomised controlled trial (RCT) that is designed and aimed to evaluate the Magic Touch balloon 0.014” and 0.018” versus standard angioplasty in a head-to-head comparison (1:1).
Initiated by the University Hospitals Jena and Leipzig in Germany and led by principal investigator (PI) Ulf Teichgräber (Jena University Hospital, Jena, Germany) alongside co-PI Thomas Zeller (University Heart Center Freiburg-Bad Krozingen, Bad Krozingen, Germany) and Dierk Scheinert (University Hospital Leipzig, Leipzig, Germany), the trial kicked off with the index patient enrolled on 31March 2022 by Nassan Malyar at the University Hospital Münster in Münster, Germany.
LIMES RCT is set to enrol 230 patients in 19 centres across Germany and Austria. The patient population will include patients presenting with documented chronic limb-threatening ischaemia (CLTI) in the target limb defined as Rutherford clinical category 4, 5 or 6 aged ≥18 years. The study evaluates patients with a reference vessel diameter (RVD) ≥2 and ≤4mm and total occlusions (100% stenosis) of the target lesion. There is no minimal lesion length required, no lesion length limitation and no limitation in number of used devices. Follow-up will be per in-house visits at 30 days, six, 12, 24 and 36 months.
The RCT will measure the efficacy of sirolimus-coated balloons in a complex setting (CLTI) of the PAD segment (located below the P3 segment of the popliteal artery to the tibiotalar joint) against the current standard of care. The study’s primary endpoints are the composite of limb salvage and primary patency through six months. The key secondary safety endpoint is the composite of major adverse limb events and perioperative death at 30 days. A blinded core lab will assess patency at six, 12 and 24 months by duplex ultrasound and quantitative vascular angiography in case of any target lesion revascularisation.
In the press release, Teichgräber commented on why the RCT is valuable in terms of DCB intervention in infrapopliteal occlusions: “BTK [below-the-knee] revascularisation deals with the most challenging vascular territory in very sick patients. LIMES will solve the question if sirolimus balloon angioplasty has the potential to become the future standard of care in BTK interventions.”
Mark Little (Royal Berkshire NHS Foundation Trust, Reading, UK) described the emergence of, and advancement within, musculoskeletal (MSK) embolotherapy as “fast-paced” during his presentation on the trends and developments in the field, delivered at this year’s European Conference on Embolotherapy (22–25 June, Nice, France). Featuring in the meeting’s Joints session, the presentation’s take-home message was that the “signs are encouraging” when it comes to MSK embolotherapy’s integration into more mainstream practice.
Among the opening statements from Little was the “[importance of discussing] agents”—“different territories need different embolic agents,” he informed delegates. For osteoarthritis of the hand or tendinopathy in the foot, “you would not want a permanent embolic”, which is where the “antiquated” antibiotic imipenem, in combination with cilastatin, comes in. It acts as a temporary embolic agent, Little explained, and it has “rapidly emerging potential.”
For example, for plantar fasciitis, which is “really difficult to treat” and “extremely painful”, imipenem/cilastatin (I/C) can be injected into the posterior tibial artery, resulting in reduced pain and plantar fascia thickness. Sports medicine, Little went on, is “a real growth area” for MSK embolotherapy, as hyperaemia that cannot be treated conservatively may be resolved with agents such as I/C. However, a current limitation, Little acknowledged is the fact that I/C is not approved for embolotherapy in many countries, and the UK and USA are not among those where approval is granted.
Nevertheless, Little conveyed the significance of the fact that MSK embolotherapy has the potential to treat “a breadth of conditions,” listing tennis elbow, for which surgical options are limited, and adhesive capsulitis, which is increasingly prevalent as a result of the increasing prevalence of diabetes.
Little then turned to his area of specialism—genicular artery embolization (GAE)—which has the “largest evidence base to date” of all MSK embolotherapies. “We have done a lot of work looking at GAE and how we can refine the treatment,” he supplemented.
By way of example, Little referred to imaging from one of his own cases—medial compartment knee osteoarthritis, which “[showed] a large area of abnormal synovitis.” The approach for this patient was to cannulate the superior medial genicular artery, Little detailed, but, crucially, “to maintain the normal in-flow vessel.”
This is “very different” to the endpoint for prostate arterial embolization—”we are not wanting to completely block the in-flow vessel”, the result of which could be necrosis. Instead, Little “[prunes] the area of abnormality while maintaining normal osseus blood flow.”
To further illustrate the potential of MSK embolotherapy, Little referenced a small study of I/C to treat chronic lower back pain that had not been responsive to conservative therapy. However, given the size of the cohort, “we still have a lot more work to do”, he admitted.
Moving on the address the scientific rationale for MSK embolotherapy, Little described how the conditions are “underpinned by [an] area of hyperaemia.” New abnormal blood vessel formation “results in the release of cytokines” followed by “[hypersensitisation] of the nerves” and “pain”.
Next on the agenda for Little was to outline how “new” pain as a symptom to treat actually is within interventional radiology (IR)—typically, the means of assessing pain-related outcomes of treatment has been limited to the visual analogue scale. But, “what if your pain goes from a 10 to a 5?” Little asked rhetorically, “what does that mean in patients’ daily lives?” This is where minimally clinical important difference as a measure of pain outcome has a role to play—except that what that looks like for GAE is, “right now, anybody’s best guess.” Hence, this should be an area of focus in the field, Little advised. An “interesting area of future research” will be “the interplay between the brain and the knee”, as “how patients view pain impacts their progress,” Little then asserted.
The presenter summarised the scope for MSK embolotherapy’s more widespread use as “encouraging”. Recent National Institute for Health and Care Excellence (NICE) guidelines want evidence for its effectiveness, Little shared, in the form of “randomised controlled trials [RCTs] against sham procedure or best current practice,” with more patient-reported outcomes. GENESIS 2—an RCT against sham procedure—is, therefore, a study to watch. Little sees longer-term data and multicentre studies following on from this.
Fielding questions from the audience following the presentation, Little responded to an enquiry into whether use of antibiotics as temporary embolic agents could lead to patients developing resistance. “A good question—I have no idea”, Little admitted, going on to say “one would intuitively think, yes.” He then acknowledged that the main issue with antibiotics for this indication is the “East/West divide”—“we [in the UK] are very much limited”, as a result of the temporary agent I/C’s lack of availability.
A follow-up question on his preferred embolic material saw Little state that the MSK community is “crying out for imipenem” and all of its “mystical, magical properties” when it comes to treating hands and feet. For knees, he continued, “there is good data for permanent embolics”.
2Fr XO Cross 14 microcatheter shown with a 0.014” guidewire
2Fr XO Cross 14 microcatheter shown with a 0.014” guidewire
Transit Scientific has reported multiple successful peripheral vascular procedures with the XO Cross catheter platform utilising pedal retrograde access.
The non-tapered 2Fr XO Cross 14 microcatheter in 90cm, 135cm, and 175cm lengths is designed to facilitate guidewire support, guidewire exchange, and contrast media injection during complex peripheral vascular interventions.
“2Fr 014 catheter-guidewire systems are an important tool for pedal and below-the-knee interventions,” said George Adams (UNC REX Healthcare, Raleigh, USA). “The XO Cross incorporates a non-tapered torquable shaft design which supports a smaller and less invasive access site from below. Tools like these can help broaden options for approaches and access techniques in CLTI [chronic limb-threatening ischaemia] patients.”
According to a Transit Scientific, the XO Cross catheter platform introduces new levels of pushability, trackability, flexibility, and torque response to access challenging lesions and complex anatomy. XO Cross’s non-tapered, metal-alloy and polymer construction delivers high fatigue resistance against tough lesions found in late-stage peripheral arterial disease (PAD) and CLTI, the company claims.
Richard Saxon (Tri-City Medical Center, Oceanside, USA) shared: “A patient presented with trifurcation disease and severe calcifications in the superficial femoral artery (SFA), popliteal, and the posterior tibial artery. The low-profile and pushability of the XO Cross 14 enabled pedal retrograde access following failed crossing and wire from above. A second XO Cross 14 (135cm) was used from above to support a flossing technique and subsequent angioplasty treatment. The unique non-tapered design of the XO Cross lends itself well to challenging limb salvage procedures that often require multiple access sites and different approaches to achieve a good outcome.”
Transit Scientific’s XO Cross platform features 24 US Food and Drug Administration (FDA)-cleared devices including 2Fr XO Cross 14 microcaths, 2.6Fr XO Cross 18 microcaths, and the 3.8Fr XO Cross 35 support catheters for use with standard 0.014”, 0.018”, and 0.035” guidewires in 90cm, 135cm, 150cm, and 175cm lengths.
A database study titled ‘Unplanned 30-day readmissions and in-hospital outcomes for the management of submassive and massive acute pulmonary embolism: Catheter-directed versus systemic thrombolysis’ has produced results that could provide some of the evidence base for preference of catheter-directed over systemic thrombolysis in treating the more severe cases of pulmonary embolism (PE).
Osman Ahmed, who is author of the study and associate professor of radiology at the University of Chicago (Chicago, USA), met with Interventional News at the Society of Interventional Radiology (SIR) 2022 Annual Meeting (11–16 June, Boston, USA) to discuss his research. The abstract was also presented by Waseem Wahood (Dr Kiran C Patel School of Allopathic Medicine, Fort Lauderdale, USA) during the meeting’s pulmonary embolism session.
Ahmed began by outlining his clinical background and what led him to pursue this research on PE treatment. Clinically, he explained, one of his main interests is venous thromboembolism, but being the co-chair of the SIR Comparative Effectiveness Research Committee—an arm of the society whose goal is to develop “evidence-based data to compare interventional radiology [IR] services and procedures with their medical and surgical alternatives”—he wanted also to incorporate this area of focus into a study.
The first question posed to Ahmed was regarding the existing PE treatment landscape and what determines whether a given patient will receive catheter-directed or systemic thrombolysis. Ahmed dubbed this “a great question” to which the answer lies in the fact that “PE in general is a heterogenous disease, with different levels of severity”—massive, submassive and low-risk. “Fortunately,” he continued, “most patients are low risk”. Expanding on this, Ahmed specified how it is the massive and submassive patients who “require hospitalisation and often follow-up intervention,” which is, “where IR comes into play.”
One of the key advantages of the catheter-based approach is that it is minimally invasive, Ahmed pointed out, however, “most society guidelines [for PE treatment] outside of IR […] do not recommend what we do.” Ahmed asserted his nonetheless widely shared belief that catheter-based thrombolysis is “safe.” Studies carried out before his, while smaller, showed “a similar rate of effectiveness” between catheter-based and systemic treatments, but the former saw “lower rates of bleeding.” Ahmed referred to this existing, promising evidence as motivation for doing his database study.
Asked then why he choose to approach the study from the angle of side effects, Ahmed offered by way of explanation the “very high chance of recurrence” with PE. “If you survive [the rate can be between] 30 and 40%”. Furthermore, Ahmed underlined, the nature of the treatment means that “if you give too much of the [PE] medication, the risk of bleeding is high, but too little and you do not clear the PE.”
Bleeding was “a big problem” in the patients from the database who had received systemic over catheter-based treatment, which often resulted in rehospitalisation—problematic in that it depletes resources and beds for patients with other conditions, Ahmed highlighted.
Moving on to discuss the results of his study—whether or not they were as expected—Ahmed conveyed how he had been surprised by how they were “very, very consistent with what we thought”. This was the case for “every metric [and even with] propensity matching.” Ultimately, rates of intra-abdominal and intracranial bleeding, as well as hospital readmissions were “all one to two times higher with systemic thrombolysis.” Ahmed acknowledged that it was an outcome that “almost felt too good to be true,” especially since the patients at higher risk of bleeding are often those who receive catheter-directed treatment. “If we were going to see no difference,” Ahmed admitted, he would have expected it to be as a consequence of the sickest patients receiving this less evidence-based treatment.
Finally, conversation turned to next steps regarding the picture of PE treatment and research in the future. “Trials […] take a lot of time and cost a lot of money,” Ahmed emphasised, which, in turn, accentuates “the beauty” of his study, conducted with a 36,000-strong patient base. “We really need [more] trials,” Ahmed affirmed, expressing his hope that the promising results his research has yielded will “pave the way” for increased government funding assigned to future PE research.
Yet, of note, is the fact that even without these prospective trials and the inclusion of catheter-directed thrombolysis in the majority of PE treatment guidelines, there has been, of late, a “tenfold increase” in the recourse to catheter-directed treatment. Ahmed ended on the following note—”We are hoping that [our study] helps provide the framework” to include catheter-directed thrombolysis in guidelines more widely.
Biotronik recently announced that it has received US Food and Drug Administration (FDA) approval of its Pulsar-18 T3 peripheral self-expanding stent system. Full US commercial launch of the device, which will begin in early August, according to the company.
Biotronik states that the Pulsar-18 T3 stent system uniquely combines three technologies. A 4 French low-profile delivery system may decrease the risk of access site complications and reduce the need for closure devices when compared to 6 French devices, the company claims. It adds that the triaxial system with braided shaft design facilitates stable and accurate implantation of the clinically proven Pulsar stent and, with its thin struts and low chronic outward force (COF), the Pulsar-18 stent contributes to a reduced mean area of restenosis.
The redesigned Pulsar-18 T3 stent system offers physicians an “intuitive and ergonomic” wheel-operated handle for one-handed stent release enhancing the ability to control deployment, according to Biotronik.
“I was immediately impressed by the new concept of the Pulsar-18 T3 system,” said Koen Deloose (AZ Sint Blasius Hospital, Dendermonde, Belgium). “The combination of having a very ergonomic handle combined with a triaxial system and also everything in a 4 French concept was, for me, quite unique.”
“The Pulsar-18 T3 stent system is an innovative solution that delivers clinically proven performance—providing effective therapy that is easy to use for physicians while minimizing metal burden and may reduce the risk of restenosis for patients,” stated David Hayes, chief medical officer, Biotronik.
Biotronik will offer the Pulsar-18 T3 in up to a 200mm stent length for treatment of long lesions, the company advises.
Biotronik details that the Pulsar-18 T3 stent system is indicated for use to improve luminal diameter in patients with symptomatic de novo, restenotic or occlusive lesions located in the superficial femoral or proximal popliteal arteries, with reference vessel diameters from 3–6mm and total lesion lengths up to 190 mm.
Instylla, a company developing liquid embolics for peripheral vascular embolotherapy, recently announced two publications that evaluated the Embrace hydrogel embolic system (HES) in preclinical porcine haemorrhage models.
In a Journal of Vascular and Interventional Radiology (JVIR)publication, Gandras et al evaluated the ability of Embrace HES to achieve haemostasis in a porcine mesenteric artery haemorrhage model that replicates injury in humans. Results demonstrated that Embrace HES achieved complete, rapid, and durable embolization in 100% of the injured arteries with a mean delivery time of 5.3 minutes. There was no angiographic evidence of non-target embolization.
“Embrace was effective in achieving haemostasis in an animal haemorrhage model without evidence of non-target embolization. This next generation liquid embolic has tremendous potential to play an important therapeutic role in a wide variety of clinical applications including haemorrhage and interventional oncology,” commented Eric Gandras, associate chief of vascular and interventional radiology at North Shore University Hospital, (Manhasset, USA) and lead author of the study.
In an independent study conducted by Kauvar et al, splenic injury and resulting haemorrhage were induced in swine models. A comparison was made between a control group having no embolic treatment to treatment groups that received embolization with Embrace HES, gel foam slurry, or coils. Under coagulopathic conditions, Embrace HES showed improved survival time and a significant reduction in bleeding compared to the control group, gel foam slurry, and coil treatments.
Northeast Scientific, a company that reprocesses single-use peripheral vascular catheters, announced recently in a press release that it has received US Food and Drug Administration (FDA) clearance for reprocessing the Philips Spectranetics 0.9mm over-the-wire Turbo-Elite laser atherectomy catheter.
This is the first time the FDA has awarded a 510(k) clearance for reprocessing this type of atherectomy catheter.
The device is used to treat peripheral arterial disease (PAD) and emits high-energy ultraviolet light to vaporise blockages inside the vessels.
Chief executive officer and and founder Craig Allmendinger discussed what this means to the company, saying, “It is validating to receive this clearance from the FDA after all the work our team undertook to meet the standards of earning a 510(k). The team at the FDA pushed us hard, and rightfully so, to prove that our methods and processes created an equivalent device to the original after reprocessing.”
He went on to say, “There is no doubt now that what we are doing is helping redefine the medical device landscape as we add another device type to our reprocessing portfolio. As we continue to expand our device types and reach, we look to further help the office-based lab physician and never compromise on patient safety.”
The company has said that it will have an additional announcement soon regarding when the 0.9mm over-the-wire Turbo-Elite laser atherectomy catheter device will be available for sale.
ReCor Medical and Otsuka Medical Devices have announced that the RADIANCE II US Food and Drug Administration (FDA) investigational device exemption (IDE) pivotal trial evaluating the Paradise ultrasound renal denervation (uRDN) system as a treatment for hypertension met its primary efficacy endpoint, demonstrating a statistically significant reduction in daytime ambulatory systolic blood pressure between treatment and a sham procedure measured at two months.
The RADIANCE II US FDA IDE pivotal trial is a randomised, sham-controlled clinical trial of the ReCor Paradise uRDN System for the treatment of patients with uncontrolled hypertension. 224 patients with mild-to-moderate uncontrolled hypertension, previously treated with up to two medications, were randomised while off medications at more than 60 study centres in eight countries.
“Despite the truly formidable challenges of conducting a complex clinical trial in the throes of the COVID-19 pandemic, we are thrilled to observe these positive results of RADIANCE II, especially in light of those we have previously reported from RADIANCE-HTN SOLO and TRIO,” said study principal investigators Ajay Kirtane (Columbia University, New York, USA) and Michel Azizi (Hôpital Européen Georges Pompidou, Paris, France). “We cannot adequately convey our thanks to the patients, coordinators, and study physicians for their collective efforts, and we very much look forward to being able to present and publish the complete study details in the near future.”
“We at Otsuka are very pleased with the positive outcome of the RADIANCE II study,” said Kazumichi Kobayashi, executive deputy president of Otsuka Medical Devices. “With three successful clinical trials of the Paradise uRDN system, we believe even more strongly that the Paradise system can become an important treatment option for patients and physicians struggling to control blood pressure.”
“ReCor is thrilled that the RADIANCE II trial met its primary efficacy endpoint. Following the positive SOLO and TRIO clinical trials, RADIANCE II adds to the evidence for the Paradise system as a potential future treatment for patients with uncontrolled hypertension,” said ReCor president and CEO, Andrew M Weiss. “We would like to express our gratitude to the principal investigators, steering committee and all investigators for their efforts throughout this important trial.”
RADIANCE II is the third and largest component of ReCor’s RADIANCE Global Program—randomised and sham-controlled studies evaluating the Paradise uRDN System in patients with hypertension. The first two studies in the series are the previously reported RADIANCE-HTN SOLO (conducted in patients with mild-to-moderate hypertension) and TRIO (conducted in those who remained hypertensive despite being on antihypertensive therapy). Both studies met their primary effectiveness endpoints.
About 6.5 million Americans over the age of 40 suffer from peripheral arterial disease (PAD). In the USA, Black adults in their 50s are at least twice as likely to suffer from PAD as their white counterparts, a disparity that continues to increase with age.
In a new paper published in Circulation, researchers at the Richard A and Susan F Smith Center for Outcomes Research in Cardiology at Beth Israel Deaconess Medical Center (BIDMC; Boston, USA) conducted a large, nationwide analysis of Medicare beneficiaries to document racial differences in revascularisation treatment for PAD, and outcomes for patients with PAD. The team found that Black adults underwent significantly more endovascular peripheral vascular interventions (PVI), were treated for more advanced disease and were also more likely to experience adverse outcomes following PVI procedures, including amputation and death.
“Black race was significantly associated with worse one-year outcomes after revascularisations, after adjusting for age and sex,” said senior corresponding author Eric Secemsky, director of Vascular Intervention at BIDMC, as well as section head of Interventional Cardiology and Vascular Research at the Smith Center for Outcomes Research at BIDMC. “This link persisted after we adjusted for individual and regional socioeconomic factors. However, the association between Black race and worse outcomes was no longer apparent after we adjusted for comorbidities, suggesting that the well documented Black-white disparities in the prevalence of PAD risk factors, including hypertension, diabetes and end-stage renal disease, explain the disproportionate development of PAD among Black adults.”
The analysis included 215,320 patients who underwent the gold-standard revascularisation procedure—PVI—between 2016 and 2018. Black adults had a higher incidence of treatment, with 0.86 percent of Black Medicare beneficiaries undergoing the procedure, compared to 0.51 percent of white Medicare beneficiaries. What is more, a greater proportion of Black adults were treated for more severe arterial disease, while more white patients were treated for a milder form of PAD. Despite their relatively greater severity of disease, a lower percentage of Black adults were prescribed key cardiovascular medications.
“Structural racism perpetuates these health disparities,” said Secemsky, who is also an associate professor of Medicine at Harvard Medical School (Boston, USA). “One important way in which these systemic and structural factors lead to worse outcomes in Black patients is through comorbidities. This suggests a critical need for targeted, upstream intervention to reduce the disproportionate burden of PAD in the Black population.”
Co-authors included Sahana Natesan, Rishi K Wadhera, Siyan Chen, Yang Song, and Robert W Yeh of the Smith Center at BIDMC; Michael R Jaff of Harvard Medical School; and Jay Giri and Howard Julien of the Perelman School of Medicine, University of Pennsylvania (Philadelphia, USA).
Monica Webb Hooper, deputy director of the National Institute on Minority Health and Health Disparities (Bethesda, USA) works to help reduce healthcare disparities and improve minority health. Among the subjects of her presentation at the second plenary of the Society of Interventional Radiology (SIR) 2022 Annual Meeting (11—16 June, Boston, USA) was the “relationship between racial discrimination and health,” of which a key takeaway was that there is “well documented evidence [that] racism worsens health,” and that therefore it is incumbent upon healthcare professionals to take steps to redress the imbalance.
Webb Hooper began her talk by clarifying that “characteristic differences between population groups, [such as sickle cell disease and colour blindness]” are not the same as health disparities. In contrast to the former, which are determined by genes or biology, the latter result from “disadvantage at multiple levels”. However, the nature of these “systemic obstacles” that racial minority groups face is such that they are “modifiable, by definition.”
Listing some “considerable” disparities when it comes to racial and ethnic minority health, Webb Hooper included overall shorter life expectancy, infant mortality, cardiovascular disease, lung cancer, sexually transmitted infections, mental health difficulties, dental ill-health and COVID-19. Webb Hooper then delved into the reasons why this is the case, beginning by highlighting how Black or African American, American Indian or Alaska Native, and Hispanic or Latino populations are all less likely to be diagnosed early with lung cancer. Consequently, they receive less treatment. Underpinning these inequities, Webb Hooper posited, it is “the assumption” among physicians and scientists “that genetics are responsible” for health issues among these groups, based on which may be less motivation and perceived necessity to intervene medically.
“Race is a sociocultural construct that has varied over time,” Webb Hooper then relayed, but that what has been constant is the “discrimination and chronic stress” to which racial and ethnic minority groups have been subjected. This is why, she noted, it is important to understand “what happens outside the body and how it affects what is going on inside the body.” A further key message for delegates was that “population differences are not the same as health disparities,” and it is believing that they are that hampers “further investigation” into the causes of these health disparities.
Conveying the degree to which racial and ethnic minority groups receive inferior care as a result of ill-founded beliefs around race and health, Webb Hooper asserts that “irrespective of socioeconomic status, [these groups] are more likely to be denied pain medication and opportunities to take part in clinical trials.”
Webb Hooper then took time to reiterate how we must accept the following commonly held belief as flawed: that health disparities either stem from biology, and therefore are not modifiable, or they have cultural underpinnings, and thus the onus lies with the members of said culture to change. There are “clear indicators” of the effects of personal, institutional and structural racism on health, which cannot be ascribed to biological nor cultural factors.
Webb Hooper then discussed the longstanding need to increase the representation among members of racial and ethnic minority groups in clinical trials. Webb Hooper’s first recommendation for how to achieve this is to “focus on setting standards for inclusion a priori.” This may mean making adjustments to inclusion criteria so as to include a sample of racial and ethnic minority individuals that reflects the wider population—this is 19% Hispanic or Latino in the USA, Webb Hooper offered by way of example.
The second recommendation she gave was to “focus on individuals’ motivations for participating in a clinical trial,” and once identified, turn those motivations into active participation. Thirdly, it is necessary to “address the reasons for low participation” among racial and ethnic minority groups. “Research teams must be willing to change their enrolment process,” she averred, suggesting that to inform this, community groups are consulted to gain on-the-ground insight into current attitudes around clinical trials. It is a case of asking more racial and ethnic minority patients to participate and recognising that they are just as willing to, Webb Hooper underlined.
Labelling these groups as “hard to reach” is an excuse, Webb Hooper concluded.
As part of the ‘Trauma and Emergencies’ session at this year’s European Conference on Embolotherapy (22–25 June, Nice, France), conference deputy chairman Otto van Delden (Amsterdam University Medical Centers, Amsterdam, The Netherlands) presented blunt abdominal trauma cases to delegates “to underscore the teaching points” that these types of clinical scenarios offer. In the course of his presentation, he addressed key questions an interventional radiologist (IR) may have regarding the treatment of blunt abdominal trauma, including “which embolic agent and technique [you should] choose for the most frequently encountered injuries.”
A noteworthy feature of this session overall was audience interaction; with each case presented, the speaker posed the question of whether to embolize and, if so, which agent to use, to the floor, before commenting on how closely the consensus from the room aligned with their preferences and choice in the real-life scenario about which they were speaking. Van Delden’s presentation gave him opportunity to convey his feeling that “blush” on a computed tomography (CT) image—indicative of vascular injury—is not a solely sufficient reason for embolizing, but that when it does not “resolve itself”, and the IR has also taken into account “age, coagulopathy and fragility”, it can be a good approach.
In both the cases van Delden put to the audience, opinion was split down the middle on whether or not to embolize, highlighting the multifaceted decision-making involved in intervening in these trauma situations. Van Delden summarised for the audience that, if they themselves are faced with the question of whether or not to embolize, the factors to consider are the extent of organ injury, haemoperitoneum, and vascular lesions, which can be seen on CT. Expanding on this, van Delden listed some of the vascular lesions, in the presence of which, embolization may be indicated: active extravasation outside or within the organ, and false aneurysm. If high-grade organ injury or enlarging haemoperitoneum show on a CT scan, then these are “predictors” of an embolization, van Delden also noted.
Coils were the most popular means of embolization among audience members for the cases van Delden presented, with 71% of the vote for the splenic injury case, which was one of those detailed by the presenter. Although coils may be a favoured choice, “you need to choose the size carefully,” van Delden cautioned, as it is essential not to occlude too much vessel, nor to have the coil move within it.
Then addressing the question of proximal or distal embolization, van Delden acknowledged that “there is no consensus” on which is best, and that it can be down to IRs’ preferences as individuals and “multiple different variables.”
“Tortuosity of vessels” and “time pressure” also come into embolization-related decisions, the presenter added, reinforcing his earlier point that embolization for trauma can divide opinion and resist consensus. “Although coils are the mainstay for treating liver injury,” a little over the majority of voting delegates would have chosen a gelfoam agent in the instance shown on screen by Van Delden, who conceded that depending on coagulopathy, a non-coil embolization may be more suitable.
The University of Texas at Arlington (UTA; Arlington, USA) announced in June 2022 that Kytai Nguyen, a UTA bioengineering professor, had received National Institutes of Health (NIH) funding to develop a dual-capability biodegradable nanoparticle for use in treating peripheral arterial disease (PAD).
The US$2.1 million grant will allow Nguyen, in collaboration with Jian Yang, a Penn State University (University Park Pennsylvania, USA) bioengineering professor, and Ralph Mason, a professor of radiology at UT Southwestern (Dallas, USA), to investigate the potential applications of a drug-delivering, fluorescent polymer. Nguyen discussed her project with Interventional News, shedding light on key aspects of this research.
Nguyen opened the conversation by recounting the emergence of nanotechnology: “I began working at UTA in 2005,” she relayed, “and at this time, nanotechnology was still new. I was interested in whether I could apply [a] nanoparticle as a drug carrier and an imaging agent.”
It was not in the PAD space that Nguyen initiated her research, however. She explained that “at first, we worked with cancer, and cardiovascular and lung disease.” The motivation for entering into this area of research stemmed from the fact that drug delivery to treat these conditions often results in side-effects for patients, she outlined. “When you deliver a drug, it will go all over the body […] Many drugs are effective, but toxic to the body.” This is where nanoparticles come in, she proceeded to detail, as they can be more specifically targeted within the body. In turn, this has “the potential to reduce side-effects.” This would amount to an improvement on existing treatments for PAD, as, like those for cancer, and cardiovascular and lung disease, drugs, as they are delivered currently, cannot always be targeted with desirable accuracy.
Then probed about the dual capabilities of both drug delivery and imaging compatibility, Nguyen shared how the polymer she is researching is naturally fluorescent. This means, she expanded, that “we can use multiple imaging modalities,” of which ultrasound is one, to determine “the location and quantity of the particle delivered.” This speaks to the shortcomings of current drug delivery methods, which lie in the fact they cannot be as easily localised. With the drug “encapsulated” inside the very polymer that facilitates precise imaging, there is no need for a separate “toxic quantum dye” in addition to the drug, to highlight where in the body the drug has travelled. “We can chase this polymer [over time],” Nguyen summarised. For PAD specifically “we want to focus on the muscle and where [within it] the nanoparticle ends up.”
Next on the discussion agenda was the significance of the polymer’s biodegradability: “We want [it to be] biodegradable so it will leave the body and not accumulate,” Nguyen stated. It is crucial, she went on, to be able to re-administer the drug “many times” when treating PAD, but drug carriers, some of which contain metals, can become toxic to the body in the long term. Her nanoparticle, however, can be “cleared by the body,” while allowing the drug it contains to act where it is targeted.
Nguyen ended by casting her mind forward to the next five years, and the milestones that await them in this project. As far as the here and now is concerned, research is at the in vitro study stage, Nguyen elucidated, underlining that “much more work” will be necessary before they can test on humans. “We are testing on mice […but] hopefully, if everything is successful, we will move on to larger animals.” Clinical trials are likely to be at least five years away, Nguyen advised.
Embolx, a medical device company developing microcatheters for arterial embolization procedures to treat cancerous tumours, benign prostatic hyperplasia, and uterine fibroids, has announced that the company has filed a 510(k) to the US Food and Drug Administration (FDA) for its new line of high-flow microcatheters, Soldier. It uses the same ultra-thin wall (UTW) technology initially developed for its flagship product Sniper.
UTW technology allows microcatheters to be smaller in outer diameter yet maintain the largest possible internal lumens. UTW, in combination with Soldier’s unique design, enables it to display best-in-class tracking, torquing, and flow rates. Currently available in Europe, Soldier’s arrival on the US market is expected to shift the paradigm and set a new standard for both high-flow microcatheters and micro-microcatheters.
“Soldier is a superior microcatheter by all measures of performance,” said Michael Allen, president, and chief executive officer of Embolx.”Using our proprietary and patented technology we are expanding our best-in-class catheter products for use in the peripheral vasculature and neurovasculature.”
The Soldier microcatheter will be available in 2.0Fr and 2.5Fr and will come in three lengths—130cm, 155cm, and 165cm. The 2.0Fr offers an 0.022″ lumen and the 2.5Fr offers an 0.027″ lumen.
The addition of the Soldier product line will expand the use of Embolx products for all types of embolization, immunotherapy, and drug-delivery procedures.
Subtle Medical, a key provider of artificial intelligence (AI) solutions for medical imaging, and Siemens Healthineers have officially announced the integration of Subtle Medical’s SubtleMR image-enhancement software into the new reconstruction pipeline of Siemens Healthineers, Open Recon. The launch was communicated in a Subtle Medical press release.
SubtleMR offers deep learning post-processing for denoising and increased sharpness on faster magnetic resonance imaging (MRI) sequences, enabling improved image quality, optimised workflow, and a better patient experience.
SubtleMR will be available on Siemens Magnetom Sola, Solafit, and Altea scanners with NX VA51. The software works with major contrasts, including T1, T2, T2 FLAIR, T2 (2D, 3D) and is compatible with the majority of MRI procedures. It is compatible with all downstream quantitative and diagnostic applications.
The Open Recon interface of Siemens Healthineers is designed to enable third-party image reconstruction and post-processing solutions to be directly integrated in the reconstruction pipeline. This way, no additional image export step is necessary, and the results are directly available on the scanner console. The reconstruction including post-processing with SubtleMR is now selectable in the user interface.
“We are proud to become the first AI technology company Siemens Healthineers has entrusted with their innovative new Open Recon interface,” said Ajit Shankaranarayanan, Chief Product Officer at Subtle Medical. “This milestone marks how powerful collaborations are between AI innovators and scanner manufacturers in order to provide the most robust imaging solutions to providers and the best care possible to patients worldwide.”
Subtle Medical’s suite of clinically validated AI-powered software solutions, SubtleMR and SubtlePET, increase the efficiency of image capture by improving the quality of both accelerated and low-dose imaging. Subtle’s solutions are compatible with all scanner models and field strengths.
Cordis has announced the start of the RADIANCY premarket clinical study in Europe.
A press release details that RADIANCY is a prospective, multicentre, single-arm study to assess the safety and efficacy of the S.M.A.R.T. Radianz vascular stent system intended for treatment of lesions in the iliac, superficial femoral, or proximal popliteal arteries via radial artery access through 30-day follow up.
The first procedure was performed by Mercedes Guerra (University Hospital of Guadalajara, Guadalajara, Spain) using the Brite Tip Radianz guiding sheath and Saberx Radianz percutaneous transluminal angioplasty (PTA) balloon catheter to facilitate delivery of the S.M.A.R.T Radianz self-expanding stent in an iliac lesion.
Upon completion of the procedure, Guerra said: “My colleagues and I are pleased to have the opportunity to perform the first case in this significant clinical study. We applaud Cordis for pursuing the technological innovation to meet the need for radial access solutions in lower extremity interventions. We look forward to contributing our findings to the global endovascular community as part of the RADIANCY clinical study.”
The RADIANCY study, led by principal investigator Raphaël Coscas (Ambroise Paré Hospital, Boulogne-Billancourt, France), is planned to enrol 159 patients at approximately 15 sites across seven European countries. “The RADIANCY study initiation marks a new course for the future management of patients with peripheral arterial disease (PAD) by expanding their treatment options from current conventional femoral to radial access,” Coscas said.
Coscas also highlighted the era of practice evolution in this space: “As the gold-standard approach in coronary interventions, radial is in its exciting inception phase for PAD and offers unequivocal patient-centric advantages in terms of early mobility and comfort, critical in both in-patient and out-patient practice settings.”
The S.M.A.R.T. Radianz vascular stent system, specifically engineered for radial access, was approved by the US Food and Drug Administration (FDA) earlier this year, and successful first-in-human procedures were performed in June 2022 by Jihad Mustapha (Cardiac & Vascular Centers for Amputation Prevention, Grand Rapids, USA).
George Adams, Cordis chief medical officer, said: “Cordis is committed to developing tools to treat complex PAD patients. Understanding the real-world, 10-year S.M.A.R.T. vascular stent system data combined with the innovation of a radial approach allows the interventionalist to treat PAD safely, efficaciously, and cost effectively. Mirroring this innovation with research and a strong educational program to advance the field is truly at Cordis’ core.”
SoniVie today announced that on 30 May this year the first patient was treated with its renal artery denervation Tivus therapeutic intravascular ultrasound technology,as part of the recently US Food and Drug Administration (FDA) investigational device exemption (IDE)-approved REDUCED1 pilot study to treat hypertension.
A company press release details that the procedure was successfully performed with Tivus at the Kaplan Medical Center (Rehovot, Israel) by Michael Jonas, principal investigator of the REDUCED1 study.
Jonas commented: “We were able to use the Tivus catheter to rapidly and efficiently perform ultrasound-based renal denervation in our patient suffering from uncontrolled hypertention. The Tivus catheter’s excellent ease of use and its ability to denervate at significant depth of the perivascular space allowed for a short, simple and straightforward procedure. We will closely follow our patient and look forward to continuing enrolment in this exciting trial.”
Renal denervation with Tivus is a minimally invasive procedure that uses high-frequency non-focused ultrasound energy to ablate nerves in the renal artery, SoniVie advises in the press release. This causes a reduction in the nerve activity, which may decrease blood pressure. The procedure is designed for patients who suffer from resistant hypertension.
“Millions of people worldwide suffer from resistant hypertension which substantially increases the risk of heart attack, stroke and kidney failure. We are genuinely happy for this important step forward. There is a lack of effective therapeutic solutions for these patients” says Christian Spaulding, CMO, SoniVie.
“This procedure represents a great fulfilment for SoniVie team, whose expertise and achievements have been focusing on developing Tivus technology for the renal denervation indication, both providing a promising treatment to the hypertensive patient and a high performing, easy to use device to the physician”, says Tomaso Zambelli, CEO, SoniVie.
A prospective, multicentre study involving the Covera vascular covered stent (BD) has confirmed the benefits of immediate, post-percutaneous transluminal angioplasty (PTA) placement of the device in treating arteriovenous graft (AVG) venous anastomotic stenosis when anatomically and clinically suitable. Writing in the Journal of Vascular and Interventional Radiology (JVIR), Bart Dolmatch (Palo Alto Medical Foundation, Mountain View, USA) and colleagues report a 30-day freedom from safety-related events of 96.4% and a six-month target lesion primary patency (TLPP) of 70.3% with the Covera stent.
The authors begin by noting that, as per three prospective, multicentre, randomised trials, placement of a covered stent has previously led to statistically superior TLPP rates compared to PTA alone in restoring flow and maintaining haemodialysis access.
They add that the current study, AVeVA (Arteriovenous stent graft in the treatment of stenosis at the graft-vein anastomosis of AV graft circuits), examined a self-expanding nitinol covered stent (Covera) that is more flexible than the device used in two of those prior studies (Flair, BD).
AVeVA study
Between August 2016 and February 2017, 110 patients were treated by investigators across 14 US centres in AVeVA—a single-arm, investigational device exemption (IDE) study without a concurrent control. Dolmatch and colleagues note that, because prospective trials of previous-generation covered stents had been completed and published, and the devices had been approved by the US Food and Drug Administration (FDA) for the indication being studied, pooled mean values from these trials as well as additional published data on the use of PTA alone for haemodialysis graft stenosis were used to develop safety- and patency-related performance goals for AVeVA.
The primary safety endpoint was 30-day freedom from an adverse event involving the access circuit resulting in additional intervention, surgery, hospitalisation or death. The primary efficacy endpoint was six-month TLPP, or the interval following treatment until the next clinically driven reintervention at the site of the target lesion or until the AVG was abandoned. Prespecified secondary endpoints included acute technical and procedural success, access circuit primary patency (ACPP), cumulative patency, number of reinterventions, index of patency function (IPF), and adverse events through two years.
Of the 181 patients who gave informed consent to participate, 71 did not meet the study eligibility criteria—with 75% deemed not to have angiographic evidence of ≥50% stenosis and clinical evidence of graft dysfunction—meaning 110 patients (mean age=64.3 years, 54.5% female, mean body mass index [BMI]=28.7kg/m2) were ultimately enrolled and treated with the Covera device. The vast majority (98.2%) had an upper-arm AVG.
New Covera data
The authors detail that the mean anastomotic lesion stenosis at the time of treatment was 71.5%, decreasing to a mean residual stenosis of 21% following PTA predilation. One covered stent was used to treat each study lesion, meaning 110 stents were deployed, and all but two of these were postdilated. The mean residual stenosis at procedure completion was 0.9%, Dolmatch and colleagues report. In all cases, the covered stent was deployed to the intended location and eliminated preprocedural symptoms of access dysfunction—constituting a technical and procedural success rate of 100%. All but two patients (98%) resumed dialysis after the procedure using their AVG.
At 30 days, freedom from adverse events was 96.4%. Four patients (3.6%) required additional reintervention and one patient (0.9%) underwent required/prolonged hospitalisation. The primary safety endpoint was therefore adjudged to be superior to the performance goal of 88% derived from prior studies and existing literature.
A total of 102 patients (92.7%) were available for the six-month primary efficacy analysis. TLPP at six months was 70.3% among these patients, the authors detail, and this was deemed superior to the prespecified performance goal of 40%. The only observed difference in patient subgroup analyses related to thrombosed AVGs, as those who presented with thrombosis within 30 days of the index procedure and/or at the time of the procedure demonstrated inferior TLPP rates at six months to those in non-thrombosis groups. Dolmatch and colleagues note that reasons behind this are unknown, but the fact this was observed in their study supports the “long-suspected belief” that a thrombosed AVG is more likely to fail due to TLPP loss, even when treated with a covered stent.
Noting secondary endpoint data, which they say should be considered observational and were calculated at predetermined intervals through the end of the study, the authors state that the Kaplan-Meier survival estimates for TLPP were 54.2% at 365 days and 36.9% at 730 days after the procedure, while Kaplan-Meier survival estimates for ACPP were 40.4%, 16.7%, and 7.8%, at 180, 365 and 730 days, respectively. A total of 91 adverse events across 53 patients (48.2%) were reported through 24 months, and 18 patients experienced device- or procedure-related events, meaning 86.3% were free from such events at 24 months.
Concluding messages
The Covera stent did an “adequate job” of maintaining target lesion patency over time, they add, but the “marked” and “ongoing” loss of ACPP (7.8% at 24 months) indicates that—regardless of TLPP improvement with a covered stent—some AVGs may be prone to recurrent stenosis or the development of new stenoses elsewhere in the circuit. The authors state that the 24-month cumulative circuit patency rate of 73.6% further supports this notion, and the finding that TLPP was “acceptable” with covered stent placement. The mean number of reinterventions to maintain patency was 1.6 at the treatment site and 3.6 in the access circuit at 24 months.
Dolmatch and colleagues conclude their JVIR report by noting that AVeVA was designed as “a first-in-human look at the Covera covered stent” in treating AVG venous anastomotic stenosis—and it demonstrated rates of freedom from major adverse events at 30 days (96.4%) and TLPP at six months (70.3%) that were both superior to literature-devised performance goals.
They also note, however, that AVeVA is not directly comparable with other, similar trials like FLAIR Pivotal, RENOVA and REVISE, and outline limitations of the current study, such as the inclusion of thrombosed AVGs and nontarget stenoses (rather than a more homogenous AVG group), and the potential for an “inherent bias” being created by its single-arm design and the selection of historical studies. “A comparative, powered, randomised study would be needed to determine patency differences between different covered stents within the same demographic population,” the authors add.
Biotronik announced the presentation of two studies on the performance of its drug-coated balloon (DCB) catheter Passeo-18 Lux at the Leipzig Interventional Course (LINC) 2022 (6–9 June, Leipzig, Germany).
The BIO REACT study was designed to better understand when and where a stent is needed following DCB for the treatment of femoropopliteal artery lesions in patients with peripheral arterial disease (PAD). Principal investigator Michael Lichtenberg (Arnsberg Vascular Center at Karolinen Hospital, Arnsberg, Germany) revealed the 12-month outcomes of this pilot study at LINC 2022.
While the use of intraoperative duplex ultrasound in this small cohort did not improve the identification of flow-limiting dissections, according to a company press release, the presented data showed that Biotronik Response Adapted Combination Therapy—combining Passeo-18 Lux DCB with Pulsar-18 T3 thin-strut stents when and where needed—is a safe and effective treatment of femoropopliteal lesions, while leaving less metal behind.
In the press release, Biotronik reports the following outcomes from BIO REACT:
Twelve-month freedom from clinically driven target lesion revascularisation (fCD-TLR): 94.8%
Twelve-month primary patency: 81.5%
Twelve-month survival: 97.2%
No major target limb amputation
“Identifying when to place a stent remains a complex issue, but the 12-month outcomes of the BIO REACT pilot study demonstrate that the Passeo-18 Lux DCB is an effective standalone therapy with a fCD-TLR rate of 94.0%,” Lichtenberg commented.
In another LINC presentation, Marianne Brodmann (Medical University Graz, Graz, Austria) reported the results of the Passeo-18 Lux DCB long lesion cohort, which combines the BIOLUX P-III all-comers registry’s long lesion subgroup and the BIOLUX P-III Spain study evaluating device performance in TASC C and D lesions >15cm.
In this pooled analysis, 159 patients with long and complex femoropopliteal lesions were treated with Passeo-18 Lux DCB. At 12 months, Biotronik reveals, the Passeo-18 Lux DCB showed good results in this real-world, challenging patient population (40.3% diabetes mellitus, 32.7% chronic limb-threatening ischaemia), with 84.4% fCD-TLR, 83.9% freedom from major adverse events, 98.6% freedom from major target limb amputation and 93.3% amputation-free survival.
The press release adds that, consistent with the results presented from the BIO REACT study, the Passeo-18 Lux DCB was shown to be an effective standalone treatment for complex lesions, with 60% of lesions not needing bailout stenting despite the long lesion length (mean lesion length, 24.9cm). “The treatment of long, complex TASC C and D femoropopliteal lesions with Passeo-18 Lux DCB as a standalone therapy is clearly shown to be safe and effective,” remarked Brodmann.
Biotronik advises that randomised controlled trials and all-comers registries have investigated safety and efficacy of Passeo-18 Lux DCB in the treatment of over 1,900 patients with PAD in the infrainguinal arteries.
Access Vascular, Inc. (AVI) has shared initial findings from a retrospective review of patient records according to a press release. These demonstrate an increase in dwell times compared to other commercially available devices and no complications when using AVI’s consistently hydrophilic materials for midline catheters.
As a result of a three-month retrospective evaluation of 29 HydroMID midline catheters at a long-term, acute care US hospital conducted in early 2022, AVI’s biomaterial-based catheters were found to have an average dwell time of 15.8 days. Furthermore, there were no incidences of phlebitis, occlusion, deep vein thrombosis (DVT), or bloodstream infections.
Traditional, polyurethane-based midline catheters have a median dwell time of only six days and an incidence of phlebitis of up to 35%, exhibit up to 7% rate of DVT, a 0.88% incidence of catheter-related bloodstream infection and an average occlusion rate of 22%.
“Midlines are an essential vascular access tool, but clinicians have been hampered for years by polyurethane-based catheters that must continually be replaced or that lead to unnecessary and frequent complications,” said Access Vascular, Inc. chief executive officer James Biggins. “These new data show that choosing the right catheter can make all the difference, giving clinicians the trust and competence they desire from their vascular access devices. We are confident that new, ongoing studies will demonstrate even longer dwell times for AVI’s biomaterial-based catheters.”
AVI’s patented hydrophilic biomaterial catheters mimic the body’s chemistry to significantly reduce the most common and costly complications associated with vascular access procedures. Given the high utilisation and complication rates of standard catheters, the use of AVI devices may meaningfully improve patient outcomes.
Philips has announced that its SmartSpeed artificial intelligence (AI)-powered magnetic resonance (MR) acceleration software has received US Food and Drug Administration (FDA) 510(k) clearance. It is one innovation within the portfolio of smart Philips MR systems showcased at the 2022 European Congress of Radiology (ECR; 13‒17 July, Vienna, Austria).
Adding advanced AI data collection algorithms to Philips’ existing Compressed Sense MR acceleration engine, Philips SmartSpeed delivers higher image resolution with scan times that are three times faster, and with virtually no loss in image quality, representing a major step forward in diagnostic confidence and MR department productivity.
With personalised treatment for complex diseases such as cancer increasing the need for high-confidence precision diagnoses, coupled with soaring caseloads due to aging populations and high levels of clinician burnout, radiology departments are under increasing pressure to improve performance, productivity, and profitability.
“Philips’ AI-based SmartSpeed reconstruction is the new benchmark among acceleration techniques for us. It improves on the company’s existing Compressed Sense in all aspects and allows a reduction in scan times with excellent image quality and diagnostic confidence,” said Grischa Bratke, radiologist and expert in musculoskeletal imaging at the University Hospital of Cologne, Cologne, Germany.
Philips SmartSpeed, the latest addition to Philips’ expanding portfolio of AI-driven, smart, connected imaging and smart workflow solutions, helps achieve the quadruple aim of improving diagnostic outcomes, enhancing patient and staff experiences, and reducing healthcare costs overall.
This latest AI-powered MR software increases resolution up to 65% and achieves up to three times faster scanning times compared to conventional MR scans. Coupled with its support for 97% of current clinical protocols – including advanced contrasts and diffusion-weighted imaging, and even quantitative imaging, Philips SmartSpeed helps increase diagnostic confidence in a wide range of cases, including those that are more complex.
The unique deep learning technology of Philips SmartSpeed is applied at the source of the MR signal and integrated with Philips’ Compressed Sense speed engine to deliver higher resolution and high signal-to-noise ratio needed for detailed images, small lesion detection and enhanced diagnosis.
Robert Jones (Birmingham, UK), Interventional radiologist and president of the Vascular Access Society of Britain and Ireland (VASBI), tells Renal Interventions at the Endovascular Access meeting (EVA; 24–25 June, Patras, Greece) that there are still significant untapped areas for research and education in the endoAVF field.
“Patient selection is a great example,” he says, noting that most of the focus to date in this area has been on vessel mapping and size criteria and the presence of the perforator. More understanding of whether pre-dialysis patients or those already on dialysis will benefit the most from endoAVF is another good example. And recognising recent studies in surgical fistulas that have demonstrated major differences in fistula use and success between ethnic groups, he points out: “We do not have this data for endoAVF.”
Inconsistencies in endpoint definitions are abundant in the literature, he warns. “I think there does need to be some consistency with definitions moving forward so we can make some meaningful comparisons between all these different studies.”
Jones also calls for more focus on cannulation. “[…] that is what is important to the patient. At the end of the day, they are the end user, and whilst we talk about the scientific side of things, there needs to be more focus, understanding and education around cannulation”.
Ra Medical Systems has announced receipt of US Food and Drug Administration (FDA) 510(k) clearance for the company’s Dabra 2.0 catheter as part of the Dabra excimer laser system. A company press release details that the catheter features enhancements including a braided overjacket design that is intended to improve deliverability and kink resistance when navigating tortuous anatomy, as well as a six-month shelf life.
“While we are pleased to receive this regulatory clearance, it comes as our board continues its evaluation of strategic alternatives to optimise our company’s path forward in the current challenging economic environment,” said Will McGuire, Ra Medical Systems CEO. “As we have previously announced, the Dabra 2.0 catheter represents an interim step in our work to develop a guidewire-compatible version of the Dabra catheter, and at this time we have no plans to commercialise the Dabra 2.0.”
On 16 May 2022 Ra Medical Systems disclosed that its board of directors is reviewing strategic alternatives with the goal of maximising shareholder value. In conjunction with this review, on 6 June 2022 the company filed a report on Form 8-K with the Securities and Exchange Commission (SEC) announcing initiation of a reduction in force under which approximately 65% of the company’s full-time employees were terminated. Non-terminated employees were offered conditional retention arrangements for a period of approximately 60 days from the date of the filing to allow for evaluation and monitoring of the company’s near-term personnel needs based in part on the company’s financial status and the board’s review of strategic alternatives. The purpose of the reduction in force is to preserve capital with the goal of maximising the opportunities available to the company during the board’s review of strategic alternatives, Ra Medical Systems advises.
Konica Minolta Healthcare Americas has announced that the company’s Dynamic Digital Radiography (DDR) technology, enabling the visualisation of anatomy in motion, will be available on the mKDR Xpress mobile X-ray system. The mobile system will also be compatible with the newest technology in wireless flat panel X-ray detectors, the AeroDR glassless high-definition detector. These new advancements in X-ray technology will be introduced at the Association for Medical Imaging Management (AHRA) 2022 Annual Meeting (10–13 July, Phoenix, USA).
DDR is the next evolution in X-ray, enhancing diagnosis and management of pulmonary diseases and orthopaedic conditions. DDR enables clinicians to visualise the dynamic interaction of anatomical structures, such as tissue and bone, with physiological changes over time. DDR is a series of individual digital images acquired at high speed and low dose. In the same study, clinicians can acquire static and dynamic images. The resulting cine loop delivers up to 40 seconds of anatomy in motion in a diagnostic-quality view with a simple acquisition performed on a conventional system.
“Pairing DDR with the high-performance mKDR Xpress enables clinicians to elevate patient care with mobile X-ray at the point of care in a hospital,” Guillermo Sander, the company’s marketing director for digital radiography explained.
The mKDR Xpress delivers exceptional imaging performance in a small footprint at the bedside or in the emergency department, operating theatre, or intensive care unit. On-board charging for two detectors and front and back storage for detectors and accessories help technologists meet the most demanding mobile X-ray imaging needs. A tube-mounted graphical user interface and image preview function help ensure clear images are visible quickly, improving efficiency.
“Konica Minolta is imagining more possibilities with diagnostic radiography and mobile X-ray to help clinicians meet their most demanding imaging needs, providing solutions that redefine what radiography can do,” Sander added. “We envision a world where advanced X-ray capabilities provide the immediacy of information that clinicians need, at a lower cost than other imaging systems, so they can make better decisions, sooner.”
Tiago Bilhim (Saint Louis Hospital, Lisbon, Portugal) presented during the Scientific Paper session at this year’s European Conference on Embolotherapy (22–25 June, Nice, France), and won the award of best abstract for his and co-authors’ ‘Long-term outcome of prostatic artery embolization for patients with benign prostatic hyperplasia’.
Bilhim et al conducted this single-centre retrospective study in 1,072 patients with follow-up over a 10-year period to assess the outcomes of prostatic artery embolization (PAE) for, as stated in paper’s title, benign prostatic hyperplasia (BPH), in patients with lower urinary tract symptoms (LUTS). The authors were able to deem PAE a “safe and effective treatment option for patients with BPH” following the study’s completion, but that various further studies can deepen understanding of the BPH and PAE landscapes.
The authors begin the paper by outlining some of the pre-existing research in the area of PAE for BPH— data have shown that compared to prostatic surgery, PAE can achieve “similar LUTS improvements with a lower adverse event profile.” However, surgery leads to improvement in all BPH objective measurements and data suggest that re-treatment rates for patients who underwent prostatic surgery may also be lower.
In his presentation, Bilhim reported that the study ran from March 2009–19, and the 1,072 patients who were studied excluded those who did not have follow-up (11% of the original study population), the 1% in whom PAE was a technical failure and the 3% who were diagnosed with prostate cancer during follow-up.
Bilhim went on to detail how each patient was evaluated for International Prostate Symptom Score (IPSS) and quality of life (QoL), prostate volume (PV)—measured with transrectal ultrasound—prostate-specific antigen (PSA), peak urinary flow rate (Qmax) and postvoid residual (PVR) volume. Follow-up appointments took place yearly and also evaluated use of prostatic medication, reintervention rates and repeat PAE and prostatectomy rates.
In terms of embolic agent, Bilhim proceeded to explain that over the ten years, various embolic agents were used. These were non-spherical polyvinyl alcohol (PVA) particles, measuring 100–300 micrometres and spherical PVA microspheres, measuring 300–500 micrometres. Some patients received treatment with trisacryl gelatin microspheres measuring 100–500 micrometres, or 250-400 micrometres polyzene-coated hydrogel microspheres. Notably, the first group treated within the study remit received PVA particles, so their follow-up was longer. Mean follow-up time was 4.39±2.37 years.
Adverse events were determined according to Cardiovascular and Interventional Radiology Society of Europe (CIRSE) criteria, and Bilhim stated that they did not consider frequency, urethral burning sensation or slight pelvic pain lasting for one to three days post-PAE as being in category, but rather as post-PAE syndrome. Reintervention, IPSS over 15, or QoL >3 were all considered ‘clinical failure,’ with need for prostatic medication registered but not counted as failure.
Bilhim then proceeded to relay his results to delegates in the audience: at the final follow-up appointment, mean IPSS and QoL improvements were -10.14±8.34 (p<.0001) and -1.87±1.48 (p<.0001) points, mean PV reduction was -6.82±41.11 cm3 (p=0.7779), mean PSA reduction was -1.12±4.60ng/mL (p=0.9713), mean Qmax increase was 2.72±6.38 mL/s (p=0.0005), mean PVR reduction was -8.35±135.75mL (p=0.6786) and mean IIEF-5 improvement was 0.18±7.40 points (p=0.4546).
The number of patients who required prostatic medication after PAE was 335, or 31.3%. The reintervention and repeat PAE rates were 3.4% and 2.3% at one year, 21.1% and 9.5% at five years and 58.1% and 23.1% at 10 years, respectively. Prostatectomy rates were 1.1% at one year, 11.6% at five years and 35.0% at 10 years, Bilhim reported.
The presenter also noted that the study saw a 90% acute urinary retention resolution rate, with the other 10% having to have surgery, and the rate of post-PAE syndrome was 23%.
In terms of difference in outcomes among the different embolic agent groups, the paper acknowledges that PVA led to lower rates of penile skin lesions, haematuria and rectal bleeding after PAE compared to the other spherical embolic agents. A possible explanation for this could be that PVA offers a lower permanent vessel occlusion.
Other trends observed during the study were that unilateral PAE was a significant predictor of clinical failure and reintervention and that those who received a repeat PAE (n=25, 25.8%) were more likely to undergo prostatectomy compared to those who only received one PAE procedure.
Bilhim et al were able to draw the conclusion that PAE gives patients lasting and long-term LUTS relief and that reintervention rates are 20% in the first five years, rising to between 30 and 60% >five years post-PAE. Addressing the ET audience, Bilhim declared PAE a “safe and effective treatment option for patients with BPH.” The study yielded “promising” findings, the presenter added, among which was that 74% of patients remained prostatectomy-free, demonstrating the potential for repeat PAE to ensure treatment effectiveness durability.
Bilhim showed his awareness of his study’s “many limitations”—namely that it was carried out retrospectively with no controls and that they “lost patients during follow-up.” Comparing the embolic agents also made the study more difficult because of different follow-up times for each group, but they did control for this factor with multivariable Cox regression analyses, Bilhim clarified.
He admitted that “we need more long-term data to keep on proving that PAE is a good alternative treatment to prostatectomy/transurethral resection of the prostate (TURP).” Studies with large cohorts are also necessary, Bilhim added, to “fill this gap in the knowledge” around BPH treatment and PAE. Future trials should compare PAE with other minimally invasive surgical treatments (MISTs), as well as look more closely at the differences in outcome when using various embolic agents, Bilhim suggested. Long-term reintervention rates also mean that the benefits of PAE in terms of faster recovery, it being less invasive with fewer adverse events and better at preserving ejaculation, “must be viewed with caution,” Bilhim advised.
Session moderator and meeting deputy chairperson Otto van Delden (University Medical Centers Amsterdam, Amsterdam, The Netherlands) asked Bilhim after he had finished presenting whether “[you can] use [whatever agent] you want.” Bilhim responded in the affirmative, before explaining the following: “What I have seen is that when you do PAE repeatedly, even though I could not prove this, [there seems to be] more recanalisation of the native prostatic artery with PVA than with spherical particles.” Nevertheless, Bilhim asserted, he has seen “no big clinical difference” among the different embolic agents—“all patients will have revascularisation from different origins.”
Regarding the frequently asked question of how PAE compares to other procedures, Bilhim sought to clarify that “you cannot compare recovery and morbidity between PAE and [surgical resection].” It is more appropriate and beneficial to draw comparisons between PAE and other MISTs, such as those which are commonly carried out in the USA.
Rounding up the post-presentation discussion, Bilhim concluded that these study data are “good” for him—” I can tell [patients] about 10-year likely outcomes.”
This study presents the largest PAE cohort with the longest follow-up data so far, with over 900 patients with follow-up data from 1–3 years, over 300 patients with available data at five years and 150 patients up to 10 years. This will be a relevant addition to the existent PAE literature as it presents the first study looking at reintervention rates up to 10 years post-PAE.
Among the most popular pieces from last month are reports on papers delivered at the Society of Interventional Radiology (SIR) 2022 Annual Meeting (11–16 June, Boston, USA), two stories of innovations in pain management, and a write-up of a call to action regarding limiting radiology staff lead exposure.
‘Surface lead contamination on personal lead radiologic protective apparel’ is a recent report published by Kieran Murphy et al (Toronto Western Hospital, Toronto, Canada). The subject of the report is free lead dust on lead aprons: the study involved testing aprons at a Toronto university hospital, which yielded the finding that 60% of aprons and thyroid shields have free surface lead.
‘Multivessel pelvic embolization during caesarean hysterectomy for placenta accreta spectrum: A single-centre experience and comparison to internal iliac artery balloon occlusion’ was presented at SIR.
The data are the result of evaluations of the company’s immunotherapy platform, which integrates an investigational class C toll-like receptor 9 (TLR9) agonist, SD-101, and the proprietary Pressure-Enabled Drug Delivery (PEDD) method of administration to overcome critical treatment barriers.
“I do not want interventional radiology to be a treatment for the rich, nor for those who live in the wealthiest countries.” Yasuaki Arai was, until recently, executive advisor to the president at Japan’s National Cancer Center in Tokyo, where he is currently a member of the interventional radiology centre.
Four of the abstracts submitted were declared ‘Abstract of the Year’ by Society of Interventional Radiology (SIR) scientific chairs. The prizes were conferred during the final plenary session of the meeting, and, according to SIR, reward the ‘best scientific work’ in terms of ‘overall quality, timeliness and content’.
An experimental formulation of a hydrogel injected into spinal discs proved safe and effective in substantially relieving chronic low back pain caused by degenerative disc disease (DDD), according to new research.
M.I.Tech is the creator of the HANAROSTENT technology, a family of conformable, non-vascular, self-expanding metal stents, which have been distributed by Boston Scientific in Japan since 2015.
Shimadzu Medical Systems USA introduced the new Trinias system, which uses artificial intelligence deep learning to improve the visibility of medical devices while using lower X-ray doses than previous models, at SIR 2022.
Damaged nerves can be regenerated with the application of a frozen needle using an advanced imaging technique called interventional cryoneurolysis, which is performed by an interventional radiologist and can offer hope to patients in persistent pain following a traumatic injury, according to an SIR press release.
The first patient has been enrolled in the US Food and Drug Administration (FDA) investigational device exemption (IDE) below-the-knee (BTK) SELUTION4BTK clinical trial involving SELUTION SLR, MedAlliance’s sirolimus-eluting balloon.
Merit Medical has announced the successful enrolment of the first patient in its WRAP registry study in a press release. This study will evaluate the clinical benefits associated with the use of the Wrapsody cell-impermeable endoprosthesis in patients receiving haemodialysis that experience stenosis or occlusion of blood vessels required for dialysis.
Globally, over two million patients with advanced kidney disease receive dialysis. Haemodialysis, the primary approach used for dialysis, requires long-term vascular access that is typically achieved through the surgical creation of an arteriovenous fistula (AVF) or placement of an arteriovenous graft (AVG). However, complications, such as stenosis and/or occlusion within the dialysis outflow circuit of an AVF or AVG, can impair vascular access which compromises the ability to provide adequate dialysis treatment. The Wrapsody cell-impermeable endoprosthesis was created to help overcome this challenge by maintaining the integrity of the dialysis outflow circuit.
Dean Huang, consultant diagnostic and interventional radiologist at King’s College Hospital in London, England, enrolled the first patient in the WRAP Registry. “The patients being treated with the Wrapsody cell-impermeable endoprosthesis have historically had few clinical options,” Huang said. “These patients have typically faced frequent reinterventions to maintain vessel patency resulting in multiple procedures and hospitalisations. The WRAP study will add to the growing body of evidence on Wrapsody’s ability to achieve durable outcomes for this vulnerable patient population.”
The WRAP registry study will enrol up to 500 patients with outflow circuit stenosis or occlusion who are receiving haemodialysis at medical facilities throughout Europe, South America, Australia, and New Zealand. Clinical outcomes of patients after the initial placement of the Wrapsody cell-impermeable endoprosthesis will be evaluated over a two-year period in accordance with the instructions for use associated with its CE Mark.
The Wrapsody cell-impermeable endoprosthesis is an expandable nitinol stent frame fully enveloped by an external layer of expanded polytetrafluoroethylene (PTFE) and an internal layer of spun PTFE with an interposed cell-impermeable layer. The Wrapsody cell-impermeable endoprosthesis system is being studied under an investigational device exemption (IDE) in the USA.
Teleflex has announced the results of several research studies that further support the safety and efficacy of the UroLift system for men living with enlarged prostate, benign prostatic hyperplasia (BPH), or those who have a wide range of prostate sizes and/or a median lobe obstruction. The data were presented at the 37th Annual European Association of Urology (EAU) Congress in Amsterdam (1—4 July) and virtually.
Key findings include:
Pooled outcomes of over 300 controlled subjects from five clinical studies revealed most men shifted to lower international prostate symptom score (IPSS) symptom severity after treatment with prostatic urethral lift (PUL). The majority of subjects (79%) improved by three points or more, and 66% of those patients moved into a lower IPSS severity grade 12 months post-treatment.
Comparative evaluation of real-world and controlled trial outcomes of PUL demonstrated that symptom improvement is not correlated with prostate size and shape. The study examined PUL outcomes in differing gland sizes and morphologies, comparing controlled trial results from BPH6 for patients with small prostate sizes and MedLift for patients with obstructive median lobes. At 24 months, all groups demonstrated significant and sustained IPSS improvement.
An analysis of US healthcare claims revealed higher de novo prescription rates after transurethral resection of the prostate (TURP) and photoselective vaporisation of the prostate (PVP) compared to PUL. The study revealed that post-surgical medication usage was significantly higher for BPH patients who were treated with more invasive surgical procedures as compared to those treated with the UroLift system.
“The UroLift system is the most well studied minimally invasive surgical therapy for BPH. In a combined analysis from five controlled studies, we found that the majority of men who had received the procedure demonstrated measurable improvement in their BPH symptoms, flow rate, and quality of life. Subjects [also] preserved their sexual function,” said Claus G Roehrborn, urologist at the University of Texas Southwestern Medical Center (Dallas, USA) and a lead author on the paper.
“The evidence presented at EAU means that urologists can further help their BPH patients make an objective, data-driven, and informed decision based on real-world evidence, particularly when faced with prostate sizes and shapes that fall outside of the range of randomised clinical trials. Our research showed not only rapid, but also durable improvement,” said Christian Gratzke, medical director, urology clinic, University Hospital, Freiburg (Freiburg, Germany).
Cydar Medical, in partnership with King’s College London, has initiated the ARIA study—a randomised controlled trial to assess the clinical, technical and cost-effectiveness of a cloud-based, artificially intelligent image fusion system in comparison to standard treatment to guide endovascular aortic aneurysm repair.
Endovascular aneurysm repair (EVAR) is an alternative to open aortic surgery due to perceived advantages in patient survival, reduced post-operative complications and shorter hospital lengths of stay.1 Despite these potential advantages, there is still significant variability in preoperative planning and sizing, problems associated with imprecise visualisation and device positioning intraoperatively, and inconsistent patient outcomes, a Cydar Medical press release states.
Rachel Clough, principal investigator of the ARIA study and clinical senior lecturer at King’s College London, said: “Our central hypothesis is that digital technology—specifically cloud-computing and artificial intelligence—can be used to assess and learn from large volumes of data to inform clinical decision making and has the potential to improve the predictability of individual patient outcomes and the consistency of outcomes in the NHS.”
The randomised trial will enrol 340 patients in 10 sites across the UK with a clinical diagnosis of abdominal aortic or thoracoabdominal aortic aneurysm suitable for endovascular treatment. The trial will follow patients for one year and assess the effect of Cydar EV Maps on clinical-, technical- and cost-effectiveness in comparison to standard treatment in endovascular aortic aneurysm repair, used for both standard and complex devices.
The study was initiated with the first patient enrolled at the Liverpool University Hospitals NHS Foundation Trust. “Cydar EV Maps is a game-changing technology for vascular navigation. The ARIA study provides a unique opportunity to demonstrate the benefits like reduced procedure time and reduction to radiation exposure, although some of the more subtle benefits related to procedural quality and reduced operator fatigue may never be directly measured but are obvious as an operator,” added Dr Simon Neequaye, Principal Investigator at the Liverpool University Hospital NHS Foundation Trust.
Cydar EV Maps is currently available in the EU, UK and US. It is certified software-as-a-medical device with an EU CE mark and US Food and Drug Administration 510(k) clearance.
References:
Greenhalgh RM, Brown LC, Kwong GP, Powell JT, Thompson SG. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: randomised controlled trial. Lancet. 2004;364(9437):843-8.
Insightec, a global healthcare company dedicated to using acoustic energy to transform patient care, announced that it has received US Food and Drug Administration (FDA) approval for an investigational device exemption (IDE) for a clinical comparative study of the Exablate Prostate system used to treat diseased prostate tissue. This study will evaluate the safety and efficacy of focal treatment using high-intensity focused ultrasound when compared to active surveillance in men living with prostate cancer.
The Insightec Exablate Prostate system uses soundwaves to ablate targeted tissue in the prostate. The treatment is performed under magnetic resonance imaging (MRI) guidance for high-resolution visualisation of the patient’s anatomy for precise targeting and real-time temperature monitoring. The single-session treatment does not require incisions and allows patients to return to normal activities quickly, with minimal complications.
“We are excited to continue this important research that can impact on the standard of care for prostate cancer treatment,” said Behfar Ehdaie, a urologic surgeon at Memorial Sloan Kettering Cancer Center (New York, USA), and principal investigator for the study. “Exablate Focused Ultrasound has been shown to provide an accurate, safe, and effective option to engage the prostate gland directly in selected patients based on two-year biopsy outcomes.”
A previous Insightec-sponsored clinical trial led by Memorial Sloan Kettering Cancer Center for the Exablate Prostate system reported minimal damage to adjacent structures and low rates of impact on potency and continence, supporting function and quality of life for patients. The new comparative study builds on the evidence of this clinical trial and aims to further enhance prostate treatment options and improve clinical outcomes.
The Insightec Exablate Prostate system received 510(k) FDA clearance in November 2021, making way for the system to be offered to patients in a commercial facility and for further clinical studies. In January 2022, the system was used to treat prostate disease in its first US commercial patient.
Results from the new study will define the role of focal therapy to delay and avoid radical therapy for men with prostate cancer and support expanded clinical adoption of the technology and increased access for patients through insurance reimbursement.
Transit Scientific's XO Score inflated with a standard off-the-shelf PTA balloon
Transit Scientific’s XO Score inflated with a standard off-the-shelf PTA balloon
Transit Scientific had shared via press release successful outcomes on multiple fistula and graft cases using its XO Score sheath platform, a first-of-its-kind metal-alloy scoring, cutting, and constraining structure (CS) device, along with off-the-shelf percutaneous transluminal angioplasty (PTA) balloons.
XO Score can be used in significant chronic dialysis fistula and graft cases using low-pressure inflation, in some cases after high-pressure PTA treatment failed.
“A patient presented with a high-grade stenotic lesion in a brachiocephalic fistula restricting venous outflow. The lesion was resistant to initial treatment using a high-pressure PTA inflated to 40 atmospheres. The lesion was then treated with the XO Score device and followed by effacement of the stenosis with standard balloon PTA inflated to nominal pressure (nine atmospheres). There was no residual stenosis and the fistula was no longer pulsatile on exam,” Jeffrey Hoggard, an interventional nephrologist at Raleigh Access Center (Raleigh, USA), shared. “XO Score presented a great treatment option for us where high-pressure PTA failed.”
Traditional PTA cutting, scoring, and constraining structure (CS) technologies are manufactured with metal or polymer wires, struts, blades, or grooves wrapped around, or fused to, the outside of the angioplasty balloon. These wires, struts, blades and/or grooves expand with the balloon to provide focal force in calcified, hyperplastic, and/or resistant lesions to prevent dissection, dilate resistant lesions, and/or prep the vessel for other intervention. Traditional systems can be bulky, difficult to use, cost-prohibitive, and require significant inventory.
The XO Score is a thin one-piece metal alloy exoskeleton sheath, with up to 22 struts/grooves, that slides over off-the-shelf angioplasty balloons. When the angioplasty balloon is inflated, the struts/grooves expand with the balloon and rotate 90° to apply focal force to the vessel. When the balloon is deflated, the XO struts/grooves rotate 90° back to an atraumatic position and the XO structure assists in balloon rewrap for removal.
XO’s technology can also be optimised to constrain balloons and prevent torsional and longitudinal shear during angioplasty balloon inflation.
The XO Score system is US Food and Drug Administration (FDA) and CE-Mark cleared to dilate stenotic material in iliac, femoral, iliofemoral, popliteal, infrapopliteal, and renal arteries and for the treatment of obstructive lesions of native or synthetic arteriovenous dialysis fistula.
Kytai Ngugen
Credit: University of Texas at Arlington
Kytai Nguyen Credit: University of Texas at Arlington
A University of Texas at Arlington (UTA; Arlington, USA) bioengineer is leading a project that will develop biodegradable nanomaterials that will take pictures and deliver medicine to combat peripheral arterial disease (PAD), the university announced in a press release.
Kytai Nguyen, a UTA bioengineering professor, is the principal investigator in the four-year, US$2.1 million National Institutes of Health (NIH) grant-funded project. She is collaborating with Jian Yang, a Penn State University (University Park Pennsylvania, USA) bioengineering professor and former UTA faculty member, and Ralph Mason, a professor of radiology at UT Southwestern (Dallas, USA).
“What is important in this project is that the technology carries fluorescent and ultrasound imaging capabilities, which will provide patients and doctors with more detailed information,” Nguyen said. “It also gives patients more targeted medicine, making it more efficient.”
PAD, more commonly known as either atherosclerosis, is a condition commonly found in the elderly. It affects more than 200 million people worldwide and is associated with high rates of morbidity and mortality.
The research aims to develop novel biodegradable nanoparticles to deliver therapeutic agents that specifically protect cells under stress conditions, facilitate the formation of blood vessels under hypoxia and allow noninvasive multimodal imaging methods.
One impact of the research is to use these new nanoparticle platforms to deliver any therapeutics locally, treat the disease effectively and monitor the treatment noninvasively by imaging. “The overall goal is to reduce complications and improve the quality of life for PAD patients,” Nguyen said.
Michael Cho, chair of the UT Arlington Bioengineering Department, said Nguyen’s innovative research could greatly help those who live with PAD.
“This cutting-edge technology has a chance to change our protocols on how to deal with atherosclerosis,” Cho said. “When you are able to target localised lesions for treatment, that is so much better for the patients and much less invasive than current treatment.”
Nguyen, who has been at UTA since 2005, received Cancer Prevention & Research Institute of Texas grants in 2010, 2016, and 2021. She also has received funding through the NIH, National Science Foundation, American Heart Association, and US departments of Education and Defense, among others.
Investigators provide clinicians with guidance on alternative imaging methods for interventional radiology procedures and strategies to maintain the short supply for emergencies, a press release announced. The guidance has been published in the Journal of Vascular and Interventional Radiology(JVIR).
“As interventionalists, adaptation is at the core of our specialty, and this situation has proved no different,” said lead author Nikki A. Keefe, Department of Radiology, University of North Carolina at Chapel Hill (Chapel Hill, USA) and her co-authors. “We have developed an initial approach to case prioritisation, and we also looked at short-term strategies for the management of existing supply to optimise utility and minimise waste.”
In response to this shortage, the American College of Radiology (ACR) Committee on Drugs and Contrast Policy has published a guidelines statement. Using these guidelines as a foundation, Keefe and her co-authors offer a set of practical solutions for dealing with the current situation.
The authors recommend creating a priority matrix covering the following categories: procedures that require iodinated contrast media versus procedures that can be deferred; those that can be performed with alternative imaging modalities such as intravascular ultrasound; and those that can be performed with an alternative contrast media.
With maximum dose recommendations, gadolinium (Gd) can be used in the vascular system even for patients with renal insufficiency. Carbon dioxide has been used as a safer alternative to iodinated contrast media in patients with renal dysfunction or allergy, although there are some associated risks. To prevent ischaemia, dosages should be timed one to two minutes apart. While alternate contrast agents have limitations in defining the anatomy of large diameter vessels such as the aorta, digital stacking of images may improve visualisation.
Intravascular ultrasound has an established role in vascular procedures, and it can obviate the use of contrast media and decrease radiation exposure and procedural times. With appropriate training, clinicians can apply intravascular ultrasound for procedures such as inferior vena cava filter placement and transvenous biopsy.
GE Healthcare recently announced that it has been able to reopen its Shanghai facility, but distribution and other supply chain issues may linger. “That being said,” Keefe and co-authors cautioned, “with China’s zero-COVID-19 policy, a shutdown may unfortunately happen again, and it would be prudent to have a plan in place should shortages recur.”
As interventional radiology (IR) evolves and expands, so too does the role of anaesthetic support to get these patients safely through their procedures. Where previously anaesthetic support was reserved for only the most acute and complex patients, now, some centres have regular anaesthetic lists supporting elective, urgent and emergency work.
Maintaining standards
Anaesthesiologists’ experience in the traditional ‘theatres’ means they can bring that knowledge across, setting standards for anaesthesia, such as recommended emergency airway equipment, a go-to box for anaesthetic emergencies like malignant hyperpyrexia, and stockage of appropriate medication. Having a regular anaesthetist also means these standards are regularly reviewed and revised.
It also brings across a culture of theatres, championing morning huddles or team briefs; completion of the WHO [World Health Organisation] checklist and debriefing sessions; efficient turnaround time between cases and better list utilisation overall.
The presence of anaesthetists within the IR suite permits the teaching of skills critical to safe patient management, airway management skills, for example, and the transfer of knowledge that will enhance patient satisfaction. Postoperative pain management is an example of such knowledge, the importance of which will be seen in years to come as the repertoire and complexity of IR procedures continues to grow.
Patient population
Studies have shown that the mean age of patients in IR is 3.5 years higher than those having surgery. With increasing age, you see increasing co-morbidities.
Certainly, in the surgical population there has been a significant increase in patient complexity as reflected in their American Society of Anaesthesiologists (ASA) Physical Status grade. Previously, ASA 1 patients made up 35% of the surgical population whereas now they make up just 15%. Naturally, the percentage of ASA 2, 3 and 4 patients has increased, and overall, patients have increased numbers of health conditions and poorer control of existing conditions.
Certain subsets of IR patients may demonstrate this heightened risk more clearly than others. A recent three-month audit of patients presenting on the anaesthetic list for lower limb angioplasty at a major teaching hospital in London, revealed that 23% of patients were octogenarians, 23% were ASA 4 and above, and 17% were not for resuscitation in the event of a cardiac arrest. Many of these patients present as urgent cases—best practice national guidance recommends that they should be revascularised within five days of their admission to hospital.3 Strict adherence to this practice leaves little time to optimise them prior to their procedure.
The nature of IR means that the patient considered too high-risk for a surgical procedure, or an open technique, is referred for a minimally invasive one instead. High-risk refers to the anticipated surgical insult associated with major surgery, which the team intend to mitigate through a minimally invasive technique, thus reducing physiological stress on the body. However, there remains an associated risk from anaesthesia, which is independent of the surgical or procedural approach. This anaesthetic risk may be significantly prolonged, in some cases, with procedures taking many hours to complete.
When anaesthetising patients in IR, it is important to strike the right balance between anaesthetic approach, procedural technique and patient risk factors. Often “a less is more” approach suits the high-risk patient better.
Type of work
The challenge comes when anaesthetists are unfamiliar with the nature of the procedure, particularly the approach and the duration. Additionally, the type of work in IR is often a mixture of elective, urgent and emergency work, meaning it is a hybrid of a traditional elective lists and emergency lists from theatres: a combination of stable patients having minor procedures, like sclerotherapy and unstable patients having life-saving procedures like embolization. A flexible and adaptable mindset is therefore needed when working in IR.
The challenge, and possibly the enjoyment, of anaesthetic lists in IR is that no two lists are alike. Patient demographics differ wildly from one to the next and procedures vary significantly from gastrointestinal procedures to vascular work.
Education and training
Anaesthetic training has not kept pace with the growth in demand for anaesthetic involvement in delivering care in the IR environment. Remote-site anaesthesia is given consideration within the anaesthetic curriculum, however, the concentration of IR services, mainly in larger teaching institutions, and the relative lack of specific focus on this subject in the training syllabus, means that most anaesthetic trainees have little to no exposure to IR until their final years of training, or until they become consultants.
The knowledge and experience gap that needs to be crossed, as a consultant, is therefore significant. The initial learning curve is steep and there is a lack of resources to support the education and training of anaesthetists who are interested in this field. It may take months to years for consultants to become comfortable with IR procedures and practices, and to acquire the mindset and techniques required to operate effectively within the IR environment. A wholesale change in thinking is needed to address this, from the teams who create the training curriculum, to the rota makers who assign trainees to theatre lists. Going forward, training lists in IR need to be seen as mandatory rather than just a tick-box option.
Location and space
One of the obstacles that face anaesthetists who work in IR is the unfamiliar environment. IR suites are often in a remote location in the hospital and away from the main theatre complex. The anaesthetic support that can be found in main theatres is not available in IR and the anaesthetist must work closely with their anaesthetic assistant to deliver care. In an emergency, help from a fellow anaesthetist is not close at hand. This much is also true for the IR anaesthetist who needs relief for a lunch break or to review a patient.
In addition, the configuration of IR suites has often not taken the needs of the anaesthetic team into consideration, with limited space for the anaesthetic machine, which can be far from the head end of the table. Access to an anaesthetic room is preferable but again with limited space, a luxury that the IR suite cannot always afford.
A combination of the above challenges breeds a reluctance in anaesthetists to deliver regular anaesthetic lists in IR.
Safety
The lack of regular anaesthetist-supported lists has led to many procedures being completed under local anaesthetic or “vocal anaesthetic”, when ideally, they should have anaesthetic involvement.
There is much debate over whether procedures, such as oesophageal dilatations, should be done under “vocal anaesthetic” with (or without) radiologist-delivered sedation, or under general anaesthetic. Centres all across the country use a different approach and each have their merits. The benefits of anaesthesia delivered by an anaesthetist is that the radiologist and their team can focus on the procedure, whilst the anaesthetist can focus on the patient, ensuring they are adequately analgised, anaesthetised and monitored.
This is ever more important when dealing with sick patients. Regular exposure to emergency work, and benefitting from formal training in intensive care medicine, anaesthetists are well versed in the management of medical emergencies that may be encountered both inside and outside of the operating theatre. Their leadership qualities come to the fore when dealing with the unstable or deteriorating patient.
Summary
Anaesthetists are uniquely placed to collaborate with IR teams on patient safety and maintaining the same standards of practice as theatres to ensure effective care is delivered.
Though there are many unique challenges to providing care in this setting, with increase in workload, it is certain that more and more centres will recognise the value of regular lists. Supported by the Society of Anaesthesia and Radiology, undoubtedly some of these challenges, like a lack of familiarity with the environment and procedures, will be rectified.
Overall, as a speciality, consideration needs to be given to adopting a surgical theatre approach to delivering care and at the centre of this is anaesthetic support.
Authors Nazia Khan and Pele Banugo are consultant anaesthetists at Guy’s and St Thomas’ NHS Foundation Trust, London and Sanya Patel is an anaesthetic trainee at Lewisham and Greenwich NHS Trust, London, UK.
Primary paediatric liver cancer is a rare disease, accounting for 1–2% of childhood cancers, or about 150 new diagnoses of paediatric liver malignancy per year in the USA. These include hepatoblastoma (HB), hepatocellular carcinoma (HCC), undifferentiated embryonal sarcoma of the liver (UESL), and rhabdoid tumour of the liver (RTL). Surgical resection is the foundation of cure for all paediatric liver tumours; however, only one-third of patients have resectable disease at diagnosis.
Allison Aguado
While chemotherapy is effective in making two-thirds of initially unresectable patients with HB resectable, effective standard-of-care chemotherapeutic regimens that render HCC, UESL, or RTL resectable have yet to be described.
Recent reports suggest that orthotopic liver transplant may be required in 20–30% of newly diagnosed paediatric liver tumours who will require lifelong medical therapy with potential episodes of rejection and occurrence of post-transplant lymphoproliferative disease.
The primary staging system used for paediatric liver tumour is PRETEXT (pre-treatment extent of tumour) classification which describes the extent of tumour in the liver based on Couinaud segmental anatomy and is used to predict overall survival. It is a pre-therapy assessment of HB and HCC but is intended to be applicable to all primary malignant liver tumours of childhood. PRETEXT annotation factors include venous involvement, extrahepatic disease, multifocality, tumour rupture, and metastatic disease. This is used to create the risk stratification system used for the Pediatric Hepatic International Tumor Trial (PHITT) which is based on PRETEXT, metastases, age, α-fetoprotein (AFP), annotation factors, and resectability.
TARE with Yttrium-90 (TARE-Y90) has demonstrated an emerging role in the treatment of primary paediatric liver tumours in several small studies. It was initially used in heavily pretreated children with HB, HCC, and transitional liver tumours (showing features of both HB and HCC) where it showed that it was feasible, safe, and demonstrated anticancer effects by imaging and decreased tumour markers. It has since been used as a component of curative therapy in two paediatric patients with HB who responded to TARE-Y90 with decreased tumour size, decreased tumour marker levels, hypertrophy of the future liver remnant, the facilitation of conventional hepatectomy, and complete remission. It has also been used as part of curative therapy in two paediatric patients with HCC, who were downstaged to hepatic resection; one is alive with no evidence of disease 18 months post-completion chemotherapy and one is alive with evidence of disease 13 months post-resection.
Earlier integration with combination therapies may offer an important option and strategy to improve survival, result in less chemotherapy delivered, decrease rates of orthotopic liver transplantation (OLT), and present potentially curative options for patient with refractory and recurrent disease. While early results are encouraging, more research is required to determine the efficacy of TARE-Y90 in children and to define the clinical scenarios where there is likely to be greatest benefit.
Allison Aguado is a paediatric interventional radiologist at Nemours Children’s Hospital, Wilmington, USA.
Interventional radiology (IR) is a growing, dynamic field, still working to define its professional identity— who we are and where we are going as a specialty. I believe an important part of that maturation rests on our ability to articulate our collective values as a professional group, particularly in regard to challenging questions that arise in our work. Through my ethics graduate education and medical training, I have come to view ‘ethics’ as just that— the collective values of a group of people. So, to help IR establish itself as a clinical specialty, we need to define and articulate the ethics of IR.
Unfortunately, many common approaches to ethics tend not to feel particularly practical or helpful in day-to-day clinical practice. Ethics often feels abstract and verbose and tends to treat clinicians as a monocultural group, assuming that the ethical issues and solutions for IR are the same as internal medicine or gynaecology. Although there are certainly common issues across healthcare, medical specialties have remarkably distinct cultures, workflows, and ways of thinking. As such, my hypothesis has been that the salient ethical issues and means of navigating
them probably vary in important ways across specialties. To make ethics feel more practical and useful, I decided to test out an applied, specialty-specific approach to ethics in IR. Instead of starting with ethical theory and a top-down approach, I work bottom-up, starting with an understanding of how people in IR are approaching an ethical issue and why, and then using that understanding alongside ethical theory to design practical approaches and tools to better navigate those issues. The ultimate goal is to foster an ethics consciousness in IR, a common understanding of our shared values and how best to navigate the sticky situations we face as a specialty.
To do this, I founded a multi-institutional working group of faculty and trainees focused on research, education, and public relations using this new approach. Creating something new always comes with challenges and setbacks, but we now have approximately 30 people affiliated with the group, and since being founded in 2019, we have published over 20 manuscripts, given multiple invited lectures at major IR conferences, and have a column in Seminars in Interventional Radiology called the ‘Ethics Corner.’ We have found that IRs face a wide array of ethical issues in their work; the vast majority consider these to be important issues but state that they often feel limited by a lack of tools and specific guidance for navigating them. Common issues include differentiating palliative from futile care, managing complications, consent and surrogate decision-making, conflicts of interest and research ethics, tribalism and medical business ethics, and social media ethics.
For example, consent is a ubiquitous part of our daily workflows and right at the core of our relationships with patients and families. Nevertheless, studies suggest that consent practices tend to be limited in quality and completeness across healthcare. This is important not only ethically, but because poor periprocedural communication and understanding is a common source of medical mistakes and lawsuits. We first completed an exploratory study of consent in IR, finding that the dynamic nature of IR practices and limited baseline public awareness can make truly informed consent particularly challenging in our specialty. To improve consent practices, we have not only been working to develop more engaging educational resources on ideal consent practices for IR, but also better patient decision aids (PDA).
PDAs are handouts, videos, or other tools that present balanced information on the risks, benefits, and alternatives of a healthcare decision, ideally at the average reading level (seventh grade in the USA), using patient-friendly, plain language. Unfortunately, current PDAs for image-guided procedures tend to be limited in quality and consistency, so we partnered with a not-for-profit called The Interventional Initiative to create better PDAs via an extensive vetting process. We then trialled them at two institutions where people were randomised to receive a PDA or not, while waiting to talk to their clinician. This way, clinicians did not have to do anything differently; rather, we took advantage of dead time in the patient flow, which is ideal for sustained adoption. We found that the people who received a PDA were not only more likely to have better understanding and satisfaction, but were also more likely to feel that their clinician had spent enough time with them and answered all their questions.
This is one example of our applied approach. Rather than writing a 50-page analysis about how interventional radiologists should ‘do better’ at consent, we instead assume that people are doing their best, try to understand current barriers, and construct environments and workflows that support better consent practices in IR without requiring more time or energy.
We are always looking for collaborators and partnerships to help establish our collective values as interventional radiologists.
Eric J Keller is a resident physician at Stanford University, Stanford, USA and founder of the Applied Ethics in IR working group.
Disclosure: Keller is a board member of The Interventional Initiative.
At the Society of Interventional Radiology (SIR) 2022 Annual Meeting (11-16 June, Boston, USA), four of the abstracts submitted were declared ‘Abstract of the Year’ by the society scientific chairs. The prizes were conferred during the final plenary session of the meeting, and, according to SIR, reward the ‘best scientific work’ in terms of ‘overall quality, timeliness and content’.
Erica Emmons
Erica Emmons (Vanderbilt University Medical Center, Nashville, USA) was one of the winners, for her paper ‘Survival outcomes and toxicities following yttrium-90 (Y90) radioembolization of colorectal cancer metastatic to the liver: 498-patient analysis from the RESiN registry.’ The purpose of the study was to report on the outcomes of 498 patients from a prospective, multicentre, observational registry of Y90 resin microspheres as treatment for colorectal liver metastases. The outcomes measured were treatment characteristics, survival, and safety.
The patients on whom Emmons et al’s study reports were treated from 2015-2020 and the cohort was 40% female (n=200) and 60% male (n=298). The median age was 60 years old.
Regarding tumour burden, it was <10% in 210 (47%), 11–25% in 115 (26%) and >26% in 125 (28%) patients. Treatment was bilobar in 257 (52%) and unilobar in 241 (48%) patients. At baseline, 180 patients (38%) had extrahepatic disease. Eastern Cooperative Oncology Group (ECOG) status was between zero and one in 441 patients (93%).
There was variation in whether Y90 was used as part of first-line therapy (17%), second line therapy (41%) and third line or beyond in 43% of patients. Fourteen per cent of patients had undergone hepatic resections before treatment with Y90, another 14% had received ablation, 6%, and 2% of patients had undergone portal vein embolization.
The median OS among the patients was 15 months after Y90 (95% confidence interval [CI], 13.2-16.9). One-, two- and three-year OS was 60%, 29%, and 19% respectively. Median OS by line of therapy was 13.9, 17.4 and 12.5 months for first-, second- and third-line. PFS across the whole group was 7.4 months (95% CI 6.4-9.5). Median PFS by line of therapy was 7.9, 10, and 5.9 months for first, second and third.
Six months after treatment, hepatic function toxicities were available in 327 patients. Sixty grade three or four hepatic function toxicities developed with bilirubin (in 29 patients), albumin (13), and aspartate aminotransferase (12) toxicity being the most common. The incidence of hepatic function toxicity at grade three or higher significantly increased with multiple lines of therapy, with bilirubin in 6% of patients after first-line, 7.8% after second-, and 10% after third-; p=0.01). Albumin was 4.2% after first-, 3.1% after second-, and 4.7% after third-line; p=0.008). Five patients (1%) died of liver failure, which was able to be attributed to radiation-induced liver disease.
Emmons’ and her co-authors’ conclusion is that Y90 resin microsphere embolization contributed to 15 months OS after treatment, with patients with the longest OS having received the treatment as part of second-line therapy.
Kieran Murphy
Kieran Murphy (Toronto Western Hospital, Toronto, Canada) also won the award, for his report on a non-inferiority, prospective, randomised controlled trial, which compared intradiscal oxygen-ozone chemonucleolysis to microdiscectomy for lumbar disc herniation radiculopathy.
Murphy’s objective was to compare the non-inferiority treatment status and clinical outcomes of the two aforementioned types of treatment in patients with refractory radicular leg pain due to single-level contained lumbar disc herniations.
The study was multicentre, carried out across three European hospital spine centres. Forty-nine patients with a mean age of 40, of whom 17 were females and 32 males, were studied. All had a single-level contained lumbar disc herniation and had been experiencing radicular leg pain for more than six weeks, as well as being resistant to medical management.
Patients were randomly assigned one of the two treatments, with 25 given intradiscal oxygen-ozone and 24 the microdiscectomy. Eighty-eight per cent (n=43) received their allocated treatment and constituted the as-treated (AT) population.
The primary outcome was overall six-month improvement in leg pain, compared to baseline. Secondary outcomes included back numerical rating pain scores (NRS), Roland Morris Disability Index (RMDI) scores and EuroQol (EQ)-5D, which were collected at baseline, one week, and one, three and six months.
In terms of the study’s results, primary analysis found the overall six-month difference between treatment groups in leg pain improvement using the AT population was -0.31 (standard error [SE]=0.84) points, favouring in microdiscectomy. Using the intention to treat (ITT) population, the difference was 0.32 (SE=0.88) points in favour of oxygen-ozone. The difference between oxygen-ozone and microdiscectomy did not exceed the non-inferiority 95% confidence lower limit of treatment difference in either the AT (95% lower limit, -1.72) or ITT (95% lower limit, -1.13) populations.
Both treatments resulted in rapid and statistically significant improvements over baseline in leg pain, back pain, RMDI, and EQ-5D that persisted in follow-up, and no outcome differences were statistically significant between the two groups.
Murphy’s conclusion is that intradiscal oxygen-ozone chemonucleolysis for single-level lumbar disc herniations that are unresponsive to medical management, met the non-inferiority criteria to microdiscectomy on six-month mean leg pain improvement. Moreover, both treatment groups achieved similarly rapid, significant and persistent clinical improvements. The study also found that 71% of patients who were randomised to the oxygen-ozone group were able to avoid having further surgery.
Bela Kis
Bela Kis (Moffitt Cancer Center, Tampa, USA) received the prize for the second time in two years. In 2020, his winning abstract was ‘Transarterial chemoperfusion treatment of unresectable pleural mesothelioma—interim results of a phase two prospective study’. This year, he won with ‘Radioembolization with Y90 glass microspheres as first-line treatment for unresectable intrahepatic cholangiocarcinoma—a prospective phase two clinical trial’.
Kis explained that patients with unresectable intrahepatic cholangiocarcinoma (IHC) have a dismal prognosis; without treatment the expected survival is three to six months. Standard-of-care first-line treatment with gemcitabine and cisplatin demonstrated improved median overall survival (OS) of 11.7 months. However, this therapy was complicated by severe adverse events in 70% of patients. Prior retrospective studies demonstrated survival benefit of Y90 radioembolization as a first-line treatment in IHC with minimal side effects. The recent phase two clinical trial (MISPHEC) of a combination of Y90 radioembolization plus chemotherapy (cisplatin and gemcitabine) as a first line-treatment in ICC showed median OS of 22 months, but 71% of patients had severe, grade three and four, adverse events. In view of these prior reports, Kis’ study aimed to evaluate the safety and efficacy of Y90 glass microsphere radioembolization as first-line treatment without chemotherapy for unresectable IHC.
Twenty-five eligible patients were enrolled in Kis’ institutional review board-approved phase two study. Eligibility criteria were absence of evidence of extrahepatic metastasis, Childs-Pugh A or B, without main portal vein thrombus, bilirubin <2mg/dL, ECOG performance status of zero to two, and not having chemotherapy, liver embolization, or radiation therapy for IHC. The primary endpoint was progression-free survival (PFS) and secondary endpoints, OS and toxicity.
Two patients were excluded from the study on the basis of unrecognised lung metastasis at the time of Y90 treatment, and right hepatectomy four weeks after Y90, respectively. Twelve women and 11 men were included, of whom the median age was 76 years.
The patients received a median dose of 136Gy radiation from the Y90 treatment. Median PFS was 5.5 months (95% CI: 3.9–7.1 months). Median OS was 27.2 months (95% CI: 8.5–4.9 months) from diagnosis and 19.4 months (95% CI: 4.6–34.1 months) from Y90 treatment.
Univariate and multivariate analyses were performed to find prognostic factors associated with PFS and OS, but none were identified. Furthermore, Kis states that, patients tolerated the radioembolization treatment well, with only two incidences of grade-three toxicity (radiation capsulitis and gastric bleed) reported. At three months, there was one grade three biochemical toxicity (elevated bilirubin).
Kis concludes that first-line treatment of IHC with radioembolization is promising from an OS and toxicity standpoint. When compared to published data on IHC, radioembolization appears to be at least as effective as systemic chemotherapy, but with a much better toxicity profile. This prospective trial suggests that radioembolization can be considered a first-line treatment for unresectable IHC, and can be a stepping stone to initiate large, multi-institutional randomised trials to compare radioembolization to chemotherapy as a first-line treatment of unresectable IHC.
Amy Deipolyi
Amy Deipolyi (Charleston Area Medical Center, Charleston, USA) was another presenter whose abstract ‘Immune activation markers and response to radioembolization of breast cancer liver metastasis: Pilot study’ won the prize. Her purpose in carrying out the study was to ascertain whether radioembolization (RE) of breast cancer liver metastasis (BCLM) activates immune function, as well as to identify the markers of immune function that are associated with RE response. RE was found to be associated with immune activation, as seen within the tumour microenvironment and peripherally. The results also suggest that peripheral markers of inflammation, including monocytes, MDSCs, and ILs may indicate a poor response to RE.
Bluegrass Vascular Technologies recently announced the publication of a paper featured on the cover of the June 2022 issue of the Journal of Vascular Surgery (JVS). The paper reports the use of the company’s Surfacer system to perform an ‘Inside-Out’ procedure and obtain central venous access in a haemodialysis patient presenting with severely symptomatic superior vena cava (SVC) syndrome.
The procedure was performed by Alexandros Mallios (Hôpital Paris Saint-Joseph, Paris, France) and his team.
“Our paper is the first to report on a fully extraanatomical, minimally invasive approach resulting in the bridging of a functioning upper extremity access to the SVC,” stated Mallios. “The use of the Surfacer system enabled us to quickly and efficiently obtain central venous access after two previous attempts to recanalise the central vein occlusion using other approaches were unsuccessful.”
“The case report presented by Dr Mallios and his colleagues further demonstrates the broad clinical utility of the Surfacer system to help facilitate gaining venous access in patients with central venous obstructions,” said Gabriele Niederauer, CEO and president of Bluegrass Vascular. “We congratulate Dr Mallios and his team on having a featured covered story in JVS associated with this interesting case, which included the use of the Surfacer system.”
This follows an announcement from April 2022 in which Bluegrass Vascular highlighted a paper, published in the Journal of Vascular Access, that detailed the use of the Surfacer system to perform the Inside-Out procedure via a transcollateral approach.
Earlier this year, the company also closed US$5 million in convertible debt financing to support the commercial expansion of its Surfacer system.
TriSalus’ clinical leadership team presented new preclinical data at the Society of Interventional Radiology (SIR) 2022 Annual Scientific Meeting (11–16 June, Boston, USA). The data are the result of evaluations of the company’s immunotherapy platform, which integrates an investigational class C toll-like receptor 9 (TLR9) agonist, SD-101, and the proprietary Pressure-Enabled Drug Delivery (PEDD) method of administration to overcome critical treatment barriers that can prevent immunotherapeutic uptake in hard-to-treat tumours.
In one abstract presentation, TriSalus highlighted data that suggest the PEDD method was more effective in delivering SD-101 into liver tissue than direct needle injection. To further support these findings, TriSalus is collaborating with Massachusetts General Cancer Center (Boston, USA) on an investigator-initiated clinical trial to evaluate whether PEDD improves the delivery of radioactive microspheres during radioembolization treatment for liver cancer, compared to a standard microcatheter.
In a second abstract presentation at SIR 2022, TriSalus highlighted new data on the development of a transvenous approach for the regional treatment of pancreatic tumours, called pancreatic retrograde venous infusion (PRVI). This preclinical data are the first of their kind to demonstrate that the PRVI approach can improve uptake and tumour response for pancreatic tumours. Unlike the liver, using the arterial systemic for drug delivery in the pancreas poses significant anatomic challenges. TriSalus has developed a novel approach to leverage the PEDD method in venous branches using a new US Food and Drug Administration (FDA)-cleared device designed for highly targeted intrapancreatic delivery of SD-101.
“Patients with liver and pancreatic tumours can experience poor outcomes due to tumour-induced immunosuppression and high intratumoral pressure that often prevent therapeutics, such as immunotherapy drugs, from reaching their targets. Existing treatment approaches, including direct needle injections and intravenous immunotherapy alone, often fail to address these barriers in a comprehensive way. By engineering new approaches to meet these challenges, we may be able to improve the treatment paradigm for liver and pancreas tumour patients,” said Steven C Katz, chief medical officer at TriSalus.
University Medical Center Utrecht (Utrecht, Netherlands) recently published the latest results from the HEPAR Primary study, which evaluated the safety and efficacy of Holmium-166 (QuiremSpheres holmium-166 microspheres) Selective Internal Radiation Therapy (SIRT) for hepatocellular carcinoma (HCC) patients (Barcelona Clinic Liver Cancer stages B and C) without curative options.
HEPAR Primary showed an acceptable toxicity profile and demonstrated an objective response rate of 54% (14/26 patients) at three months after mRECIST evaluation of target liver lesions. The news was shared by Terumo Interventional Systems, the company behind the technology.
“We are very excited about the safety and efficacy results of our HCC study, in which we have been using QuiremScout for the work-up and QuiremSpheres for the SIRT treatment. At the start of our study, we did not have the opportunity to use the pre-treatment planning functionalities of the Q-Suite imaging software (launched in September 2020),” said author, Marnix Lam (University Medical Center Utrecht, Utrecht, Netherlands). “Looking towards the future, I strongly believe that we can achieve even better clinical outcomes by truly individualising the treatment of each patient using the entire Holmium platform. Therefore, we are currently recruiting patients in a new multi-centre iHEPAR study to further demonstrate the importance of individualising SIRT in HCC using the full Holmium platform.
The Holmium platform consists of three integrated products, QuiremScout holmium-166 microspheres, QuiremSpheres holmium-166 microspheres and Q-Suite imaging software, that allow healthcare professionals to select patients with confidence, deliver treatment with precision and plan and verify with accuracy.
“We are delighted with the results of the HEPAR Primary study, which demonstrate the benefits of Holmium SIRT in the treatment of primary liver cancer. This study is an additional demonstration of the value of our Holmium platform and using QuiremScout and QuiremSpheres together. We are confident this will continue supporting the adoption of the Holmium platform,” said Laurent Domas, global vice president of strategy and therapy development, Interventional Oncology Terumo.
The findings of a collaborative research project at the University of California San Diego, San Diego, USA were presented in an abstract titled ‘Multivessel pelvic embolization during caesarean hysterectomy for placenta accreta spectrum: A single-centre experience and comparison to internal iliac artery balloon occlusion’ at the Society of Interventional Radiology (SIR) 2022 Annual Meeting (11–16 June, Boston, USA).
This collaboration among interventional radiology, obstetrics and gynaecology, and maternal foetal medicine teams aimed to compare how intraoperative pelvic embolization performed to reduce blood loss during surgical management of placenta accreta spectrum (PAS) versus internal iliac artery balloon occlusion (IIABO). The abstract’s lead author, Christine Boone, explained to Interventional News ahead of the presentation her surprise at the extent of blood loss reduction with embolization compared IIABO, alongside some of the other aspects of her research.
Regarding the study’s results, Boone first outlined her prediction that blood loss would be “similar or better” among the embolization group. “But what surprised me was by how much [embolization improved outcomes],” Boone went on to acknowledge. In the IIABO group, she noted, median blood loss was 2.5 litres, where any amount over one litre in a caesarean section delivery is considered a haemorrhage. “It was a lot more before [occlusion], and people had to get blood transfusions,” Boone said, contextualising the benefit that IIABO intervention brings. Yet, the median blood loss, she then noted, with embolization, was only 675ml “which is not even considered a haemorrhage by the criteria for caesarean [delivery].” In this group, no patients needed transfusions, which was not the case for the occlusion group. Boone labelled this “a really striking difference,” accounting for her surprise at her study’s findings. Of note, the comparative procedure times for IIABO and embolization, which were an average of 35 and 64 minutes, respectively, Boone admitted that the duration of the procedures is an important consideration. While the longer duration of the embolization procedures did not present issues in the context of the study, it may in some cases.
Christine Boone
The abstract was also recognised as ‘exceptional’ among those presented at the meeting. Additionally, Boone received the SIR Foundation Resident Research Award during the meeting’s award ceremony plenary session on Monday 13 June.
Boone began by relaying to Interventional News how she was inspired to study the applications of interventional radiology (IR) in women’s health after “[repeatedly] hearing about how maternal mortality was increasing in the USA” as she was finishing medical school. “I thought this was so strange,” she admitted, given “how we pay so much for healthcare in this country.”
Expanding on what drew her into women’s health and IR, she conveyed her passion for being “able to intervene, especially in postpartum haemorrhage situations” and that “that was the thing that would often kill women in childbirth.” Boone went on to underline how haemorrhage management can be achieved in “as little as 15 minutes,” and that this is one of the reasons why she sees her area of research as a “really exciting opportunity to help.”
Learning more about placenta accreta spectrum disorders, Boone highlighted as “fascinating”, not just from a treatment point of view, but also from a scientific standpoint. “The more I read about it, the more I learned that it was almost like a malignancy […] it does not respect boundaries […] and behaves like a cancer.” Spreading greater awareness about the disease is, therefore, something about which Boone feels strongly.
Quizzed on the two treatment options compared in her research project, Boone first conveyed how there is, currently, no standard of care regarding PAS treatment. Different clinicians may choose different approaches, including hysterectomy, as well as leaving the placenta in place to manage bleeding (the latter, however, brings with it risk of infection). IR provides a further swathe of treatment options, such as embolization and balloon occlusion, Boone detailed.
According to Boone, this application balloon occlusion “came earlier”, but that it is not necessarily used more often than embolization nowadays, as there isn’t data available on this. Nevertheless, the fact remains that there is more research on the former type of treatment. Aortic balloons are used in trauma situations, and so are widely seen as an effective method for stopping blood flow, hence the recourse to them in a PAS treatment scenario, Boone proceeded. She then detailed how aortic balloons have, in fact, been used for PAS cases during surgery, but that this threatens limbs and other organs by stopping blood flow to everywhere below where the balloon is inflated. Consequently, “the benefit of the [IIABO] is that it is more selective […]—the internal iliac artery [supplies] blood to everything in the pelvis, but the legs are excluded”.
Despite this advantage of IIABO, Boone then shared her thoughts on why embolization may work better still: “The placenta in PAS does not respect [anatomic] boundaries, including its vascular supply and so it can pull blood from the abdominal wall [for example].” This may mean that, in certain cases, the IIABO’s role is insufficient, as it is not stopping blood flow to additional vessels in question. Embolization is favourable in these cases, Boone outlined, expanding on this point with the following explanation: “[with embolization], we are looking for collaterals […] we can adapt the therapy to the unique situation of the patient and where the blood is coming from.”
The discussion then turned to the specific particles one can use for embolization to treat PAS. Boone began by conceding that no study to date has compared particle types for this indication. There can be different approaches to embolization and the type of particle is an important consideration in this strategy. Studies to determine optimal embolization strategies and embolic type would be a significant next step. Another “good future direction” for research would be subgroup analysis, as the study is ongoing. Boone explained, however, for now, the number of patients is too low for this to be possible. “There is definitely something to be said for gravidity [and there also could be] for the number of caesarean sections a patient has had,” Boone stated.
In conclusion, Boone told Interventional News how she sees these results as “huge”, and she is excited to see the impact they might have for PAS care. She also took the opportunity to give insight into her other area of research. Currently used in the treatment planning of pelvic venous disease at the University of California San Diego, Boone shared her interest in taking 4D flow magnetic resonance imaging (MRI) into the area of PAS, to see if it could aid in identifying where the placenta is drawing blood from in each specific patient’s case, ahead of the procedure, which could make treatment faster.
Peripheral arterial disease (PAD) produces a global health burden and remains a leading cause of disability, limb loss and reduced quality of life. PAD is also a proxy for cardiovascular and cerebrovascular death. Endovascular therapies have become widely used among symptomatic patients refractory to medical and exercise therapy alone, including stents, drug-eluting balloons, atherectomy, and vessel modification devices.
Our current understanding of the biologic mechanisms of these devices remains incomplete. Endovascular practitioners need a deep understanding of the vascular biology and biomechanics of endovascular therapies to enable critical appraisal, identify gaps in existing knowledge and define unmet needs for their current and future patients.
Chronically occluded lower extremity arteries, particularly long-segment TASC-C and -D lesions, were long considered untreatable with percutaneous approaches and amenable only to surgical bypass. Endovascular techniques which intentionally create an intramural channel within the arterial media, followed by angioplasty with or without stent placement, were first described by Bolia but have since evolved to encompass a wide array of dedicated technologies. This approach, known as subintimal recanalisation, has now become routine for many interventionalists. What is remarkable is that the vascular remodeling following subintimal recanalisation almost completely replicates the histologic elements of a native artery.
Understanding the remodelling changes after this approach can guide selection of subsequent use of other endovascular techniques to maintain vessel patency and limb preservation.
Angioplasty balloons and stents as delivery platforms for anti-proliferative drugs to the therapeutic targets of fibroblasts and smooth muscle cells within the media and adventitia have become widely utilised in endovascular therapy. Interventionalists need to distinguish cytostatic from cytotoxic drugs, understand their pharmacokinetics and mechanisms within the cell cycle. Perhaps as importantly, various coating and polymeric delivery systems (excipients) differ greatly in efficiency and efficacy and are significant determinants of clinical benefits of these therapies.
Timothy Clark
Bioabsorbable scaffolds offer enormous potential to provide a stent-like scaffold to optimise arterial remodelling, while resorbing over time to leave no permanent implant behind. These devices gained rapid, nearly global adoption in the coronary vessels until the risks of late thrombosis were recognised and led to their near-abandonment. In the peripheral vascular applications, bioabsorbable scaffolds face a demanding list of attributes: high radial force, predictable resorption without particulate embolization or thrombosis, and sufficient radio-opacity to enable precise deployment within heavily calcified vessels. Despite these challenges, several promising technologies may soon yield these devices for the periphery with favourable effects on vascular remodelling.
Atherectomy is a widely utilised technique in endovascular therapy, but randomised trials dating back to first-generation plaque excisional devices have consistently struggled to show a compelling, cost-effective clinical benefit of this therapy. A wide array of atherectomy systems have since evolved, however the extent to which these devices remove significant quantities of plaque, thrombus, or cellular/fibrotic deposits remains insufficiently understood. Vascular remodelling after atherectomy is variable and often unpredictable, and intraprocedural risks of embolic debris worsening underlying limb ischaemia remain an ongoing concern. A broader understanding of the vascular biology behind the purported mechanisms of various atherectomy systems is needed.
Vessel preparation techniques employ devices to score, cut, sonicate, or create microfenestrations in a vessel wall prior to subsequent angioplasty or stent placement. These techniques are considered beneficial when peripheral arteries are highly calcified or extremely stenotic. It is key to understand the vessel wall modifications that occur with these ‘vessel prep’ devices and to what extent these modifications confer a benefit in sustaining vessel patency.
Lastly, self-expanding nitinol stents, including bare-metal, drug-eluting and polytetrafluoroethylene-covered, are widely used in the femoropopliteal artery. The femoropopliteal artery experiences among the highest levels of torsion and compression within the body. These stents are typically laser-cut, electropolished nitinol tubes which are shape-set to undergo prescribed expansion upon delivery within a vessel. Specific stent design features may be less prone to strut fractures and thereby, intimal hyperplasia and thrombosis. Certain stent designs
can create spiral laminar flow, which may reduce wall shear stress and platelet activation.
Each of these topics were explored within a Categorical Course at the Society of Interventional Radiology Annual Scientific Meeting (11–16 June, Boston, USA). By understanding the biology of vascular remodelling, which occurs following endovascular interventions including angioplasty, subintimal recanalisation of chronic total occlusions, stent placement and atherectomy, we hoped to provide further insight to vascular interventionists to distinguish existing endovascular devices based on design, mechanism and performance.
Timothy Clark is director of interventional radiology at Penn Presbyterian Medical Center, University of Pennsylvania, Philadelphia, USA, and professor of clinical radiology in the Department of Radiology at the Perelman School of Medicine, University of Pennsylvania, Philadelphia, USA.
Disclosures: Clark is a consultant for BD, Boston Scientific, Teleflex, B. Braun and Baylis Medical, and receives royalties from Teleflex and Merit Medical. He is founder of Forge Medical and NeuRx Medical.
The 2022 European Congress on Interventional Oncology (ECIO) took place 24–27 April in Vienna, Austria. Interventional News spoke to chairman Philippe Pereira (SLK-Kliniken, Stuttgart, Germany) to hear his thoughts on the new addition to the meeting programme for this year: the foundation interventional oncology (IO) course.
Q: Why is the launch of this course such a landmark event? What will it mean for the area of IO and its trainees going forward?
A: IO is rapidly continuing to establish itself as the fourth pillar of cancer care alongside medical, surgical and radiation oncology. To the advantage of the right patients, IO can be combined with surgery, systemic treatment and, in some instances, with radiation therapy. Moreover, IO procedures can be hugely beneficial not only for the recovery times of the patient, but they are often far more cost-effective when compared to other therapies. The most effective way to increase the possibilities for patients to benefit from minimally invasive oncology treatments is for interventional oncologists to practise as fully fledged clinicians rather than simply as technicians, holding outpatient clinics and participating fully in discussions at multidisciplinary team meetings. In order to do this successfully, they must learn the basics of oncology in relation to the conditions they treat, so that they can engage in meaningful discussions with other clinicians and patients.
During ECIO 2022, we had the first foundation course in IO ever to have been held in Europe. The foundation course is for interventional radiologists who are not yet familiar with minimally invasive oncological procedures, and this day-long foundation course on the basics of oncology, including all surgical disciplines and radiation therapy offers a fantastic opportunity to get started in this field. The course came into being based on a very important concept, namely the recognition that interventional oncologists must be educated as true medical doctors (oncologists), and not just carry out the role of a technician.
The goal of the course is, ultimately, to improve cancer care by increasing clinicians’ knowledge of multidisciplinary and multimodal treatment strategies: IO offers safe and effective treatment for patients with a variety of malignancies. In recent years, potentially curative interventional radiology (IR) procedures have also emerged, making an increasingly significant contribution to the treatment of cancer patients. And this does not only hold true in a palliative setting. These developments are what is responsible for establishing IO as the fourth pillar of cancer care, alongside medical, surgical and radiation oncology, as I mentioned. IO procedures, when applied to the right patients, achieve excellent oncological results with fewer complications and shorter hospital stays than conventional surgery. As a result, they are less expensive and more cost-effective than surgery.
Despite these advantages, many countries do not have the infrastructure and provisions for carrying out IO procedures, and this even includes those countries where IR is well established. Across the globe and within Europe too, the spectrum of available IO procedures varies substantially, making it difficult to offer this service to patients in a reliable manner. This variation also makes it harder for tumour boards to make recommendations as to the best multidisciplinary IR treatments for patients.
Q: What were some of the meeting highlights for you?
A: It is a bit difficult to answer this question as the chairman of the meeting (!), but I would say, maybe, the sessions that focused on combined treatments were a highlight, as this is a field that is continuously evolving. The contents of the sessions gave insight into some of the developments we will see in the future, underlining that multidisciplinary approaches can achieve some of the best results for lung and metastatic cancer patients in particular. The take-home message here is that no single clinician or oncological specialty alone has the solution for cancer patients. Other highlights were the clinical research sessions that will establish IO in future treatment algorithms, the place of artificial intelligence in IO, but also emergencies in IO as well as and the session on IO in paediatrics, without forgetting the famous ‘Morbidity and Mortality’ session.
Q: What is your impression of how the course went?
A: This course was the first multinational event after COVID-19. Nevertheless, the course was packed, and there were numerous enthusiastic comments from some of the younger attendees, and also from the experienced clinicians on the faculty.
The best question or comment (even if we did not allow enough time to discuss it at length) was from a young participant: “…but who decides on the treatment of a cancer patient, the oncologist, the surgeon, the radiotherapist or the interventional radiologist?” This, I felt was especially pertinent as it was asked without any preconceptions, and it best reflects the need for this kind of course.
In the USA, liver transplantation continues to be the best chance at long-term survival for patients suffering from the sequelae of end-stage liver disease. However, recent data from the Organ Procurement and Transplant Network (OPTN) suggest that there are 13,000 patients in the USA who are listed for liver transplant at any given time. Of that number, a high percentage of patients will either pass away while waiting for liver transplantation or be delisted due to complications of liver disease making transplantation difficult or impossible. For many of these patients, we have found that interventional radiology (IR) and the techniques we are able to offer can help prolong patient survival on a waiting list or reduce the number of delistings due to technical limitations.
With that said, many of the patients who do go on to receive a successful liver transplant, will end up with post-transplant liver complications. This could be as many as 30% of patients, and a significant number can benefit from endovascular or percutaneous intervention. The benefit of a multidisciplinary approach and, specifically, the use of endovascular techniques for many peritransplant vascular complications, is the ability to avoid major surgery or revisions.
Although peri-liver transplant patients comprise such a complex group, of whom many could benefit from these IR services, there are data to suggest that a large number are still not being offered interventional services in both a pre- and post-transplant setting. Some of the contributing factors are lack of awareness among referring providers regarding the services we can provide; lack of patient awareness; and lack of consensus among interventional radiologists themselves about the best treatment plans for these
complex patients.
Our own experience has been that when patients are offered interventional radiology services, the outcomes of liver transplantation for our centre as a whole improves. Formal incorporation of IR into the Multidisciplinary Liver Transplant group (including representation on the Liver Selection Committee), and establishment of an IR and hepatology-led multispecialty portal venous thrombosis clinic are some of the ways in which our IR team has provided access to many of the advanced techniques that should be offered to the Liver Transplant patient cohort. Indeed, use of advanced portal vein recanalisation techniques, pretransplant large portosystemic shunt embolization, and optimisation of liver graft arterial flow through hepatic artery stenting and splenic embolization for portal hyperperfusion are examples of how IR can maximise liver transplant centre outcomes.
Given the current issues facing pre- and post-hepatic transplantation vascular management, we proposed the ‘Advanced IR hepatic and splenic vascular interventions in peritransplant patients’ course as a new forum for the recent Society of Interventional Radiology (SIR) 2022 Annual Scientific Meeting, Boston, USA. This session provided a forum for experts in the field to discuss these complex cases in a format that generated robust discussion and questions.
Muneeb Ahmed is chief of the division of vascular and interventional radiology and vice chair for interventional services at Beth Israel Deaconess Medical Center, Boston, USA. He is also associate professor of radiology at Harvard Medical School, Boston, USA.
Vijay Ramalingam is co-director of interventional radiology for the Mesenteric Venous Thrombosis Program at Beth Israel Deaconess Medical Center. He is also an instructor at Harvard Medical School.
SoniVie recently announced that on 5 May 2022 the US Food and Drug Administration (FDA) granted investigational device exemption (IDE) approval for its REDUCED1 pilot study to treat resistant hypertension patients with renal artery denervation using the company’s therapeutic ultrasound ablation system (TIVUS).
“We are very pleased that the FDA has approved the REDUCED1 (Renal denervation using ultrasonic catheter emitted energy) study. Sites initiation has started, and many clinical teams have responded very favourably about participating in the study. There is a significant number of patients that may benefit from our technology and we are happy to announce this important step towards the introduction of TIVUS in the USA. There is a lack of effective therapeutic solutions for patients suffering from resistant hypertension, and physicians are looking forward to a safe, effective and easy to use device treatment,” says Christian Spaulding, CMO, SoniVie.
“This is a significant US regulatory milestone for SoniVie, starting the feasibility study using the ultrasound ablation platform in the USA for the renal denervation indication. This is a major step and priority in the company’s history,” says Tomaso Zambelli, CEO, SoniVie.
The REDUCED1 study will further expand the company’s clinical experience based on two clinical trials in renal denervation performed using the earlier generation of the TIVUS.
According to SonieVie, renal denervation with TIVUS is a minimally invasive procedure that uses high-frequency non-focused ultrasound energy to ablate nerves in the renal artery. The company claims that this causes a reduction in the nerve activity, which may decrease blood pressure. This procedure is designed for patients who suffer from resistant hypertension.
Shimadzu Medical Systems USA introduced the new Trinias system, which uses artificial intelligence deep learning to improve the visibility of medical devices while using lower X-ray doses than previous models, at the Society of Interventional Radiology Annual Meeting (SIR 2022; 11–16 June, Boston, USA).
This is the first time AI has been incorporated into the image-processing engine of an angiography system, the company declared in a press release.
The new Trinias system also offers an extensive new feature set to simplify workflow, allowing a more efficient clinical operation in any medical setting, the company reported. Shimadzu has also launched a subscription service that ensures software can always be updated to the current version, making the Trinias system a more sustainable product designed for long-term use.
Angiography systems are used to perform angiographic examinations, where the physician inserts a catheter through a blood vessel in the patient’s wrist or inguinal region to a specific site and observes an area of disease or concern, and to perform catheterisation procedures, where a therapeutic device is inserted in the patient and used to dilate blood vessels or perform other interventional procedures.
Medical facilities are increasingly operating angiography systems at low radiation levels to reduce X-ray doses, but low radiation levels also lead to X-ray noise that reduces device visibility. To support the low-dose operation of angiography systems by medical facilities and ever-smaller therapeutic devices that reduce the burden on patients, Shimadzu has developed SCORE Opera, a new image-processing technology that uses AI to ensure catheterisation procedures are safe even at low radiation doses.
Cordis recently announced the first-in-human use of the Radianz radial peripheral system by Jihad Mustapha at Advanced Cardiac & Vascular Centers (ACV) Grand Rapids, USA.
The Radianz radial peripheral system solution includes Brite Tip Radianz guiding sheath used to optimise lower extremity lesion access, the Saberx Radianz percutaneous transluminal angioplasty (PTA) catheter to facilitate treatment, and the S.M.A.R.T. Radianz vascular stent system to help maintain patency for lasting favourable outcomes.
The system is purposely engineered for radial access, which, the company claims, is proven to produce fewer vascular complications and higher patient satisfaction than femoral approaches.
Mustapha, chief executive officer and director of endovascular intervention at Advanced Cardiac & Vascular Centers (ACV) for Amputation Prevention, commented: “My colleagues at ACV and I are pleased to have successfully performed the first procedures using the Radianz radial peripheral system. We believe this portfolio represents true innovation in meeting the need for radial access solutions for lower extremity intervention.”
“We are extremely pleased with the positive feedback from Dr Mustapha and proud that these first-in-human cases were performed so successfully and by such a highly esteemed physician,” said Cordis CEO Shar Matin. “When used as a comprehensive treatment solution for vascular disease, we believe the unique capabilities of the Radianz radial peripheral system have the potential to positively impact outcomes and improve quality of life for patients.”
According to a company press release, multiple studies have demonstrated overwhelming patient preference for radial versus femoral access. Studies also show that patient ambulation time can be reduced from hours to minutes, and that patients experience improved mobility and comfort from the outset, the release continues.
In addition to the clinical benefits of the Radianz radial peripheral system, Cordis claims that radial access can reduce the total cost of care. The company references a systematic review of 14 randomised controlled trials that found radial access lowered hospital costs in the USA by up to US$1,116 per procedure in duration-of-stay costs compared to femoral access.
The Radianz radial peripheral system portfolio is expected to launch later this year in the USA and in the near future in Japan, the company advises.
Artio Medical today announced the closing of US$28 million in oversubscribed Series A2 and Series A3 financing, bringing the total amount raised by the company to date to US$74 million.
Funds will be used to support US commercialisation efforts for the recently cleared Solus Gold embolisation device and to accelerate the development of Artio’s broad portfolio of products, including expanding the company’s engineering and manufacturing capabilities, a press release details.
Artio is currently developing 10 products for the peripheral vascular market, including the Solus Gold and Solus Flex embolisation devices for peripheral vessel occlusion and the Amplifi vein dilation system—which is designed to prepare haemodialysis patients for successful arteriovenous fistula vascular access site creation.
Artio is also currently developing four products for the neurovascular market, including the Endura embolisation system comprising a detachable balloon and coils for the treatment of saccular brain aneurysms.
“We would like to thank our existing investors for their continued strong support and also welcome a new group of investors to Artio,” stated Joseph McConnell, vice president of Finance and Business Operations at Artio. “We have the opportunity to do something really special here, to bring a new generation of medical devices to market with the potential to save lives, reduce disability, and improve the quality of life for millions of people. This new capital will help Artio expand our team and scale our operations to deliver on that mission.”
M.I.Tech is the creator of the HANAROSTENT technology, a family of conformable, non-vascular, self-expanding metal stents, which have been distributed by Boston Scientific in Japan since 2015. The agreement consists of a purchase price of KRW 14,500 per share, which represents a total of KRW 291.2 billion or approximately $230 million at current exchange rates, subject to closing adjustments.
Non-vascular gastrointestinal and airway stents are used to help clear occlusions or strictures in various areas of a patient’s anatomy, including the biliary tree, pancreatic duct, oesophagus, colon and duodenum. In many cases, stent placement is minimally invasive and may aid faster patient recovery compared to surgery.
The HANAROSTENT technology features a unique hook-cross nitinol design intended to provide a natural and flexible fit within a patient’s anatomy, as well as flared ends to help prevent stent migration.
“M.I.Tech is an innovator in non-vascular stent development, with product offerings that complement our existing stent portfolio, including the differentiated AXIOS stent and Electrocautery enhanced delivery system and the flexible and conformable Agile oesophageal stent system,” said Art Butcher, executive vice president and group president for medical surgery and Asia Pacific, Boston Scientific. “We are committed to investing in technologies that advance care for patients around the world and are eager to work more closely with M.I.Tech to expand their international footprint.”
The company expects to complete the transaction in the second half of 2022, subject to customary closing conditions. The impact to generally accepted accounting principles and adjusted earnings per share is expected to be immaterial in 2022.
Cordis Names George Adams, MD as Chief Medical Officer
George Adams
Royal Philips today announced the latest results from the Tack optimised balloon angioplasty (TOBA) II below-the-knee (BTK) clinical trial, demonstrating that the Philips endovascular system—Tack (4F)—provides a sustained treatment effect and positive impact on quality of life for patients with chronic limb-threatening ischaemia (CLTI) out to three years of clinical follow-up. The Tack 4F is the first and only device of its kind approved by the US Food and Drug Administration (FDA), according to a company press release.
The TOBA II BTK trial studied the safety and efficacy of post-angioplasty dissection repair using the Philips Tack endovascular system in patients with CLTI and infrapopliteal disease. Philips details that the Tack endovascular system is a unique specialised implantable device to optimise the treatment of dissections in patients with CLTI. Endpoints included rates of major adverse events, target lesion revascularisation (TLR), target limb salvage (TLS) and quality of life (QoL) metrics.
“Based on 36-month follow-up in the TOBA II BTK trial, which is following 233 patients at 41 sites internationally, the Tack endovascular system offers a new standard in repairing below-the-knee arterial dissections,” said co-principal investigator George Adams (UNC Rex Hospital, Raleigh, USA), who presented the results at the New Cardiovascular Horizons (NCVH) conference (31 May–3 June, New Orleans, USA).
Adams added: “The device stands to significantly benefit patients with CLTI whose treatment with balloon angioplasty often leads to this particular complication, which typically goes untreated and unaddressed, to the detriment of long-term clinical outcomes.”
The three-year analysis of TOBA II BTK results includes the following clinical insights on the Tack endovascular system:
93.9% target limb salvage in CLTI patients at three years
69.6% freedom from clinically-driven target lesion revascularisation across all patients at three years
Sustained improvement in established clinical classification systems including the Rutherford clinical category and haemodynamics in ankle- and toe-brachial indices
Sustained improvement in patient-reported quality-of-life and mobility measures
“In treating peripheral arterial disease below the knee with balloon angioplasty, dissections of the popliteal, tibial and peroneal arteries occur with considerable frequency,” explained Chris Landon, business leader of Image Guided Therapy Devices at Philips. “With the Tack endovascular system from Philips, interventionists can reliably repair below-the-knee arterial dissections – and in doing so, improve major amputation rates and quality of life.”
Philips has previously reported data from the TOBA II and III studies, which evaluated the Tack endovascular system for superficial femoral and proximal popliteal artery dissection repair following uncoated balloon angioplasty and/or drug-coated balloon (DCB) angioplasty. These multicentre, global and European studies demonstrated that the use of the Tack endovascular system resulted in dissection resolution following uncoated or DCB angioplasty.
In TOBA II, which involved uncoated and drug-coated balloons, dissection repair with the Tack System resulted in 89.6% and 86.5% 12-month primary patency (uncoated balloon group) and freedom from CD-TLR
In TOBA III, which involved drug-coated balloons, dissection repair with the Tack endovascular system resulted in 95.0% and 97.5% 12-month primary patency and freedom from CD-TLR
There were no major adverse events reported through 30 days in either study.
Together, the TOBA II, TOBA III and TOBA II BTK trials support the safety and efficacy of the Tack endovascular system for post-PTA dissection repair in above- and below-the-knee arterial disease. According to Philips, the 36-month TOBA II BTK data reported at NCVH adds to the “robust” body of clinical evidence supporting the safety and effectiveness of the Tack Endovascular System in both vessel beds.
Philips Tack endovascular system is currently available for sale in the USA and some EU countries. Further information, including safety information, is available here.
Damaged nerves can be regenerated with the application of a frozen needle under advanced imaging guidance, according to new research to be presented at the Society of Interventional Radiology Annual Scientific Meeting (SIR; 11–16 June, Boston, USA).
The technique, called interventional cryoneurolysis, is performed by an interventional radiologist and can offer hope to patients in persistent pain following a traumatic injury, according to an SIR press release.
“The idea that we can induce regeneration of damaged nerves simply by placing a cold needle through the skin under imaging guidance is extremely exciting,” said the lead author of the study, J. David Prologo (Emory University School of Medicine, Atlanta, USA). “This research answers the call from United States legislators and specialty medical societies to develop alternatives to opioids for the management of pain.”
Researchers at Emory University treated eight patients with chronic nerve pain related to a prior trauma with computed tomography (CT)-guided interventional cryoneurolysis. CT-guided cryoneurolysis uses imaging to place a needle and freeze damaged nerves, causing them to degenerate and lose function. “What happens next is almost magical,” Prologo says. “If the nerve is exposed to the correct amount of cold, over the correct area, for the right amount of time, it will regenerate—replacing the previously damaged nerve with a healthy one.”
In this study, the average time from traumatic injury to the procedure was 9.5 years. There were no procedure related complications or adverse events, and all patients returned to their baseline strength over time—confirming regeneration of the targeted nerve. In six of the eight patients, pain symptoms dramatically improved following regeneration—reflected as a collective decrease of 4.6 points in Visual Analog Scale pain scores. The average time from the procedure to the final contact point was 1.9 years.
Prologo believes that the interventional radiology skillset applied to nerve freezing has many applications for treatment of complex pain. “We are using this regeneration technique not only to manage nerve pain induced by trauma—but also for pudendal neuralgia, post-mastectomy pain, post-surgical pain, and many other conditions historically managed with narcotics,” says Prologo. “Interventional radiologists can place these needles safely in precise locations all over the body, allowing access to pain generators that were previously unreachable and giving hope to patients who struggle with pain.”
An experimental formulation of a hydrogel injected into spinal discs proved safe and effective in substantially relieving chronic low back pain caused by degenerative disc disease (DDD), according to new research to be presented at the Society of Interventional Radiology Annual Scientific Meeting (SIR; 11–16 June, Boston, USA). Hydrogels have been used for a number of years to treat DDD, but the current study is the first test of this particular gel in humans, according to an SIR press release.
After six months, all participants in this small study reported significantly less low back pain—declining from an average self-reported pain level of 7.1 down to 2.0 on a scale of zero to 10. They also experienced greatly improved physical function, with average scores falling from 48 to six on a questionnaire to gauge the impact of low back pain in preventing patients from the ability to perform normal activities.
“If these findings are confirmed in further research, this procedure may be a very promising treatment for chronic low back pain in those who have found insufficient relief from conservative care,” said lead author Douglas P. Beall (Clinical Radiology of Oklahoma, Edmond, USA). “The gel is easy to administer, requires no open surgery, and is an easy procedure for the patient.”
The gel used in this study, Hydrafil, is a second-generation hydrogel developed by ReGelTec, Inc. In 2020, it received US Food and Drug Administration (FDA) breakthrough device designation, which allows expedited review when early evidence suggests an experimental product may provide more effective treatment than current options for treating a serious condition.
The research team enrolled 20 patients, aged 22 to 69, with chronic DDD low back pain. Each described their pain as four or higher on the 10-point scale. None had found more than mild relief from conservative care, which includes rest, analgesics, physical therapy, and back braces.
Patients were sedated for the procedure, and the gel was heated to become a thick liquid. Guided by fluoroscopic imaging, researchers used a 17-gauge needle to inject the gel directly into the affected discs, where the gel filled in cracks and tears, adhering to the disc’s centre and outer layer.
“We really have no good treatments for degenerative disc disease, aside from conservative care,” said Beall. “Surgery is statistically no more effective than conservative care and can potentially make things worse; nerve ablation is appropriate for only a few patients; and existing hydrogels are inserted through an incision as a soft solid, which can pop out of place if you’re not highly skilled in placing it.”
“Because this gel is injectable, it requires no incision, and it augments the whole disc, restoring its structural integrity, which nothing we have currently can do,” he said.
Degenerative disc disease is the leading cause of chronic low back pain, one of the world’s most common medical conditions. Healthy discs cushion the spine’s vertebrae, facilitating movement and flexibility. With normal aging, though, they can become dry, thin, cracked or torn, causing pain or loss of motion. By age 60, most people have at least some disc degeneration.
A simple diagnostic procedure, followed by an interventional radiology treatment known as fallopian tube recanalisation, could allow a high percentage of women struggling with infertility from blocked fallopian tubes to conceive with less involved or, in some cases, no further invasive fertility procedures, according to new research to be presented at the Society of Interventional Radiology Annual Scientific Meeting (SIR; 11–16 June, Boston, USA). Researchers said in a press release that most women with with blocked fallopian tubes could have their condition easily corrected.
“This procedure and treatment can help women make an informed decision about infertility treatments. And for many, it can actually give them the chance to conceive naturally,” said Lindsay Machan (University of British Columbia, Vancouver, Canada), a lead author of the study. “As women increasingly desire more thorough discussions of available options and input into their medical care, they appreciate detailed information to help them make choices. This is especially true with fertility treatments.”
Researchers at the University of British Columbia Hospital (Vancouver, Canada) studied cases from 2015 to 2021 involving 956 women with infertility who had previously been diagnosed as having one or both fallopian tubes blocked based on the standard diagnostic procedure used to assess the openness of fallopian tubes, known as hysterosalpingogram (HSG). The women then underwent a selective salpingography to confirm their HSG diagnosis and, if needed, underwent fallopian tube recanalisation. In many cases, researchers said, the purported blockage was only a piece of mucus that was easily removed.
The diagnostic examination known as selective salpingography showed that nearly one in four (23.8%) had been mistakenly told they had one or both fallopian tubes blocked. Of those with a blockage, over half (56.7%) were unblocked using a fine wire in the fallopian recanalisation process, researchers said. In summary, 80.5% of women in the study who had previously been told they had tubal blockages left the same day with both fallopian tubes open after a simple outpatient procedure. In an additional 15.9%, a more precise diagnosis of significant tubal disease was made that in many cases, potentially altered treatment options.
Selective salpingography uses X-ray guidance to insert a tiny catheter through the cervix and into the opening of the fallopian tubes. A contrast dye is then injected to assess whether the tubes are open or blocked. The interventional radiologist, in many cases, is then able to perform recanalisation which opens the tube using a fine guidewire. The procedure is performed as an outpatient under light sedation and typically takes under 30 minutes.
Machan said the research suggests that selective salpingography should be offered more broadly in assessing and treating female infertility. “Fertility treatments can be expensive and out of reach for many women,” he said. “Infertility is also an emotional, often heart-breaking journey, so having this diagnostic procedure and treatment available could be life-changing.”
May’s top 10 stories on Interventional News include a report of long-term data on the safety of femoropopliteal endovascular treatment with paclitaxel-coated devices, FDA clearance of a new fibred detachable coil, and coverage of two developments in the use of robotics for performing interventions with increased accuracy.
Magneto Thrombectomy Solutions (Magneto), a medical devices company developing thrombectomy solutions for the treatment of ischaemic stroke and pulmonary embolism, presented successful first-in-human (FIH) results showing safety and feasibility of the eTrieve system, a catheter based on electric fields for removing blood clots, in patients with acute pulmonary embolism (PE).
The Royal Australian and New Zealand College of Radiologists (RANZCR) has issued a statement addressing the Australian and global shortage of iodinated contrast media.
New long-term data from the SAFE-PAD (Safety assessment of femoropopliteal endovascular treatment with paclitaxel-coated devices) study were presented as late-breaking clinical research at the Society for Cardiovascular Angiography & Interventions (SCAI) 2022 Scientific Sessions (19–22 May, Atlanta, USA).
Shockwave Medical announced that long-term data from the Disrupt PAD III trial found that superior vessel preparation with intravascular lithotripsy (IVL) led to excellent long-term outcomes out to two years with preservation of future treatment options compared to percutaneous transluminal angioplasty (PTA) in the treatment of calcified peripheral arterial disease (PAD).
The new addition to Micromate makes it possible for physicians to rely on pre- and intraoperative scans to plan the intervention, the company behind the robot Interventional Systems, announced in a press release. These planning capabilities can then be leveraged to navigate and guide instruments to the trajectory automatically with submillimetre accuracy.
Interventional Systems recently announced a new collaboration with Johns Hopkins University (Baltimore, USA) in a company press release. The research team at Johns Hopkins, led by Axel Krieger and Lidia Al-Zogbi, will not only investigate ways to improve the Micromate system but leverage the platform nature of the robot and identify new anatomical locations or applications, whose accuracy or safety issues could be addressed by using a robot.
Boston Scientific has received US Food and Drug Administration (FDA) 510(k) clearance for the EMBOLD Fibered Detachable Coil, which is indicated to obstruct or reduce the rate of blood flow in the peripheral vasculature. The first procedure using the device was performed recently at the University of Alabama (Birmingham, USA).
CLS Americas announced it will debut its office-based, magnetic resonance (MR)/ultrasound (US) fusion-guided, TRANBERG Thermal Therapy System for high-precision focal laser ablation of soft tissue, such as prostate cancer tumours, at the American Urological Association (AUA) 2022 Conference (May 13–16, New Orleans, USA).
Germany-based endovascular simulator supplier CATHI has joined forces with UK-based Vascular Simulation Solutions (VSS) to offer the world’s first online training masterclass using endovascular simulation coupled to a structured curriculum, the company said in a press release.
TriSalus Life Sciences announced the enrolment of the first patient in its Pressure-Enabled Regional Immuno-Oncology (PERIO-02) clinical study in a press release.
‘Surface lead contamination on personal lead radiologic protective apparel’ is a recent report published by Kieran Murphy et al (Toronto Western Hospital, Toronto, Canada). The subject of the report is free lead dust on lead aprons: the study involved testing aprons at a Toronto university hospital, which yielded the finding that 60% of aprons and thyroid shields have free surface lead. Murphy et al draw on their results to make recommendations for addressing this professional occupational health issue. The contents of the report will be presented at the Society of Interventional Radiology (SIR) 2022 Annual Scientific Meeting (11–16 June, Boston, USA).
The purpose of the study, the authors outline in their abstract, was to evaluate the extent of surface lead dust contamination on lead radiation protection apparel (RPA) used in Toronto-based university teaching hospital radiology departments. They then compared these results with those from pre-existing reports that point towards lead RPA being a biohazard in and of itself, despite its crucial role in protecting radiologists and other technicians during diagnostic and interventional procedures.
Murphy et al state having surveyed a convenience sample of RPA, which was kept mounted on the wall outside the angiography and emergency departments. As part of the sampling, the team recorded the following information about each specimen: lead equivalency, manufacturer, quality of lead, year of purchase and product type (i.e. lead apron, thyroid collar, or garments combining the two). A combination of visual inspection, fluoroscopy and the use of LeadCheck rapid testing was used to assess both the condition of the RPA and the extent of surface lead contamination.
Of the 69 RPA items surveyed, one failed a radiological quality inspection check, and eight items were in poor condition—the majority of all garments were over five years old and made from a lead/tin-composite material that had a 0.5mm lead equivalency. The authors also break down the RPA items in the report by their type: lead aprons (n=11); lead aprons with thyroid collars (n=25); and separate thyroid collars (n=8). The key finding is as follows: “The overall prevalence of surface lead contamination on RPA surfaces based on LeadCheck sampling was 60.9% (95% confidence interval [CI]: 49.1%, 71.5%). Surface lead contamination was significantly (p=0.0035) higher on thyroid collars (78.8% [95% CI: 62.2%, 89.3%]) than on lead aprons (44.4% [95% CI: 29.5%, 60.4%]).”
Murphy et al then proceed to discuss the significance of their own clinical findings, drawing the conclusion that they support what previous studies conducted in the USA, Europe, Taiwan and Canada have shown: surface lead dust is “[highly prevalent]” in radiology departments. Two studies referenced in the authors’ report went as far as to look at the potential toxicity of lead dust exposure, sampling blood and hair. On the basis of the sum of these investigations (which found the presence of lead in the technologists’ hair, thus indicating ingestion risk), the authors make recommendations for improving conditions for the continued use of lead RPA, in order to reduce risk to personnel wearing the garments.
Firstly, the authors highlight that their recommendations are all the more necessary as there are no current regulations in place to mandate risk assessment for lead exposure from RPA in workplaces with radiation exposure. Moreover, Murphy et al underline that all the RPA they surveyed had passed radiologic quality control tests, but that this does not preclude the presence of surface lead dust. The conclusion from this is that “stringent protocols” must be formulated and followed in terms of cleaning RPA, as well as the shielding structures made of lead. In addition, the authors accentuate the importance of further studies into the toxicity impact of long-term lead exposure among personnel.
Alongside their recommendations, the authors draw attention to the limitations of their investigation, which evaluated “only a small sample of lead aprons and thyroid collars for surface lead dust contamination at a single institution.” They also point to the inexpensive LeadCheck test as yielding less reliable results than may have been achieved with other methods. Murphy et al add to the limitations the fact that the RPA they surveyed was made exclusively of a lead composite material; for this reason, they suggest that their results may not be wholly applicable to solid lead RPA. Lastly, they acknowledge that, when comparing their results with previous studies’, they may not have included all relevant literature, leading to potential omission of key findings which could have produced a different conclusion.
A final note from the authors in their report is that “there is no established safe level of lead” and, therefore, surface lead dust contamination should be continuously monitored where RPA and lead room shields are being used. Likewise, personnel and those responsible for workplace risk assessment should be aware of any defective equipment which may need to be taken out of use to reduce exposure to lead dust.
“I do not want interventional radiology to be a treatment for the rich, nor for those who live in the wealthiest countries.” Yasuaki Arai is an interventional radiologist who was, until recently, executive advisor to the president at Japan’s National Cancer Center in Tokyo, where he is currently a member of the interventional radiology centre. He founded the Japan Interventional Radiology in Oncology Study Group (JIVROSG) and is a prolific physician-inventor, including of the tip-deflecting microcatheter. He answers some of Interventional News’ questions.
What attracted you to a career in interventional radiology (IR)?
IR attracted me because it was an area where I knew that my enthusiasm, skills, ideas and efforts could improve patient distress directly and quickly. No other medical specialty ever really appealed to me as much, but prior to deciding to become a doctor, I did think I would like to be a chef.
Who are, or were, your mentors?
When I started in IR, the specialty did not exist in Japan yet. So, I did not have a mentor. I learned angiography from a book, but I did the rest while thinking for myself. For me, my patients may have been a kind of mentor, as it was their conditions and also the patients themselves that would tell me whether the procedure I had done was right or wrong, good or not so good for them.
Could you describe a particularly memorable case of yours?
Selecting one case is not easy, but doing novel procedures that no one anywhere in the world has done before is always memorable. For example, the implantation of a catheter and port system via the left subclavian artery for hepatic arterial infusion chemotherapy; extra-anatomical shunt creation between the hepatic vein and the ascites cavity, the portal vein and the splenic vein, between biliary
trees, and so on.
You founded the JIVROSG: what prompted you to set this group up?
I learned the importance of clinical trials and evidence in discussion with medical oncologists when I presented the results of hepatic arterial infusion chemotherapy for liver metastasis at a conference. It was one of the international conferences of loco-regional treatment that took place during the 80s in Europe. The oncologists I met taught me that randomised controlled trials (RCTs) are necessary for proper scientific evaluation of emerging treatments. It made sense to me then that conducting clinical trials and presenting evidence is something that we should be doing in Japan too.
And what are some of the most exciting findings to come out of the JIVROSG?
There are two purposes of JIVROSG clinical trials. One is to answer clinical questions in IR. Another is to be able to use evidence to obtain approval for IR devices that, until that point, did not have sufficient evidence to support approval. In the case of the former, the positive results of an RCT of palliative IR procedures such as percutaneous vertebroplasty for painful bone metastases and percutaneous transoesophageal gastric tubing (PTEG) to relieve patients of the pain associated with standard nasogastric tubes were very exciting. An example of an exciting finding of the latter variety was a clinical trial of conventional transarterial chemoembolization (cTACE) for hepatocellular carcinoma (HCC) in collaboration with scientists in South Korea. With this clinical trial, lipiodol for TACE was approved in Japan, and then approved all over the world. Similarly, a clinical trial of the liquid embolic material N-butyl 2-cyanoacrylate (NBCA) is due to be approved in Japan. We hope it will go on to have an even wider-reaching impact on the world of IR.
What are the most challenging aspects of using IR techniques to diagnose and treat cancers?
Progress in IR happens at a rapid pace and sometimes this is even too fast for the evidence to be recognised by physicians outside of IR. As a result, sometimes IR procedures are not recommended, even when the patient is a good candidate for IR treatment. This is probably one of the most challenging aspects of using IR to diagnose and treat cancers. We will need to put in continual effort to make IR a standard treatment in modern medicine.
You have been involved in research and development to bring a number of medical devices to market such as the implantable port and the tip-deflecting microcatheter. What is an example of a cutting-edge device that is currently transforming how you treat patients in your field?
There are many fascinating, unsolved problems. Of most interest to me is how we treat stenotic lesions of the small intestine. With advances in endoscopy, the gastrointestinal tract and bile ducts are becoming less the domain of the interventional radiologist, and more the field of endoscopists. However, the small intestine, which the endoscope cannot reach, remains the realm of IR. I hope to establish techniques and devices to treat stenotic lesions of the small intestine percutaneously.
As former executive advisor to the president at Japan’s National Cancer Center, what are your hopes for the future of interventional radiology in oncology?
The recent progress of systemic medical treatments with molecular target agents and immunotherapies is tremendous. However, I feel that the importance of regional treatments such as surgery, radiation therapy and IR are sometimes forgotten about. There are not many cancers that can be completely treated with systemic medical therapy alone. So, I think it is very important to work on establishing guidelines for the appropriate combinations of systemic therapy and IR for particular types of patients. I hope that IR will, before too long, be recognised as one of the undisputed standard therapies in oncology.
You were named a distinguished fellow at Cardiovascular and Interventional Society of Europe (CIRSE) 2017. What would you like to see the 2022 meeting’s programme include?
Unfortunately, there is a big gap within the world of IR, not only between IR and other specialties. It is the gap between the economically rich and less rich countries. The progress of IR is great, but the costs involved are also growing rapidly. I do not want IR to be a treatment for the rich, or those who live in the wealthiest countries. I think it is very important to enable patients who live in poorer countries to be treated with IR. It will not be easy, but it would be great if we could start discussing how we go about bringing ‘cheaper IR’ into worldwide medical practice.
This year, the Japanese Society of Interventional Radiology (JSIR), the Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR), and the International Symposium of Interventional Radiology (ISIR) are holding a joint meeting. What are the most common issues facing IR in the widespread geographical region that is Asia and the Pacific?
The area of Asia is very large, and the economic situation, medical systems and social attitudes are very different country to country. So, the biggest problem with IR in Asia is that it is difficult to all come together as professionals working in diverse countries to make unified recommendations or establish common practices. However, more IR doctors than ever before will participate in APSCVIR 2022, which is a step in the right direction. Also, APSCVIR has been playing a central role in promoting educational programmes through webinars, and this has allowed IR professionals to share ideas and practices across geographical, cultural and economic borders.
What are your hobbies and interests outside of medicine?
Mountain climbing, playing music and cooking are some of my favourite pursuits. Mountain climbing and cooking are similar to IR, because I must make decisions quickly in order to achieve the best results; the results will clearly reveal whether my decision was a good one or not. As for music, I perform in a live ‘Beatles Night’ concert with professional musicians every four months. I play bass, piano and do vocals, and I think that music is more difficult than my work as an IR.
The first patient has been enrolled in the US Food and Drug Administration (FDA) investigational device exemption (IDE) below-the-knee (BTK) SELUTION4BTK clinical trial involving SELUTION SLR, MedAlliance’s sirolimus-eluting balloon.
Michael Lichtenberg, chief of the angiology department at the Klinikum Hochsauerland (Arnsberg, Germany), said: “I am excited to begin an important trial which will establish the evidence that this novel technology benefit patients suffering from critical limb threatening ischaemia (CLTI).
“So far nothing has worked consistently in this patient population. The early clinical data from SELUTION SLR registries are encouraging and I have seen the performance of this new technology in my routine work. This study is designed to prove that SELUTION SLR is more effective than the current standard of care in this difficult patient population”.
The start of enrolment in the study follows IDE approval in the US one week ago. The BTK indication for SELUTION SLR was granted breakthrough device designation by the FDA in 2019.
The aim of the SELUTION4BTK clinical trial is to demonstrate the superior efficacy and equivalent safety of SELUTION SLR compared to plain (uncoated) balloon angioplasty (POBA) in the treatment of BTK arteries in CLTI patients. The trial is a prospective, multicentre, single blinded, randomised study.
A total of 377 patients will be randomised 1:1 to either SELUTION SLR or the control. According to MedAlliance, this is the first study of its kind where real-world patients with critical limb ischaemia can be included. Patients are being enrolled at approximately 40 sites across the US, Europe and Asia.
“I am very proud of the MedAlliance team which has been able to initiate this study so quickly and have the first patient enrolled only a week after receiving IDE approval”, added Jeffrey Jump, MedAlliance chairman and CEO. “This is a great achievement and a major milestone for MedAlliance.”
SELUTION SLR was awarded CE Mark approval for the treatment of peripheral artery disease in February 2020 and for the treatment of coronary artery disease in May 2020. The US FDA has awarded SELUTION SLR with four breakthrough designations: for the treatment of atherosclerotic lesions in native coronary arteries; coronary in-stent restenosis; peripheral below-the-knee and AV-Fistula indications.
Arjo has announced the development of a new intraoperative Doppler system that includes a single-use, sterile intraoperative probe and Dopplex DMX Vascular Doppler.
This latest system provides immediate evidence of a successful vascular reconstructive procedure by capturing the bloodflow waveforms with the surgical probe and displaying it on the high-resolution colour display of the DMX Doppler, say Arjo, adding that the Doppler results can then be stored on the micro SD card for later review or transfer to a computer.
The company add that bloodflow sound is also improved with the Dynamic Digital Noise Reduction (DDNR) system that eliminates background noise when moving the probe. The probe is single-use and provided sterile to reduce the risk of infection during surgery. By providing quality assurance of blood flow intraoperatively, time and costs of a potential re-operation can be avoided and ischemic time can be significantly reduced. The Dopplex single-use intraoperative probe and DMX Doppler can assist in the performance of safe surgery, it claims.
Simon Larsen, managing director of Arjo, said: “Quality control is vitally important in performing surgery, if secondary intervention and re-operation are to be avoided. Our Dopplex Single Use Intraoperative system enables surgeons to perform an Intraoperative Doppler ultrasound assessment with sound and waveform display and allows for storage in the Electronic Medical Records for documentation. The system brings high level quality assurance to patients and healthcare providers.”
Cardio Flow has announced it recently received US Food and Drug Administration (FDA) clearance for the company’s FreedomFlow peripheral guidewire.
According to a company press release, the FreedomFlow guidewire features a stainless steel core-to-tip design with a fixed distal-spring coil which was developed to provide support for diagnostic and therapeutic devices used in treating plaque blockages in arteries both above and below the knee.
The newguidewire features a silicone-coated spring coil along with a silicone coating on the distal 200cm that eases the crossing of difficult blockages, the release adds. Furthermore, it states that the 0.014-inch core-to-tip design provides interventionists superior torque transmission and precise control when delivering therapeutic devices.
Cardio Flow has also revealed that Jihad Mustapha (Advanced Cardiac & Vascular Centers for Amputation Prevention, Grand Rapids, USA) recently completed the first commercial case with the new guidewire on a patient presenting with complex multi-vessel disease with blockages below the knee, requiring a pedal loop.
Mustapha was impressed with the trackability and versatility of the FreedomFlow guidewire, the company reports, noting, “I was able to deliver three PTA [percutaneous transluminal angioplasty] balloons, one IVUS [intravascular ultrasound] catheter, and a therapeutic device across the single guidewire—all glided easily along the FreedomFlow wire. This new product has the potential to save time and costs in the endovascular lab, given its versatility in crossing occlusions and ability to deliver multiple interventional devices on a single guidewire.”
Outlining Adept Medical’s process for identifying and solving ergonomic issues in the cath lab.
With technological advancements over the last 10 years rapidly changing the scope of atrial treatment, radial has quickly become the access point of choice for clinicians globally. Between 2011 and 2018, radial access adoption for diagnostic angiograms increased from 17.5% to 60.4%, and from 14% to 51.8% for percutaneous coronary intervention (PCI) procedures¹, and this trend is set to rise.
This change of technique has led to clinicians having to adapt the interventional lab environment, making improvements to patient set-up for the radial approach, protecting the clinician, and considering workspace ergonomics. As designers of advanced patient supports, Adept Medical has been collaborating with industry-leading experts to address identified needs in improving the interventional lab working environment.
Adept Medical first launched the STARBoard as part of the STARSystem in 2013. After seeing the need for a device to facilitate ease of radial access during interventional cardiology procedures, the company developed a solution alongside experts in the interventional cardiology field, allowing for quick, effective presentation of the patient’s wrist for radial access. Since its launch in 2013, Adept Medical has successfully placed upwards of 2,600 units of the STARBoard in market globally and experienced a positive uptake for a device to provide ongoing procedural repeatability in the cath lab.
After surveying existing users, spanning from New Zealand to the UK, Adept Medical has gathered insight into the benefits the STARSystem has provided clinicians in the cath lab, when compared to their previous way of working.
The Adept Medical STARSystem offers an ergonomic procedural position for the safe wire/device manipulation
Wire/device manipulation and security
When first witnessing procedures without a device to manage radial access, Adept Medical noticed that often the equipment and wires would be placed over the patient, causing concern of the wires kinking during advancement, or dislodgement of wires from the access site completely. When using the Adept Medical STARSystem, clinicians can easily position and place the wire for ease of manipulation on the work surface of the STARTable.
In a recent study, completed by Adept Medical, the company found that users of the STARSystem had an 87% satisfaction rate with the ergonomic procedural position of wire/device manipulation and an 83% satisfaction rate with wire/device security when using the STARSystem, compared to not using it.
Ergonomic procedural position for the clinician
Without correct positioning of the patient, the clinician is often left having to bend over to gain radial access and complete wire manipulation, particularly in instances when left-arm access is required. Using a rigid arm board or rolled towels offers little flexibility when considering patient management, and often leaves the clinician restricted in movement throughout the procedure.
The STARSystem has been designed to improve the clinician’s posture by having a rotatable arm board that can be positioned correctly to their working preferences. The left arm support allows radial access to be gained on the left-hand side, with the patient’s arm then able to be draped across the abdomen so the clinician can continue to work as normal on the right-hand side. This allows for better working ergonomics for the clinician, eliminating the need of having to bend over the patient and consequently causing back issues.
In a recent study conducted by Adept Medical, it was discovered that users of the STARSystem have an 81% satisfaction rate in the ergonomic procedural position of back straightness using the device, compared to when not using it.
The Adept Medical STARSystem handle design provides reassurance for the patient, limiting movement during radial access procedures
Managing patient restlessness and movement
During procedures where the patient is under conscious sedation, the risk of restlessness and movement is a concern for clinicians who manage patient safety and imaging outcomes.
After understanding the requirements of the clinician, Adept Medical noticed that patients often need a security reminder to avoid excess restlessness and movement. The handle design of the STARSystem allows the patient to grip an object which provides reassurance throughout the procedure and therefore limits movement compared to not using any methods of patient security. The concaved channel also assists with forearm containment preventing it rolling sideways.
In Adept Medical’s recent study, the company found that clinicians had a 81% satisfaction rate in the STARSystem’s ability to control patient restlessness and movement when compared to their previous method.
Gaining hyperextension of the wrist for access
One of the STARSystem’s key features is its ability to present the patient’s wrist quickly and effectively for proximal radial access when hyperextension is required for ease of puncture. The STARSystem handle is designed to be manipulated to rotate the patient’s wrist from a medially rotated position to a hyperextended position, allowing the radial artery to be presented for puncture. This can often be a cumbersome process without having the degree of manipulation and rotation that the STARSystem provides.
In Adept Medical’s recent study, clinicians had an 85% satisfaction rate in the STARSystem’s ability to hyperextend the patient’s wrist using the device, when compared to their previous method.
Product set-up time when performing left and right arm radial access
Having to create custom solutions for each procedure to set the patient up for radial access is less than ideal. Rolling towels for support, or taping patients to homemade arm boards is a lengthy process for the clinical team, affecting the time to set-up and procedural repeatability. These solutions offer less procedural flexibility, which can also cause delays in gaining access to begin the procedure.
The length of the STARSystem adapts to each patient’s size once they grip the handle. Adept Medical designed the STARBoard to allow for multiple levels of adaptability to comfortably suit most patient sizes.
Clinicians in Adept Medical’s study rated their level of satisfaction with product set-up time when performing right arm and left arm radial approach at 77% and 75% respectively using the STARSystem compared to their previous method.
The Adept Medical STARSystem presents the patient’s wrist effectively for proximal radial access when hyperextension is required for puncture
The solution
Adept Medical’s development journey of designing a complete radial solution for left and right access has been one derived from strong clinical input. With Adept Medical adopting a solution when radial access was first gaining traction, it allowed the company to understand pain points and offer benefits to a technique that was novel for many clinicians.
According to the company, its findings show that the STARSystem forms a complete and effective ergonomic solution that offers benefits to the clinician during radial access for both patient management and clinician workflow and comfort.
All of Adept Medical’s patient positioning equipment and operator supports are proudly designed and manufactured at the company’s site in New Zealand.
References:
1. Doll, J, Beaver, K, Naranjo, D, et al. 2022. Trends in Arterial Access Site Selection and Bleeding Outcomes Following Coronary Procedures, 2011–2018. Circulation: Cardiovascular Quality and Outcomes.
Global Embolization Oncology Symposium Technologies (GEST; 19–22 May, New York, USA) provided delegates and faculty alike with the opportunity to hear about worldwide approaches to hepatocellular carcinoma (HCC) treatment. The dedicated session comprised discussion of various curative-intent therapies, how to define this as a concept, and how the scope of it might be expanded beyond that which achieves recurrence-free survival. A key takeaway from the session was that the next generation of interventional radiologists hold radiation segmentectomy in high regard, with its advantages now playing out in the form of clinical data.
The session began with Donna D’Souza’s (University of Minnesota, Minneapolis, USA) presentation titled ‘(Thermal) ablation is the only curative-intent therapy for early-stage HCC’. However, she immediately offered the disclaimer that, in reality, she does not believe that it is the only way to treat with curative intent, especially now that we are in “the era of radiation segmentectomy”. Robert Lewandowski (Northwestern University, Chicago, USA) followed on the subject of the latter.
D’Souza started by explaining that the updated 2022 Barcelona Clinic Liver Cancer (BCLC) guidelines still recommend ablation for unresectable, small HCC, with the new addition of transarterial chemoembolization (TACE) or radioembolization as a second-line therapy if ablation is not feasible.
Regarding the definition of ‘curative-intent’, D’Souza described it based on a comparison with surgical resection, which is widely viewed as “the gold standard” for curative-intent therapy for HCC. She elaborated that the rate of complete pathologic necrosis (CPN) after ablation is also of importance in determining local cure rates.
D’Souza proceeded to detail recent data, including randomised controlled trial data out of Hong Kong, which allocated 109 patients to surgical resection and 109 to radiofrequency ablation (RFA). The paper, published in 2017, comprised data gathered over a median follow-up period of 7.7 years, and showed no difference in local recurrence rate, disease-free survival, and survival to 10 years, between ablation and resection, even for larger lesions. D’Souza highlighted the significance of these findings: “traditionally, surgery outperforms ablation for lesions between three and 5cm”. Moreover, the SURF randomised controlled trial, of which some of the results were published in 2021, demonstrated that there was, again, no difference in recurrence-free survival, nor overall survival, at five years.
In conclusion, D’Souza underlined how “ablation is the most evidence-based curative-intent treatment modality for HCC for interventional radiologists”, and also highlighted the high complete pathologic necrosis rates that have been achieved in
recent studies.
Lewandowski then pivoted to explore the curative-intent capacity of ablative, segmental transarterial radioembolization (TARE), using the case of a 95-year-old female who survived two years after undergoing ablative radiation segmentectomy for HCC. Lewandowski explained that the definition of ‘curative intent’ can and should be expanded beyond its current status: achieving a comparable degree of CPN to surgical resection. The implications of a broader scope of the term could be that it comes to encompass treatments that facilitate bridging or downstaging to transplant, namely TARE.
Lewandowski emphasised the role of dosimetry, citing his awareness of threshold doses: targeting HCC with 190 Gray sees almost three times the rate of CPN when compared to lower doses, and targeting a threshold dose of 400 Gray has yielded 100% CPN explant in a retrospective study.
Finally, given the opportunity to field questions from the audience and each other, the panel touched on cryoablation and its performance relative to that of thermal ablation. “There are some pretty good data out there showing that it is effective [and can] outperform RFA,” D’Souza outlined. She also responded to Lewandowski on the topic of SBRT: “in some centres it is becoming more common,” while the existing literature still favours RFA. Panel moderator Nadine Abi-Jaoudeh (University of California Irvine, Irvine, USA) corroborated D’Souza’s “last-resort” approach to using SBRT, but made the point that “younger radiation oncologists are excited about the therapy’s potential.”
Medtronic has announced approval from the US Food and Drug Administration (FDA) for the IN.PACT 018 paclitaxel-coated percutaneous transluminal angioplasty (PTA) balloon catheter, a drug-coated balloon (DCB), indicated for the interventional treatment of peripheral arterial disease (PAD) in the superficial femoral and popliteal arteries.
“The IN.PACT 018 DCB will allow physicians to better address challenging cases, such as those with narrow lesions or complex anatomies,” said Prakash Krishnan (Icahn School of Medicine at Mount Sinai, New York, USA), who also serves on a scientific advisory board for Medtronic. “The available long-term data [from the IN.PACT Admiral studies] on its benefits gives physicians another effective treatment for PAD in complex anatomies.”
The IN.PACT 018 DCB uses the same drug coating formulation and is built upon equivalent technology to the IN.PACT Admiral DCB, which is compatible with 0.035” guidewires. The IN.PACT 018 DCB is indicated for PTA of de novo, restenotic, or in-stent restenotic lesions with lengths up to 360 mm with vessel diameters of 4‒7 mm. It is engineered to cross tight lesions, provide better deliverability and is compatible with 0.018″ guidewires, Medtronic states in a press release.
The IN.PACT 018 DCB will be the only commercially available DCB with a 200cm over-the-wire (OTW) catheter length, providing physicians the option to treat via femoral or radial access. This is in addition to the to the 130 cm OTW catheter length.
“Medtronic is committed to offering physicians a suite of products to treat patients with PAD. Based on feedback from our clinical community and the need for an 018” guidewire compatible DCB, Medtronic is excited to bring this technology to market in the U.S,” said David Moeller, president of the Peripheral Vascular Health Operating Unit at Medtronic. “The addition of the IN.PACT 018 DCB further reinforces Medtronic’s commitment to being the market leader in drug-coated balloons.”
MedAlliance’s Selution SLR drug-eluting balloon (DEB) has received investigational device exemption (IDE) approval from the US Food and Drug Administration, making it the first limus DEB to be available to US patients, the company announced in a press release.
The Selution SLR (sustained limus release) is a novel sirolimus-eluting balloon that provides a controlled sustained drug release, similar to a drug-eluting stent (DES). The device was granted breakthrough device designation by the FDA in March 2019 and further in September 2019 for below-the-knee (BTK) indications in peripheral artery disease.
“This is a major milestone for MedAlliance,” the company states in its press release. MedAlliance has announced it will begin enrolment in the below-the-knee (BTK) IDE randomised clinical trial (RCT) SELUTION4BTK immediately outside of the US and early this summer in US centres. Principal investigators of the study are Ehrin Armstrong (Adventist Heart and Vascular Institute, St Helena, USA), Marianne Brodmann (Medical University of Graz, Division of Angiology, Austria), and Tjun Tang (Singapore General Hospital, Singapore).
Selution SLR was awarded CE mark approval for the treatment of peripheral artery disease in February 2020. The device has shown early promising clinical results in treatment of patients with chronic limb threating ischemia (CLTI) and below-the-knee artery disease.
In the PRESTIGE study which was presented as a late breaking trial at VIVA 2021 (5–7 October, Las Vegas, USA) by Tang, use of Selution SLR in complex BTK lesions resulted in sustained safety and efficacy outcomes out to 18 months. An additional 75 patients with BTK disease and Selution SLR treatment have been studied in the PRISTINE registry and the results are scheduled to be presented at LINC 2022 (6–9 June, Leipzig, Germany).
Based on the early data following the use of Selution SLR in treatment of BTK disease, MedAlliance has moved forward with the design of the SELUTION4BTK RCT to further investigate the safety and efficacy of this device and prepare for US FDA approval.
Selution SLR’s technology involves unique MicroReservoirs made from biodegradable polymer intermixed with the anti-restenotic drug sirolimus. These MicroReservoirs provide controlled and sustained limus release (SLR) of the drug. Extended release of sirolimus from stents has been demonstrated highly efficacious in both coronary and peripheral vasculatures.
MedAlliance’s proprietary CAT (cell adherent technology) enables the MicroReservoirs to be coated onto balloons and adhered to the vessel lumen when delivered via an angioplasty balloon.
Selution SLR is available in Europe and all other countries where the CE mark is recognised.
VentureMed Group recently announced that it has completed enrolment of a randomised controlled trial (RCT) titled ‘Flex Vessel Prep prior to PTA for the treatment of obstructive lesions in the native AVF’. This RCT was conducted to assess primary patency at six months when using Flex Vessel Prep system prior to percutaneous transluminal angioplasty (PTA) versus PTA alone for the treatment of obstructive lesions of native arteriovenous fistulas (AVFs) in the upper extremity.
The FLEX RCT was a prospective, multicentre, randomised study conducted in seven sites across the USA. Seventy-five patients were enrolled and includes 30-day, three-month, and six-month follow-up.
“Although fistula are the preferred access for haemodialysis, fistula dysfunction and failure remains a significant issue in AV dialysis access care. Balloon angioplasty considered the gold standard by most, still has its limitations due to the resistant and recurrent nature of these hyperplasic lesions, often requiring the use of high-pressure balloons,” said Sanford Altman (Open Access Vascular Access, Miami, USA). “These high-pressure balloon treatments can cause vessel wall damage accelerating restenosis and shortening the time between interventions. By utilising the Flex Vessel Prep prior to angioplasty, we are hoping to see improved vessel compliance, reducing the need for high-pressure balloons while reducing the barotrauma to the vessel wall thereby extending the primary patency and time between interventions.”
“This RCT builds upon the rich and diverse data we are gathering for the Flex system. The rapid enrolment of these 75 patients at seven US centres during a COVID-19 surge is encouraging”, said Denis Harrington, president and chief executive officer of the VentureMed Group. “We are excited to report our previous study, the FLEX AV Registry, will be presented at the VASA 2022 Symposium (6–9 June,Charleston, USA). 2022 is becoming a very impressive year for Flex Vessel Prep”.
Shockwave Medical and Genesis MedTech Group announced today that they have successfully obtained approval from China’s National Medical Products Administration (NMPA) to market and sell the Shockwave intravascular lithotripsy (IVL) system with the Shockwave C2 coronary IVL catheters and the Shockwave M5 and S4 peripheral IVL catheters in China.
A joint venture between Genesis MedTech and Shockwave was formed in March of 2021 as a partnership to distribute Shockwave’s products in China and to leverage Genesis MedTech’s Wuxi research and development and production base to accelerate the manufacturing of Shockwave’s products for the local Chinese market.
The Shockwave M5 and S4 IVL catheters, which are used for the treatment of peripheral arterial calcification lesions, are approved in the USA, the European Union, and other select international jurisdictions and have been used to help treat more than 50,000 patients globally who suffer from peripheral arterial disease (PAD). The Shockwave C2 coronary IVL catheters, which are used for the treatment of coronary arterial calcification lesions, are approved in the USA, the European Union, and other select international jurisdictions, and have been used to help treat more than 70,000 patients globally who suffer from coronary artery disease.
In July 2021, Yundai Chen of the Chinese People’s Liberation Army General Hospital (Beijing, China) led a team to perform the first clinical IVL procedure in China to treat a patient with severely calcified coronary artery lesions. “Shockwave IVL technology is an innovative solution for treating coronary artery calcification, especially when the calcium is deep in the artery. The technology is easy to use, which is good for increasing access,” commented Chen.
In August of 2021, Weiguo Fu and Zhihui Dong, both of Zhongshan Hospital (affiliated to Fudan University, Shanghai, China) led their team to successfully complete the first clinical IVL procedure in China on severely calcified lesions in peripheral arteries. Fu said: “Shockwave IVL provides a powerful solution to calcified lesions that could not be effectively treated in the past. It is a promising and indispensable approach for the future.”
With an ageing population, there is an increasing incidence of calcified vascular disease in China. According to the Chinese Expert Consensus on the Diagnosis and Treatment of Calcific Coronary Lesions 2021 (Expert Consensus Statement 2021), the risk of developing coronary artery calcification increases with age, with an incidence rate of about 50% in people aged 40–49 years and about 80% in people aged 60–69 years. Calcification is also a common problem in patients with PAD. According to Statistica, China had a population of over 1.4 billion in 2020, 50% of whom were over the age of 40.
“Approval in China represents another milestone in the international expansion for Shockwave’s IVL technology. We are very appreciative of the work and the quick regulatory approval by the NMPA—despite the difficult conditions in China in the past months—and its recognition of IVL’s clinical value for patients in China,” said Doug Godshall, chief executive officer of Shockwave Medical. “Genesis MedTech is a perfect partner for Shockwave in China and this accomplishment underscores the value of their established infrastructure and local relationships. We look forward to our continued relationship as we bring IVL to physicians and patients in China for treatment of arterial calcification.
Adept Medical says it has responded to the call from interventional radiologists for a device to comfortably support and manage a patient in the prone position with the launch of its new Prone Support solution, which will be available from 23 May 2022.
The Prone Support is the ideal solution for supporting and managing a prone patient, providing comfortable patient positioning during C-arm image-guided procedures, according to Adept. It is a versatile device designed to support a patient in the prone position for multiple procedure types and is stably held for the duration of a procedure by the patient’s weight.
“Optimal patient positioning is one of the key steps for a successful procedure. The Adept Medical Prone Support allows for a posterior approach for imaging-based diagnostic and guided interventional procedures. We worked closely with local interventional radiologists and other medical professionals to develop a product that allows for a consistent and comfortable patient experience. A driving goal was to produce a solution that maintains the balance of simplicity and complexity when providing functional adjustability that could accommodate a wide range of patients. We believe the Adept Medical Prone Support will be very well-received and become the state-of-the-art device for prone patient positioning,” said James Kember, lead product design engineer, Adept.
The arm supporting surface is cantilevered out from the imaging table, accommodating a variety of patient sizes and mobility ranges comfortably. The elevated cushioned face support provides additional comfort with clearance through the centre to reduce any anxiety experienced from being contained and providing space for nasal oxygen prongs.
The head-supporting assembly can also be removed completely to suit specific patient or case needs, according to Adept. The Prone Support can be simply placed underneath the mattress using the baseboard design, allowing for efficient set-up and removal on most C-arm imaging tables.
New long-term data from the SAFE-PAD (Safety assessment of femoropopliteal endovascular treatment with paclitaxel-coated devices) study were presented today as late-breaking clinical research at the Society for Cardiovascular Angiography & Interventions (SCAI) 2022 Scientific Sessions (19–22 May, Atlanta, USA). The analysis found no meaningful difference in survival between patients treated with a paclitaxel drug-coated device and those treated with a non-drug-coated device for up to six years after the index procedure, regardless of the patient’s mortality risk and device type.
The SAFE-PAD study was created in collaboration with the US Food & Drug Administration (FDA) to evaluate the long-term safety of paclitaxel-coated devices compared with non-paclitaxel-coated devices for femoropopliteal artery revascularisation among a broad, real-world population of patients with peripheral arterial disease (PAD).
The study included Medicare beneficiaries ≥66 years treated with a drug-coated device or non-drug-coated device from 1 April 2015 to 31 December 2018. Non-inferiority between devices was evaluated for mortality through 21 July 2021. A number of prespecified subgroups, including a cohort at the lowest risk of mortality defined as those aged 66–70 with no chronic limb-threatening ischaemia (CLTI) and ≤2 comorbidities, were evaluated.
“Our goal is to give patients the most durable treatment possible that will keep them out of the hospital and living their lives. Patients with PAD tend to be of lower socioeconomic status, more likely to be underserved minority populations and often need to travel long distances or take time off work to seek treatment,” said Eric Secemsky (Beth Israel Deaconess Medical Center, Boston, USA). “Not having access to important treatment options known to reduce the risk of repeat intervention can have a substantial influence on our PAD patients, ultimately impacting their outcomes and quality of life. The findings presented today add to the growing body of evidence showing these devices are safe for use.”
Of 168,553 patients, 70,584 (41.9%) were treated with a drug-coated device. Median follow-up was 3.52 years. The weighted cumulative incidence of mortality at 6.3 years was 63.6% with non-drug-coated devices and 62.5% with drug-coated devices (p<0.0001). Findings were consistent among all subgroups. In particular, there was no difference in risk among those at lowest risk of mortality (n=4,212; weighted hazard ratio [HR], 0.98; 95% confidence interval [CI], 0.87–1.10).
Researchers note that were will future several reports from the SAFE-PAD study with a final report published in the next two years.
Shockwave Medical announced today that long-term data from the Disrupt PAD III trial found that superior vessel preparation with intravascular lithotripsy (IVL) led to excellent long-term outcomes out to two years with preservation of future treatment options compared to percutaneous transluminal angioplasty (PTA) in the treatment of calcified peripheral arterial disease (PAD).
As previously published, IVL at 30 days demonstrated superiority over PTA in the primary endpoint analysis, defined as procedural success with a residual stenosis less than or equal to 30% without flow-limiting dissection, prior to drug-coated balloon (DCB) or stent, with a rate of 65.8% vs. 50.4% (p=0.0065) as determined by an independent angiographic core lab. Additionally, PAD III showed that IVL achieved a reduction in frequency and severity of flow-limiting major dissections (1.4% vs. 6.8%, p=0.03), a reduction in stent implantation rate (4.6% vs. 18.3%, p<0.001) and no distal embolisation or perforation events.
These new long-term results found that the powered secondary endpoint of primary patency (defined as freedom from clinically-driven target lesion revascularisation [CD-TLR], restenosis determined by duplex ultrasound and provisional stenting) favoured IVL over PTA at one year (80.5% vs. 68.0%, p=0.017) and remained favourable through two years (Kaplan-Meier estimate: 74.4% vs. 57.7%, p=0.005), respectively.
“Prior to the PAD III study, there were limited long-term data available to provide treatment guidance for this challenging population since patients with severe calcification have historically been excluded from endovascular trials,” said William Gray (Main Line Health, Wynnewood, USA), co-principal investigator of PAD III who presented the long-term results. “The primary endpoint at 30 days showed IVL to be a superior vessel preparation strategy by demonstrating stenosis resolution with significantly fewer complications including severe dissections and the subsequent need for bailout stent implantation. Avoiding unplanned stent implantations allows interventionalists to preserve all their future treatment options should reintervention be necessary. These new long-term data show that vessel preparation with IVL followed by DCB result in excellent efficacy and durable patency out to two years, and taken together the acute and long-term results reinforce IVL as a preferred vessel preparation strategy for calcified femoropopliteal disease.”
Disrupt PAD III was a prospective, multicentre, randomised study designed to demonstrate the safety and effectiveness of IVL as a vessel preparation procedure in moderate to severely calcified superficial femoral and popliteal lesions, followed by a DCB or stent. The study enrolled 306 patients randomised between IVL and PTA at 45 sites in the USA, Germany, Austria, and New Zealand. In the IVL arm, 82.9% of patients were classified by the angiographic core lab as having severe calcification, with an average calcified lesion length of 129.4mm. Joining Gray as co-principal investigator of the study was Gunnar Tepe (RoMed Clinic Rosenheim, Rosenheim, Germany).
The Royal Australian and New Zealand College of Radiologists (RANZCR) has issued a statement addressing the Australian and global shortage of iodinated contrast media.
The release explains that GE Healthcare—the manufacturer of Omnipaque and Visipaque and the primary supplier of contrast media in Australia—has recently faced supply issues due to the current outbreak of COVID-19 and subsequent lockdown in Shanghai, China, affecting the company’s manufacturing plant.
“RANZCR is liaising with the Therapeutic Goods Administration (TGA), which is seeking alternative supplies of contrast to address the shortfall,” the statement reads, noting that updates can be found on the TGA website.
The release continues: “RANZCR recommends that medical practitioners considering referring a patient for a CT during this time consult with a radiologist for advice on alternative imaging modalities or other strategies that could be used to diagnose and manage their patients.”
In addition, RANZCR communicates that it endorses the recommendations of the American College of Radiologists (ACR) Committee on Drugs and Contrast Media that radiology practices and hospitals implement a range of strategies to conserve current supplies of contrast to manage patient care. These recommendations include “utilise alternative studies to answer the clinical question such as non-contrast CT, MRI with or without gadolinium-based contrast media, ultrasound with or without ultrasound contrast agents, nuclear medicine, or PET-CT, when feasible,” and “look for alternative versions of contrast agents, which may be marketed under a different brand name or intended clinical use”.
Finally, the release notes that RANZCR further endorses the recommendations in the recent article by Joseph Cavallo and Jay Pahade (both Yale School of Medicine, New Haven, USA), titled “Practice management strategies for imaging facilities facing an acute iodinated contrast media shortage” published in the American Journal of Roentgenology, which provides details to support practice management during this contrast shortage.
Late-breaking trial data presented at EuroPCR 2022 (17–20 May, Paris, France) underscore the potential of renal denervation as an adjunctive therapy to treat hypertension, complementing existing first-line treatments including lifestyle modifications and medication, attendees of the conference heard.
Day one of the four-day international interventional cardiology meeting, which has returned to an in-person format in Paris for the first time since 2019, saw the release of data from three clinical studies assessing the use of renal denervation as a treatment for hypertension—the Global Symplicity Registry, SPYRAL HTN-ON MED and an analysis of ultrasound renal denervation from the RADIANCE HTN SOLO and TRIO trial cohorts.
Speaking in a press conference ahead of the presentation of the data, Felix Mahfoud (Saarland University Hospital, Hamburg, Germany) told attendees that renal denervation represents a device-based treatment option to tackle the problem of hypertension.
“Despite all advances in care we still have a significant proportion [of patients] that are either undiagnosed or not sufficiently controlled to target blood pressure, and that holds true for almost all regions and geographies around the world,” he told assembled press, pointing out that the release of the data also coincides with the 2022 World Hypertension Day, which carries an aim to communicate to the public the importance of hypertension and its serious medical complications, and to provide information on prevention, detection and treatment.
“We know from large meta analyses and prospective randomised clinical trials that reducing blood pressure is impactful for patients,” he added. “The problem is not that we do not know that blood pressure is an issue and is serious, the problem is that we have available drugs that work quite well but patients do not like them and patients do not take them.
“There is obviously an unmet need, and renal denervation represents a device-based treatment option to tackle that problem,” he said.
Mahfoud then previewed data to be released later in the day during a hot-line session at EuroPCR, the three-year Global Symplicity Registry results, assessing blood pressure and major adverse cardiovascular events (MACE) after renal denervation using Medtronic’s Symplicity system.
The results show that a 10% time in target range increase in the first 12 months reduces the odds of MACE events in the following 24 months and led to the conclusion that sustained blood pressure reduction after renal denervation predicts a meaningful reduction in clinical events. In this large, global registry, which involved 3,077 patients, those who underwent radiofrequency renal denervation spent a greater amount of time in target blood pressure range and had less cardiovascular events including cardiovascular death, myocardial infarction, and stroke.
The presenter commented that, though the data come with some limitations, they are “encouraging” and show for the first time patients with a higher time in target range have reduced events. “That should convince people that lowering blood pressure with renal denervation translates into improved outcomes,” he remarked.
David Kandzari
Also presenting data during the same EuroPCR session, David Kandzari (Piedmont Heart Institute, Atlanta, USA) offered three-year data from the SPYRAL HTN-ON MED trial, investigating Medtronic’s Symplicity Spyral renal denervation system, giving an overview of the impact of renal denervation on long-term time in target blood pressure range compared with sham control.
Time in target therapeutic range has become an established and validated measure of control for chronic disease conditions, Kandzari said in his presentation, adding that specific to hypertension, time in target range is an independent measure of blood pressure control and is an independent predictor of cardiovascular events.
Kandzari noted that early results from the pilot study showed that patients who underwent renal denervation while on antihypertensive medications had lower blood pressure when compared to the sham control group, the effect of renal denervation on blood pressure burden over time had not been established.
With this latest report, a time in target therapeutic range analysis was performed using data comparing the two groups over three years and showed that the renal denervation and AH group had significantly higher time in target therapeutic range with more time in the blood pressure target range at two and through to three years as compared to the sham group, thus affirming the sustained efficacy of renal denervation over late-term follow-up.
Also presenting alongside Mahfoud and Kandzari, Ajay Kirtane (Columbia University Irving Medical Center/NewYork Presbyterian Hospital, New York, USA) offered findings of a patient-level pooled analysis of ultrasound renal denervation in the RADIANCE HTN SOLO and TRIO trials.
The analysis examined data tracking the use of ultrasound renal denervation using the Paradise (Recor Medical) system in a drug resistant population (three years or more of antihypertensive medications) taken from the RADIANCE-HTN TRIO study, and from RADIANCE-HTN SOLO, in a population with mild to moderate hypertension (controlled on 1-2 antihypertensive medications or uncontrolled on 0-2 medications).
The results of the analysis showed that there was no heterogeneity in effect on blood pressure reduction and medication burden. Those results looking at a mixed population over a six-month period favoured ultrasound renal denervation over the sham population and the pooled analysis of the RADIANCE-HTN trials suggests “the response to ultrasound renal denervation is similar in the presence or absence of medications and consistent across the whole spectrum of hypertension.”
Vivasure Medical has announced the closing of the first tranche of €22 million (US$23 million) as part of its Series D financing round that could reach up to €52 million (US$54 million) in total.
The company states that the financing, led by a multinational strategic corporation, includes an option to buy Vivasure upon certain milestones. Other participants in this Series D financing round include a second strategic corporate investor as well as existing investors, Fountain Healthcare Partners, Orchestra BioMed, LSP Health Economics Fund managed by the EQT Life Sciences team, Panakès Partners and Evonik Venture Capital.
The financing will support the US and European clinical development and regulatory approval of the company’s portfolio of fully absorbable, patch-based large-bore percutaneous vessel closure devices for transcatheter endovascular and cardiovascular procedures, a press release details. These devices include PerQseal and PerQseal+ for arterial closure and PerQseal Blue for venous closure.
Vivasure’s PerQseal technology consists of a proprietary bioabsorbable intravascular patch that seals the vessel from the inside, returning the artery or vein to its natural state without leaving behind the remains of any materials such as collagen, metal implants or sutures commonly used in other closure technologies.
According to Vivasure, the PerQseal device is the first sutureless and fully absorbable synthetic implant for large-bore arterial vessel punctures and is available to physicians in Europe for use in transcatheter endovascular procedures, including transcatheter aortic valve replacement (TAVR), thoracic endovascular aortic repair (TEVAR) and endovascular aneurysm repair (EVAR).
The company communicates that its next-generation PerQseal+ device has an enhanced bioabsorbable patch designed to address more complex patient anatomies and is currently under clinical evaluation in Europe and the USA.
Vivasure is also developing PerQseal Blue, designed exclusively for sutureless and fully absorbable large-bore venous vessel closure following percutaneous cardiovascular procedures, such as transcatheter mitral valve repair or replacement (TMVR), transcatheter tricuspid valve repair or replacement (TTVR) and leadless pacemaker implants. The company claims that, currently, there are no sutureless options available for vessel closure following large-bore venous procedures.
“While tremendous progress has been made for minimally invasive structural heart procedures, vascular issues related to the closure of the procedure remain the most common complication of these interventions,” said Azeem Latib, section head and director of interventional cardiology and director of structural heart interventions at Montefiore Health System (New York, USA). “The novel PerQseal technology is designed to address these shortcomings and has tremendous potential to improve patient outcomes and enhance procedure efficiency.”
Germany-based endovascular simulator supplier CATHI has joined forces with UK-based Vascular Simulation Solutions (VSS) to offer the world’s first online training masterclass using endovascular simulation coupled to a structured curriculum, the company said in a press release.
At its heart is the CATHISsimulator, which is fully functional with all standard software systems including every iOS system and Oculus VR (virtual reality).
The training is supported by a structured curriculum, delivered by specialist endovascular instructors with many years‘ clinical experience. The programme is targeted at specialist trainees in every year of their course, medical students on a condensed course, and interested interventionists. The scope of the package includes endovascular aneurysm repair (EVAR) for carotid, renal, iliac, femoral and tibial artery angioplasties. In addition, the curriculum includes training on emergency vascular cases such as ruptured aneurysms and visceral bleeding and trauma.
“The importance of periodical continuous education, training and structured curricula of interventional procedures has been confirmed by numerous clinical experts around the globe“, noted CATHI managing director of marketing and sales Manuela Werner. “With this joint venture between VSS and our company we are combining top-level expertise with our near-to-reality simulation systems.“
Consultant vascular surgeon Abdullah Jibawi (Ashford and St Peter’s Hospital NHS Foundation Trust, Chertsey, UK), who is involved with delivering the new programme, added: “We have built our curriculum with the end user in mind in every minute detail. We want to answer the real need for training by allowing a layer-by-layer build-up of skills and decision-making […] Our programme introduces the ability to train interventionists over a specified period of time, followed by a customised exposure to a specified product line to fine-tune their experience as needed.“
CLS Americas announced it will debut its office-based, magnetic resonance (MR)/ultrasound (US) fusion-guided, TRANBERG Thermal Therapy System for high-precision focal laser ablation of soft tissue, such as prostate cancer tumours, at the American Urological Association (AUA) 2022 Conference (May 13–16, New Orleans, USA).
The system is designed to work with multiple MR/US fusion image guidance systems for precise and accurate ablation in a minimally invasive setting, while preserving healthy prostate tissue.
“CLS is pleased to introduce its office-based, fusion-guided TRANBERG Thermal Therapy System at this year’s AUA conference,” stated Michael Magnani, president of CLS Americas. “We are commercialising this innovative technology so that patients can benefit from being treated with focal laser ablation in a urology office or clinic instead of a hospital.”
“While treating prostate cancer tumours successfully is the primary goal, some current treatment options expose patients to unacceptably high risks of complications such as erectile dysfunction or urinary incontinence,” said Fernando J Bianco, investigator-in-chief for the Urological Research Network, and principal investigator of the Phase I clinical study running at Urological Research Network, Miami Lakes, USA. “Based on my initial clinical trial experience with the TRANBERG laser, I believe that partial gland fusion ablation provides the precision to successfully treat the cancerous lesions while offering patients a superior side effect profile. The ongoing study will provide us with more information on this.”
Interventional Systems recently announced a new collaboration with Johns Hopkins University (Baltimore, USA) in a company press release. The research team at Johns Hopkins, led by Axel Krieger and Lidia Al-Zogbi, will not only investigate ways to improve the Micromate system but leverage the platform nature of the robot and identify new anatomical locations or applications, whose accuracy or safety issues could be addressed by using a robot.
Johns Hopkins University has always been at the forefront of numerous innovations in robotic-assisted surgery, more recently with the development of a robotic platform capable of performing laparoscopic surgery on the soft tissue of a pig without the guiding hand of a human, on a significant step toward procedure automation.
Through this agreement, Interventional Systems strengthens its strategy of close cooperation with leading academic institutions.
“These partnerships are extremely important for us”, shares Interventional Systems chief product officer Pedro Costa. “They allow the crosspollination of ideas and technologies between the industry and the academy, allowing us to design better, safer, and more innovative products, and brings research and students closer to what is actually happening on the market. This benefits the patient and, ultimately, the entire healthcare system. We are excited to get started and are sure that Interventional Systems will learn immensely throughout this process. We hope we can teach as much”.
A report from the American Venous Forum (AVF) 2022 meeting (23–26 February, Orlando, USA) on the comparative merits and demerits of dedicated and non-dedicated stents heads the list of Interventional News’ April top 10 articles. Some of the other most read pieces include the latest profile on Karim Valji, a conversation with Robert Hinchliffe, and a debate covering some of cancer treatment’s current controversies.
Venous stenting was a hot topic at the recent American Venous Forum (AVF) annual meeting (23–26 February, Orlando, USA). Catching the audience’s attention, Lilian Tran highlighted a head-to-head study of dedicated versus non-dedicated stents.
Medtronic recently voluntarily recalled a subset of its IN.PACT Admiral and IN.PACT AV paclitaxel-coated percutaneous transluminal angioplasty (PTA) balloon catheters due to the potential for pouch damage resulting in a loss of sterility.
Karim Valji is professor of radiology at the University of Washington (Seattle, USA) and professor Emeritus at the University of California, San Diego (USA) and speaks to Interventional News about his career.
Looking ahead to the CX Symposium, (which has now taken place: 26–28 April, London, UK) Robert Hinchliffe (University of Bristol, Bristol, UK) dubs the session on the “hurting leg” a highlight.
Alucent Biomedical announced in a press release that it has enrolled the first patient in ACTIVATE II, an Australia-based first-in-human clinical trial to evaluate the safety and efficacy of its natural vascular scaffolding (AlucentNVS) technology.
Truvic Medical shared via press release that it has received 510(k) clearance from the US Food and Drug Administration (FDA) for the Prodigy thrombectomy system, designed for the treatment of peripheral vascular thrombus.
One of the key takeaways from the debate session at this year’s Society of Interventional Oncology (SIO) meeting (24–28 March, San Francisco, USA) was that radiation oncology has seen much innovation, and that this must continue in order to provide the best outcomes for patients into the future.
Cydar Medical recently announced it has entered a strategic collaboration with Medtronic. Under the pilot arrangement, Cydar’s EV Maps software will be introduced to up to 40 new global sites, combining Cydar’s augmented intelligence technology with Medtronic’s services and case support.
An analysis showed benefit of XARELTO plus aspirin in reducing thrombotic hospitalisations for peripheral arterial disease (PAD) patients with and without chronic kidney disease (CKD).
TriSalus Life Sciences announced the enrolment of the first patient in its Pressure-Enabled Regional Immuno-Oncology (PERIO-02) clinical study in a press release.
The trial is evaluating SD-101, an investigational toll-like receptor 9 (TLR9) agonist, in adults with locally advanced, metastatic, or unresectable hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (ICC). SD-101 will be administered using the Pressure-Enabled Drug Delivery (PEDD) method in combination with systemic checkpoint inhibitors.
Initiated at The University of Texas MD Anderson Cancer Center (Houston, USA) with additional sites anticipated, the study is the second in a series of clinical trials assessing TriSalus’ immunotherapy platform across multiple indications.
The initial trial using this platform, the PERIO-01 study, is actively enrolling and is evaluating the safety of SD-101 administered by PEDD in combination with checkpoint inhibitors in patients with uveal melanoma with liver metastases.
“Patients with advanced HCC or ICC often have limited options when seeking treatment, as checkpoint inhibitors have had some success in these indications but results are not what we want them to be in most cases,” said Steven C Katz, chief medical officer at TriSalus. “The PERIO-02 clinical trial has potential to advance the scientific foundation required to help address this unmet need, deliver new therapies to improve clinical outcomes, and ultimately, give patients a better chance to respond more reliably to different forms of immunotherapy.”
While immunotherapy has yielded significant advances in cancer treatment, unique properties of liver tumours, including immune response suppression and high intratumoral pressure, can prevent optimal delivery and performance of therapeutics and limit the overall effectiveness of immunotherapy for patients with liver cancers.
“With the PERIO-02 trial, we are striving to enable immunotherapy for the most common primary liver tumours,” said Katz. “The study is implementing a multifaceted approach by testing the integration of an immunotherapeutic, SD-101, with a [US Food and Drug Administration]-cleared delivery device, to hopefully induce the type of immune response that we are so eager to see for patients with HCC and ICC.”
The eTrieve catheter for removing blood clots in patients with acute pulmonary embolism
Magneto Thrombectomy Solutions (Magneto), a medical devices company developing thrombectomy solutions for the treatment of ischaemic stroke and pulmonary embolism, presented successful first-in-human (FIH) results showing safety and feasibility of the eTrieve system, a catheter based on electric fields for removing blood clots, in patients with acute pulmonary embolism (PE).
The data, presented at Biomed Israel 2022, the international life science and healthtech conference in Israel (May 10–12, Tel Aviv), showed a significant reduction in right ventricle/left ventricle ratio and alleviation of PE-associated symptoms.
“Magneto provides intermediate and high-risk PE patients with a unique solution for safely and effectively removing large clots blocking the arteries in the lungs,” said Piotr Musialek (John Paul II Hospital, Krakow, Poland) and an investigator in the study. “The combination of a large-diameter ‘vacuum cleaner’ with electro-mechanical thrombus extraction, allows an immediate resolution of dyspnoea and swift recovery of the cardio-respiratory system.”
The prospective, single-arm, multicentre first-in-human study assessed the initial safety and performance of eTrieve in treating patients with acute PE. The study enrolled 10 participants across three sites in Denmark and Poland. Results show that the procedure, performed under light sedation only, was safe with no device related complications. The primary performance endpoint was also met, with significant reduction of right ventricle to left ventricle volume 48 hours post-intervention. Significant clot volumes were removed, and alleviation of PE-associated symptoms was demonstrated. The catheter removed both fresh and organised clots and successfully removed blood clots of all sizes and types, from locations that could not have been safely reached using other techniques.
Prof. Asger Andersen (Aarhus University Hospital, Aarhus, Denmark), principal investigator of the study, added, “large bore aspiration of central clots with possibility to retrieve segmental clots with the eTrieve catheter, optimises the possibility for complete pulmonary revascularisation in acute PE.”

 clearance for its NED embolization device")

 AngioDynamics has announced the first patient has been enrolled in the RECOVER-AV clinical trial, a prospective, multicentre, international, single-arm study evaluating the AlphaVac multipurpose mechanical aspiration (MMA) F1885 system in the treatment of acute, intermediate-risk pulmonary embolism (PE).
AngioDynamics has announced the first patient has been enrolled in the RECOVER-AV clinical trial, a prospective, multicentre, international, single-arm study evaluating the AlphaVac multipurpose mechanical aspiration (MMA) F1885 system in the treatment of acute, intermediate-risk pulmonary embolism (PE).


 New regulations have come into effect in the UK which place a greater emphasis on medical device manufacturers to monitor the safety and performance of their products.
New regulations have come into effect in the UK which place a greater emphasis on medical device manufacturers to monitor the safety and performance of their products.
 Inquis Medical has announced that its Aventus thrombectomy system has received 510(k) clearance from the US Food and Drug Administration (FDA) for an expanded indication to treat pulmonary embolism (PE).
Inquis Medical has announced that its Aventus thrombectomy system has received 510(k) clearance from the US Food and Drug Administration (FDA) for an expanded indication to treat pulmonary embolism (PE).































 Narayanan and his team are currently collecting data on the combination of IntelliBlate with their robotic technology and planning software for microwave ablation. “So far, it has worked very well,” he stated, “but the more patients you treat, the more your experience is enhanced. We believe in collecting data and analysing it. In a few years, we will be able to see the picture this creates for the technology and publish on that,” he continued.
Narayanan and his team are currently collecting data on the combination of IntelliBlate with their robotic technology and planning software for microwave ablation. “So far, it has worked very well,” he stated, “but the more patients you treat, the more your experience is enhanced. We believe in collecting data and analysing it. In a few years, we will be able to see the picture this creates for the technology and publish on that,” he continued.
 A keynote session on the future of interventional oncology (IO) brought artificial intelligence (AI) to the forefront of discussion, highlighting both its potential and the ethical, legal, and regulatory challenges it presents. During his talk at the
A keynote session on the future of interventional oncology (IO) brought artificial intelligence (AI) to the forefront of discussion, highlighting both its potential and the ethical, legal, and regulatory challenges it presents. During his talk at the 



 You are currently on the executive committees of CIRSE and BSIR. How do these roles cross-pollinate with your daily practice?
You are currently on the executive committees of CIRSE and BSIR. How do these roles cross-pollinate with your daily practice? 


 “For me, it was essentially love at first sight,” confessed Gary Siskin (Albany Medical Center, Albany, USA), stating his enthusiasm for
“For me, it was essentially love at first sight,” confessed Gary Siskin (Albany Medical Center, Albany, USA), stating his enthusiasm for 

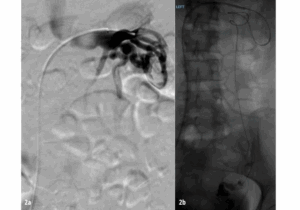







 Celebrating the 50th anniversary of the
Celebrating the 50th anniversary of the 


 R3 Vascular
R3 Vascular




















 Transcending region and socioeconomic status, a global
Transcending region and socioeconomic status, a global 


 VentiV Scientific has announced the US Food and Drug Administration (FDA) clearance of VentiV mechanical thrombectomy system to remove blood clots from the peripheral vasculature including the new VentiV Pulse platform.
VentiV Scientific has announced the US Food and Drug Administration (FDA) clearance of VentiV mechanical thrombectomy system to remove blood clots from the peripheral vasculature including the new VentiV Pulse platform.






 Evident Vascular has announced the successful closing of its Series B financing with new investors Shangbay Capital and two undisclosed multinational strategics joining founding investor Vensana Capital. A press release details that the funding will accelerate development of the company’s advanced
Evident Vascular has announced the successful closing of its Series B financing with new investors Shangbay Capital and two undisclosed multinational strategics joining founding investor Vensana Capital. A press release details that the funding will accelerate development of the company’s advanced 
 Merit Medical Systems has announced that the six-month results from the randomised arm of the Wrapsody arteriovenous access efficacy—WAVE—trial are scheduled for publication in the April issue of Kidney International, ahead of the presentation of 12-month results from the trial at the Society of Interventional Radiology’s 50th annual scientific meeting (29 March–2 April, Nashville, USA).
Merit Medical Systems has announced that the six-month results from the randomised arm of the Wrapsody arteriovenous access efficacy—WAVE—trial are scheduled for publication in the April issue of Kidney International, ahead of the presentation of 12-month results from the trial at the Society of Interventional Radiology’s 50th annual scientific meeting (29 March–2 April, Nashville, USA).


 You were the first in the USA to be accepted and graduate from the direct pathway at the University of Pennsylvania Hospital. How did this come about and what was your experience?
You were the first in the USA to be accepted and graduate from the direct pathway at the University of Pennsylvania Hospital. How did this come about and what was your experience? 







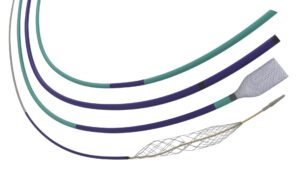




 Stereotaxis has announced a US Food and Drug Administration (FDA) regulatory submission for the first robotically navigated catheter designed to expand usage of robotic magnetic navigation into the broader endovascular field.
Stereotaxis has announced a US Food and Drug Administration (FDA) regulatory submission for the first robotically navigated catheter designed to expand usage of robotic magnetic navigation into the broader endovascular field.






 Biotronik is partnering with Egg Medical to co-sell Egg Medical’s EggNest radiation protection systems for healthcare workers in the USA.
Biotronik is partnering with Egg Medical to co-sell Egg Medical’s EggNest radiation protection systems for healthcare workers in the USA.
 Teleflex has today announced it has entered into a definitive agreement to acquire Biotronik’s
Teleflex has today announced it has entered into a definitive agreement to acquire Biotronik’s 




 A new guideline from the American Society of Echocardiography (ASE) aims to provide more detail for clinicians performing ultrasound-guided vascular cannulation.
A new guideline from the American Society of Echocardiography (ASE) aims to provide more detail for clinicians performing ultrasound-guided vascular cannulation.


 Akura Medical
Akura Medical




 The Society of Interventional Oncology (SIO) has announced the launch of a new research database and educational initiative, the
The Society of Interventional Oncology (SIO) has announced the launch of a new research database and educational initiative, the  clearance for Tembo embolic system")















 The Mount Sinai Hospital has announced that it has performed its first procedure—and the first in New York City, USA—using the Hydros (PROCEPT BioRobotics) robotic system designed to treat benign prostatic hyperplasia (BPH), or an enlarged prostate.
The Mount Sinai Hospital has announced that it has performed its first procedure—and the first in New York City, USA—using the Hydros (PROCEPT BioRobotics) robotic system designed to treat benign prostatic hyperplasia (BPH), or an enlarged prostate. 











 AngioDynamics has announced the publication of the results from the Acute Pulmonary Embolism Extraction Trial with the AlphaVac system—APEX-AV—in the Journal of the Society for Cardiovascular Angiography & Interventions (JSCAI).
AngioDynamics has announced the publication of the results from the Acute Pulmonary Embolism Extraction Trial with the AlphaVac system—APEX-AV—in the Journal of the Society for Cardiovascular Angiography & Interventions (JSCAI).
 Inquis Medical has announced completion of patient enrolment in its AVENTUS clinical trial, a pivotal investigational device exemption (IDE) trial evaluating the safety and efficacy of the company’s Aventus thrombectomy system for the treatment of pulmonary embolism (PE).
Inquis Medical has announced completion of patient enrolment in its AVENTUS clinical trial, a pivotal investigational device exemption (IDE) trial evaluating the safety and efficacy of the company’s Aventus thrombectomy system for the treatment of pulmonary embolism (PE).
 Gore has announced recent CE mark of a lower profile Viabahn VBX balloon expandable endoprosthesis (VBX stent graft).
Gore has announced recent CE mark of a lower profile Viabahn VBX balloon expandable endoprosthesis (VBX stent graft).

 4.
4. 7.
7. 








 Data from a new study have found that venous leak embolization yields additional clinical improvement and treatment potential in patients with vasculogenic erectile dysfunction (ED) resistant to phosphodiesterase-5-inhibitors (PDE5i) due to mixed arterio-venous disease. These findings were recently published in the journal
Data from a new study have found that venous leak embolization yields additional clinical improvement and treatment potential in patients with vasculogenic erectile dysfunction (ED) resistant to phosphodiesterase-5-inhibitors (PDE5i) due to mixed arterio-venous disease. These findings were recently published in the journal 


 A minimally invasive procedure provides significant relief from knee pain and may prevent the need for knee replacement surgery in people with osteoarthritis, according to a study presented at the Radiological Society of North America (
A minimally invasive procedure provides significant relief from knee pain and may prevent the need for knee replacement surgery in people with osteoarthritis, according to a study presented at the Radiological Society of North America (


 In November, the most read stories from Interventional News included a profile of current Society of Interventional Oncology (SIO) president, Muneeb Ahmed (Beth Israel Deaconess Medical Center, Boston, USA); an update on liquid biopsy and its application in interventional radiology practice according to Bruno Damascelli (Fondazione Falciani ONLUS, Milan, Italy) et al; and two-year SPYRAL HTN-ON MED results regarding renal denervation.
In November, the most read stories from Interventional News included a profile of current Society of Interventional Oncology (SIO) president, Muneeb Ahmed (Beth Israel Deaconess Medical Center, Boston, USA); an update on liquid biopsy and its application in interventional radiology practice according to Bruno Damascelli (Fondazione Falciani ONLUS, Milan, Italy) et al; and two-year SPYRAL HTN-ON MED results regarding renal denervation. 
 The
The 


















 A retrospective evaluation has found that more than a third of old strokes discovered via head
A retrospective evaluation has found that more than a third of old strokes discovered via head 











 Healionics Corporation has today announced that its STARgraft arteriovenous graft—which it states is designed to provide a safer and more reliable means of bloodstream access for
Healionics Corporation has today announced that its STARgraft arteriovenous graft—which it states is designed to provide a safer and more reliable means of bloodstream access for 






 As your presidency of the SIO comes to a close, what have been your greatest achievements?
As your presidency of the SIO comes to a close, what have been your greatest achievements? 







 A focus session dedicated to quality-of-life (QoL) outcomes in
A focus session dedicated to quality-of-life (QoL) outcomes in 






 The US Food and Drug Administration (FDA) has approved Akura Medical’s investigational device exemption (IDE) application to initiate the QUADRA-PE study evaluating the Katana thrombectomy system in patients with acute pulmonary embolism (PE).
The US Food and Drug Administration (FDA) has approved Akura Medical’s investigational device exemption (IDE) application to initiate the QUADRA-PE study evaluating the Katana thrombectomy system in patients with acute pulmonary embolism (PE).
 Royal Philips has announced enrolment of the first patient in the US THOR IDE clinical trial, which will study an innovative combined laser atherectomy and intravascular lithotripsy (IVL) catheter.
Royal Philips has announced enrolment of the first patient in the US THOR IDE clinical trial, which will study an innovative combined laser atherectomy and intravascular lithotripsy (IVL) catheter.


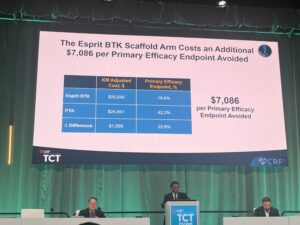

 The
The 





 Cook Medical’s
Cook Medical’s 




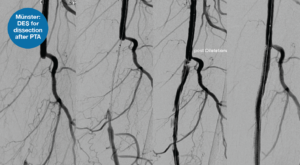


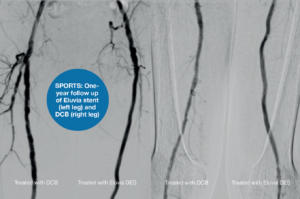

 In a
In a 



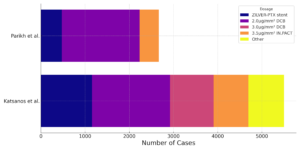












 Their results showed that six-month patency was “significantly” higher for both TLPP (89.8% vs. 62.8%, p<0.0001) and ACPP (72.6% vs. 57.9%, p<0.015) in patients treated with Wrapsody when compared with patients randomised to PTA. Additionally, in a summary of safety events through 30 days post treatment, there was no significant difference between the groups with very low event rates in both. Freedom from 30-day safety event rate was 96.6% in the Wrapsody group versus 95% in the PTA group.
Their results showed that six-month patency was “significantly” higher for both TLPP (89.8% vs. 62.8%, p<0.0001) and ACPP (72.6% vs. 57.9%, p<0.015) in patients treated with Wrapsody when compared with patients randomised to PTA. Additionally, in a summary of safety events through 30 days post treatment, there was no significant difference between the groups with very low event rates in both. Freedom from 30-day safety event rate was 96.6% in the Wrapsody group versus 95% in the PTA group.

 A new study shows that a minimally invasive treatment for
A new study shows that a minimally invasive treatment for 




 Sirtex Medical has today announced that it has received certification according to European medical device regulation (MDR) 2017/745 for SIR-Spheres Y90 resin microspheres and its delivery systems, paving the way for the European launch of the SIROS delivery system.
Sirtex Medical has today announced that it has received certification according to European medical device regulation (MDR) 2017/745 for SIR-Spheres Y90 resin microspheres and its delivery systems, paving the way for the European launch of the SIROS delivery system.





 Immunophotonics has announced a collaboration with The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) around a phase 2/3 clinical trial.
Immunophotonics has announced a collaboration with The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) around a phase 2/3 clinical trial.







































 “What I find interesting when using the Imactis system with the addition of CBCT is, due to the wide bore, you can very easily jump from one modality to another,” he detailed. In practice, Lambros is able to plan the trajectory of the needle on the initial CBCT scan while the patient’s arms are down, and then precisely choose the entry point using Imactis. This way, Lambros and his team can view the virtual anatomical mapping alongside the real-time control images to proceed with absolute confidence.
“What I find interesting when using the Imactis system with the addition of CBCT is, due to the wide bore, you can very easily jump from one modality to another,” he detailed. In practice, Lambros is able to plan the trajectory of the needle on the initial CBCT scan while the patient’s arms are down, and then precisely choose the entry point using Imactis. This way, Lambros and his team can view the virtual anatomical mapping alongside the real-time control images to proceed with absolute confidence. Although centres today seek to offer the highest-quality treatment to their patients, investment in new technologies can appear unattainable due to cost-efficiency and time to installation. GE HealthCare interventional chief executive officer Arnaud Marie told Interventional News hat he heeded this challenge, and explained that their vision for Imactis was to be able to “integrate with already available CT-scanners and innovations emerging from start-ups, academics and other large companies, so we can leverage our ecosystem to seamlessly provide the best-in-class solution”. With this ethos in mind, Marie explained how GE HealthCare has collaborated with companies such as Centerline Biomedical—a provider of X-ray navigation technology—to help to bring beneficial solutions to market.
Although centres today seek to offer the highest-quality treatment to their patients, investment in new technologies can appear unattainable due to cost-efficiency and time to installation. GE HealthCare interventional chief executive officer Arnaud Marie told Interventional News hat he heeded this challenge, and explained that their vision for Imactis was to be able to “integrate with already available CT-scanners and innovations emerging from start-ups, academics and other large companies, so we can leverage our ecosystem to seamlessly provide the best-in-class solution”. With this ethos in mind, Marie explained how GE HealthCare has collaborated with companies such as Centerline Biomedical—a provider of X-ray navigation technology—to help to bring beneficial solutions to market. “My vision is that there will be a convergence of technologies to provide integrated systems that will enable delivery of these procedures in a much more predictive, democratised and safer way for both for the patient and the interventionalist through reducing exposure to radiation.”
“My vision is that there will be a convergence of technologies to provide integrated systems that will enable delivery of these procedures in a much more predictive, democratised and safer way for both for the patient and the interventionalist through reducing exposure to radiation.”


 The European Society of Cardiology (
The European Society of Cardiology (
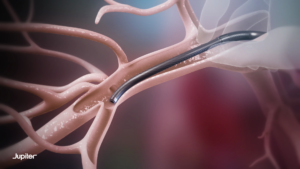






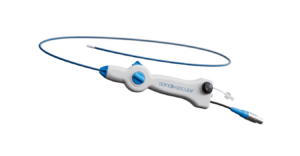













 In a
In a 












 Having been involved in several CIRSE committees for many years, how has the programme adapted to scientific innovation and what key developments stick out in your memory of previous congresses?
Having been involved in several CIRSE committees for many years, how has the programme adapted to scientific innovation and what key developments stick out in your memory of previous congresses? 
 approval for Morph DNA steerable introducer sheath family")
 BioCardia has submitted a 510(k) for approval of its patented Morph DNA steerable introducer sheath to the US Food and Drug Administration (FDA).
BioCardia has submitted a 510(k) for approval of its patented Morph DNA steerable introducer sheath to the US Food and Drug Administration (FDA).
 China’s National Medical Products Administration (NMPA) has granted a Class III Medical Devices Certificate of Registration for the msRDN radiofrequency renal denervation system (SyMap Medical).
China’s National Medical Products Administration (NMPA) has granted a Class III Medical Devices Certificate of Registration for the msRDN radiofrequency renal denervation system (SyMap Medical).




















 A recent survey conducted by
A recent survey conducted by




 Penumbra has announced that it has received CE mark approval and so has initiated the European launch of BMX81 and BMX96, devices which are designed for neurovascular management of ischaemic and haemorrhagic stroke.
Penumbra has announced that it has received CE mark approval and so has initiated the European launch of BMX81 and BMX96, devices which are designed for neurovascular management of ischaemic and haemorrhagic stroke.
 Medical Templates has announced that they have received US Food and Drug Administration (FDA) clearance for their Cube Navigator software for planning of percutaneous, computed tomography (CT)-guided interventions.
Medical Templates has announced that they have received US Food and Drug Administration (FDA) clearance for their Cube Navigator software for planning of percutaneous, computed tomography (CT)-guided interventions.  Navigation is gaining importance in the field of interventional radiology (IR), mainly driven by expanding treatment options in oncology and improved patient outcomes through the use of minimally-invasive procedures, the press release states. Smaller targets, more complex access routes, and time and personnel constraints have all contributed to the increased adoption of CT navigation systems.
Navigation is gaining importance in the field of interventional radiology (IR), mainly driven by expanding treatment options in oncology and improved patient outcomes through the use of minimally-invasive procedures, the press release states. Smaller targets, more complex access routes, and time and personnel constraints have all contributed to the increased adoption of CT navigation systems.



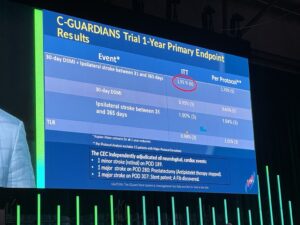 New data from the C-GUARDIANS pivotal investigational device exemption (IDE) trial support consideration of
New data from the C-GUARDIANS pivotal investigational device exemption (IDE) trial support consideration of 




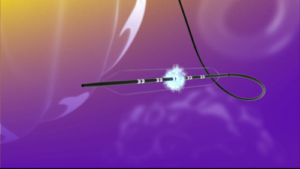






 New multisociety clinical practice guidelines for the management of lower extremity
New multisociety clinical practice guidelines for the management of lower extremity 
 Majorie van Helvert (University of Twente, Enschede, The Netherlands) and Michel Reijnen (Rijnstate Hospital, Arnhem, The Netherlands) are currently conducting research on ultrafast contrast-enhanced ultrasound blood flow quantification in
Majorie van Helvert (University of Twente, Enschede, The Netherlands) and Michel Reijnen (Rijnstate Hospital, Arnhem, The Netherlands) are currently conducting research on ultrafast contrast-enhanced ultrasound blood flow quantification in 
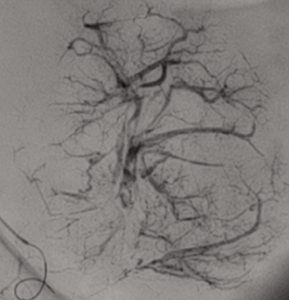

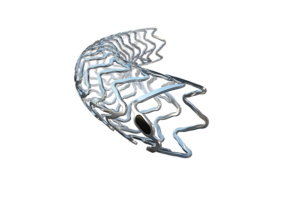

 New clinical results highlight the need for inclusive approaches and comprehensive examinations of treatment options for
New clinical results highlight the need for inclusive approaches and comprehensive examinations of treatment options for 



 Late-breaking data from the ENGULF trial showed that a novel dual-action
Late-breaking data from the ENGULF trial showed that a novel dual-action 









 In response to Ugwueze, interventional radiologist Sangjoon Park (Seoul National University Hospital, Seoul, South Korea) shared his experience in Ethiopia and recounted difficulties in transporting enough lipiodol to the centre there. Park averred that trainee interventional radiologists there should not be trained in these procedures if they have no access to the devices/therapeutic agents. “Bottom line, there’s some things that you can do and some things that you can’t—so you have to decide on what procedures you can do to the best of your ability.”
In response to Ugwueze, interventional radiologist Sangjoon Park (Seoul National University Hospital, Seoul, South Korea) shared his experience in Ethiopia and recounted difficulties in transporting enough lipiodol to the centre there. Park averred that trainee interventional radiologists there should not be trained in these procedures if they have no access to the devices/therapeutic agents. “Bottom line, there’s some things that you can do and some things that you can’t—so you have to decide on what procedures you can do to the best of your ability.”











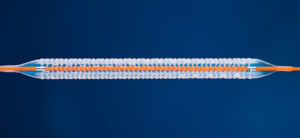 Abbott has announced that the US Food and Drug Administration (FDA) has approved the Esprit BTK everolimus-eluting resorbable scaffold system (Esprit BTK system), a breakthrough innovation for people with chronic limb-threatening ischemia (CLTI) below-the-knee (BTK).
Abbott has announced that the US Food and Drug Administration (FDA) has approved the Esprit BTK everolimus-eluting resorbable scaffold system (Esprit BTK system), a breakthrough innovation for people with chronic limb-threatening ischemia (CLTI) below-the-knee (BTK).



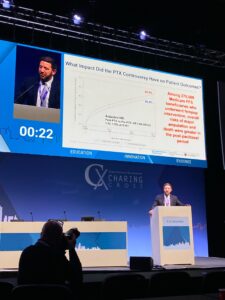

 Showcasing cutting-edge applications of
Showcasing cutting-edge applications of 






 FastWave Medical has announced the issuance of its fourth utility patent by the United States Patent and Trademark Office (USPTO) for its laser-intravascular lithotripsy (IVL) platform.
FastWave Medical has announced the issuance of its fourth utility patent by the United States Patent and Trademark Office (USPTO) for its laser-intravascular lithotripsy (IVL) platform.








 If you want to be involved in organising an IR Bites workshop local to you or just stay up to date with future IR Bites Workshops scan the
If you want to be involved in organising an IR Bites workshop local to you or just stay up to date with future IR Bites Workshops scan the 






 Debates will shed new light on controversies in the treatment of aortic disease at the 2024 Charing Cross (CX) Symposium, alongside practical sessions with a focus on techniques and technologies in both aortic endovascular and open surgical repair.
Debates will shed new light on controversies in the treatment of aortic disease at the 2024 Charing Cross (CX) Symposium, alongside practical sessions with a focus on techniques and technologies in both aortic endovascular and open surgical repair.
















 The
The 















 In a session dedicated to neonate, infant and paediatric interventional radiology (IR), Hisham Alshehri (King Abdulaziz University, Jeddah, Saudi Arabia) gave a talk at the
In a session dedicated to neonate, infant and paediatric interventional radiology (IR), Hisham Alshehri (King Abdulaziz University, Jeddah, Saudi Arabia) gave a talk at the 









 Marie then defines the third tenet that shaped the development of Embo ASSIST AI—to provide integrated patient care—and explains how the software brings together the “silos” which he states make up healthcare. By speeding up data consolidation, Marie hopes the AI technology can “link those different silos—from the doctor, the technician, the nurses—through information sharing, to revolutionise” the patient care pathway. Throughout this process, Marie states that the company’s overarching refrain was to ask: How can it be summarised? How can it be accelerated? “We are all patients, or have been patients,” he states. “We want interventionists to have access to the best data and tools.”
Marie then defines the third tenet that shaped the development of Embo ASSIST AI—to provide integrated patient care—and explains how the software brings together the “silos” which he states make up healthcare. By speeding up data consolidation, Marie hopes the AI technology can “link those different silos—from the doctor, the technician, the nurses—through information sharing, to revolutionise” the patient care pathway. Throughout this process, Marie states that the company’s overarching refrain was to ask: How can it be summarised? How can it be accelerated? “We are all patients, or have been patients,” he states. “We want interventionists to have access to the best data and tools.”






 In a roundtable dedicated to comparing training pathways for interventional radiology (IR) in Saudi Arabia, the Middle East and North Africa (MENA), Europe and North America, discussion levelled on the challenges faced by many and heard first-hand experiences of trainees around the globe.
In a roundtable dedicated to comparing training pathways for interventional radiology (IR) in Saudi Arabia, the Middle East and North Africa (MENA), Europe and North America, discussion levelled on the challenges faced by many and heard first-hand experiences of trainees around the globe.
























 Efemoral Medical
Efemoral Medical Sensome has announced enrolment of the first patients into a feasibility clinical study using the Clotild smart guidewire in
Sensome has announced enrolment of the first patients into a feasibility clinical study using the Clotild smart guidewire in 

 The REDUCED-1 study, a US Food and Drug Administration (FDA) investigational device exemption (IDE)-approved pilot study of the treatment of hypertension with the proprietary Therapeutic Intra-Vascular Ultrasound (TIVUS) system (SoniVie), has completed enrolment.
The REDUCED-1 study, a US Food and Drug Administration (FDA) investigational device exemption (IDE)-approved pilot study of the treatment of hypertension with the proprietary Therapeutic Intra-Vascular Ultrasound (TIVUS) system (SoniVie), has completed enrolment.


 Baird Medical Devices, a microwave ablation medical device developer and provider in China and the USA, has recently announced that it has performed its first thyroid microwave ablation procedure in the USA since obtaining registration clearance from the US Food and Drug Administration (FDA) on November 22, 2023.
Baird Medical Devices, a microwave ablation medical device developer and provider in China and the USA, has recently announced that it has performed its first thyroid microwave ablation procedure in the USA since obtaining registration clearance from the US Food and Drug Administration (FDA) on November 22, 2023. technology broadens patient applicability for complex disease management")



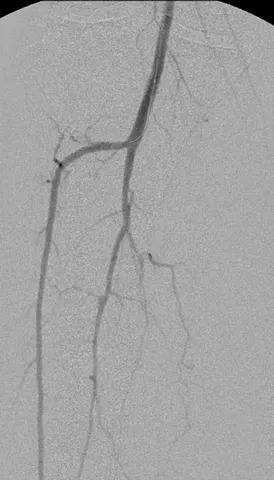








 Endovascular Engineering (E2) has announced US Food and Drug Administration (FDA) investigational device exemption (IDE) approval for its ENGULF US pivotal trial.
Endovascular Engineering (E2) has announced US Food and Drug Administration (FDA) investigational device exemption (IDE) approval for its ENGULF US pivotal trial.


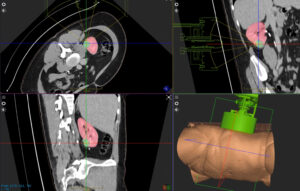




 Proceedings from an expert consensus roundtable that discussed the benefits of
Proceedings from an expert consensus roundtable that discussed the benefits of 
 GE HealthCare has entered into an agreement to acquire MIM Software, a provider of artificial intelligence (AI)-enabled image analysis and workflow tools across multiple care areas, including oncology, urology, neurology, and cardiology
GE HealthCare has entered into an agreement to acquire MIM Software, a provider of artificial intelligence (AI)-enabled image analysis and workflow tools across multiple care areas, including oncology, urology, neurology, and cardiology
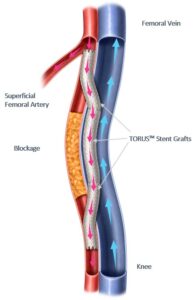



 AnX Robotica
AnX Robotica
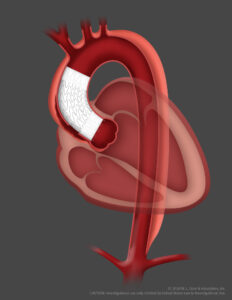 Gore has announced the first patient implantation of the Gore ascending stent graft in the ARISE II trial, describing this as an exciting step in the development of treatments for pathologies involving the ascending aorta using endovascular repair rather than traditional open surgery.
Gore has announced the first patient implantation of the Gore ascending stent graft in the ARISE II trial, describing this as an exciting step in the development of treatments for pathologies involving the ascending aorta using endovascular repair rather than traditional open surgery.
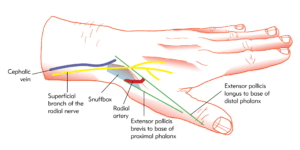


 Microbot Medical, developer of the Liberty endovascular robotic surgical system, has entered into a collaboration agreement with Corewell Health.
Microbot Medical, developer of the Liberty endovascular robotic surgical system, has entered into a collaboration agreement with Corewell Health.
 Terumo Medical
Terumo Medical







 OncoSil Medical
OncoSil Medical
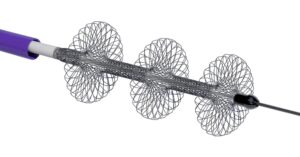





 A panel of leading experts has welcomed guidance published by the
A panel of leading experts has welcomed guidance published by the 





 system ‘revolutionises’ pulmonary embolism treatment")




 Medtronic has announced approval from the USA Food and Drug Administration (FDA) for the Symplicity Spyral renal denervation (RDN) system for the treatment of hypertension. The company has said that it will immediately begin commercialisation following the approval.
Medtronic has announced approval from the USA Food and Drug Administration (FDA) for the Symplicity Spyral renal denervation (RDN) system for the treatment of hypertension. The company has said that it will immediately begin commercialisation following the approval.























 Interventional News’ most read stories in October included significant data releases from TCT 2023 (23–26 October, San Francisco, USA); results from a study investigating sex disparities in outcomes post-TCAR; among several device updates.
Interventional News’ most read stories in October included significant data releases from TCT 2023 (23–26 October, San Francisco, USA); results from a study investigating sex disparities in outcomes post-TCAR; among several device updates.












 Endovascular Engineering (E2) has announced positive initial results from its ENGULF study, demonstrating successful outcomes among the first 15 patients evaluated in the trial using the Hēlo thrombectomy system for the treatment of acute sub-massive pulmonary embolism.
Endovascular Engineering (E2) has announced positive initial results from its ENGULF study, demonstrating successful outcomes among the first 15 patients evaluated in the trial using the Hēlo thrombectomy system for the treatment of acute sub-massive pulmonary embolism.


 A recent publication in the journal
A recent publication in the journal 















 The
The 






 clearance for its FreedomFlow orbital atherectomy peripheral platform")














 His brilliant surgical skills were recognised by innumerable international surgical societies as well as the White House Medical Unit for the support he provided during the visit of President George H Bush to London in 1991. More recently, Professor Greenhalgh became a company director, founding BIBA Medical with his son, Stephen, in 1994. Professor Greenhalgh was editor-in-chief of the company’s foremost medical publication,
His brilliant surgical skills were recognised by innumerable international surgical societies as well as the White House Medical Unit for the support he provided during the visit of President George H Bush to London in 1991. More recently, Professor Greenhalgh became a company director, founding BIBA Medical with his son, Stephen, in 1994. Professor Greenhalgh was editor-in-chief of the company’s foremost medical publication, 











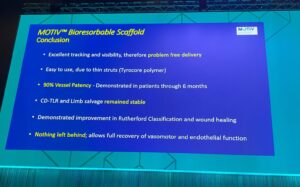 Presenting their updated results, Rand conveyed their “excellent” outcomes, underlining data which show a 2% clinically-driven TLR rate and 95% limb-salvage rate among their patient cohort. Continuing, he reported “high primary patency rates”—81.7% at 24-months—and presented a 98.3% CD-TLR outcome, including a case study to visually bolster these data and display the positive healing results of an individual in their patient population.
Presenting their updated results, Rand conveyed their “excellent” outcomes, underlining data which show a 2% clinically-driven TLR rate and 95% limb-salvage rate among their patient cohort. Continuing, he reported “high primary patency rates”—81.7% at 24-months—and presented a 98.3% CD-TLR outcome, including a case study to visually bolster these data and display the positive healing results of an individual in their patient population.













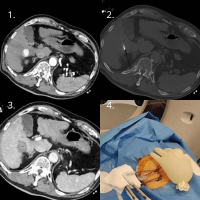



")




![“The PAIRS IR curriculum […] will be published by the 2024 annual meeting”](https://interventionalnews.com/wp-content/uploads/sites/13/2023/08/ayman-al-sibaie.jpg "“The PAIRS IR curriculum […] will be published by the 2024 annual meeting”")










 Algorithms came to the forefront next, with Brodmann stepping in to deliver the absent Maria Ruffino’s (Institute of Imaging of Southern Switzerland, Lugano, Switzerland) presentation on the need for clarity on the best aortoiliac lesion treatment. A compelling discussion followed, where it was suggested by one audience member that lack of evidence-based treatment in this area could be due to physicians’ preference. In conversation with Interventional News, Brodmann said: “This is indeed the case. Therefore, there is a need for creating strong treatment algorithms in different areas.” This, she suggested, was a need that could be met by physicians.
Algorithms came to the forefront next, with Brodmann stepping in to deliver the absent Maria Ruffino’s (Institute of Imaging of Southern Switzerland, Lugano, Switzerland) presentation on the need for clarity on the best aortoiliac lesion treatment. A compelling discussion followed, where it was suggested by one audience member that lack of evidence-based treatment in this area could be due to physicians’ preference. In conversation with Interventional News, Brodmann said: “This is indeed the case. Therefore, there is a need for creating strong treatment algorithms in different areas.” This, she suggested, was a need that could be met by physicians. Following one packed day of presentations came another, with the session on lesion treatment opening with further discussion from Rammos, who presented on a rotational atherothrombectomy device. In the subsequent talks on lesions, Mercedes Guerra (University Guadalajara Hospital, Guadalajara, Spain) gave a strong presentation on the need for better classification of extremely calcified lesions, which she said require their own treatment approach.
Following one packed day of presentations came another, with the session on lesion treatment opening with further discussion from Rammos, who presented on a rotational atherothrombectomy device. In the subsequent talks on lesions, Mercedes Guerra (University Guadalajara Hospital, Guadalajara, Spain) gave a strong presentation on the need for better classification of extremely calcified lesions, which she said require their own treatment approach.





 The Society for Cardiovascular Angiography & Interventions (SCAI) has welcomed the review of scientific data related to the premarket approval applications for two renal denervation systems, describing this as a “step forward to advancing access to additional therapies for people with uncontrolled hypertension”.
The Society for Cardiovascular Angiography & Interventions (SCAI) has welcomed the review of scientific data related to the premarket approval applications for two renal denervation systems, describing this as a “step forward to advancing access to additional therapies for people with uncontrolled hypertension”.










 Data on hundreds of thousands of patients who have received lower limb endovascular treatment provide confidence in
Data on hundreds of thousands of patients who have received lower limb endovascular treatment provide confidence in  References:
References: 
 In 2010, the
In 2010, the 







 Xeltis
Xeltis





 Interventional News’ most popular stories from July included point of view pieces from interventional radiologists on fallopian tube recanalisation and interventions for postpartum haemorrhage, respectively; news of an editorial from The Cardiovascular Interventional Radiological Society of Europe (CIRSE) which takes a stance on paclitaxel-coated devices; and a report of a Society of Interventional Radiology (SIR) position statement offering recommendations on the management of chronic iliofemoral venous obstruction with endovascular placement of metallic stents.
Interventional News’ most popular stories from July included point of view pieces from interventional radiologists on fallopian tube recanalisation and interventions for postpartum haemorrhage, respectively; news of an editorial from The Cardiovascular Interventional Radiological Society of Europe (CIRSE) which takes a stance on paclitaxel-coated devices; and a report of a Society of Interventional Radiology (SIR) position statement offering recommendations on the management of chronic iliofemoral venous obstruction with endovascular placement of metallic stents.





 clearance for XR90 augmented reality-based visualisation and navigation platform")






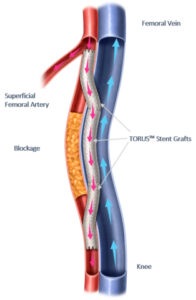


 In June 2023,
In June 2023,




 CX audience deems paclitaxel not dangerous
CX audience deems paclitaxel not dangerous
 Following
Following 


 Boston Scientific has received US Food and Drug Administration (FDA) 510(k) clearance for its Embold soft and packing coils, the company has announced in a press release. The coils are designed for use in a variety of embolization procedures.
Boston Scientific has received US Food and Drug Administration (FDA) 510(k) clearance for its Embold soft and packing coils, the company has announced in a press release. The coils are designed for use in a variety of embolization procedures.












 As announced at the Society for Vascular Surgery (SVS) Vascular Annual Meeting (VAM 2023; 14–17 June, National Harbor, USA), the
As announced at the Society for Vascular Surgery (SVS) Vascular Annual Meeting (VAM 2023; 14–17 June, National Harbor, USA), the 

 In this newly published venous ovine study, fibred
In this newly published venous ovine study, fibred 





























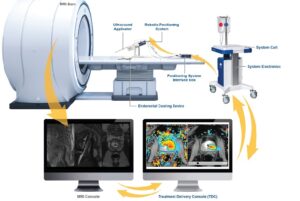

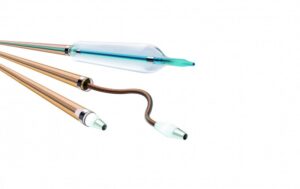

 Medtronic has announced that Ken Washington has been appointed chief technology and innovation officer.
Medtronic has announced that Ken Washington has been appointed chief technology and innovation officer.









 Govindarajan Narayanan, chief of interventional oncology at Miami Cancer Institute and a vascular interventional radiologist with Miami Cardiac & Vascular Institute (both Miami, USA), successfully treated the first patient in the USA with a liver tumour using
Govindarajan Narayanan, chief of interventional oncology at Miami Cancer Institute and a vascular interventional radiologist with Miami Cardiac & Vascular Institute (both Miami, USA), successfully treated the first patient in the USA with a liver tumour using 





 Discussing the role of
Discussing the role of  Speaking in the Vanguard session on the first day of the 2023
Speaking in the Vanguard session on the first day of the 2023 
 Setting the audiences sights on the horizon at the 2023
Setting the audiences sights on the horizon at the 2023  Bentley
Bentley















 The US Food and Drug Administration (FDA) has granted the third investigational device exemption (IDE) approval for Concept Medical’s MagicTouch sirolimus-coated balloon (SCB). Along with this latest IDE approval for the treatment of small vessels, Concept Medical received two other IDE approvals for the MagicTouch SCB family of products for the treatment of coronary
The US Food and Drug Administration (FDA) has granted the third investigational device exemption (IDE) approval for Concept Medical’s MagicTouch sirolimus-coated balloon (SCB). Along with this latest IDE approval for the treatment of small vessels, Concept Medical received two other IDE approvals for the MagicTouch SCB family of products for the treatment of coronary 





 A question from Manj Gohel (Cambridge University Hospitals NHS Foundation Trust, Cambridge, UK) on what the Charing Cross (CX) audience should take back to their multidisciplinary team meetings from the first-time presentation of BASIL-2 led chief investigator Andrew Bradbury (University of Birmingham, Birmingham, UK) to deliver the stark message: a patient who needs a below-the-knee revascularisation with or without a femoropopliteal revascularisation is likely to do better if they are treated with a best endovascular-first strategy rather than a vein bypass-first approach.
A question from Manj Gohel (Cambridge University Hospitals NHS Foundation Trust, Cambridge, UK) on what the Charing Cross (CX) audience should take back to their multidisciplinary team meetings from the first-time presentation of BASIL-2 led chief investigator Andrew Bradbury (University of Birmingham, Birmingham, UK) to deliver the stark message: a patient who needs a below-the-knee revascularisation with or without a femoropopliteal revascularisation is likely to do better if they are treated with a best endovascular-first strategy rather than a vein bypass-first approach.
 “A trial of two strategies”
“A trial of two strategies”
 Bentley has bought its main supplier, the Switzerland-based Qmedics, Bentley has recently announced in a press release. It also announced its plan of initial public offering (IPO), which is planned for autumn/winter 2023/2024, depending on market conditions.
Bentley has bought its main supplier, the Switzerland-based Qmedics, Bentley has recently announced in a press release. It also announced its plan of initial public offering (IPO), which is planned for autumn/winter 2023/2024, depending on market conditions.
 Vestibular schwannomas
Vestibular schwannomas





 GE HealthCare is further advancing its precision care strategy with CT-Navigation, which offers clinicians detailed, real-time, 3D computed tomography (CT) images for stereotactic needle guidance across an array of care areas, including interventional and oncological procedures, as well as biopsies, ablations, drainage, and therapeutics.
GE HealthCare is further advancing its precision care strategy with CT-Navigation, which offers clinicians detailed, real-time, 3D computed tomography (CT) images for stereotactic needle guidance across an array of care areas, including interventional and oncological procedures, as well as biopsies, ablations, drainage, and therapeutics.
 BlackSwan Vascular, a privately held company that is developing innovative therapies in endovascular
BlackSwan Vascular, a privately held company that is developing innovative therapies in endovascular 












 evidence on MSK metastases")
 At the
At the 
















 A new investigation into the association between
A new investigation into the association between 







 clearance")




 A total of £10 million has been awarded to the Medicines and Healthcare products Regulatory Agency (MHRA)—an executive agency of the UK Department of Health and Social Care (DHSC)—to help bring innovative new medicines and medical technologies to UK patients more quickly, His Majesty’s (HM) Treasury has announced.
A total of £10 million has been awarded to the Medicines and Healthcare products Regulatory Agency (MHRA)—an executive agency of the UK Department of Health and Social Care (DHSC)—to help bring innovative new medicines and medical technologies to UK patients more quickly, His Majesty’s (HM) Treasury has announced.
 When receiving treatment for
When receiving treatment for 
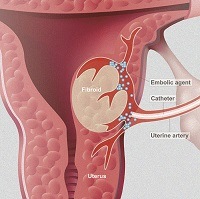




 NeoDynamics, a medical device company dedicated to advancing the diagnosis and care of cancer, recently announced that the company has been granted a Chinese patent for the needle design employed in the
NeoDynamics, a medical device company dedicated to advancing the diagnosis and care of cancer, recently announced that the company has been granted a Chinese patent for the needle design employed in the 

 New interventional oncology data from Galvanize demonstrate positive preclinical and early clinical study results using the Aliya pulsed electric field (PEF) system.
New interventional oncology data from Galvanize demonstrate positive preclinical and early clinical study results using the Aliya pulsed electric field (PEF) system.


 The European Union’s Council of Ministers has today adopted a resolution to extend the deadline for the certification of medical devices under the Medical Devices Regulation (MDR).
The European Union’s Council of Ministers has today adopted a resolution to extend the deadline for the certification of medical devices under the Medical Devices Regulation (MDR).


 Lead researchers Clifford Weiss and Daniel Giraldo Herrera (Johns Hopkins University School of Medicine, Baltimore, USA) presented their recent bariatric arterial embolization (BAE) study at the Society of Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA). Their research found that the procedure was associated with “significant” weight loss that did not affect muscle mass, as detected by whole-body magnetic resonance imaging anthropometry.
Lead researchers Clifford Weiss and Daniel Giraldo Herrera (Johns Hopkins University School of Medicine, Baltimore, USA) presented their recent bariatric arterial embolization (BAE) study at the Society of Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA). Their research found that the procedure was associated with “significant” weight loss that did not affect muscle mass, as detected by whole-body magnetic resonance imaging anthropometry.
 Robert A Lookstein, who is executive vice chair, Diagnostic, Molecular and Interventional Radiology at the Icahn School of Medicine at Mount Sinai Hospital (New York, USA) today presented the results of a subanalysis of Thrombolex’s National Heart, Lung and Blood Institute (NHLBI)-sponsored RESCUE trial during the late-breaking trial session at the Society for Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA).
Robert A Lookstein, who is executive vice chair, Diagnostic, Molecular and Interventional Radiology at the Icahn School of Medicine at Mount Sinai Hospital (New York, USA) today presented the results of a subanalysis of Thrombolex’s National Heart, Lung and Blood Institute (NHLBI)-sponsored RESCUE trial during the late-breaking trial session at the Society for Interventional Radiology (SIR) annual scientific meeting (4–9 March, Phoenix, USA).


 and Dr. Minhaj S. Khaja (right) on the day of the procedure.")




















 Xeltis has raised €32 million in a Series D2 equity fundraise, backed by a syndicate of current and new investors, which the company says will enable it to progress its clinical programmes into pivotal trials.
Xeltis has raised €32 million in a Series D2 equity fundraise, backed by a syndicate of current and new investors, which the company says will enable it to progress its clinical programmes into pivotal trials.![PAIRS 2023: “[Opening] the gate” to IR in the Middle East and North Africa](https://interventionalnews.com/wp-content/uploads/sites/13/2023/02/rana-featured.jpg "PAIRS 2023: “[Opening] the gate” to IR in the Middle East and North Africa")







 Renal denervation represents another treatment option in patients with uncontrolled resistant hypertension and may be used in selected patients deemed intolerant to antihypertensive drugs.
Renal denervation represents another treatment option in patients with uncontrolled resistant hypertension and may be used in selected patients deemed intolerant to antihypertensive drugs.



















 1. CTO of the left superficial femoral artery in a male patient suffering from severe claudication left calf.
1. CTO of the left superficial femoral artery in a male patient suffering from severe claudication left calf.








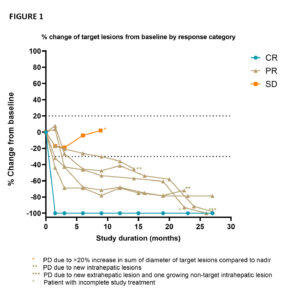

 A team of specialists at Ulis Hospital (Ulis,
A team of specialists at Ulis Hospital (Ulis, 











 GE Healthcare announced it has entered into an agreement to acquire Imactis, an innovator in computed tomography (CT) interventional guidance across an array of care areas. Imactis is a
GE Healthcare announced it has entered into an agreement to acquire Imactis, an innovator in computed tomography (CT) interventional guidance across an array of care areas. Imactis is a 






 AVS has announced that it raised US$20 million in Series B financing, which the company says will accelerate clinical trial timelines for its device for peripheral application in pulsatile intravascular lithotripsy (PIVL) cases and advance development and preclinical work on a PIVL device for coronary cases.
AVS has announced that it raised US$20 million in Series B financing, which the company says will accelerate clinical trial timelines for its device for peripheral application in pulsatile intravascular lithotripsy (PIVL) cases and advance development and preclinical work on a PIVL device for coronary cases.










 Data have been presented for the first time at the
Data have been presented for the first time at the 


 clearance of BodyTom 64")


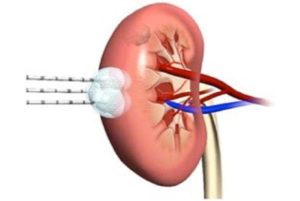

 The Swiss Federal Assembly has voted in favour of accepting medical devices with US Food and Drug Administration (FDA) marketing authorisation in Switzerland.
The Swiss Federal Assembly has voted in favour of accepting medical devices with US Food and Drug Administration (FDA) marketing authorisation in Switzerland.





























 But, right now, in the immediate aftermath of lockdowns, Patel recounts witnessing “a chorus of excitement and eagerness to be completely in-person,” at SIR 2022. “Screen fatigue is real,” Patel adds, attributing the “[palpable] desire to continue to meet in person” to this fact. Jaworski has observed the same enthusiasm for the in-person RSNA annual meeting: “Currently, our in-person registration is up 54% from this time last year, while our virtual meeting is on a par with 2021,” he relays to Interventional News. This follows an RSNA 2021 meeting for which attendance was “in line with our expectations”—30,000 attendees, of whom 6,000 attended virtually.
But, right now, in the immediate aftermath of lockdowns, Patel recounts witnessing “a chorus of excitement and eagerness to be completely in-person,” at SIR 2022. “Screen fatigue is real,” Patel adds, attributing the “[palpable] desire to continue to meet in person” to this fact. Jaworski has observed the same enthusiasm for the in-person RSNA annual meeting: “Currently, our in-person registration is up 54% from this time last year, while our virtual meeting is on a par with 2021,” he relays to Interventional News. This follows an RSNA 2021 meeting for which attendance was “in line with our expectations”—30,000 attendees, of whom 6,000 attended virtually.


 BEST-CLI meets “astronomic” need for high-quality, practice-changing data
BEST-CLI meets “astronomic” need for high-quality, practice-changing data


















 In the USA,
In the USA, 





 XACT Robotics announced that its ACE Xtend remote control unit received US Food and Drug Administration (FDA) clearance, allowing users to robotically insert and steer the XACT ACE Robotic System remotely from the control room. The first-of-its-kind feature for computed tomography (CT)-guided percutaneous procedures is designed to improve physician workflows while limiting physician and other users’ exposure to radiation, and to reduce physical strain.
XACT Robotics announced that its ACE Xtend remote control unit received US Food and Drug Administration (FDA) clearance, allowing users to robotically insert and steer the XACT ACE Robotic System remotely from the control room. The first-of-its-kind feature for computed tomography (CT)-guided percutaneous procedures is designed to improve physician workflows while limiting physician and other users’ exposure to radiation, and to reduce physical strain.




 Xeltis today announced what it describes as “very promising” preliminary efficacy and safety results from one of the centres participating in the AXESS study—a first-in-human (FIH) clinical trial of its restorative haemodialysis access graft, Axess.
Xeltis today announced what it describes as “very promising” preliminary efficacy and safety results from one of the centres participating in the AXESS study—a first-in-human (FIH) clinical trial of its restorative haemodialysis access graft, Axess.




 Paediatric interventional radiologist Alex Barnacle (Great Ormond Street Hospital, London, UK) gave the Josef Roesch Lecture at the
Paediatric interventional radiologist Alex Barnacle (Great Ormond Street Hospital, London, UK) gave the Josef Roesch Lecture at the 

























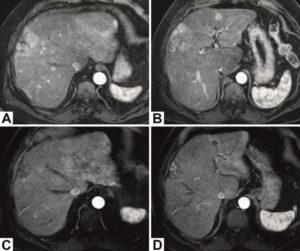


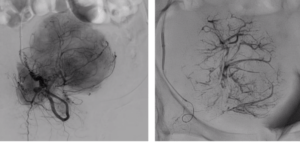


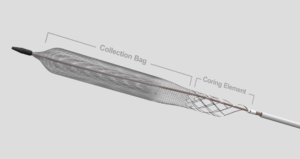




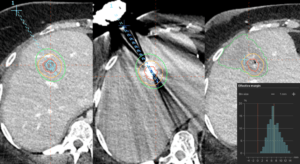









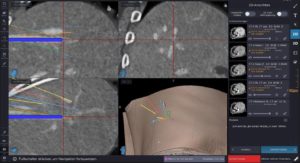




 The first US patient has been enrolled in the US Food and Drug Administration (FDA) SELUTION4BTK (below-the-knee) clinical trial evaluating Selution SLR, MedAlliance’s novel sirolimus-eluting balloon. This follows investigational device exemption (IDE) approval in the USA in
The first US patient has been enrolled in the US Food and Drug Administration (FDA) SELUTION4BTK (below-the-knee) clinical trial evaluating Selution SLR, MedAlliance’s novel sirolimus-eluting balloon. This follows investigational device exemption (IDE) approval in the USA in 















 Gore has announced the acquisition of InnAVasc Medical, a privately held medical technology company focused on advancing care for patients with end-stage renal disease who utilise graft circuits for dialysis treatment.
Gore has announced the acquisition of InnAVasc Medical, a privately held medical technology company focused on advancing care for patients with end-stage renal disease who utilise graft circuits for dialysis treatment.
 Fluidx Medical disclosed study results examining extent of vessel filling using the
Fluidx Medical disclosed study results examining extent of vessel filling using the 






 for Turbo-Elite laser atherectomy catheter reprocessing")
 Northeast Scientific, a company that reprocesses single-use peripheral vascular catheters, announced recently in a press release that it has received US Food and Drug Administration (FDA) clearance for reprocessing the Philips Spectranetics 0.9mm over-the-wire Turbo-Elite laser
Northeast Scientific, a company that reprocesses single-use peripheral vascular catheters, announced recently in a press release that it has received US Food and Drug Administration (FDA) clearance for reprocessing the Philips Spectranetics 0.9mm over-the-wire Turbo-Elite laser 






 for new Soldier high-flow microcatheter")








 clearance for the Dabra 2.0 catheter")
 Ra Medical Systems has announced receipt of US Food and Drug Administration (FDA) 510(k) clearance for the company’s Dabra 2.0 catheter as part of the Dabra excimer laser system. A company press release details that the catheter features enhancements including a braided overjacket design that is intended to improve deliverability and kink resistance when navigating tortuous anatomy, as well as a six-month shelf life.
Ra Medical Systems has announced receipt of US Food and Drug Administration (FDA) 510(k) clearance for the company’s Dabra 2.0 catheter as part of the Dabra excimer laser system. A company press release details that the catheter features enhancements including a braided overjacket design that is intended to improve deliverability and kink resistance when navigating tortuous anatomy, as well as a six-month shelf life.
 Konica Minolta Healthcare Americas has announced that the company’s Dynamic Digital Radiography (DDR) technology, enabling the visualisation of anatomy
Konica Minolta Healthcare Americas has announced that the company’s Dynamic Digital Radiography (DDR) technology, enabling the visualisation of anatomy 


 Among the most popular pieces from last month are reports on papers delivered at the
Among the most popular pieces from last month are reports on papers delivered at the 
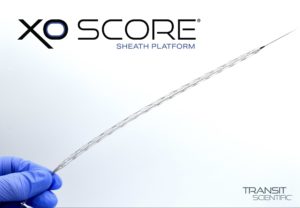





 with Yttrium-90 in paediatric primary liver tumours")









 TriSalus’ clinical leadership team presented new preclinical data at the Society of Interventional Radiology (SIR) 2022 Annual Scientific Meeting (11–16 June, Boston, USA). The data are the result of evaluations of the company’s immunotherapy platform, which integrates an investigational class C toll-like receptor 9 (TLR9) agonist,
TriSalus’ clinical leadership team presented new preclinical data at the Society of Interventional Radiology (SIR) 2022 Annual Scientific Meeting (11–16 June, Boston, USA). The data are the result of evaluations of the company’s immunotherapy platform, which integrates an investigational class C toll-like receptor 9 (TLR9) agonist, 






 SoniVie recently announced that on 5
SoniVie recently announced that on 5 


 Artio Medical today announced the closing of US$28 million in oversubscribed Series A2 and Series A3 financing, bringing the total amount raised by the company to date to US$74 million.
Artio Medical today announced the closing of US$28 million in oversubscribed Series A2 and Series A3 financing, bringing the total amount raised by the company to date to US$74 million.












 Arjo has announced the development of a new intraoperative Doppler system that includes a single-use, sterile intraoperative probe and Dopplex DMX Vascular Doppler.
Arjo has announced the development of a new intraoperative Doppler system that includes a single-use, sterile intraoperative probe and Dopplex DMX Vascular Doppler.



defining curative intent for HCC")









 The Royal Australian and New Zealand College of Radiologists (
The Royal Australian and New Zealand College of Radiologists (


 Germany-based endovascular simulator supplier CATHI has joined forces with UK-based Vascular Simulation Solutions (VSS) to offer the world’s first online training masterclass using endovascular simulation coupled to a structured curriculum, the company said in a press release.
Germany-based endovascular simulator supplier CATHI has joined forces with UK-based Vascular Simulation Solutions (VSS) to offer the world’s first online training masterclass using endovascular simulation coupled to a structured curriculum, the company said in a press release.  A report from the American Venous Forum (AVF) 2022 meeting (23–26 February, Orlando, USA) on the comparative merits and demerits of dedicated and non-dedicated stents heads the list of Interventional News’ April
A report from the American Venous Forum (AVF) 2022 meeting (23–26 February, Orlando, USA) on the comparative merits and demerits of dedicated and non-dedicated stents heads the list of Interventional News’ April 










