
 Tim Wittig (Leipzig, Germany) has shared primary outcomes from MOTIV-BTK as a podium-first presentation at the 2026 Charing Cross (CX) Symposium (21–23 April, London, UK). This prospective, multicentre, single-blind randomised controlled trial is designed to assess the Motiv sirolimus-eluting bioresorbable scaffold (Reva Medical).
Tim Wittig (Leipzig, Germany) has shared primary outcomes from MOTIV-BTK as a podium-first presentation at the 2026 Charing Cross (CX) Symposium (21–23 April, London, UK). This prospective, multicentre, single-blind randomised controlled trial is designed to assess the Motiv sirolimus-eluting bioresorbable scaffold (Reva Medical).
During a session focused on the latest data for drug-eluting resorbable scaffolds (DRS) in lower-limb disease, Wittig shared that the objective of MOTIV-BTK was to evaluate the safety and efficacy of the Motiv scaffold for the treatment of infrapopliteal lesions in patients with chronic limb-threatening ischaemia (CLTI) by randomised comparison with standard balloon angioplasty.
The presenter detailed that the trial, which involved 45 investigational sites across the USA and Europe, included a total of 292 patients presenting with Rutherford category 4 or 5. Patients were randomised 1:1 to treatment with either the Motiv bioresorbable scaffold or percutaneous transluminal angioplasty (PTA) with a standard uncoated balloon.
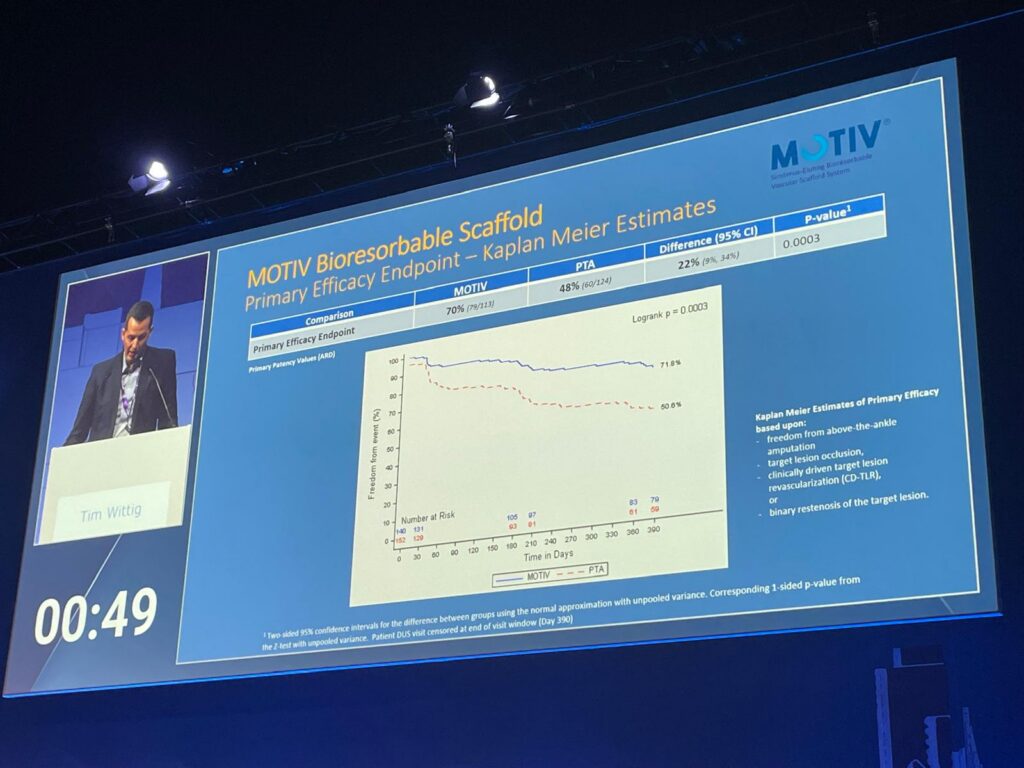
With regard to endpoints, Wittig outlined the primary safety endpoint as freedom from major adverse limb events (MALE) and all-cause perioperative death, evaluated at 30 days. This was defined as freedom from the composite of all-cause death, above-the-ankle amputation, or major reintervention of the index limb involving the infrapopliteal arteries. Continuing, the presenter noted that the primary efficacy endpoint was a composite of limb salvage and primary patency, evaluated at one year, defined as freedom from above-the-ankle amputation, target-lesion occlusion, clinically driven target-lesion revascularisation, or binary restenosis of the target lesion.
Delving into the details of patient clinical follow-up for the trial’s intention-to-treat population, Wittig shared that, of the 192 patients randomised to either Motiv (140) or PTA (152), the respective figures at six-month follow-up were 132 and 142, dropping to 128 and 135 at the one-year mark.
On key baseline demographics, historical risk factors and lesion characteristics, Wittig noted that there were no statistically significant differences between the two arms.
Looking at the procedural endpoint data, Wittig pointed to a device success rate of 95.8% in the Motiv arm, as well as acute technical success and acute procedural success rates of 91.5% vs. 72.3% and 89.7% vs. 67.3% for the Motiv and PTA arms, respectively.
On safety, Wittig shared that early safety was preserved, with no perioperative deaths and no above-the-ankle amputations in either arm, in addition to very low major reintervention rates overall. He reported a 99.3% rate of freedom from MALE and perioperative death at 30 days in the Motiv arm compared to a figure of 98.6% in the PTA arm.
Furthermore, Wittig reported that primary efficacy was superior with Motiv, highlighting a 22% absolute risk difference between the 70% rate in the Motiv arm and the 48% rate in the PTA arm. The presenter shared a secondary efficacy endpoint rate of 81% in the Motiv arm compared to a 62% rate in the PTA arm, representing a 19% absolute risk difference. He elaborated that the superiority of Motiv over PTA was evident by six months, supporting an “early and clinically meaningful benefit”.
Concluding, Wittig stated that the primary efficacy endpoint of limb salvage and primary patency was found to be “clearly superior at 12 months” with a 22% absolute risk difference when compared to PTA.
The presenter stressed that the trial included more complex patients than prior bioresorbable scaffold below-the-knee (BTK) trials, with a higher average of 68.5% Rutherford category 5 patients as compared to LIFE-BTK (48.2%), a modestly longer lesion on average (54mm) compared to LIFE-BTK (44mm) and over 30% of enrolled patients presenting with total occlusions.
Furthermore, Wittig emphasised that early clinical benefit has been established with superiority demonstrated as early as six months and safety established throughout follow-up with non-inferiority to PTA.











