
This advertorial is sponsored by Merit Medical.

Conventional pre-shaped microcatheter technology has evolved over the last decade, yet significant limitations still exist. In particular, the shape of a standard microcatheter cannot be changed or manipulated while inside a patient’s vasculature. As a user of this innovative technology, Jason C Hoffmann (New York, USA) details his first-hand experience.
Selective cannulation of small arterial branch vessels for targeted/superselective angiography or embolization is commonly performed; however, conventional pre-shaped microcatheter use has limitations when in complex arterial vasculature, including tortuous or angulated vessels.
In these scenarios, the operator must often perform multiple microcatheter and wire exchanges to select the target vessel. This can take a considerable amount of time, require use of numerous devices, and may result in a substantial radiation dose to the patient and procedural staff. If the target vessel cannot be superselected, a less-targeted embolization must be performed, or the procedure is abandoned altogether. In either scenario, the case will take longer, with implications for increased cost and resource use, and has the potential for complications and untoward events.
The development of a steerable microcatheter (SwiftNINJA® steerable microcatheter; Merit Medical Systems) is an innovation that offers an alternative approach to selective cannulation. This technology represents a new class of device, designed with a tip that articulates up to 180 degrees in opposing directions, providing real-time ability to change the angulation of the microcatheter tip while navigating through the vasculature.
The device can be used with or without a microwire which allows the injection of contrast while advancing or manipulating the steerable microcatheter. In my experience, this consistently leads to efficient selective cannulation of small vessels throughout the body, with a level of steerability that simply is not provided by any pre-shaped conventional microcatheter.
I can also inject contrast while advancing or manipulating the steerable microcatheter, allowing for precise control and improved vessel targeting. Decreased time to target vessel selection can have multiple benefits for the patient, primary operator, and procedural staff in the room. Advantages include decreased procedure times, increased procedural efficiency, fewer microcatheter and microwire exchanges, reduced fluoroscopy times, and lower radiation exposure.
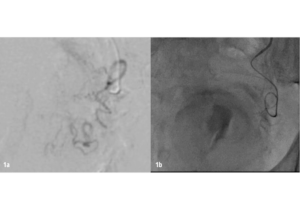
SwiftNINJA steerable microcatheter use in moderate and high complexity angiography and/or embolization has routinely helped me to be successful and efficient. In 2019, I published my results, comparing steerable microcatheter to conventional microcatheter use in 40 procedures that involved moderate to highly difficult vessel selection.1 Statistically significant improvements in target vessel selection time—12 vs. 462.5 seconds (Figures 1a-b)—number of microwires used (0 vs. 2), total procedure time (75 vs. 112.5 minutes), and body-mass index (BMI) adjusted radiation exposure were found in the steerable microcatheter group.
Since publishing my early steerable microcatheter results, I have used the device in hundreds of prostate artery embolization (PAE) procedures, as well as superselective embolization of distal hepatic, renal, bladder, visceral and small pelvic arterial branches in a variety of scenarios. Cases have included treatment of traumatic injury, benign prostatic hyperplasia (BPH), hematuria, malignancy and non-traumatic causes of bleeding. Most of these procedures were performed with only the steerable microcatheter, and no microwire was needed. I continue to find that patients and my team benefit from steerable microcatheter use due to increased efficiency, high technical success rates, reliable target vessel selection and decreased radiation exposure.
Reducing vessel selection time in a prostate artery embolization case
An 85-year-old man with a long-standing history of BPH presented with severe lower urinary tract symptoms (LUTS) and intermittent gross hematuria. Despite multiple medical treatments, including three transurethral resection of the prostate (TURP) procedures over the past two years, the patient’s condition had not improved. His International Prostate Symptom Score (IPSS) was 29 (severe), and his Urinary Quality of Life Score was 5 (unhappy).
Using a 2.4Fr SwiftNINJA through a 5Fr guide catheter, the left prostatic artery was selected in 12 seconds without a guidewire thanks to the steerability of the microcatheter tip. Proximal and then distal embolization of the left prostate artery with 300–500μ Embosphere microspheres (Merit Medical) was performed following the proximal embolization first, then embolize distal (PErFecTED) technique. The right prostate artery was then selected–again using the SwiftNINJA without a guidewire—in nine seconds and embolization was performed using the same technique.
Final angiography confirmed successful embolization of both left and right prostatic arteries. The patient was discharged the same day, with no hematuria or urinary retention reported since the procedure. At one month post-procedure, patient’s IPSS decreased from 29 to 7 and Urinary Quality of Life score decreased from 5 to 1.
Successful gonadal vein embolization through extremely tortuous anatomy
A 43-year-old female presented with chronic pelvic pain. Despite extensive diagnostic work-up, no definitive cause for the pain was found, except for prominent left parauterine veins/varicosities and an enlarged left ovarian vein.
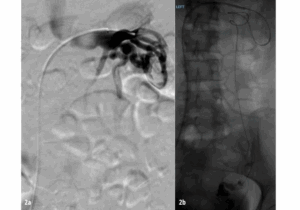
The patient was diagnosed with symptomatic pelvic venous reflux/pelvic congestion syndrome, and the plan was to proceed with venography and embolization. Due to extreme tortuosity of the gonadal venous vasculature preeminently, a 2.4Fr SwiftNINJA steerable microcatheter was used to efficiently navigate through the extremely tortuous vessels and into the inferior aspect of the left ovarian vein. Embolization was performed with sodium tetradecyl sulfate sandwiched in between packs of platinum microcoils.
Post-embolization digital subtraction venography demonstrated an appropriate angiographic result, with embolization of the left ovarian vein, but brisk antegrade blood flow in the left renal vein. The patient was discharged home in stable condition four hours post procedure, and experienced only mild flank discomfort for 24–36 hours post-procedure, relieved with ibuprofen. Her pelvic congestion syndrome symptoms markedly improved by the time she was seen for a post procedure office visit approximately six weeks later (Figure 2a-b).
References
- Hoffmann, J.C., Minkin, J., Primiano, N. et al. Use of a steerable microcatheter during superselective angiography: impact on radiation exposure and procedural efficiency. CVIR Endovasc 2, 35 (2019). https:// doi.org/10.1186/s42155-019-0078-9
Jason C Hoffmann is an interventional radiologist with NYU Langone Health in Mineola, New York, USA.









